Bordetella pertussis presentation
14
Whooping Cough: You Won’t be Bored When I Tella ‘Bout This Kaitlin Allinger
-
Upload
john-demeter -
Category
Healthcare
-
view
183 -
download
2
Transcript of Bordetella pertussis presentation
Whooping Cough:You Won’t be Bored When I Tella
‘Bout This Kaitlin Allinger

Patient Information• Whoopi G., a 7 month old female, was brought to the hospital
because she had been experiencing numerous rapid coughing episodes that end with a long inspiratory effort that makes a “whoop” sound.
• These episodes sometimes cause her to turn blue and/or vomit.
• It was also noted that during the week prior to these episodes she had a runny nose, sneezing, occasional coughing, and a low-grade fever.
• Physical examination revealed that her pulse was 165 beats per minute and respiratory rate was 70 breaths per minute.
• A CBC was ordered and showed elevated lymphocytes.
• Gram-negative coccobacilli were recovered from a specimen collected from the posterior nasopharynx.
• The patient was diagnosed with whooping cough.
Explanation of Patient History and Results• A characteristic symptom is repetitive coughing spells that
cause a patient to gasp for breath
• Can lead to cyanosis and vomiting
• Lymphocytosis
• Caused by pertussis toxin
• Elevated pulse and respiratory rate
• Coughing spells cause difficulty breathing
• Insidious onset
• Initial symptoms similar to the common cold

Clinical Significance
• Bordetella pertussis • Causative agent of whooping cough
• Primarily affects infants and young children, especially if they are not vaccinated
• Adults and adolescents can become infected, but the disease is much milder and may be asymptomatic
http://www.cdc.gov/vaccines/pubs/pinkbook/pert.html#diagnosis
Clinical Significance
• Complications include:
• Secondary bacterial pneumonia- 5.2%
• The cause of most pertussis-related deaths
• Seizures- 0.8%
• Encephalopathy – 0.1%
• Death – 0.2%
• 83% of deaths occur in infants <3 months

Clinical Features• Incubation period: usually 7-10 days• 3 Stages:
http://www.cdc.gov/pertussis/images/Pertussis-timeline-lg.jpg

Epidemiology
• Worldwide
• Infection only occurs in humans
• Adults are often the source of infection for children
• Highly contagious, especially during the first 1-2 weeks
• Transmitted by respiratory droplets
http://pathmicro.med.sc.edu/ghaffar/bord-hemo.htm

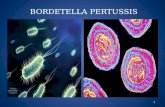
Culture Characteristics
• Aerobic Gram-negative coccobacilli
• Fastidious
• Regan Lowe Media (Charcoal Blood Agar)
• Selective for Bordetella sp.
• Incubate at 35C, moist chamber, ambient air
• Growth at 2 days
• Appearance on Regan-Lowe:
• -Small, domed, glistening,
white/gray colonies
https://catalog.hardydiagnostics.com/cp_prod/content/hugo/Regan-LoweCharcBldAgar.htm

Identification• Laboratory diagnosis of Bordetella pertussis by culture:
• 2 specimens, one through each nostril, collected from the posterior nasopharynx with a Dacron or calcium alginate swab
• Transport in Amies or Regan-Lowe transport medium
• Inoculate on Regan-Lowe agar (35C, ambient air, moist chamber)
• Hold for 7 days
• Identify suspicious colonies with a Gram-stain and fluorescein-labeled antisera or agglutinating antisera
• No routine susceptibility testing is performed
http://www.stanfordlab.com/esoteric/Virology.html
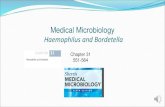
Virulence Mechanisms
• Pertussis toxin
• Contributes to bacterial binding of cilia, causes lymphocytosis, and impairs chemotaxis
• Adenylate cyclase toxin
• Inhibits phagocyte and NK cell functions
• Tracheal cytotoxin
• Inhibits DNA synthesis and promotes cell death
• Filamentous hemagglutinin and pertactin
• Attachment to epithelial cells

Fig. 1: Synergy between pertussis toxin and filamentous hemagglutinin in binding to
ciliated respiratory epithelial cells.
Tozzi A E et al. CMAJ 2005;172:509-515
©2005 by Canadian Medical Association
Treatment and Prevention
• Mostly supportive therapy
• Erythromycin is the drug of choice – used to decrease the number of organism in secretions to prevent the spread of infection
• Vaccine
• DTap (pediatric) or Tdap (adolescent and adults)
• Contains:
• Inactivated diphtheria and tetanus toxins
• Acellular pertussis subunit
http://ghstravelsafe.com/vaccinations/

Treatment and Prevention
• Pediatric vaccination schedule:
• 4 doses of DTap are given
• The first 3 doses given at 4- to 8-week intervals starting at 6 weeks to 2 months of age
• The fourth dose should be given at 15–18 months of age
• Adolescents and Adults
• Tdap is given as a booster (a weaker formulation)
• Given at 11-18 years of age (11 or 12 is recommended)
• Can also be given to adults 19-64 years old
http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/pert.pdf

Sources
• http://www.cdc.gov/vaccines/pubs/pinkbook/pert.html#diagnosis
• http://pathmicro.med.sc.edu/ghaffar/bord-hemo.htm
• http://www.cmaj.ca/content/172/4/509.full.pdf+html
• Mahon, Connie R., Donald C. Lehman, and George Manuselis. Textbook of Diagnostic Microbiology. Maryland Heights, MO: Saunders/Elsevier, 2011. 423-426. Print.