
BRCA1 in the family: A case description of the psychological implications
9
BRCA1 in the Family: A Case Description of the Psychological Implications A.C. DudokdeWit, 1 * A. Tibben, 1,2 P.G. Frets, 2 E.J. Meijers-Heijboer, 2 P. Devilee, 4 J.G.M. Klijn, 3 J.C. Oosterwijk, 5 and M.F. Niermeijer 2 1 Department of Medical Psychology and Psychotherapy, Erasmus University Rotterdam, Rotterdam, The Netherlands 2 Department of Clinical Genetics, Erasmus University Rotterdam and University Hospital Dijkzigt, Rotterdam, The Netherlands 3 Dr. Daniel den Hoed Cancer Center Rotterdam, Rotterdam, The Netherlands 4 Department of Pathology and Human Genetic, State University Leiden, Leiden, The Netherlands 5 Department of Clinical Genetics, State University Leiden and University Hospital Leiden, Leiden, The Netherlands Our experience with the first family in the Netherlands for whom predictive DNA- testing for Hereditary Breast and Ovarian Cancer (HBOC) became an option is de- scribed. This serves to illustrate the com- plex emotional impact on a family as a whole, and upon the members separately, of becoming aware that breast and ovarian cancer is hereditary, and the implications of undergoing predictive testing. All family members received genetic counseling and were offered pre- and post-test psychologi- cal follow-up. We observed two important roles within the family. One member became ‘‘the mes- senger of the news’’ informing the relatives of the hereditary character of cancer in the family. Another was ‘‘the first utilizer’’ of the new options; namely, the predictive DNA- test and preventive surgery. This first uti- lizer became the example to the rest of the family. Decisions made about preventive treatment (prophylactic ovariectomy and/or mastectomy) were based on the experiences within the family, whether one identified with an affected family member with breast or with ovarian cancer. The actions and reactions perceived were illustrative of what kind of support provi- sions should be provided in addition to the genetic and oncological counseling for HBOC. Moreover HBOC should be consid- ered both as an individual and a family problem and be treated as such in genetic counseling. Am. J. Med. Genet. 71:63–71, 1997. © 1997 Wiley-Liss, Inc. KEY WORDS: predictive DNA-test; genetic counseling; HBOC; BRCA1; family dynamics; breast can- cer INTRODUCTION In 1993, the International Breast Cancer Linkage Consortium reported that approximately 45% of fami- lies with a high incidence of early onset (age <50 years) breast cancer, and at least 80% of families with in- creased incidence of combined early breast and ovarian cancer, are due to the BRCA1 gene on chromosome 17q [Easton et al., 1993]. This finding made predictive DNA-testing by linkage analysis possible in some fami- lies. In October 1994, the identification of a strong can- didate for BRCA1 allowed direct mutation analysis in individuals at-risk [Miki et al., 1994]. Women carrying the BRCA1 gene have an 85% risk of developing breast cancer and a 63% risk of develop- ing ovarian cancer before the age of 70 years [Easton et al., 1995]. Male gene carriers have an 8% risk of pros- tatic carcinoma before the age of 70 (three-fold the population risk). Male and female gene carriers have a 6% risk of colonic cancer before the age of 70 (four-fold the population risk) [Ford et al., 1994]. The efficacy of chemoprevention or intensive screening (self- examination and/or mammography) in this high risk group, and also prophylactic surgery, are still contro- versial [Eng et al., 1994]. The uptake of the predictive DNA-test among first degree relatives of familial breast cancer patients is expected to be high [Lerman et al., 1994a,b; Chaliki et al., 1995; Lerman et al., 1995a], especially among fe- male relatives who are reported to anticipate a higher negative impact compared to males [Struewing et al., 1995]. However more recent work indicates that only a Contract grant sponsor: NWO; Contract grant number: 960 10 803. *Correspondence to: A.C. DudokdeWit, Department of Medical Psychology and Psychotherapy, Erasmus University Rotterdam, P.O. Box 1738, 3000 DR Rotterdam, The Netherlands. E-mail: [email protected] Received 19 June 1996; Accepted 7 December 1996 American Journal of Medical Genetics 71:63–71 (1997) © 1997 Wiley-Liss, Inc.
Transcript of BRCA1 in the family: A case description of the psychological implications

BRCA1 in the Family: A Case Description of thePsychological Implications
A.C. DudokdeWit,1* A. Tibben,1,2 P.G. Frets,2 E.J. Meijers-Heijboer,2 P. Devilee,4 J.G.M. Klijn,3J.C. Oosterwijk,5 and M.F. Niermeijer2
1Department of Medical Psychology and Psychotherapy, Erasmus University Rotterdam, Rotterdam, The Netherlands2Department of Clinical Genetics, Erasmus University Rotterdam and University Hospital Dijkzigt,Rotterdam, The Netherlands
3Dr. Daniel den Hoed Cancer Center Rotterdam, Rotterdam, The Netherlands4Department of Pathology and Human Genetic, State University Leiden, Leiden, The Netherlands5Department of Clinical Genetics, State University Leiden and University Hospital Leiden, Leiden, The Netherlands
Our experience with the first family in theNetherlands for whom predictive DNA-testing for Hereditary Breast and OvarianCancer (HBOC) became an option is de-scribed. This serves to illustrate the com-plex emotional impact on a family as awhole, and upon the members separately, ofbecoming aware that breast and ovariancancer is hereditary, and the implications ofundergoing predictive testing. All familymembers received genetic counseling andwere offered pre- and post-test psychologi-cal follow-up.
We observed two important roles withinthe family. One member became ‘‘the mes-senger of the news’’ informing the relativesof the hereditary character of cancer in thefamily. Another was ‘‘the first utilizer’’ of thenew options; namely, the predictive DNA-test and preventive surgery. This first uti-lizer became the example to the rest of thefamily. Decisions made about preventivetreatment (prophylactic ovariectomy and/ormastectomy) were based on the experienceswithin the family, whether one identifiedwith an affected family member with breastor with ovarian cancer.
The actions and reactions perceived wereillustrative of what kind of support provi-sions should be provided in addition to thegenetic and oncological counseling forHBOC. Moreover HBOC should be consid-ered both as an individual and a family
problem and be treated as such in geneticcounseling. Am. J. Med. Genet. 71:63–71,1997. © 1997 Wiley-Liss, Inc.
KEY WORDS: predictive DNA-test; geneticcounseling; HBOC; BRCA1;family dynamics; breast can-cer
INTRODUCTION
In 1993, the International Breast Cancer LinkageConsortium reported that approximately 45% of fami-lies with a high incidence of early onset (age <50 years)breast cancer, and at least 80% of families with in-creased incidence of combined early breast and ovariancancer, are due to the BRCA1 gene on chromosome 17q[Easton et al., 1993]. This finding made predictiveDNA-testing by linkage analysis possible in some fami-lies. In October 1994, the identification of a strong can-didate for BRCA1 allowed direct mutation analysis inindividuals at-risk [Miki et al., 1994].
Women carrying the BRCA1 gene have an 85% riskof developing breast cancer and a 63% risk of develop-ing ovarian cancer before the age of 70 years [Easton etal., 1995]. Male gene carriers have an 8% risk of pros-tatic carcinoma before the age of 70 (three-fold thepopulation risk). Male and female gene carriers have a6% risk of colonic cancer before the age of 70 (four-foldthe population risk) [Ford et al., 1994]. The efficacy ofchemoprevention or intensive screening (self-examination and/or mammography) in this high riskgroup, and also prophylactic surgery, are still contro-versial [Eng et al., 1994].
The uptake of the predictive DNA-test among firstdegree relatives of familial breast cancer patients isexpected to be high [Lerman et al., 1994a,b; Chaliki etal., 1995; Lerman et al., 1995a], especially among fe-male relatives who are reported to anticipate a highernegative impact compared to males [Struewing et al.,1995]. However more recent work indicates that only a
Contract grant sponsor: NWO; Contract grant number: 960 10803.
*Correspondence to: A.C. DudokdeWit, Department of MedicalPsychology and Psychotherapy, Erasmus University Rotterdam,P.O. Box 1738, 3000 DR Rotterdam, The Netherlands. E-mail:[email protected]
Received 19 June 1996; Accepted 7 December 1996
American Journal of Medical Genetics 71:63–71 (1997)
© 1997 Wiley-Liss, Inc.
subset of Hereditary Breast and Ovarian Cancer(HBOC) family members are likely to request predic-tive testing when available [Lerman et al., 1996]. Untilrecently the psychological aspects of being at-risk, andactually undergoing predictive DNA-testing for HBOC,were rarely studied. Studies so far report that the mainreasons for wanting the test are to help research and toclarify the situation for their offspring [Watson et al.,1995]. Women at-risk were found to have high levels ofpsychological distress, as well as persistent and intru-sive worries about developing breast cancer [Kash etal., 1992; Lerman and Schwartz 1993; Lerman et al.,1995b]; however, a substantial proportion does not fol-low recommended breast cancer screening guidelines.It has also been observed that young women at highrisk expressed resentment about their family historyand even of their own breasts [Biesecker et al., 1993].Identified female gene carriers suffered from depres-sion, confusion, persistent worries, and sleep distur-bances shortly after disclosure of the test results[Lynch et al., 1993]. The relief felt by non-carriers wasshort lived and soon replaced by worries about possibleerroneous results of the test and concerns about rela-tives who were identified as carriers. More recently itwas reported that, 1 month after testing, non-carriersshowed reduction in depression, role, and sexual im-pairment, while for proven gene carriers depressionand role impairment stayed the same [Lerman et al.,1996]. It was also reported that individuals at-risk forHBOC have indicated that there is a need for consis-tent information from all of those professionals (e.g.,oncologist, clinical geneticist, gynecologist, etc.) theyare consulting [DudokdeWit et al., 1994].
So far, individuals at-risk and the implications of thetest for them have been described. However, little to noattention has been paid to the implications of the teston the whole family. The one aspect, i.e., the individualand her/his reasons for testing, cannot be understoodwithout knowledge on the other, i.e., the family and anunderstanding of what testing for HBOC means for
them. Family dynamics play a major role in how indi-viduals at-risk cope with the threat of an autosomaldominant late-onset disease [Kessler and Bloch, 1989],and in the motivation for taking the test and theireventual adaptation to the test result [Tibben et al.,1990]. Case descriptions are rare in the genetic field.The advantage of a case description is that the topic,i.e., the psychological implications of predictive DNA-testing for the BRCA1 gene, is also made accessible tothose with different theoretical orientation. A detaileddescription can guide the reader to a better under-standing [Kessler, 1994].
Empirical observations of families coming for thetest demonstrated the crucial roles of either being ‘‘themessenger of the news’’: the relative who starts thestudy investigating the genetic nature of HBOC in afamily, or being ‘‘the first utilizer’’: the first at-risk per-son in such a family who decides to take the predictivetest, or to undergo preventive surgery. Noticing thesehighly vulnerable roles, we decided to describe thisfamily from their perspective. The intense contrastingflows of emotions, tensions, and anxieties are exempli-fied in the case history presented, and may help otherprofessionals to identify and support relatives in fami-lies with hereditary late-onset disorders in similar situ-ations.
MATERIALS AND METHODS
Linkage and Mutation Analysis
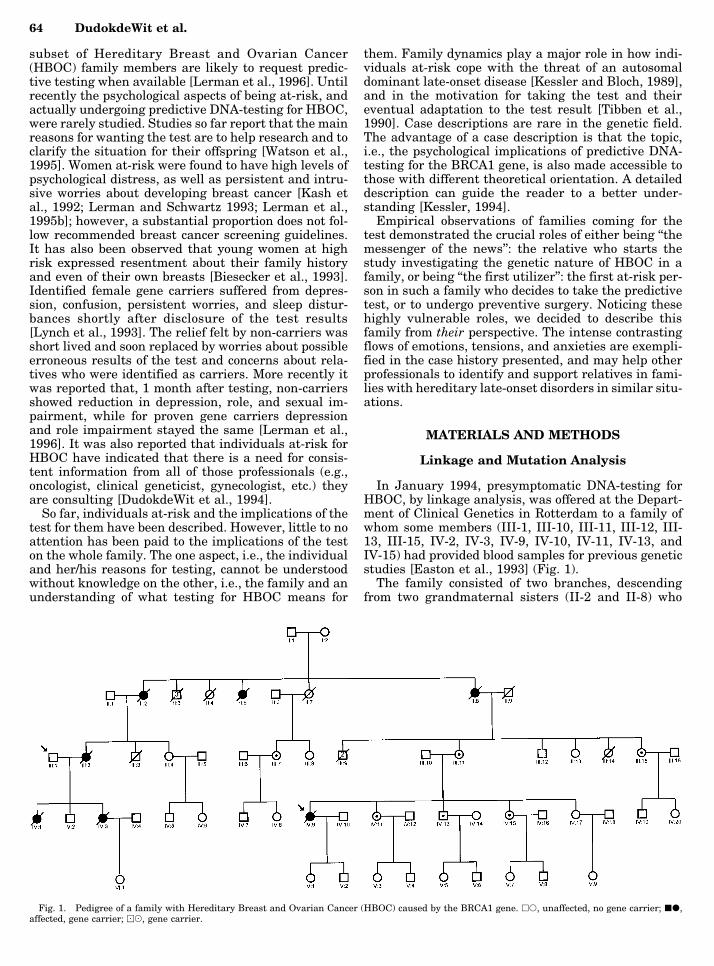
In January 1994, presymptomatic DNA-testing forHBOC, by linkage analysis, was offered at the Depart-ment of Clinical Genetics in Rotterdam to a family ofwhom some members (III-1, III-10, III-11, III-12, III-13, III-15, IV-2, IV-3, IV-9, IV-10, IV-11, IV-13, andIV-15) had provided blood samples for previous geneticstudies [Easton et al., 1993] (Fig. 1).
The family consisted of two branches, descendingfrom two grandmaternal sisters (II-2 and II-8) who
Fig. 1. Pedigree of a family with Hereditary Breast and Ovarian Cancer (HBOC) caused by the BRCA1 gene. hs, unaffected, no gene carrier; jd,affected, gene carrier; )(, gene carrier.
64 DudokdeWit et al.

were both diagnosed with ovarian cancer. Breast can-cer was diagnosed at the ages of 43, 35, 29, and 34 inone daughter (III-2) and three granddaughters (IV-1,IV-3, and IV-9), respectively, of these two women.
The likelihood ratio for linkage, expressed as the lodscore, was calculated using the LINKAGE algorithm,under assumption of incomplete age dependent pen-etrance as described by Easton et al. [1993]. A lod scoreof 1.31 was obtained using D17S250 and D17S479 in athree-point analysis [Cornelis et al., 1995]. Becausethis family by definition has hereditary breast-ovariancancer (e.g., multiple breast and ovarian cancer casesamong first degree relatives at a young age), the pos-terior probability that it is due to BRCA1, on the basisof this lod score and observed heterogeneity [Easton etal., 1993], was > 98%. As this was considered suffi-ciently reliable, the family was offered the individualpredictive DNA-test, by linkage analysis. Those whoresponded (III-7, III-8, III-13, III-15, IV-8, IV-11, IV-13,IV, 15, and IV-17) were re-sampled for diagnostic test-ing in order to confirm the research data, when havingparticipated in the research phase.
When it became possible, the linkage results wereconfirmed by direct mutation analysis of BRCA1. A 1bp insertion in codon 431 (exon 11), leading to a frame-shift and premature chain-termination during proteintranslation, was identified in all those individuals (II-2,II-5, II-8, III-2, III-7, III-11, III-15, IV-1, IV-3, IV-9,IV-11, IV-13, and IV-15) previously shown to carry theat-risk haplotype [Hogervorst et al., 1995].
Participants
The family members who participated in the re-search phase of the linkage study were informed byletter that predictive DNA-testing was possible. Theywere invited to the Department of Clinical Genetics, tofurther discuss the implications of this test. All wereoffered psychological follow-up during this first ses-sion. To date, all family members with whom a contactwas established (the entire third and fourth generationwith exception of Mrs. III-4 and her children, see Fig.1), accepted the invitation, but not all took the predic-tive test or wanted psychological follow-up. Eight fe-males at 50% risk wanted to be tested (III-7, III-8, III-13, III-15, IV-8, IV-11, IV-15, and IV-17). One woman(IV-9), at that moment without symptoms, had beentreated for breast cancer and wanted to know her ownrisk of ovarian cancer and the chances of passing thegene on to her children. Another woman (III-11) wasexpected to be an obligate gene carrier; both hermother (II-8) and daughter (IV-9) were affected.
One married-in spouse (III-1) whose wife and daugh-ter died and whose other daughter was in the terminalphase of breast cancer, requested additional counsel-ing. One male at 50% risk (IV-13) did take the predic-tive DNA-test. Three others (III-12, IV-2, and IV-7)came for information but did not opt for the test (yet)[DudokdeWit et al., 1996].
Methods
Testing was offered to individuals at 50% risk whowere over 18 years of age. The inclusion criteria were
absence of major mental illness and an ability to giveinformed consent. The protocols for both the predictiveDNA-test and the psychological follow-up study wereadapted from the Dutch Huntington’s disease testingprogram [Tibben et al., 1993] (Table I).
Individuals at-risk and their partners were seenthree times by the clinical geneticist: first to be in-formed (session 1); after 1 month for blood sampling(session 2); and approximately 6 weeks later for thetest result (session 3). All appointments were followedby contact with the psychologist (A.C.D.d.W.) at whicha semi-structured interview took place and question-naires were handed out. The first session with the psy-chologist was primarily to introduce the study and tobecome acquainted; the couple were interviewed to-gether. They were both asked about their family his-tory and their experiences with disease and death; an-other subject during this first session was the motiva-tion to be tested. During the second session with thepsychologist, the individual at-risk and the respectivepartner were interviewed separately. During this con-tact the pros and cons of testing were discussed; atten-tion was paid to the decision-making process abouttreatment options; the dissimilar impact of inheritingthe BRCA1 gene for males and females was discussed;and the way in which the predictive DNA-test could bediscussed with the parents, siblings, friends, and part-ner was evaluated. Attention was also paid to the in-
TABLE I. Predictive DNA-Testing for HBOC Department ofClinical Genetics, Rotterdam
Sessiona
Preparation for test1 Exploration test demand and motiviation
–information about HBOC, inheritance, DNA-test–introduction to the psychological follow-up study–exploration of the family history, experiences with
death and disease and the motivation to be tested–completion of questionnaires
2 Additional information about DNA-testing and bloodsampling
–exploration of consequences of disclosurealternatives, discussion of possible treatment
–blood sampling–in-depth interview separately with the individual
at-risk and the partner, discussing among otherspros and cons of testing
–completion of questionnaires
3 Disclosure of test result–handing out the test result, asking for consent to
contact GP and oncologist–contact with psychologist
Follow-up after disclosure4 Within 24 hours telephone contact to discuss intial
response to the test result5 After 1 week
–in-depth interview with the tested individual andthe partner separately
–completion of questionnaires6 After 6 months
–in-depth interview with the tested individual andthe partner separately
–completion of questionnaires
aThe sessions are held with the individual at-risk and the respective part-ner by a clinical geneticist, followed by the appointment with the psycholo-gist (in italics).
BRCA1 in the Family 65

fluence of HBOC on the sexual relationship of thecouple.
After the test result had been handed out by theclinical geneticist, the couple was seen by the psycholo-gist; at that moment no interview was conducted.Within 24 hours, telephone contact with both gene- andnon-carriers took place to discuss the initial reactionsto the test result. Two more appointments were madewith the psychologist (i.e., sessions 5 and 6), 1 weekand 6 months after the test result. During these ses-sions the impact of HBOC, the impact of their own testresult, and the impact of the test results of relativeswas discussed. Subsequently, the impact of all this ontheir daily life and upon the relationship of the partici-pants with their parents, siblings, friends, and partnerwas explored. Additional attention was paid to the de-cision-making process about treatment options, to theinfluence of HBOC on the sexual relationship of thecouple, and to the dissimilar impact of inheriting theBRCA1 gene for males and females. The question-naires covered the attitude towards the test, expecta-tions about the test result and its impact on variableareas of life, general psychological functioning includ-ing experienced depressive feelings, anxiety, intrusivefeelings, and avoidance behavior (which is discussedelsewhere). All participants were free to stop the pro-cedure whenever they wanted, or to have additionalappointments with the clinical geneticist or the psy-chologist. If a need for additional psychological supportwas expressed, the individual at risk and his/her part-ner were referred to another psychologist of the team(A.T., P.G.F.).
RESULTS
The Messenger of the News: Mr. A (III-1)
Mr. A, in his late forties, was the first ‘‘messenger ofthe news.’’ He lost his wife to ovarian cancer and adaughter, mother of a young girl, to breast cancer. An-other daughter developed breast cancer with metasta-ses, in spite of regular screening, and was in the ter-minal phase of the disease. When Mr. A suspected thehereditary nature of breast cancer in his wife’s family,he wanted it studied particularly in view of the futureof his 3-year-old granddaughter. His attempts to con-tact his wife’s relatives to tell them about the geneticnature of breast and ovarian cancer were not appreci-ated by most of them. It seemed to induce reactivationof the grief felt by the children (III-11, III-12, III-13,and III-15) at the early loss of their mother (II-8). Asone of them, Mrs. (III-11), stated ‘‘it was in the past andit will stay in the past’’; she refused any further contactwith him. Mr. A was resented for having started thismyriad of information. However, partly due to Mrs.(IV-9)’s efforts to mobilize her branch of the family forthe linkage study, Mr. A eventually succeeded in ob-taining pedigree information on breast and ovariancases in his wife’s family resulting in the realization ofthe predictive DNA-test, first by linkage, later by mu-tation analysis.
The Other ‘‘Messenger of the News’’ in ThisFamily and the ‘‘First Utilizer’’ of the Predictive
DNA-Test: Mrs. B (IV-9)
Mrs. B was both a ‘‘messenger of the news’’ and the‘‘first utilizer’’ of the predictive DNA-test. Mrs. B hadhad bilateral breast conserving surgery because ofbreast cancer in her early thirties and feared metasta-ses. Now, in her mid-thirties, she wanted to know moreabout her risk of ovarian cancer and the risk for herchildren. She identified herself with her terminally illcousin and was afraid to die. Although she resentedMr. A (III-1) for causing emotional upheaval, she tookup the information because of her own fear of death.Within her own branch of the family, she tried to per-suade her relatives to join the study on linkage analy-ses. She felt rather isolated during this period becauseher symptom-free mother (III-11) and two of her threesisters (IV-15 and IV-17) neither understood nor appre-ciated her actions to obtain all the information in orderto realize the predictive DNA-test for herself and herrelatives.
When the family study turned out to be informativefor predictive testing by linkage analysis, she took thetest, thus becoming the ‘‘first utilizer.’’ She wasstrongly motivated to establish her risk for ovariancancer as soon as possible. She considered prophylacticovariectomy if found to be a gene carrier. Not unexpect-edly, she was identified as a gene carrier; nevertheless,the confirmation of her fears still came as a shock. Fol-lowing this result, she and her husband requested ad-ditional psychological counseling on the timing andcarrying out of ovariectomy. Being well informed, shefeared premature menopausal symptoms, which in hercase could not be prevented by hormonal substitutionbecause that would bring an additional cancer risk forher remaining breast tissue. Eventually, when she un-derwent an ovariectomy in the Rotterdam cancer cen-ter, by chance microscopic metastases of her breastcancer were found. Distant metastases manifested af-terwards, without clear objective response to differentsystematic treatment modalities. She deeply regrettedthat bilateral total mastectomy had not been carriedout instead of the breast conserving surgery and radio-therapy that she had received in the general hospitalshe visited in the past. She urged her family to takeappropriate notice of what had happened to her.
The family reacted very strongly to the news of herrecurrent metastases and progressively declininghealth; they paid less attention to the hereditary back-ground of HBOC in the family and their own personalrisks. For long, the family was focused on Mrs. B andcould hardly believe that she could not be cured.Within the year she died.
Her sisters (IV-11 and IV-15), brother (IV-13), andlater also her youngest sister (IV-17) took the predic-tive DNA-test. Her youngest sister, who became preg-nant after a good result, told that she felt guilty to-wards Mrs. B and was afraid that her pregnancy wouldbe held against her. She did not dare discuss her feel-ings about her pregnancy with Mrs. B.
66 DudokdeWit et al.

‘‘The First Utilizer’’ of Preventive Surgery:Mrs. C (IV-11)
Mrs. C was the second family member, but the firstsymptom-free risk carrier (50% genetic risk) to take thepredictive DNA-test, and was also the ‘‘first utilizer’’ ofpreventive surgery. She wished to know her risk andthe options for preventive measures if necessary. Sheproved, like her sister, to be a gene carrier. The wors-ened physical condition of her sister Mrs. B (IV-9)strengthened her pretest opinion in favor of preventivesurgery. After oncological counseling, she opted for pro-phylactic mastectomy first, and a prophylactic ovariec-tomy in a later stage, so hormone substitution to pre-vent premature menopausal symptoms would becomean option.
Mrs. C did not want to share her worries and fearsabout the preventive surgery with her relatives, wish-ing to be a good and strong example for her own daugh-ter (not yet a teenager) and the other female relatives.In this way she wished to show her daughter how tocope with the disease and anxieties, and to reassureher should she be found to be a gene carrier as well.
Mrs. C was supported by the positive attitude of hersurgeon who emphasized the importance of personaldecision-making on preventive surgery. He also intro-duced her to a woman who had undergone mastectomywith breast reconstruction with whom Mrs. C couldshare her fears and uncertainties about the impact ofpreventive surgery.
Her husband supported her in the decision for pro-phylactic surgery. The impact of HBOC upon the sex-ual relationship, however, could hardly be discussed.
Other Identified Gene Carriers
Mrs. (IV-15), a sister of Mrs. B (IV-9) and Mrs. C(IV-11), also proved to be a gene carrier. She decidedagainst prophylactic surgery, while benign breast tis-sue abnormalities had already been found shortly afterthe test. She did receive regular screening. During ascreening session, taking place in the week her sisterdied, abnormalities in the ovaries were observed whichappeared to be of a benign and temporary nature. Atthe cremation of her sister Mrs. B (IV-9), Mrs. (IV-15)decided to have a total mastectomy.
Three identified female gene carriers (III-7, III-11,and III-15) from the older generation chose to have aprophylactic ovariectomy, but no mastectomy. Theyviewed ovarian cancer as threatening because in theirprevious generation the women had died of ovariancancer at the same age as they were now. Two of thesewomen found the decision to undergo prophylacticovariectomy somewhat easier since they were alreadypostmenopausal and had completed families. Onewoman had difficulty losing the necessary amount ofweight in order to have a prophylactic ovariectomy. Allthree women regarded preventive breast removal a toointrusive option.
An Obligate Gene Carrier: Mrs. D (III-11)
A symptom free woman/man with an affected motherand a child who develops symptoms can be seen as
‘‘sandwiched’’ between two generations with cancer.The proof by linkage or mutation analysis that breastand ovarian cancer is caused by the BRCA1 gene insuch a family immediately implies that such a person isan obligate gene carrier, leaving the women 85% risk ofdeveloping breast cancer and a 63% risk of developingovarian cancer before the age of 70 years [Easton et al.,1995].
In this family Mrs. D was still free of symptoms,while her mother (II-10) had died of ovarian cancer andher daughter Mrs. B (IV-9) had had bilateral breastcancer. Both of them proved to be gene carriers. Ini-tially, Mrs. D strongly avoided any confrontation withinformation on HBOC. However, she was persuaded byher eldest daughter Mrs. B (IV-9) to have a bloodsample taken in the research phase. When the familystudy turned out to be conclusive for predictive testingby linkage analysis, Mrs. D was informed about theheredity of breast and ovarian cancer in her family andthus her own risk. The diagnosis had been confirmed inthe laboratory, but no additional testing was offered toher. She expressed no intention to pay much attentionto HBOC. Her husband was upset and expressed hisfears concerning his eldest daughter Mrs. B (IV-9),with whom he was particularly close. At a later stage,he sought professional support for his wife, in contra-diction to her own wishes, because he felt she could nothandle the situation. Later he understood that such anincentive should come from his wife herself. No ap-pointment for psychological support was made till now.
Throughout the testing period and after the resultsMrs. D stayed very close to her third daughter Mrs.(IV-15). Mrs. D described herself as being a very goodexample of the fact that being a female gene carrier isnot that devastating, since she is still symptom-free inher mid-fifties. However, Mrs. D eventually decided tohave a prophylactic ovariectomy and follows a breastcontrol program in the Rotterdam cancer center. Shedeveloped peritoneal ovarian cancer at a later stageand subsequently became terminally ill.
The Male Test Candidate: Mr. E (IV-13)
Mr. E’s first cited reason to take the predictive DNA-test was to help research; he later reported that hewanted to know his test result for his daughter. Hefailed to attend the second appointment on two occa-sions. Mr. E was found to be a gene carrier. After thetest result he talked at great length about HBOC andthe impending death of his sister Mrs. B (IV-9). Sixmonths later the impact of his test result was still over-shadowed by his sister’s illness.
DISCUSSION
The Messenger of the News: Mr. A (III-1)
Mr. A was unable to express his grief on the previousand imminent losses. However, he expressed anxietyabout the risk for HBOC in his granddaughter. The
BRCA1 in the Family 67

search for the genetics of HBOC in his family appar-ently served as a containment of the threat, and anattempt to obviate future disaster for his granddaugh-ter. This has been described as ‘‘the crusade of the ul-timate rescuer’’ and might serve as a psychologicaldefense against anxiety and intense grief [Yalom,1980].
In this particular family, Mr. A had a very active roleas ‘‘messenger of the news’’ in motivating his familymembers to participate in a linkage study. Now thattesting is becoming more easily available there will beless necessity for this role. However, even when muta-tion analysis is possible the news still has to spreadthrough the family and there will always be memberswho want to ‘‘rescue’’ their relatives [Yalom, 1980].
The ‘‘messenger of the news’’ is often particularlyvulnerable. He/she sees him/herself confronted by thetask to inform relatives (both healthy and affected) andto ask them to participate in linkage and/or mutationanalysis. This is initially on a research basis, but it willlead to routine family study which enables risk predic-tion for at-risk persons (risk carriers). Guilt feelingsmay be induced in the ‘‘messenger of the news’’ whenseeing what this information has done to his/her fam-ily. Aggression and revulsion could be directed againstthe ‘‘messenger of the news’’ by relatives invited to par-ticipate.
Ego strength and the coping capacities of ‘‘the onewho dares to come for the information’’ are easily over-estimated by the strength of the motivation of the mes-senger. Professionals involved must recognize this dif-ficult role and acknowledge the emotional ramifica-tions. It is important to take the pre-existing familyrelations into account: is there any contact and if sowhat kind of contact? The ‘‘messenger of the news’’may be helped by discussing how to bring the news tothe family, in personal contact, by phone, mail, and tothe whole family together or separately; what kind ofreactions can be expected; what type of informationwill be gained and will be provided by the program; isthere someone in the family to share this role with,etc.? On the other hand the ‘‘messenger of the news’’also might need to be coached, in order to help him/herto understand that there might be relatives who do notwant to be ‘‘saved,’’ or who have a different pace andneed to take things slow. Additional counselingon the experienced emotions certainly needs to be of-fered.
Counselors should be aware that there might besome inherent conflict in their relationship to the ‘‘mes-senger of the news’’: he/she may serve a useful purposein alerting and encouraging participation, but the mes-senger’s role is not a ‘‘sanctioned’’ one. The counselorshould be aware of their own feelings of helplessness[Martindale 1987; Thies et al., 1993; Thomassen et al.,1993] and be careful not to consider the test as the onlyoption. Furthermore, counselors should recognize thatthe messenger’s view of the family is the view of onlyone individual and other avenues and perspectives onthe family should be sought in order to obtain an ‘‘ob-jective’’ view of the family.1
The Other ‘‘Messenger of the News’’ in ThisFamily and the ‘‘First Utilizer’’ of the Predictive
DNA-Test: Mrs. B (IV-9)
It seemed that warding off the death anxiety was thedriving force behind the information seeking behaviorof Mrs. B [Miller et al., 1988]. As ‘‘the first utilizer,’’ shewas the ultimate person who exemplifies the meaningof both the genetic risk (by her illness) and the predic-tive DNA-test to the family. Mrs. B reported that shefelt like a ‘‘guinea pig’’ during the initial phase of thestudy. Professionals involved and laymen did take aninterest in her case, but she felt they were not inter-ested in her as a person. She was tired of being alwaysthe first and strongest, and she longed for someone shecould lean on. This prompted her request for additionalprofessional support for herself and her husband.
The ‘‘First Utilizer’’ of Preventive Surgery:Mrs. C (IV-11)
Mrs. C was the first identified gene carrier in thefamily who chose preventive surgery. She said that shefelt she had no choice after seeing her sister Mrs. B(IV-9) and her cousins (IV-1 and IV-3) die at such ayoung age. She felt very responsible to give a good ex-ample, and to diminish the fear in her relatives to takesimilar decisions. Therefore she did not dare to ask forsupport within the family. The associated responsibil-ity concerning her relatives was a great burden for her.At the same time her family was mainly focused uponMrs. B’s (IV-9) terminal illness.
It is important to discuss in counseling what will begained by prophylactic mastectomy and/or ovariectomyas well as what will be lost for a woman and her hus-band. We did notice, however, that expected changes inthe sexual relation after preventive surgery were noteasily discussed beforehand. After the operation thecouple talked more freely about their sexual relation-ship, but only in positive terms. The adverse effects ofprophylactic ovariectomy and total mastectomy ontheir sexual relationship were not discussed. We foundit an important observation that this couple could notacknowledge the less positive aspects of the operations(e.g., prevention vs. loss). Although this one observa-tion is not enough to draw conclusions, it definitelyindicates that further study is needed.
The ‘‘first utilizer’’ is often under pressure to providebenefits for herself as well as the family. The familyhas no experience with predictive DNA-testing; there-fore the ‘‘first utilizer’’ feels obliged to show how it allworks. In counseling, the individual choice and themeaning of this for the other family members are ofcourse linked, but should not be addressed as one sub-ject; they should be discussed as different topics so as toenable the first utilizer to perceive the unexpected bur-dens resulting from functioning as an ‘‘example’’ intheir family.
The Obligate Gene Carrier: Mrs. D (III-11)
Having knowledge about the dominant inheritancepattern of HBOC might imply that a person ‘‘sand-wiched’’ between an affected mother and child under-stands that she/he has to be a gene carrier. On the1We thank the anonymous reviewers for this suggestion.
68 DudokdeWit et al.

other hand, it is comprehensible that such a personmaintains hope that it is ‘‘just coincidence,’’ so theother children (and in case of a woman, she herself), arenot at an increased risk for breast and ovarian cancer.In counseling an obligate gene carrier it is important totake both options, acknowledgment and denial, into ac-count. This woman, Mrs. D, participated in the re-search phase of the linkage study, when linkage wasfound she was informed about her genetic status. Shewas not offered additional testing as it was assumedthat she already understood that she had to be a genecarrier now that her mother and daughter had provento be gene carriers. She had, however, been denying thepossible consequences of the found linkage to herselfand had been seeing her affected daughter as a spo-radic case of breast cancer. We learned from thiswoman how important it is to start testing the oldestgeneration first (when wanting to be tested), and tooffer all individuals in a HBOC family the same infor-mation and options in a testing protocol; this because itis never certain that even very ‘‘obvious’’ information isunderstood and taken in.
In this family, being without symptoms and never-theless a gene carrier, Mrs. D could deny the impact ofthe test results in her family. She was, at that moment,living proof that one does not have to die young frombreast and ovarian cancer when found to be a genecarrier. This might have enabled her to suppress feel-ings of guilt about passing the gene on to her childrenand their offspring.
The Male Test Candidate: Mr. E
The main focus of attention and concern has been thewomen at-risk, both for most professionals involved[American Society of Human Genetics 1994] and forthe men in the family [DudokdeWit et al., 1996]. Byfocusing on their female relatives and their risks (lifeand death), the impact of testing for the men at-risk isput into a perspective that minimalizes its relevance. Itis important to keep in mind that men are also deeplyaffected when their female relatives (mothers, sistersand daughters) are at-risk, with all the potential con-sequences.
Advantages and Disadvantages of aCase Description
We have described one family as a mere inspirationto all healthcare workers working with families at-riskfor HBOC and other late-onset disorders. Through thiscase description of an HBOC family we aim to enhanceunderstanding of what testing means, not only for theindividual but also for the entire family. One of themain advantages is, as already described in the Intro-duction, that the impact of DNA-testing is made un-derstandable to others with a different theoretical ori-entation [Kessler, 1994]. Besides advantages there arealso disadvantages to a case description. Only one fam-ily has been described which might reduce the gener-alizability of the findings. However, we recognizedsimilar observations in work done with newly diag-nosed families with Huntington’s disease (unpublisheddata) and families at-risk for presenile dementia
[Tibben et al., 1997]. The latter publication reportedthat the ‘‘messenger’’ was often the patient’s spousebecause the hereditary disease was generally first dis-cussed with him/her; their informing the relatives of-ten caused emotional upheaval and they were oftenresented for this. In addition, the family members par-ticipated both in the research phase of linkage analysisand in the actual testing protocol; this might introducesome bias by potential extensive attention from the re-searchers [Wiggins et al., 1992].
The observations described are restricted to the ap-pointments with the psychologist at the department ofclinical genetics, from the first contact until the lastapproximately 9 months later (the time range of thepsychological follow-up study they participated in).Events happening within the family within this periodcould be described. The impact of events taking placeafterwards, such as the illnesses of Mrs. (III-11), couldnot be described as no new contact was established.The author working at the Rotterdam cancer center(J.G.M.K.) added the information.
COUNSELING
In order to maintain confidentiality when counselingfamily members simultaneously, strict organization isnecessary. The counsellors (geneticist, psychologist,oncologist, and administrative staff) involved should dotheir best to respect the privacy of the family members.Thus during the first session the following should beaddressed:
1. The attention is focused upon the needs of theindividual with the appointment. Counselors should beaware not to be seduced into discussing the implica-tions of the genetic status of family members (such aswhether a family member made the right decision,etc.). The impact on the individual in counseling con-cerning what is happening to the rest of the family can,of course, be discussed.
2. Although part of a family, each member is, as faras possible, counseled as an individual case. The indi-vidual at-risk may have heard all kind of informationfrom family members or even no information at all. It isimportant that the knowledge of DNA and predictivetesting is thoroughly checked and completed whenneeded.
3. Taking the test, or not, should be an enterprise ofthe person at-risk and the respective partner and not afamily enterprise; however, the decision will be influ-enced by the events taking place in the family.
4. The individual taking the test is the only one towhom the test result will be disclosed; the test resultcan not be picked up by another relative. [This nottaking in consideration the discussion about those at25% risk (International Huntington Association andthe World Federation of Neurology Research Group onHuntington’s Chorea 1994)]. He or she is free to post-pone the appointment until the last second when nec-essary.
5. Concerning the test result, it is very important todiscuss whether they want to be with relatives at thedepartment of clinical genetics, or not. When relativeswant to receive their test result at the same time, mul-
BRCA1 in the Family 69

tiple rooms ought to be reserved; a separate room foreach of them to receive their own test result. After ev-erybody has received his/her own test result they canmeet together if they so wish. If someone does not wantother family members to know that he or she is takingthe test, an appointment is scheduled distinctly apartfrom that of other family members.
In conclusion practical issues, such as mentionedabove, should be discussed with individuals at-riskplanning to be tested in order to be able to safeguardtheir privacy. Contradictory as it may seem, to be fullyable to treat all family members as individuals, thepsychological impact of predictive testing on both theindividual and family level should be addressed in ge-netic counseling. This in order to differentiate between,and to understand the motivation fed by both indi-vidual and family matters. A multidisciplinary teamincluding a psychologist is needed to offer counselorssupervision concerning the intertwinement of indi-vidual and family motives for predictive testing. If aneed for additional psychological support is expressed,the individual at risk and his/her partner can be re-ferred to the psychologist of the team.
CONCLUDING REMARKS
In genetic counseling for predictive DNA-testing it isvery important to acknowledge that individuals show avariety of mechanisms to cope with threatening infor-mation and treatment options. Caregivers involved inpredictive testing programs should be aware of thesepersonal adaptation mechanisms.
The family unit ought to be preserved and guarded,and certainly not harmed. Participants of predictivetesting need to know what the test can do to the familyunit and existing relationships. It should be ensuredthat predictive testing will provide the most benefitand least harm for all individuals and families in-volved.
There are major challenges in genetic research toobtain consent, protect privacy and confidentiality, andsafeguard divergent and conflicting intrafamilial andintergenerational interests, and all this whilst keepingthe research on track [MacKay 1993]. Our experienceemphasizes that a strong collaboration of all disciplinesinvolved (molecular and clinical geneticist, oncologist,psychologist, medical ethicist, and general practitio-ner) involved is a sine qua non for conducting geneticstudies, in order to meet these challenges.
ACKNOWLEDGMENTS
This research was supported by NWO grant 960 10803 to the first author. The authors are very grateful tothe individuals at-risk and their partners who haveparticipated in this study.
REFERENCES
American Society of Human Genetics (1994): Statement of the AmericanSociety of Human Genetics on genetic testing for breast and ovariancancer predisposition. Am J Hum Genet 55:i–iv.
Biesecker BB, Boehnke M, Calzone K, Markel DS, Garber JE, Collins FS,
Weber BL (1993): Genetic counseling for families with inherited sus-ceptibility to breast and ovarian cancer. JAMA 269:1970–1974.
Chaliki H, Loader S, Levenkron JC, Logan-Young W, Hall WJ, Rowley PT(1995): Women’s receptivity to testing for a genetic susceptibility tobreast cancer. Am J Public Health 85:1133–1135.
Cornelis RS, Vasen HF, Meijers-Heijboer H, Ford D, van Vliet M, vanTilborg AA, Cleton FJ, Klijn JG, Menko FH, Meera Khan P, et al.(1995): Age at diagnosis as an indicator of eligibility for BRCA1 DNAtesting in familial breast cancer. Hum Genet 95:539–544.
DudokdeWit AC, Meijers-Heijboer EJ, Tibben A, Frets PG, Klijn JGM,Devilee P, Niermeijer MF (1994): Effect on a Dutch family of predictiveDNA-testing for hereditary breast and ovarian cancer. Lancet 344:197.
DudokdeWit AC, Tibben A, Frets PG, Meijers-Heijboer EJ, Niermeijer MF(1996): Males at-risk for the BRCA1 gene, the psychological impact.Psycho-Oncol 5:251–257.
Easton DF, Bishop DT, Ford D, Crockford GP (1993): Genetic linkageanalysis in familial breast and ovarian cancer: results from 214 fami-lies. The Breast Cancer Linkage Consortium. Am J Hum Genet 52:678–701.
Easton DF, Ford D, Bishop DT (1995): Breast and ovarian cancer incidencein BRCA1-mutation carriers. Breast Cancer Linkage Consortium. AmJ Hum Genet 56:265–271.
Eng C, Stratton M, Ponder B, Murday V, Easton D, Sacks N, Watson M,Eeles R (1994): Familial cancer syndromes. Lancet 343:709–713.
Ford D, Easton DF, Bishop DT, Narod SA, Goldgar DE (1994): Risks ofcancer in BRCA1-mutation carriers. Breast Cancer Linkage Consor-tium. Lancet 343:692–695.
Hogervorst FB, Cornelis RS, Bout M, van Vliet M, Oosterwijk JC, Olmer R,Bakker B, Klijn JG, Vasen HF, Meijers-Heijboer H, et al. (1995): Rapiddetection of BRCA1 mutations by the protein truncation test. NatGenet 10(2):208–212.
Huggins M, Bloch M, Wiggins S, Adam S, Suchowersky O, Trew M, KlimekM, Greenberg CR, Eleff M, Thompson LP, et al. (1992): Predictive test-ing for Huntington disease in Canada: adverse effects and unexpectedresults in those receiving a decreased risk. Am J Med Genet 42:508–515.
International Huntington Association and the World Federation of Neu-rology Research Group on Huntington’s Chorea (1994): Guidelines forthe molecular genetics predictive test in Huntington’s disease. J MedGenet 31:555–559.
Kash KM, Holland JC, Halper MS, Miller DG (1992): Psychological dis-tress and surveillance behaviors of women with a family history ofbreast cancer. J Natl Cancer Inst 84:24–30.
Kessler S (1994): Predictive testing for Huntington disease: a psycholo-gist’s view. Am J Med Genet 54:161–166.
Kessler S and Bloch M (1989): Social system responses to Huntingtondisease. Fam Process 28:59–68.
Lerman C and Schwartz M (1993): Adherence and psychological adjust-ment among women at high risk for breast cancer. Breast Cancer ResTreat 28:145–155.
Lerman C, Audrain J, Croyle RT (1994a): DNA-testing for heritable breastcancer risks: Lessons from traditional genetic counseling. Mini-Series:Advances in behavioral medicine research on breast cancer. An Behav-ioral Med 16:327–333.
Lerman C, Daly M, Masny A, Balshem A (1994b): Attitudes about genetictesting for breast-ovarian cancer susceptibility. J Clin Oncol 12:843–850.
Lerman C, Seay J, Balshem A, Audrain J (1995a): Interest in genetictesting among first-degree relatives of breast cancer patients. Am JMed Genet 57:385–392.
Lerman C, Lustbader E, Rimer B, Daly M, Miller S, Sands C, Balshem A(1995b): Effects of individualized breast cancer risk counseling: A ran-domized trial. J Natl Cancer Inst 87:286–292.
Lerman C, Narod S, Schulman K, Hughes C, Gomez-Caminero A, BonneyG, Gold K, Trock B, Main D, Lynch J, Fulmore C, Snyder C, Lemon SJ,Conway T, Tonin P, Lenoir G, Lynch H (1996): BRCA1 testing in fami-lies with hereditary breast-ovarian cancer. JAMA 275:1885–1892.
Lynch HT, Watson P, Conway TA, Lynch JF, Slominski-Caster SM, NarodSA, Feunteun J, Lenoir G (1993): DNA screening for breast/ovariancancer susceptibility based on linked markers. A family study. ArchIntern Med 153:1979–1987.
MacKay CR (1993): Discussion points to consider in research related to thehuman genome. Hum Gene Ther 4:477–495.
Martindale B (1987): Huntington’s chorea: Some psychodynamics seen in
70 DudokdeWit et al.

those at risk and in the responses of the helping professions. Br JPsychiatry 150:319–323.
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavti-gian S, Liu Q, Cochran C, Bennett LM, Ding W, et al. (1994): A strongcandidate for the breast and ovarian cancer susceptibility gene BRCA1.Science 266:66–71.
Miller SM, Summerton J, Brody DS (1988): Styles of coping with threat:Implications for health. J Pers Soc Psychol 54:142–148.
Struewing JP, Lerman C, Kase RG, Giambarresi TR, Tucker MA (1995):Anticipated uptake and impact of genetic testing in hereditary breastand ovarian cancer families. Cancer Epidemiol Biomarkers Prevention4:169–173.
Thies U, Bockel B, Bochdalofsky V (1993): Attitudes of neurologists, psy-chiatrists, and psychotherapists towards predictive testing for Hun-tington’s disease in Germany. J Med Genet 30:1023–1027.
Thomassen R, Tibben A, Niermeijer MF, van der Does E, van de Kamp JJ,Verhage F (1993): Attitudes of Dutch general practitioners towardspresymptomatic DNA-testing for Huntington disease. Clin Genet 43:63–68.
Tibben A, Vegter-van der Vlis M, van de Kamp JJ, Roos RA, RooijmansHG, Frets PG, Verhage F (1990): Testing for Huntington’s disease withsupport for all parties. Lancet 335:553.
Tibben A, Frets PG, van de Kamp JJ, Niermeijer MF, Vegter-van der VlisM, Roos RA, van Ommen GJ, Duivenvoorden HJ, Verhage F (1993):Presymptomatic DNA-testing for Huntington disease: pretest attitudesand expectations of applicants and their partners in the Dutch pro-gram. Am J Med Genet 48:10–16.
Tibben A, Stevens M, van der Wert GMWR, Niermeijer MF, van Duijn CM,van Swieten JC (1997): Preparing for Presymptomatic DNA-testing forearly onset Alzheimer Disease/Cerebral Hemorrhage and hereditaryPick Disease. J Med Genet 34:63–72.
Watson M, Murday V, Lloyd S, Ponder B, Averill D, Eeles R (1995): Genetictesting in breast/ovarian cancer (BRCA1) families. Lancet 346:583.
Wiggins S, Whyte P, Huggins M, Adam S, Theilmann J, Bloch M, ShepsSB, Schechter MT, Hayden MR (1992): The psychological consequencesof predictive testing for Huntington’s disease. Canadian CollaborativeStudy of Predictive Testing. N Engl J Med 327:1401–1405.
Yalom ID (1980): ‘‘Existential Psychology’’ New York: Basic Books, Inc.
BRCA1 in the Family 71


















