Breast feeding -...
20
FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010 1 BREAST FEEDING 'Exclusive breastfeeding’ means that not giving any prelacteal drinks including honey, water, 'holy' or ritually blessed water, sugar or glucose water, gripe water,juices,vitamins or foods other than breast milk, for the first six months. Principles of successful breastfeeding are: All expectant mothers should be motivated and prepared for Breast feeding, at the time of antenatal visits. Starting to breastfeed within an hour after birth - this ensures that the infant receives colostrums. Breastfeed on demand, whenever baby cries for it, and continue feeding as long as baby wants it. Proper latching to the breast with complete lip seal along the areola is must for effective feeding. Feed from both breasts; feed both fore milk and hind milk. The frequency and duration of feeding proportionately determines the milk output. To prevent abdominal distension,colics,and regurgitation, burp well after each feed Not giving any other food or fluids such as water or infant formula during the first six months. Breast feeding positions: Position Situation Lateral position feeding Post operatively Foot ball position In twins, hypotonic baby Cradle position Premature or small weight babies Sitting with back rest Any baby Colostrum For the first 72 hours after the delivery breasts secrete thick, sticky and yellowish in colour milk known as colostrum. It is easily digestible, contains more proteins and vitamins A& K, anti- infective elements to protect your newborn against infections. Although colostrum is secreted in small quantities (30-90ml), it is sufficient to meet the energy needs of a normal newborn during the first few days of life.
Transcript of Breast feeding -...

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
1
BREAST FEEDING
'Exclusive breastfeeding’ means that not giving any prelacteal drinks including honey, water,
'holy' or ritually blessed water, sugar or glucose water, gripe water,juices,vitamins or foods other
than breast milk, for the first six months.
Principles of successful breastfeeding are:
All expectant mothers should be motivated and prepared for Breast feeding, at the time of
antenatal visits.
Starting to breastfeed within an hour after birth - this ensures that the infant receives
colostrums.
Breastfeed on demand, whenever baby cries for it, and continue feeding as long as baby
wants it.
Proper latching to the breast with complete lip seal along the areola is must for effective
feeding.
Feed from both breasts; feed both fore milk and hind milk.
The frequency and duration of feeding proportionately determines the milk output.
To prevent abdominal distension,colics,and regurgitation, burp well after each feed
Not giving any other food or fluids such as water or infant formula during the first six
months.
Breast feeding positions:
Position Situation
Lateral position feeding Post operatively
Foot ball position In twins, hypotonic baby
Cradle position Premature or small weight babies
Sitting with back rest Any baby
Colostrum
For the first 72 hours after the delivery breasts secrete thick, sticky and yellowish in colour milk
known as colostrum. It is easily digestible, contains more proteins and vitamins A& K, anti-
infective elements to protect your newborn against infections. Although colostrum is secreted in
small quantities (30-90ml), it is sufficient to meet the energy needs of a normal newborn during
the first few days of life.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
2
Benefits of breast feeding:
Benefits to mother Benefits to baby
Easy, readymade, complete and
economical and comfortable. Can be
given at any time, anywhere in any
position.
Breast feeding stimulates secretion of
oxytocin which helps the uterus to
contract and control post partum
bleeding.
Frequent nursing suppresses ovulation
through prolactin secretion, and
provide protection against another
pregnancy.
Lower risk of breast and ovarian
cancer
Make night feeds and travel convenient
Attachment between mother and child
helps in bonding.
Right amount of fatty acids, lactose,
water, and amino acids for human
digestion, brain development, and
growth
Human milk transfers to the infant a
mother's antibodies to disease; hence
it’s a custom-designed to fight the
diseases.
Breast-fed baby's digestive tract
contains large amounts of
Lactobacillus bifidus, beneficial
bacteria that prevent the growth of
harmful organisms.
Attachment between mother and child
helps in bonding.
Benefits to society
Contributes to child survival
Decreases health care cost
Contributes to population control by natural way
Breast feeding - mothers with special needs
A. Maternal illnesses
Tuberculosis Treat mother, initiate and continue breast feeding, treat baby with
prophylactic dose of INH, if mother is a case of open tuberculosis.
Diabetes Initiate and continue breast feeding
Epilepsy No contraindications.
Hepatitis -B Risk of transmission should be weighed against the risk of developing
other infections and allergies. Initiate and continue breast feeding, treat
baby with Hepatitis immunoglobulin and vaccine.
HIV infection HIV virus can pass through breast milk & could be responsible for up
to 10% of the causes of mother to child transmission. However in
cases where the woman cannot afford top feeds, breast feeding is
recommended since the mortality from gastrointestinal infection is
high.
Herpes No contraindications. temporary discontinue if lesion on breast

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
3
B. Medicines and Nursing Mothers
Most medications have not been tested in nursing women, so no one knows exactly how a given
drug will affect a breast-fed child.
Drugs that are safe for nursing Drugs to be given with caution
in nursing or avoid
Drugs that are contraindicated
for nursing
Acetaminophen
Antiepileptics (although
one, Primidone, should
be given with caution)
most antihistamines
Alcohol in moderation
most antihypertensives
Aspirin (should be used
with caution)
Caffeine (moderate
amounts in drinks or
food)
Codeine
Decongestants
Ibuprofen
Insulin
Quinine
Thyroid medications
Amiodarone
Anthroquinone
Atropine
Aspirin
Birth control pills
Bromides
Calciferol
Dyhydrotachysterol
Metoclopramide
Metronidazole
Phenobarbitone
Primidone
Sulfasalazine
Reserpine
Bromocriptine
Chemotherapy Drugs
Ergotamine
Lithium
Methotrexate
Drugs of Abuse
Tobacco Smoke
Amphetamines
Chloramphenicol
Cimetidine
Clemastine
DES
Gold
Iodides, thyuracil
Meporbamate
Nicotine
Tetracycline
Phenindione
References:
1. Training manual on breastfeeding management-United Nations Children Fund.
2. BPNI(breast feeding promotion network of India) training module
3. BPNI website - http://www.bpni.org/breastfeeding/goodness
FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
4
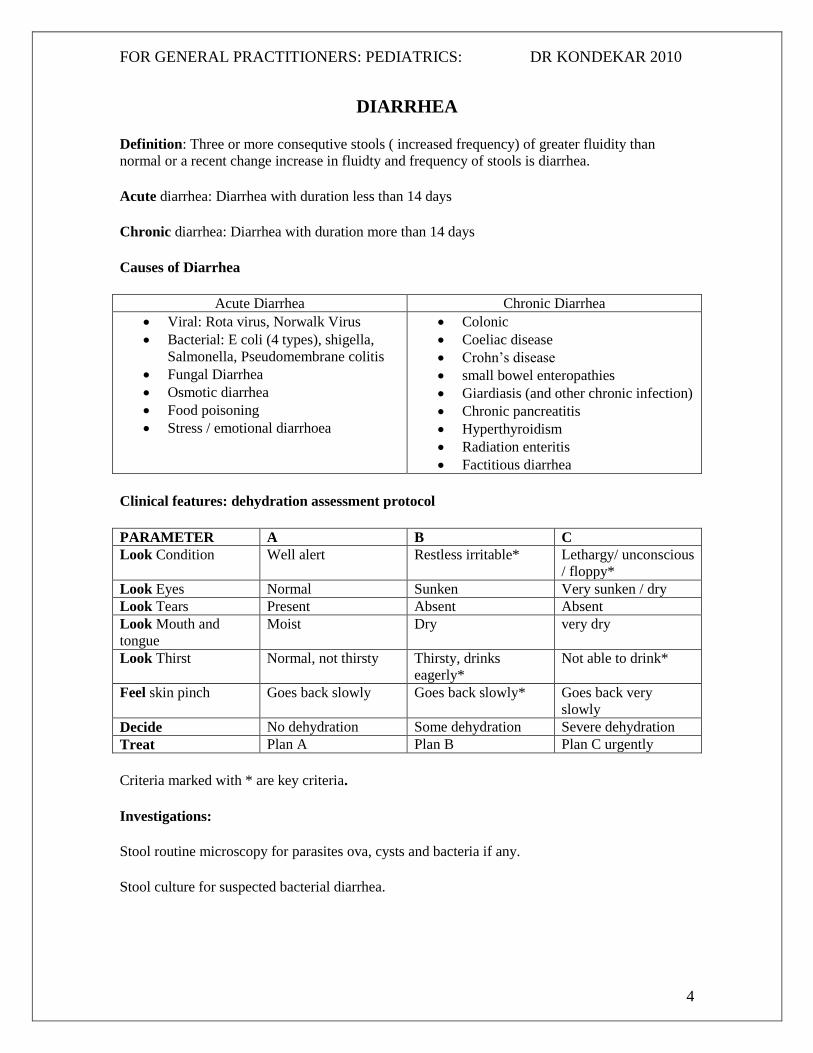
DIARRHEA
Definition: Three or more consequtive stools ( increased frequency) of greater fluidity than
normal or a recent change increase in fluidty and frequency of stools is diarrhea.
Acute diarrhea: Diarrhea with duration less than 14 days
Chronic diarrhea: Diarrhea with duration more than 14 days
Causes of Diarrhea
Acute Diarrhea Chronic Diarrhea
Viral: Rota virus, Norwalk Virus
Bacterial: E coli (4 types), shigella,
Salmonella, Pseudomembrane colitis
Fungal Diarrhea
Osmotic diarrhea
Food poisoning
Stress / emotional diarrhoea
Colonic
Coeliac disease
Crohn’s disease
small bowel enteropathies
Giardiasis (and other chronic infection)
Chronic pancreatitis
Hyperthyroidism
Radiation enteritis
Factitious diarrhea
Clinical features: dehydration assessment protocol
PARAMETER A B C
Look Condition Well alert Restless irritable* Lethargy/ unconscious
/ floppy*
Look Eyes Normal Sunken Very sunken / dry
Look Tears Present Absent Absent
Look Mouth and
tongue
Moist Dry very dry
Look Thirst Normal, not thirsty Thirsty, drinks
eagerly*
Not able to drink*
Feel skin pinch Goes back slowly Goes back slowly* Goes back very
slowly
Decide No dehydration Some dehydration Severe dehydration
Treat Plan A Plan B Plan C urgently
Criteria marked with * are key criteria.
Investigations:
Stool routine microscopy for parasites ova, cysts and bacteria if any.
Stool culture for suspected bacterial diarrhea.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
5
Treatment:
Management of dehydration
Plan A: counsel the parents regarding
Continued feeding
Extra fluids for large volume diarrhea
Identify and return for medical advice if signs or symptoms of
dehydration.
Extra fluids in the form of WHO ORS, plain water soup, rice water and
yoghurt. Amount to be given <2 yrs, 50-100 ml per large stool and above
2 yr age 100-200 ml ORS per large stool.
Plan B:
The formula for ORS recommended by WHO and UNICEF contains:
3.5 gms gms sodium chloride (common salt)
2.9 gms trisodium citrate dihydrate
1.5 gms potassium chloride
20 gm glucose (anhydrous)
The above ingredients are dissolved in one liter of clean water.
Amount of ORS to be given in first 4-6 hours
Age Up to 4 months 4-12 months 1-2 yrs 2-5 yrs
Weight <6 kg 6-10 kg 10-12 kg 12-19 kg
Ml of ORS 200-400 400-700 700-900 900-1400
In absence of ORS, dehydration can be prevented by making ORS by adding 1 level teaspoon (5
ml) of salt should be mixed with 8 level teaspoons of sugar in a litre of drinking water
administered orally by parents in the child's own home.
If dehydration persists, large volume stools continue, vomiting and abdominal distention is
present and / or urine out put has not picked up, hospitalize the child and change to plan C.
Plan C:Start the child on IV fluids gives 100ml/kg of Ringer’s Lactate/ Normal saline as below:
Age First give 30ml/kg in Followed by 70ml/kg in
Infant 1 hour 5 hours
1-5 years 30 minutes 2.5 yrs
Reassess the child every 2 hrs and if dehydration persists, fluid rate may be increased, and if
dehydration settles, gradually ORS to be introduced as soon as child can drink.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
6
Indications for antibiotics:
Amebiasis: Metronidazole 30mg/kg/day in divided doses for 10 days
Bacillary dysentery: Septran 6 mg/kg/day for 7 days, or cephalosporins like cefixime
10mg/kg/day for 7 days.
References:
1. Essential Pediatrics, Ghai O. P., 3rd edition, 193-195
2. Please see the link - http://rehydrate.org/dd/su19.htm

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
7
IMMUNISATION
National Immunisation Schedule:
Age Vaccines
Birth BCG OPV0
6 weeks DTP1, OPV1 ( and BCG if not given earlier)
10 weeks DTP2 OPV 2
14 weeks DTP3 OPV3
9 months Measles
16-24 months DTP OPV
5-6 years DT*
10 years TT**
16 years TT
For pregnant women
Early in pregnancy TT1 or booster
One month after TT1 TT2
* If primary immunization history is not available, second dose of DT may be given after
a month.
** If primary immunization history is not available, second dose of TT to be given after 1
month.
IAP also recommends inclusion of hepatitis –B, MMR, Typhoid and Haemophilus
Influenzae b in the time table. However, in view of the mild nature of chickenpox and
hepatitis A, these two are recommended as additional vaccines.
Indian Academy of Pediatrics recommends their members to prescribe additional
vaccines to their child patients depending upon the availability at the vaccines and the
affordability of the patents. However, it is mandatory to administer all the UIP vaccines
as a priority.
IAP Immunization guidelines:
1. To prevent perinatal transmission, birth dose of Hepatitis B vaccine within 12 hours is
essential. BCG, OPV and Hepatitis B vaccines, when missed at birth can be started at the
completion of 6 weeks.
2. Combined DPTwc / Hepatitis B / Hib vaccines can be given at 6, 10, 14 weeks.
3. In addition to ‘Routine OPV doses’, the recommended ‘Pulse OPV doses’ are also
mandatory during PPI campaigns.
4. For Typhoid* immunization, earliest age recommended : whole cell vaccine at 6 months,
Vi antigen at 2 years and Oral Ty21a vaccine at 6 years. Revaccination every 3 years.
5. Apart from the earliest age indicated, MMR, Typhoid, Varicella and Hepatitis A can be
given at any age, relevant to local epidemiology.
6. Td (Tetanus / diphtheria toxoid) should be preferred to TT (Tetanus toxoid) where
available.
7. Varicella and Hepatitis A are additional vaccines as recommended by Indian
Academy of Pediatrics.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
8
Vaccination schedule for an unimmunised child
Age Less than 7 yrs More than 7 years
First visit BCG*, OPV*, DTPw/DTPa HB Td, HB
Second visit, 1 month later OPV*, DTPw/ DTPa, HB Td, HB
Third visit 1 month later Measles, MMR, typhoid MMR typhoid
Fourth visit, 6 months after first DTPw/ DTPa, HB HB
Every 3 years Typhoid Typhoid
*OPV BCG not after 5 yr age.
IAP recommendations for Immunisation of HIV infected children
Vaccine IAP recommendations
Asymptomatic HIV infection Symptomatic HIV infection
BCG Yes, at birth No
DTPw/DTPa Yes, at 6, 10 , 14 weeks Yes
OPV Yes, at 6, 10, 14 weeks Yes, IPV
Measles Yes at 6 & 9 months Yes
MMR Yes Yes CD4% > 15%
Hepatitis B Yes, as for uninfected children Yes, double each dose
Hib Yes Yes
Typhoid Vi Yes Yes
Pneumococcal Yes Yes
Influenza Yes >(6 month age) Yes
Varicella Yes (2 doses at 6-8 weeks interval) Yes (2 doses at 6-8 weeks interval) CD4>15%
Hepatitis A Yes Yes
References: 1.IAP committee on o immunization IAP Guidebook of immunization, 2005-2006
2. http://www.iapindia.org/circumstances.cfm

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
9
HELMINTHIASIS (WORM INFESTATIONS)
Mode of Infestation: feco-oral contamination through food/water/ soil
Problems: Malabsorption, blood loss, malnutrition and failure thrive and various vitamin and
mineral deficiencies, abdominal pain, diarrhea or constipation and failure to thrive
Whip worm:
Signs/ symptoms: Asymptomatic, bloody diarrhea, rectal prolapse, growth retardation,
malnutrition.
Treatment: Mebendazole 100mg twice a day for 3 days, for mo than 2 yrs age.
Albendazole 400 mg single dose for > 10 kg and 200 mg single dose for weight <10 kg
Mebendazole retention enema
Round worm: (Ascaris Lumbricoids)
Signs/ symptoms: vague abdominal pain, cough, eosoniphilia, bowel obstruction
Treatment: Elixir Piperacillin citrate 75mg/kg orally 2 days or Mebendazole 100mg BD for 3
days, or pyrantel pamoate 11 mg/kg single dose, or Albendazole 400mg single dose.
Hook worm: (Ankylostoma)
Signs/ symptoms: ground itch, intense pruritis, erythema, vesicular rash at the site of penetration,
chronic PEM, iron deficiency pneumonia
Treatment: Elixir Piperacillin citrate 75mg/kg orally 2 days or Mebendazole 100mg BD for 3
days, or pyrantel pamoate 11 mg/kg single dose, or Albendazole 400mg single dose. Plus iron
therapy 6mg/kg/day, ferrous sulphate.
Prevention: wearing footwear, avoid open air defecations
Pin worm: Enterobius vermicularis
Signs/ symptoms: age group 5-14 yrs, asymptomatic, or perianal or perineal pruritis
Treatment: Pyrantel Pamoate day 1 and day 14, or Mebendazole / albendazole and retreatment
after 2 weeks. Treat all family members simultaneously. Nails should be trimmed short.
Undergarments to be dried in sun, thorough cleaning of toilet seats, floors, discourage perianal
scratching
.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
10
Tape worm (Tinea solium)
Signs/ symptoms: occurs due to consumption of beef and pork infected with larvae. Avoid
unwashed raw vegetables.
Treatment: niclosamide 40mg/kg/dose f/b saline purges after 1hr. or praziquentel 10mg/kg/dose,
in cysticercosis; praziquentel 50mg/kg/day for 10 days
Albendazole 15 mg/kg/day for 28 days
SKIN INFESTATIONS
Dermatophytoses (ring worms)
These are caused by a group of closely related fungi with a propensity to invade the
stratum corneum, hairs, nails.
Tinea Capitis: Infection of the hair shaft and surrounding skin causing alopecia, brittle hairs.
Treatment : Oral griseofulvin microcrystaline
Tinea corporis : involves the skin of face, trunk and extremeties. The typical lesion starts as dry
and mildly erythematous, elevated, scaly papule and spreads centrifugally, clearing centrally.
Treatment : Topical antifungal- are effective.
Scabies
It’s caused by itch mite, Sarcaptos scabiei var, hominis. Usually transmitted by direct contact
with infected person. The eruption is highly pruritic and consists of burrows, wheals, papules,
vesicle, and eczematous dermatitis.
Treatment: application of 1% gamma benzene hexachloride or BB lotion to entire body below
neck, full family may be treated.
Pediculosis
Lice infests (head, body and pubic) hair. Body louse is also a vector for typhus, Trench fever.
Itching, Excoriations on the scalp, posterior neck, and upper back; bite reactions; secondary
bacterial infection; and cervical lymphadenopathy are common manifestations.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
11
Treatment: The goal of therapy is to eliminate lice and eggs.
Linen, clothing, and other materials may be treated with hot water washing.
Eyelash infestation can be treated effectively with petrolatum ointment (eg, Vaseline).
Permethrin 5% (Elimite) or 1% (Nix) lotion -- DOC, especially for infants >2 mo and
small children
Lindane 1% shampoo Not very safe in children due to transcutaneous absorption leading
to neurotoxicity
References:
1. Essential Pediatrics, Ghai O. P.,3rd edition
2. Textbook of pediatrics, Nelson, pocket companion, Indian ed ,454-455
3. http://www.emedicine.com/emerg/topic409.htm

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
12
Pneumonia or acute respiratory infection (ARI)
ARI is a major cause of mortality and morbidity in children below 5 yr age. Majority of ARI are
self limiting but pneumonia is a serious life threatening event with high fatality rate.
Sepctrum of ARI
Upper respiratory infection, common cold, pharyngitis and otitis
Lower respiratory infections: bronchitis, bronchiolitis, pneumonia
Clinical assessment:
History: Age, presence of cough and its duration, immuno compromising illnesses like measles/
diarrhea/ inability to walk, drink eat. convulsions, irregular breathing, apnea, cyanosis and
treatment taken.
Observe for fast breathing, rate >60/min for age less than 2 months
rate >50/min for age 2 – 12 months
rate >40/min for age 12 months – 5 yrs
look for chest in drawing,
look for signs of serious illness = refusal to feed, drowsiness, grunting, wheeze, stridor etc
CLINICAL CLASSIFICATION AND TREATMENT STRATEGIES IN PNEUMONIA:
AGE 0-2 MONTHS
SIGNS CLASSIFICATION TREATMENT PLAN
Normal respiratory rate No pneumonia Home remedies, continue
feeding, watch for signs of
severity
Increased respiratory rate Severe pneumonia Parenteral antibiotics
supportive
Increased respiratory rate and
chest indrawing
Very severe illness Start parenteral antibiotics /
refer to higher center
AGE 2 months -5 years
SIGNS CLASSIFICATION TREATMENT PLAN
Normal respiratory rate No pneumonia Home remedies, continue
feeding, watch for signs of
severity
Increased respiratory rate pneumonia Cotrimoxazole at home or
Center
Increased respiratory rate and
chest indrawing
Severe pneumonia Start parenteral antibiotics
Other signs/ symptoms of
severity
Very severe disease Start parenteral antibiotics /
refer to higher center

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
13
MANAGEMENT:
A. TREATMENT OF PNEUMONIA
Cotrimoxazole is the drug of choice, the dosages as below:
Age/ weight Pediatric tablet 100S+20T Pediatric syp 100S+20T per 5 ml
2-12 mo or 6-9 kg 2 tablets twice a day 5ml twice a day
1-5 yr or 10-19 kg 3 tab twice a day 7.5 ml twice a day
Daily for 5 days
Reassess after 48 hrs, if no improvement or worsening continue 2 more days, sos hospitalize
if worsening.
B. TREATMENT OF SEVERE PNEUMONIA
ANTIBIOTIC DOSE INTERVAL ROUTE
First 48 hrs
Benzyl penicillin or 50000U/kg /dose 6 hrly IM
Ampicillin 50mg/kg/dose 6 hrly IM
Chloramphenicol 25mg/kg/dose 6 hrly IM
If improved give next 3 days the following
Procain penicillin 50000U/kg/dose Once IM
Ampicillin 50mg/kg/dose 6 hrly IM
Chloramphenicol 25/mg/kg/dose 6 hrly IM
If no improvement after total 5 days, change the antibiotic
Ampicillin to be changed to chloramphenicol
Chloramphenicol to be changed to cloxacillin 25/mg/kg/dose 6 hourly with gentamicin
2.5mg/kg/dose 8 hrly, if imnproved - orally
C. symptomatic treatment for fever and wheezing
D. monitor fluids and intake
E. advise mother on home management
Treat with antibiotics for 5 days, and then continue for 3 days after recovery, if cloxacillin or
gentamicin is used, give for 3 weeks.
F. Treatment of very severe pneumonia
Treat in FRU or district hospital. Chloramphenicol IM is the drug of choice.Treat 48 hours, if
improved switch to oral chloramphenicol. If worsens, IM clox and gentamicin.
PNEUMONIA in LESS THAN 2 MONTH AGE :Treat as severe pneumonia, hospitalize.
Antibiotic (injections) Dose Age < 7 days 7 days to 2 months
Benzyl penicillin or 50000U/kg /dose 12 hrly 6 hrly
Ampicillin 50mg/kg/dose 12 hrly 6 hrly
Gentamicin 2.5 mg/kg/dose 12 hrly 6 hrly

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
14
MANAGEMENT OF NO PNEUMONIA
No antibiotics
Home care, continue feeding, nasal saline drops, home made remedies,
No cough syrups
Watch for signs of pneumonia.
References:
1. National Child survival and safe motherhood program. Program interventions guidelines,
MCH Division, Ministry of Health, Govt of India, New Delhi, 1994.
2. IAP textbook of Pediatrics,Ist ed,5-6
FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
15
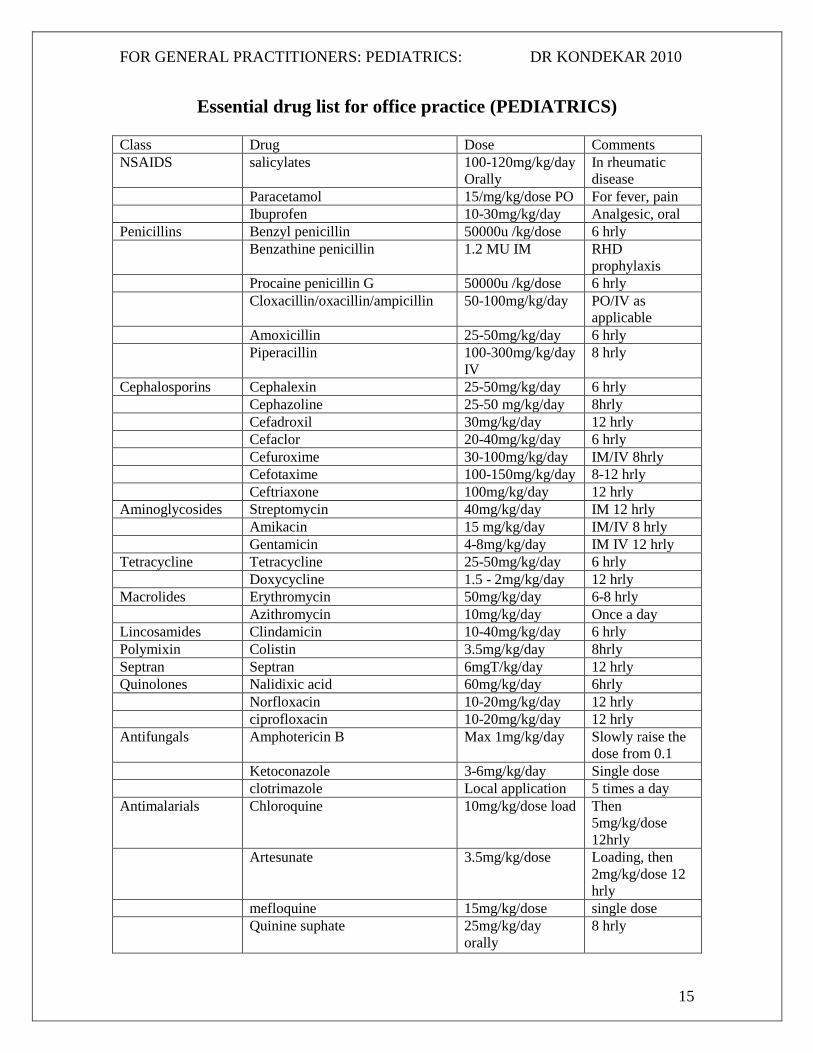
Essential drug list for office practice (PEDIATRICS)
Class Drug Dose Comments
NSAIDS salicylates 100-120mg/kg/day
Orally
In rheumatic
disease
Paracetamol 15/mg/kg/dose PO For fever, pain
Ibuprofen 10-30mg/kg/day Analgesic, oral
Penicillins Benzyl penicillin 50000u /kg/dose 6 hrly
Benzathine penicillin 1.2 MU IM RHD
prophylaxis
Procaine penicillin G 50000u /kg/dose 6 hrly
Cloxacillin/oxacillin/ampicillin 50-100mg/kg/day PO/IV as
applicable
Amoxicillin 25-50mg/kg/day 6 hrly
Piperacillin 100-300mg/kg/day
IV
8 hrly
Cephalosporins Cephalexin 25-50mg/kg/day 6 hrly
Cephazoline 25-50 mg/kg/day 8hrly
Cefadroxil 30mg/kg/day 12 hrly
Cefaclor 20-40mg/kg/day 6 hrly
Cefuroxime 30-100mg/kg/day IM/IV 8hrly
Cefotaxime 100-150mg/kg/day 8-12 hrly
Ceftriaxone 100mg/kg/day 12 hrly
Aminoglycosides Streptomycin 40mg/kg/day IM 12 hrly
Amikacin 15 mg/kg/day IM/IV 8 hrly
Gentamicin 4-8mg/kg/day IM IV 12 hrly
Tetracycline Tetracycline 25-50mg/kg/day 6 hrly
Doxycycline 1.5 - 2mg/kg/day 12 hrly
Macrolides Erythromycin 50mg/kg/day 6-8 hrly
Azithromycin 10mg/kg/day Once a day
Lincosamides Clindamicin 10-40mg/kg/day 6 hrly
Polymixin Colistin 3.5mg/kg/day 8hrly
Septran Septran 6mgT/kg/day 12 hrly
Quinolones Nalidixic acid 60mg/kg/day 6hrly
Norfloxacin 10-20mg/kg/day 12 hrly
ciprofloxacin 10-20mg/kg/day 12 hrly
Antifungals Amphotericin B Max 1mg/kg/day Slowly raise the
dose from 0.1
Ketoconazole 3-6mg/kg/day Single dose
clotrimazole Local application 5 times a day
Antimalarials Chloroquine 10mg/kg/dose load Then
5mg/kg/dose
12hrly
Artesunate 3.5mg/kg/dose Loading, then
2mg/kg/dose 12
hrly
mefloquine 15mg/kg/dose single dose
Quinine suphate 25mg/kg/day
orally
8 hrly

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
16
Sulfadoxine pyrimethamine 20mg/kg of
sulfadoxine
Single dose
orally
Antiprotozoal Chloroquine 10mg/kg/day 8 hrly 10-21 days
Furazolidone 5-8mg/kg/day 8hrly
Metronidazole 10-50mg/kg/day 8 hrly
Antivirals Acyclovir 5ml/kg/dose 8 hrly for 10
days
Antiemetics Domperidone 0.3 mg/kg/dose 8 hrly
Antihistaminics Astemizole 2mg/10kg BW OD
Chlorpheniramine 0.5mg/kg/day 8 hrly
Cyproheptadine 0.25mg/kg/day 8 hrly
Antituberculous Isoniazid 5mg/kg/dose Daily morning,
single dose
Rifampicin 10mg/kg Daily morning,
single dose
Ethambutol 20mg/kg/day
Pyrazinamide 25mg/kg/day
Antiasthmatics Salbutamol 0.15mg/kg/dose Oral or
nebulisation
Terbutalin 0.005 to
0.01mg/kg/dose
Subcutaneus
injection
Aminophylline 2-5 mg/kg bolus
Cardiac Digoxin 0.01mg/kg/dose Maintenance
dose
Reference:
1. Rational drug therapy in children, Essential Pediatrics, Ghai O. P., 3rd edition, 420-428

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
17
CALCIUM PREPARATIONS
Calcium is one of the most important elements in the diet because it is a structural component of
bones, teeth, and soft tissues and is essential in many of the body's metabolic processes
Recommended daily intake (of elemental calcium)
Infants 0–6 months 400 mg
6–12 month 600 mg
children 1–10 years 800 mg
11–24 years 1,200 mg
Over 24 years 800 mg
Pregnant women 1,200 mg
Prophylactic dose/ maintenance 60-100 mg/kg/day
Sources = Dairy products, meats, and some seafood (sardines, oysters) are excellent sources of
calcium. Spinach, beet greens, beans, and peanuts are among the best plant-derived sources.
THERAPEUTIC DOSE=100-200 mg/kg/day, of elemental calcium.
CALCIUM COMPOUNDS:
Calcium carbonate and phosphate preparations have the highest concentration of elemental
calcium - about 40%. Calcium carbonate is found in preparations such as Tums, Os-Cal, and
Citrate. The elemental calcium content of calcium citrate is 21%, of calcium lactate 13%, and of
calcium gluconate, 9%.
VIT-D Vitamin D is required for calcium absorption. (RDA= 200-400 IU/day)
VIT-D supplements in Rickets-
Stoss’s regime= inj vitamin D, 6 lac IU given PO, on Day-1 and Day 14
THERAPEUTIC DOSE=100-200 mg/kg/day, of elemental calcium
What increases calcium absorption?
Acidic conditions in the intestine- Calcium carbonate needs to be taken with meals, as the acidity
of the stomach is greater when food is being digested. This acidic environment allows for its
absorption. Calcium citrate, however, is absorbed more efficiently than calcium carbonate on an
empty stomach, so it needs to be taken between meals.
VIT-D Vitamin D is required for calcium absorption.

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
18
What decreases calcium absorption?
Oxalic acid, phytates, dietary fibers, laxatives, Great excesses of the minerals phosphorous and
magnesium in proportion to calcium Tannins in tea – decreases calcium absorption.
Avoid taking calcium at the same time as Tetracycline , iron supplements, thyroid hormones, or
corticosteroids, because calcium binds to these substances, interfering with their effectiveness and
also its own absorption.
References:
1. Nelson textbook of Pediatrics
2. Drug Index
3. http://dietary-supplements.info.nih.gov/factsheets/calcium.asp
FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
19
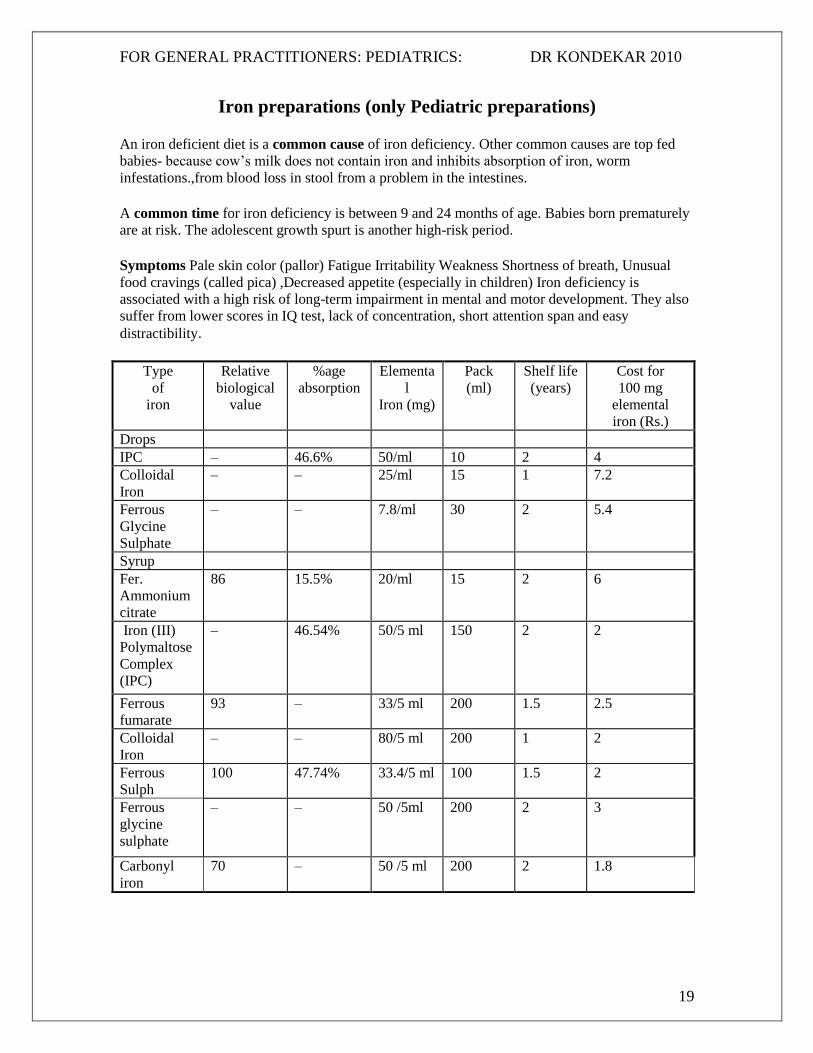
Iron preparations (only Pediatric preparations)
An iron deficient diet is a common cause of iron deficiency. Other common causes are top fed
babies- because cow’s milk does not contain iron and inhibits absorption of iron, worm
infestations.,from blood loss in stool from a problem in the intestines.
A common time for iron deficiency is between 9 and 24 months of age. Babies born prematurely
are at risk. The adolescent growth spurt is another high-risk period.
Symptoms Pale skin color (pallor) Fatigue Irritability Weakness Shortness of breath, Unusual
food cravings (called pica) ,Decreased appetite (especially in children) Iron deficiency is
associated with a high risk of long-term impairment in mental and motor development. They also
suffer from lower scores in IQ test, lack of concentration, short attention span and easy
distractibility.
Type
of
iron
Relative
biological
value
%age
absorption
Elementa
l
Iron (mg)
Pack
(ml)
Shelf life
(years)
Cost for
100 mg
elemental
iron (Rs.)
Drops
IPC – 46.6% 50/ml 10 2 4
Colloidal
Iron
– – 25/ml 15 1 7.2
Ferrous
Glycine
Sulphate
– – 7.8/ml 30 2 5.4
Syrup
Fer.
Ammonium
citrate
86 15.5% 20/ml 15 2 6
Iron (III)
Polymaltose
Complex
(IPC)
–
46.54%
50/5 ml
150
2
2
Ferrous
fumarate
93 – 33/5 ml 200 1.5 2.5
Colloidal
Iron
– – 80/5 ml 200 1 2
Ferrous
Sulph
100 47.74% 33.4/5 ml 100 1.5 2
Ferrous
glycine
sulphate
– – 50 /5ml 200 2 3
Carbonyl
iron
70 – 50 /5 ml 200 2 1.8

FOR GENERAL PRACTITIONERS: PEDIATRICS: DR KONDEKAR 2010
20
Instructions :
Maintenance dose of iron supplements: 2mg/kg/day of elemental iron for 2 months.
Therapeutic dose of iron supplements: 6 mg/kg/day of elemental iron for 2 months.
Best absorbed on empty stomach and with vitamin –C,
Dietary fibers, cheese, yoghurt, coffee,tea, calcium salts decreases absorption.
Gastritis ,constipation, vomiting are common side effects.
Ref : “Iron Formulations in Pediatric Practice”, J. Nagpal, P.Choudhury, Indian
Pediatrics 2004; 41:807-815