
bone support broch · FASE INYECTABLE ESPERA FASE MODEABLE 0 30s 3 min 5 min 7 min 9 min ~15 min...
8
CERAMENT |BONE VOID FILLER Rapid and complete bone remodeling ® TM
Transcript of bone support broch · FASE INYECTABLE ESPERA FASE MODEABLE 0 30s 3 min 5 min 7 min 9 min ~15 min...

CERAMENT |BONE VOID FILLERRapid and complete bone remodeling
®
TM
PR 0364-03 en US Brochure_single page layout.indd 1 21/09/2018 10:56

CERAMENT |BONE VOID FILLERCERAMENT is an injectable, moldable, drillable and radiopaque bone substitute which provides rapid and complete bone remodeling within 6-12 months1,2,3.
Consistent mixing and handling that is true to the time chart
3 min 5 min30s0 7 min 9 min ~15 min
Si no se requiere brocado para lacolocación de tornillos, la herida puede cerrarse en
cualquier momento despues de 10 minutos
MEZCLADO ESPERA ESPERABROCADO Y COLOCACIÓN DE TORNILLOS
FASE INYECTABLE ESPERA FASE MODEABLE
3 min 5 min30s0 7 min 9 min ~15 min
MIX WAIT WAITDRILLING& SCREW INSERTION
INJECT WAIT MOLD
Time and use chart
3 min 5 min30s0 7 min 9 min ~15 min
If drilling & screw insertion is not required, the wound can be closed
anytime after 10 minutes
MIX WAIT WAITDRILLING & SCREW
INSERTIONINJECT WAIT MOLD
R Injectable, Moldable, Drillable1,2,3
R Rapid and complete bone remodeling1,2,3
R Highly visible under � uoroscopy 2
R 30 second, enclosed mix
R Not temperature sensitive
R Non-exothermic
R Robust clinical data
Unique features:
REFERENCES1. Svacina. Case Reports in Orthopedics Volume 2016, Article ID 4160128.
2. Kaczmarczyk et al. BMC Musculosketelal disorders (2015) 16:369
3. Abramo et al J Biomed Mater Res Part B: Appl Biomater 92B: 281–286, 2010.
4. Nilsson M, Zheng M H, Tägil M: Expert Rev. Med. Devices 10(5), 675-684, 2013.
5. Nilsson M, Wang JS, et al. J. Bone Joint Surg. Brit. 86B(1), 120-125,
6. Voor MJ, Borden J, Burden RL Jr, Waddell SW. Cancellous bone defect healing with a novel calcium sulfate - hydroxyapatite composite injectable bone substitute.Presented at: 56th Annual Meeting of the Orthopaedic Research Society, New Orleans, 2010..
®
®
PR 0364-03 en US Brochure_single page layout.indd 2 21/09/2018 10:56
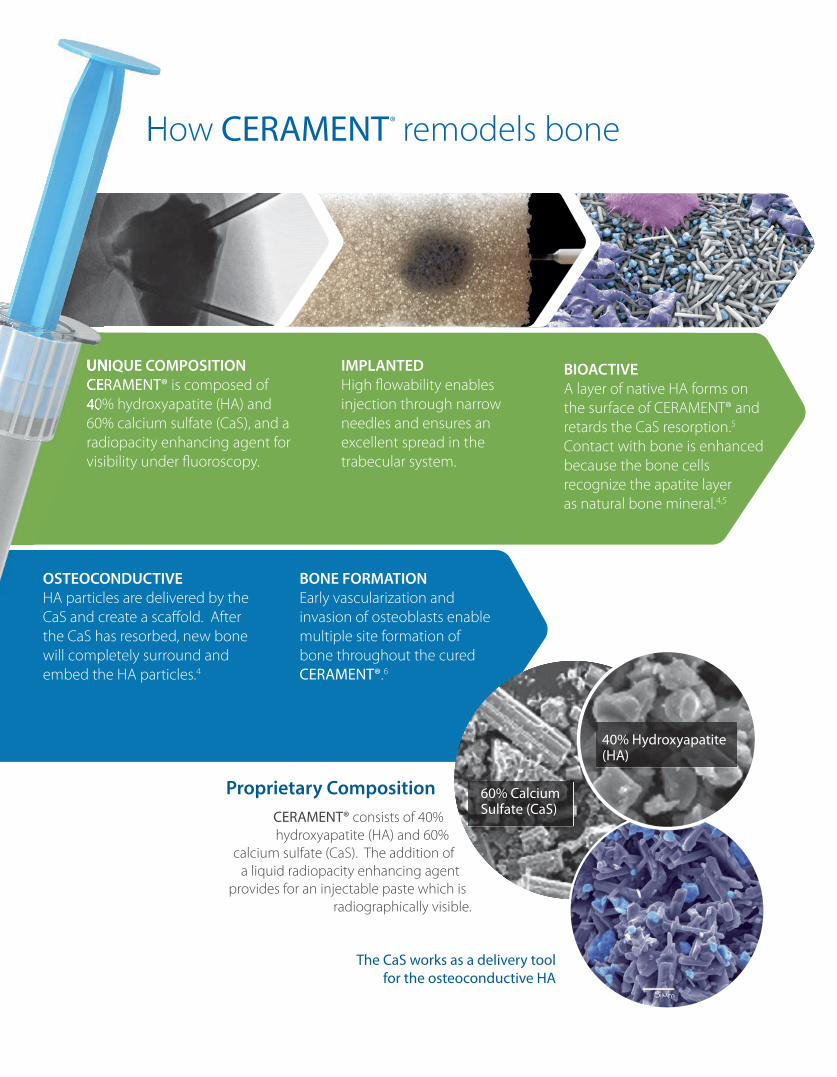
IMPLANTEDHigh fl owability enables injection through narrow needles and ensures an excellent spread in the trabecular system.
BIOACTIVEA layer of native HA forms on the surface of CERAMENT® and retards the CaS resorption.5 Contact with bone is enhanced because the bone cells recognize the apatite layer as natural bone mineral.4,5
OSTEOCONDUCTIVEHA particles are delivered by the CaS and create a scaff old. After the CaS has resorbed, new bone will completely surround and embed the HA particles.4
BONE FORMATIONEarly vascularization and invasion of osteoblasts enable multiple site formation of bone throughout the cured CERAMENT®.6
How CERAMENT remodels bone
The CaS works as a delivery tool for the osteoconductive HA
Proprietary CompositionCERAMENT® consists of 40% hydroxyapatite (HA) and 60%
calcium sulfate (CaS). The addition of a liquid radiopacity enhancing agent
provides for an injectable paste which is radiographically visible.
UNIQUE COMPOSITIONCERAMENT® is composed of 40% hydroxyapatite (HA) and 60% calcium sulfate (CaS), and a radiopacity enhancing agent for visibility under fl uoroscopy.
60% CalciumSulfate (CaS)
40% Hydroxyapatite (HA)
®How
UNIQUE COMPOSITIONCERAMENT®40% hydroxyapatite (HA) and
PR 0364-03 en US Brochure_single page layout.indd 3 21/09/2018 10:56

Proven Results More than 9 years of clinical evidence, more than 40 pre-clinical and clinical studies and four year patient follow-up data, demonstrate the safety, effi cacy and long-term bone remodeling capabilities of CERAMENT®.
Case 1: Trauma
Bicondylar Osteoporotic Tibial PlateauFractureA female (88 years old) underwent open reduction and internal fi xation of angulated, impacted, displaced and unstable left tibial plateau bicondylar fracture, with percutaneous lateral plate application.
CERAMENT®|BONE VOID FILLER was injected to fi ll resulting void after fracture reduction. Fig A & B.
At 18 months patient was clinically improved and ambulating well.
Radiographs showed remodeling of CERAMENT®|BONE VOID FILLER into new bone. Fig C & D.
Figure C. At 18 months anteriorposterior radiograph demonstrating excellentincorporation of CERAMENT®|BONE VOID FILLER into new bone.
Figure D. At 18 months lateral radiograph demonstrating excellent incorporation of CERAMENT®BONE VOID FILLERinto new bone.
Figure A. Intra operative anterior-posterior radiograph placement of CERAMENT®|BONE VOID FILLER
Figure B. Intra operative lateralradiograph placement of CERAMENT®|BONE VOID FILLER
Credit:
Dr. Prashant Desai, D.O.Lakeland Regional Medical Center, Lakeland, Florida, USA
PR 0364-03 en US Brochure_single page layout.indd 4 21/09/2018 10:56

Case 2 : Reconstructive Orthopedics
Hip RevisionA 61-year old male with a history of well- positioned, well functioning bilateral uncemented THAs presented with progressive left hip pain over 6 months.
X-rays showed a large cystic osteolytic lesion in the left acetabulum involving the superior dome and the medial wall with extension into the ischium. CT scan confi rmed extensive amount of osteolysis.
Intraoperatively, signifi cant wear of the polythylene liner allowing subluxation of the femoral head was found. The cup was solidly fi xed and was not revised. The femoral head was exchanged for a new 32 mm head and the liner was ex-changed to a10-degree elevated lip liner.
A 2x2cm window was made above the acetabulum at the level of the cyst.
The cyst was curetted and fi lled with 32cc CERAMENT®|BONE VOID FILLER (Fig. 1). Once CERAMENT® had set, the wound was irrigated and closed.
At 6 weeks post-op, the patient had good and painless range of motion and was weight-bearing without aides. X-rays confi rmed good positioning of the ac-etabular implant CERAMENT® is still visible (Fig. 2). At 11 weeks post-op, CE-RAMENT® is no longer visible (Fig. 3).
At 8 months post-op, the patient was doing well and was pain-free. X-rays demonstrated CERAMENT® to be nearly completely resorbed and replaced with new cancellous bone (Figs. 4 & 5).
Figure 1. Figure 2.
Figure 3. Figure 4.
Figure 5.
Credit:
Thomas Baier, M.D.Advocate Condell Medical Center, Libertyville, IL USA
PR 0364-03 en US Brochure_single page layout.indd 5 21/09/2018 10:56

Case 3 : Foot and Ankle
Treatment of displacedintra-articular calcaneal fracture
A female (54 years old) with a displaced intra-articular calcaneal fracture had open reduction and internal fi xation (ORIF) (Fig. A). The resulting bone void after fracture reducation was fi lled with CERAMENT®|BONE VOID FILLER.
Removal of the plate at 5 months due to pain (no signs of infection) facilitated a bone biopsy which showed early signs of new bone growth where CERAMENT® was implanted (Fig B).
At 7 months the patient demonstrates a good result and is fully weight-bearing. (Fig. C).
Figure A. X-ray immediately post surgery.
Figure B. Histology at 5 months showing new bone growth.
Figure C. X-ray after removal of the plate and is fully weight-bearing.
Credit:
Damiano PapadiaReparto di Ortopedia e, Traumatologia Ospedale, Santa Chiara, Trento, Italy
PR 0364-03 en US Brochure_single page layout.indd 6 21/09/2018 10:56

Case 4 : Ortho-Oncology
Minimally Invasive Treatment of a Benign Proximal Humeral Cyst
Large unicameral bone cyst (UBC) of the proximal humerus with thinning of proximal cortices (Fig. 1).
The cyst was aspirated using a large-boreneedle then exchanged for a cannulafor pressure relief during injection of CERAMENT®|BONE VOID FILLER (Fig. 2, 3).
An additional cannula was placed into the distal part of the cyst. The CERAMENT®|BONE VOID FILLER delivery syringe was attached to the end of the distal cannula and injected one minute after mixing to ensure complete fi lling of the void via a bottom-to-top (distal to proximal) technique.
30cc of CERAMENT®|BONE VOID FILLER was injected. Iohexol provides visibility of product under fl uoroscopy (Fig. 3) and the post-operative radiograph (Fig. 4).
6 week X-ray demonstrates a white ‘halo eff ect’ outlining the cyst (Fig. 5). At 3 months, early bone remodeling is seen, along with a ‘puddling eff ect’ at bottom of cyst (Fig. 6).
5 month X-ray shows on-going replacement of CERAMENT®|BONE VOID FILLER with new cancellous bone (Fig. 7).
Figure 1. Figure 2.
Figure 3. Figure4.
Figure 5. Figure 6.
R R
RR
Figure 7.
Credit:
Joseph Benevenia, M.D.Rutgers University Hospital, Newark, NJ
PR 0364-03 en US Brochure_single page layout.indd 7 21/09/2018 10:56

1.877.719.6718 | [email protected] order
BONESUPPORT, INC., 60 William St, Suite 330, Wellesley, MA 02481
Restoring health to improve the quality of life for patients with bone disorders.
T: 1.877.719.6718 www.bonesupport.com
TM
Ordering Information
Product
Zimmer Biomet Codes (goodthrough 5/20/19)
CERAMENT®|BONE VOID FILLER 5 mL A0210-09 800-4000
CERAMENT®|BONE VOID FILLER 10 mL A0210-08 800-4001
CERAMENT®|BONE VOID FILLER 18 mL A0210-11 800-4002
PR 0346-03 en US
Acetabular revision surgery utilizing CERAMENT®|BONE VOID FILLER3
Pre-operative acetabular fracture
RECONSTRUCTIVE ORTHOPEDICS
RECONSTRUCTIVE ORTHOPEDICS
At 12 months - bone remodelingand hip mobility observed radiographically3
Pre-operative ap radiograph of tibial plateau fracture1
TRAUMA TRAUMA
THE PROBLEM THE SOLUTION
Intra-operative ap radiograph showing placement of CERAMENT®|BONE VOID FILLER1
At 18 months ap radiograph demonstrating excellent incorporation of CERAMENT®|BONE VOID FILLER by new bone1
Pre-operative lateral radiograph of calcaneal bone cyst2
BONE CYST BONE CYST
Intra-operative percutaneousreplacement of bone void with CERAMENT®|BONE VOID FILLER2
24-month post-operative lateral radiograph demonstrating complete incorporation by bone2
REFE
REN
CE IM
AG
ES R
EPRO
DU
CED
BY
KIN
D P
ERM
ISSI
ON
OF:
1. D
r P D
esai
, Lak
elan
d Re
gion
al m
edic
al C
ente
r, La
kela
nd F
lorid
a U
SA
2
. D
r L D
iDom
enic
o, A
djun
ct P
rofe
ssor
, Ohi
o Co
llege
of P
odia
tric
Med
icin
e, Y
oung
stow
n, O
hio,
USA
3.
Dr J
Sva
cina
, Bod
den-
Klin
iken
Rib
nitz
-Dam
gart
en, G
erm
any
BONESUPPORT Codes (e� ective 10/21/18)
PR 0364-03 en US Brochure_single page layout.indd 8 21/09/2018 10:56


















