Breathing mechanics
54
Moderator : Dr Padmanabha Presenter : Dr Nikhil mp
-
Upload
gaganbrar18 -
Category
Education
-
view
1.592 -
download
1
Transcript of Breathing mechanics

Moderator : Dr Padmanabha
Presenter : Dr Nikhil mp


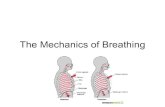
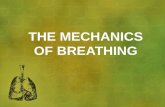
Diaphragm Dome shaped muscle . Inserted to lower rib. Phrenic nerve- C 3, 4, 5.. Abdominal contents are pushed
forward and downward & vertical dimension of chest cavity is increased.
Transverse diameter increased.

Paradoxical movement. External intercostals Ribs are pulled upward & forward
causing increase in lateral & AP of thorax.
“Bucket handle movement” “Pump handle movement”. Accessory muscles scalene & sternocliedomastoid.



Passive during quiet breathing. Active - exercise and hyperventilation. Muscles of abdominal wall. When muscles contract intraabdominal
pressure rise & diaphragm is pushed upwards.

Movements of lung is passive.
Impedence of the respiratory system.
Elastic resistance. Non elastic resistance.

Lung & chest wall.
Surface forces at alveolar gas liquid interface.

Lungs and chest have elastic properties.
Chest has tendency to expand.
Lungs have tendency to collapse .
Recoil properties of chest due to components that resist deformation.
In case of lung - elastin fibres & surface tension forces acting at air fluid interface.

Elastic recoil of the lungs is measured in terms of compliance.
Compliance is defined as change in lung volume per unit change in transmural pressure gradient.
150 to 200ml/cm H2O. Static . Dynamic. Stiff lungs have low compliance.

Reduced compliance fibrosis. alveolar edema.
Increased compliance emphysema. aging .

Previously – elastin fibres.
Von-Neergaard – surface tension acting at the air water interface lining the alveoli.

Surface tension at an air-water interface produces forces that reduce the area of the interface.
Alveoli can be compared to a bubble. Gas pressure within the bubble is higher
than the sorrounding. Laplace equation, P= 2T/R P=Pressure within the bubble T =surface tension R = radius of bubble


Low surface tension of alveolar lining fluid and its dependance on alveolar radius – surfactant.
Alveolar epithelial cells- type II.
90% lipids & rest protiens and carbohydrate.
Dipalmitoyl phosphatidyl choline.

To maintain the stability of alveoli.
Immunology of the lung.


Most Frictional resistance to air flow.
Thoracic tissue deformation.

Gas flows from area of high pressure to area of low pressure
The rate at which it does is a function of the pressure difference and the resistance to gas flow

2 types
Laminar flow
Turbulent flow

Gas flows along a straight unbranched tube as a series of concentric cylinders that slide over one another,with peripheral cylinder stationary and central fastest,advancing cone forming a parabola



FG will reach end of the tube while volume entering the tube is less than the volume of the tube
Significant alveolar ventilation tidal volume < volume of the
airways

Friction between tube wall and fluid is negligible.
Significant alveolar ventilation when the tidal volume < the volume of airways.

Inefficient for purging the contents of the tube.
Gas sampled from periphery may not be representative of the gas in the centre.
Requires a critical length of tubing before typical flow pattern .

Gas flow is proportional to pressure gradient and constant being resistance to gas flow.
∆ P =flow x resistance.
∆ P = pressure gradient.

Hagen-poiseuille eqn,gas flow in straight unbranched tube
Pressure G X ∏ X r4Flow rate= 8 X length X viscosity

8 X length X viscosity Resistance = ∏ X radius4
Viscosity is the only property of gas relevant in laminar flow

High flow rates. Branched or irregular tubes. Sharp angles Irregular movement of gas molecules . Square front replaces cone front.



No FG can reach the end of the tube until amount of gas entering the tube is equal to the volume of the tube.
Frictional forces are important.

More effective in purging the contents of the tube.
Best conditions for drawing a representative sample of gas.

Driving pressure is proportional
To the square of the gas flow.
Density of gas.
Inversely proportional to the fifth power of radius.
Independent of viscosity.

The nature of gas flow .
Linear velocity of gas X tube diameter X gas density
gas viscosity
< 2000 - laminar. > 4000 - turbulent. Both between 2000 - 4000. Low resistance . Establishment of laminar flow faster.


Frictional resistance
In healthy people,Larger airways responsible
Smaller airways : small contribution

Velocity of gas flow & airway diameter decreases in successive airway generations.
Entrance length greater. Frequent divisions.

Gas mixtures having low Reynolds number beneficial in large airway disease.
Physical characteristics of airway lining will influence frictional resistance.

Primarily due to viscoelastic resistance.
Lung & chestwall tissues.

Airway diameter Physical compression Contraction of smooth
muscles

Effect of lung volume on resistance to breathing
Airway resistance is an inverse function of lung volume
At low lung volume ,flow related airway collapse occurs
Expiratory airway collapse Valve effect Gas trapping
CPAP & PEEP

Closing capacity Lung volume at which airways in
the dependant part of the lung begins to close.
Closing volume = closing capacity –
RV.

< FRC in young adults.
Equal to FRC at 44 yrs in supine position & 66yrs in upright position.
When FRC < closing capacity SHUNT.

Reversal of normal transmural pressure gradient
During maximal forced expiration –intrathoracic pressure is above atmospheric pressure
Pressure drops equal pressure point
Downstream transmural pressure is
reversed Airway collapse



When expiration is passive
Work of breathing is done by inspiratory muscles.
Half dissipated as heat & half stored as PE.
PE is available for expiration.

Actual work by respiratory muscles is small.
02 consumption – 3ml/min.
Efficiency is 10%.
When maximum ventilation is approached efficiency falls to lowest level.

Work done to overcome elastic resistance increases as tidal volume increases.
Work done to overcome airflow resistance increases as RR increases.

Nunn’s respiratory physiology,6th edition.
Respiratory physiology ,JOHN B .WEST,8th edition.
Millers anaesthesia,6th edn.
Clinical anaesthesiology,G.Edward morgan,4th edn.