Breastfeeding Practice and Breastfeeding Self-efficacy Among first time Nepalese Adolescent Mothers
35
-
Upload
ambika-rai -
Category
Health & Medicine
-
view
99 -
download
3
Transcript of Breastfeeding Practice and Breastfeeding Self-efficacy Among first time Nepalese Adolescent Mothers


Background & Significance Background & Significance
Gap of Knowledge
Research Objectives & Questions
Research HypothesisResearch Hypothesis
Definition of Terms
Literature Review
Expected Benefits
Timeframe of the Study
Methodology
Conceptual Framework
Outline
References

Background and significance
Breastfeeding practice is divided by WHO (2002, 2009) into 3 types:
1) Exclusive breastfeeding refers to the practice of a mother in providing infants only her breast milk. No other liquids or solids are given – not even water – with the exception of oral rehydration solution, or drops/syrups of vitamins, minerals or medicines or breast milk; 2)
2) Partial breastfeeding refers to practice of a person giving a baby some breastfeeds, and some artificial feeds, either milk or cereal, or other food; 3)
3) No breastfeeding refers to a practice of a mother in providing her infant formula or non maternal expressed milk. In this study, maternal breastfeeding practice will be measured by breastfeeding practice questionnaire using open ended and closed questions (Yimyam, 2013).

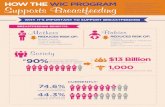
Benefits of breastfeeding

Recommendation
☺World Health Organization (WHO) and the United Nations International Children's Fund (UNICEF) recommended the practice of breastfeeding and state that “breastfeeding is an unequalled way of providing ideal food for growing infants’’.
☺As a global health recommendation, infants should be exclusively breastfed for the first six months of their lives followed by continued breastfeeding for up to two years to achieve optimal growth, development and health of the infant (WHO, 2007; 2009; UNICEF, 2013).
Recommendation

Glo
ba
l bre
as
tfee
din
g s
itua
tion
Worldwide, only 40% of newborns were breastfed within the first hour of birth,
Nearly same proportion(38%) of infants were breastfed until the age of six months (WHO, 2002).
In 2012, 85 million newborns failed to receive breastfeeding at the first six month of life,
Half of them (40 million) were from Asia.
In South Asia, the percentage of Infants who are breastfed within one hour of birth was 78% & at six months was 65% (UNICEF, 2013a; WHO, 2014b).


Duration Exclusive Breastfeeding
Partial Breastfeeding
At birth 74% 15%
At one month 78% 38%
At six month 53% 69-79%
(Nepal demographic health survey [NDHS], 2011;Ulak, Chandyo, Mellander, & Shrestha, 2012).
The Breastfeeding rates in Nepal

What are Influencing factors?

Situation of adolescent mothers Situation of adolescent mothers in Nepalin Nepal
According to the World Health Organization (WHO),
adolescence is a transition stage between childhood and
adulthood.
Age between 10 to 19 years is considered to be the critical
phase in this transition (WHO, 2014).
Nepalese girls often get married at an early age:
41% to 52.3% girls in Nepal get married before or at the age
of 18 years (Maharjan, Karki, Shakya, & Aryal, 2012; Nepal demographic
health survey [NDHS], 2011) and
17% of girls under the age of 20 years had already given
birth or were pregnant with their first child (NDHS, 2011).
According to the World Health Organization (WHO),
adolescence is a transition stage between childhood and
adulthood.
Age between 10 to 19 years is considered to be the critical
phase in this transition (WHO, 2014).
Nepalese girls often get married at an early age:
41% to 52.3% girls in Nepal get married before or at the age
of 18 years (Maharjan, Karki, Shakya, & Aryal, 2012; Nepal demographic
health survey [NDHS], 2011) and
17% of girls under the age of 20 years had already given
birth or were pregnant with their first child (NDHS, 2011).

However, maternal age maternal age (Ajibade, et.al., 2013; Nadler, 2007; Shetty &
Shetty, 2013; Atuyambe, et.al, 2008; Infant Feeding Surveillance System [IFSS], 2012)
and and breastfeeding self–efficacy breastfeeding self–efficacy (Dennis, 2002; Blythe, et.al., 2004;
Britton, et.al.,2007; Meedya, Fahy & Kable, 2010) have been identified as the
key factors for breastfeeding practice key factors for breastfeeding practice among mothers
where adolescent mothers’ breastfeeding practice duration
were shorter compared to adult mothers (Blyth et al., 2002; Santo, 2007;
Mossman, et.al., 2008; Beattie–Fairchild & Dennis, 2013; Yimyam, 2013).

In Nepal....
Similarly, Nepalese adolescentadolescent mothers' breastfeeding
practice has been significantly lower than significantly lower than adult mothers (Aryal,
2007; Khanal, Adhikari, Sauer, & Zhao, 2013) due to lack of breastfeeding skill,
knowledge and confidence in breastfeeding (Khanal et.al, 2013).
Studies support that there could be numerous other factors to
this, however, self–efficacy and maternal age self–efficacy and maternal age play the most
significant role in breastfeeding practice and efficiency among
young mothers.

Gap of knowledge
Most of the studies conducted to investigate maternal
breastfeeding self–efficacy and breastfeeding practice
among adolescent mothers (Blythe, 2002; Mossman, et.al, 2008; Beattie–
Fairchild & Dennis, 2013) have been carried out in different countries
with different cultural and socio–economic contexts to
Nepal. Thus, the studies could be territorial; both culturally
and geographically, and thus difficult to generalize.
Equally, those studies that were conducted in Nepal were
conducted only among general population (Keller, 2010; Khanal et Al.,
2013; Shrivastava, Singh, & Shah, 2013; Paudel & Giri, 2014).

Cont.. The results from the study of general population may not give
true picture or explain the situation of Nepalese Adolescent
mothers’ breastfeeding practice and breastfeeding self–
efficacy.
Therefore, this study aims to explore and compare
breastfeeding self efficacy among Nepalese adolescent
mothers who provide different types of infant feeding during the
first six weeks of postpartum life.
The results can be used as a baseline information for
breastfeeding policy makers and related health centres in order
to develop proper strategies to improve breastfeeding practice
among Nepalese adolescent mothers.

Objectives of the Study
To describe breastfeeding practice at six
weeks of postpartum among adolescent mothers
in Nepal
To compare the differences in breastfeeding
self-efficacy among adolescent mothers with
exclusive, partial and no breastfeeding practice
at six weeks in Nepal
Objectives of the study

Research QuestionsResearch questions
How do adolescent mothers in Nepal breastfeed
their infants at six weeks of postpartum?
Are there any differences in breastfeeding self-
efficacy among adolescent mothers with exclusive,
partial and no breastfeeding practice at six weeks?

Breast feeding self-
efficacy level is different
among adolescent mothers
practicing exclusive, partial
and no breastfeeding feeding.

Definition of Terms
Breastfeeding
Practice
Breastfeeding Self-
efficacy
Adolescent Mother
Definition of terms

Breastfeeding practice
Breastfeeding practice is the feeding activities of an infant with breast milk at six weeks of postpartum period (UNICEF, 2013). Breastfeeding practice is divided into 3 types defined by WHO (2002,
2009) as: 1) Exclusive breastfeeding 1) Exclusive breastfeeding refers to the practice of a mother in providing infants only her breast milk. No other liquids or solids are given – not even water – with the exception of oral rehydration solution, or drops/syrups of vitamins, minerals or medicines or breast milk. 2) Partial breastfeeding 2) Partial breastfeeding refers to practice of a person giving a baby some breastfeeds, and some artificial feeds, either milk or cereal, or other food. In this study, partial breastfeeding will be refers as mother in providing her infant with her breast milk together with non human milk or formula including additional solid or semisolid any food or liquid. 3) No breastfeeding 3) No breastfeeding refers to a practice of a mother in providing her infant formula or non maternal expressed milk.
In this study, maternal breastfeeding practice will be measured by breastfeeding practice questionnaire using open ended and closed questions (Yimyam, 2013).

Breastfeeding self-efficacyBreastfeeding self-efficacy
refers to a mother’s confidence in her ability to breastfeed her
infant(Dennis, 1999). In this study, maternal breastfeeding self-efficacy
will be measured by Dennis breastfeeding self-efficacy short-form
scale (BSES-SF) (2003).
Adolescent MothersAdolescent Mothers
refers to first time Nepalese women who have given birth at the
age under of 20 years.

8.1 Definition and benefits of breastfeeding8.2 Global situation and trends8.3 Influence on breastfeeding initiation 8.4 Breastfeeding practice among adolescent mothers 8.5 Breastfeeding Self-Efficacy 8.5.1 Definition and concept 8.5.2 Measurement of breastfeeding self-efficacy 8.5.3 Breastfeeding Self-Efficacy and breastfeeding
practice8.6 Breastfeeding practice among adolescent mothers in
Nepal 8.6.1 Adolescent mothers in Nepal 8.6.2 Breastfeeding practice among Nepalese adolescent
mothers 8.6.3 Measurement of Breastfeeding practice

• The study conceptual framework is based on Bandura's
self-efficacy theory (1977), and other literature reviews.
According to Bandura, human behaviour is predicted by
overall self-efficacy of an individual. Dennis (2002)
concluded this theory with breastfeeding behaviour of
mothers. It states that mothers with higher self-efficacy
have higher rate of breastfeeding practice compared to
mothers with lower self-efficacy, and mothers who
perform different types of breastfeeding practice have
different level of self-efficacy.

Methodology

Design Descriptive Comparative Study Descriptive Comparative Study
Population Nepalese adolescent mothers Nepalese adolescent mothers attending the Baby Clinic in Paropakar Maternity and Women's hospital with six week old
healthy babies.
Sample Size o Power analysisPower analysis; alpha level of α = 0.05 and power test (1– β) of 0.80 (Polit & Hungler, 1999). The population effect size of 0.3 is estimated as medium size (Cohen, 1990). The calculated sample size was 88, but in anticipation of possible 20% loss of subjects 22 more samples were added bringing the final sample population to 110.
Sampling Method
o Purposive sampling method Purposive sampling method (January 2015 clinic record shows that the total number of mothers visiting the clinic was 70 – 100 per day).
Inclusion Criteria
Mother with at least six weeks old healthy infants. No maternal and infant complications that interferes with
breastfeeding. Infant with normal birth weight of at least 2,200 – 4,000 grams. Mothers who are willing to participate, and are able to read and
write Nepali language.
Research Settings
o Well Baby Clinic in Paropakar Maternity and Women's hospital, Kathmandu, Nepal

Research Instruments
Breastfeeding Self-efficacy Short Form Scale
Breastfeeding Practice
1
2
3

Personal Data Profile containing closed ended and open
ended questions on demographic data including maternal
age, maternal education, and maternal occupation, family
income, and characteristics of family, numbers of family
member as well as pregnancy and childbirth history
including parity, and gestational age, complications during
pregnancy, labour and postpartum
The Breastfeeding Self Efficacy– Short Form (2002)
- 14 self report questionnaire
- 5 point Likert type scale
-Score with a possible range from 14 – 70
-All items preceded by the phrase "I can always"

The Breastfeed Practice (2013)The modified breastfeeding practice form is based on Boundary points cut-offs and preposition breastfeeding practices tool (Yimyam, 2014) consists of six open ended and closed ended preceding with;1. Have you ever breastfeeding your infant?2. Are you still be breastfeeding?3. When did you start and stop breastfeeding?4. Are there other milk or any foods or water that you gave to your infant?5. What are those foods and supplements?6. When did you start and stop to give those foods and supplents?
From mothers’ response, breastfeeding practice will be
classified into three groups:
a) exclusive breastfeeding
b) partial breastfeeding
c) no breastfeeding


Why Breastfeeding Practice tool?
It is useful to measure breastfeeding practice at a particular age of infant
It helps to distinguish either postpartum mothers are breastfeeding and not breastfeeding their infants
It helps to classify the types of breastfeeding practice among mothers

Psychometric properties Psychometric properties of questionnaire of questionnaire
Test of Validity

Test of Reliability

Da
ta co
llect io
n p
roc
edu
re
Research proposal will be submitted & reviewed by ethical committees.
Letters from the dean of FON will be issued & related documents will be submitted to the Paropakar maternity and women's hospital in Nepal and Paropakar well baby unit of the hospital.
Request for data collection and explanation about the study will be submitted to hospital Directors and Nursing Supervisors from selected units.
Samples will be approached based on medical records & inclusion criteria.
Verbal information about the study will be given to the samples if they meet the criteria and are willing to participate in the study.
• Face to face interview will be carried out.•Consent will be obtained and then questionnaires distributed.
•Clarification on questions will be made on request. •Responses will be collected.

Data analysis procedure

Expected benefits

Thank You