Bone marrow pathology · • Bone marrow manifestations of infections and systemic diseases...
44
Bone marrow pathology October 2013 BHS Educational Course
Transcript of Bone marrow pathology · • Bone marrow manifestations of infections and systemic diseases...

Bone marrow pathology
October 2013
BHS Educational Course
• Technical aspects
• Interpretation of BMB

Introduction: technical aspects of
histology
• Identification of a disease process or a
diagnosis
• By tissue analysis
• Tissue preparation to allow
microscopic evaluation
• Knowledge of normal histology and
disease processes

BM biopsy: tissue preparation
• Fixation: buffered formalin, B5 fixative, (Bouin)
• Decalcification:
acid decalcifiers: formic acid (1-2 days),
rapid decalcifier (1 hour)
chelating decalcifiers: EDTA (2-4 days)
electrolysis: Sakura TDETM 30 decalcifier
system (1h ½)
ultrasonic decalcification in EDTA: (2 hours)
• Embedding: paraffin, (“plastic” methylmetacrylate)
New!

Fixation for at least
6 hours
Decalcification
90 min
Overnight automated
processing
Embedding in paraffin cold plate

H&E immunohistochemistry
microtome
Hot plate

tissue
AG
PRIMARY MOUSE ANTISERUM
chromogen

BMB
• Indications: diagnosis, staging, response to treatment & follow-up
• Intrinsic BM diseases MDS/AML
MPD
MDS/MPD
Plasma cell proliferations
Lymphomas
Mast cell proliferation
…
• Infections (opportunistic infections in eg. HIV)
• Vitamin deficiencies
• Metastatic disease
• …

The pathological report
• Representativity: length + composition of BMB
• Cellularity: estimation of % cells versus fat cells
cave hypoplastic AML /MDS
• Hematopoietic cell types
architecture / distribution
maturation
dysplastic features
• Other relevant information
lymfoid infiltrates
stroma , blood vessels, .. (eg amyloid)
presence of granulomas
fibrosis

Histologic Interpretation of BMB: morphology
Pattern recognition: morphological important
clues
- Cellularity
- Focal lesions
- Fibrosis
- Dysplasia
- Disease specific clues
Age and bone marrow cellularity
Mean and 95% range in 177 cases of sudden death
Anterior Iliac crest specimens decalcified and paraffin-embedded
Hartsock et al. Am J Clin Pathol 1965; 43: 326-31

Quantification of bone marrow fibrosis
0 No reticulin fibres demonstrable
1 Occasional fine individual fibres and foci of a fine fibre network
2 Fine fibre network throughout most of the section; no coarse fibres
3 Diffuse fibre network with scattered thick coarse fibres but no mature collagen
4 Diffuse often coarse fibre network with areas of collagenization
Diagnostic clues
• Predominant cell type
• Necrosis
• Gelatinous transformation
• Granulomas
• Lymphoid infiltrates
• Blast count (CD34 , CD117, …)
• …

Histologic Interpretation of BMB:
immunohistochemistry
• Hematological marker: LCA
• “Myeloid markers”: MPO, CD15, CD34, CD68,
CD117
• “Lymphocytic markers”: CD3, CD5, CD20,
CD10, CD21, CD23, CD30,CD138, kappa, lambda …
• Erythroid marker: GlycophorinA
• “Megakaryocytic marker”: FVIII, LAT1,
CD61

« the hypercellular marrow »
• Correlation with age
• Predominant cell type
lymfoid lymphoma
plasma cell myeloma
myeloid
MKC
erythroid cells
blasts
panmyelosis: 3 series
….
• Neoplastic vs reactive
dysplasia
N°cells
presence of disease related features: clustering, fibrosis,
….

« the hypocellular marrow »
• Correlation with age
• Presence of dysplastic features?
hypoplastic MDS
• Increase of blasts? hypoplastic AML
• Hypoplasia / aplasia: reactive
lymphocytes and plasma cells

Pattern recognition
• The hypercellular marrow
myeloid: MDS – AML – MDS/MPD
MPD: CML- PRV
leukemoid reaction
lymphoid: reactive infiltrates, lymphoma
plasmacells: MM
mastcells: mastocytosis
• The hypocellular marrow
aplasia – MDS – AML
• The fibrotic marrow (reticulin / collagen)
MPD (IMF) – AML(M7) - MDS/MPD- mastocytosis – lymphoma – metastatic carcinoma- auto-immune MF – HIV myelopathy-…

Pattern recognition
• The necrotic marrow
ALL – neuroblastoma- DIC/antiphospholipiden syndr – medication
or chemoR/ effect - sickle cell anemia- GvHD- severe infections-
…
• The “dysplastic” marrow
MDS – HIV – vit deficiencies – BM regeneration – chronic
alcoholism – heavy metals – infections – auto-immunity –
paraneoplastic
• The granulomatous marrow
infections (viral-fungal-bacterial-toxo), Hodgkin and non-Hodgkin
lymphomas, CML, AML, ALL, MDS, carcinomas, drugs, auto-
immune disorders, foreign bodies, .

Dysplasia/ dysmyelopoiesis
Dysgranulopoiesis: INCOMPLETE MATURATION / LACK IN GRANULOCYTES (LEFT SHIFT)
PRESENCE OF “IMMATURE CELLS” AWAY FROM THE BONEY TRABECULAE
ABNORMALLY LOCATED IMMATURE PRECURSORS (ALIP)
Dyserythropoiesis: ABSENCE OF MATURATION WITHIN THE ERYTHRON (SYNCHRONISATION)
PREDOMINANTLY LATE STAGE MATURATION CELLS
MITOTIC FIGURES
MEGALOBLASTOID FEATURES (MAINLY IN RARS)
Dysmegakaryopoiesis: SMALL MEGAKARYOCYTES
HYPO OR HYPERLOBULATION OF THE NUCLEUS
MONOLOBULAR MEGAKARYOCYTES OF ALL SIZES
NO CLUSTERING OF MEGAKARYOCYTES
NON-LOBULATED NUCLEI RING NUCLEI
MULTIPLE NUCLEI
NAKED NUCLEI

Left shifted granulopoiesis

MEGALOBLASTOID RED SERIES

DYSMEGAKARYPOIESIS

ABNORMALLY LOCATED IMMATURE PRECURSORS OR ALIP
VERY SMALL, ROUND TO OVAL CELLS OCCURRING AS
SINGLE CELLS OR IN SMALL CLUSTERS AWAY FROM
THE BONEY TRABECULAE
HAVING ALMOST NO CYTOPLASM
THIN BUT WELL DEMARCATED NUCLEAR MEMBRANE
FINE NUCLEAR CHROMATINE AND SMALL BUT INCONSPICUOUS
NUCLEOLUS
TO BE COMPARED WITH MYELOBLASTS RESIDING
ALONG BONE TRABECULAE
MOSTLY CD34 POSITIVE
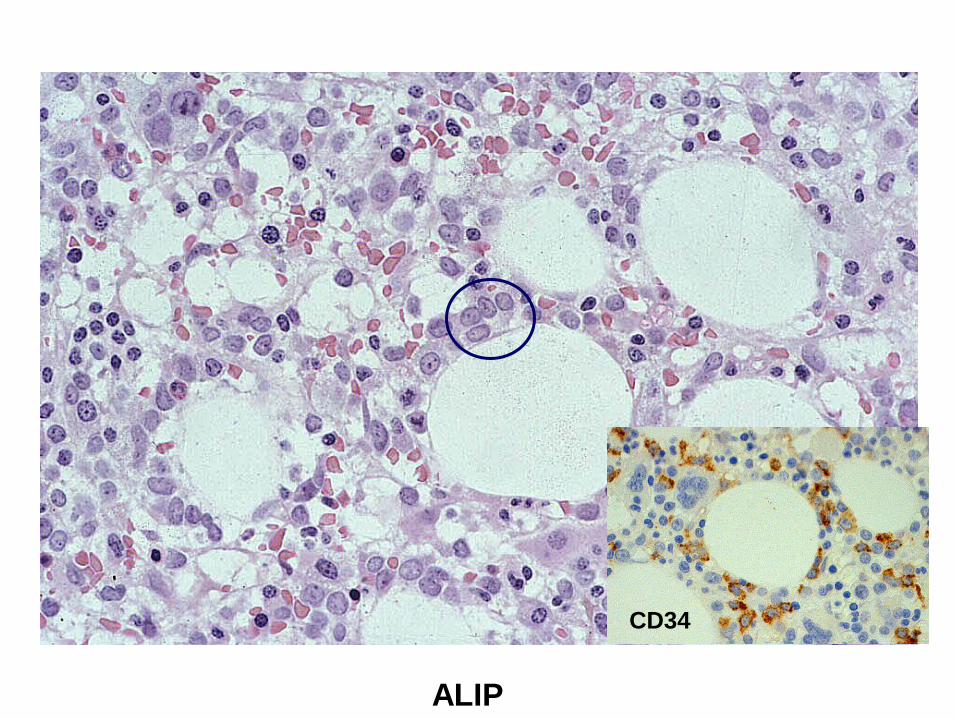
ALIP
CD34
Myeloproliferative features
• High cellularity (100% in CML)
• Fibrosis (in IMF)
• Clustering of MKC (PV, ET, IMF)
• Small MKC in CML
• Very large MKC (PV, ET, IMF)

Identification of blasts
• « round » immature cells
• Dd blasts versus precursors
• CD34
• (CD117)
• Other markers: CD68, MPO

Staging • Carcinomas

Staging & Follow-up
• Lymphomas: Hodgkin & non-Hodgkin
lymphomas

What does the clinician
expect from the pathologist?
• 1) is the BM infiltrated by lymphoma?
• 2) what is the (sub)type of lymphoma?
• 3) additional information on
hematopoiesis, stromal alterations,
therapy-effect, …
Bone marrow involvement by lymphoma
• Often focal involvement
• Ideally bilateral iliac crest BM biopsy
• Ideally step sections of BM biopsy
• Sometimes extensive fibrosis
• Some lymphomas can easily be missed by
cytology and flow, due to the low number of
neoplastic cells (e.g. Hodgkin, THRBCL)

Advantages of bone marrow biopsy:
• overall assessment of neoplastic infiltration: Pattern of involvement - extent of involvement - morphology/cytology of neoplastic cells
May give diagnostic or prognostic clues
• Overall assessment of hematopoiesis and stromal component: bone marrow fibrosis, necrosis, T-cell infiltration after treatment for FL with Rituximab, mast cells in LPL, erythrocyte extravasation in HCL,…
• Immunohistochemistry
“a reliable identification of the subtype of lymphoma can be made in
a significant number of cases”

Disadvantages of BM biopsy
• IHC: some antibodies (e.g. CD103,
CD25) do not work on paraffin
embedded material
• Kappa/lambda: difficult to detect
clonality in B-cells, easy for plasma
cells
Pattern of involvement by
lymphoma:
• Focal non-trabecular
• Focal trabecular
• Diffuse interstitial
• Diffuse solid
• Intrasinusoidal/intravascular

Bone marrow involvement by B-cell lymphoma
NHL type Incidence Pattern
B-ALL/LBL 40-60% Patchy, interstitial
CLL/ SLL 45-75% Nodular, non-paratrabecular
LPL 75-90% Vaguely nodular, non-paratrabecular
MCL 50-80% Nodular, para + non-paratrabecular
FL 40-70% paratrabecular
Splenic MZL ~100% Nodular, non-paratrabecular and
intrasinusoidal (usually focal and in
combination with other infiltration
patterns)
DLBCL 8-35% Nodular, diffuse
THRBCL 0-62% Nodular, diffuse
Intravascular BCL 10-20% intrasinusoidal
Burkitt 20-35% Interstitial (diffuse)
Hairy cell leukemia ~100% Interstitial diffuse

Large paratrabecular
infiltrate
Diagnostic bone marrow biopsy: Reticulin stain
CD20 CD10
Diagnosis: follicular lymphoma

Diffuse interstitial infiltration pattern
“hairy” cells: pale cytoplasm
Reticulin fibrosis, extravasated rbc
Associated hematopoietic alterations
-Hyperplastic (megaloblastoid) RCS
-Dysplastic MKC
-Hypoplastic myelopoiesis
Hairy cell leukemia
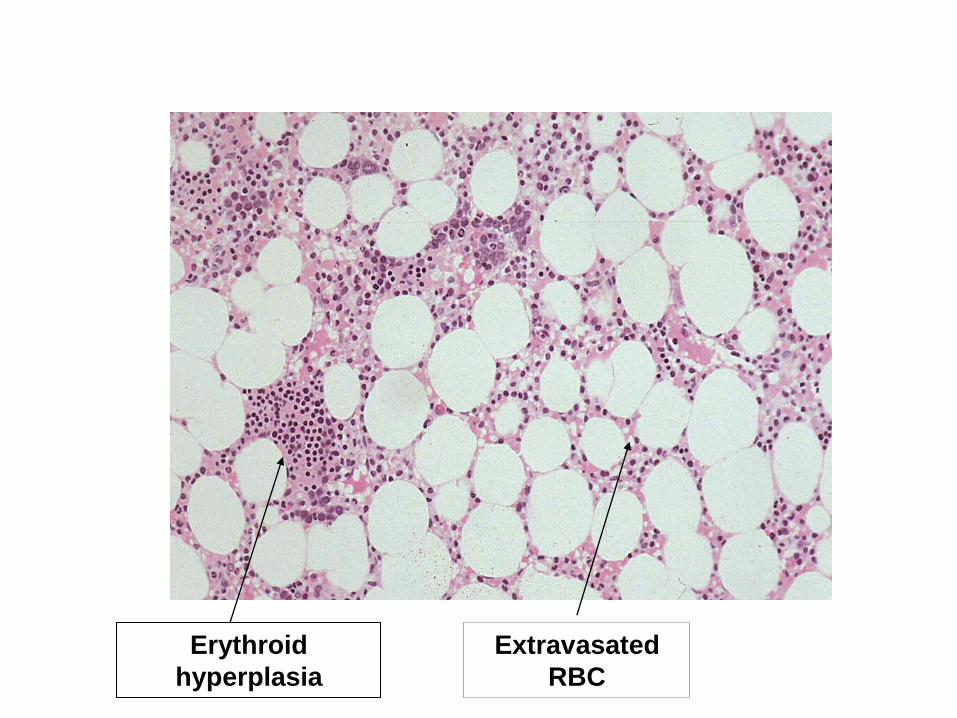
Erythroid
hyperplasia
Extravasated
RBC

Interstitial hairy cells
CD20

Diagnostic bone marrow biopsy CD20
CD20 Diagnosis: DLBCL

Diagnostic bone marrow biopsy CD15
CD30 Diagnosis: classical HL
Pitfalls
• Hematogones vs ALL/BL
• Reactive vs neoplastic infiltrates
• Therapy effect: post-Rituximab T-cell
infiltrates
Cytologic/Morphologic assessment
• Discordant morphology: most often DLBCL
in LN , small B-cell infiltration in BM
• Transformation: Richter transformation in
CLL, transformation to DLBCL
• Morphological variant: MCL, blastoid
variant

Fibrosis in
lymphoproliferative diseases • “Any lymphoproliferation – from benign lymphocytic
aggregates to replacement of the BM in CLL- is accompanied by varying degrees of increase in reticulin fibers, particularly within nodules, when present.”
Current Diagnostic pathology 1997:4:36-44
Most frequently:
• Hairy cell leukemia
• Multiple myeloma
• Classical Hodgkin’s lymphoma
• DLBCL
• THRBCL
Cave: underestimation of BM infiltration on aspirate and flow or even discordant results with bone marrow biopsy

In conclusion: bone marrow examination
• Indication: diagnosis, staging, response to
treatment & follow-up
• Material: BM aspiration smears, core biopsy (min
length 2cm) , touch imprints, clot sections and PB
smears
• Methods: cytology, histology,
immunohistochemistry, flow cytometry,
karyotyping, (F)ISH, PCR
Ideally: combined approach
“BM involvement in NHL: increased diagnostic sensitivity by combination of
immunocytology, cytomorphology and trephine histology” Br J Haematol
1992
References • Guidelines for subtyping small B-cell lymphomas in bone marrow
biopsies. Henrique, Achten, Maes et al. Virchows Arch, 1999, 435:
549-558
• Bone marrow manifestations of infections and systemic diseases
observed in the bone marrow trephine biopsy. Diebold, Molina,
Camilleri-Broët et al. Histopathology 2000, 37: 199-211
• The bone marrow trephine biopsy: a review of normal histology.
Brown, Gatter. Histopathology 1993,22:411-422
• Hodgkin and non-Hodgkin lymphoma involving bone marrow.
Viswanatha, Foucar. Seminars in diagnostic pathology, 2003,20: 196-
210