
Bodrum – 21/08/2011. Outline 1.Introduction -History, Radiation damage - Cancer “epidemic” 2....
52
Bodrum – 21/08/2011
-
Upload
ferdinand-maxwell -
Category
Documents
-
view
216 -
download
2
Transcript of Bodrum – 21/08/2011. Outline 1.Introduction -History, Radiation damage - Cancer “epidemic” 2....

Bodrum – 21/08/2011

Outline1.Introduction -History, Radiation damage - Cancer “epidemic”
2. Treatment of Cancer Issues of Importance Forms of radiation treatment Energy deposited versus depth in matter Intensity Modulated Radiation Therapy Fractionation in Radiation Therapy
3. Advantages in Hadron Radiation Therapy Bragg Peak and sparing of tissue Successful Tumour regression
4. Other considerations Effect of nuclear reactions – charged particles - neutrons Choice of accelerators Beam transport Moving organs Treatment planning and dose verification
Bodrum – 21/08/2011

Radiation – A Blessing
Hand with ring
Right Coronary ArteryBodrum – 21/08/2011
Radiation Damage in Biological Systems
• In biological organisms, radiation damage occurs due to the ionisation of atoms and molecules in cells.
• The production of ions can result in chemical reactions which breakmolecular bonds in proteins and other important biological molecules.
• Typically 1-> 40 eV of energy is needed to ionize a molecule or atom, thus radiations such as and which can have energies in the 100keV to few MeV range, can individually result in the ionisation of thousands of atoms or molecules.
• Biological damage can subsequently result either by cells beingkilled or mutating (which can result in cancer). A large enough dosewill destroy sufficient numbers of cells to kill the organism.
Bodrum – 21/08/2011

Bodrum – 21/08/2011

by age 65
over lifetime
lifetime risk
by age 65
over lifetime
lifetime risk
Bladder 0.7 3.3 1 in 30 0.2 1.3 1 in 79Brain and CNS 0.4 0.7 1 in 147 0.3 0.5 1 in 207Breast … … … 5.6 10.9 1 in 9Cervix … … … 0.6 0.9 1 in 116Kidney 0.4 1.1 1 in 89 0.2 0.6 1 in 162Large bowel 1.4 5.7 1 in 18 1.1 4.9 1 in 20Leukaemia 0.4 1.0 1 in 95 0.3 0.8 1 in 127Lung 1.7 8.0 1 in 13 1.0 4.3 1 in 23Melanoma 0.4 0.7 1 in 147 0.5 0.9 1 in 117Multiple myeloma 0.1 0.6 1 in 177 0.1 0.5 1 in 204Non-Hodgkin lymphoma 0.6 1.4 1 in 69 0.4 1.2 1 in 83Oesophagus 0.4 1.3 1 in 75 0.2 1.1 1 in 95Ovary … … … 0.9 2.1 1 in 48Pancreas 0.3 1.0 1 in 96 0.2 1.1 1 in 95Prostate 0.9 7.3 1 in 14 … … …Stomach 0.5 2.3 1 in 44 0.2 1.2 1 in 86Uterus … … … 0.6 1.4 1 in 73
% of cohort that develop cancer
Table 5.1: Risk of being diagnosed with cancer by age 65 and over a lifetime, England and Wales, 1997
Males Females
Bodrum – 21/08/2011

2%
6%8%
14%
15%23%
35%36%
46%
48%51%52%54%
61%
73%77%
87%2%
6%
7%12%13%
23%36%
45%47%47%
47%62%
64%65%
77%
96%
PancreasLung
OesophagusStomach
BrainMultiple myeloma
LeukaemiaOvaryKidneyColon
Rectum NHL
BladderCervix UterusBreast
MelanomaPancreas
LungOesophagus
BrainStomach
Multiple myelomaLeukaemia
KidneyNHL
RectumColon
LarynxBladderProstate
MelanomaTestis
Wom
en
Men
Five-year relative survival
10-50% survival: 32% of cases
More than 50% survival:
less than 10% survival:
More than 50% survival:
10-50% survival: 22% of cases
less than 10% survival:
Five year age standardised relative survival (%), adults diagnosed 1996-1999, (England & Wales by sex and site)
Bodrum – 21/08/2011

Cancer is characterised by a disorderly proliferation of cells that can invade adjacent tissues and spread via the lymphatic system or blood vessels to other parts of the body.
Cancer
Bodrum – 21/08/2011

Treatment of Cancer
1. Surgery to excise or resection a tumour
2. Chemotherapy
3. Radiation treatment
Treatment is highly individual. It depends on the organ
Involved, the nature of the tumour, its size, its location
relative to other organs etc. All of these factors will
Influence the oncologist in deciding what treatment to
propose. The treatment may be any combination of 1-3.
Bodrum – 21/08/2011

Some issues of Importance in Treatment using radiation
1. Hypoxia – tumours may outgrow their blood supply and they run out of Oxygen, which is highly radiosensitive.
2. High LET (Linear Energy Transfer) – the higher the density of ionisation the greater the fraction of damage to the DNA/Cell is due to direct rather than indirect action.
3. Side scatter – The way in which photons scatter means that there is much more sideways scattering than in the case of hadron beams. This exposes the normal tissue to a greater risk of secondary malignancy.
4. Number 3 is particularly important if tumour is close to another organ sensitive to radiation. This is particularly bad for children – roughly speaking 30% experience a 2nd. Malignancy after five years.
Bodrum – 21/08/2011

Forms of Radiation Treatment
1. Brachytherapy – A sealed source is placed close to the tumour. This maximises the dose to the tumour and minimises radiation to normal tissue further away. Good for cervix, prostate, breast etc
2. Unsealed sources – taken by infusion or ingestion. Usually chosen so that the radioisotope is selectively absorbed by the affected organ. Examples – 131I which selectively goes to the thyroid or 153Sm lexidoman which goes to damaged bone and spares normal bone. Advantage is that it is highly focussed on organ concerned but technique is limited to a few situations.
3. External beam – either of photons or hadrons. In former case the source of photons can be a large 60Co source or bremsstrahlung from an electron beam produced by an electron linear accelerator. By far the most commonly used hadron beams are proton and carbon beams although other beams have been used in the past. Typically cyclotrons are used to produce the proton beams and the carbon beams are produced in a synchrotron.
Bodrum – 21/08/2011
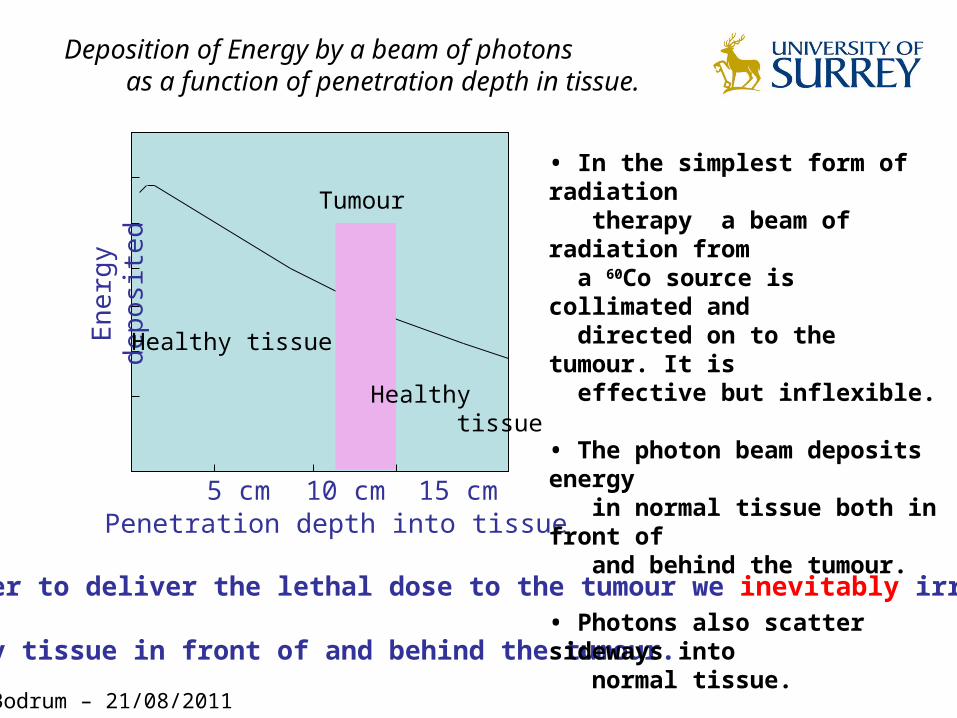
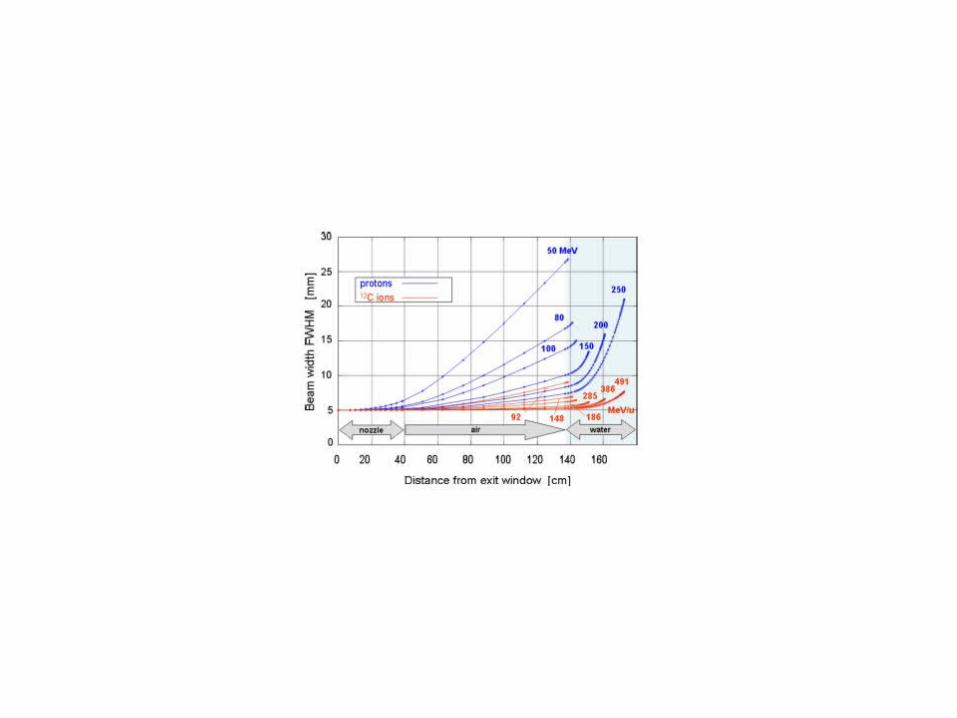
In order to deliver the lethal dose to the tumour we inevitably irradiate
healthy tissue in front of and behind the tumour.
Penetration depth into tissue5 cm 10 cm 15 cm
En
erg
y d
epo
site
d
Tumour
Healthy tissue
Healthy tissue
Deposition of Energy by a beam of photons as a function of penetration depth in tissue.
• In the simplest form of radiation therapy a beam of radiation from a 60Co source is collimated and directed on to the tumour. It is effective but inflexible.
• The photon beam deposits energy in normal tissue both in front of and behind the tumour.
• Photons also scatter sideways into normal tissue.
Bodrum – 21/08/2011

Bodrum – 21/08/2011

Bodrum – 21/08/2011

Intensity Modulated Radiation Therapy.
1. Using the two beams reduces the fraction of radiation in normal tissue
2. We can readily extend this idea to the use of multiple beams from different directions. This is now the method of choice since it reduces the risk of secondary malignancies.
3. Typically irradiation from 9 directions is used.
4. How does it work? - First a CT scan is used to define the position and extent of the tumour and the positions of any nearby structures. - Computer simulation is then used to plan the beam direction, shape etc so that the full extent of the tumour is irradiated. - Number of beams is decided.
Bodrum – 21/08/2011

Bodrum – 21/08/2011

Fractionation in Radiation Therapy.
1. As indicated on the previous slide the radiation is not all delivered at once.
Typically in the U.K. and elsewhere it is delivered in a series of “fractions”
- a dose of about 60-70Gy is delivered in 1.8-2 Gy at a time.
2.Why fractionation? - a) It allows normal cells time to recover Tumour cells are generally less efficient in repair between fractions. - b) tumour cells in relatively radio-resistant phase may cycle into sensitive phase - c)Tumour cells chronically or acutely hypoxic may re-oxygenate between fractions.
Normal cells
Tumour cells
Cell recovery impossible below this line
Each arrow represents a dose
Lethal dose
Bodrum – 21/08/2011

Normal cells
Tumour cells
Cell recovery impossible below this line
Repopulation
Each arrow represents a dose of radiation
Lethal dose
• Sometimes the fractionation has to be speeded up because if it takes too long the tumour may have time to repopulate. • For children fractions are often smaller to reduce the incidence of late onset side effects.• Sometimes two fractions/day are used towards the end because tumours regenerate more quickly when smaller.
Bodrum – 21/08/2011
Bodrum – 21/08/2011

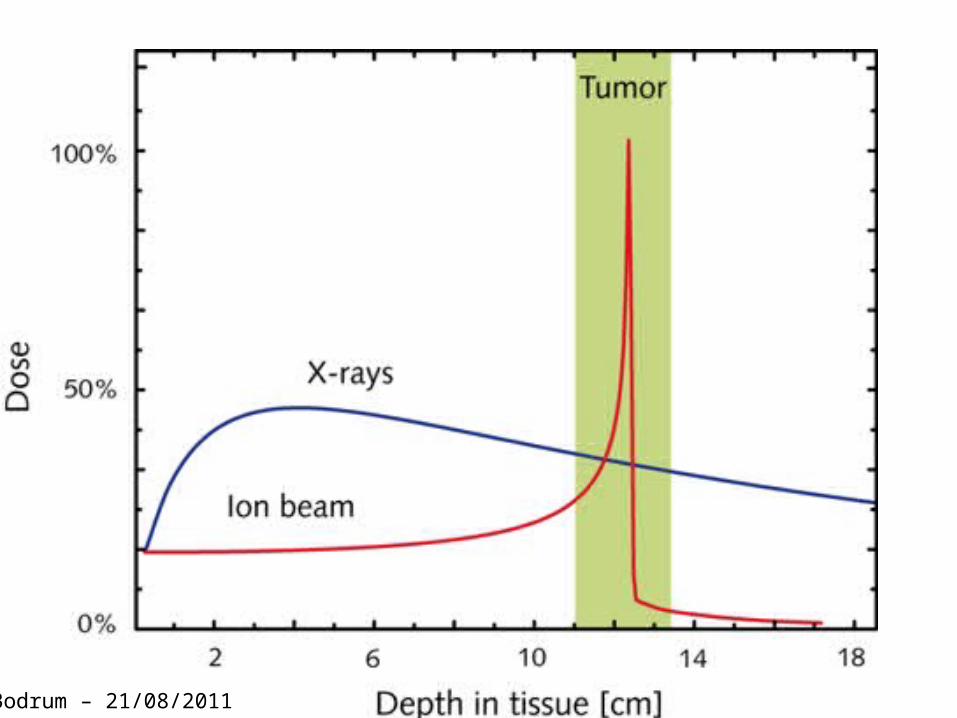
Note:- A 10% increase in dose to the tumour typically produces a 20% improvement in the tumour control rate from 50 – 60%.Hadron beams are readily controlled – we can spread out the Bragg Peak by varying the beam energy and rastering the beam.
Bodrum – 21/08/2011

Dose Distributions for Photons (X-rays)and hadrons (protons and carbon ions)
Single field ofPhotons or hadrons
Bodrum – 21/08/2011

We can also irradiate from different directions with hadrons. In other words Intensity Modulated Hadron Therapy
Dose map for Photons (X-rays) and ProtonsBodrum – 21/08/2011

Prior to therapy 3 months after carbon ion therapy
total tumor dose 60 GyE
Tumor regression
Bodrum – 21/08/2011

Tumor regression (Chordoma)
Prior to therapy 6 weeks after treatment(Axial NMRI Scan)
Bodrum – 21/08/2011

Bodrum – 21/08/2011
Bodrum – 21/08/2011

Bodrum – 21/08/2011

Some other Considerations
•All of that seems very straightforward – It is not so easy in practice
•There are some other things to consider - Effect of nuclear reactions – charged particles - neutrons
- choice of accelerators
- beam transport
- moving organs
- Treatment planning and dose verification
Bodrum – 21/08/2011

Fragmentation Reactions
• Stopping process is dominated by collisions with atomic electrons
• Probability of nuclear collisions is tiny by comparison but it has significant effects particularly at large penetration depths
• Central collisions – complete disintegration
• Peripheral collisions - fragmentation
Bodrum – 21/08/2011

Fragmentation Reactions
• Peripheral collisions – fragmentation –most frequent reactions because of geometry
• Well described by Abrasion-ablation model of Serber – two step process
• First step – nucleons are abraded in overlap(fireball) region.Remaining nucleons are spectators.
• Second step – projectile and target fragments evaporate nucleons and clusters of nucleons as well as gammas.
Bodrum – 21/08/2011

Fragmentation Reactions
• What effects does this have for therapy? There are three.
1.Nuclear reactions cause a loss of primary beam particles and a build up of lower Z fragments – these effects becoming more and more important with increasing penetration depth.
2.The secondary beam-like fragments have essentially same velocity as beam - thus they have a longer range and produce a tail beyond the Bragg peak
3. Angular distributions of fragments are determined by kinematics and are focussed in forward direction but they have a much larger lateral spread than the primary ions where the spread is mainly due to multiple Coulomb scattering.
Bodrum – 21/08/2011

Fragmentation Reactions
• Cross-section for charge changing Reactions is smaller for 12C than for 10B or 14N – Shell effects
• 52% of 12C ions reach Bragg peak at 16cm depth in H2O
• Tail beyond Bragg peak is mainly composed of H and He.
• Bragg Peak/Entrance ratio decreases with energy or penetration depth
• Bragg peak broadens and tail extends
All these effects reduce effectivenessof treatment but are well understood.
D.Schardt et al,GSI-Report 2008

Neutrons from Reactions
• All modalities produce neutrons – photons, protons, carbon ions
• They are produced in reactions on beam focussing elements and in the body – remember the body is mostly water.
• Early facilities placed shielding close to the body – as a result a high flux of neutrons in the forward direction was incident on the body.
• Carbon ions – At 200 Mev/u stopping in H2O we get 0.54 neutrons/ion on a 125 cm3 target volume we get < 8mGy per treatment Gy
• Comparing neutron doses from protons and carbon ions it is found that they are comparable because although the carbon produces more neutrons the primary beam of protons needed to give the same dose is much larger
• The doses are included in the treatment planning
Bodrum – 21/08/2011
Choice of Accelerators
• In research the key feature we want from an accelerator system is flexibility
• In Therapy we require reliability and stability of operation and extreme care in beam control.
• This is the key to operation in a clinical environment and to patient safety.
Bodrum – 21/08/2011

Choice of Accelerators
• For Heavy ions the choice is between Cyclotrons and Synchrotrons.
• Cyclotrons are - easy to operate - highly reliable - compact - commercially available and relatively less expensive - Beam intensity stable and readily controlled but no energy variation other than by degraders.
• Synchrotrons are - Fast energy variation on pulse by pulse basis - but they need an injector and a delicate extraction system
• Other types – Very active area of research to develop more compact machines that fit easily in a clinical setting.e.g Laser Wakefield accelerator, FFAG (fixed focussing alternating gradient ring, an induction linac based on high-gradient insulators.
Bodrum – 21/08/2011

Beam Transport
• Basic choice is between passive and active systems or a combination.
Delivery system takes beam to the Tumour, distributes it over the targetVolume accurately and homogeneously
Choices – fully passive or fully active
Passive – beam is adapted in 3D to the target volume by passive non-variable field shaping elements
Beam is first broadened by a scattering system.Bragg peak is spread out by a range modulator to cover tumour depthSpread out Bragg peak(SOBP) can be shifted in range by absorber plates.
Collimator cuts out field area as defined by largest target contour.Range compensator adjusts the distal depth pattern taking into account Complex tissue composition. These are patient specific.
Major Limitation – Fixed width of SOBP. Bodrum – 21/08/2011
Beam Transport
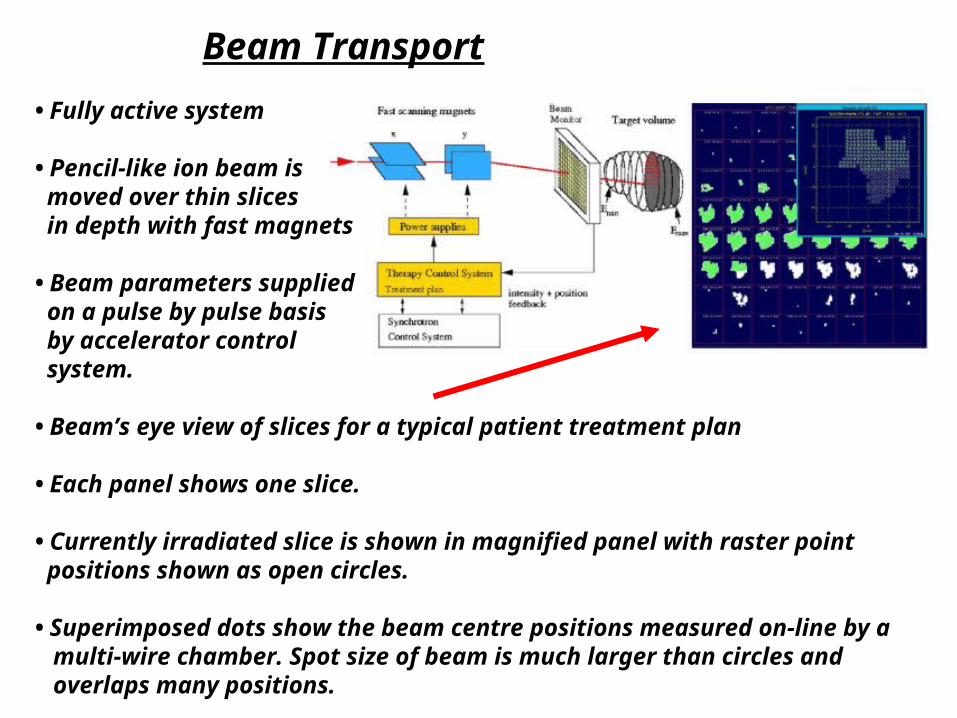
• Fully active system
• Pencil-like ion beam is moved over thin slices in depth with fast magnets
• Beam parameters supplied on a pulse by pulse basis by accelerator control system.
• Beam’s eye view of slices for a typical patient treatment plan
• Each panel shows one slice.
• Currently irradiated slice is shown in magnified panel with raster point positions shown as open circles.
• Superimposed dots show the beam centre positions measured on-line by a multi-wire chamber. Spot size of beam is much larger than circles and overlaps many positions.
Beam Transport
• Advantages – No patient-specific or field-specific hardware needed and so any irregular volume can be filled.
- Dose can be varied voxel to voxel to compensate for a)any pre-irradiation, b)contributions from secondary fragments, c) variations in RBE
• Disadvantages – Very Strict demands on control and safety systems
- Strict demands on accelerator performance - stability - reproducibility of beam position
• In GSI raster scan system (3D system) single ion is delivered to individual spot to 10-6 m precision. System stops irradiation if measured parameters are outside accepted tolerances. There are also redundant measures of dosimetric parameters for safety.
Bodrum – 21/08/2011

Moving Organs
•To date scanning beams have mainly been applied to organs that can be immobilised. The full power of the system to fill an irregular tumour is exploited.• Abdomen and Thorax-one cannot avoid breathing,heart pulsation, bladder and gut filling. Much more serious for hadrons than photons.•Solutions- Expansion of target volume, rescanning-many repeated irradiations at lower dose, gating(for example at maximum of exhalation there is a flat period. Thus one can gate on this and only irradiate whilst it is flat.),tracking
Spatial shift ofTarget volume inThorax during breathing
Bodrum – 21/08/2011

Treatment Planning and Dose Verification• Step 1. – define and delineate the target volume. CT used to get quantitative information on anatomical structures. Has to be done in same conditions as for irradiation. Often used together with PET and nMRI
• 3D model of treatment geometry is made to find suitable beam directions avoiding critical structures. For hadrons only a few directions are necessary. In general total dose to the body is lower for hadrons than for photons.
• Modelling needed to ensure equal doses to every voxel in target is highly complex – optimum superposition of 10-20,000 pencil beams with individual energy, position and particle number to reach required dose. This involves getting the RBE right for each voxel.
Skull base tumour treated at GSI, biologicallyEffective dose distribution achieved withPlanning system –excellent sparing of critical Organs(brain stem and optical nerves) with three fields
Bodrum – 21/08/2011
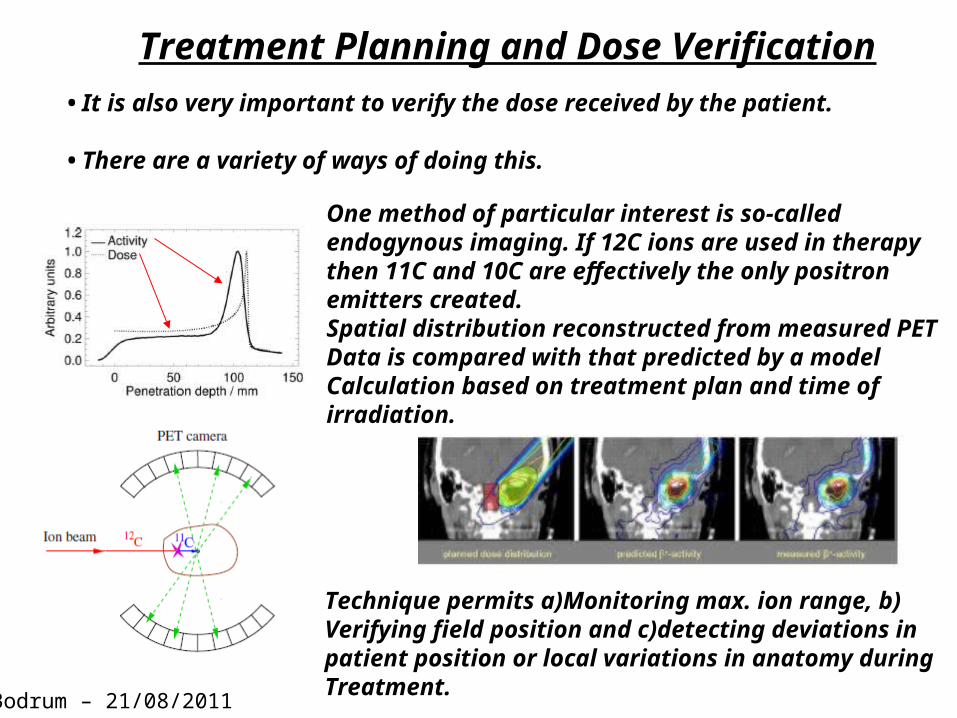
Treatment Planning and Dose Verification• It is also very important to verify the dose received by the patient.
• There are a variety of ways of doing this.
One method of particular interest is so-called endogynous imaging. If 12C ions are used in therapythen 11C and 10C are effectively the only positronemitters created.Spatial distribution reconstructed from measured PETData is compared with that predicted by a model Calculation based on treatment plan and time of irradiation.
Technique permits a)Monitoring max. ion range, b)Verifying field position and c)detecting deviations in patient position or local variations in anatomy duringTreatment.
Bodrum – 21/08/2011

Hadron Therapy
• Hadron Therapy is demonstrably successful and is increasing in use with new facilities under construction in Germany, France, Italy, etc
• At present Synchrotron is best machine for this application
• A fully active beam transport system is possible which reduces irradiation of normal tissue
• It benefits from endogynous imaging.
• D.Schardt et al., Rev.Mod.Phys.82 (2010) 383 and references therein.
Bodrum – 21/08/2011


Genetic Information
● Information needed for production and functioning of new organism is carried in the chromosomes of the germ cells (sperm and ova)
● Normal human somatic cell contains 46 chromosomes
● Mature sperm and ovum cells contain 23 chromosomes each.
● On fertilisation the resulting cell, called a zygote, contains full 46.
● This happens in a fallopian tube, after 8-10 days it migrates to the uterus
● Over 9 months successive divisions and differentiation occur and eventually produce the new individual.
● In every division the chromosomes`are`replicated. The units of information are carried in the DNA






Cancer & Radiotherapy• Cancer is characterised by a disorderly
proliferation of cells that can invade adjacent tissues and spread via the lymphatic system or blood vessels to other parts of the body.
• The aim of radiotherapy is to deliver enough radiation to the tumour to destroy it without irradiating normal tissue to a dose that will lead to serious complications (morbidity).

















