Bone grafts and substitutes
55
S.K IMRAN ALI PG IN MS ORTHOPAEDICS GANDHI MEDICAL COLLEGE
-
Upload
imran-ali -
Category
Health & Medicine
-
view
138 -
download
2
Transcript of Bone grafts and substitutes
S.K IMRAN ALI
PG IN MS ORTHOPAEDICS
GANDHI MEDICAL COLLEGE
Bone grafts are bone that is transplanted from one area of the skeleton to another to aid in healing, strengthening or improving function.
Bone or bone-like materials used in bone grafts may come from same person, from a donor or from a man-made source.

Bone grafting is used to repair bone fractures that are extremely complex,pose a significant risk to the patient,fail to heal properly.
Bone grafting is also used to help fusion between vertebrae, correct deformities, provide structural support for fractures of the spine.
In addition to fracture repair ,bone grafting is used to repair defects in bone caused by
congenital disorders traumatic injury or surgery for bone cancer
Types 0f Bone graftBased on source:
Autograft ,Isograft ,Allograft, Xenograft
Based on contents: Cortical, Cortico-cancellousCancellous
Based on Vascularity: vascular, Non-Vascular
Based on method of preservation: fresh, frozen, freeze dried, demineralized
Synthetic grafts or Substitutes
Orthopic transfer: host site is of same tissue as that from which graft was donated
Heterotopic transfer: here bone is transferred to a new environment (e.g bone placed in a bed of soft tissue)
Types of Bone Graft Substitutes
Allograft bone used alone or in combination with other materials
Eg; Allogro , Dynagraft Grafton
Mesenchymal stem cells (marrow)
TGF-β, BMP-7-(OP)-1 , FGF
BMP-2—Infuse
PDGF + TGF-β + autograft
Osteograf , Norian STS, ProOsteon , Osteostet
Cortoss, OPLA, Immix,
Allograft-based
Cell-based
Factor-based
Ceramic-based
Polymer-based
Four types of bone cells are located within and around bone matrix.
Osteoblasts, which produce the bone matrix Osteocytes, mature osteoblasts that maintain the bone Osteoclasts, which break down and remove bone tissue.
Bone lining cells, which cover bone surfaces.
Together, these four types of cells are responsible for building the bone matrix, maintaining it, and remodeling the bone as needed.
There are three ways that a bone graft can help repair a defect.
Osteogenesis, the formation of new bone by the cells contained within the graft.
Osteoinduction, a chemical process in which molecules contained within the graft (bone morphogenetic proteins,) convert the patient's cells into cells capable of forming bone.
Osteoconduction, a physical effect whereby the graft matrix configures a scaffold on which cells in the recipient form new bone.


Types of Bone Grafts Autograft
Allograft
Bone graft substitutes
Most have osteoconductive properties
Osteoinductive agents
rhBMP-2 (Infuse) and rhBMP-7 (OP-1)

Autografts“Gold standard”
Standard by which other materials are judged
May provide osteoconduction, osteoinduction and osteogenesis
Drawbacks
Limited supply
Donor site morbidity
Autografts types Cancellous
Cortical
Free vascular transfers
Bone marrow aspirate
Cancellous Bone Grafts
Three dimensional scaffold (osteoconductive)
Osteocytes and stem cells (osteogenic)
A small quantity of growth factors (osteoinductive)
Little initial structural support
Can gain support quickly as bone is formed

Cortical Bone Grafts
Less biologically active than cancellous bone
Less porous, less surface area, less cellular matrix
Prolonged time to revascularizarion
Provides more structural support
Can be used to span defects
Vascularized cortical grafts
Better structural support due to earlier incorporation
Also osteogenic, osteoinductive.
Bone Marrow Aspirate Osteogenic
Mesenchymal stem cells (osteoprogenitor cells) exist in a 1:50,000 ratio to nucleated cells in marrow aspirate
Numbers decrease with advancing age
Can be used in combination with an osteoconductive matrix
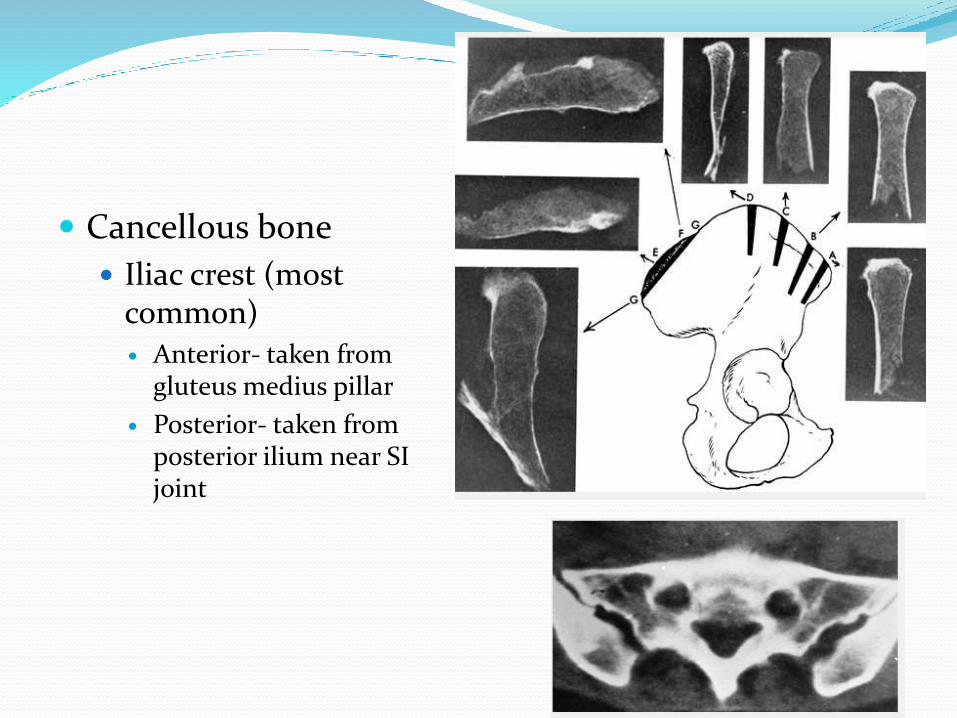
Cancellous bone
Iliac crest (most common) Anterior- taken from
gluteus medius pillar
Posterior- taken from posterior ilium near SI joint
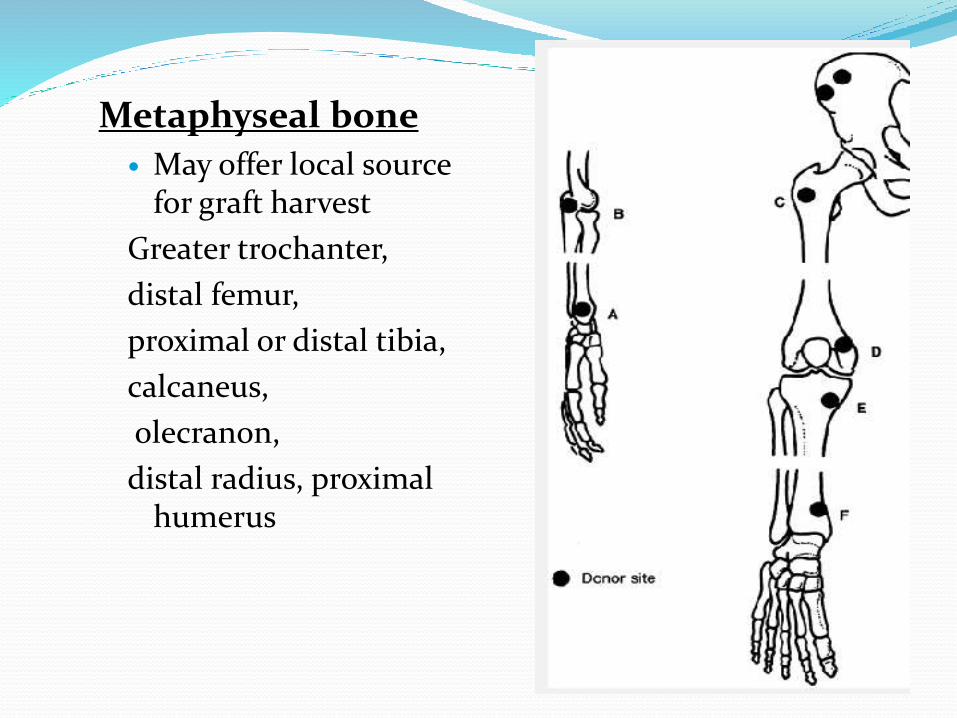
Metaphyseal bone
May offer local source for graft harvest
Greater trochanter,
distal femur,
proximal or distal tibia,
calcaneus,
olecranon,
distal radius, proximal humerus
Autograft HarvestCancellous harvest technique
Cortical window made with osteotomes
Cancellous bone harvested with gouge or currette
Can be done with trephine instrument
Circular drills for dowel harvest
Commercially available trephines or “harvesters”
Can be a percutaneus procedure
Autograft Harvest Cortical
Fibula common donor
Avoid distal fibula to protect ankle function
Preserve head to keep LCL, hamstrings intact
Iliac crest
Cortical or tricortical pieces can be harvested in shape to fill defect

Bone Allografts Cancellous or cortical
Plentiful supply
Limited infection risk (varies based on processing method)
Provide osteoconductive scaffold
May provide structural support
Available in various forms
Processing methods may vary between companies / agencies

Bone Allografts Fresh
Highly antigenic
Limited time to test for immunogenicity or diseases
Use limited to joint replacement using shape matched osteochondral allografts
Highest risk of disease transmission and immunogenicity ,BMP preserved and therefore osteoinductive
Bone Allografts Fresh frozen
Less antigenic
Time to test for diseases
Strictly regulated by FDA
Preserves biomechanical properties
Good for structural grafts
Less immunogenicity than fresh
BMP preserved and therefore osteoinductive

Bone AllograftsFreeze-dried
Even less antigenic
Time to test for diseases
Strictly regulated by FDA
Can be stored at room temperature up to 5 years
Mechanical properties degrade
Least structural integrity
BMP depleted (purely osteoconductive)
Lowest likelihood of viral transmission

Graft Incorporation Hematoma formation
Release of cytokines and growth factors

Graft Incorporation Hematoma formation
Release of cytokines and growth factors
Inflammation
Development of fibrovascular tissue

Graft Incorporation Hematoma formation
Release of cytokines and growth factors
Inflammation
Development of fibrovascular tissue
Vascular ingrowth
Often extending Haversian canals
Graft Incorporation Hematoma formation
Release of cytokines and growth factors
Inflammation
Development of fibrovascular tissue
Vascular ingrowth
Often extending Haversian canals
Focal osteoclastic resorption of graft
Graft Incorporation Hematoma formation
Release of cytokines and growth factors
Inflammation
Development of fibrovascular tissue
Vascular ingrowth
Often extending Haversian canals
Focal osteoclastic resorption of graft
Intramembranous and/or endochondral bone formation on graft surfaces
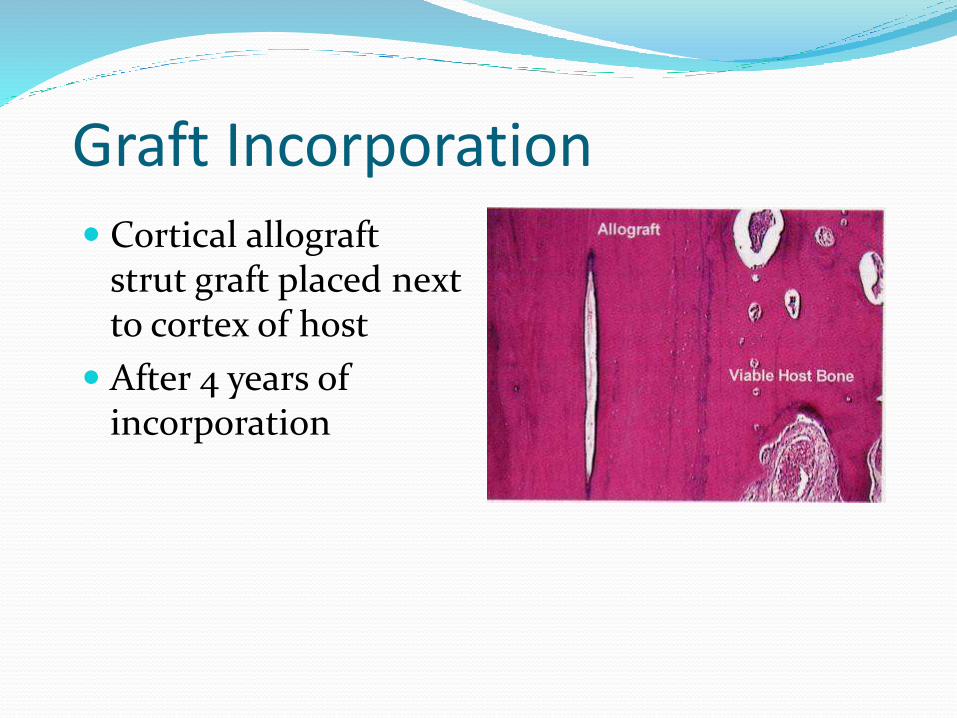
Graft Incorporation Cortical allograft
strut graft placed next to cortex of host
After 4 years of incorporation
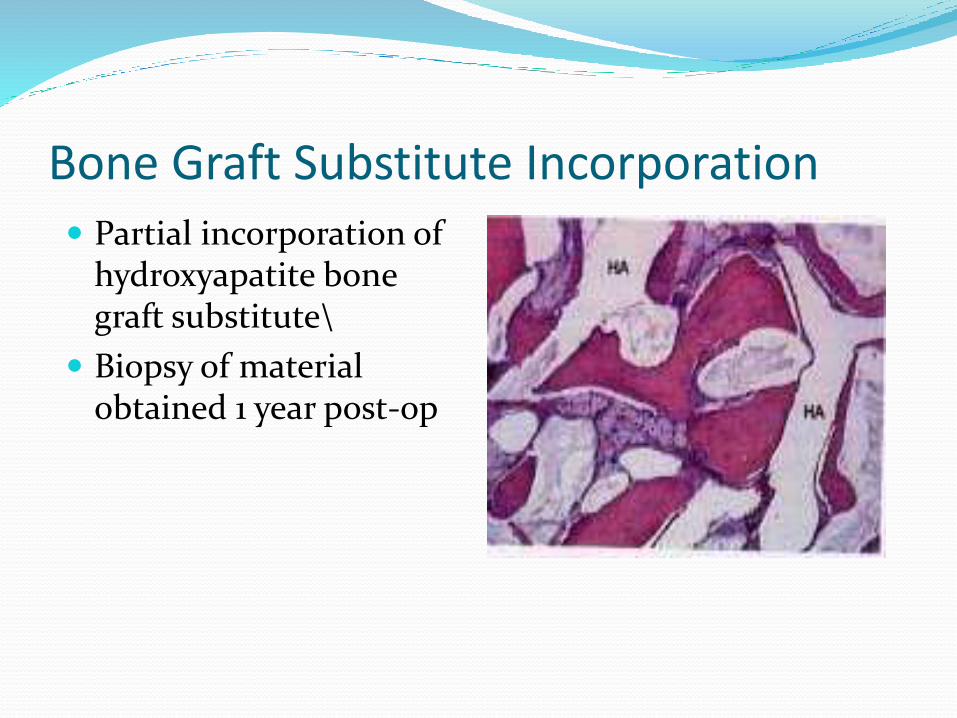
Partial incorporation of hydroxyapatite bone graft substitute\
Biopsy of material obtained 1 year post-op
Bone Graft Substitute Incorporation

WHY ARE WE INTERESTED IN BONE GRAFT ALTERNATIVES
BONE GRAFT MORBIDITY- 9%1. PROLONGED WOUND DRAINAGE2. HEMATOMAS 3. INFECTIONS4. NERVE INJURY5. PROLONGED PAINLARGER THE AMOUNT OF GRAFT MORE ARE THE LIKELIHOOD OF COMPLICATIONSAUTOLOGUS BONE GRAFT IS NOT SUFFICIENT IN SOME CASES LIKEBONE CYSTS, BONE DEFECTS, TUMORS ETC….

Bone Graft Substitutes
Need for bone graft alternatives has lead to development of numerous bone graft substitutes
Avoid morbidity of autogenous bone graft harvest
Mechanical properties vary
Most offer osteoconductive properties
Some provide osteoinductive properties
Ideal bone graft substitute Should be
biocompatible,
bioresorbable,
osteoconductive,
osteoinductive,
structurally similar to bone,
easy to use
cost-effective.
Currently marketed products are variable in their composition, their mechanism of action and the claims made about them.

Bone Graft SubstitutesPotential Roles
Extender for autogenous bone graft Large defects
Multiple level spinal fusion
Enhancer To improve success of autogenous bone graft
Substitute To replace autogenous bone graft
Bone Graft Substitutes
Calcium phosphate
Calcium sulfate
Collagen based matrices
Demineralized bone matrix
Hydroxyapatite
Tricalcium phosphate
Osteoinductive proteins
Bone Graft Substitutes
Resorption rates vary widely
Dependant on composition
Calcium sulfate - very rapid
Hydroxyapatite (HA) – very, very slow
Some products may be combined to optimize resorptionrate
Also dependant on porosity, geometry
Bone Graft Substitutes Mechanical properties vary widely
Dependant on composition
Calcium phosphate cement has highest compressive strength
Cancellous bone compressive strength is relatively low
Many substitutes have compressive strengths similar to cancellous bone
All designed to be used with internal fixation
Calcium PhosphateInjectable pastes of calcium and phospate
Norian SRS (Synthes/Stratec)
Alpha BSM (Etex/Depuy)
Callos Bone Void Filler (Skeletal Kinetics)

Calcium Phosphate
• Injectable• Very high compressive strength once
hardens• Some studies of its use have allowed
earlier weightbearing and range of motion

Osteoconductive void filler
Low compressive strength – no structural support
Rapidly resorbs
May be used as a autogenous graft extender
- Available from numerous companies
- Osteoset, Calceon 6, Bone Blast, etc.
Calcium Sulfate
Pellets
Pellet injectors
Bead kits
Allows addition of antibiotics
Injectable
May be used to augment screw purchase
Calcium Sulfate
Collagen Based Matrices
Highly purified Type 1 bovine dermal fibrillar collagen
Bone marrow is added to provide bone forming cells
Collagraft (Zimmer) Collagen / HA / Tricalcium
phosphate
Healos (Depuy) Collagen / HA
Demineralized Bone Matrix Prepared from cadaveric human bone
Acid extraction of bone leaving
Collagen
Noncollagenous proteins
Bone growth factors
BMP quantity extremely low and variable
Sterilized which may decrease the availability of BMP

Available from multiple vendors in multiple preparations
Gel
Putty
Strip
Combination products with cancellous bone and other bone graft substitute products
Demineralized Bone Matrix

Growth factor activity varies between tissue banks and between batches
While they may offer some osteoinductive potential because of available growth factors, they mainly act as an osteoconductive agents
Demineralized Bone Matrix
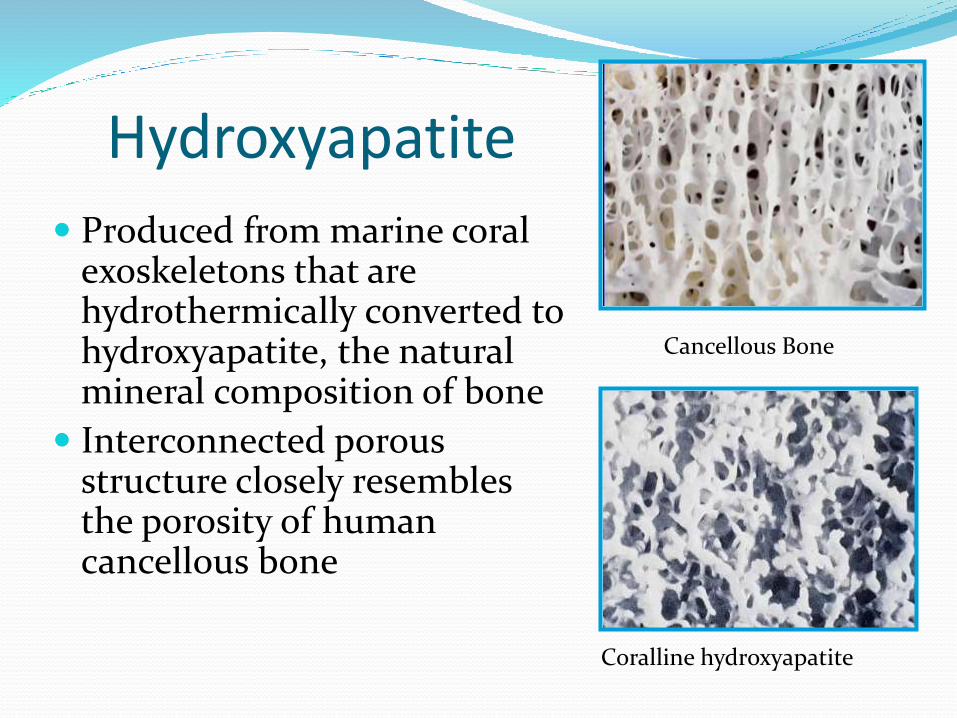
Hydroxyapatite
Produced from marine coral exoskeletons that are hydrothermically converted to hydroxyapatite, the natural mineral composition of bone
Interconnected porous structure closely resembles the porosity of human cancellous bone
Coralline hydroxyapatite
Cancellous Bone

Hydroxyapatite Available in various size blocks & granules
ProOsteon 500
Very slow resorption
ProOsteon 500 R
Only a thin layer of HA
Faster resorption

Tricalcium Phosphate Wet compressive strength slightly less than
cancellous bone
Available as blocks, wedges, and granules
Numerous tradenames Vitoss (Orthovita)
ChronOS (Synthes)
Conduit (DePuy)
Cellplex TCP (Wright Medical)
Various Theri__ names (Therics)
Bone Morphogenetic Proteins
Produced by recombinant technology
Two most extensively studied and commercially available
BMP-2 (Infuse) Medtronics
BMP-7 (OP-1) Stryker Biotech
Demineralized Bone Matrix Acidic extraction of bone matrix from allograft
removes the minerals and leaves the collagenous and noncollagenous structure and proteins
Properties
osteoconductive without structural support
minimally osteoinductive despite preservation of osteoinductive molecules
interproduct and interlot variability is common

Synthetics Silicate based grafts Aluminum oxideAlumina ceramic bonds bind to bone in response to stress and
strain Calcium phosphate grafts - Osteoconduction and osteointegration
- Biodegrade very slowly- Highest compressive strength- Many prepared as ceramics (heated to fuse into crystals)- Examples include: tricalcium phosphate, Norian (Synthes), hydroxyapatitie(tradename Collagraft by Zimmer)
Calcium sulfate- Osteoconductive- Quick resorption- Examples include: OsteoSet (Wright medical)
Coralline hydroxyapatine- Calcium carbonate skeleton is converted to calcium phosphate via a thermoexchange process (Interpore)Calcium carbonate-Chemically unaltered marine coral- Osteoconductive
Bone morphogenetic proteins (BMP) Osteoinductive properties
stimulates undifferentiated perivascular mesenchymalcells to differentiate into osteoblasts through serine-threonine kinase receptors
rhBMP-2 and rhBMP-7 are FDA-approved for application in long bones and spine
Complications
under or overproduction of bone
inflammatory responses
early bone resorption
Reamer Irrigator Aspirator System Indications – To clear the medullary canal of bone
marrow and reaming debris – To clear the medullary canal of
infected bone tissue – To effectively size the medullary canal
for the acceptance of an intramedullaryimplant or prosthesis
To harvest finely morselizedautogenous bone and bonemarrow for any surgical procedures that require bone graft in order to facilitate fusion and/or fill bone defects.
These procedures include spinal fusion, joint arthrodesis, total joint replacement, fracture repair, nonunion, maxillofacial reconstruction, and tumor removal

BONE BANK Deals with procurement, storage & supply of Bone Goals : to preserve integrity of graft
to reduce immunogenicityto ensure sterility
Procedure:Legal status- permission from donor or from next of kinDonor selection: no infection by Hx or physical exam
no deep tissue woundsafebrile hospital coursemax 72 hrs 0f Resp assistanceno prolonged steroid therapy or on long actingisotopesno hx of IV drug abuse
Time interval between death and harvest should be <12hrs for unrefrigerated body & <24hrs for a refregirated one
Procurement Procedure:
Performed in regular OT within12-24 hrs of death.
Ileum , femur, tibia, humerus ,ribs.
Capsules , tendons & ligaments retained.
Pelvis procured at the end to prevent contamination frombowel.
Grafts are placed in cold tissue culture medium(RL) to which100mg/L of Sterptomycin sulfate & 80mg/L of Gentamycinsulfate are added.
After removal of grafts, bodyframe is reconstructed withsticks cut to the length of extremity &fixed by plaster.

Storage :Bones are wrapped in sterile cloth with 2-3 layers of sterile drapes.Cartilagenous ends are soaked in 8%DMSO in RL which acts as
cryoprotectant for the cartilage .Sterilisation : When cadaver grafts have been obtained under aseptic conditions there is
no need to employ sterilisation procedures. They were used in the past and are rarely used now due to deleterious effect on bone.
Diadvantages :Bone becomes discoloured and brittle.Solubility of collagen & GAG is increased.Fibrillar network of bone matrix is destroyed.Reduces bone inductive capacity.Retrieval of bone: bones are thawed just prior to use in RL /NS to which
antibiotics are added.Bones preserved at freezing temparatures require atleast 1hr at room
temparatue before use.