
Bone, soft tissue and skin tumors - كلية الطب · Soft tissue tumors •soft tissue refers...
30
Bone, soft tissue and skin tumors By: Shefaa’ qa’qa’
-
Upload
truonghanh -
Category
Documents
-
view
229 -
download
0
Transcript of Bone, soft tissue and skin tumors - كلية الطب · Soft tissue tumors •soft tissue refers...
Bone, soft tissue and skin tumors
By: Shefaa’ qa’qa’
Bone tumors
• Most bone neoplasms develop during the first several decades of life and have a propensity for the long bones of the extremities.
• The occurrence in certain age groups and predilection for particular anatomic sites provides important diagnostic clues about specific types of tumors. For example, osteosarcoma peaks during adolescence and most frequently involves the knee whereas chondrosarcoma affects older adults and involves the pelvis and proximal extremities.
• metastases (adenocarcinoma) and hematopoietic tumors far outnumber primary bone neoplasms.
• Bone sarcomas are lethal in 50% of cases.
• Bone tumors may present in a number of ways. The more common benign lesions are often asymptomatic incidental findings. Many tumors, however, produce pain or a slow-growing mass. In some circumstances the first hint of a tumor’s presence is a pathologic fracture.
• Radiographic imaging studies have an important role in diagnosing these lesions. In addition to providing the exact location and extent of the tumor, imaging studies can detect features that narrow the diagnostic possibilities. Ultimately, in almost all instances biopsy is necessary for definitive diagnosis.
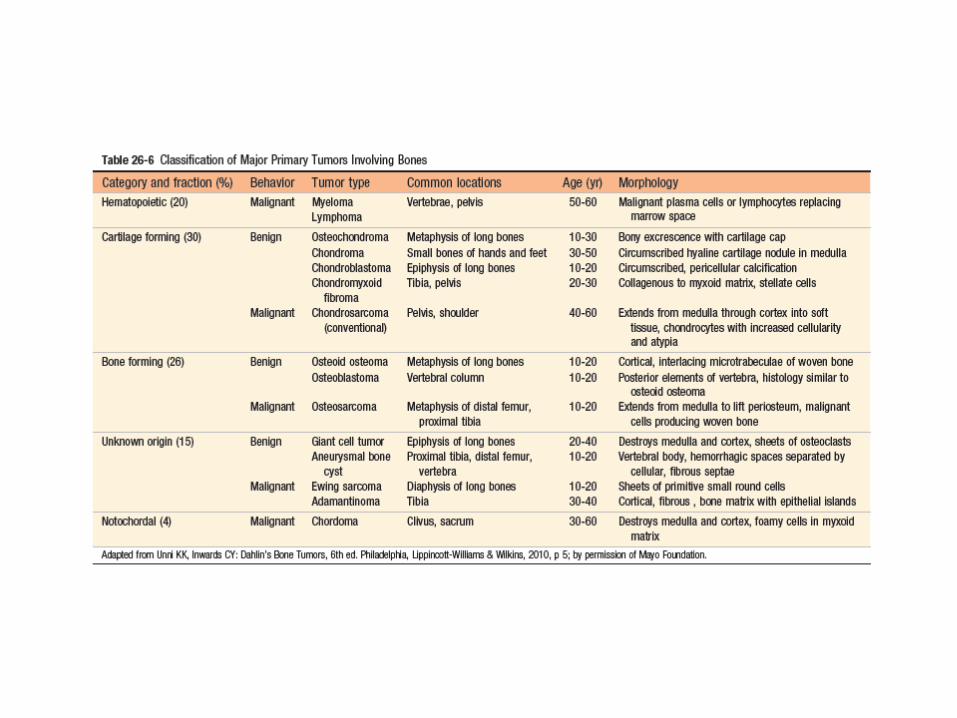
• When possible, bone tumors are classified according to the normal cell or matrix they produce. Lesions that do not have normal tissue counterparts are grouped according to their clinicopathologic features .
• Benign tumors greatly outnumber their malignant counterparts and occur with greatest frequency within the first three decades of life, whereas in older adults, a bone tumor is likely to be malignant.
• Excluding neoplasms originating from hematopoietic cells (myeloma, lymphoma, and leukemia), osteosarcoma is the most common primary cancer of bone, followed by chondrosarcoma and Ewing sarcoma.
• Insults that induce chronic injury and inflammation, such as bone infarcts, chronic osteomyelitis, Paget disease, radiation, and metal prostheses, increase the risk of bone neoplasia, possibly because proliferation associated with chronic inflammation and repair set the stage for acquisition of oncogenic mutations.
Osteosarcoma
• Osteosarcoma is a malignant tumor in which the cancerous cells produce osteoid matrix or mineralized bone.
• It is the most common primary malignant tumor of bone, exclusive of myeloma and lymphoma.
• Osteosarcomas typically present as painful, progressively enlarging masses. Sometimes a sudden fracture of the bone is the first symptom.
• Osteosarcoma occurs in all age groups but has a bimodal age distribution; 75% occur in persons younger than 20 years of age. The smaller second peak occurs in older adults, who frequently suffer from conditions known to predispose to osteosarcoma—Paget disease, bone infarcts, and prior radiation.
• Overall, men are more commonly affected than women (1.6 : 1).
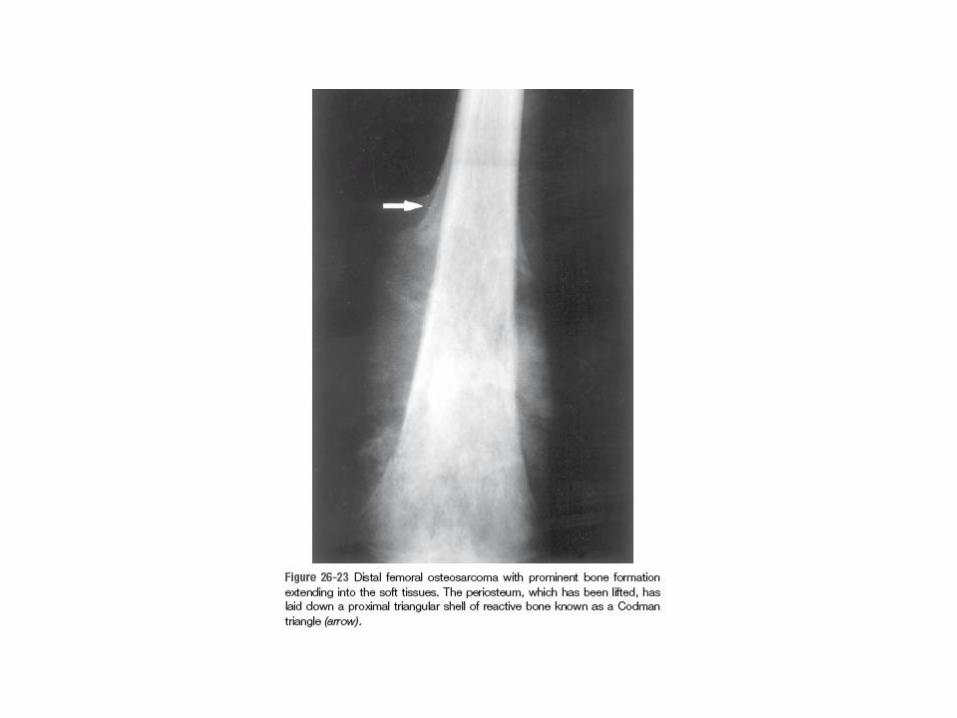
• Any bone can be involved. The tumors usually arise in the metaphyseal region of the long bones of the extremities, and almost 50% occur about the knee (i.e., distal femur or proximal tibia).
• Pathogenesis: Approximately 70% of osteosarcomas have acquired genetic abnormalities such as complex structural and numerical chromosomal aberrations. Molecular studies have shown that these tumors usually have mutations in well-known tumor suppressors and oncogenes, including the following: - RB - TP53 - INK4a - MDM2 and CDK4
• Several subtypes of osteosarcoma are recognized and are grouped according to:
- Site of origin (intramedullary, intracortical, or surface) - Histologic grade (low, high) - Primary (underlying bone is unremarkable) or secondary to preexisting disorders (benign tumors, Paget disease, bone infarcts, previous radiation) - Histologic features (osteoblastic, chondroblastic, fibroblastic, telangiectatic, small cell, and giant cell).
• Clinical Course: Osteosarcoma is treated with a multimodality approach that includes neoadjuvant chemotherapy, which is given under the assumption that all patients have occult metastases at the time of diagnosis, followed by surgery. The prognosis of osteosarcoma has improved substantially since the advent of chemotherapy, with 5-year survival rates reaching 60% to 70% in patients without overt metastases at initial diagnosis. These aggressive neoplasms spread hematogenously to the lungs. Unfortunately, the outcome for patients with metastases, recurrent disease or secondary osteosarcoma is still poor (<20% 5-year survival rate).
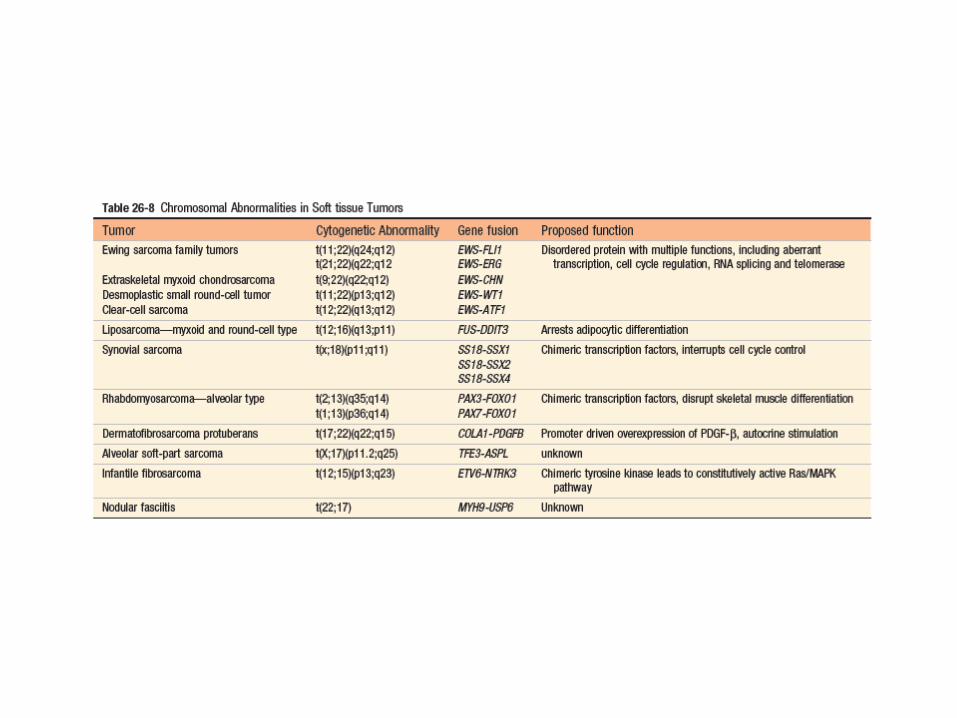
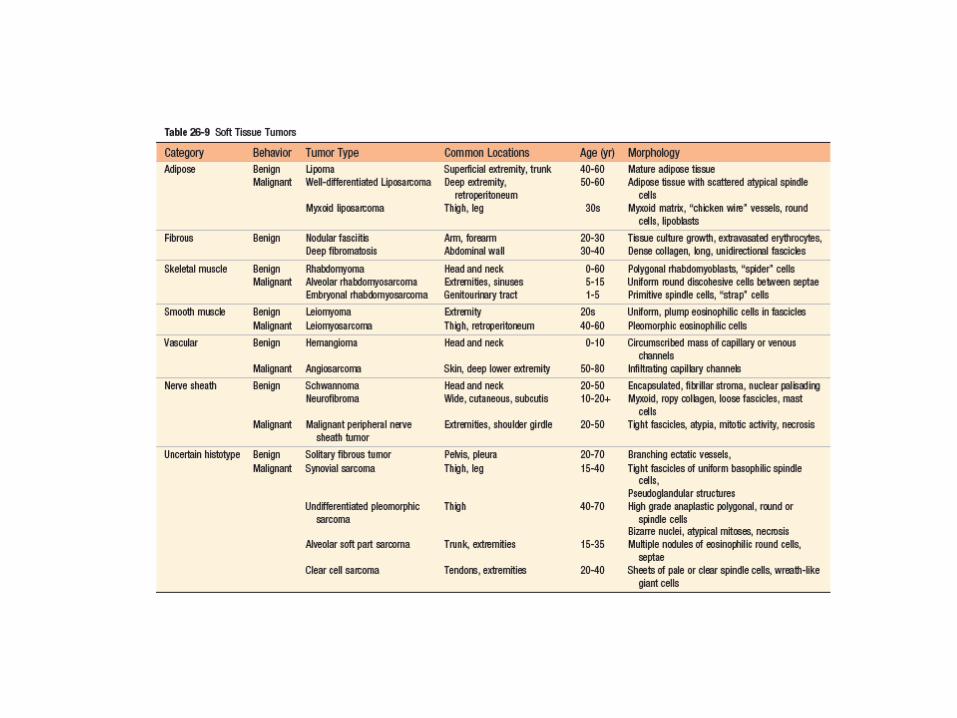
Soft tissue tumors
• soft tissue refers to non-epithelial tissue excluding the skeleton, joints, central nervous system, hematopoietic and lymphoid tissues.
• With the exception of skeletal muscle neoplasms, benign soft tissue tumors outnumber their malignant counterparts (sarcomas), by 100 fold.
• Most soft tissue tumors arise in the extremities, especially the thigh.
• Pathogenesis:
The majority of sarcomas are sporadic and have no known predisposing cause. A small minority of soft tissue neoplasms are associated with germline mutations in tumor suppressor genes (neurofibromatosis 1, Gardner syndrome, Li-Fraumeni syndrome, Osler-Weber Rendu syndrome). A few tumors can be linked to known environmental exposures such as radiation, burns or toxins.
• Although all soft tissue tumors probably arise from pluripotent mesenchymal stem cells, rather than mature cells, tumors can be classified into:
- Tumors that recapitulate a mature mesenchymal tissue (e.g., skeletal muscle) can be further subdivided into benign and malignant forms.
- Tumors composed of cells for which there is no normal counterpart (e.g., synovial sarcoma, undifferentiated pleomorphic sarcoma).
• Clinically, soft tissue tumors range from benign, selflimited lesions that require minimal treatment to intermediate grade, locally aggressive tumors with minimal metastatic risk to highly significant metastatic risk and mortality. aggressive malignancies with
• Pathologic classification integrates morphology (e.g., muscle differentiation), immunohistochemistry and molecular diagnostics.
Skin tumors
• Epidermal Tumors
• Tumors of the Dermis
• Adnexal (Appendage) Tumors
Melanoma
• Melanoma is the most deadly of all skin cancers and is strongly linked to acquired mutations caused by exposure to UV radiation in sunlight.
• Melanoma is a relatively common neoplasm that can be cured if it is detected and treated when it is in its earliest stages. Today, as a result of increased public awareness of the signs of cutaneous melanoma, most are cured surgically.
• The great preponderance of melanoma arises in the skin; other sites of origin include the oral and anogenital mucosal surfaces (i.e., oropharynx, gastrointestinal and genitourinary tracts), esophagus, meninges, and the uvea of the eye.
• Pathogenesis: - The overwhelming majority of melanoma is sporadic and is related to a single predisposing environmental factor: ultraviolet radiation (UVR) damage from sun exposure. UVR is associated strongly with DNA damage. - Melanomas most commonly arise on sun-exposed surfaces, particularly the upper back in men and the back and legs in women. - lightly pigmented individuals are at higher risk than are darkly pigmented individuals (diminishing melanin production in skin thus presumably increasing the amount of damage that sun-exposure wreaks on melanocytes ). - About 10% to 15% of melanomas are inherited as an autosomal dominant trait
Since melanomas sometimes occur in dark-skinned individuals and at body sites that are not sun-exposed, sunlight is not always an essential predisposing factor, and other environmental factors may also contribute to risk. The more common mutations in melanoma are: CDKN2A ----- p16/INK4a BRAF NRAS
• Unlike benign nevi, melanomas show striking variations in color, appearing in shades of black, brown, red, dark blue, and gray. On occasion, zones of white or flesh-colored hypopigmentation also appear, sometimes due to focal regression of the tumor. The borders of melanomas are irregular and often notched, unlike the smooth, round, and uniform borders of melanocytic nevi.
• Clinical Features: The most important warning signs, sometimes called the ABCDEs of melanoma, are: (1) Asymmetry (2) irregular borders (3) Variegated color (4) increasing diameter (5) evolution or change over time, especially if rapid. - Melanoma of the skin is usually asymptomatic, although itching or pain may be early manifestations. - The majority of lesions are greater than 10 mm in diameter at diagnosis. - The most consistent clinical signs are changes in the color, size, or shape of a pigmented lesion. Other features of pigmented lesions that should raise concern are a diameter greater than 6 mm, any change in appearance, and new onset of itching or pain.
Squamous Cell Carcinoma
• Squamous cell carcinoma is the second most common tumor arising on sun-exposed sites in older people, exceeded only by basal cell carcinoma.
• Invasive squamous cell carcinomas are usually discovered while they are small and resectable.
• Less than 5% of these tumors metastasize to regional nodes; these lesions are generally deeply invasive and involve the subcutis.
• Pathogenesis: - The most important cause of cutaneous squamous cell carcinoma is DNA damage
induced by exposure to UV light.----------- TP53 mutations - A second common association is with immunosuppression, most notably chronic
immunosuppression as a result of chemotherapy or organ transplantation. Immunosuppression may contribute to carcinogenesis by reducing host surveillance and increasing the susceptibility of keratinocytes to infection and transformation by oncogenic viruses, particularly human papilloma virus (HPV).
- Other risk factors for squamous cell carcinoma include: disorders of DNA repair, such as xeroderma pigmentosum. industrial carcinogens (tars and oils), chronic ulcers and draining osteomyelitis, old burn scars, ingestion of arsenicals, Ionizing radiation, and (in the oral cavity) tobacco and betel nut chewing.
Basal Cell Carcinoma
• Basal cell carcinoma is the most common invasive cancer in humans.
• These are slow-growing tumors that rarely metastasize. The vast majority is recognized at an early stage and is cured by local excision. However, a small number of tumors (<0.5%) are locally aggressive and potentially disfiguring.
• They occur at sun-exposed sites in lightly pigmented elderly adults.
• As with squamous cell carcinoma, the incidence of basal cell carcinoma is increased in the setting of immunosuppression and in disorders of DNA repair, such as xeroderma pigmentosum.
• Pathogenesis:
Most basal cell carcinomas have mutations that lead to unbridled Hedgehog signaling---- Loss of function of PTCH mutations
• Basal cell carcinomas usually present as pearly papules containing prominent dilated subepidermal blood vessels (telangiectasias).
• Advanced lesions may ulcerate, and extensive local invasion of bone or facial sinuses may occur after many years of neglect or in unusually aggressive tumors, explaining the archaic designation rodent ulcers.


















