
Competition Between Steric Hindrance and Hydrogen Bonding ...

Bonding Between Metals and Polymers for Dental Devices
Omar Saleh Alageel
Faculty of Dentistry, McGill University
Montreal, Canada
December, 2013
A thesis submitted to McGill University in partial fulfillment of the requirements of the degree
of M.S.c in Dental Sciences.
© Omar Alageel 2013

2
Table of Content
Dedication ...................................................................................................................................... 4
Acknowledgements ........................................................................................................................ 5
List of Figures ................................................................................................................................ 6
List of Tables ................................................................................................................................. 8
Abbreviations ................................................................................................................................. 9
Abstract ........................................................................................................................................ 10
Résumé ......................................................................................................................................... 12
Chapter 1: Introduction ............................................................................................................ 14
Chapter 2: Background and Literature Review ..................................................................... 16
2. Esthetics and Dental Occlusion .................................................................................. 16
2.1. Edentulism ................................................................................................................ 16
2.1.1. Treatment of Edentulous Patients .......................................................................... 17
2.1.1.1. Treatment of Partially Edentulous Patients ......................................................... 18
2.1.1.1.1. Fixed Partial Dentures ...................................................................................... 18
2.1.1.1.2. Dental Implants ................................................................................................ 19
2.1.1.1.3. Removable Partial Dentures ............................................................................ 21
2.1.1.2. Treatment of Completely Edentulous Patients ................................................... 23
2.1.1.2.1. Removable Complete Dentures ....................................................................... 24
2.1.1.2.2. Fixed Complete Dentures ................................................................................ 25
2.2. Malocclusion ............................................................................................................. 26
2.2.1. Treatment of Malocclusion .................................................................................... 26
2.2.1.1. Fixed Appliances ................................................................................................ 27
2.2.1.2. Removable Appliances ....................................................................................... 28
2.3. Materials Used in Dentures and Orthodontic Devices .............................................. 29
2.3.1. Metals ..................................................................................................................... 29
2.3.1.1. Titanium .............................................................................................................. 30
2.3.1.2. Cobalt-Chromium ............................................................................................... 31
2.3.1.3. Stainless Steel ..................................................................................................... 32
2.3.2. Ceramic .................................................................................................................. 32
2.3.3. Polymers and Composites ...................................................................................... 33
2.3.3.1. PMMA ................................................................................................................ 34
2.3.3.2. Bis-GMA ............................................................................................................ 37
2.4. Bonding Systems in Dentures and Orthodontic Appliances ..................................... 39
2.4.1. Mechanical Bonding .............................................................................................. 39
2.4.2. Chemical Bonding ................................................................................................. 40
2.5. Debonding in Dentures and Orthodontics Appliances…........................................... 41
2.5.1. Bonding between Alloys and PMMA .................................................................... 42

3
2.5.2. Bonding between Wrought Wire and PMMA ....................................................... 43
2.5.3. Bonding between Brackets and Composite ........................................................... 45
2.6. Aryldiazonium Salts .................................................................................................. 46
2.6.1. Grafting of Diazonium Salts .................................................................................. 47
2.6.2. Diazonium Grafted Layer Properties ..................................................................... 48
2.6.3. Applications of Aryldiazonium Salts ..................................................................... 49
2.6.4. Aryldiazonium Salts as Dental Adhesive .............................................................. 50
2.6.5. Diazonium Grafted Layer Analysis ....................................................................... 50
2.6.5.1 X-ray Photoelectron Spectrometer (XPS) ............................................................ 51
2.6.5.2 Contact Angle Measurement ................................................................................ 54
Chapter 3: Hypothesis and Objective ...................................................................................... 55
3.1. Hypothesis.................................................................................................................. 55
3.2. Thesis Objective......................................................................................................... 55
Chapter 4: List of References ................................................................................................... 56
Chapter 5: Manuscript I: Bonding Metals to Poly-Methyl Methacrylate Using
Aryldiazonium Salts ...................................................................................................... 62
5.1. Abstract ..................................................................................................................... 62
5.2. Introduction................................................................................................................ 63
5.3. Materials and Methods .............................................................................................. 67
5.4. Results and Discussion.............................................................................................. 71
5.5. Conclusion................................................................................................................. 80
5.6. References.................................................................................................................. 81
Chapter 6: Manuscript II: Surface Chemical Treatment of Orthodontic Brackets for
Improved Tooth Adhesion ............................................................................................ 85
6.1. Abstract ..................................................................................................................... 85
6.2. Introduction................................................................................................................ 86
6.3. Materials and Methods .............................................................................................. 89
6.4. Results........................................................................................................................ 94
6.5. Discussion ................................................................................................................. 97
6.6. Conclusion .............................................................................................................. 101
6.7. References ............................................................................................................... 102
Chapter 7: Conclusion.............................................................................................................. 105
Chapter 8: Appendices ............................................................................................................ 106
8.1. Report of Invention ................................................................................................. 107
8.2. Poster I .................................................................................................................... 108
8.3. Poster II ................................................................................................................... 109
8.4. Poster III .................................................................................................................. 110
8.5. Poster IV & V.......................................................................................................... 111

4
Dedication
I dedicate my thesis to my parents, brothers, and sisters for their endless encouragement
and support throughout the course of this thesis. Also, I dedicate this thesis to my
wonderful and supportive wife and to my beautiful boy.
5
Acknowledgements
First of all I would like to thank Allah Almighty for providing me blessings, help, and courage to
accomplish this thesis and achieve my desired goals.
I would like to express my genuine appreciation to my supervisor Dr. Faleh Tamimi for his
encouragement, supervision, support, and immense knowledge. I am grateful for his generous
guidance from the initial to the final stage of this project. Also, I would thank enormously my
co-supervisor Dr. Marta Cerruti for her suggestions, feedback, and facilities throughout the
completing of my thesis.
In addition, thanks to all my colleagues and friends especially Mohamed-Nur abdalla and Hazem
Eimar for their constant and unconditional help to complete this project. Thanks to Dr. Jean-
Marc Retrouvey, Dr. Rubens Albuquerque and Paige Kozak for their help and guidance.
Finally, I would like to thank King Saud University, Saudi Arabia for the scholarship and the
grant to complete this research.

6
List of Figures
Figure 2.1: Replacing missing teeth using fixed partial denture (Bridge).
Figure 2.2: Dental implant components for the single-unit fixed prosthesis.
Figure 2.3: The mandibular removable partially denture (RPD).
Figure 2.4: Complete partial dentures for maxillary and mandibular arches.
Figure 2.5: The implants-supported complete denture (overdentures).
Figure 2.6: Fixed complete dentures that supported on several dental implants.
Figure 2.7: Fixed appliance for malocclusion treatment.
Figure 2.8: Removable appliance for malocclusion treatment (retainers).
Figure 2.9: Scheme of the polymerization reaction of PMMA.
Figure 2.10: Schematic diagram of the chemical reaction for Bis-GMA.
Figure 2.11: Scheme describing grafting of diazonium salts of a substrate.
Figure 2.12: Diagram describing X-ray photoelectron spectroscopy (XPS) components.
Figure 5.1: The custom-made silicone mold used to prepare the PMMA-Ti specimen; and
mechanical test specimen before and after mechanical testing.
Figure 5.2: Scheme depicting reaction sequence performed in first (primer) and second
(adhesive) steps.
Figure 5.3: XPS surveys; elemental compositions; high resolution C 1s spectra on Ti surface for
different groups.
Figure 5.4: Photographs of water droplets placed on different Ti groups.

7
Figure 5.5: Tensile strength of the bond between PMMA and treated Ti surfaces.
Figure 5.6: Bond strength of PMMA and stainless steel wires for the control group and
that were treated with diazonium.
Figure 5.7: Drawing shows the acrylic removable partial denture with small volume of
PMMA to support the wire.
Figure 6.1: Photographs showing bracket debonding at the interface between brackets and
composite.
Figure 6.2: Digital photographs illustrating the different types of brackets used in this study; and
schematic drawing of preparation and mechanism of testing the tensile and shear bonding
strength between brackets and Bis-GMA.
Figure 6.3: Schematic diagram of the reactions performed in the first and second solutions of
Bis-GMA/diazonium treatment.
Figure 6.4: XPS general surveys and the elemental compositions for the untreated and treated
brackets.
Figure 6.5: The ultimate tensile force N and bond strength MPa of the different stainless steel
brackets. The ultimate shear force N and bond strength MPa of the different stainless steel
brackets.
Figure 6.6: Photograph of untreated L bracket group and treated S bracket group that were
bonded to the anterior teeth using the adhesive based on Bis-GMA; and drawing shows fixed
orthodontic appliances with different size of brackets.

8
List of Tables
Table 2.1: The bond strengths between titanium and PMMA (MPa) by using different bonding
methods.
Table 2.2: The bond strengths (MPa) between PMMA and cobalt –chromium or stainless steel
using different bonding methods.
Table 5.1: The bond strengths between titanium and PMMA (MPa) using different bonding
methods.
Table 5.2: Conditions tested in the second step. The overall solution volume was 12 ml, and was
water-based.

9
Abbreviations
AFM ....................................................................................................... Atomic force microscopy
Bis-GMA ................................................................................ Bisphenol A glycidyl methacrylate
CAD/CAM .........................................Computer Aided Design / Computer Aided Manufacturing
Co-Cr ................................................................................................................. Cobalt-Chromium
CP...................................................................................................................... Commercially Pure
DFT ......................................................................................................... Density functional theory
DMLS................................................................................................. Direct Metal Laser Sintering
HCl ..................................................................................................................... Hydrochloric acid
HNO3 .............................................................................................................................. Nitric acid
H3PO2 ......................................................................................................... Hypophosphorous acid
H2SO4 .......................................................................................................................... Sulfuric acid
HEMA ................................................................................................. Hydroxyethyl methacrylate
MMA .............................................................................................................. Methyl methacrylate
µm ................................................................................................................................. Micrometer
MPa .............................................................................................................................. Megapascal
NaNO2 ..................................................................................................................... Sodium nitrite
N .......................................................................................................................................... Newton
PAP................................................................................................................ Polyaminophenylene
pH ....................................................................................................................................... Acidity
PMMA ................................................................................................... Poly-methyl methacrylate
PPD ................................................................................................................. p-phenylenediamine
RPD ...................................................................................................... Removable partial denture
TEGDMA .................................................................................. Triethyleneglycol-dimethacrylate
Tg ........................................................................................................ Glass transition temperature
Ti ....................................................................................................................................... Titanium
ToF-SIMS .......................................................... Time-of-flight secondary ion mass spectrometry
XPS ............................................................................................ X-ray photoelectron spectroscopy

10
Abstract
Many dental devices combine acrylic (i.e. poly-methyl methacrylate or bisphenol A-glycidyl
methacrylate) and metallic parts (i.e. titanium or stainless steel) that are bonded together. These
devices often present catastrophic mechanical failures due to weak bonding between their acrylic
and metallic components. These devices include dental prostheses, combining metallic
frameworks (i.e. titanium) and wrought wires with acrylic resin; and orthodontic appliances,
combining acrylic resin with stainless steel wrought wires or composite with stainless steel
brackets. The bonding between metals and polymers in dental devices is usually performed by
the mechanical interlocking, but its bond strength is still too low for dental applications. The
bond strength between them would be high if the chemical bonding, which does not occur
spontaneously, uses in addition to the mechanical interlock. The objective of this study was to
develop a new method of creating a strong chemical bond between alloys and polymers for
dental devices based on diazonium chemistry.
The chemical bond between metals (i.e. titanium or stainless steel) and polymers (i.e. poly-
methyl methacrylate, PMMA or Bisphenol A-glycidyl methacrylate, Bis-GMA) was achieved in
two steps. In the first reaction step (primer), the aryldiazonium salts were chemically reduced to
form aryl radicals which spontaneously got grafted onto the metallic surfaces. The second step of
the reaction (adhesive) was optimized to achieve covalent binding between the grafted layer and
PMMA or Bis-GMA. The chemical composition of the treated surfaces was analyzed with X-ray
photoelectron spectroscopy (XPS), and the bonding strengths between alloys and PMMA or Bis-
GMA were measured.

11
XPS characterization and contact angle measurement confirmed the presence of a polymer coat
on the treated metallic surfaces. Whereas, the mechanical test results showed a significant
increase of the tensile bond strength between PMMA and treated titanium or stainless steel wire
by 5.2 and 2.5 folds, respectively, compared to the untreated control group (P<0.05). Moreover,
the bonding strength between metallic brackets and Bis-GMA composite was increased after the
treatment depending on the bracket design by 2 to 3.9 folds compared to untreated brackets.
Diazonium chemistry provides an effective way of achieving a strong chemical bond between
alloys and PMMA or Bis-GMA. The resulting bonding method can be utilized to further improve
the properties of dental devices, reduce debonding of dental prostheses and brackets, provide
more leverage in orthodontic cases with complex mechanics, and allow the use of brackets with
smaller bases.

12
Résumé
De nombreux appareils dentaires sont composés d'acrylique (c'est à dire d'un poly -méthacrylate
de méthyle ou de bisphénol A- glycidyle méthacrylate) et de parties métalliques (par exemple en
titane ou en acier inoxydable) qui sont collés ensemble. Ces dispositifs présentent souvent des
défaillances mécaniques catastrophiques en raison de la faiblesse de la liaison entre les
composantes en acrylique et celles en métal. Ces dispositifs comprennent les prothèses dentaires,
alliant des cadres métalliques (c’est à dire de titane) et fils forgé avec de la résine acrylique, et
les appareils orthodontiques, combinant de la résine acrylique avec des fils forgé en acier
inoxydable ou un composite avec des supports en acier inoxydable. La force de liaison entre eux
serait élevée si la liaison chimique, ce qui ne se produit pas spontanément, est utiliser en plus du
verrouillage mécanique.
Dans la première étape de la réaction, les sels d’aryl diazonium sont réduits chimiquement pour
former des radicaux aryles qui sont spontanément greffés sur les surfaces métalliques La
deuxième étape de la réaction a été optimisée pour réaliser la liaison entre la couche greffée et le
PMMA ou le Bis-GMA. La caractérisation XPS et la mesure de l'angle de contact a confirmé la
présence d'une couche de polymère sur les surfaces métalliques traitées. Les résultats des essais
mécaniques ont montré une augmentation significative de la force d'adhérence à la traction entre
le PMMA et le titane traité ou d'un fil en acier inoxydable de 5,2 et 2,5 plis, respectivement, par
rapport au groupe témoin non traité (p < 0,05).
13
La chimie de diazonium fournit un moyen efficace d'atteindre une liaison chimique forte entre
les alliages et le PMMA ou le Bis-GMA. Le procédé de collage qui en résulte peut être utilisé
pour améliorer les propriétés des appareils dentaires, réduire le décollement de prothèses
dentaires et des supports, et permettre l'utilisation de supports avec des bases plus petites.

14
Chapter 1: Introduction
Dental devices such as dental prostheses and orthodontic appliances are commonly used for
treatment of dental problems such as edentulism and malocclusion [1-6]. Dental prosthesis is an
artificial device used to replace natural teeth for partially or completely edentulous patients.
Dental prostheses such as fixed partial dentures, metal-cast removable partial dentures, and all-
acrylic removable partial dentures are the most common treatment options for partially
edentulous patients while the removable complete dentures are the most common prostheses for
completely edentulous patients [1-5, 7-11]. Furthermore, fixed and removable orthodontic
appliances are the most common treatment methods for malocclusion patients [3, 4].
Dental devices usually are a combination of polymeric (i.e. poly-methyl methacrylate and
bisphenol A-glycidyl methacrylate) and metallic parts (i.e. titanium, cobalt-chromium, and
stainless steel) that are bonded together. The bonding between metals and polymers in dental
devices is usually preformed by mechanical and/or chemical bonds. The metallic framework (i.e.
titanium and cobalt-chromium) in the removable partial dentures (RPD) is usually bonded to
poly-methyl methacrylate (PMMA) by interlocking the PMMA into the irregularities of the
metals that can be prepared by creating small retentions or sandblasting the metals substrates [11,
12]. The metallic wrought wire in the all-acrylic removable partial dentures and removable
orthodontic appliances is usually formed in a zig-zag configuration to provide retention in
PMMA denture base. Orthodontic brackets were developed with a large base designed to
increase the surface area and compensate for the lack of adhesion between brackets and

15
bisphenol A-glycidyl methacrylate (Bis-GMA) composite; however, large brackets have a
negative effect on patient satisfaction and oral health [13-17].
Dental devices often present catastrophic mechanical failures due to lack of bonding between
their acrylic and metallic components leading to prostheses failures and brackets loss [18-21].
The bonding between alloys and polymers in dental devices can be improved using strong
chemical bond (adhesives), which does not occur spontaneously, in addition to the mechanical
interlock. There are several dental adhesives that can be used between metals and polymers for
dental prostheses and orthodontic devices, but the bonding strength reported so far is insufficient
[20, 22-24].
This research provides a new way of creating a strong chemical bond between alloys (i.e.
titanium and stainless steel) and polymers (i.e. PMMA and Bis-GMA) for dental devices based
on diazonium chemistry. This new adhesive can be used on titanium or stainless steel surfaces to
increase their bonding strength to PMMA or Bis-GMA composite. Increased bond strength
between alloys and polymers through diazonium treatment would improve the properties of
dental devices, reduce debonding between alloys and polymers in dental prostheses and
orthodontic brackets, provide more leverage in cases with complex mechanics, and allow the use
of brackets with smaller bases resulting in fewer complications associated with esthetics and oral
hygiene.

16
Chapter 2: Background and Literature Review
2. Esthetics and Dental Occlusion
Esthetics and well aligned teeth contribute to a healthy masticatory function, pleasant smile, and
adequate phonetics [2]. Loss of teeth (edentulism) and malocclusion can have a negative impact
on patients’ self esteem and masticatory function [6]. These negative impacts can be improved
with dental prostheses which replace missing teeth or orthodontic devices that correct tooth
malocclusion [1-6].
2.1. Edentulism
Edentulism refers to patients missing some or all their natural teeth. A person is completely
(fully) edentulous when missing all the teeth, or partially edentulous when missing some but not
all the teeth. Although the rates of edentulism vary in the world, the number of people who are
completely or partially edentulous is large [25]. It is estimated that 15 % of the global population
is completely edentulous [7]. In particular, 12% of the population in the United States is
completely edentulous which equal to 36,000,000 people [26]. Moreover, 71.5% of USA
population between age 65 and 75 years old is partially edentulous [27]. In Canada, the
population of the completely edentulous patients in 2010 was 6.4% of the whole country and
21.7 % among adults between 60 and 79 years old [25]. The rate of complete and partial
edentulism in the population increase among elderly people, and it will increase in the future due
to aging of the population [27]. Currently, the percentage of elderly people in the United States is
13%, but it is expected to double by the year 2030 [27].

17
The incidence of tooth loss in some developed countries is 0.1 to 0.3 tooth for every person per
year [1]. Tooth loss is associated with age, socioeconomic status and lifestyle. The number of
missing teeth is high among elderly people (age 65 years and older) while poor oral hygiene,
tobacco and alcohol consumptions are the most common risk factors for missing teeth [1, 27].
Education, access to dental care, and insurance coverage are the other common factors
contributing loss of teeth [25].
Edentulism has serious of consequences on patents’ general and oral health as well as on quality
of life [25]. Tooth loss contributes to anatomical changes of the mouth and face [25]. For
instance, the bone and residual ridge are expected to shrink after tooth loss affecting patients’
esthetic and challenging future treatments [27]. Having unacceptable aesthetics is the most
common concern for edentulous patients especially when the missed teeth are in the visible
anterior region. Furthermore, patients’ phonetic usually change after tooth loss because the
contacts between the maxillary and mandibular teeth are changed. Losing the ability of chewing
food effectively is the major functional issue; In fact, chewing food effectively involves
subdivision of food by the occlusal force of the teeth, and bringing food into the occlusal surface
of the teeth by the oral tissues including the tongue and the cheek [25, 27].
2.1.1. Treatment of Edentulous Patients
Edentulous patients’ treatment depends on many factors, such as number of missing teeth, oral
tissue structure, and patient’s preferences. The goal of the treatment is to restore function,
esthetics and phonetics using a prosthesis that cooperates with the existing natural teeth and
tissues [11]. There are many treatment options available to replace missing teeth [1-5, 8-11]. In

18
this introduction, the treatment options will be discussed for the partially edentulous patients first
and then for the completely edentulous patients.
2.1.1.1. Treatment of Partially Edentulous Patients
The common treatment options for the partially edentulous patients are fixed partial dentures
supported by natural teeth or dental implants, or removable partial dentures retained by natural
teeth or dental implants [1, 5, 8, 10].
2.1.1.1.1. Fixed Partial Dentures
One or more missing teeth can be replaced with fixed partial dentures such as bridges. Bridges
are prostheses that replace missing teeth by anchoring on the teeth or implants adjacent to the
missing teeth (Figure 2.1) [1]. Tooth supported bridges (conventional bridges) are the most
common treatment because of their cost and time needed for completion. Bridges can also
replace two or three adjacent missing teeth according to the edentulous span (the length of the
arch where teeth are missing), occlusal stress, and health of the remaining natural teeth [4, 28].
The principle of bridge prosthesis is preparing the natural teeth adjacent to the edentulous span
as abutments to support the artificial teeth. The bridge (Figure 2.1) usually consists of at least
two retainers which are copings supported on natural tooth abutments, and one or more units
connected to the retainers, called pontics, that replace the missing teeth [1, 4, 28].
Bridges are usually fabricated with metals (full metal), ceramics (full ceramic) or a combination
of both (metal-ceramic restorations) [28]. Full metal bridges (i.e. gold or cobalt-chromium) have
the best mechanical performance but their esthetics is unacceptable especially when the missing
teeth are in the anterior region [1, 4]. The metal-ceramic bridge is the common type, and it

19
consists of a metal framework and a ceramic veneer that is built up over the metal [1, 4]. The
function and esthetics provided by metal-ceramic and full ceramic bridges are excellent and
comparable to that of natural teeth. However, there is a major disadvantage for using bridges that
is the need for trimming the adjacent natural teeth to allow attachment of the bridge [4, 28].
Figure 2.1: Replacing missing teeth using a fixed partial denture (Bridge). A: the prepared tooth for anchoring the bridge
(abutments), B: retainers, C: pontic.
2.1.1.1.2. Dental Implants
A dental implant is a biocompatible device placed in the jawbone to provide support and
retention for the artificial dental teeth and prostheses [29]. Dental implants are not new; in
ancient history Egyptians shaped seashells and inserted them into the jaw [11]. However, the
modern dental implant concept begun in 1952 when Dr. Per-Ingvar Branemark accidentally
discovered that living bone interacts and binds to titanium and this property became to be known
as osseointegration [4, 11, 30]. The first titanium dental implant used to replace a missing tooth
was done in 1965, and since then the application and market for dental implants has been
continuously growing [4, 30]. Dental implants have been subject to significant improvements in
materials and design that raised the success rates for dental implants and make them a very
popular choice for replacing missing teeth [4, 11, 31]. It is estimated that more than 450,000
dental implants are being placed every year [30].

20
Osseointegration is the most important factor for the success of dental implants treatment. There
are many factors affecting osseointegration that should be considered before treatment such as
age of the patient, bone quality, smoking, and alcohol consumptions [10]. Dental implants
(Figure 2.2) can be used to support or retain different prosthesis types such as crowns, bridges,
removable partial dentures, and complete dentures [1, 4].
Treatments of edentulous patients with implant-retained dental prostheses eliminate many of the
disadvantages associated with traditional dental prostheses [1, 4, 11]. The traditional removable
partial dentures or complete parietal dentures rely on oral tissues to hold the denture resulting in
discomfort, while implant supported or retained dentures have superior function and comfort for
patients than traditional removable partial dentures. Moreover, using implants to support or
retain dentures are more esthetic than using unesthetic metallic clasps in the traditional
removable partial dentures which located in the labial or lingual sides of teeth [7, 8]. Replacing
one or more teeth using bridge treatment require to trim down the adjacent natural teeth next to
the edentulous span that are not preferred for many patients and it can be avoided by using dental
implants [1].
The most metals used in dental implants are the pure titanium (grade I to IV) and titanium alloys,
such as Ti-6Al-4V [4]. The main components of the dental implants are the implant cylinder
(root), which is inserted inside bone, and the abutment, which retains or supports the dental
prosthesis (Figure 2.2) [4, 10]. The abutment is usually screw-fastened onto the implant’s root.
Dental implants vary according to the design and size of the cylinder and implant-abutment
connection [10]. Implants roots are usually cylindrical in shape with lengths between 6 to 20 mm
and diameters between 3 to 6 mm [10]. The surface of the implants root is treated via many

21
techniques to increase the bonding between implants and bone (osseointegration) including
sandblasting, etching, and spray coating [4, 10].
Figure 2.2: Dental implant components for the single-unit fixed prosthesis. A: implant cylinder (root); B: screw-fastened
implant abutment and; C: artificial crown fixed on the abutment of the dental implant.
2.1.1.1.3. Removable Partial Dentures
A removable partial denture (RPD) is a prosthesis that replaces one or more missing teeth, and is
supported and retained by the remaining natural teeth, tissue, and/or implants. Removable partial
dentures provide high function and pleasing esthetics and they are designed to be removed and
reinserted by the patient [4]. Removable partial dentures are suitable for partially edentulous
patients who are not able to have fixed prostheses because of their health conditions or the length
and location of the edentulous span [7].
The design of removable partial dentures depends on the number and location of missing teeth
and on the health of oral tissues and natural teeth that will support and retain the prosthesis [9].
Partially edentulous arches can be classified into many different classifications according to the
number and location of the missing teeth. The classification named Kennedy is the most
accepted because it is simple and easy to apply; it divides the partial edentulous arches into four
groups [7-9, 32]. The most common groups of Kennedy classification are class I and class II.
Class I defines bilateral edentulous areas located posterior to the remaining teeth while class II
defines unilateral edentulous areas located posterior to the remaining teeth [32]. Class III of

22
Kennedy classification defines tooth bounded unilateral edentulous areas while class IV indicates
a single edentulous area located anterior to the remaining natural teeth and crossing the midline
[32]. Removable partial dentures design depends on the dental arch classification; for example,
the RPD’s design in Kennedy class I and II rely both on teeth and oral tissues for support and
retention of the prosthesis while in class III and IV support and retention is provided solely by
the remaining teeth [7].
The typical removable partial denture, cast-metal RPD, consists of a metal framework, artificial
teeth, and an acrylic denture base. The metal framework consists of four parts (Figure 2.3): major
connectors, minor connectors, direct retainers, and indirect retainers [4, 5, 7, 33]. A major
connector is used to connect all the main parts of the prosthesis and helps distribute the occlusal
force into selected teeth and tissues while a minor connector is used to connect the major
connector or the denture base to other components such as clasps, rests, direct and indirect
retainers [5]. A direct retainer is a component that engage a tooth to provide retention and resist
movements away from the oral tissues and natural teeth, and it can be intracoronal or
extracoronal [33, 34]. Clasps are the most common extracoronal retainers and they usually
consist of a lingual arm, a buccal arm, and a rest, and they are used in different designs including
circumferential clasps, bar clasps, ring clasps, and roach clasps [5, 33]. The rest provides vertical
support and it can be located on the occlusal, lingual, or incisal tooth surface. Indirect retainers
assist the direct retainers to prevent rotation or displacement of distal extensions of the denture
and it is usually composed of a rest [35]. The removable partial denture (RPD) metal framework
is connected to the acrylic-resin denture base (poly-methyl methacrylate; PMMA) and to the
acrylic teeth [36]. The main materials used in the metal framework of cast-metal removable
partial dentures are cobalt-chromium, gold, or titanium.

23
Figure 2.3: (Left) the mandibular partially edentulous arch before treatment. (Middle): the mandibular framework for
the removable partial denture and its components of A: major connector; B: minor connector; C: rests; D: direct
retainer; E: indirect retainer. (Right) the removable partial denture (RPD) on the edentulous arch.
An alternative version of the RPDs is the acrylic RPD. The acrylic RPDs, known as temporary
RPDs, are made of an all-acrylic base (poly-methyl methacrylate; PMMA), acrylic teeth, and
wrought wire clasps for retention. The acrylic RPDs are easy to fabricate and less expensive than
the cast-metal RPDs and its esthetic is acceptable [4]. However, the acrylic RPDs are consider
temporary prostheses and not recommended for long-term prosthesis because of their poor
mechanical properties such as strength [4].
Dental implants can be used to provide support and retention for removable partial dentures [4,
8]. Implant-retained removable partial dentures are similar to conventional removable partial
dentures supported by natural teeth and tissue, although they also gain additional support and
retention from the dental implants. Implant-retained RPD provide better function, esthetics and
comfort than conventional removable partial dentures [8].
2.1.1.2. Treatment of Completely Edentulous Patients
The common available treatments for complete edentulism are removable complete dentures and
fixed complete dentures.

24
2.1.1.2.1. Removable Complete Dentures
Complete dentures have been considered the standard treatment option for complete edentulism.
Complete dentures are prostheses that replace all missing teeth in the maxillary or mandibular
arch (Figure 2.4). Complete dentures are supported and retained by the oral tissues and mucous
membranes when the anatomy and the functional tonicity of the patients’ mouth are adequate [7,
26]. Removable complete dentures generally consist of a denture base, made of acrylic (poly-
methyl methacrylate; PMMA) or metal, and artificial teeth, made of acrylic or composite resin
[4, 7]. Removable complete dentures provide acceptable esthetics at a reasonable cost compared
to implant-supported prosthesis; however, several issues are associated with complete dentures
such as low denture stability especially in the lower arch [4, 7, 26]. Moreover, complete dentures
need to be changed or refitted every few years due to the shrinkage and changes in bone and
supporting tissues [4].
Figure 2.4: Complete partial dentures for maxillary and mandibular arches.
Overdentures are complete dentures retained by dental implants. This type of dentures solves
main problem associated with complete dentures that is the lack of stability in the lower jaw in
patients with severe alveolar ridge atrophy [4]. There are two major types of overdentures;

25
removable overdentures and fixed overdentures. Removable overdentures are similar to
conventional complete dentures, but they are retained by two to four dental implants using clip-
bar, spheres, or magnetic attachments (Figure 2.5) [4]. The removable overdentures provide high
stability and retention in the mouth and are less expensive than the alternative implant-supported
prosthesis. However, this type of prostheses must be removed daily for cleaning [4, 7, 26].
Figure 2.5: The implants-supported complete denture (overdentures); two-implants support the mandibular removable
overdentures.
2.1.1.2.2. Fixed Complete Dentures
Fixed overdentures are complete dentures retained and supported directly by dental implants.
Fixed complete dentures (Figure 2.6) consist of a denture-base, made of acrylic or metal, and
teeth, made of acrylic or porcelain, fixed on dental implants [4]. This prosthesis is the best
available treatment for edentulous patients because it provides superior esthetics, comfort, and
function. However, fixed overdentures have several disadvantages such lengthy cost, difficult
fabrication process [4]. Nevertheless, fixed complete dentures are considered the most
recommended treatment for edentulous patients [4].
26
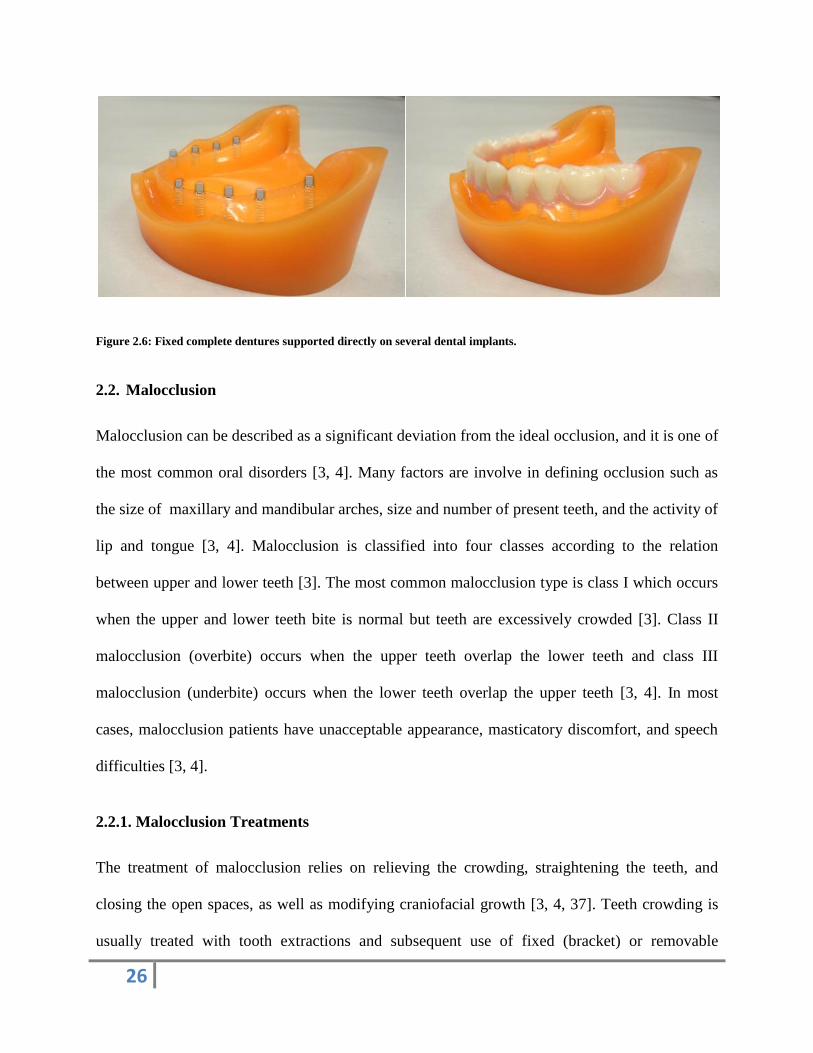
Figure 2.6: Fixed complete dentures supported directly on several dental implants.
2.2. Malocclusion
Malocclusion can be described as a significant deviation from the ideal occlusion, and it is one of
the most common oral disorders [3, 4]. Many factors are involve in defining occlusion such as
the size of maxillary and mandibular arches, size and number of present teeth, and the activity of
lip and tongue [3, 4]. Malocclusion is classified into four classes according to the relation
between upper and lower teeth [3]. The most common malocclusion type is class I which occurs
when the upper and lower teeth bite is normal but teeth are excessively crowded [3]. Class II
malocclusion (overbite) occurs when the upper teeth overlap the lower teeth and class III
malocclusion (underbite) occurs when the lower teeth overlap the upper teeth [3, 4]. In most
cases, malocclusion patients have unacceptable appearance, masticatory discomfort, and speech
difficulties [3, 4].
2.2.1. Malocclusion Treatments
The treatment of malocclusion relies on relieving the crowding, straightening the teeth, and
closing the open spaces, as well as modifying craniofacial growth [3, 4, 37]. Teeth crowding is
usually treated with tooth extractions and subsequent use of fixed (bracket) or removable

27
orthodontic appliances for tooth alignment and space closure [4, 37]. The cases that require
growth modification of the jaws are treated with fixed or removable functional appliances [3,
37]. Finally, removable appliances (retainers and space maintainers) are used to hold the teeth in
their position after the orthodontic treatment is finished.
2.2.1.1. Fixed Appliances
Fixed orthodontic appliances are appliances that are fitted and fixed on the teeth and cannot be
removed by patients. Fixed appliances move teeth from malaligned positions to the correctly
aligned ones. This treatment option can be used to treat most malocclusions; however, they have
many disadvantages in terms of esthetics, oral hygiene, and cost. Fixed appliances usually
consist of bands, metallic wires, and brackets that are cemented to teeth through an adhesive, as
well as other active components such as springs, elastics, and separators (Figure 2.7) [3, 4, 37].
The wires are made of alloys such as stainless steel, cobalt-chromium, cobalt-chromium-nickel,
and titanium [11, 16]. Brackets are made of different materials such as ceramics or plastics,
although most of them are made of metallic alloys (i.e. stainless steel and cobalt-chromium) [16,
37]. Brackets are designed with bases that provide micromechanical interlocking to improve the
bonding between brackets and composite for better adhesion to teeth [17, 38, 39]. The brackets
are usually bonded bucally or lingually to teeth using adhesives based on methacrylate composite
such as Bis-GMA, TEGDMA, and HEMA [3, 4, 16, 37].

28
Figure 2.7: Fixed appliance for malocclusion treatment that consists of A: brackets and B: metallic wires.
2.2.1.2. Removable Appliances
Removable orthodontic appliances can be removed by patients for cleaning or on the social
sensitive occasions. They are less expensive and their fabrication consumes less chair-side time,
but they are not recommended for treatment of complex cases [4]. Removable orthodontic
appliances have different designs and functions and they usually consist of an acrylic baseplate
as well as active and retention components [3, 37]. Removable appliances are commonly used to
maintain tooth position after treatment (i.e. retainers) (Figure 2.8), as well as for moving, tipping,
and titling teeth using active components such as springs, screws, or bows [4, 37, 40] Retention
components, such as clasps, and most active components are fabricated from metallic wires (i.e.
stainless steel) bending to the desire shape and embedded to the acrylic baseplate [4, 40]. The
baseplate provides stability and support for the active and retentive components and is usually
made of poly-methyl methacrylate (PMMA) [37, 40].

29
Figure 2.8: Removable appliance (retainers) that consists of A: metallic wires (retention components) and B: acrylic
denture base and used to maintain teeth after treatment.
2.3. Materials Used in Dentures and Orthodontic Devices
The materials used for fabricating dentures and orthodontic appliances can be classified into four
categories: metals, ceramics, polymers, and composites [11, 41]. These categories are different
from each other in terms of their physical and mechanical properties, processing methods, and
cost [11, 41]. Metals are primarily used in dental prostheses and orthodontic devices when
durability and strength are required while ceramics are used when esthetics is important [42].
Polymeric materials are commonly used because they combine excellent esthetic and mechanical
properties at a reasonable cost [42]. Underneath we address in detail each one of these
categories.
2.3.1. Metals
Pure metallic elements alone have inadequate properties for dental applications; thus, dental
alloys that combine various elements suitable to be used in dental prostheses [41]. Generally,
dental alloys should fulfill many different criteria including biocompatibility, corrosion
resistance, strength, hardness, melting temperature, and economic aspects that are useful for
dental applications [11, 42]. Alloys used in dental devices are either laser sinters machines,

30
casted into customized shapes or with wrought wires [11]. Casting alloys used for dental
prostheses are divided into high noble alloys, noble alloys, and base-metals alloy [41, 42]. Alloys
are considered high-noble when more than 60% of their composition is a noble metals such as
gold, platinum, and palladium; noble if the noble metals is 60 to 25%; or base-metal when noble
content is less than 25% [41]. Base-metal alloys are used extensively in all dental prostheses
because of their excellent mechanical properties and low cost. Dental alloys have different
physical, chemical, and biological properties based on their elemental compositions [41, 42].
Underneath we address in detail the main groups of alloys used in dentistry.
2.3.1.1. Titanium
Titanium (Ti) raises great interest in dentistry due to its excellent properties; it is highly
biocompatible which being significantly less expensive than noble metals, such as gold [41-45].
Titanium has excellent mechanical and physical properties, such as high strength and low
density, that helps to withstand the mastication force which make it more comfortable for
patients [42]. Moreover, titanium has low modulus and thermal conductivity with good chemical
stability and corrosion resistance [42-46]. Titanium alloys (i.e. Ti-6Al-4V) are widely used in
dental implants and wrought wires for dental prostheses and orthodontic appliances, and has
recently raised interest as materials for dentures frameworks [41]. However, titanium alloys are
difficult to cast because they require special and expensive furnaces due to their high melting
point; therefore, the use of titanium in casted frameworks for removable and fixed prostheses is
limited [41, 46]. Milling systems, such as Computer Aided Design / Computer Aided
Manufacturing (CAD/CAM), enables the use of titanium in removable and fixed prostheses
frameworks that can be designed through computer software and milled in a machine [41].
Moreover, the Direct Metal Laser Sintering (DMLS) is a new technology that can be used to
31
produce fixed or removable prosthesis frameworks of Ti [41]. DMLS works by applying a high-
power laser to fuse many layers the powdered metal (i.e. Ti and Co-Cr) building up the desired
three-dimensional frameworks [41].
2.3.1.2. Cobalt-Chromium
Removable partials frameworks and metal bases of ceramic-metal restorations such as crowns
and bridges are commonly made of cobalt-chromium alloys (Co-Cr) [41, 46]. Cobalt-chromium
casting alloys used in frameworks of removable partial dentures and in ceramic-metal
restorations may have small differences in their composition used to control specific properties
such as the coefficient of expansion and strength [36, 41]. The percentage of cobalt in the alloy is
usually around 60% and it is responsible for increasing strength, hardness, and elastic modulus
while the chromium content is usually less than 30% and it is responsible for the corrosion
resistance [41, 46]. Beside cobalt and chromium, these alloys include low concentrations of other
elements such as carbon, silicone and molybdenum that help improve their properties (i.e.
hardness and melting point) [41].
Cobalt-chromium alloys are suitable for dental prostheses because of their mechanical properties
and low cost [36, 41, 42]. For instance, mechanical properties of cobalt-chromium alloys such as
tensile strength, yield strength and hardness are excellent. The low density of the cobalt-
chromium which is half of gold density is also an advantage in dental prostheses [41]. Cobalt-
chromium also can be machined with milling systems to fabricate fixed or removable prostheses
through Computer Aided Design / Computer Aided Manufacturing (CAD/CAM) or Direct Metal
Laser Sintering (DMLS) [41, 42].

32
2.3.1.3. Stainless Steel
Steel is an alloy of iron and carbon, and stainless steel is a modification of steel that contains
chromium, manganese and other elements to provide stainlessness [41, 42]. Stainless steel
cannot be cast, and it is frequently used in dentistry in its wrought form or as readymade
products (i.e. orthodontic brackets and bands) that provided by dental suppliers [16, 37].
Wrought wires are used for fabricating orthodontic appliances and acrylic removable prosthesis
(temporary RPD) [41, 42, 46]. Most stainless steel alloys used for dental applications contain
72% iron, 18% chromium, 1% carbon and low concentration of other elements such as nickel,
molybdenum and silicon [41]. The mechanical performance of stainless steel is excellent in
tension, bending, and torsion; however, its high ductility sometimes could be a problem for
stainless steel wrought wires [41, 42].
2.3.2. Ceramic
Dental ceramics (porcelain) are a mixture of three materials: quartz, feldspar, and kaolin, fired at
high temperature [41]. Dental ceramics are classified into two groups according to their
applications: ceramics for the metal-ceramic prostheses (porcelain fused to metal) or for all-
ceramics prostheses [41, 42]. The common examples of metal-ceramic prostheses are crowns and
bridges while the inlays, onlays, veneers, and full ceramics crowns are the common applications
for full ceramic prostheses [41]. Dental ceramics in metal-ceramics restorations are built up on
metal base frameworks, and they are composed of three layers: opaque, dentin, and enamel [41].
The opaque is used to mask the black color of metals, while the dentin is the main bulk of the
restoration. Finally, the enamel is added to add transparency to the artificial teeth.

33
Ceramics are the best available materials used in dental prostheses for matching the esthetics of
human teeth because they can mimic tooth color, shade, and transparency [41, 42]. Dental
ceramics are hygienic, biocompatible, and chemically stable in the oral cavity [42]. However,
ceramics are brittle and weak in tension [42]. The newly developed all-ceramic materials such as
zirconia and alumina have high strength are now widely used as all ceramic prosthesis through
different techniques such as heat-pressing, slip-casting, sintering, and computer aided design/
computer aided manufacturing (CAD/CAM) [41, 42].
2.3.3. Polymers and Composites
Polymers were introduced in dentistry in 1840s when Goodyear discovered vulcanized rubber as
denture-base material for dental prostheses [47]. This polymer was used in denture-base material
for over seventy-five years although it had poor aesthetic and bad taste. In the 1930s, the poly-
methyl methacrylate (PMMA) was introduced in dentistry and became the most frequently used
polymer in dental prostheses [48]. Artificial teeth and denture bases for dental prostheses are the
main area where polymers are used in dentistry [11]. Polymers are also used for different dental
applications such as impression material, impressions trays, fillings, adhesives, and orthodontics
appliances [42].
Dental composites are usually a combination of polymers and ceramics that result a new material
with superior properties [41, 47]. Dental composites are based on methacrylate polymers, such as
bisphenol A glycidyl methacrylate (Bis-GMA), and they are used in as filling materials to restore
damaged teeth and as adhesive for orthodontic brackets [41, 42]. Dental composites are
becoming popular in dentistry because of their esthetics and mechanical properties.
34
2.3.3.1. PMMA
Poly-methyl methacrylate (PMMA) has been used in many important dental applications such as
impression trays, artificial crowns and bridges, and in orthodontic and maxillofacial appliances
[41]. In addition, PMMA is the main material used in dentures, including removable partial
dentures, removable complete dentures, and fixed complete dentures. It is estimated that PMMA
represents 95% of all polymers used in dental prostheses [49].
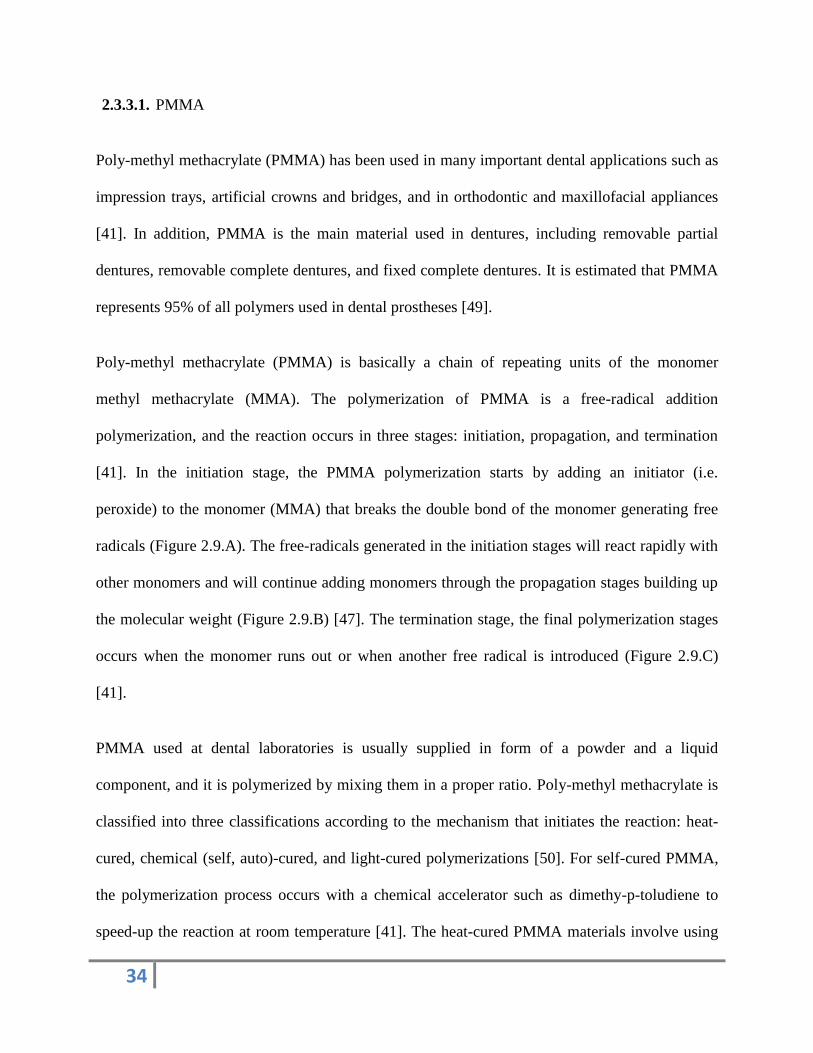
Poly-methyl methacrylate (PMMA) is basically a chain of repeating units of the monomer
methyl methacrylate (MMA). The polymerization of PMMA is a free-radical addition
polymerization, and the reaction occurs in three stages: initiation, propagation, and termination
[41]. In the initiation stage, the PMMA polymerization starts by adding an initiator (i.e.
peroxide) to the monomer (MMA) that breaks the double bond of the monomer generating free
radicals (Figure 2.9.A). The free-radicals generated in the initiation stages will react rapidly with
other monomers and will continue adding monomers through the propagation stages building up
the molecular weight (Figure 2.9.B) [47]. The termination stage, the final polymerization stages
occurs when the monomer runs out or when another free radical is introduced (Figure 2.9.C)
[41].
PMMA used at dental laboratories is usually supplied in form of a powder and a liquid
component, and it is polymerized by mixing them in a proper ratio. Poly-methyl methacrylate is
classified into three classifications according to the mechanism that initiates the reaction: heat-
cured, chemical (self, auto)-cured, and light-cured polymerizations [50]. For self-cured PMMA,
the polymerization process occurs with a chemical accelerator such as dimethy-p-toludiene to
speed-up the reaction at room temperature [41]. The heat-cured PMMA materials involve using

35
thermo sensitive accelerators that can be activated using a heat source (i.e. hot water bath,
microwave). The light-cured PMMA contains photo sensitive accelerator that are activated upon
exposure to light [41, 47].
Figure 2.9: Scheme of the polymerization reaction of PMMA. A: the initiation stage using initiator; B: PMMA in the
propagation stage; C: the PMMA in the termination stage.
Heat-cured and self-cured PMMA powders are consisted of high molecular weight poly-methyl
methacrylate (PMMA) as main constituent, initiators (i.e. benzoyl peroxide), dyes (i.e. mercuric
sulphide or cadmium sulphide), opacifiers (i.e. zinc oxide or titanium oxide), and plasticizer (i.e.
dibutyl phthalate) [51]. The PMMA liquid consists of methyl methacrylate monomer (MMA),
cross-linking agent (i.e. glycol dimethacrylate), plasticizer (i.e. dibutyl phthalate), and inhibitor
(hydroquinone). The differences between heat-cured and the self-cured PMMA is the chemical
accelerator (i.e. dimethy-p-toludiene) only added into the liquid of the self-cured PMMA [51].
The dyes and opacifiers in dental PMMA are used to provide the required esthetic to mimic the
natural appearance of teeth and oral tissues [41]. The cross-linking agent is added to the liquid to
improve strength, hardness and wear resistance while the plasticiser is added to the PMMA
powder to reduce the rigidity and the glass-transition temperature (Tg) [51]. Finally, adding the

36
inhibitor in the PMMA liquid is to extend the shelf-life of the liquid for long term storage [41,
51].
Unlike heat-cured PMMA, light-cured PMMA is usually supplied as one single component in the
form of a premixed rope or sheet that is activated and polymerized quickly by exposing it to
visible blue light [47]. Recently, the light-cured PMMA has become very popular in many dental
applications because it is easier and faster to process than either heat or self-cured PMMA.
Although the mechanical and physical properties of PMMA are influenced by the concentration
of its components (i.e. monomer and initiator) and curing conditions (i.e. temperature, time, and
cycling process), PMMA properties are very suitable for dental prostheses [52]. The glass
transition temperature (Tg) for the heat-cured (125oC) and self-cured (90
oC) PMMA exceed the
requirements for temperature resistance in the oral cavity [52]. Moreover, the mechanical
properties for PMMA, such as toughness and hardness, are acceptable. The tensile strength (55
and 90 MPa) and flexural strength in the PMMA consider very high compared to different
polymers [52]. The fatigue life and impact strength in the PMMA are the main problems because
they are low and can lead to the prostheses’ failure [52]. Furthermore, the shrinkage percentage
(6.2 %) is another disadvantage of PMMA that can prevent dentures from fitting accurately into
the patient’s mouth [51]. The esthetic properties of PMMA are excellent because PMMA can be
transparent or colored for matching the colors of the teeth and tissues, and can even incorporate
small colored fibers to give a veined appearance [51, 52]. Poly (methyl methacrylate) is a
biocompatible polymer that is non toxic and does not cause irritations to the oral tissue after it is
fully polymerized [50, 51]. However, there is a concern about the biocompatibility of PMMA in
dentures containing small amounts of residual (un-reacted) monomers that cause toxicity,

37
allergy, and irritation to the oral tissues, and they can be transferred to blood through saliva,
affecting organs, such as liver, kidney, and heart [50]. Furthermore, toxicity of self-cured PMMA
is higher than that of heat-cured PMMA because it contains higher amounts of toxic residual
monomer, initiators, and activators [51]. Moreover, dental technicians, who work with PMMA to
fabricate dentures, face more toxicity and allergies because they are exposed to MMA-vapor
while processing it [50]. Generally, the toxicity of PMMA in dental devices is considered very
low and safe when polymerized properly.
The differences between heat-cured and self-cured PMMA is that heat-cured PMMA has higher
molecular weight, strength, fatigue life, and impact resistance than self-cured PMMA [47]. the
porosity, deformation, and distortion in the heat-cured PMMA is lower than self-cured PMMA
especially when it is heated gradually and uniformly during the polymerization process [47].
Light-cured PMMA presents lower shrinkage and faster and easier processing than self-cured
and heat-cured PMMA [47].
2.3.3.2. Bis-GMA
The Bis-GMA (bisphenol A glycidyl methacrylate) is a resin composites based on a methacrylate
that was introduced to dentistry in the 1960s to improve the mechanical and aesthetic properties
of dental polymers. Bis-GMA is used widely in dental prostheses, dental fillings, and adhesives
for orthodontic appliances [41, 48]. Bis-GMA is a combination of one part of bis-phenol and two
parts of glycidyl methacrylate that are polymerized in a free-radical addition reaction (Figure
2.10) [52]. Bis-GMA has high molecular weight and high viscosity because of the hydrogen
bonding. Bis-GMA based dental resins consist of four major components: the organic polymer
matrix, an inorganic filler, a coupling agent, and an initiator-accelerator system [41]. Fillers such

38
as quartz, fused silica, and glasses are the major portion of the composite that can be in macro,
micro, or nano size and helps increase the hardness and reduce thermal expansion and shrinkage
[41, 52]. Coupling agents are added into the Bis-GMA composite to covalently bind the matrix
to the fillers. The light-cured polymerization for the Bis-GMA composite is the preferred
technique while the self-cured polymerization can occurs with peroxide initiators at room
temperature; the dual-cured is a combination of light and chemical activation [41, 52, 53].
Figure 2.10: Schematic diagram of the chemical reaction for Bis-GMA.
The shrinkage percentage in the Bis-GMA (2.7%) is lower than in PMMA (6.2 %) while the
compressive strength for the Bis-GMA (110-160 N/mm2) is higher than PMMA (75 N/mm
2)
[51]. Furthermore, the modulus elasticity of Bis-GMA (11200 N/mm2) is much higher than
PMMA (1800 N/mm2) [51]. Therefore, it is preferred to use the Bis-GMA for dental prosthesis
that withstands a high compression and impact strengths. The polymerization reaction of Bis-
GMA can take up to 24 hours to be full and complete; therefore during this period, this polymer
can present some toxicity due to release of un-reacted reagents [51, 52]. The biocompatibility of
Bis-GMA is better than the biocompatibility of PMMA because it contains a lower amount of

39
residual monomer [51, 52]. Moreover, light-cured Bis-GMA has been found to be less toxic and
irritating to oral tissues than self-cured Bis-GMA [52].
2.4. Bonding Systems in Dentures and Orthodontic Appliances
Dental prostheses and orthodontics appliances usually combine metallic (i.e. Ti, Co-Cr, and
stainless steel) and polymeric (i.e. PMMA and Bis-GMA) parts. Theses metallic and polymeric
parts in dental devices are joint together to prevent mechanical failure at the interfaces between
them and maintain the integrity of the appliance or prosthesis [41, 54]. Weak bonds allow cracks
to form, grow, and split the metal-polymer interfaces causing dental device failure [11]. Strong
bonding between metals and polymers is also important to prevent bacteria colonies to grow at
the interface causing stains and bad smell [41]. It also important in the fixed orthodontic
appliances since strong bond will prevent the debonding between brackets and teeth which cause
bracket loss [3, 4, 13-17, 37, 55]. Bonding at the interface between metals and polymers can be
improved using mechanical or chemical approaches.
2.4.1. Mechanical Bonding
The mechanical bond between metals and polymers can be formed by penetration and
interlocking of the polymer into the irregularities of the metal surface [11, 12]. Surface
irregularities also help increase the surface area of metals and consequently the overall bond
strength. Orthodontic brackets are designed with bases have micromechanical interlocking to
improve the bonding between brackets and composite [17, 38, 39]. Accordingly, the most
common methods for creating a mechanical bond between metals and polymers can be done by
creating surface irregularities on metallic substrates using sandblasting (air abraded) or chemical
etching. Sandblasting can be performed by applying a stream of aluminum oxide particles with a

40
size between 50 to 250 µm against the metallic substrates under high pressure for 10 to 60
seconds, this roughens the metallic surfaces and provides mechanical bond to the polymers [54].
This technique also helps to remove all the rust and loose particles from the metal surface after
casting, and it is commonly used on metal frameworks of dental prosthesis such as fixed partial
and removable partial dentures. Another way to create surface irregularities is using the Rocatec
System, a silica-coating to metals at high temperature [54]. Chemical-etching with acids such as
H2SO4, HCl and HNO3 at pH≈1.0 is another way of creating surface irregularities micro to nano-
size (0.5 to 2 µm). Etching is an effective way to increase the mechanical bond of polymers to
metals [56].
2.4.2. Chemical Bonding
Chemical bonding involves the formation of covalent, ionic, or hydrogen bonds on the surfaces
interface. However, chemical bond between alloys and polymers does not occur spontaneously.
Achieving a chemical bond at the interference between alloys and polymers usually requires the
use of an adhesive on the metal substrates [18, 23, 57-70]. Adhesives are materials that are
applied on surfaces to permanently join two or more parts together through a bonding process
[20, 22]. Using adhesives between alloys and polymers for dental prosthesis is not common, but
it has recently raised interest [23].
Dental adhesives are mostly a composed of a hydrophilic monomer carried in solvents that react
violently with an initiator in free radical polymerization [24]. Dental adhesive containing
molecule 4-META (Methacryloxy ethyl trimellitate anhydride) was the first commercial metal-
adhesive launched in the market in 1982 under the name name Super-Bond C&B [23, 24]. Then,
the chemical component MDP (Methacryloyloxydecyl dihydrogen phosphate) was added in 1983
41
with 4-META to enhance the bonding of metals to polymers; however, these primers were only
used with non-noble metals [23]. The primers that contain VBATDT (Vinylbenzyl-n-propyl
amino triazine dithione) knows as V-Primer or Alloy Primer were marketed in 1994 to be used
with noble and non-noble metals [23, 70]. More recently, many different metal-adhesives based
on phosphonic acid monomer or phosphonates such as MHPA (Methacryloxyethexy
phosphonacetate), MEPS (Methacryloxydecly thiophosphate derivative) under commercial
names such as the AZ Primer have become available in the market [23, 24]. MDDT
(Methacryloxydecly dithiooctanoate), commercially known as Metal Link Primer, are suitable to
be used with noble and non-noble metals [24, 70].
Dental silane coupling agents that contain MPS (Methacryloyloxy propyltrimethoxy silane) or
MATP (Methacryloxypropyl-trimethoxysilane) are used in dentistry to enhance the bond
between polymers and metals or ceramics [24, 71]. The silane group provides a covalent bonding
between polymers and silica-based materials (ceramics) or active metallic substrates, but the
bonding to silica-based materials is significantly higher than the non-silica based such as metals
[71, 72]. There are many different commercial dental silane coupling agents used in dentistry
such as RelyX, Bisco Porcelain Primer, Cimara, ESPE Sil, and Pulpdent [71, 72].
2.5. Debonding in Dentures and Orthodontics Appliances
Composite materials that combine polymers with alloys often suffer from mechanical failure at
the interface between them. In fact, dental devices often present catastrophic mechanical failures
due to lack of bonding between their metallic and polymeric components [18, 19]. These devices
include dental prostheses, combining metallic frameworks (i.e. titanium and cobalt-chromium)
and wrought wires with acrylic (PMMA); and orthodontic appliances, combining acrylic

42
(PMMA) with stainless steel wrought wires or Bis-GMA composite with stainless steel brackets.
Chemical bonding between alloys and polymers in dental devices does not occur spontaneously.
Therefore, the bonding between alloys and polymers in dental devices is usually provided by the
micromechanical interlocking or sandblasting which barely creates a mechanical bond on the
metallic surface that can bind to polymer. However, this bond is insufficient to prevent the
debonding at the metal-to-polymer interface [18, 19].
2.5.1. Bonding between Alloys and PMMA
Several bonding methods are currently used to increase the bonding strength between PMMA
and alloys in dental prostheses [18, 57-69]. Still, the bond strength achieved between PMMA and
metals so far is insufficient. The highest tensile strength in the literature for the bond between
PMMA and titanium using a combination of sandblasting and bonding agents phosphonate-based
adhesives (MHPA, MDP and VDT; table 2.1) was only 23.5 MPa [58, 60, 62-64, 66, 69]. That is
much lower than the tensile strength of PMMA that is around 65 MPa [73].
Table 2.1 summarizes the bond strengths obtained with different bonding agents between
titanium and poly-methyl methacrylate (PMMA) for dental prostheses. Most bonding methods
reported in the literature require sandblasting the metallic surface; and all of them are based on
molecules containing either silane or phosphonate [18, 57-69]. Sandblasting increases the surface
area of titanium while silane and phosphonate covalently bind the acrylic to the titanium; thus,
increasing the overall bonding strength [56].
In the literature, the bond strengths between titanium and PMMA have been measured with
different mechanical tests including shear bond, four-point bending, and tensile strength tests
[18, 57-69]. However, the strengths reported for each bonding agent depend on the test used.

43
Higher bonding strengths are reported for the four-point bending and shear bond tests (reported
values range between 25.5 to 42.5 MPa and 7.0 to 46.6 MPa, respectively), while the lowest
values are obtained with the most challenging test, i.e. the tensile strength test (0 to 23.5 MPa).
The latter test is the most accurate technique to measure bond strength because it applies a direct
and uniform force to the surface [74]. On the contrary, the shear bond and four-point bend tests
do not distribute stress uniformly on the testing surfaces [48].
Table 2.2 summarizes the literature of the bonding strength of poly-methyl methacrylate with
either cobalt-chromium or stainless steel alloys. All the metallic samples reported in table 2.2
were sandblasting, and the bonding agents were similar to the agents in table 2.1 that are based
on molecules that contain either silane or phosphonate [62, 68, 75-80]. The higher bond strength
reported for cobalt-chromium was 29.1 MPa in the shear bond tests using the bonding agents
META and MATP while the highest bond strengths for the stainless steel in the shear bond tests
were 51.0 and 50.3 MPa using the bonding agents BPDM and MAC [62, 76-80].
2.5.2. Bonding between Wrought Wire and PMMA
Wrought wires are used in many acrylic devices such as dental prostheses and orthodontic
appliances [16]. These wires usually are made of stainless steel or cobalt-chromium alloys that
lack the ability to bind chemically to acrylic [41]. For these reasons, dental devices that combine
wrought wires with acrylic, such as acrylic removable partial dentures, face technical limitations
when not enough volume of acrylic is available to support the wire. Surprisingly, very little
research has been done in order to improve the adhesion between these wires and acrylic.
Therefore it would be of great interest to develop a bonding agent that could increase the
adhesion between wrought wires and acrylic.

44
Table 2.1: The bond strengths between titanium and PMMA (MPa) by using different bonding methods.
Bonding Agent
(Commercial name)
Surface
Topography
Type of PMMA used
(Commercial name)
Testing
Technique
Bond
Strength
(MPa)
Ref.
None Sandblasted Self-cured with EGDMA and TBB
(Super- Bond C&B)
Shear bond 38.1±2.3 [68]
“ “ Heat-cured Tensile strength 20.0 [69]
“ “ “ “ 16.1±1.6 [58]
“ “ “ “ 3.2±0.4 [62]
“ “ Self -cured with BP (Multi- Bond) Shear bond 13.6±1.6 [68]
“ “ Self-cured “ 9.9 [18]
MHPA (AZ Primer) “ “ “ 46.6 [18]
MDP and VTD (Alloy Primer) “ “ “ 45.7 “
“ “ Self-cured with EGDMA and TBB
(Super- Bond C&B)
“ 39.8±2.0 [68]
“ “ Self -cured with BP (Multi- Bond) “ 22.0±6.6 “
“ “ Heat-cured “ 27.5 ±4.0 [57]
“ “ “ Tensile strength 16 .0±3.6 [62]
MDDT and MHPA (Metal Link
Primer )
“ Self-cured Shear bond 45.4 [18]
“ “ Self-cured with EGDMA and TBB
(Super- Bond C&B)
“ 39.6±2.5 [68]
“ “ Self -cured with BP (Multi- Bond) “ 16.5±2.3 “
MATP (Espe-Sil) Polished Heat-cured “ 0.0 [67]
“ Sandblasted “ “ 5.9±2.1 “
MATP “ Self-cured Tensile strength 14.3 [66]
MATP (Silicoater M D) “ “ Shear bond 21.9± 1.7 [59]
MATP and Silicate Coating (Espe-
Sil; Rocatec System)
“ Heat-cured “ 16.2±2.3 [67]
Silicate Coating (Rocatec System) “ Self-cured “ 38.7 [18]
“ “ Heat-cured “ 23.8±1.7 [58]
META “ Heat-cured (Trevalon) Four-point bend 31.9 ±1.5 [65]
“ “ Heat-cured (Metadent) “ 42.5±2.2 “
“ “ Heat-cured Tensile strength 21.0 [69]
META (Super bond) “ “ Shear bond 19.1 ±8.9 [57]
META (New Metacolor) “ Self-cured “ 21.5± 2.2 [59]
MDP (Estenia Opaque Primer) “ “ “ 42.7 [18]
“ “ Heat-cured “ 7.0 ±3.0 [57]
MDP “ “ Tensile strength 23.5 [69]
“ “ Self-cured with EGDMA and TBB
(Super- Bond C&B)
“ 21.2±4.7 [64]
“ “ “ “ 16.2±5.9 [63]
MDP (Cesead ) “ Self-cured Shear bond 19.0± 2.2 [59]
MEPS (Thermoresin) “ “ “ 14.0± 0.6 “
MPS and n-propylamine Polished Heat-cured Four-point bend 25.5±6.4 [61]
MAC (MR Bond) “ “ Tensile strength 7.4 ±2.1 [62]
DOPA “ “ “ 1.8 [60]
Abbreviations: BP: benzoyl peroxide; DOPA;3,4-dihydroxyL-phenylalanine; MAC:11-metacryloyloxyundecan 1,1-dicarboxylic; MATP:
Methacryloxypropyl-trimethoxysilane; MDDA:10-methacyloyloxydecyl 6,8-dithioctanoate; MDP:10-Methacryloyloxydecyl dihydrogen
phosphate; MDDT:10- methacryloxydecly 6,8-dithiooctanoate; MEPS: methacryloxydecly thiophosphate derivative; META: Methacryloxy ethyl trimellitate anhydride; MHPA;6-Methacryloxyethexy phosphonacetate; MPS:3-Methacryloxypropyl trimethoxysilane; TBB:tribuylborane;
VTD:10-Methacryloyloxydecyl dihydrogen phosphate.

45
Table 2.2: The bond strengths (MPa) between PMMA and cobalt –chromium or stainless steel using different bonding
methods.
Abbreviations: AEAPS: N-(2-aminoethyl)-3-aminopropyltrimethoxysilane; AETA: 4-acryloxydecly trimelliate anhydride; BPDM:adduct 2-hydroxyethyl methacrylate and 3,4,4’,5’-biphenyl tetracarboxylic anhydride; DGEBA: diglycidylether of bisphenol; MAC-:11-
metacryloyloxyundecan 1,1-dicarboxylic; MATP: Methacryloxypropyl-trimethoxysilane; MDDT:10- methacryloxydecly 6,8-dithiooctanoate;
MDP:10-Methacryloyloxydecyl dihydrogen phosphate; MEPS: methacryloxydecly thiophosphate derivative; META: Methacryloxy ethyl trimellitate anhydride; MHPA;6-Methacryloxyethexy phosphonacetate; TEOS:tetraethoxysilane; VTD:10-Methacryloyloxydecyl dihydrogen
phosphate.
2.5.3. Bonding between Brackets and Composite
Orthodontic brackets are made of stainless steel, and are bonded to teeth through a composite
adhesive based on polymers such as Bis-GMA, that adhere very well to teeth but very poorly to
metal resulting in bracket debonding [3, 4, 16, 37]. Brackets debonding or bracket loss are more
common in complex orthodontic treatments that require intensive forces applied on severely
crowded or angulated teeth to move them into their correct positions [81, 82]. Therefore,
orthodontic brackets were developed with large bases designed to increase the surface area and
Type of metal Bonding Agent
(commercial name)
Type of PMMA
used
Testing Technique Bond Strength
(MPa)
Ref.
Cobalt –Chromium None Self-cured Tensile strength 6.8 ±2.3 [80]
“ “ Heat-cured “ 3.4±0.6 [62]
MDP and VTD (Alloy Primer) “ “ 17.1±2.6 “
“ “ Self-cured “ 19.2 ±6.0 [80]
“ META (UBar) “ “ 8.6 ±2.7 “
“ META and MATP “ “ 29.1±6.3 [79]
“ MAC (MR Bond) “ “ 25.6 ±6.4 [80]
“ “ Heat-cured “ 17.8±4.0 [62]
Stainless steel None Self-cured “ 20.0 [78]
“ “ “ Shear bond 21.3±2.7 [77]
“ “ “ “ 19.2±3.6 [76]
“ MDP (Estenia Opaque Primer) “ “ 35.4±2.0 “
“ “ “ “ 49.4±1.3 [77]
“ MDP and VTD (Alloy Primer) “ “ 48.8±1.6 “
“ “ “ “ 34.3±1.9 [76]
“ MDDT and MHPA (Metal Link Primer ) “ “ 34.4±1.7 “
“ “ “ “ 48.8±1.4 [77]
“ “ “ Tensile strength 38.3 [78]
“ META (Meta Fast primer) “ “ 36.0 “
“ META (Super bond) “ Shear bond 49.4±1.5 [77]
“ MEPS (Metal primer PII) “ “ 48.1±1.3 “
“ “ “ Tensile strength 31.1 [78]
“ MAC (MR Bond) “ Shear bond 50.3±2.3 [77]
“ AETA (Acryl Bond) “ “ 49.9±1.5 “
“ BPDM (All-Bond 2) “ “ 51.0±0.8 “
“ DGEBA and AEAPS + MATP and TEOS “ “ 9.7 ± 1.5 [75]

46
compensate for the lack of adhesion [14, 16]. The resulting large brackets are more likely to
affect the quality of life of the patients in terms of food impaction and esthetic concerns, whereas
food impaction around and beneath the brackets lead to increased rates of demineralization and
tooth caries [13-16]. Most of the research conducted to increase the adhesion of brackets has
been limited to modifications of the surface pattern of the bracket base in order to increase
micromechanical interlocking that only achieved minor improvements [14]. Accordingly, a
chemical adhesive system that would increase the bond strength between orthodontic brackets
and dental composite would be of great interest because it could prevent brackets loss and result
in a reduction of the size of brackets that translates into less dental problems associated to them.
2.6. Aryldiazonium Salts
Aryldiazonium salts or diazonium compounds are organic compounds that have the molecular
structure R-N2+
which R is Aryl group contains a phenyl group [83]. Diazonium salts can be
prepared by the reaction knows as diazotization or diazotisation [83, 84]. Diazonium was
described in the middle of the 19th
century, and the name diazonium was from French “diazote”
which means two nitrogen atoms [84]. Then, it has been able to generate azo compounds from
diazonium salts that are important coloring materials, and they were recognized by dyes
industries [83, 84]. In the last two decades, aryldiazonium salts have raised interest for
modifying materials surfaces in numerous applications [83, 85-88]. The interest of using
aryldiazonium salts is because their ease of preparation and reduction, strong covalent bonding
between various materials, large choices of functional groups on the compound, and cost [83, 89-
91].
47
2.6.1. Grafting of Diazonium Salts
There are different methods for grafting diazonium salts on various substrates, and the most
common methods are electro-grafting, ultrasonication grafting, heating grafting, photo grafting,
and redox grafting [83, 84, 86, 92]. Initially, diazonium grafting was performed using
electrochemical reduction that occurs by transfer one electron wave (0.02 to 0.56 V) to
aryldiazonium salts in aprotic or acidic mediums [84, 86, 92, 93]. This reduction leads to reduce
aryldiazonium salts generating free radicals that bind on substrate surfaces [84, 92]. Moreover,
grafting aryldiazonium salts has been achieved under ultrasonication in an acidic solution, being
the ultrasonic frequency of 20 KHz the most efficient one for reducing aryldiazonium salts [84,
86, 94]. Heating or microwave heating an acidic solution containing aryldiazonium salts in
presence of sodium nitrate (NaNO2) at temperature of 60 to 80oC has been proven to graft
aryldiazonium salts on different surfaces [84, 86, 95]. Also, it has been shown that it is possible
to graft aryldiazonium salts on various surfaces using UV (ultraviolet) light or mechanical
assistance [83, 86, 96]. Finally, redox grafting is the more recent and simpler than other grafting
methods. In this method, diazonium salts can be grafted using a reducing agent (i.e. iron powder
or hypophosphorous acid) that activate the aryldiazonium salts and form aryl radicals that
covalently bind to different surfaces (Figure 2.11) [84, 86, 92, 97-99].

48
Figure 2.11: Scheme describing grafting of diazonium salts of a substrate: (a) diazotisation of p-phenylenediamine (PPD);
(b) formation of aryl radicals by reducing aryldiazonium using iron powder or hypophosphorous acid; (c) attachment of
aryl radicals to substrates surfaces; (d) growing of diazonium salts as multi-layers.
2.6.2. Diazonium Grafted Layer Properties
One of the most interesting points of diazonium salts is their ability to be reduced and graft
simply and rapidly onto almost any surface, including metals, glass, and carbon. The grafted
layer forms a strong covalent bond to any surfaces that can be used as coupling agents between
different substrates [83, 84, 89, 93, 100-102]. Diazonium structure allows large choices of
functional groups and has two active sites that can be used as a self adhesive layer between
different materials [84, 92]. Moreover, the grafted aryl-layer can be used to improve the physical
and chemical properties of different material surfaces [84, 86, 89, 102].

49
The grafted layer obtained with diazonium salts has been proved to be stable for at least 6
months in harsh conditions including ultrasonication and heating. It was also found that these
grafted layers are partially stable after removing or scratching by electrical or mechanical
methods [84]. The covalent bond formed between diazonium layers and substrates has been
previously observed by XPS (X-ray photoelectron spectroscopy), Raman, AFM (atomic force
microscopy), ToF-SIMS (time-of-flight secondary ion mass spectrometry), and with DFT
(density functional theory) [83, 84, 91, 100, 103].
The grafted layer is usually formed as a multi-layers rather than mono-layer [84]. The multi-
layers occur because the free radicals generated from the reduction can also react with the first
grafted layer and form other layer on it (Figure 2.11.d). The grafted layers grow until electrons
are unable to be transferred through the grafted layers and stop the reaction [84]. Grafted layers
are not homogenous, and their thickness can range from few nanometers to one micron [83, 84].
The thickness depended on the amount of aryldiazonium salts and type of substrates that
aryldiazonium salts graft to it. However, the thickness of grafted layers on metals surfaces is
usually found to be 2-6 nm [83, 84, 87, 104, 105].
2.6.3. Applications of Aryldiazonium Salts
Surface modification with aryldiazonium salts have been used for multiple applications, such as
corrosion resistance, abrasion resistance, and electrical insulation, in many biomedical,
environmental, and industrial applications [84]. There are more than 100 patents on
aryldiazonium salts in these applications, and many of these patents are base on the use of
diazonium salts as coupling agents between different material surfaces [83, 84, 86]. Diazonium
salts were used in many industrial applications, such as inkjet ink and fuel cells [83, 84]. Carbon

50
blocks treated with diazonium result in useful elastomers with high abrasion resistance that can
be used with tires to reduce fuel consumption [84]. Diazonium salts were used in the biomedical
filed for drug delivery and modifying surgical stents [83, 84]. They were used also in biosensors,
functional polymer coatings, protein arrays, molecular electronic junctions [83, 84, 86, 106-108].
2.6.4. Aryldiazonium Salts as Dental Adhesive
Aryldiazonium salts have not been used in dentistry; however, they would be of great interest
due to their ability to act as coupling agent between metals and polymers for dental applications.
Aryl diazonium salts have more attracting properties and features than other available dental
adhesives. First, aryl diazonium salt can react rapidly with surfaces, produce a very active
radical, and give strong adhesion on any surfaces (i.e. noble metals, base metals, ceramics,
polymers, and composites) [83, 89]. Therefore, dental adhesives based on aryldiazonium salts
could works with any type of materials as a multi-purpose adhesive.
The thickness of the diazonium layer is less than 1 µm that is another advantage of this dental
adhesive because it will help to reduce the thickness and weight of dental prostheses [84].
Another advantage of using aryl diazonium as dental adhesive is the cost which would be
reasonable since the raw materials to produce this adhesive are commercially available at a low
cost [84].
2.6.5. Diazonium Grafted Layers Analysis
Several methods can be used to characterize aryl diazonium layer such as X-ray photoelectron
spectroscopy (XPS), Raman spectroscopy, IR-ellipsometry, and contact angle measurements.
However, the best way to assess diazonium grafted layers on metallic surface is by XPS (X-ray
51
photoelectron spectroscopy) because of its unique ability to characterize external thin chemical
coating [83, 84, 91, 100, 103].
2.6.5.1. X-ray Photoelectron Spectrometer (XPS)
X-ray photoelectron spectroscopy (XPS) is the most commonly used method for surface analysis
because it is commercially available and provides clear information on surface chemical
composition [109]. This technique was called ESCA (electron spectroscopy for chemical
analysis) but it changed because there are many surface-electron spectroscopy techniques and the
name for each technique should be precise [109]. XPS is a sensitive technique that provides
quantitative information on the elemental and chemical composition of the outermost 10 nm or
less of n the solid surface [109-112]. XPS can detect all elements in the periodic table except
hydrogen and helium [109, 111].
The surface to be analyzed with XPS is irradiated with X-ray source that penetrates the surface
for a depth ~1 micrometer and emits electrons (photoelectron) which have a binding energy less
than the X-ray energy [109, 110]. The electron analyser determines the binding energy (Eb) of
the photoelectron. The photoelectron kinetic energy (Ek) can be determined through an equation
(Ek=hv-Eb) using the binding energy (Eb) and the energy of the incident radiation (hv) [109-111].
The resulting binding energies are unique from different atoms that show on XPS spectrum as
peaks [109]. The elemental identity, quantity of an element, and chemical state are also
determined.
The main components of XPS (Figure 2.12) are an X-ray source, an ultra-high vacuum (UHV),
and an electron-energy analyzer [109]. Al Kα or Mg Kα X-ray sources are the most common

52
ones because the width and line energy for Al Kα or Mg Kα are suitable for XPS [109, 110].
XPS is a very sensitive technique; therefore, it requires vacuums of the order of 10-8
Pa or lower
to protect samples from surface contamination [109]. The electron-energy analyzer is used to
analyze the energies of electrons ejected from samples which will be quantified in a detector
system (Figure 2.12).
Figure 2.12: Diagram describing X-ray photoelectron spectroscopy (XPS) components.
XPS general survey is a scan that covers the entire binding energy (0 to 1000 eV) of a surface at
low energy resolution that can be used to identify the elements and the quantity of each atoms on
the surface [109, 110]. Moreover, high resolution XPS spectra can be obtained for each element
(i.e. C1s and O 1s) in specific regions to provide specific chemical bonding information [109,
110].
In the first study of this thesis, aryl diazonium layer was analyzed by a monochromatic X-ray
photoelectron spectrometer K Alpha (Thermo Fischer Scientific Inc, East Grinstead, UK). XPS

53
was used for determining the relative quantities and chemical environments of the elements on
the Ti and surfaces. Control and treated Ti samples were carefully cleaned in an ultrasonic bath
with acetone, ethanol, and distilled water for 5 minutes, and they were stored in contamination
free tubes for less than 24 hours before XPS analysis. The setup was equipped with an Al Kα X-
Ray radiation source (1486.6 eV, 0.834 nm), a micro-focused monochromator and an ultrahigh
vacuum chamber (10-9
torr). Survey scans were obtained over the range of 0-1350 eV with pass
energy of 200 eV at a step of 1.0 eV, and high resolution scans were collected with pass energy
of 50 eV at a step of 0.1 eV. Energies were calibrated by setting the binding energy of the carbon
bonded to hydrogen or carbon (C-(H, C)) at 285.0 eV on all samples. Data analysis and peak
fitting were performed using Avantage (5.41v, Thermo Fischer Scientific Inc, East Grinstead,
UK) chemical surface analysis software.
In the second study of the thesis, the aryl diazonium layer was analyzed similarly to the first
study, but it was done with a different XPS model (VG Scientific ESCLAB 3 MIKII). XPS was
used for determining the relative quantities and chemical environments of the elements on the
stainless steel brackets surfaces. The XPS in the second study was equipped with Mg Kα X-Ray
radiation source (1253.6 eV), a micro-focused monochromator and an ultrahigh vacuum chamber
(10-9
torr). Survey scans for all samples were obtained over the range of 0-1350 eV with pass
energy of 100 eV at a step of 1.0 eV. The high resolution scans were collected with pass energy
of 20 eV at a step of 0.05 eV. All spectra were referenced to C-C/C-H of the C 1s spectrum at
285.0 eV.

54
2.6.5.2. Contact Angle Measurements
Contact angle measurement is used to quantify the angle formed by a liquid drop at a solid
surface. Contact angles measurements are useful to understand the wettability and hydrophobicity
of a solid surface because they are sensitive to the first layers of the materials surfaces and the
technique is easy to apply [84]. Therefore, contact angles measurement is a helpful technique to
analyze the grafted diazonium layers on different surfaces.
In this thesis, the contact angle measurements was recorded and analyzed at room temperature on
contact angle meter (OAC 15, Data Physics, Germany). Experimentally, a liquid drop of distilled
water (2ml) was deposited on the Ti surfaces of each samples (control and treated) and the angles
between the drop and surfaces was measured. The static contact angle was automatically
calculated and the side view images were captured. From the contact angle measurements results,
it would be easy to distinguish the properties of first layer of different Ti surfaces that are related
to hydrophobicity of surface [84].
55
Chapter 3: Hypothesis and Objective
3.1. Hypothesis
Aryldiazonium salts could be used to improve the binding between metals and polymers used in
dental applications.
3.2. Thesis Objective
The objective of this study was to develop a new method of creating a strong chemical bond
between alloys and polymers for dental devices based on diazonium chemistry. The objective of
the thesis consists of the two specific objectives addressed in two separate manuscripts that were
divided based on their application in dentistry. Manuscript I assesses the bonding between metals
and PMMA for dental prostheses while Manuscript II investigates the bonding between metals
and Bis-GMA for orthodontic appliances.
56
Chapter 4: List of References
1. Wiskott, H.W.A., Fixed prosthodontics : principles and clinics2011, London; Chicago:
Quintessence Publishing.
2. Türp, J., C. Greene, and J. Strub, Dental occlusion: a critical reflection on past, present
and future concepts. Journal of Oral Rehabilitation, 2008. 35(6): p. 446-453.
3. Gill, D.S.N.F.B. Orthodontics principles and practice. 2011.
4. Christensen, G.J. A consumer's guide to dentistry. 2002.
5. Carr, A.B. and D.T. Brown, Chapter 5 - Major and Minor Connectors, in McCracken's
Removable Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 29-55.
6. Chapter 8 - Esthetic Dentistry: Cosmetic Dentistry; Improving Your Smile, in A
Consumer's Guide to Dentistry (Second Edition)2002, Mosby: Burlington. p. 45-56.
7. Freedman, G.A. and ScienceDirect. Contemporary esthetic dentistry. 2012.
8. Phoenix, R.D., et al. Stewart's clinical removable partial prosthodontics. 2008.
9. Carr, A.B. and D.T. Brown, Chaper 2 - Considerations for Managing Partial Tooth Loss:
Tooth Replacements From the Patient Perspective, in McCracken's Removable Partial
Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 8-15.
10. Palmer, R.M. and L.C. Howe. Implants in Clinical Dentistry. 2011.
11. Craig, R.G., J.M. Powers, and R.L. Sakaguchi, Craig's restorative dental materials2006,
St. Louis, Mo.: Mosby Elsevier.
12. Vallittu, P.K., A Review of Methods Used to Reinforce Polymethyl Methacrylate Resin.
Journal of Prosthodontics, 1995. 4(3): p. 183-187.
13. Horiuch, S., et al., Enamel bonding of self-etching and phosphoric acid-etching
orthodontic adhesives in simulated clinical conditions: Debonding force and enamel
surface. Dental Materials Journal, 2009. 28(4): p. 419-425.
14. Bishara, S.E., et al., The effect of repeated bonding on the shear bond strength of a
composite resin orthodontic adhesive. The Angle Orthodontist, 2000. 70(6): p. 435-443.
15. Årtun, J. and S. Bergland, Clinical trials with crystal growth conditioning as an
alternative to acid-etch enamel pretreatment. American Journal of Orthodontics, 1984.
85(4): p. 333-340.
16. Brantley, W.A. and T. Eliades. Orthodontic materials scientific and clinical aspects.
2001.
17. Sharma-Sayal, S.K., et al., The influence of orthodontic bracket base design on shear
bond strength. American Journal of Orthodontics and Dentofacial Orthopedics, 2003.
124(1): p. 74-82.
18. Matsuda, Y., et al., Bond Strength of Poly(methyl methacrylate) Denture Base Material
to Cast Titanium and Cobalt-Chromium Alloy. Journal of Adhesive Dentistry, 2010.
12(3): p. 223-229.
19. Jagger, D., A. Harrison, and K. Jandt, The reinforcement of dentures. Journal of Oral
Rehabilitation, 1999. 26(3): p. 185-194.
20. Rothfuss, L.G., et al., Resin to metal bond strengths using two commercial systems. The
Journal of Prosthetic Dentistry, 1998. 79(3): p. 270-272.

57
21. Cooper, L.F., B.M. Limmer, and W.D. Gates, “Rules of 10”—Guidelines for Successful
Planning and Treatment of Mandibular Edentulism Using Dental Implants. Compendium
of continuing education in dentistry (Jamesburg, NJ: 1995), 2012. 33(5): p. 328.
22. Ebnesajjad, S. Handbook of adhesives and surface preparation technology, applications
and manufacturing. 2011.
23. Minami, H. and T. Tanaka, History and current state of metal adhesion systems used in
prosthesis fabrication and placement. Journal of Oral Science, 2013. 55(1): p. 1-7.
24. Ikemura, K. and T. Endo, A review of our development of dental adhesives-Effects of
radical polymerization initiators and adhesive monomers on adhesion. Dental Materials
Journal, 2010. 29(2): p. 109-121.
25. Emami, E., et al., The Impact of Edentulism on Oral and General Health. International
Journal of Dentistry, 2013. 2013.
26. Massad, J., Chapter 24 - Complete Denture Esthetics, in Contemporary Esthetic
Dentistry2012, Mosby: Saint Louis. p. 560-574.
27. Carr, A.B. and D.T. Brown, CHAPTER 1 - Partially Edentulous Epidemiology,
Physiology, and Terminology, in McCracken's Removable Partial Prosthodontics
(Twelfth Edition)2011, Mosby: Saint Louis. p. 2-7.
28. Smith, B.G.N.H.L.C. Planning and making crowns and bridges. 2007.
29. Weiss, C. and A. Weiss. Principles and practice of implant dentistry. 2001.
30. Sullivan, R.M., Implant dentistry and the concept of osseointegration: a historical
perspective. CDA Journal, 2001. 2911: p. 737-745.
31. Palmer, R.M., et al., Implants in clinical dentistry2002: Taylor & Francis.
32. Carr, A.B. and D.T. Brown, Chapter 3 - Classification of Partially Edentulous Arches, in
McCracken's Removable Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint
Louis. p. 16-20.
33. Carr, A.B. and D.T. Brown, Chapter 7 - Direct Retainers, in McCracken's Removable
Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 67-95.
34. Carr, A.B. and D.T. Brown, Chapter 8 - Indirect Retainers, in McCracken's Removable
Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 96-102.
35. Carr, A.B. and D.T. Brown, Chapter 6 - Rests and Rest Seats, in McCracken's Removable
Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 56-66.
36. Carr, A.B. and D.T. Brown, Chapter 9 - Denture Base Considerations, in McCracken's
Removable Partial Prosthodontics (Twelfth Edition)2011, Mosby: Saint Louis. p. 103-
114.
37. Melsen, B. Adult orthodontics. 2012.
38. Iizuka, Y., et al., Bond strength of an orthodontic bonding material and adhesion energy
of artificial saliva to an experimental titanium bracket. Orthodontic Waves, 2011. 70(1):
p. 21-26.
39. Bishara, S.E., et al., Effect of time on the shear bond strength of glass ionomer and
composite orthodontic adhesives. American Journal of Orthodontics and Dentofacial
Orthopedics, 1999. 116(6): p. 616-620.
40. Luther, F.N.-M.Z. Removable orthodontic appliances and retainers principles of design
and use. 2013.
41. Sakaguchi, R.L. and J.M. Powers. Craig's restorative dental materials. 2012.
42. Narayan, R., Biomedical materials, 2009, Springer: New York.

58
43. Liu, X., et al., Plasma surface modification of titanium for hard tissue replacements.
Surface and Coatings Technology, 2004. 186(1): p. 227-233.
44. Wen, C., et al., Processing and mechanical properties of autogenous titanium implant
materials. Journal of Materials Science: Materials in Medicine, 2002. 13(4): p. 397-401.
45. Paital, S.R. and N.B. Dahotre, Calcium phosphate coatings for bio-implant applications:
Materials, performance factors, and methodologies. Materials Science and Engineering:
R: Reports, 2009. 66(1): p. 1-70.
46. O'Brien, W.J. Dental materials and their selection. 2008.
47. Dental Materials and Their Selection. 4 ed, ed. P.F. William J. O'Brien2008, Hanover
Park, IL: Quintessence Publishing Co, Inc.
48. Vuorinen, A.M., et al., Bonding of BisGMA–TEGDMA-Resin to Bulk Poly
(Paraphenylene) Based Rigid Rod Polymer. Composite Interfaces, 2011. 18(5): p. 387-
398.
49. Usanmaz, A., J. Ateş, and A. Doğan, Thermal and mechanical properties of
microwave‐and heat‐cured poly (methyl methacrylate) used as dental base material.
Journal of Applied Polymer Science, 2003. 90(1): p. 251-256.
50. Rupali Gautam, R.D.S., Vinod P. Sharma, Ramashanker Siddhartha, and R.K. Pooran
Chand, Biocompatibility of polymethylmethacrylate resins used in dentistry. Wiley
Periodicals, 2012.
51. Rahul Bhola, S.M.B., Hongjun Liang, Brajendra Mishra, Biocompatible Denture
Polymers – A Review. Trends Biomater, 2010. 23(3): p. 129-136.
52. Deb, S., Polymers in dentistry. Proceedings of the Institution of Mechanical Engineers,
Part H: Journal of Engineering in Medicine, 1998. 212(6): p. 453-464.
53. Blatz, M.B., A. Sadan, and M. Kern, Resin-ceramic bonding: A review of the literature.
The Journal of Prosthetic Dentistry, 2003. 89(3): p. 268-274.
54. Chapter 13 - Materials for Adhesion and Luting, in Craig's Restorative Dental Materials
(Thirteenth Edition)2012, Mosby: Saint Louis. p. 327-347.
55. Wendl, B., et al., Comparative bond strength of new and reconditioned brackets and
assessment of residual adhesive by light and electron microscopy. The European Journal
of Orthodontics, 2011. 33(3): p. 288-292.
56. Le Guéhennec, L., et al., Surface treatments of titanium dental implants for rapid
osseointegration. Dental Materials, 2007. 23(7): p. 844-854.
57. Kawaguchi, T., et al., Effect of surface preparation on the bond strength of heat-
polymerized denture base resin to commercially pure titanium and cobalt-chromium
alloy. Dental Materials Journal, 2011. 30(2): p. 143-150.
58. May, K.B., et al., Silane to enhance the bond between polymethyl methacrylate and
titanium. Journal of Prosthetic Dentistry, 1995. 73(5): p. 428-431.
59. Fujishima, A., Y. Fujishima, and J.L. Ferracane, Shear bond strength of 4 commerical
bonding system to cp ti. Dental Materials, 1995. 11(2): p. 82-86.
60. Hamming, L.M., et al., Mimicking mussel adhesion to improve interfacial properties in
composites. Composites Science and Technology, 2008. 68(9): p. 2042-2048.
61. Ekstrand, K., I.E. Ruyter, and H. Oysaed, Adhesion to titanium of methacrylate-based
polymer materials. Dental Materials, 1988. 4(3): p. 111-115.
62. Kim, S.-S., et al., Effect of adhesive primers on bonding strength of heat cure denture
base resin to cast titanium and cobalt-chromium alloy. The Journal of Advanced
Prosthodontics, 2009. 1(1): p. 41-6.

59
63. Kwon, T.-Y. and Y. Imai, Influence of molecular weight of PMMA in PMMA/MMA-
TBB resin on durability of adhesion to titanium against thermal stress in water. Dental
Materials Journal, 2006. 25(2): p. 291-297.
64. Imai, Y. and Y. Ikeda, Effect of adding ethylene glycol dimethacrylate to resin cements:
durability against thermal stress of adhesion to titanium. Dental Materials Journal, 1997.
16(1): p. 74-7.
65. Mudford, L., R.V. Curtis, and J.D. Walter, An investigation of debonding between heat
cured PMMA and titanium alloy (Ti-6Al-4V). Journal of Dentistry, 1997. 25(5): p. 415-
421.
66. Gbureck, U., et al., Modified PMMA cements for a hydrolysis resistant metal-polymer
interface in orthopaedic applications. Acta Biomaterialia, 2005. 1(6): p. 671-676.
67. Segerstrom, S. and I.E. Ruyter, Adhesion properties in systems of laminated pigmented
polymers, carbon-graphite fiber composite framework and titanium surfaces in implant
suprastructures. Dental Materials, 2009. 25(9): p. 1169-1177.
68. Koizumi, H., et al., Bond strength to primed Ti-6Al-7Nb alloy of two acrylic resin
adhesives. Dental Materials Journal, 2006. 25(2): p. 286-290.
69. Tsuchimoto, Y., et al., Effect of 4-MET- and 10-MDP-based primers on resin bonding to
titanium. Dental Materials Journal, 2006. 25(1): p. 120-124.
70. Ikemura, K., et al., Effect of the combination of dithiooctanoate monomers and acidic
adhesive monomers on adhesion to precious metals, precious metal alloys and non-
precious metal alloys. Dental Materials Journal, 2011. 30(4): p. 469-477.
71. Matinlinna, J., L. Lassila, and P. Vallittu, Evaluation of five dental silanes on bonding a
luting cement onto silica-coated titanium. Journal of Dentistry, 2006. 34(9): p. 721-726.
72. Lung, C.Y.K. and J.P. Matinlinna, Aspects of silane coupling agents and surface
conditioning in dentistry: An overview. Dental Materials, 2012. 28(5): p. 467-477.
73. Sperling, L.H., Mechanical Behavior of Polymers, in Introduction to Physical Polymer
Science2005, John Wiley & Sons, Inc. p. 557-612.
74. Van Meerbeek, B., et al., Relationship between bond-strength tests and clinical outcomes.
Dental Materials, 2010. 26(2): p. e100-e121.
75. Pellice, S.A., D.P. Fasce, and R.J.J. Williams, Development of a bilayer coating to
improve the adhesion between stainless steel and in situ-polymerized poly(methyl
methacrylate). Journal of Applied Polymer Science, 2007. 105(4): p. 2351-2356.
76. Ishikawa, Y., et al., Effects of alumina air-abrasion and acidic priming agents on bonding
between SUS XM27 steel and auto-polymerizing acrylic resin. Journal of Oral Science,
2007. 49(3): p. 191-5.
77. Mikami, A., Comparative evaluation of metal priming agents applied for bonding of
magnetic stainless steel with acrylic repair resin. Journal of Oral Science, 2007. 49(4): p.
277-81.
78. Chen, J., et al., Effect of surface treatment with commercial primers on tensile bond
strength of auto-polymerizing resin to magnetic stainless steel. Int Chin J Dent, 2005. 5:
p. 7-11.
79. Kurata, S. and K. Umemoto, Synthesis of new silane coupling agents with a trimellitic
anhydride group and application as primers for ceramics and alloys. Dental Materials
Journal, 2007. 26(6): p. 800-804.

60
80. Banerjee, S., et al., In vitro tensile bond strength of denture repair acrylic resins to primed
base metal alloys using two different processing techniques. Journal of Prosthodontics,
2009. 18(8): p. 676-683.
81. Nanda, R.K.S. Current therapy in orthodontics. 2010.
82. Nanda, R. and M. Upadhyay, Sheldon Friel Lecture 2011Skeletal and dental
considerations in orthodontic treatment mechanics: a contemporary view. The European
Journal of Orthodontics, 2012.
83. Mahouche-Chergui, S., et al., Aryl diazonium salts: a new class of coupling agents for
bonding polymers, biomacromolecules and nanoparticles to surfaces. Chemical Society
Reviews, 2011. 40(7): p. 4143-4166.
84. Chehimi, M.M.W.I. Aryl diazonium salts new coupling agents in polymer and surface
science. 2012.
85. Mevellec, V., et al., Grafting polymers on surfaces: A new powerful and versatile
diazonium salt-based one-step process in aqueous media. Chemistry of Materials, 2007.
19(25): p. 6323-6330.
86. Gam-Derouich, S., et al., Diazonium Salt-Derived 4-(Dimethylamino) phenyl Groups as
Hydrogen Donors in Surface-Confined Radical Photopolymerization for Bioactive Poly
(2-hydroxyethyl methacrylate) Grafts. Langmuir, 2012. 28(21): p. 8035-8045.
87. Pinson, J. and F. Podvorica, Attachment of organic layers to conductive or
semiconductive surfaces by reduction of diazonium salts. Chemical Society Reviews,
2005. 34(5): p. 429-439.
88. Belanger, D. and J. Pinson, Electrografting: a powerful method for surface modification.
Chemical Society Reviews, 2011. 40(7): p. 3995-4048.
89. Salmi, Z., et al., On the interfacial chemistry of aryl diazonium compounds in polymer
science. Chemical Papers, 2012. 66(5): p. 369-391.
90. Jiang, D.E., B.G. Sumpter, and S. Dai, Structure and bonding between an aryl group and
metal surfaces. Journal of the American Chemical Society, 2006. 128(18): p. 6030-6031.
91. Boukerma, K., et al., X-ray photoelectron spectroscopy evidence for the covalent bond
between an iron surface and aryl groups attached by the electrochemical reduction of
diazonium salts. Langmuir, 2003. 19(15): p. 6333-6335.
92. Viel, P., et al., Covalent grafting onto self-adhesive surfaces based on aryldiazonium salt
seed layers. Journal of Materials Chemistry, 2008. 18(48): p. 5913-5920.
93. Delamar, M., et al., Covalent modification of carbon surfaces by grafting of
functionalized aryl radicals produced from electrochemical reduction of diazonium salts.
Journal of the American Chemical Society, 1992. 114(14): p. 5883-5884.
94. Mangeney, C., et al., Electroless ultrasonic functional ization of diamond nanoparticles
using aryl diazonium salts. Diamond and Related Materials, 2008. 17(11): p. 1881-1887.
95. Liu, J., et al., Microwave-assisted functionalization of single-wall carbon nanotubes
through diazonium. Journal of Nanoscience and Nanotechnology, 2007. 7(10): p. 3519-
3523.
96. Pan, Y., et al., Fabrication, Characterization, and Optoelectronic Properties of Layer-by-
Layer Films Based on Terpyridine-Modified MWCNTs and Ruthenium(III) Ions. Journal
of Physical Chemistry C, 2010. 114(17): p. 8040-8047.
97. Combellas, C., et al., Spontaneous grafting of iron surfaces by reduction of
aryldiazonium salts in acidic or neutral aqueous solution. Application to the protection of
iron against corrosion. Chemistry of Materials, 2005. 17(15): p. 3968-3975.

61
98. Pinson, J., Attachment of Organic Layers to Materials Surfaces by Reduction of
Diazonium Salts, in Aryl Diazonium Salts2012, Wiley-VCH Verlag GmbH & Co.
KGaA. p. 1-35.
99. Ghodbane, O., G. Chamoulaud, and D. Belanger, Chemical reactivity of 4-bromophenyl
modified glassy carbon electrode. Electrochemistry Communications, 2004. 6(3): p. 254-
258.
100. Adenier, A., et al., Study of the spontaneous formation of organic layers on carbon and
metal surfaces from diazonium salts. Surface Science, 2006. 600(21): p. 4801-4812.
101. Hinge, M., et al., On the electrografting of stainless steel from para-substituted
aryldiazonium salts and the thermal stability of the grafted layer. Surface and Coatings
Technology, 2010. 205(3): p. 820-827.
102. Gam-Derouich, S., et al., A versatile route for surface modification of carbon, metals and
semi-conductors by diazonium salt-initiated photopolymerization. Surface Science, 2011.
605(21): p. 1889-1899.
103. Doppelt, P., et al., Surface modification of conducting substrates. Existence of azo bonds
in the structure of organic layers obtained from diazonium salts. Chemistry of Materials,
2007. 19(18): p. 4570-4575.
104. Bernard, M.C., et al., Organic layers bonded to industrial, coinage, and noble metals
through electrochemical reduction of aryldiazonium salts. Chemistry of Materials, 2003.
15(18): p. 3450-3462.
105. Sun, G., et al., Infrared spectroscopic ellipsometry (IRSE) and X-ray photoelectron
spectroscopy (XPS) monitoring the preparation of maleimide-functionalized surfaces:
from Au towards Si (111). Surface and Interface Analysis, 2011. 43(9): p. 1203-1210.
106. Bergren, A.J., et al., Molecular electronics using diazonium-derived adlayers on carbon
with Cu top contacts: critical analysis of metal oxides and filaments. Journal of Physics-
Condensed Matter, 2008. 20(37).
107. Corgier, B.P., C.A. Marquette, and L.J. Blum, Diazonium-protein adducts for graphite
electrode microarrays modification: Direct and addressed electrochemical
immobilization. Journal of the American Chemical Society, 2005. 127(51): p. 18328-
18332.
108. Liu, G., M.N. Paddon-Row, and J.J. Gooding, Protein modulation of electrochemical
signals: application to immunobiosensing. Chemical Communications, 2008(33): p.
3870-3872.
109. Bubert, H.J.H., Surface and thin film analysis : principles, instrumentation,
applications2002, Weinheim: Wiley-VCH.
110. Venezia, A.M., X-ray photoelectron spectroscopy (XPS) for catalysts characterization.
Catalysis Today, 2003. 77(4): p. 359-370.
111. Feldman, L.C. and J.W. Mayer, Fundamentals of surface and thin film analysis. Vol. 119.
1986: North-Holland New York.
112. Van der Heide, P.W.I. X-ray photoelectron spectroscopy an introduction to principles and
practices. 2012.

62
Chapter 5: Manuscript I
Bonding Metals to Poly-Methyl Methacrylate Using Aryldiazonium Salts
Omar Alageel a, Mohamed-Nur Abdallah
a, Zhong Yuan Luo
b, Marta Cerruti
b, Faleh Tamimi
a
a Faculty of Dentistry, McGill University, Montreal, QC, Canada
b Department of Mining and Materials Engineering, McGill University, Montreal, QC, Canada
5.1 Abstract
Many dental devices, such as partial dentures, combine acrylic and metallic parts that are bonded
together. These devices often present catastrophic mechanical failures due to weak bonding
between their acrylic and metallic components. The bonding between alloys and polymers (e.g.
poly-methyl methacrylate, PMMA) usually is just a mechanical interlock, since they do not
chemically bond spontaneously. The objective of this study was to develop a new method to
make a strong chemical bond between alloys and polymers for dental prostheses based on
diazonium chemistry. The method was based on two steps. In the first step (primer),
aryldiazonium salts were grafted onto the metallic surfaces. The second step (adhesive) was
optimized to achieve covalent binding between the grafted layer and PMMA. The chemical
composition of the treated surfaces was analyzed with X-ray photoelectron spectroscopy (XPS),
and the tensile bonding strength between metals and poly-methyl methacrylate was measured.
XPS and contact angle measurements confirmed the presence of a polymer coating on the treated
metallic surfaces. Mechanical tests showed a significant increase in bond strength between

63
PMMA and treated titanium or stainless steel wire by 5.2 and 2.5 folds, respectively, compared
to the untreated control group (P<0.05). Thus, diazonium chemistry is an effective technique for
achieving a strong chemical bond between alloys and PMMA, which can help improve the
mechanical properties of dental devices.
Keywords
Dental prosthesis; bonding diazonium; poly-methyl methacrylate; titanium; stainless steel
5.2. Introduction
Chemical bonding between alloys and polymers does not occur spontaneously; in fact, composite
materials that combine polymers with alloys often suffer from mechanical failure at the interface
between them. One example of this challenge is dental devices, which often present catastrophic
mechanical failures due to weak bonding between their metallic and polymeric components [1-
3]. These devices include dental prostheses, combining metallic frameworks and wrought wires
with acrylic resin; and orthodontic appliances, combining acrylic resin with stainless steel
wrought wires.
Poly-methyl methacrylate (PMMA) is extensively used in denture materials for dental prostheses
and orthodontic devices because of its biocompatibility, excellent esthetic, and mechanical
properties [4]. Titanium (Ti) is increasingly used in dental implants, implant abutments, and
milled prostheses because of its excellent mechanical properties (i.e. strength to weight ratio) and
biocompatibility [5]. PMMA and Ti in dental prostheses are usually bonded by mechanical
interlocking the PMMA into the irregularities of the Ti surface [2, 6, 7]. Further improvement in
the bonding strength between Ti and PMMA is still needed to prevent debonding, which are
64
otherwise common in clinical practice, and reduce microleaks at the Ti/PMMA interface that
causes accumulation of oral debris and discoloration of denture base materials [1, 2, 8]. Ti-
PMMA bond can be strengthened by adding a chemical link between PMMA and Ti, since Ti
and PMMA do not chemically bind together spontaneously [1, 7, 9-13].
Several methods have been tested to increase the bond strength between polymers and alloys in
dental prostheses [1, 9, 12, 14-24]. Table 5.1 summarizes the strengths obtained by binding
PMMA and Ti with different methods, measured with shear bond, four-point bending, and
tensile strength tests. In general, higher bond strengths are reported for the four-point bending
and the shear bond tests (values ranging between 25.5 to 42.5 MPa and 7.0 to 46.6 MPa,
respectively), while the lowest values are obtained with the tensile strength test (0 to 23.5 MPa).
Indeed, the latter test is the most challenging one; however, it is also the most accurate technique
to measure bond strength because it applies a direct and uniform force to the surface [25]. On the
contrary, the shear bond and four-point bend tests do not distribute stress uniformly on the
surfaces being tested [26].
Most of the methods reported in Table 5.1 require sandblasting the metallic surface, and all of
them use either silane or phosphonate groups to create a chemical bond between the two surfaces
[1, 9, 12, 14-24]. Silanes and phosphonates covalently bind to Ti, while sandblasting increases
the surface area of the exposed Ti, thus increasing the overall bonding strength [27]. The highest
bond strengths reported were achieved using phosphonate-based adhesives (MHPA, MDP and
VDT; see Table 5.1) in combination with sandblasting. Specifically, the highest tensile strength
reported without sandblasting was 7.4 MPa [12], while using a combination of sandblasting and
bonding agents the tensile strength went up to 23.5 MPa [12, 15, 17, 19-21, 24]. These values are

65
still too low for dental applications. Overdentures, for example, have to resist biting forces of up
to 662.2 N, and pressures of up to 51.1MPa [28]. This implies that masticatory forces can exceed
the strength of the Ti-PMMA bond and lead to prosthesis failure. An ideal goal would be to have
a metal/PMMA interface that is at least as strong as PMMA alone, which has a tensile strength of
65 MPa [29].
Another example of metal-acrylic interface found in dental applications is that between wrought
wires and acrylic-based dental devices such as dental prostheses and orthodontic appliances [30].
Wrought wires are usually made of stainless steel or cobalt-chromium alloys, which both lack
the ability to bind chemically to acrylic resins [31]. To overcome this problem, dental devices
combining wrought wires with acrylic such as acrylic removable partial dentures cannot be made
when not enough volume of acrylic is available to support the wire. Surprisingly, hardly anyone
has looked into improving the adhesion between wrought wires and acrylic.
In this paper we will show a technique to improve the binding between PMMA and alloys used
in dental applications based on diazonium chemistry. Aryldiazonium salts have been used to
modify material surfaces for many applications [32, 33]. Diazonium ions can be produced from
aromatic amines and grafted onto almost any surface, including metals, glass, and carbon [34-
37]. Initially, diazonium grafting was performed using electrochemical reduction, but recently
this has been achieved using chemical reducing agents in acidic solutions [38]. The reducing
agents transform the aryldiazonium salts into aryl radicals, which can covalently bind to the
surface of interest [39, 40]. If an extra amino group is present on the aryldiazonium precursor, a
polyaminophenylene (PAP) layer is formed on the metallic surface. The amino groups sticking
out from the PAP layer can be further activated in a second step, and used to bind a second layer

66
onto the original surface [39, 41]. In this work, we optimize such second step to bind PMMA
and metals for dental applications.
Table 5.3: The bond strengths between titanium and PMMA (MPa) using different bonding methods.
Bonding Agent
(Commercial name)
Surface Topography Type of PMMA used
(Commercial name)
Testing
Technique
Bond
Strength
(MPa)
Ref.
None Sandblasted Self-cured with EGDMA and
TBB (Super- Bond C&B)
Shear bond 38.1±2.3 [23]
“ “ Heat-cured Tensile strength 20.0 [24]
“ “ “ “ 16.1±1.6 [15]
“ “ “ “ 3.2±0.4 [12]
“ “ Self -cured with BP (Multi- Bond) Shear bond 13.6±1.6 [23]
“ “ Self-cured “ 9.9 [1]
MHPA (AZ Primer) “ “ “ 46.6 “
MDP and VTD (Alloy Primer) “ “ “ 45.7 “
“ “ Self-cured with EGDMA and
TBB (Super- Bond C&B)
“ 39.8±2.0 [23]
“ “ Self -cured with BP (Multi- Bond) “ 22.0±6.6 “
“ “ Heat-cured “ 27.5 ±4.0 [14]
“ “ “ Tensile strength 16 .0±3.6 [12]
MDDT and MHPA (Metal Link
Primer )
“ Self-cured Shear bond 45.4 [1]
“ “ Self-cured with EGDMA and
TBB (Super- Bond C&B)
“ 39.6±2.5 [23]
“ “ Self -cured with BP (Multi- Bond) “ 16.5±2.3 “
MATP (Espe-Sil) Polished Heat-cured “ 0.0 [22]
“ Sandblasted “ “ 5.9±2.1 “
MATP “ Self-cured Tensile strength 14.3 [21]
MATP (Silicoater M D) “ “ Shear bond 21.9± 1.7 [16]
MATP and Silicate Coating (Espe-
Sil; Rocatec System)
“ Heat-cured “ 16.2±2.3 [22]
Silicate Coating (Rocatec System) “ Self-cured “ 38.7 [1]
“ “ Heat-cured “ 23.8±1.7 [15]
META “ Heat-cured (Trevalon) Four-point bend 31.9 ±1.5 [9]
“ “ Heat-cured (Metadent) “ 42.5±2.2 “
“ “ Heat-cured Tensile strength 21.0 [24]
META (Super bond) “ “ Shear bond 19.1 ±8.9 [14]
META (New Metacolor) “ Self-cured “ 21.5± 2.2 [16]
MDP (Estenia Opaque Primer) “ “ “ 42.7 [1]
“ “ Heat-cured “ 7.0 ±3.0 [14]
MDP “ “ Tensile strength 23.5 [24]
“ “ Self-cured with EGDMA and
TBB (Super- Bond C&B)
“ 21.2±4.7 [20]
“ “ “ “ 16.2±5.9 [19]
MDP (Cesead ) “ Self-cured Shear bond 19.0± 2.2 [16]
MEPS (Thermoresin) “ “ “ 14.0± 0.6 “
MPS and n-propylamine Polished Heat-cured Four-point bend 25.5±6.4 [18]
MAC (MR Bond) “ “ Tensile strength 7.4 ±2.1 [12]
DOPA “ “ “ 1.8 [17]
Abbreviations: BP: benzoyl peroxide; DOPA;3,4-dihydroxyL-phenylalanine; MAC:11-metacryloyloxyundecan 1,1-dicarboxylic; MATP: Methacryloxypropyl-trimethoxysilane; MDDA:10-methacyloyloxydecyl 6,8-dithioctanoate; MDP:10-Methacryloyloxydecyl dihydrogen
phosphate; MDDT:10- methacryloxydecly 6,8-dithiooctanoate; MEPS: methacryloxydecly thiophosphate derivative; META: Methacryloxy ethyl
trimellitate anhydride; MHPA;6-Methacryloxyethexy phosphonacetate; MPS:3-Methacryloxypropyl trimethoxysilane; TBB:tribuylborane;
VTD:10-Methacryloyloxydecyl dihydrogen phosphate.

67
5.3. Materials and Methods
5.3.1. Materials
Poly-methyl methacrylate (PMMA) and methyl methacrylate (MMA) were obtained from Great
Lakes Orthodontics (Tonawanda, NY), and were used without any further purification. The rest
of the reagents were obtained from Sigma Aldrich (St. Louis, MO). P-phenylenediamine (PPD),
sodium nitrate (NaNO2), sodium dodecyl sulfate (SDS), benzoyl peroxide (BP), and iron powder
(Fe) were used as received. Concentrated hydrochloric acid (HCl) was diluted in distilled water
(DW) to a concentration of 0.5M.
The metallic samples used in the experiments were either orthodontic wrought wires (stainless
steel) or polished rectangular bars (Ti). The wrought wires (Tur-Chrome S.S, Rocky Mountain
Orthodontic, Denver, CO) had a diameter of 0.6 mm and were cut into 200.0 mm long sections.
The Ti samples (Ti alloy grade 2, McMaster-Carr, Cleveland, OH) were obtained as rectangular
bars (6.4, 12.7 and 305.0 mm) and cut into smaller sections (12.7, 6.4 and 6.4 mm) using an
abrasive cutter (Delta AbrasiMet, Buchler, Whitby, ON).
5.3.2 Preparation of the metallic samples
The Ti samples were polished using a six step polishing method to obtain a flat surface. First,
they were polished by means of a water-cooled trimmer and 240-to-600 grit silicon carbide
papers (Paper-c wt, AA Abrasives, Philadelphia, PA). Then, they were further polished on a
polishing wheel (LapoPol-5, Struers, Rodovre, Denmark) using two types of polishing cloths;
rough-to-intermediate polishing cloth (15-0.02μm; TexMet C) and final polishing cloth (1-
0.02μm; ChemoMet), with Colloidal Silica Suspension (≤ 0.06μm; MasterMet; Buchler,

68
Whitby, ON). The orthodontic wrought wires did not undergo any specific preparation prior to
surface treatment besides being cleaned. All metallic samples were cleaned in an ultrasonic bath
(FS20D Ultrasonic, Fisher Scientific, Montreal, Canada) with DW, ethanol, and acetone for 5
minutes in each solution at 37 oC.
5.3.3. Surface treatment of the metallic samples
The surface treatment was performed in a two steps protocol based on p-phenylenediamine
diazotization (primer and adhesive). Both steps were carried out in acidic DW solution at pH≤2,
since diazonium cations are stable at pH ≤2.5, at room temperature in a simple glass beaker [39,
41]. The first step (primer) was conducted as follows: PPD (0.054g; 0.05M) and NaNO2 (0.034g;
0.05M) were dissolved in a glass beaker containing 10 ml of 0.5 M HCl. After ultrasonicating
the solution for 5 minutes, all metallic samples except control group were immersed in the
solution and Fe powder (0.250g) was added as a reducing agent. The samples were left to react
for 15 minutes before ultrasonicating them in DW and acetone for 5 minutes. This first step leads
to spontaneous grafting of a polyaminophenylene (PAP) layer on the metallic samples (i.e.
titanium and stainless steel wrought wire). These samples are referred to as metal-PAP from here
onwards.
Different approaches were investigated in the second (adhesive) step in order to optimize the
adhesion of MMA to metal-PAP samples. These approaches can be summarized in four groups
(Table 5.2). All groups share the following process: NaNO2 (0.034g; 0.05M) was dissolved in
10ml of 0.5 M HCl. Then, the metal-PAP samples were introduced in the solution before adding
Fe powder (0.250g). In the first group, only the monomer (MMA) was added to the solution. In
groups 4, 5 and 6, a surfactant (SDS, 0.026 g) was added along with MMA to help solubilize the

69
hydrophobic monomer [42, 43]. The reaction was allowed to continue for 15 minutes in the
ultrasonic bath and for another 30 minutes on the bench top; during this period the monomer
polymerized and formed a thin layer of PMMA on the metallic surface. In groups 5 and 6, an
initiator (benzoyl peroxide, BP) was added after the fifteen minute sonication stage to accelerate
the polymerization reaction on the metallic surface. Finally, the samples were thoroughly rinsed
with acetone, and then ultrasonicated in DW and acetone for 5 minutes in order to discard any
ungrafted matter.
Table 5.4: Conditions tested in the second step. The overall solution volume was 12 ml, and was water-based.
Groups Metal Solution Abbreviation HCl 0.5 M; NaNO2 0.05M;
Fe 0.25g; MMA 2.0 ml
(ml)
SDS
(M)
[BP]
(mg/ml)
1 Ti None Control 0 0 0 2 Ti None D 0 0 0 3 Ti MMA Emulsion without SDS D+M 12 0 0
4 Ti MMA Emulsion with SDS D+M+E 12 9. 10 -3 0
5 Ti MMA Emulsion with SDS and initiator D+M+E+I 12 9. 10 -3 8-48
6 SS MMA Emulsion with SDS and initiator D+M+E+I 12 9. 10 -3 40
D: diazonium grafting (step 1); M: monomer (MMA); E: emulsifier (SDS); I: initiator (BP); Ti: titanium; SS: stainless steel.
5.3.4. Spectroscopic analysis
A monochromatic X-ray photoelectron spectrometer K Alpha (Thermo Fischer Scientific Inc,
East Grinstead, UK) was used for determining the relative quantities and chemical environments
of the elements on the Ti surfaces. The setup was equipped with an Al Kα X-Ray radiation
source (1486.6 eV, 0.834 nm), a micro-focused monochromator and an ultrahigh vacuum
chamber (10-9
torr). For all the groups (control; D; D+M; D+M+E; D+M+E+I), survey scans
were obtained over the range of 0-1350 eV with a pass energy of 200 eV at a step of 1.0 eV,
while high resolution scans were collected with a pass energy of 50 eV at a step of 0.1 eV.
Energies were calibrated by setting the binding energy of the carbon bonded to hydrogen or
carbon (C-(H, C)) at 285.0 eV on all samples. Data analysis and peak fitting were performed
70
using Avantage (5.41v, Thermo Fischer Scientific Inc, East Grinstead, UK) chemical surface
analysis software.
5.3.5. Contact angle measurement
Hydrophobicity of the Ti surfaces in all groups was evaluated by the contact angle measurement
that was recorded and analyzed at room temperature on contact angle meter (OAC 15, Data
Physics, Germany). The static contact angle was automatically calculated by measuring the angle
produced by a drop of DW (2ml) placed on the Ti surface of each samples, and the side view
images were captured.
5.3.6. Mechanical tests
Tensile test was used to measure the bond strength between PMMA and the metallic surface. To
test the Ti-PMAA bond strength, a custom-made mold was fabricated from a silicone (Exaktosil
N 21, Bredent, Germany) (Figure 5.1.a), and a piece of Ti was fixed in the middle of the mold.
Then, a mix of PMMA powder and MMA liquid monomer (Biocryl Resin Acrylic, Great Leakes,
NY) with ratio of 2:1 was poured to fill the sides of the mold. The PMMA was left to set for
three hours at room temperature and humidity. This procedure generated a final specimen that
was 130 mm long, 13 mm wide and 3 mm thick with two grips of bulk PMMA polymerized at
the sides of the Ti samples (Figure 5.1.b). After complete setting of the acrylic resin, the tensile
bond strength between PMMA and Ti was measured using a universal testing machine (H25K-S,
Tinius Olsen Testing Machine Co., Inc Willow Grove, PA) set up at a constant speed of 10
mm/min. The tensile force was applied to the specimen until fracture occurred at the PMMA-Ti

71
interface, and the strength of the bond between Ti and PMMA was calculated in megapascals
(MPa).
The specimens used to test the bond between wrought wire and PMMA were prepared using a
different custom-made silicone mold. The resulting specimens consisted of 20 mm of wrought
wire embedded vertically into a plate of PMMA (3 mm thick; 20 mm wide; 130 mm long)
(Figure 5.1.c). The acrylic plate and the wire were secured into a universal testing machine (as
described earlier) in order to measure the tensile strength of the bond between the wire and the
PMMA.
Figure 5.1: (a) the custom-made silicone mold used to prepare the PMMA-Ti specimen; (b) the Ti-PMMA specimen
before and after mechanical testing; (c) the stainless steel wrought wire-PMMA specimen before and after mechanical
testing.
5.3.7. Statistical analysis
Statistical analysis on all XPS, contact angle, and mechanical test results was performed using
Origin 8.0 (Origin lab, Northampton, MA). All the data were analyzed using nonparametric tests,
Kruskal-Wallis test and the significance level was set at p<0.05.
72
5.4. Results and discussion
The diazonium chemistry method that we used to bind PMMA and dental alloys consisted of two
steps. In the first step, PPD was first transformed into an amino diazonium cation by adding one
equivalent of NaNO2 (Figure 5.2.a). The diazonium cation was then reduced with Fe to achieve
an aminophenyl radical (Figure 5.2.b). This radical spontaneously grafted onto the titanium
surface (Figure 5.2.c), and kept reacting with itself forming multilayers (PAP, Figure 5.1.d) [39].
The second step (adhesive) of the reaction was optimized in order to achieve covalent binding
between metals and PMMA for applications in dental prostheses. The amino groups of the PAP
layer were reduced to radicals using again NaNO2 and Fe in an acidic environment, as in the first
step (Figure 5.2.e). The radicals reacted with MMA, and formed a thin PMMA layer on top of
the metal-PAP (Figure 5.2.f; SDS was used in some samples to solubilize MMA). In some of the
samples, PMMA chain length was increased by adding BP, which helped the formation of more
MMA radicals (Figure 5.2.g).
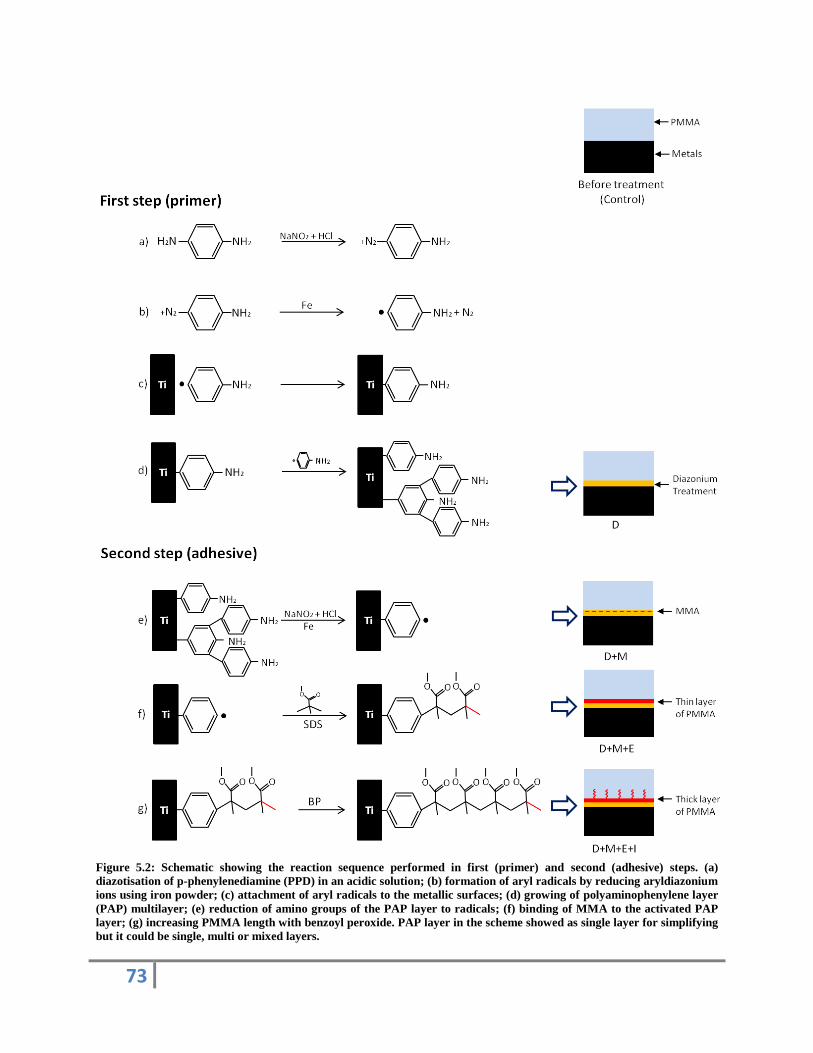
73
Figure 5.2: Schematic showing the reaction sequence performed in first (primer) and second (adhesive) steps. (a)
diazotisation of p-phenylenediamine (PPD) in an acidic solution; (b) formation of aryl radicals by reducing aryldiazonium
ions using iron powder; (c) attachment of aryl radicals to the metallic surfaces; (d) growing of polyaminophenylene layer
(PAP) multilayer; (e) reduction of amino groups of the PAP layer to radicals; (f) binding of MMA to the activated PAP
layer; (g) increasing PMMA length with benzoyl peroxide. PAP layer in the scheme showed as single layer for simplifying
but it could be single, multi or mixed layers.

74
XPS results (Figures 5.3.a and 5.3.b) showed that the Ti surface for the control (untreated)
samples was covered by TiO2 and carbon; the carbon has to be related to the unavoidable
contamination upon exposition to air prior to XPS analysis [44]. The bond strength between the
untreated polished Ti and PMMA was very low (1.54±1.02 MPa), indicating that the mechanical
and chemical bonds between Ti and PMMA were minimal (Figure 5.5.a). It is hard to find a
comparison between this value and what reported in the literature (Table 5.1), since all the data
reported for PMMA-Ti bonds on untreated samples refer to sandblasted Ti surfaces, which
provides an increased mechanical bond. After sandblasting, the reported tensile strengths vary
between 3.2 and 20.0 MPa [1, 9, 12, 14-24, 27]. In fact it is extremely difficult to test the bond
between a polished Ti surface and PMMA, since the samples tend to fail very quickly [25].
XPS confirmed the grafting of a PAP layer on the Ti surface after the first step of the diazonium
treatment (Scheme 5.2.d): indeed, the samples from group D showed 4.3% N on their surface,
and an increased C content from 17.9% (control samples) to 64.2% (Figure 5.3.b). Ti content
was decreased from 20.5% in control samples to 6.2% in group D confirming the presence of the
PAP layer covering the Ti surface. The high resolution C 1s spectra (Figure 5.3.c) showed that
the components relative to hydrocarbon (C-C/C-H, centered at 285.0 eV), C-O and C-N groups
(centered at 286.4 eV), and carboxyl groups (O-C=O, centered at 288.8 eV) changed from 61.2,
26.7, and 12.1% respectively in control samples to 79.6, 18.3, and 2.1% respectively in group D.
The drastic decrease of the carboxyl groups is especially indicative of the formation of the PAP
layer, since no carboxyls should be present in this layer.
Contact angle measures gave more evidence of the grafting of the PAP layer on Ti surfaces
(Figure 5.4). A DW contact angle of 53.5±14.8° was measured for polished titanium before
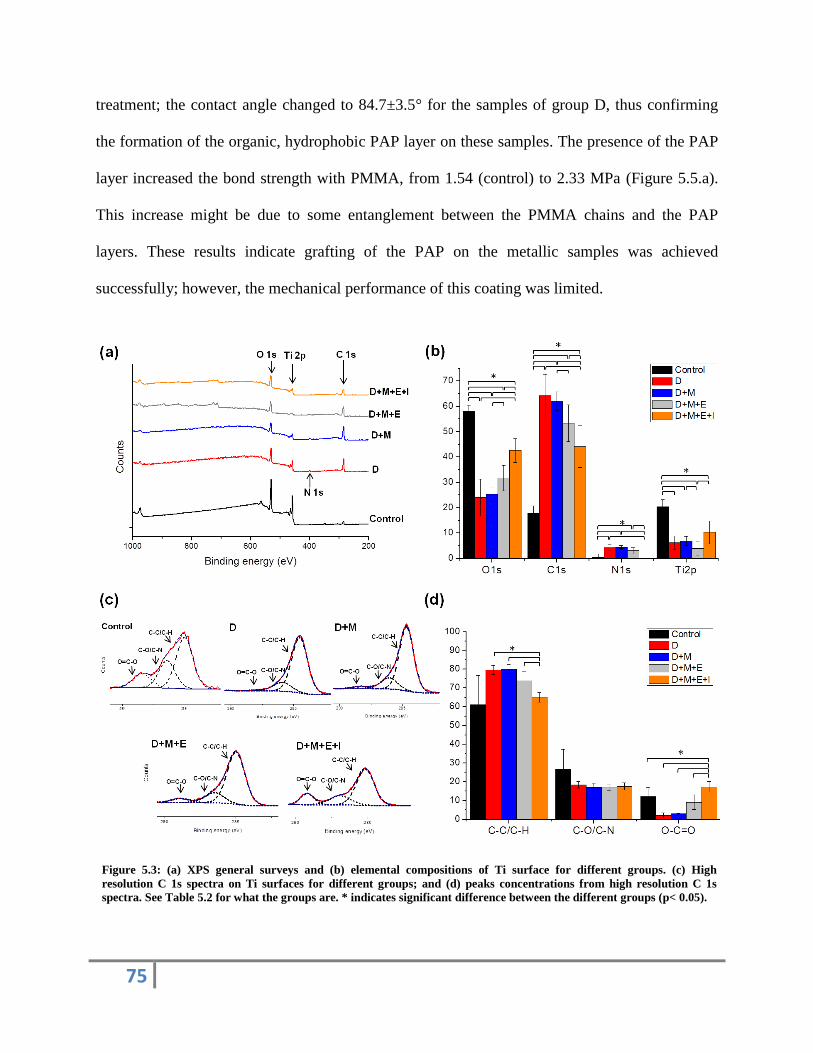
75
treatment; the contact angle changed to 84.7±3.5° for the samples of group D, thus confirming
the formation of the organic, hydrophobic PAP layer on these samples. The presence of the PAP
layer increased the bond strength with PMMA, from 1.54 (control) to 2.33 MPa (Figure 5.5.a).
This increase might be due to some entanglement between the PMMA chains and the PAP
layers. These results indicate grafting of the PAP on the metallic samples was achieved
successfully; however, the mechanical performance of this coating was limited.
Figure 5.3: (a) XPS general surveys and (b) elemental compositions of Ti surface for different groups. (c) High
resolution C 1s spectra on Ti surfaces for different groups; and (d) peaks concentrations from high resolution C 1s
spectra. See Table 5.2 for what the groups are. * indicates significant difference between the different groups (p< 0.05).

76
Figure 5.4: Photographs of water droplets placed on different Ti groups; the contact angle for control group was
53.5±14.8°; D= 84.7±3.5°; D+M= 84.1±1.9°; D+M+E= 83.1±0.5°; D+M+E+I= 82.4±0.9°. See Table 5.2 for what the
groups are * indicates significant difference between the different groups (p< 0.05).
Figure 5.5: (a) Tensile strength of the bond between PMMA and treated Ti surfaces. See Table 5.2 for what the groups
are. (b) Tensile strength of the bond between PMMA and Ti as a function of BP concentration in the aqueous phase of
MMA emulsion. * indicates significant difference between the different groups (p< 0.05).
The second step of the treatment (adhesive) was designed to change the amino ends of the metal-
PAP layer (-C6H4-NH2) into diazonium radicals (-C6H4-N2•) and then grow a few layers of
PMMA on it. As a first attempt, together with the reactants used to achieve the reduction of the
NH2 group into the diazonium radical, we added the MMA monomer alone (group D+M). This
did not lead to the formation of PMMA on top of the PAP layer. In fact, XPS and contact angle
results for the group D+M are quite similar to those of group D (Figures 5.3 and 5.4), and the
mechanical tests showed almost identical bond strengths for the groups D+M and D (Figure

77
5.5.a). The reason for the failure to grow PMMA in this condition is that MMA is a hydrophobic
monomer, hardly soluble in the aqueous solution used to modify the Ti surface.
XPS and mechanical tests indicate that the polymerization of PMMA in group D+M+E, which
includes the addition of SDS to solubilize MMA in the second step, was better than in group
D+M [43, 45]. We added SDS with a concentration of 9x10-3
M; this concentration was above
SDS critical micelle concentration (8.2x10-3
M [42]), so that SDS could disperse MMA in the
aqueous reaction solution by forming micelles around MMA droplets [43, 46]. The droplet size
of such micelles was reported to be in the range of 30 to 100 nm [47].
XPS confirmed the presence of PMMA on the grafted layer in group D+M+E by showing an
increase in oxygen up to 31.7% as well as a decrease in the concentration of Ti down to 3.9%,
indicating that PMMA was polymerized on the metal-PAP layer covering the Ti surface (Figure
5.3.b). Despite the slight decrease in overall C, the high resolution C 1s spectra for group
D+M+E showed an increase in O-C=O group concentration up to 9.1% compared to the previous
groups at concentration of 3.0%, thus confirming PMMA polymerization [48-50] (Figures 5.3.c
and 5.3.d). The contact angle in group D+M+E was 83.1±0.5° confirming the presence of
hydrophobic layer on these samples (Figure 5.4). The formation of a PMMA adhesive layer
increased the tensile bond strength between PMMA and the treated Ti in group D+M+E up to
3.4±1.2 MPa (P<0.05) (Figure 5.5.a). Most likely this was due to the entanglement achieved
between the PMMA chains in solution and those grown on the Ti-PAP surface thanks to the
better solubilization of the MMA monomer.
To further increase the bond strength between PMMA and Ti, we added BP to help
polymerization (group D+M+E+I). Increasing the length of the PMMA chain that grows on the

78
metal-PAP layer was critical to increase the strength of the bond between Ti and PMMA [51].
PMMA polymerizes by free radical addition polymerization, which requires the presence of an
initiator such as BP to start. BP is a relatively unstable compound, which forms radicals simply
upon heating or irradiation. BP radicals react with MMA and create MMA radicals, which then
propagate and grow longer and longer PMMA chains [31]. BP is the most commonly used
initiator for PMMA polymerization [52-54]. Thus, we added BP to the MMA emulsion in
different concentrations, and the bonding strength between Ti and PMMA increased remarkably.
In group D+M+E+I, XPS showed the N concentration was negligible after PMMA
polymerization with BP, which indicates that the PAP layer was covered by the thick layer of
PMMA formed (Figure 5.3.b). The formation of a thick PMMA layer is confirmed by the
increase in O content up to 42.6% on the surface of this sample and the increase in the O-C=O
component up to 17.6% in the high resolution C1s spectrum (Figure 5.3) [48-50]. Contact angle
measures in group D+M+E+I confirmed the formation of the hydrophobic PMMA layer on these
samples, and the contact angle was significantly difference (82.4±0.9°) compared to control
group (53.5±14.8°) (Figure 5.4). The addition of BP leads to the strongest tensile bond between
PMMA and Ti (8.14±1.10 MPa). This bond strength was significantly higher than that achieved
in any other group (P<0.05) (Figure 5.5). The resulting high bond strength indicates that
formation of a thicker PMMA layer containing long PMMA chains that can entangle very
strongly with the PMMA chains that are polymerized in the bulk PMMA casted on the sample.
The highest bond strength for titanium-PMMA (8.14±1.10 MPa) was obtained at BP
concentration of 40 mg/ml (Figure 5.5.b). At concentrations higher than 40 mg/ml, BP caused a
slight decrease on the bond strength between PMMA and titanium; this might be because BP
attacked the PAP layer grafter on the Ti surface.

79
A similar two step method including all the improvements for the second step described for the
Ti-PMMA bond was applied to bind PMMA and stainless steel wrought wire. The bonding
achieved in this case (4.34±0.68 MPa) was significantly higher than if it was left untreated
(1.71±0.23 MPa) (Figure 5.6). Acrylic removable partial dentures and orthodontic removable
appliances that combine stainless steel wrought wires and PMMA are usually cannot be made
when not enough volume of PMMA is available to support the wire [30, 31]. By increasing bond
strength between stainless steel wrought wire and PMMA through this treatment, more leverage
is possible for fabricating acrylic-based dental devices when not enough volume of acrylic is
available to support the wire (Figure 5.7).
Figure 5.6: Bond strength of PMMA and stainless steel wires for the control group and stainless steel wrought wire that
were treated with diazonium in MMA emulsion using the surfactant SDS and the initiator. * indicates significant
difference between the different groups (p< 0.05).

80
Figure 5.7: Schematic showing the acrylic removable partial denture with a small volume of PMMA to support the wire;
the short wire treated according to the proposed optimized two-step diazonium method should be stable enough in
PMMA to allow prosthesis retention.
5.5. Conclusion
The treatment of metallic surfaces (titanium and stainless steel) with diazonium ions in a two-
step procedure where the second step includes an emulsion containing monomer (MMA), an
emulsifier (SDS), and an initiator (BP) increase the bond strength of PMMA to Ti, and PMMA
to stainless steel wrought wire by 5.2 and 2.5 folds respectively compared to untreated control
groups. The bond strength achieved between polished Ti and PMMA is higher than that achieved
with any other method reported in the literature. The increased bond strength achieved between
Ti and PMMA is likely to be able to prevent dental prostheses failure. Also, it might help reduce
microleaks at the Ti/PMMA interface, thus preventing accumulation of oral debris and
discoloration of denture base materials and improving esthetics and oral hygiene [1, 2, 8]. This
bonding technique provide more leverage for fabricating acrylic-based dental devices when not
enough volume of acrylic is available to support the wire Although there are several commercial
methods to bind metals to PMMA for dental prostheses, the method proposed in this paper
significantly improved the bond strength between PMMA and polished Ti compared to all other
available methods. Further improvements may be obtained by combining this technique with
mechanical interlocking.

81
Acknowledgments
The authors would like to acknowledge King Saud University in Riyadh, Saudi Arabia; Natural
Sciences and Engineering Research Council (NSERC) of Canada–Discovery grant (F.T. and
M.C.); Canada Research Chair Foundation (M.C); and the Fondation de l’Ordre des dentists du
Québec (FODQ), Le Réseau de recherche en santé Buccodentaire et osseuse (RSBO) for their
financial support. Thanks to Enrique Lopez Cabarcos and Xuan Tuan Le for their technical
support.
5.6. References
1. Matsuda Y, Yanagida H, Ide T, Matsumura H, Tanoue N. Bond strength of poly(methyl
methacrylate) denture base material to cast titanium and cobalt-chromium alloy. J Adhes
Dent, 2010; 12:223-9.
2. Rothfuss LG, Hokett SD, Hondrum SO, Elrod CW. Resin to metal bond strengths using
two commercial systems. J Prosthet Dent, 1998; 79:270-2.
3. Cooper LF, Limmer BM, Gates WD. “Rules of 10”—Guidelines for successful planning
and treatment of mandibular edentulism using dental implants. Compend Contin Educ
Dent, 2012; 33:328.
4. Gautam R, Singh RD, Sharma VP, Siddhartha R, Chand P, Kumar R. Biocompatibility of
polymethylmethacrylate resins used in dentistry. J Biomed Mater Res Part B, 2012;
100B:1444-50
5. Narayan R. Biomedical materials. New York: Springer; 2009.
6. Vallittu PK. A review of methods used to reinforce polymethyl methacrylate resin. J
Prosthodont, 1995; 4:183-7.
7. NaBadalung DP, Powers JM, Connelly ME. Comparison of bond strengths of denture base
resins to nickel-chromium-beryllium removable partial denture alloy. J Prosthet Dent,
1997; 78:566-73.
8. Jacobson T. The significance of adhesive denture base resin. Int J Prosthodont, 1989;
2:163.
9. Mudford L, Curtis RV, Walter JD. An investigation of debonding between heat cured
PMMA and titanium alloy (Ti-6Al-4V). J Dent, 1997; 25:415-21.
10. Jacobson TE, Chang JC, Keri PP, Watanabe LG. Bond strength of 4-META acrylic resin
denture base to cobalt chromium-alloy. J Prosthet Dent, 1988; 60:570-6.
11. Taira Y, Yang L, Atsuta M. Comparison of four fluoride etchants in bonding between
titanium and a self-curing luting agent. Dent Mater J, 2006; 25:345-51.

82
12. Kim S-S, Vang M-S, Yang H-S, Park S-W, Lim H-P. Effect of adhesive primers on
bonding strength of heat cure denture base resin to cast titanium and cobalt-chromium
alloy. J Adv Prosthodont, 2009; 1:41-6.
13. Taira Y, Imai Y. Primer for bonding resin to metal. Dent Mater, 1995; 11:2-6.
14. Kawaguchi T, Shimizu H, Lassila LVJ, Vallittu PK, Takahashi Y. Effect of surface
preparation on the bond strength of heat-polymerized denture base resin to commercially
pure titanium and cobalt-chromium alloy. Dent Mater J, 2011; 30:143-50.
15. May KB, Fox J, Razzoog ME, Lang BR. Silane to enhance the bond between polymethyl
methacrylate and titanium. J Prosthet Dent, 1995; 73:428-31.
16. Fujishima A, Fujishima Y, Ferracane JL. Shear bond strength of 4 commerical bonding
system to cp ti. Dent Mater, 1995; 11:82-6.
17. Hamming LM, Fan XW, Messersmith PB, Brinson LC. Mimicking mussel adhesion to
improve interfacial properties in composites. Compos Sci Technol, 2008; 68:2042-8.
18. Ekstrand K, Ruyter IE, Oysaed H. Adhesion to titanium of methacrylate-based polymer
materials. Dent Mater, 1988; 4:111-5.
19. Kwon T-Y, Imai Y. Influence of molecular weight of PMMA in PMMA/MMA-TBB resin
on durability of adhesion to titanium against thermal stress in water. Dent Mater J, 2006;
25:291-7.
20. Imai Y, Ikeda Y. Effect of adding ethylene glycol dimethacrylate to resin cements:
durability against thermal stress of adhesion to titanium. Dent Mater J, 1997; 16:74-7.
21. Gbureck U, Grubel S, Thull R, Barralet JE. Modified PMMA cements for a hydrolysis
resistant metal-polymer interface in orthopaedic applications. Acta Biomater, 2005; 1:671-
6.
22. Segerstrom S, Ruyter IE. Adhesion properties in systems of laminated pigmented
polymers, carbon-graphite fiber composite framework and titanium surfaces in implant
suprastructures. Dent Mater, 2009; 25:1169-77.
23. Koizumi H, Furuchi M, Tanoue N, Yanagida H, Yoneyama T, Matsumura H. Bond
strength to primed Ti-6Al-7Nb alloy of two acrylic resin adhesives. Dent Mater J, 2006;
25:286-90.
24. Tsuchimoto Y, Yoshida Y, Mine A, Nakamura M, Nishiyama N, Van Meerbeek B, et al.
Effect of 4-MET- and 10-MDP-based primers on resin bonding to titanium. Dent Mater J,
2006; 25:120-4.
25. Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A, et al.
Relationship between bond-strength tests and clinical outcomes. Dent Mater, 2010;
26:e100-e21.
26. Vuorinen AM, Dyer SR, Lassila LVJ, Vallittu PK. Bonding of bisgma–tegdma-resin to
bulk poly (paraphenylene) based rigid rod polymer. Compos Interfaces, 2011; 18:387-98.
27. Le Guéhennec L, Soueidan A, Layrolle P, Amouriq Y. Surface treatments of titanium
dental implants for rapid osseointegration. Dent Mater, 2007; 23:844-54.
28. Fukuda M, Takahashi T, Nagai H, Iino M. Implant-supported edentulous maxillary
obturators with milled bar attachments after maxillectomy. J Oral Maxillofac Surg, 2004;
62:799-805.
29. Sperling LH. Mechanical behavior of polymers. Introduction to physical polymer science:
John Wiley & Sons, Inc.; 2005. p. 557-612.
30. Brantley WA, Eliades T. Orthodontic materials scientific and clinical aspects. Stuttgart;
New York, NY: Thieme; 2001.

83
31. Sakaguchi RL, Powers JM. Craig's restorative dental materials. St. Louis, Mo.:
Elsevier/Mosby; 2012.
32. Gam-Derouich S, Lamouri A, Redeuilh C, Decorse P, Maurel Fo, Carbonnier B, et al.
Diazonium salt-derived 4-(dimethylamino) phenyl groups as hydrogen donors in surface-
confined radical photopolymerization for bioactive poly (2-hydroxyethyl methacrylate)
grafts. Langmuir, 2012; 28:8035-45.
33. Mahouche-Chergui S, Gam-Derouich S, Mangeney C, Chehimi MM. Aryl diazonium salts:
a new class of coupling agents for bonding polymers, biomacromolecules and
nanoparticles to surfaces. Chem Soc Rev, 2011; 40:4143-66.
34. Adenier A, Barré N, Cabet-Deliry E, Chaussé A, Griveau S, Mercier F, et al. Study of the
spontaneous formation of organic layers on carbon and metal surfaces from diazonium
salts. Surf Sci, 2006; 600:4801-12.
35. Hinge M, Gonçalves ES, Pedersen SU, Daasbjerg K. On the electrografting of stainless
steel from para-substituted aryldiazonium salts and the thermal stability of the grafted
layer. Surf Coat Technol, 2010; 205:820-7.
36. Gam-Derouich S, Mahouche-Chergui S, Turmine M, Piquemal JY, Hassen-Chehimi DB,
Omastová M, et al. A versatile route for surface modification of carbon, metals and semi-
conductors by diazonium salt-initiated photopolymerization. Surf Sci, 2011; 605:1889-99.
37. Delamar M, Hitmi R, Pinson J, Saveant JM. Covalent modification of carbon surfaces by
grafting of functionalized aryl radicals produced from electrochemical reduction of
diazonium salts. J Am Chem Soc, 1992; 114:5883-4.
38. Combellas C, Delamar M, Kanoufi F, Pinson J, Podvorica FI. Spontaneous grafting of iron
surfaces by reduction of aryldiazonium salts in acidic or neutral aqueous solution.
Application to the protection of iron against corrosion. Chem Mater, 2005; 17:3968-75.
39. Viel P, Le XT, Huc V, Bar J, Benedetto A, Le Goff A, et al. Covalent grafting onto self-
adhesive surfaces based on aryldiazonium salt seed layers. J Mater Chem, 2008; 18:5913-
20.
40. Pinson J. Attachment of organic layers to materials surfaces by reduction of diazonium
salts. Aryl Diazonium Salts: Wiley-VCH Verlag GmbH & Co. KGaA; 2012. p. 1-35.
41. Mevellec V, Roussel S, Tessier L, Chancolon J, Mayne-L'Hermite M, Deniau G, et al.
Grafting polymers on surfaces: A new powerful and versatile diazonium salt-based one-
step process in aqueous media. Chem Mater, 2007; 19:6323-30.
42. Tessier L, Deniau G, Charleux B, Palacin S. Surface Electroinitiated Emulsion
Polymerization (SEEP): A Mechanistic Approach. Chem Mater, 2009; 21:4261-74.
43. Deniau G, Azoulay L, Bougerolles L, Palacin S. Surface Electroinitiated Emulsion
Polymerization: grafted organic coatings from aqueous solutions. Chem Mater, 2006;
18:5421-8.
44. Cai K, Müller M, Bossert J, Rechtenbach A, Jandt KD. Surface structure and composition
of flat titanium thin films as a function of film thickness and evaporation rate. Appl Surf
Sci, 2005; 250:252-67.
45. Kermabon-Avon G, Bressy C, Margaillan A. Statistical design strategies to optimize
properties in miniemulsion polymerization of methyl methacrylate. Eur Polym J, 2009;
45:1208-16.
46. Schork FJ, Luo Y, Smulders W, Russum J, Butté A, Fontenot K. Miniemulsion
Polymerization. In: Okubo M, editor. Polymer Particles: Springer Berlin Heidelberg; 2005.
p. 129-255.

84
47. Souilem I, Muller R, Holl Y, Bouquey M, Serra C, Vandamme T, et al. A novel
low‐pressure device for production of nanoemulsions. Chem Eng Technol, 2012; 35:1692-
8.
48. Nathawat R, Kumar A, Acharya NK, Vijay YK. XPS and AFM surface study of PMMA
irradiated by electron beam. Surf Coat Technol, 2009; 203:2600-4.
49. Ton-That C, Shard AG, Teare DOH, Bradley RH. XPS and AFM surface studies of
solvent-cast PS/PMMA blends. Polymer, 2001; 42:1121-9.
50. Shinonaga Y, Arita K. Antibacterial effect of acrylic dental devices after surface
modification by fluorine and silver dual-ion implantation. Acta Biomater, 2012; 8:1388-93.
51. Sperling LH. Introduction to physical polymer science. Hoboken, N.J.: Wiley; 2006.
52. Silikas N, Al-Kheraif A, Watts DC. Influence of P/L ratio and peroxide/amine
concentrations on shrinkage-strain kinetics during setting of PMMA/MMA biomaterial
formulations. Biomaterials, 2005; 26:197-204.
53. Oldfield F, Yasuda H. ESR study of MMA polymerization by a peroxide/amine system:
bone cement formation. J Biomed Mater Res, 1999; 44:436-45.
54. Ikemura K, Endo T. A review of our development of dental adhesives-Effects of radical
polymerization initiators and adhesive monomers on adhesion. Dent Mater J, 2010;
29:109-21.

85
Chapter 6: Manuscript II
Surface Chemical Treatment of Orthodontic Brackets for Improved Tooth Adhesion
Omar Alageel a, Paige Kozak
a, Mohamed-Nur Abdallah
a, Jean-Marc Retrouvey
a, Marta
Cerrutib, Faleh Tamimi
a
a Faculty of Dentistry, McGill University, Montreal, QC, Canada
b Department of Mining and Materials Engineering, McGill University, Montreal, QC, Canada
6.1. Abstract
Adhesives for orthodontic brackets, such as Bis-GMA (Bisphenol A-glycidyl methacrylate)
composite resin, adhere strongly to teeth but very poorly to metallic brackets resulting in
frequent bracket deboning. To compensate for the lack of adhesion, metal orthodontic brackets
were developed with large bases that have an unfavorable impact on esthetics and hygiene.
Objective: The purpose of this study was to develop a new surface treatment, based on
diazonium chemistry that facilitates chemical bonding between metallic brackets and Bis-GMA
composite. Methods: Three models of stainless steel brackets were first coated with diazonium
ions to allow covalent binding on their surfaces. The brackets were then immersed in an
emulsion of Bis-GMA monomer and an initiator to build up Bis-GMA polymer chains on the
surface of the diazonium layer. The chemical composition of the treated metal brackets was
analyzed by X-ray photoelectron spectroscopy (XPS) and the tensile and shear bonding strengths
between Bis-GMA composite and surface-treated metallic orthodontic brackets were measured.

86
Results: XPS result confirmed the presence of a treatment coat on the metallic brackets and the
bond strength between these coated brackets and Bis-GMA was increased after the treatment by
2 to 3.9 folds compared to untreated brackets. Conclusion: The surface treatment method
proposed in this study can be utilized to reduce bracket debonding and to decrease the current
surface area of metal brackets by at least 50%.
Keywords
orthodontic brackets; bonding; diazonium; aryl radical; bisphenol A-glycidyl methacrylate; Bis-
GMA; stainless steel.
6.2. Introduction
Esthetics is one of the main concerns for patient acceptance of any orthodontic appliance [1].
Although metal brackets are considered unesthetic, they have proven to be more reliable and
effective than plastic or ceramic brackets [2, 3]. Metal brackets are usually made of stainless
steel, and are bonded to teeth using adhesive [4]. The most popular bonding system for
orthodontic brackets is a Bis-GMA (Bisphenol A-glycidyl methacrylate) composite [4, 5]. This
composite consists of an organic matrix (Bis-GMA), an inorganic filler, a coupling agent and an
accelerator system that can be polymerized quickly via a free radical polymerization mechanism
using a chemical activator, a photo activator (light), or a dual activator [5, 6]. This bonding
system adheres very well to the enamel of teeth but very poorly to metallic brackets [7-15].
The weak bonding between brackets and composite is the main factor for bracket debonding that
is a common occurrence in daily clinical practice for average rates between 4.7 to 6 percent
(Figure 6.1) [13]. Brackets loss has many negative impacts on the treatment such as extending

87
treatment duration and chair time, and costing more money for using new materials [4]. Bracket
loss is more common in complex orthodontic treatment, where the mechanics of severely
crowded or angulated teeth require strong forces to correct the malocclusion [16, 17]. In fixed
appliances therapy, bands are fitted around a tooth, usually on molars, to provide extra strength,
but they have unfavorable impact on patient comfort, esthetics and oral hygiene [4]. However,
using buccal tubes instead of bands would be more sufficient if they bonded well to teeth [4].
To compensate for this lack of adhesion between brackets and composite, orthodontic brackets
were developed with large textured bases designed to increase the surface area and mechanical
retention [7-9]. Larger brackets have a negative impact on patient satisfaction and oral health due
to increased food impaction, rates of demineralization and caries and reduced comfort and
esthetics [4, 7, 8, 14, 15].
Figure 6.1: Photographs showing bracket debonding at the interface between brackets and composite. a: bracket
debonded from a mandibular canine due to its weak bond to composite that remains on teeth ;b: brackets basses showing
little composite on the surface indicating the debonding was as a result of the weak bond of brackets to composite .
Most of the research conducted to increase the adhesion of brackets to composite has been
limited to modifications of the surface pattern of the bracket base in order to increase
micromechanical interlocking, and has only achieved minor improvements [7, 9, 18, 19].
88
Accordingly, a chemical adhesive system that could increase the bond strength between
orthodontic brackets and dental composite would be of great interest for clinical orthodontic
practice because it could prevent brackets loss and result in a reduction of the size of brackets
that translates into less dental problems associated to them.
Aryl diazonium salts have been the subject of much recent research, and their ability to modify
many materials surfaces for many applications [20, 21]. The value of aryl diazonium salts lie in
its ease of preparation, rapid reduction, and to the strong covalent bonding [21, 22]. Diazonium
ions can be produced from aromatic amines and grafted onto almost any surface, including
metals, glass, and carbon [22-26]. Initially, diazonium grafting was performed using
electrochemical reduction, but recently this has been achieved using chemical reducing agents in
an acidic solution [27]. The reducing agents activate the aryldiazonium salts and form aryl
radicals that covalently bind to the surface of interest [28, 29]. If an extra amino group is present
on the aryldiazonium precursor, this group can be further activated in a second step, and used to
bind a second layer onto the original surface [28, 30].
The objective of this study was to develop a new surface treatment, based on diazonium
chemistry that facilitates chemical bonding between metallic brackets and Bis-GMA composite.
Improving bond strength between orthodontic brackets and composite resin will reduce bracket
debonding, provide more leverage in cases with complex mechanics, permit the use of buccal
tubes instead of using molars bands, and allow the use of brackets with smaller bases resulting in
fewer complications associated with esthetics and oral hygiene.

89
6.3. Materials and Methods
6.3.1 Teeth
Twenty-four extracted human teeth were collected from adult patients with dental conditions that
required tooth extraction. The extraction procedure was performed in the McGill Undergraduate
Dental Clinic after obtaining approval from the McGill University Health Center Ethical
Committee and informed consent of the patients. Upon extraction, teeth were immersed in 10%
formalin solution (BF-FORM, Fisher Scientific, Canada) for 1 week. The teeth were then
cleaned with distilled water in an ultrasonic bath (FS20D Ultrasonic, Fisher Scientific, Canada)
for 60 min at 25oC and polished for 1 min with a low-speed dental handpiece (M5Pa, KAB-
Dental, USA) using SiC cups (Pro- Cup, sdsKerr, Italy) and dental prophylaxis pumice of low
abrasive capability (CPRTM, ICCARE, USA). Next, the teeth were rinsed again in an ultrasonic
bath before storing in labelled Eppendorf tubes with 10% formalin solution for further analysis.
6.3.2 Mold preparation
Teeth were cleaned with water and air-dried. Each tooth was partially embedded in a mold of
plaster of Paris. Teeth were oriented to be perpendicular to the surface of the plaster mold in
order to test shear strength.
6.3.3 Brackets
Three different commercial models of stainless steel orthodontic brackets were used in this
study: buccal tubes baseless brackets for maxillary first molars (n=60; surface area of 0.325 by
0.300 cm; Rocky Mountain Orthodontic, Denver, CO) referred to as group R (Figure 6.2.a);

90
maxillary anterior teeth large brackets (n= 64; base dimension of 0.380 by 0.260 cm; 3M Unitek,
Monrovia, CA) referred to as group L (Figure 6.2.b); and mandible lateral teeth small brackets
(n=60; base dimension of 0.275 by 0.255 cm; 3M Unitek, Monrovia, CA) referred to as group S
(Figure 6.2.c). In each group, 40 brackets were used for tensile bond strength test between two
brackets and Bis-GMA, while 20 brackets were used for the shear bond strength test of brackets
bonded to teeth using Bis-GMA adhesive. All brackets were ultrasonicated in distilled water,
ethanol and acetone for 5 minutes prior to surface treatment.
Figure 6.2: Digital photographs illustrating the different types of brackets used in this study: (a) baseless buccal tubes
brackets (referred as group R); (b): 3M Unitek bracket with large basses (referred as group L), (c): 3M Unitek bracket
with small basses (referred as group S). Schematic drawing showing the preparation and mechanism of testing (d) tensile
and (e) shear bonding strength between brackets and Bis-GMA.
91
6.3.4 Treatment Materials
P-phenylenediamine (PPD), sodium nitrate (NaNO2), sodium dodecil sulfate (SDS), benzoyl
peroxide (BP), Bisphenol A-glycidyl methacrylate (Bis-GMA), hypophosphorous acid (H3PO2),
and hydrochloric acid (HCl) were purchased from Sigma Aldrich (St. Louis, MO) and were used
without any further purification. Concentrated hydrochloric acid (HCl) was diluted in distilled
water to a concentration of 0.5 M.
6.3.5 Surface Treatment Process
Brackets were treated in two solutions (primer and adhesive). Both solutions were prepared at
room temperature in an acidic deionized water solution at pH≤2, since diazonium cations are
stable at pH ≤2.5 [28, 30]. The first solution (primer) was prepared by dissolving PPD (0.054g;
0.05M) and NaNO2 (0.034g; 0.05M) in a beaker containing 10 ml of 0.5 M HCl (Figure 6.3.a).
Then, hypophosphorous acid (H3PO2; 0.66 ml) was added to the primer solution as a reducing
agent to form the aryl radical (Figure 6.3.b). The stainless steel brackets were then introduced
into the primer solution and left to react for 15 minutes before ultrasonicating them in distilled
water and acetone for 5 minutes. This first treatment solution leads to the formation of a
diazonium layer on the stainless steel brackets (Figure 6.3.c) [28].
The second solution (adhesive) was prepared by dissolving NaNO2 (0.034g; 0.05M) and SDS
(0.026 g, 9x10-3
M) in a beaker containing 10 ml of HCl (0.5 M). SDS was added into the
solution as a surfactant to help solubilize the hydrophobic monomer solution [31, 32]. Then, the
hypophosphorous acid (H3PO2; 0.66 ml) was added to the adhesive solution (Figure 6.3.d). Next,
the brackets treated with primer solution were introduced into the adhesive solution and Bis-

92
GMA (2.3g/2.0 ml of ethanol) was added. After 15 minutes of sonication, an initiator (benzoyl
peroxide (BP), 40 mg/ml) was added to accelerate the polymerization reaction on the metallic
surface (Figure 6.3.e). The reaction was allowed to continue for an additional 15 minutes in the
ultrasonic bath and 30 minutes on the bench top. During this time, the monomer polymerized and
formed a thin layer of Bis-GMA on the diazonium-brackets surface (Figure 6.3.f). Finally, the
brackets were ultrasonicated in distilled water and acetone for 5 minutes.
Figure 6.3: Schematic diagram of the reactions performed in the first and second solutions of Bis-GMA/diazonium
treatment; (a): diazotisation of p-phenylenediamine (PPD) in an acidic solution; (b): formation of aryl radicals by
reducing aryldiazonium using H3PO2; (c): attachment of aryl radicals to brackets; (d): reduction of amino groups of the
diazonium layer to radicals; (e): binding of Bis-GMA to the activated diazonium layer; (f): polymerization of Bis-GMA.
*The grafted layer in the scheme showed as single layer for simplifying but it could be single, multi or mixed layers.
6.3.6 X-ray Photoelectron Spectroscopy
A monochromatic X-ray photoelectron spectrometer K Alpha (VG Scientific ESCLAB 3 MIKII)
was used to determine the relative quantities and chemical environments of the constituent
elements on four stainless steel brackets of group L. The setup was equipped with Mg Kα X-Ray
radiation source (1253.6 eV), a micro-focused monochromator and an ultrahigh vacuum chamber
(10-9
torr). For all samples, survey scans were obtained over the range of 0-1350 eV with pass
energy of 100 eV at a step of 1.0 eV, while high resolution scans were collected with pass energy
of 20 eV at a step of 0.05 eV. All spectra were referenced to C-C/C-H of the C 1s spectrum at
285.0 eV.

93
6.3.7 Mechanical Tests
The mechanical performance of the bonding between brackets and composite were assessed
using tensile and shear strength tests (Figure 6.2). For the tensile strength test, pairs of identical
brackets were bonded together with a light-cured Bis-GMA composite adhesive (Transbond XT
Light Cure; 3M Unitek, Monrovia, CA) and light cured for 30 seconds. The brackets were pulled
apart using a universal testing machine (Instron, 5569, Grove City, PA) set up at a constant speed
of 5 mm/min (Figure 6.2.d).
In order to evaluate the shear strength of the bond between brackets and Bis-GMA composite on
teeth, the buccal surfaces of teeth were first etched with an etchant gel (EZ Etch; Dentsply, York,
PA) for 30 seconds, rinsed with distilled water and air-dried. Then, the Transbond adhesive
primer (3M Unitek, Monrovia, CA) was applied to the tooth surface. Next, Bis-GMA composite
adhesive (Transbond XT Light Cure; 3M Unitek, Monrovia, CA) was applied to the base of a
single bracket, positioned on the tooth surface before being light cured for 30 seconds. A load
applied parallel to the long axis of the tooth with the universal testing machine, as described
earlier, generated a shear force at the interface between teeth and brackets (Figure 6.2.e).
6.3.8 Statistical Analysis
The average of the X-ray photoelectron spectroscopy and bond strength with associated standard
deviation was calculated for each group. The statistical analysis was performed using Origin 8.0
(Origin lab, Northampton, MA). All data were analyzed using t-test and Kruskal-Wallis test and
the significance level was set at p < 0.05.

94
6.4. Results
6.4.1 X-ray Photoelectron Spectroscopy (XPS)
X-ray photoelectron spectroscopy (XPS) results confirmed the presence of a diazonium/Bis-
GMA layer on treated bracket surfaces. The surface elemental composition for the stainless steel
brackets changed after diazonium/Bis-GMA treatments (Figure 6.4.a). The elements present on
the untreated stainless steel (control) brackets were carbon, oxygen, chromium, and iron;
however, only carbon and oxygen were present after treatment. The carbon content (C 1s; at
285.0 eV) increased from 43.2% in the untreated group to 81.4% after treatment, while oxygen
content (O 1s; at 532.0 eV) decreased from 43.2% in the untreated group to 17.2% after
treatment. Chromium (Cr 2p; at 576.5 eV), and iron (Fe 2p3; at 708.5 eV) were present only on
the untreated brackets in concentrations of 9.6% and 4.4% respectively.
The high resolution carbon (C 1s) spectra for the untreated brackets showed different carbon
peaks from the treated brackets (Figure 4.b). The untreated group included the C-C, C-O/C-O-C,
and O-C=O carbon peaks in concentrations of 31.3, 5.4, and 4.2%, respectively, while in the
treated group the peaks were C=C, C-C, C-O/C-O-C, and O-C=O with concentrations of 37.9,
22.3, 16.8, and 3.3%, respectively.

95
Figure 6.4: (a): XPS general surveys and elemental compositions for the untreated (control) and treated brackets; (b):
high resolution XPS C 1s spectra for the untreated and treated brackets. * indicates significant difference between groups
(p< 0.05).
6.4.2 Mechanical Tests
The mechanical tests showed that the tensile and shear bond strengths between Bis-GMA
composite and brackets treated with diazonium/Bis-GMA were significantly higher than
untreated (control) brackets for all bracket groups (Figures 6.5). Tensile bonding strengths
between Bis-GMA and treated brackets for groups R, L, and S were 4.62±0.87, 4.15±1.00, and
4.49±1.30 MPa, respectively, and they are significantly higher than untreated brackets
(1.41±0.64, 1.57±0.99, and 2.22±1.39 MPa respectively) (Figure 6.5). The shear bonding
strengths of brackets in groups R, L, and S that were treated with diazonium/Bis-GMA and
bonded to teeth with Bis-GMA composite were significantly higher 3.83±1.47, 6.67±2.52 and
6.71±2.51 MPa, respectively, than the untreated brackets 1.94±1.25, 1.84±1.07, and 1.72±1.06
MPa (Figure 6.5).

96
From the mechanical tests results, tensile and shear bond strengths for the untreated (control)
brackets to Bis-GMA composite were almost similar and not significantly different between
control groups in R, S, and L. However, the baseless brackets in group R are better than brackets
with bases (groups S and L) in the tensile bond strength after diazonium/Bis-GMA treatment
while brackets with bases in groups S and L are better than the baseless brackets (group R) in the
shear bond strength after diazonium/Bis-GMA treatment.
Figure 6.5: (a):The ultimate tensile force N (Left) and bond strength MPa (Right) of the different stainless steel brackets
R, L, and S that were untreated (control) or treated with diazonium/Bis-GMA treatment and bonded to another bracket
with Bis-GMA composite. (b):The ultimate shear force N (Left) and bond strength MPa (Right) of the different stainless
steel brackets R, L, and S that were untreated (control) or treated with diazonium/Bis-GMA treatment and bonded to
teeth with adhesive based on Bis-GMA. * indicates significant difference between the different groups (p< 0.05).
97
6.5. Discussion
Numerous studies have been done to improve the bonding strength between polymers and metals
[33-36]. However, very little studies have been reported for improving the bonding between
metallic brackets and composite adhesive aside from studies based on micromechanical
interlocking with textured bracket bases [9, 18, 19]. Within the limit of our knowledge, this is the
first study improved the chemical bonding between brackets and adhesive composite.
The chemical bonding between metallic brackets and adhesive composite in this study was
achieved in two solutions. The first solution (primer) was formed a grafted layer of
aryldiazonium salts on the bracket, and the reaction started by diazotisation of p-
phenylenediamine (PPD) and sodium nitrite (NaNO2) in acidic solution (Figure 6.3.a). Then, the
aryldiazonium salt was reduced chemically by adding hypophosphorous acid (H3PO2) as a
reducing agent to form aryl radicals (Figure 6.3.b), that bind to metallic brackets (Figures 6.3.c)
[28]. The second solution (adhesive) was designed to change the amino ends of the grafted layer
(-C6H4-NH2) into diazonium radicals (-C6H4-N2•) using H3PO2 (Figure 6.3.d), and then grow
layers of Bis-GMA on it (Figure 6.3.e). Bis-GMA chains were longer after adding the benzoyl
peroxide (BP) that would achieve high bond strength to adhesive composite (Figures 6.3.f).
The presence of diazonium/Bis-GMA treatment on the stainless steel bracket surfaces was
confirmed by XPS. Chromium (Cr 2p) and iron (Fe 2p3), which are the characteristic
constituents of stainless steel alloys, were only showed in the XPS survey of the untreated
brackets. Carbon (C1s) in the untreated group was probably was probable due to the unavoidable
air contamination upon exposed to air prior to XPS analysis since the high resolution carbon
(C1s) spectra revealed the presence of carbon peaks at C-C, C-O, and O-C=O which is consistent
98
with samples of air alone [37]. As expected, the total amount of carbon (C1s) found on the
treated group was higher than that found in the untreated (control) group while chromium and
iron concentrations became negligible most likely due to the presence of a Bis-GMA layer on
bracket surfaces. Furthermore, the high resolution carbon (C1s) spectra for the treated brackets
presented carbon peaks (C=C, C-C, C-O, and O-C=O) that corresponding to pure Bis-GMA
samples (Figure 6.4) [5].
The bonding between stainless steel brackets and Bis-GMA was assessed with two different
debonding tests. The tensile bond strength test measured the direct bond strength between the
bracket and Bis-GMA composite resin while the shear bond strength test mimicked the
debonding of brackets on teeth [38]. Brackets used in this study were either baseless (group R) or
with bases (groups L and S). Typically, bracket bases are designed with micromechanical
interlocking to increase the surface area of brackets and the bonding between brackets and Bis-
GMA composite [9, 38, 39]. The mechanical tests showed that brackets bases gain minor
improvements for tensile and shear bond strength between brackets and Bis-GMA composite
before the treatment, and they were not statistically significant to baseless brackets group.
However, brackets bases help for increasing the shear bond strengths after using diazonium/Bis-
GMA treatment.
Diazonium/Bis-GMA treatment increased the tensile bond strength between Bis-GMA resin and
brackets by 3.3, 2.6, and 2.0 folds in groups R, L, and S respectively (p< 0.05) while the
treatment increased shear bond strength by 2.0, 3.6 and 3.9 folds respectively (p< 0.05) for
similar groups (Figure 6.5). The increase of tensile bond strength in baseless brackets (group R)
was higher than in brackets with bases (group L and S), while the increase of shear bonding
99
strength for brackets with bases (group L and S) was higher than baseless brackets (group R).
This means that baseless brackets (group R) benefit more from the diazonium/Bis-GMA
treatment in tensile bond strength that assess direct bonding between brackets and composite [9,
38]. Whereas, brackets with bases (groups L and S) benefit from the treatment in shear bond
strength probably because the bases was designed with micromechanical interlock providing
high retention to composite and exhibiting more friction during shear testing [9, 38].
Increased bond strength between brackets and Bis-GMA composite through diazonium/Bis-
GMA treatments can be utilized to reduce the debonding of orthodontic brackets, a common
occurrence in clinical practice that prolongs treatment duration and chair time [13]. Thus, fixed
appliances therapy would be more effective and resistance to failure after using diazonium/Bis-
GMA treatment on brackets than without treatment. By increasing bond strength between
brackets and composite, more leverage is possible for complex orthodontic mechanics that
usually failed because the debonding [16, 17]. Moreover, the bands around teeth in fixed
orthodontic treatments could become obsolete when the strong bonding of buccal tubes to molar
teeth is attained using diazonium/Bis-GMA treatment [4]. Using buccal tubes in the orthodontic
treatment provide better esthetics, comfort, and oral hygiene than using molars [4].
Increased bond strength between brackets and Bis-GMA composite can also be applied to
bracket design by decreasing bracket size from 50 to 74% of its original size. S brackets are the
smallest available metallic brackets produced by in 3M Unitek; and they are designed for the
mandible anterior teeth while L brackets are designed for the maxillary anterior teeth with
corresponding bracket bases 28% larger than those of the S bracket. According to our results, it
would be possible to use S-sized brackets on the maxillary anterior teeth (Figure 6.6.b) instead of
100
using the L bracket (Figure 6.6.a). Moreover, the manufacturers of orthodontic brackets would
be able to design brackets with bases of half their current size, or smaller, according to the
bonding strength results presented in this study (Figure 6.6).
Using small brackets size is beneficial for patients and orthodontists; it can improve the patients’
primary concern of esthetics while undergoing fixed orthodontic treatment [1]. Smaller brackets
are also more comfortable for patients since they cause less oral tissue irritation than larger
brackets. Using small orthodontic brackets provides better oral hygiene than large one because
food impaction around and beneath the brackets will be reduced and cleaned easily preventing
tooth caries [7, 14, 39, 40]. The small amount of residual composite on the teeth after finishing
orthodontic treatments using small brackets could helps orthodontists to reduce the chairside
time when removing the residual composite from the teeth; and it also minimize the negative
impacts of the residual composite on teeth when have smaller amount of demineralization and
less etched area of teeth [7, 14].

101
Figure 6.6: Photograph of untreated L bracket group (a) and treated S bracket group (b) that were bonded to the
anterior teeth using Bis-GMA composite. The bracket in (b) was treated with diazonium/Bis-GMA and its shear bond
strength (47.65±17.85 N) was 364% higher than the shear bonding strength (18.03±10.50 N) of bracket (a) while its size is
28% less and the size of (a). (c) drawing shows fixed orthodontic appliances with the original size of metallic brackets
bonded on teeth, and (d) brackets with bases 50% smaller size than original brackets as a results of using diazonium/Bis-
GMA treatment.
6.6. Conclusion
The treatment of the metal orthodontic brackets with diazonium ions in an emulsion containing
Bis-GMA (Bisphenol A-glycidyl methacrylate) monomer, an emulsifier (SDS), and an initiator
(BP) increased the bond strength between brackets and Bis-GMA composite. The
diazonium/Bis-GMA treatment increased the bonding strength between Bis-GMA and brackets
by 2 to 3.9 folds compared to untreated brackets. Although brackets bases provide minor
improvement of the bond strength between brackets and composite, it helps for increasing the
shear and tensile bond strength after using diazonium/Bis-GMA treatment. This bonding
technique could be used to prevent bracket debonding, treat complex orthodontic cases requiring
increased leverage, and decrease the size of metal brackets by at least 50%.

102
Acknowledgments
The authors would like to acknowledge King Saud University in Saudi Arabia, Riyadh; Natural
Sciences and Engineering Research Council (NSERC) of Canada–Discovery grant; the
Fondation de l’Ordre des dentists du Québec (FODQ), and Le Réseau de recherche en santé
Buccodentaire et osseuse (RSBO) for their financial support.
6.7. References
1. Shukla, C., et al., Comparison of Mean Shear Bond Strength of Light Cure, Self-Cure
Composite Resins, Self-Etching and Moisture-Insensitive Primers: An in vitro Study. J
Indian Orthod Soc, 2012. 46(3): p. 61.
2. Maijer, R. and D. Smith, Variables influencing the bond strength of metal orthodontic
bracket bases. Am J Orthod, 1981. 79(1): p. 20-34.
3. Bazakidou, E., et al., Evaluation of frictional resistance in esthetic brackets. Am J Orthod
Dentofacial Orthop, 1997. 112(2): p. 138-144.
4. Grist, F. Basic guide to orthodontic dental nursing. 2010.
5. Sakaguchi, R.L. and J.M. Powers. Craig's restorative dental materials. 2012.
6. Blatz, M.B., A. Sadan, and M. Kern, Resin-ceramic bonding: A review of the literature. J
Prosthet Dent, 2003. 89(3): p. 268-274.
7. Bishara, S.E., et al., The effect of repeated bonding on the shear bond strength of a
composite resin orthodontic adhesive. Angle Orthod, 2000. 70(6): p. 435-443.
8. Brantley, W.A. and T. Eliades. Orthodontic materials scientific and clinical aspects.
2001.
9. Sharma-Sayal, S.K., et al., The influence of orthodontic bracket base design on shear
bond strength. Am J Orthod Dentofacial Orthop, 2003. 124(1): p. 74-82.
10. Gill, D.S.N.F.B. Orthodontics principles and practice. 2011.
11. Christensen, G.J. A consumer's guide to dentistry. 2002.
12. Melsen, B. Adult orthodontics. 2012.
13. Wendl, B., et al., Comparative bond strength of new and reconditioned brackets and
assessment of residual adhesive by light and electron microscopy. Eur J Orthod, 2011.
33(3): p. 288-292.
14. Horiuch, S., et al., Enamel bonding of self-etching and phosphoric acid-etching
orthodontic adhesives in simulated clinical conditions: Debonding force and enamel
surface. Dent Mater J 2009. 28(4): p. 419-425.
15. Årtun, J. and S. Bergland, Clinical trials with crystal growth conditioning as an
alternative to acid-etch enamel pretreatment. Am J Orthod, 1984. 85(4): p. 333-340.
16. Nanda, R.K.S. Current therapy in orthodontics. 2010.

103
17. Nanda, R. and M. Upadhyay, Sheldon Friel Lecture 2011Skeletal and dental
considerations in orthodontic treatment mechanics: a contemporary view. Eur J Orthod,
2012.
18. Keizer, S., J.M. ten Cate, and J. Arends, Direct bonding of orthodontic brackets. Am J
Orthod, 1976. 69(3): p. 318-327.
19. Bishara, S.E., et al., Effect of a fluoride-releasing self-etch acidic primer on the shear
bond strength of orthodontic brackets. Angle Orthod, 2002. 72(3): p. 199-202.
20. Gam-Derouich, S., et al., Diazonium Salt-Derived 4-(Dimethylamino) phenyl Groups as
Hydrogen Donors in Surface-Confined Radical Photopolymerization for Bioactive Poly
(2-hydroxyethyl methacrylate) Grafts. Langmuir, 2012. 28(21): p. 8035-8045.
21. Mahouche-Chergui, S., et al., Aryl diazonium salts: a new class of coupling agents for
bonding polymers, biomacromolecules and nanoparticles to surfaces. Chem Soc Rev,
2011. 40(7): p. 4143-4166.
22. Chehimi, M.M.W.I. Aryl diazonium salts new coupling agents in polymer and surface
science. 2012.
23. Adenier, A., et al., Study of the spontaneous formation of organic layers on carbon and
metal surfaces from diazonium salts. Surf Sci, 2006. 600(21): p. 4801-4812.
24. Hinge, M., et al., On the electrografting of stainless steel from para-substituted
aryldiazonium salts and the thermal stability of the grafted layer. Surf Coat Technol,
2010. 205(3): p. 820-827.
25. Gam-Derouich, S., et al., A versatile route for surface modification of carbon, metals and
semi-conductors by diazonium salt-initiated photopolymerization. Surf Sci, 2011.
605(21): p. 1889-1899.
26. Delamar, M., et al., Covalent modification of carbon surfaces by grafting of
functionalized aryl radicals produced from electrochemical reduction of diazonium salts.
J Am Chem Soc, 1992. 114(14): p. 5883-5884.
27. Combellas, C., et al., Spontaneous grafting of iron surfaces by reduction of
aryldiazonium salts in acidic or neutral aqueous solution. Application to the protection of
iron against corrosion. Chem Mater, 2005. 17(15): p. 3968-3975.
28. Viel, P., et al., Covalent grafting onto self-adhesive surfaces based on aryldiazonium salt
seed layers. J Mater Chem, 2008. 18(48): p. 5913-5920.
29. Pinson, J., Attachment of Organic Layers to Materials Surfaces by Reduction of
Diazonium Salts, in Aryl Diazonium Salts2012, Wiley-VCH Verlag GmbH & Co.
KGaA. p. 1-35.
30. Mevellec, V., et al., Grafting polymers on surfaces: A new powerful and versatile
diazonium salt-based one-step process in aqueous media. Chem Mater, 2007. 19(25): p.
6323-6330.
31. Tessier, L., et al., Surface Electroinitiated Emulsion Polymerization (SEEP): A
Mechanistic Approach. Chem Mater, 2009. 21(18): p. 4261-4274.
32. Deniau, G., et al., Surface Electroinitiated Emulsion Polymerization: grafted organic
coatings from aqueous solutions. Chem Mater, 2006. 18(23): p. 5421-5428.
33. Ikemura, K., et al., Effect of the combination of dithiooctanoate monomers and acidic
adhesive monomers on adhesion to precious metals, precious metal alloys and non-
precious metal alloys. Dent Mater J, 2011. 30(4): p. 469-477.
104
34. Segerstrom, S. and I.E. Ruyter, Adhesion properties in systems of laminated pigmented
polymers, carbon-graphite fiber composite framework and titanium surfaces in implant
suprastructures. Dent Mater, 2009. 25(9): p. 1169-1177.
35. Tsuchimoto, Y., et al., Effect of 4-MET- and 10-MDP-based primers on resin bonding to
titanium. Dent Mater J, 2006. 25(1): p. 120-124.
36. Koizumi, H., et al., Bond strength to primed Ti-6Al-7Nb alloy of two acrylic resin
adhesives. Dent Mater J, 2006. 25(2): p. 286-290.
37. Cai, K., et al., Surface structure and composition of flat titanium thin films as a function
of film thickness and evaporation rate. Appl Surf Sci, 2005. 250(1): p. 252-267.
38. Iizuka, Y., et al., Bond strength of an orthodontic bonding material and adhesion energy
of artificial saliva to an experimental titanium bracket. Orthod Waves, 2011. 70(1): p. 21-
26.
39. Bishara, S.E., et al., Effect of time on the shear bond strength of glass ionomer and
composite orthodontic adhesives. Am J Orthod Dentofacial Orthop, 1999. 116(6): p. 616-
620.
40. Schaneveldt, S. and T.F. Foley, Bond strength comparison of moisture-insensitive
primers. Am J Orthod Dentofacial Orthop, 2002. 122(3): p. 267-273.

105
Chapter 7: Conclusion
Metallic surface treatment with diazonium ions can be used as substrate for polymerizing dental
polymers such as PMMA and Bis-GMA. This process results in direct covalent bonding between
dental polymers and metals that can be used to improve mechanical strength of bond between Ti
and PMMA, stainless steel wrought wire and PMMA, and stainless steel brackets and Bis-GMA
by 5.2, 2.5, and 2.0 folds respectively compared to untreated control groups. Increased bond
strength between metals and polymers used in dental devices would help to prevent their
frequent debonding and subsequent failures. This new bonding technique achieved strong
binding between metals and PMMA, and its bond strength on polished Ti to PMMA was the
strongest among the available bonding systems. The treatment can be used to make acrylic
removable dentures and appliances when only small volume of acrylic is available to support the
wire. This bonding technique based on diazonium could be used to prevent bracket debonding,
treat complex orthodontic cases requiring increased leverage, and decrease the size of metal
brackets by at least 50%.

106
Chapter 8: Appendices
8.1. Report of Invention
A report of invention was received on November, 27, 2012 for the invention entitled “bonding
between metals and polymers”.
8.2. Poster I
A poster was presented at Dentistry Research Day- McGill University on March 29, 2012.
8.3. Poster II
A poster was presented at Dentistry Research Day- McGill University on March 26, 2013.
8.4. Poster III
A poster was presented at Materials Research Society (MRS) fall-meeting 2013 at Boston, USA
on December 4, 2013.
8.5. Poster IV
A poster was presented at the Oral and Bone Health Research (RSBO) Scientific Day at the
Estrimont in Orford, QC, Canada on January 17th
, 2014.
8.6. Poster IV
A poster was presented at the American Association for Dental Research (AADR/CADR)
Annual Meeting, Charlotte, USA on March 20th, 2014.

107

108

109

110

111




![Bonding between Atoms [4] - Unesp](https://static.fdocuments.us/doc/165x107/61c7749506afd0620067c2dc/bonding-between-atoms-4-unesp.jpg)













