Bones and Joints PDF
12
Ruby Walsh The leading jockey underlines the importance of good joint care A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT MARCH WWW.HEALTHNEWS.IE INSIDE A patient case study on osteoporotic fractures P4 LEARN Dr Caitriona Cunningham on the basics of physiotherapy P6 EXPERT TIPS 10 steps to easier living with arthritis P10 Bones & Joints
-
Upload
ben-phillips -
Category
Documents
-
view
263 -
download
3
Transcript of Bones and Joints PDF

Ruby WalshThe leading jockey
underlines the importance of good joint care
A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT
MARCH WWW.HEALTHNEWS.IE
INSIDE A patient case study on osteoporotic fractures P4
LEARN Dr Caitriona Cunningham on the basics of physiotherapy P6
EXPERT TIPS 10 steps to easier living with arthritis P10
Bones & Joints

A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT2 WWW.HEALTHNEWS.IE MEDIAPLANET
Professor John O’Byrne, Profes-sor of orthopa-edic and trauma surgery at The Royal College of Surgeons in
Ireland (RCSI), believes that there is much room for improvement in the way that bone and joint injuries are treated, starting from the very first assessment where the accident took place.
“Irish healthcare, when it can be ac-cessed, is as good as anywhere else in the world,” says O’Byrne. “So the stan-dards of care are really high, but the problem is accessing the care.”
“I often speak with surgeons who have done some training in North America, Canada, Australia, no
matter where you go you will find that we are in a good place not just for orthopaedic surgeons but for all mem-bers of the teams. We have a good healthcare when it comes to trauma.”
The problems may rise in the logistics of dealing with these injuries. “We need to improve the organisation of the trauma services, and that means nominating some centres to take more trauma than other centres,” says O’Byrne.
At the moment, the orders for an emergency response team are to bring the patient to the closest hos-pital, regardless of the type of injury that he or she may be suffering.
This approach, according to O’Byrne, is highly mistaken, be-cause many hospitals do not have the right structures and facilities to
‘Bring patients to the right hospital,’ surgeon urges Ireland enjoys some of the best orthopaedic healthcare in the world, but the difficulty to access it can be detrimental, says one of the country’s leading experts
“Ireland has good healthcare, but we need to improve our organisation when it comes to trauma”
READ MORE ON WWW.HEALTHNEWS.IE
Which hip?Consultant orthopaedic surgeon Mr Stephen Kearns on how to make the right hip replacement choice P9
Dr Ossi Riekkinen On the benefits that new technology can bring when diagnosing osteoporosis, and the importance of early diagnosis P11
Patient case studySinead Torbin’s story underlines why it’s important for people to check if they have risk factors for osteoporosis
work on this type of injuries. “One thing that we would like to
see, as the RCSI, is that trauma pa-tients are not sent to hospitals that do not have orthopaedic surgeons anymore,” says O’Byrne.
“It is not right for the patient, it is not right for the hospital, it is not right for the doctor who receives the patient. Research has shown pretty conclusively that mortality and mor-bidity can be improved if patients are brought straight to a hospital where there is an orthopaedic surgeon.”
“In the UK there has been a good rationalisation of trauma services, in Ireland that is not as easy to do, be-cause the population’s spread is very different: of course most of the po-pulation is around Dublin, but if you look at the trauma, the traumas are
well spread around the country, and facilities differ from place to place.”
The issue is tricky, because it would bring responsibility to the ambulance team to assess where to carry a patient, and maybe choose a more distant hospital ahead of the more local one, because the farther hospital has better facilities. “We would never think of driving an-other hour with an injured patient, but if it is only 15-20 minutes, of course you would do it.”
“It is understandable the con-cerns that people have, and the reas-surance everybody gets as soon as the patient reaches the hospital, but if the carers could bring them to the right hospital and not just the clo-sest… it is just having a structure in place to allow them to do that.”
Please Recycle Follow us facebook.com/MediaplanetIE @MediaplanetIE @MediaplanetUK
Managing Director: Carl Soderblom Content and Production Manager: Henrietta Hunter Designer: Juraj Príkopa Sales Manager: Alex Williams Project Manager: Ben Phillips E-mail: [email protected] Mediaplanet contact information: Phone: +44 (0) 203 642 0737 E-mail: [email protected]
IN THIS ISSUE
Professor John O’ByrneProfessor of Orthopaedic &
Trauma Surgery at RCSI
By Ben Murnane

A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT4 WWW.HEALTHNEWS.IE
Fi f t y - t w o - y e a r-old Pat Sheehan maintains a heal-thy and active li-festyle, enjoying jogging and regu-lar games of golf.
But when Pat was 37, he under-went surgery after having a heart attack and now receives ongoing treatment plans and monitoring to keep his heart healthy.
Despite keeping up his healthy lifestyle Pat admits he was shock-ed to discover recently that he had a severe case of osteoporosis which
had caused a fracture to his spine.“Last August, I was about two
weeks into the Couch to 5k jog-ging programme when I felt a sud-den pain in my back,” says Pat. “I initially assumed it was muscle pain so I didn’t do much about it. About two weeks later, I was away on a golfing trip and was routinely swinging the golf club, when I ex-perienced another sharp pain in my back so I was advised to get an MRI scan.”
Mr John McCabe, Spine Surge-on at Galway University Hospitals, confirmed to Pat that his MRI scan
Pat Sheehan shares his experience of the balloon kyphoplasty procedure and discusses the stigma surrounding osteoporotic fractures
A case study on osteoporotic fractures
By Clodagh Dooley
Developing a pathway of care
COLUMN
Mr John McCabeSpine Surgeon at Galway University Hospitals
Many people who get spinal fractures in Ireland are never treated for the underlying disease: osteoporosis. Reasons for this include lack of knowledge and resources
Mr John McCabe, Spine Surgeon at Galway University Hospitals, emphasises that early screening and diagnosis of osteoporotic frac-tures is vital.
“With people living longer, it’s inevitable that a high proportion will suffer from bone weakness meaning there is an increase in pe-ople developing an acute, painful condition of the spine, where they develop a fracture. Osteoporosis isn’t purely an elderly disease - it can also effect anyone from young female athletes to active males.”
Balloon kyphoplasty is the key surgical procedure for treating oste-oporotic fractures where a cement-like material is injected into the fractured bone. However, Mr McCabe, who is also president of the Irish Spine Society, explains that this is currently poorly supported in Ire-land and access to spinal specialists with his level of expertise is low.
“Balloon kyphoplasty patients can expect a significant reduction in pain, an increase in their quality of life and maintenance of a nor-mal lifestyle,” says Mr McCabe, who performed the first kyphoplasty procedures in the UK and Ireland 14 years ago. There have been over five million cases internationally over the last 15 years and in some countries it’s well-funded, but we are well behind.”
“The treatment is there, the need is there, but unfortunately the services aren’t. We need a structure that we can roll out in the Irish health service for people with these fractures, a simple pathway for family doctors and their patients. We will fight our corner and try to get the resources allocated to develop services, but there needs to be a focus on it on a national level.”
INSPIRATION
Pat SheehanPatient and recipient of a
balloon kyphoplasty
DO YOU SUFFER FROM ACUTE BACK PAIN AS A RESULTOF OSTEOPOROSIS?PEOPLE WITH VERTEBRAL COLUMN FRACTURES HAVE LOTS OF QUESTIONS
For more information please visit the balloon kyphoplasty section on: www.medtronic.co.uk

MEDIAPLANETA SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT
had indeed shown signs of a fractu-re of his L2 (second lumbar vertebra) but this wasn’t the result of any vigo-rous exercise - the underlying cause was severe osteoporosis.
“I’m 52 and I would have thought that osteoporosis is a disease that el-derly women get. I certainly didn’t expect to be diagnosed but Mr McCabe made me aware of the fact that younger people and younger men, like myself, do get osteoporosis.
“After the scan, Mr McCabe was extremely helpful and suggested I undergo balloon kyphoplasty. It was under general aesthetic and an
inserted balloon placed the bone back into the original position whi-le added cement stabilised it. Thank-fully it worked out very well. Two days after, the pain I had been expe-riencing in my back was gone. I even went for a three-mile walk!”
This is one of the many benefits of balloon kyphoplasty – regular lifestyle routines don’t need to be sacrificed.
“I asked Mr McCabe how soon I could resume normal activities and he recommended weight-bearing ex-ercise – exercises that work against gravity in order to strengthen the bo-ne such as brisk walking.”
Although Pat does stand a signi-ficantly higher risk of future fractu-res because of his “extremely soft bo-nes”, continuing to treat the underly-ing cause, osteoporosis, is crucial to avoiding these.
“I’m now under the care of an ex-cellent rheumatologist, John Ca-rey, and have a long-term treatment plan, including a daily injection of medication for two years and a further regimen of treatment after-wards. Mr McCabe advised if I ever got a pain in my back again, the first thing I should do is get an MRI and not assume that it is something else.
“This applies to anyone in a simi-lar situation as me. If you have a per-sistent pain in your back and you can’t put your finger on what caused it, get an MRI scan to rule out an osteoporotic fracture or more sinis-ter causes, such as cancer. I feel that there’s an unawareness among the general population of osteoporosis and the potential bone breakages and fractures that you can get as a result – you don’t need to be old, in-active or fragile for this to occur. So if my experience helps to raise awareness in this area, then that’s a great thing.”
”If you have a
per sistent pain
in your back and
you can’t put your
finger on what
caused it, get it
checked”
Read more on www.healthnews.ie
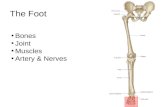
Step 1 Insertion of percutaneous cannula and balloon
Step 2Balloon inflation
Step 3Injection of Cement
Step 4Cannula Removal
The 4 steps of a balloon kyphoplasty
EXPERT TIPS
THE MEDTRONIC MISSIONTo contribute to human welfare through the application of biomedical engineering in the research, design, manufacture, and sale of instruments or appliances that alleviate pain, restore health and extend life
INTRODUCING BALLOON KYPHOPLASTY Understanding Vertebral Compression Fractures and Balloon Kyphoplasty Treatment
FRACTURE REDUCTION
VOID CREATION
STABILIZATION
UC201607226 EE EMO4899

A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT6 WWW.HEALTHNEWS.IE MEDIAPLANET
“One role of
the physio-
therapist is
to encourage
young people
to be active
so that they
can build
bone
strength”
A physiotherapist can work with a patient to decide on the most appropriate management for acute and long-term bone and joint pain — or help people who simply want advice about getting active
advise people to engage in impact and strengthening exercise throughout their lives to maintain bone strength and muscle health. “Some people av-oid exercise, either on the basis that it might be bad for their joints, or that they have osteoporosis,” actually, we all ex-perience muscle loss as we age and joint aches and pains are common but it can create more problems if you don’t stay active. Yet you may need guidance from a physiotherapist to get you started.”
If you have any concerns about bone or joint aches or pains, you can contact a pri-vate physiotherapy practitioner directly — but the advice is to always see your GP first. And when you choose a physiothe-rapist, make sure that they are a Charte-red practitioner. As state registration of Physiotherapists is on the way , this will provide greater transparency for mem-bers of the the public, enabling them to make more informed choices.
When the body’s mo-vement and fun-ction is threatened by factors including age, injury, disease,
joint and muscle conditions , your GP may refer you to a physiotherapist. This can be a misunderstood profession, with some patients believing that a physioth-erapist will simply offer manual thera-py or manipulation of affected areas and they may: yet physiotherapy is a much broader healthcare specialty than that.
“A physiotherapist takes a holistic view,” says Dr Caitriona Cunningham of the Irish Society of Chartered Physiothera-pists, the professional body representing over 3,000 Chartered Physiotherapists in Ireland. “Their role is to assess the indivi-dual, come to a clinical diagnosis and then work with the patient to decide on the most appropriate management for them. They may ask: is exercise the most appro-priate approach in this particular case, at this point in time? Will this patient benefit from manual therapy or a joint injection? Does this person need further investiga-tions, and/or medications? They’ll be able
to offer treatment and advice for acute bone and joint pain based on current best evidence, and provide guidance on long-term bone and joint pain management which will usually involve exercise.They also have knowledge of the appropriate re-ferral pathways in the health system”
Self-managementSome people presenting to a physiothe-rapist with joint aches and pains may be diagnosed with arthritis or degenerative changes of their joints, says Cunningham. But, she stresses, if arthritis is diagnosed, a physiotherapist will be able to help the patient self-manage the condition, even if it becomes chronic. “Some people need to see a professional to be empowered to ma-nage their chronic conditions,” she says. “Physiotherapy can help do that, and so maximise function and quality of life.”
Yet physiotherapists don’t only of-fer treatment to those with acute or ch-ronic pain. “They can also advise people who are feeling well to get active,” says Cunningham. “Increasing numbers of physiotherapists are focussing on health promotion and primary prevention. For
example, if you want to take up exerci-se but are concerned about keeping your joints healthy, a physiotherapist can as-sess you and advise which exercises to do and which ones to avoid.”
Keeping activeIn terms of bone health and osteoporo-sis, one role of the physiotherapist is to encourage young people to be active so that they can build bone strength and to
Physiotherapy: an active approach to bone and joint health
By Tony Greenway
We all ex perience muscle loss as we age, so physiotherapists promote staying active
Dr Caitriona Cunningham Irish Society of Chartered
Physiotherapists
Read more on www.healthnews.ie
PHOTO: THINKSTOCK


A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT8 WWW.HEALTHNEWS.IE MEDIAPLANET
What is buttermilk?Cuinneog Buttermilk is the luscious liquid left over
from the churning of our fabulous fermented
Cuinneog Country Butter.
HEALTH BENEFITS OF BUTTERMILKButtermilk is low in fat ( less than 1%), high in potassium, vitamin
B12, calcium and riboflavin which is important for body growth and
red blood cell production. It aids in the release of energy from
proteins. Buttermillk is also a good source of phosphorus.
Those with digestive problems are often advised to drink buttermilk,
as it is more quickly digested. Buttermilk is not only good for your
insides it is also great for your skin.
Cuinneog fermented Butter & Buttermilk are available to buy
nationwide in Supervalu, Dunnes Stores & Tesco and also in
independent artisan stores. www.cuinneog.com
“The best
strategy
to avoid
injury is
just to stay
fit and
strong:
this will
minimise
damage
and
enable
quicker
recovery”
Irish champion jockey Ruby Walsh speaks about the many injuries he’s had in his career, and what keeps him going in spite of the risk
stay fit and strong, be in the best shape possible to minimise damage and also to enable your body to recover quicker.”
Irish Injured JockeysWalsh is currently chairman of Irish Injured Jockeys, which was establis-hed in 2014 in order to increase awa-reness and raise funds for injured jockeys. No doubt his own experience of injury helped him realise the im-portance of the organisation.
“Irish Injured Jockeys was set up to gi-ve support to riders at various stages of their lives when they need it. This can be in the form of tangible support when they are out due to injury, assistance in education or retraining during or after their riding career is over, or support in their lives post-riding.”
Irish Injured Jockeys is totally fun-ded by donations and fundraising from within the horseracing industry and the wider public. They have an office in the RACE complex in Kildare Town, where they provide a valuable resource and con-tact point for jockeys as well as a central administration for people who may wish to undertake fundraising or make dona-tions. Visit their website at irishinjured-jockeys.com to find out more.
As for Walsh and his own career – he still has many wins in him yet, he reck-ons. “I still have a great hunger for the competition and get immense satisfac-tion from what I do,” he says.
Injuries go with the territory but are not slowing him down.
“Injuries don’t affect my drive or ent-husiasm. The mind forgets physical pain quickly enough!”
Ruby Walsh is no stranger to bone and joint injuries. The nine-time leading jockey at Chelten-ham and multiple Grand National win-
ner has – like all the best jockeys – had many falls during the course of his care-er, leading to fractures, broken bones and dislocated shoulders.
Who would choose such a dangerous profession? “There are undoubtedly risks every time you go out,” admits Walsh. “But what keeps me going is that I love what I do – I’ve always wanted to be a jockey, since I was a young kid.”
Walsh has broken the same leg twice, suffered wrist fractures, broken arms, cracked vertebrae, a dislocated hip, a cracked elbow, dislocated shoulders – and more. Despite all this, he considers himself one of the lucky ones.
“Even though I’ve had many injuries, I’ve escaped anything really serious. I’ve only had one operation – for shoulder li-gament damage.”
His worst ever injury was a dislocated right hip, he says; this occurred in 2001 at Listowel. “This was extremely painful, and kept me out for eight weeks.”
Treatments and preventionTreatments for Walsh have mostly invol-ved rest and taking prescribed medica-tions, along with physiotherapy and rehab.
“Physiotherapy and rehab have been vital for my recovery – they still are for most injuries.
“Doctors even now differ on recovery plans,” Walsh says. “Medical practice has
changed somewhat – it used to be that rest was seen as the main tool for recove-ry, but now pressure is regularly advised rather than rest.”
It can also happen, of course, that a jockey suffers an injury he is not initially aware of – this is particularly dangerous, as it is prone to get worse without recog-nition and treatment. Walsh once had what turned out to be a crushed T7 verte-brae, which was only diagnosed and tre-ated four weeks after it happened.
Early diagnosis is obviously key – but once you are correctly diagnosed, pa-tience and keeping up with your treat-ment regimen are the most important things, says Walsh. “Time is really the best cure, when it comes to making a full recovery.”
Walsh laughs when asked if there are any strategies he can share in terms of avoiding injury. “Don’t fall!
“But seriously, it is inevitable that falls will happen, so the best strategy is just to
Miracle manBy Clodagh Dooley
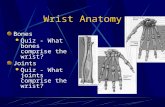
A HISTORY OF RUBY WALSH’S INJURIES
NEWS
Ruby WalshChampion jockey and chairman,
Irish Injured Jockeys
Broken legs
(1999/2000)
Dislocated hip
(2001)
Dislocated
shoulder
(2007)
Double
leg-break
(November 2010)
Two fractured
wrists
(2000)
Fractured hip
(2003)
Broken arm
(April 2010)
Crushed vertebra
in neck
(July 2011)

WWW.HEALTHNEWS.IE 9MEDIAPLANET A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE INDEPENDENT
“The best
choice
balances
the latest
technology
with a
proven track
record”
Mr Stephen Kearns on technology versus track record
to be more wear-resistant, so a cerami-cised ball with a cross-linked poly-lined cup appears to be a good option.”
The use of cement is also an issue. A majority of hip replacements in Ireland are cemented - the pin is secured into the cavity of the femur with cement. Where cement is used it releases chemi-cals into the bloodstream, in rare cases causing cardiac issues. Hips can be im-planted without cement, these hips are securely implanted (hammered into pla-ce) and then have a special coating that makes the bone grow onto the stem. Ce-ment may be a good choice where the bone is thin or the cavity of the femur is very wide. However both cemented and uncemented hip components have de-monstrated excellent results.
Overall, he insists: “No one material or procedure suits everyone. The choice should be based on the individual patient and the experience of the surgeon.”
The science of hip re-placement has pro-gressed significant-ly since its inception and remain one of the most successful med-ical procedures ever
devised. There is a huge choice of devi-ces from multiple manufacturers avai-lable, but the newest or most expensive are not always the best choice.
“Patients often ask for the newest technology but hips have to last as long as possible. So, in fact, the best choice ba-lances the latest technology with a pro-ven track record and take into account the individual patient,” says Mr Stephen Kearns, consultant orthopaedic surgeon, Galway university hospitals.
A total hip replacement consists of a metal and/or plastic cup to replace the natural socket and a ball replacing the natural head of the femur. A stem is
placed in the cavity of the femur to sup-port the artificial head. The most com-monly used in Ireland today are those with a metal ball and a polyethylene (‘po-ly’) cup. However hips can be implanted as an all ceramic combination or just a ceramic femoral head.
There is however one other option: the ceramicised metal ball and poly cup. The ceramicised ball is created by heating metal to high temperatures, converting the surface layer into a ceramic.
To clarify which is the best option sur-geons world wide have been collecting data on patients after hip replacement in joint registries. Data from one of the-se, the Australian Joint Registry, shows that after ten years ceramicised metal on poly joints require revision (replace-ment) in 3.3 per cent of cases whereas for metal on poly the figure is 4.3 per cent. Hips comprising ceramic on poly had a 4.6 per cent revision rate and ceramic on
ceramic 5.1 per cent. Similar trends are seen in registries world wide.
The type of poly also makes a difference: “Cross-linked poly, where the material has been modified, appears
Hip Replacement –Choosing the hip for you
Mr Stephen KearnsConsultant orthopaedic surgeon,
Galway university hospitals

A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT10 WWW.HEALTHNEWS.IE MEDIAPLANET
“Osteopenia
and
osteoporosis
are wisepread
issues and we
must continue
to raise
awareness”
Osteoporosis is a disease which causes the insides of a person’s bones to become fragile and break very easily
Coeliac Disease (gluten sensitivity), Crohn’s disease or Ulcerative Colitis.
It is important to note that many pe-ople who get the blood test for Coeliac di-sease are negative. A person can be gluten sensitive, but not a true Coeliac. Therefore if a Coeliac test is negative but symptoms persist, a gluten and wheat free diet may reduce or eliminate symptoms.
There are nearly 200 causes of bo-ne loss. It’s time to ask the question: do you have any risk factors? It is es-sential that any causes of bone loss are found and addressed, not assumed. The causes can be found by blood tests and an extensive questionnaire. So-me of the most common causes are: low levels of Vitamin D, family his-tory of a broken hip, the menopause, steroids, chemotherapy, eating disor-ders, stress, excess alcohol and smo-king to name a few.
Osteopenia and osteoporosis are widespread issues and we must conti-nue to raise awareness. For more infor-mation, take a look at the activities of the Irish Osteoporosis Society Charity. The Charity runs the National helpli-ne and can be contacted at 01 637 5050 and on irishosteoporosis.ie
It is known as the “Silent di-sease”, but the effects are not silent. Osteoporosis is a major public health hazard with a high death rate for those undiagnosed. €500+ million was spent in 2013
just on treating broken bones. Osteoporosis is preventable and treatable in the majority of pe-ople, but only 15 per cent are di-agnosed, leaving 280,000 undi-agnosed. Osteopenia is the early stages of Osteoporosis, however more people break bones in this range than with Osteoporosis.
50 per cent of women and 25 per cent of men over 50 have osteoporosis, and it affects all age groups, including children and pregnant women. This is why it is essential that parents ensure their children have a diet rich in calci-um and vitamin D, along with being physically active.
There is a major problem worldwide of low levels of Vitamin D, particularly in postmenopausal women. In Ireland 74 per cent of adults and 88 per cent of primary school children take less than half of the recommended daily amounts of vitamin D. Vitamin D is not only essential for bone health, but is al-so important for muscle function and
balance. A deficiency of Vitamin D can cause rickets in children and osteomalacia in adults.
Unfortunately, Ireland does not have the weather for people to get their vitamin D from the sun throughout the year, which presents problems gi-ven that it is essential for the absorp-tion of calcium. Milk supplemented by Vitamin D, fortified yogurts and oily fish are very easy ways to get your daily amounts. A 200ml glass of fortified milk contains approximately 40 per cent of your daily recommended Vitamin D (5ug) and a litre of fortified milk con-tains the daily amount of Vitamin D.
A growing number of human meta-bolic, epidemiologic, and animal stu-dies are indicating that low levels of Vi-tamin D, appear to be linked to the fol-lowing conditions: Immune function diseases such as: breast, colon and pro-state cancer) Type 1 Diabetes and mul-tiple sclerosis, but further research is required to prove and understand the-se links. Low Vitamin D levels have al-so been associated with TB and Fibro-myalgia, and low levels this vitamin in a person can mimic the aches and pains of fibromyalgia.
In more extreme cases, a lack of absorption of Vitamin D may occur in gastrointestinal disorders such as
Osteoporosis and Vitamin DBy Professor Moira O’Brien FRCPI, FFSEM, FFSEM (UK) FTCD
Read more on www.healthnews.ie
NEWS
Getting enough Vitamin D,calcium and protein as wellas regular weight-bearingexercise is the key tomaintaining bone health. Butin Ireland people of all agesaren’t getting enough VitaminD*. That’s why we need to topup our levels through foods that offer plenty of Vitamin D – likeAvonmore Super Milk, which provides 100% of your dailyVitamin D needs in just one glass**.
Find out more about SuperMilk and Vitamin D atavonmore.ie/supermilk
YOUR DAILY VITAMIN D, AT EVERY AGE.
* Irish Universities Nutrition Alliance.** EU Reference Intake.
SUPPORTING HEALTHY BONES FOR LIFE.
10 Steps to Easier Living with Arthritis
EXPERT TIPS
5Find new ways to stay active
2Don’t delay, see your doctor
1Don’t delay, see your doctor
6 Learn techniques to help manage your pain
3Work with your healthcare team and be an important part of it
7Acknowledge your feelings and seek support
9Balance your life
4Know about your treatment options
8Make food choices that count
10Make contact with Arthritis Ireland
Professor Moira O’BrienPresident, Irish
osteoporosis society
Source: Arthritis Ireland

WWW.HEALTHNEWS.IE 11MEDIAPLANET A SUPPLEMENT BY MEDIAPLANET DISTRIBUTED WITHIN THE IRISH INDEPENDENT
Bindex® is the world’s first pocket-sized, research-proven tool for osteoporosis screening and diagnostics.
Osteoporosis diagnostics are currently performed only at secondary care. Bindex® was created to cover this early diagnosis gap; it has been validated according to international guidelines, and its measurements are thus comparable to standard diagnostic procedures using dual energy x-ray absorptiometry (DXA).
Bindex® offers research-proven accurate results comparable to DXA, and has a 90% accuracy in detecting osteoporosis or an increased risk for the disease.
www.bindex.fi
“One of
the major
challenges
is the
pathway
from
primary
care to
larger
hospitals”
Dr Ossi Riekkinen discusses the importance of diagnosing osteoporosis early, and the role of new technology in achieving this goal
do not have to wait for a DXA scan to receive an initial diagnosis.
“A just-published article in Oste-oporosis International shows that if we use such devices in primary healthcare, we can diagnose about 70 per cent of patients to be either healthy or osteoporotic – only 30 per cent really need a DXA scan.”
Riekkinen thinks that technological developments can play a major role in improving access to swift diagnosis, in turn improving access to treatments and enabling a greater quality of life.
“There is a saying: Cancer may kill you but osteoporosis may take your life.
“In the EU as a whole, the annual cost of bone fractures is about €40 bil-lion. But the real cost is the human cost. It is so important to be able to di-agnose osteoporosis early and prevent as many fractures as possible.”
Osteoporosis is a severe condi-tion, where the sufferer’s bone mass and structu-re have changed and so he or she is
more prone to fractures and bone brea-kage. The primary group at risk is post-menopausal women, but the disease can affect younger women and men too.
The current gold-standard method for diagnosing osteoporosis is Dual Energy X-ray Absorptiometry – what’s known as a DXA or DEXA scan. This usually involves attending a large central hospital, where the patient’s bone density is measured.
Globally, over 75 per cent of osteoporo-sis sufferers go undiagnosed and never receive treatment.
Dr Ossi Riekkinen, a medical phy-sicist and co-founder of a Finnish start-up, Bone Index, says that early
diagnosis is crucial: “If you have an osteoporotic fracture, that is a most sig-nificant risk factor for another fracture, so it is extremely important to find pa-tients early and treat them.”
One of the major challenges when it comes to diagnosis is the pathway from primary care to the larger hospitals where DXA scanning is available: due to costs, only patients in a few high-risk groups receive automatic referral, and waiting lists can be long.
Riekkinen offers an example from his own family: “My mother-in-law is in her mid-80s; she is still very ac-tive mentally, but she can hardly move due to several fractures in her spine – she had already experienced two or three fractures before she was able to get a referral for bone density measurement. The reason for her frac-tures is osteoporosis, but she had to wait for a formal diagnosis.”
There are now new scanning devices that can be used to detect osteoporosis in a primary care setting, or by a doc-tor or nurse on a home visit. Patients
OsteoporosisNew technologies bring new hope
By Ben Murnane
Dr Ossi RiekkinenMedical physicist and co-founder
of Bone Index