Brainstem - bowenstaff.bowen.edu.ng
55
Brainstem Overview & Medulla Oblongata ANATOMY PROGRAMME
Transcript of Brainstem - bowenstaff.bowen.edu.ng

BrainstemOverview & Medulla Oblongata ANATOMY PROGRAMME

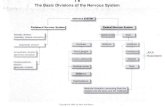
Definition andRelations
2
● The brainstem is the part of the brain that lies
between the cerebrum and the spinal cord.
● It has the following important functions:
○ Regulatory functions (respiratory and
cardiovascular centers along with autonomic
functions)

Definition andRelations
3
○ Cranial nerves nuclei (from III to XII)
○ Regulation of the level of consciousness
○ Serves as a conduit for ascending and
descending tracts
● It lies in the posterior cranial fossa.

Definition andRelations
4
● It’s composed of three parts mainly:
○ Midbrain.
○ Pons.
○ Medulla oblongata.
● The cerebellum is considered a part of the
brainstem in some references.

Eljack’s Lecture Notes in Neuroscience. Fig. 4-1
©2015 all rights reserved9

Siegel, A, Sapru, H.N. Essential Neuroscience.
(3rd ed.). Philadelphia: Lippincott Williams &
Wilkins; 2015. Fig. 9-1 10

External Features of theBrainstem
7
● There are four hillocks in the posterior aspect
of the midbrain: two superior and two inferior
colliculi.
● Pons is the largest part of the brainstem and it
hasparallel horizontal fibers.

● The superior, middle, and inferior cerebellar
peduncles connect the midbrain, pons, and
medulla with the cerebellum, respectively.
● It may be difficult to distinguish the lower part
of the medulla from the spinal cord.
External Features of theBrainstem
8

Eljack’s Lecture Notes in Neuroscience. Fig. 4-1
©2015 all rights reserved13

Siegel, A, Sapru, H.N. Essential Neuroscience.
(3rd ed.). Philadelphia: Lippincott Williams &
Wilkins; 2015. Fig. 9-1 14

Internal Structures of theBrainstem
11
● The brainstem constitute a passage for all
tracts that originate from the brainstem or
terminate in the spinal cord.
● All ascending tracts that reach cerebral cortex
pass through the brainstem.

Internal Components of the Brainstem
● All cranial nerves nuclei are located in the
brainstem except the olfactory and optic
nerves.
● The tectum constitute the roof of the midbrain.
● The tegmentum is a part of the brainstem
resembling the core of the midbrain and pons.
Internal Structures of theBrainstem
12

Internal Components of the Brainstem
● The reticular formation lies in the tegmentum of
the brainstem.
● The basilar areas lie anterior to the tegmentum.
Internal Structures of theBrainstem
13

Haines, Duane. Fundamental
Clinical Applications. 4th
Neuroscience For Basic And
ed.
Philadelphia: Elsevier, 2013. Fig.
10-218

Principles of Cranial NervesNuclei
15

Importance of ThisSection
16
● Understanding these principle enable the
student to understand the complexity of the
cranial nerves development, origin, structure,
and functions.
● This part is poorly understood by medical
students which results in difficulty in learning
about cranial nerves.

Classification of Cranial NervesComponents
17
● There are some overlaps and exceptions!
● According to the direction of the component:
○ Afferent: means going from peripheral
tissues to the brain (inward signal).
○ Efferent: means going from the brain to
peripheral tissues (outward signal). [consider
Efferent=Exit to memorize].

Classification of Cranial NervesComponents
18
● According to the innervated tissue:
○ Somatic: innervates primarily
muscles, joints, tendons, skin,
somatic parts.
○ Visceral: innervates primarily
skeletal
and other
smoothmuscles, viscera, and glands.

Classification of Cranial NervesComponents
19
● According to the receptors and muscle:
○ General: standard afferents and efferents
going to different body parts.
○ Special: to the muscle from mesenchyme of
the branchial arches (muscles of
mastication) and from highly specialized
receptors (e.g.chemoreceptors).

Classification of Cranial NervesComponents
20
● Every component has one classification of the
each category.
● Examples of components:
○ General somaticefferent (GSE).
○ Specialvisceral efferents (SVE).
○ General visceralefferent (GVE).
○ General somaticafferent (GSA).

25Snell, R.S. Clinical Neuroanatomy. (7th ed.). Philadelphia: Lippincott Williams &
Wilkins; 2010. Table 11-1

26
Duane. FundamentalHaines,
Neuroscience For Basic And Clinical
Applications. 4th ed. Philadelphia: Elsevier,
2013. Fig. 10-7

Anatomy of the MedullaOblongata
23

ExternalFeatures
24
● It develops from the myelencephalon (lower
part of thehindbrain.
● Connected to the pons rostrally and to the
spinal cord caudally.
● It has a conical shape (broader superiorly).

● The junction between the spinal cord and the
medulla is at the origin of the first cervical
spinal nerve (level of foramen magnum).
● The central canal of the spinal cord continues
to the lower part of the medulla.
25
ExternalFeatures

ExternalFeatures
26
● The medulla is divided based on the presence
of the fourth ventricle into:
○ Caudal (closed) medulla
○ Rostral (open) medulla

Waxman, S.G. Clinical Neuroanatomy. (27th ed.).:
McGraw-Hill; 2013. Fig. 7-7B
27

32Waxman, S.G. Clinical Neuroanatomy. (27th ed.).:
McGraw-Hill; 2013. Fig. 7-7C

ExternalFeatures
29
● There is the anterior median fissure in the
anterior surface of the medulla.
● Lateral to the anterior median fissure lie the
medullary pyramids (containing the
corticospinal and corticobulbar tracts).

ExternalFeatures
30
● The medullary olives lie posterolaterally to the
pyramids. They are produced by the inferior
olivary nuclei.
● The inferior cerebellar peduncles lie posterior
to the olives.

35Snell, R.S. Clinical Neuroanatomy. (7th ed.). Philadelphia:
Lippincott Williams & Wilkins; 2010. Fig. 5-9A

36
ExternalFeatures
● The posterior median sulcus lies in the posterior
part of the caudal medulla.
● Lateral to the posterior median sulcus in the
caudal medulla there are the gracile and
cuneate tubercles produced by the gracile and
cuneate nuclei, respectively.

37Snell, R.S. Clinical Neuroanatomy. (7th ed.). Philadelphia: Lippincott
Williams & Wilkins; 2010. Fig. 5-9B

Basics on the InternalFeatures
34
● Medulla oblongata contains grey and white
matter.
● Sulcus limitans is important to differentiate
between sensory and motor nuclei.

Basics on the InternalFeatures
35
● We divided the medulla anatomically into four
levels:
○ Level of pyramidal (motor) decussation
○ Level of lemniscus (sensory) decussation
○ Level of the olives (midmedullary level)
○ Level of pontomedullaryjunction

Level of PyramidalDecussation
36
● Around 90% of corticospinal tracts fibers
decussate atthis level.
● The cuneate and gracile nuclei (posterior
column nuclei) appear at this level to their
respective fasciculi.

Level of PyramidalDecussation
37
● The substantia gelatinosa of the spinal cord
becomes continuous with the spinal nucleus of
the trigeminal nerve.
● Fibers of the anterolateral system and fibers of
the spinal trigeminal tract lie adjecent to each
other in the lateral medulla.

Haines, Duane. Fundamental Neuroscience For Basic And Clinical
Applications. 4th ed. Philadelphia: Elsevier, 2013. Fig. 11-6
38

Level of LemniscusDecussation
39
● The internal arcuate fibers (forming the medial
lemniscus) decussate at this level anterior to
central grey and posterior to the pyramids.
● The spinal nucleus of the trigeminal nerve lies
lateral to the internal arcuate fibers.

Level of LemniscusDecussation
40
● The nucleus ambiguus lies medial to the spinal
trigeminal nucleus (SE components to the
glossopharyngeal and vagus nerves).
● The spinothalamic and spinotectal tracts lie
lateral to the lemniscus decussation.

45Haines, Duane. Fundamental Neuroscience For Basic And Clinical
Applications. 4th ed. Philadelphia: Elsevier, 2013. Fig. 11-8
Level of theOlives
42
● Section at this level passes across the inferior
part of the fourth ventricle.
● Many cranial nerve nuclei appear at this level.
● The most prominent nuclei are the olivary
nuclear complex especially the inferior olivary
nucleus.

● The restiform body forms a prominent
elevation on the posterolateral aspect of the
medulla. It contains many cerebellar afferents.
● The spinal trigeminal tract and nucleus are
interior to the restiform body.
Level of theOlives
43

48Haines, Duane. Fundamental Neuroscience For Basic And Clinical
Applications. 4th ed. Philadelphia: Elsevier, 2013. Fig. 11-11

Lesions of the MedullaOblongata
45

Arnold-ChiariSyndrome
46
● Congenital herniation of cerebellar tonsils and
medulla through the foramen magnum.
● Results in hydrocephalus and involvement of
the last four cranial nerves along with
cerebellar signs.
Lateral MedullarySyndrome
47
● Also known as “Wallenberg’s syndrome”.
● Results from a vascular lesion of the vertebral
and posterior inferior cerebellar arteries.
● Signs and symptoms include:
○ Loss of pain and temperature on the
opposite side of the body and the ipsilateral
face

Lateral MedullarySyndrome
48
○ Loss of coordination
○ Vertigo
○ Loss of the gag reflex
○ Difficulty with speech and swallowing
○ Horner’s syndrome

53Snell, R.S. Clinical Neuroanatomy. (7th ed.). Philadelphia:
Lippincott Williams & Wilkins; 2010. Fig. 5-31

Medial MedullarySyndrome
50
● Also known as the “Déjérine’s syndrome”.
● Results from damage to the medial branches of
the vertebral artery or the anterior spinal artery.
● Signs and symptoms include:
○ Contralateral hemiparesis.

Medial MedullarySyndrome
51
○ Contralateral impaired prorioceptionand
tactile sensations
○ Ipsilateral paralysis of the tongue muscles
● In case of anterior spinal artery oclusion, signs
and symptoms may be bilateral
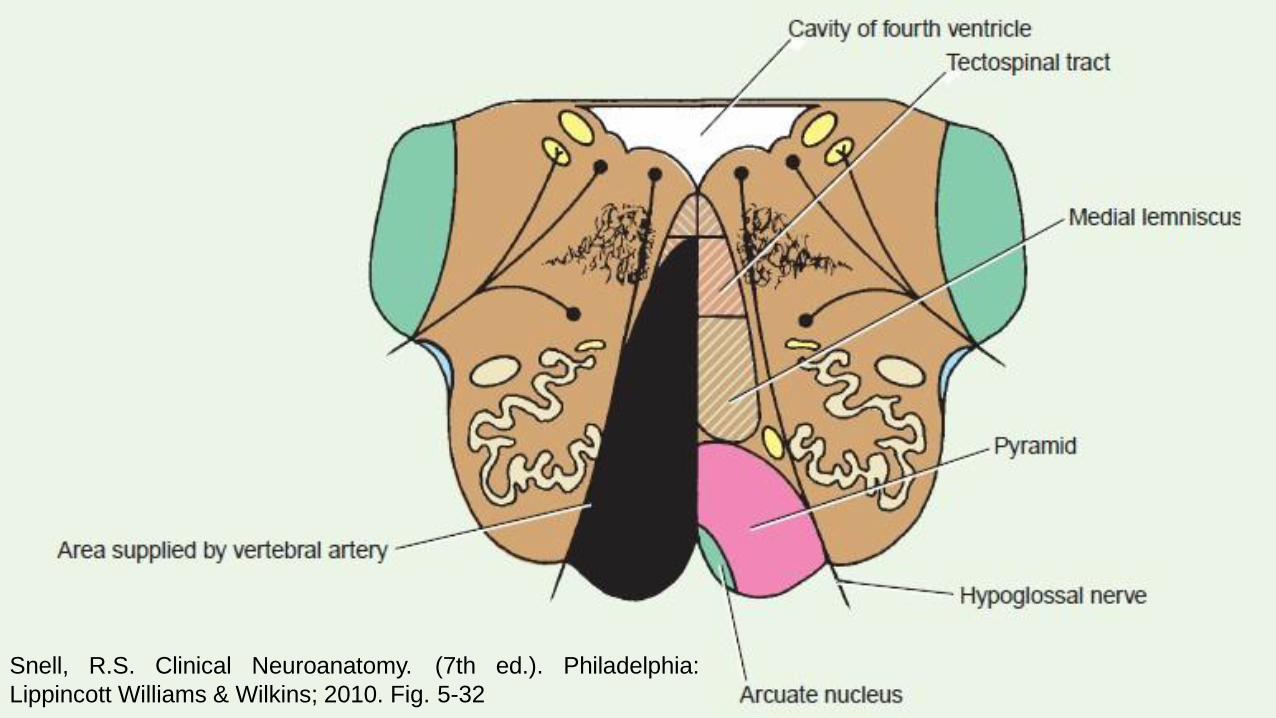
56Snell, R.S. Clinical Neuroanatomy. (7th ed.). Philadelphia:
Lippincott Williams & Wilkins; 2010. Fig. 5-32

FurtherReadings
53
● Sinnatamby, C.S. Last's Anatomy Regional and
Applied. (12th ed.). : Churchill Livingstone; 2011.
● Snell, R.S. Clinical Neuroanatomy. (7th ed.).
Philadelphia: Lippincott Williams & Wilkins; 2010.

FurtherReadings
54
● Eljack, A. A. E. Eljack’s Lecture Notes in
Neuroscience. Khartoum; 2015.
● Siegel, A, Sapru, H.N. Essential Neuroscience.
(3rd ed.). Philadelphia: Lippincott Williams &
Wilkins; 2015.

● Waxman, S.G. Clinical Neuroanatomy. (27th
ed.). :McGraw-Hill; 2013.
● Medical Neuroscience MOOC by Duke
University |Coursera.
● Haines, Duane. Fundamental Neuroscience For
Basic And Clinical Applications. 4th ed.
Philadelphia: Elsevier, 2013
FurtherReadings
55