
Board\Papers - NHS Bury
275
Greater Manchester NHS Greater Manchester Board Meeting (The Board Meeting of the 10 Greater Manchester PCTs) To be held on Thursday, 10 November 2011 Salford Suite, St James’s House, Pendleton Way, Salford, M6 5FW AGENDA Part I 2.00 p.m. Public Meeting (a) Open Agenda for Members of Public to raise items 2.15 p.m. Start of Trust Board Meeting 1 Apologies for Absence 2 Declaration of Interests 3 Minutes of the Meeting held on 8 September 2011 (attached) 4 Matters Arising (attached) 5 Chairman’s Communications Chairman (verbal report) 6 Report of the Chief Executive Chief Executive (attached) 7 Report of the Medical Director Medical Director (attached) POLICY AND STRATEGY 8 Public Sector Reform Paper Director of Policy and External Relations (attached) PERFORMANCE 9 Performance Report Director of Nursing, Quality & Performance a. Performance b. Quality c. HR (attached) 1
Transcript of Board\Papers - NHS Bury
Greater Manchester
NHS Greater Manchester Board Meeting (The Board Meeting of the 10 Greater Manchester PCTs)
To be held on Thursday, 10 November 2011
Salford Suite, St James’s House, Pendleton Way, Salford, M6 5FW
AGENDA
Part I 2.00 p.m. Public Meeting (a) Open Agenda for Members of Public to raise items
2.15 p.m. Start of Trust Board Meeting
1 Apologies for Absence
2 Declaration of Interests
3 Minutes of the Meeting held on 8 September 2011
(attached)
4 Matters Arising
(attached)
5 Chairman’s Communications Chairman
(verbal report)
6 Report of the Chief Executive Chief Executive
(attached)
7 Report of the Medical Director Medical Director
(attached)
POLICY AND STRATEGY
8 Public Sector Reform Paper Director of Policy and External Relations
(attached)
PERFORMANCE
9 Performance Report Director of Nursing, Quality & Performance
a. Performance b. Quality c. HR
(attached)
1
10 Public Health Performance Report Director of Public Health
(attached)
11 An emerging childhood contagious infection: TB Director of Public Health
(attached)
12 Finance Report Director of Finance
(attached)
PROCESS
13 Development of Commissioning Support Services Board Director of Commissioning Development
(attached)
14 Terms of Reference Paper Board Secretary
(attached)
15 Assurance Framework Board Secretary
(attached)
16 Governance – Managing the Transition Board Secretary
(attached)
MINUTES & REPORTS
17 Report of the Audit Committee Director of Finance
(attached)
18 Audit Management Letter Director of Finance
(attached)
19 Healthy Futures Report Director of Service Transformation
(attached)
20 Clinical Commissioning Board Report Director of Policy & External Relations
(attached)
21 Locality Board Summary Document Director of Finance
(attached)
22 NHS Greater Manchester Remuneration Committee Minutes – 14 July 2011
(attached)
FOR INFORMATION 23 Any Other Business
24 Reflection
Date and Time of Next Meeting – 12 January 2012, 2pm
2

PART II
Members of the press and public are excluded from the remainder of this meeting under Section 1(2) Public Bodies (Admission to Meetings) Act 1960 Chairman: Professor. E. Fairhurst Chief Executive: Dr. M. Burrows
3

4
Minutes NHS Greater Manchester Board Meeting Date: 8 September 2011 Venue: Salford Suite, St James House, Pendleton Way, Salford, M6 5FW Present: Professor Eileen Fairhurst - Chairman
Mr Terry Atherton – Non-Executive Director Dr Mike Burrows - Chief Executive Mrs Claire Yarwood - Director of Finance
Dr Raj Patel – Medical Director Ms Jan Hutchinson – Director of Public Health Mr Warren Heppolette –Director of Policy and External Relations
Dr Julie Higgins - Director of Commissioning Development Mrs Hilary Garratt - Director of Nursing, Quality and Performance Ms Leila Williams – Director of Service Transformation
Mrs Andrea Anderson – Director of HR and OD Mr Riaz Ahmad – Non-Executive Director Dr Kailash Chand – Non-Executive Director
Mr David Edwards – Non-Executive Director Mr Paul Horrocks – Non-Executive Director Mrs Pam Senior – Non-Executive Director Mr Alan Stephenson – Non-Executive Director
Mrs Andrea Anderson – Associate Director of Human Resources and Organisational Development Ms Evelyn Asante-Mensah – Non-Executive Director Mr Michael Greenwood – Non-Executive Director Mr Rob Bellingham - Board Secretary Cllr Cliff Morris – Association of Greater Manchester Authorities (AGMA)
+ 10 members of the public/ NHS Staff Minute
No Item
11/36 Apologies for Absence
Ms Joyce Redfearn – Association of Greater Manchester Authorities (AGMA)
11/37
Declaration of Interests Mr Riaz Ahmad – Non-Executive Director – declared an interest in item 13 on the agenda, The Performance Report, indicating that his son was an employee of Pennine Acute Hospitals NHS Trust.
5

11/38 Minutes of the meetings held on 14 July 2011 The minutes of the meeting held on the 14th July 2011 were approved as a correct record of the meeting with the following two amendments:
• Item 11/30, the fourth bullet point to be removed, Board did not agree to create locality management footprint for Bolton, Manchester, Salford and Trafford, but to undertake further discussions to finalise the arrangements in these localities.
• Item 11/34, the minute should read that it was agreed that all future Board meetings should take place in Salford.
11/39 Matters Arising: Appointment of Vice Chairman, Audit Committee Chair and Remuneration and Terms of Service Committee Chair Professor Fairhurst confirmed the following appointments, which had been discussed at part 2 of the Board meeting held on 14th July: Vice Chairman:
• Mr Terry Atherton – Non-Executive Director and • Mr Michael Greenwood – Non-Executive Director
Audit Committee Chair:
• Mr Riaz Ahmad – Non-Executive Director Audit Committee Members:
• Mr Paul Horrocks – Non-Executive Director • Mr Alan Stephenson – Non-Executive Director • Ms Evelyn Asante-Mensah – Non-Executive Director
Remuneration and Terms of Service Committee Chair:
• Mr Terry Atherton – Non-Executive Director Remuneration and Terms of Service Committee Members:
• All Non Executive Directors Report of the Chief Executive (14 July minute 20) Dr Burrows confirmed that he had met with representatives from Manchester and Oldham Councils and was planning to meet with Bury Council. It was confirmed that the action relating to GP Commissioner sign off of the options and underpinning business cases for the Healthy Futures consultation process had been completed. It was confirmed that the action relating to annual report sign off in localities had been completed.
6
Corporate Governance Manual (14 July minute 22) Dr Burrows confirmed that no requests for amendment to the Corporate Governance Manual had been received. Mr Greenwood indicated that he had a query with regards to the minute of this item, he highlighted that he had been unable to attend the previous meeting but had given the Chairman his comments and proposal that maximum subsidiarity should be given to localities in the decision making process. Mr Atherton shared his recollection of the Board discussion; he confirmed that Mr Greenwood’s comments had been taken into account and that although no formal resolution was passed in this regard, the schedule of reservation and delegation was felt to support this way of working and therefore had been approved on this basis, Mr Horrocks advised that he did agree with some of the points raised by Mr Greenwood, in particular how to ensure minimum duplication of work. Professor Fairhurst suggested that this item be added to the agenda for further discussion at the Board development session on the 15 September 2011. Public Health Performance Report (14 July minute 26) Local health profiles for all Greater Manchester districts were distributed at the meeting. Locality Management Arrangements (14 July minute 30): Ms Asante-Mensah asked for clarification with regards to the timeframe for finalising the locality management arrangements relating to Bolton, Manchester, Salford and Trafford. Dr Burrows confirmed that a meeting had taken place with Councillor Morris in Bolton. A way forward had been agreed for further operational discussions to take place. Mr Horrocks asked if the intention was to have a single management team for each footprint. Dr Burrows advised that managing resilience during the transition was a priority and that the management structures of each of the locality footprints would be context specific and dependant on specific issued within localities, such as the stage of development of Clinical Commissioning Groups.
11/40 Chairman’s Communications Professor Fairhurst shared with colleagues that she had been invited to Chair the Greater Manchester Collaborative Leadership in Applied Health Research and Care, (CLAHRC) Board.
7
The Chairman communicated that the Greater Manchester and Cheshire Cancer Network had been awarded £250,000 to fund a campaign to promote the early detection and diagnosis of Kidney and Bladder Cancer, which continues to be a challenge for Greater Manchester.
11/41
Report of the Chief Executive Dr Burrows introduced his report, in particular highlighting and asking members to note the publication of the Neuromuscular Service Review report. Dr Burrows highlighted two items requiring Board approval:
• Greater Manchester Health Protection Project. • Midwifery Led Unit Recommendations – NHS Bury, Heywood,
Middleton and Rochdale. Dr Burrows confirmed that NHS Bury and NHS Heywood, Middleton and Rochdale locality Boards agreed not to proceed with the establishment of stand alone midwifery units in Rochdale and Bury. In line with the Greater Manchester scheme of reservation and delegation, the Board of NHS Greater Manchester were asked to formally approve the locality Boards recommendations. Mrs Yarwood asked that some consideration be given to section five, Information Governance, (IG), in particular the table within the update. This demonstrated that six of the ten localities within Greater Manchester were graded unsatisfactory using the IG Assessment Tool. Assurance was given that work is to take place involving internal auditors and IG leads from each of the ten localities to make sure robust, consistent processes are in place to ensure compliance. Dr Chand questioned why two localities with same percentage score had received different performance ratings. Mrs Yarwood explained that the score is made up of different criteria with different weightings applied. Mrs Yarwood agreed to share the detailed information if required. Mr Horrocks enquired if it would be possible for NHS Greater Manchester to achieve the deadline relating to PCTs having a provisionally agreed list of property transfers by the 14th
September 2011. . Dr Burrows confirmed
that Mr Tim Evans, Managing Director, NHS Bolton, was leading on this piece of work and was confident that the 14th September deadline would be met. He confirmed that at present, LIFT Estates were not covered and that further guidance was expected with regard to the remaining estate. Mrs Yarwood clarified that Providers would be offered a package of assets, and they would be able to accept or decline the package. However it would not be possible for providers to select individual elements of the package. Mr Evans will be available help localities to mediate any issues with providers. The Board:
• Noted the contents of the Chief Executive’s report
8

• Noted the case for change and supported the continued scoping and development of the Greater Manchester Health Protection workstream.
• Endorsed the recommendations of the NHS Bury and NHS Heywood, Middleton and Rochdale Locality Boards not to proceed with the development of stand alone Midwife Led Units in Bury and Rochdale.
11/42
M/A Raj
Report of the Medical Director Dr Patel introduced his report, announcing and introducing Dr David Valentine as the new Associate Medical Director with responsibility for general practice, co-ordination of a framework for performance monitoring, professional registration and revalidation across Greater Manchester. Dr Patel confirmed that the process to recruit to two additional posts to support QIPP and clinical leadership and service design were ongoing. Dr Patel indicated that his report provided some context to the Clinical Commissioning Board proposal which featured later on the agenda. Dr Patel confirmed that since the last Board meeting, the Chairs of CCGs across Greater Manchester have established a monthly leadership meeting in the form of a CCG Chairs Council. The first meeting took place on the 6th September. The council will take on an advisory role to encourage, debate, discussion and collaborative learning. The Board noted the content of the Medical Director’s report.
POLICY AND STRATEGY
11/43 NHS Greater Manchester Delivery Plan Mr Heppolette introduced the report, stating that the NHS Greater Manchester Delivery Plan was an in year business plan that captures the key actions for delivery across all ten localities. The Board of NHS Greater Manchester will be regularly appraised with regard to the plan’s delivery. The next stage of the development process will be the development of a NHS Greater Manchester Assurance Framework to support this focus on delivery. Mr Greenwood commented that the paper was very thorough but questioned the ability to deliver the actions that need to be completed in localities without implementing the subsidiarity approach referred to in his earlier comments. Mr Greenwood also noted that a key task for the cluster is to develop a strategy for the acute sector in Greater Manchester and that this should be clearly defined within the delivery plan. Dr Burrows confirmed to Mr Greenwood that the work to develop a strategy for the acute sector is covered in section five of the report entitled QIPP Delivery. The NHS Greater Manchester Board has oversight of the work via the Programme Board.
9

Mrs Yarwood added that the Delivery Plan brings the transitional arrangements together with national expectations and local objectives. The plan therefore needed to address Greater Manchester wide issues relating to capacity, resilience and new ways of working to achieve the objectives throughout the transition. Mr Ahmad expressed concern that the Board only had oversight of the major financial and performance challenges and indicated that there should be more delegation to achieve this. The Chairman suggested that the matter of ensuring Board members have the correct oversight of issues is discussed in more detail at the Board development session. The Board:
• Endorsed the proposed Delivery Plan and requested the development of a corresponding Assurance Framework and Risk Register.
11/44
M/A Mike B
Safe and Sustainable Report Dr Burrows introduced the report, noting that the document outlined the proposed approach to achieve a configuration of hospital services across Greater Manchester that provides, safe, high quality, accessible services for the population. He indicated that current models of delivery and growing costs are unsustainable and NHS Greater Manchester is committed to developing new models of care that will leave a legacy of sustainable hospital services. The proposed work would form part of the level 3 QIPP work programme. Mr Ahmad questioned the statement outlined in section 3.3 which indicated that no hospitals would close as a result of this work. Dr Burrows clarified that the reference in the document was to District General Hospital Sites and that the document would be amended to reflect that. Mr Greenwood asked that the Board receive regular updates with regard to the progress of this work, including project deliverables and timelines. He stated that he felt that this was an important priority for Greater Manchester and should be subject to significant Board involvement and challenge. Ms Williams as the Lead Director responsible for the delivery of the QIPP Programme welcomed the level of Board interest and challenge. She committed to ensuring that the Board receive the requested project information, timeline and progress updates. Mr Greenwood asked for clarification with regard to the figure associated with the Greater Manchester funding to manage the transition, as this was not explicitly stated in the paper. Dr Burrows stated that a definite figure could not be given at this point. He indicated however, that the fund would be used as a catalyst for change and would not be used as a means of furthering unsustainable models of provision.,
10

The Board:
• Supported the establishment of a ‘Safe and Sustainable’ programme of work, owned collectively by NHS Greater Manchester, to develop new models of care.
• Agreed to establish a Greater Manchester level source of funding to manage the transition.
11/45
Clinical Commissioning Board Proposal Dr Patel introduced the paper asking for Board to approve the establishment of a clinically led Executive Committee of NHS Greater Manchester. Dr Patel outlined that the proposal would meet the statutory requirements, honour the membership regulations for PCTs and the GM agreed scheme of delegation. The Clinical Commissioning Board would be a committee of the NHS Greater Manchester Board. Dr Patel noted that within the Association of Greater Manchester PCTs existed a Commissioning Programme Board that acted for the ten PCTs across Greater Manchester. This proposal would see some of the membership of this group transferring to the new committee to ensure corporate memory. Each CCG would be asked to nominate a member from each locality area. Membership from professional groups such as finance and Public Health would also be included. Ms Asante-Mensah questioned if the membership was flexible enough, given the transitional nature of the arrangements and the need to ensure that all CCGs were represented. Dr Patel advised that the proposed membership was based on current locality PCT boundaries. Where there is more than one CCG in a locality area, a single nomination would be requested to represent all CCGs. The Board:
• Supported the proposed arrangements for the establishment of a clinically led Executive Committee of NHS Greater Manchester
• Agreed the principles and process for membership of the Committee and
• Agreed the proposed Terms of Reference for the Committee.
11/46 Greater Manchester Clinical Networks – Future Arrangements Dr Patel introduced the report explaining that currently there were a number of networks, which are engaged in specific pieces of work, mostly relating to specific disease areas. This proposal contained in the report set out a vision for a Greater Manchester Clinical Networks function to work more cohesively together and build on the work already undertaken by the Commissioning Programme Board last year to realise efficiencies and generate savings. Mr Heppolette added that the proposal also built on the emerging thinking for commissioning support and shared services across Greater Manchester. It confirms the priority of QIPP areas and secures clinical leadership for specific disease areas. It was suggested that by integrating the business
11

management arrangements, promoting more cohesive working and realigning priorities, savings and efficiencies could be made. Mrs Senior welcomed the report and stated that she was pleased to see it on the agenda. She felt the paper went some way to addressing the concern that in the past clinical networks were very provider driven, when our priority is to ensure that we will commission for the best outcomes for our population. Dr Chand asked for clarification of the membership and its relationship to a possible Clinical Senate. Dr Patel responded that at present clear guidance around Clinical Senates was not available, it is understood however that CCGs will need wider clinical representation from the acute sector and nursing. Dr Patel indicated that an integrated clinical network function would provide a platform to enable Greater Manchester to move quickly if required to set up a Clinical Senate. Dr Burrows added the Clinical Networks need to be accountable to Clinical Commissioning Groups to ensure that we commission to a common standard across Greater Manchester. Professor Fairhurst agreed that the paper proposed a way to address the inadequacies of the current system, with a view to ensuring the best services for the population of Greater Manchester The Board endorsed the proposed model for Greater Manchester’s clinical networks.
PERFORMANCE
11/47
Maintaining and Improving Quality during the Transition Mrs Garratt introduced her report, outlining its aim to set out the duties of PCT Clusters to secure and improve quality during the transition. She indicated that the paper highlighted the key actions for both NHS Greater Manchester and Local Commissioning Groups. Mr Atherton indicated the fact that when organisations go through significant organisational change, associated risks are encountered. He proposed that NHS Greater Manchester should have a robust policy to ensure people are able to flag issues and concerns regarding quality and safety easily. Dr Burrows advised the Department of Health did set out clear guideline on how to listen to the views of and treat whistle blowers. The NHS Greater Manchester Executive team will look at a local policy and bring this back to Board. The Board: Accepted the responsibilities for securing safety and quality during the transition and were supportive of the roles and duties of endorsing the
12

11/48
actions and duties of both NHS Greater Manchester and its sub structures. Performance Report Mrs Garratt introduced the report, providing the Board with an overview of key performance issues, split into three key areas, Performance, Quality and Risk. Mrs Garratt stated that the report built upon the update given to Board at the last meeting and was therefore longer in length than would routinely be the case, to ensure that the Board received a full picture of the performance pressures within Greater Manchester. Performance: The following issues were highlighted as part of this performance overview:
• Continued challenge around 18-week wait performance – Anticipated recovery by the end of September in Stockport FT and Pennine Acute, Central Manchester FT recovery position is expected to be achieved by December. Additional capacity for Paediatrics was being progressed at Alder Hey.
• Diagnostics issues remain at Pennine Acute and Central Manchester FT. Anticipated that Pennine Acute will be resolved by October. Issues at Central Manchester are more difficult because of the Paediatric element.
• NWAS – Considerable improvement in the last two months but the situation will require further close monitoring as winter approaches.
Ms Asante-Mensah asked if there was a further update with regards to additional capacity at Central Manchester as her understanding was that the additional capacity being offered from Alder Hey would not bring forward the timing of the achievement of the 18 week referral to treatment target, which is still anticipated to be December. She questioned whether the additional costs incurred would therefore represent value for money. Mrs Garratt acknowledged that the additional capacity would not change the overall December trajectory for achieving the 18 week wait. However, the additional capacity would support the delivery of the duty as commissioners to meet children’s constitutional rights. The Board noted the contents of the Performance Report, the performance risks identified within it. The Board approved and mandated the recommendations outlined as follows:
• to continue to work with Providers to ensure sustained delivery of their Referral to Treatment, A&E and Diagnostic recovery plans
• to continue to work with Commissioners and Providers to deliver a material improvement in Cancer performance over the next quarter.
• to work alongside Commissioners to deliver continuing performance improvement and improved processes for system
13
management. • to ensure local commissioners and Providers continue to work
to maximise the use of re-enablement/winter planning to secure improvements in excess bed day costs and associated patient experience.
• to establish a pre-authorisation Board, tasked with tracking development of CCG towards the authorisation, supported by a series of communities of practice.
• to further develop the HR Framework to establish performance targets
Quality: Mrs Garratt introduced the Quality Report providing the Board with its first overview of the key quality areas in accordance with the National Assurance Framework arising from the publication of the Francis report on Mid-Staffordshire Hospitals., It was noted that the self assessment process in Greater Manchester took place before the introduction of the Clusters, so some of the processes will require updating for safety and quality. Mrs Garratt drew the Board’s attention to the self assessment results shown in table A and B of the report, which had been validated by the SHA. Mrs Garratt noted that these results were a snapshot in time and that since their publication Pennine Acute had done a significant amount of work on their internal assurance processes and verbal confirmation has been received from the SHA that they are now fully compliant will all aspects identified in the report. Mrs Garratt highlighted the following issues for Board’s attention:
• VTE performance risk assessment results by Provider, highlighting
that Stockport and Bolton have both failed the target. Adhering to this measure is very important in saving lives.
• Significant concern with regards to the health outcomes received for Stroke across the region with the exception of Salford, indicating significant need for improvement.
Dr Patel updated that at the first GP Council Meeting, GPs were concerned with the Greater Manchester Stroke performance and acknowledged that the model was not achieving what it should in terms of patient outcomes and required a review. Mr Greenwood stated that the results were a measure of process, rather than outcome and that, in fact there had been huge improvement in outcomes. Dr Burrows confirmed that the results of the review were evidence based and while there had been huge improvements locally, when compared nationally, Greater Manchester as a whole does not compare favourably.
14

Mr Amhad noted that it was very important to improve stroke performance, to ensure improved quality of life for patients. The Board:
• Approved the Quality and Safety Reports key recommendations. • Approved a standardised approach to the inclusion of the quality
improvement programme in the 2012/13 contracts. • Accepted its responsibility to promote improved delivery of
Stroke Services across Greater Manchester and supported NHS Greater Manchester to use performance notices where Providers sustain a level of poor performance.
• Approved the implementation of a process to identify and develop staff who can become stronger leaders and commissioners to improve quality standards and keep patients safe from harm.
• Required that quality and safety be kept as a standing item on the Board performance report.
• Agreed that this would represent a priority issue for CCGs. Risk Report: Mrs Garratt introduced the report, acknowledging that Mr Bellingham had worked with the Governance Leads from each of the ten localities to bring together the high level risks. The next step is to work with a sub group to develop an assurance framework and harmonise the risk reporting to ensure that Board are assured that they have line of sight on the Greater Manchester high level risks. The Board noted the contents of the report and approved the next phase of the programme as follows:
• The development of an assurance process, designed to assess risk management arrangements in all localities, with areas for improvement identified together with plans for rectification.
• Development of a Greater Manchester wide thematic based approach to risk reporting by local commissioners. This will support cluster wide identification of key risk issues based on common issues and local gaps within the CCGs footprint.
• Development of a Cluster Assurance Framework for presentation at the November Board meeting.
11/49 Public Health Performance Report Ms Hutchinson presented the report, indicating that it reflected the Greater Manchester Public Health Directors recommendation to report to the Cluster Board on the following issues:
• All Age, All Cause Mortality • Performance reports considered at the preceding Directors of Public
Health meeting • Notification of set piece analysis or information commissioned by or
made available to the GM Directors of Public Health and or wider
15
stakeholders Dr Chand questioned what impact the current economic situation and the NHS reforms are having on inequalities. Ms Hutchinson acknowledged that rising unemployment particularly among young people does have an impact on aspiration and is a concern. On the whole there was an improvement in GCSE and A Level results which is positive; however the gap in inequalities is increasing between areas of affluence and deprivation. Ms Hutchinson advised that in terms of the NHS Reforms the future is still unclear and more information on the transfer of Public Health to Local Authorities is awaited. However, Ms Hutchinson reported that she had been encouraged by the interest that CCGs are taking in Public Health. Mr Edwards noted that a good example of the benefit of having Public Health within Local Authorities is their ability to effect licensing laws and the price of alcohol. Ms Asante-Mensah reminded Board that reducing inequalities can not be done in isolation, each organisation has its part to play and partnership working is key. Mr Horrocks stated his concerns with regard to the low level of NHS staff receiving the flu vaccination in previous years. Mr Horrocks questioned why the take up of the vaccination by NHS Staff was so poor. Ms Hutchinson confirmed the low level of uptake which was due to a number of factors, notably misconceptions around the potential for the vaccine to give recipients the flu the, which is completely untrue. Professor Fairhurst suggested that all Board members consider having their flu vaccination at the next Board meeting and publicising this, to dispel some of the misconceptions and to encourage staff to have the vaccination. Professor Fairhurst asked that the recommendation in the Public Health Report be changed from noted to a recommendation that Directors of Public Health ensure local performance issues are reported in their localities and relevant recovery plans are developed and delivered. The Board: Noted the Public Health performance report and agreed the proposed focus areas for future reports. Required each of the Directors of Public Health to ensure action plans are in place within localities to address the performance issues set out in this report and for these action plans to be reported to locality boards and Health and Well Being Boards.
11/50 Finance Report Mrs Yarwood introduced the report, indicating that all the Greater Manchester PCTs were forecasting achievement of their year-end financial
16

targets. The Board’s attention was drawn to the fact that the Department of Health were currently undertaking a significant number of data collection exercises, which is a considerable amount of work for locality finance teams. Mrs Yarwood stated that she had not received any comments with regards to the format of the Finance report and, consequently assumed that all Board members were happy with the current structure. The report outlined the overall financial position of the ten PCTs and highlighted risks and updates on the QIPP Programmes. Mrs Yarwood asked the Board to note the budgets that have been delegated to CCGs outlined in section eight of the report, which show some significant differences across Greater Manchester localities. Some concern was expressed that in some areas the financial responsibility for budgets has been transferred but not the responsibility to manage the contractual and quality aspects outlined in the contracts. The Board noted the content of the report.
11/51 62 Day Cancer Wait Mrs Garratt introduced the report, to brief Board on the recommendations arising from an independent review of performance against the 62 day cancer waiting time standard across Greater Manchester (and Central and Eastern Cheshire). Mrs Garratt indicated that some management resource had been secured to take the work forward and asked Board to endorse the direction of travel in terms of positioning the network and to endorse the action plan to improve performance. The Board accepted the recommendations contained within the report and commended the action plan to the GMCCN Team as a basis for ensuring an improvement in performance.
PROCESS
11/52 Delivering Effective Governance Mr Bellingham introduced his report, which set out a framework for ensuring that NHS Greater Manchester implements effective systems and processes for Corporate Governance, including the relationships between localities and the Greater Manchester cluster. The report gave an overview of the issues in terms of assurance facing NHS Greater Manchester through the transition. He asked the Board to note that Appendix 2 of the report provided an overview of all the assurance arrangements in place within Greater Manchester. Professor Fairhurst asked colleagues who attended a development session on the 28th July, which considered some of these issues, to share the salient points of the discussion at that meeting. Ms Asante-Mensah updated that her recollection was that all agreed that
17
there was a desire to get to the point of consistency across Greater Manchester, in terms of pace, direction of travel and getting CCGs to a point where they are able to take a leading role in the commissioning process, as they work towards authorisation. The consensus was that all localities wanted to move to this point as quickly as possible so that by March 2012 the Greater Manchester position was one of consistency across the patch and therefore all CCGs could proceed to shadow form, with PCTs supporting CCGs. Mr Stephenson confirmed Ms Asante-Mensah’s recollections adding that all felt that they should be focusing on this development in each locality as soon as practical. Mr Edwards questioned why when the overriding view had been that this needed to happen quickly, had the assumption that GPs should be doing this be omitted from the document. Dr Patel stated that CCG Chairs do have an aspiration to develop quickly but are often restricted because they are not able to give the assurance to locality Boards and because they can not offer the assurance locality Boards are reluctant to devolve the responsibility. Dr Patel advised that some measured risk taking in devolving responsibility is required, i.e. a light touch assurance that would allow CCGs to develop. Dr Higgins indicated that the CCG assessment criteria is becoming increasingly clear. The SHA are to run a risk assessment process based in these initial criteria as follows:
• CCG footprint and issues re co-terminosity with Local Authority • The presence of a mandate within each CCG • Direction of travel with regard to CCG
Dr Higgins added that when the SHA assesses the CCGs in terms of their Governance, it will be looking at where the CCG Shadow Board sits in reference to the Cluster Board, with a direct “line of sight” needed from the CCG to the Cluster. Dr Higgins and Dr Patel confirmed that they are in the process of visiting all CCGs over the next few months, taking a programme management approach to supporting CCGs to harmonise management support across the ten localities. Mr Atherton asked that Board formally endorse all the ten locality Boards assurance structures which were submitted and partially reflected in the document. The Board
• Noted the content of the paper • Approved the cluster management arrangements described in
sections 3 and 4 of the report • Approved the locality governance models described in section 5
18

• Mandated the requirement for these models to develop and evolve in the light of the implementation of Clinical Commissioning Groups.
11/53 Voluntary Redundancy Proposal Mrs Anderson introduced the paper, outlining that all localities within Greater Manchester were still required to reduce management costs, noting that other measures including reducing the use of agency staff, and Mutually Agreed Resignation Schemes (MARS) have already been implemented. The paper outlined the proposal to create a Greater Manchester wide voluntary redundancy and retirement scheme. Mrs Anderson confirmed that the scheme would offer the Agenda for Change terms and conditions. The draft proposal of the scheme has been circulated to Executive Directors, HR Leads and Staff representatives. Staff applying for voluntary redundancy or early retirement would have to meet strict eligibility criteria. Ms Asante-Mensah questioned the timing of the proposal as some localities may be partway through a MARS process. Mrs Anderson confirmed that the intention was to run the voluntary redundancy and retirement scheme after all other MARs schemes have closed and finished. Mr Atherton asked that the context to the paper was provided so that the Board could be assured that in agreeing this proposal they were not inadvertently creating a skill gap by losing business critical and experienced staff during the transition. Mr Greenwood agreed that it would be beneficial for Board to understand what the overall strategy was that the scheme was trying to achieve. He outlined that there was vastly different levels of resource available across the ten localities and accepting the scheme, without this context being set out, would present a risk to individual localities business continuity. Dr Burrows clarified for Board that there was a clear mandatory challenge to reduce running costs and this was one way to do this, but noted the concerns raised by members. Dr Higgins reminded Board members that the NHS Greater Manchester cluster is a transitional body to help facilitate the transfer to GPCCGs and that we can not continue to work in ten separate ways, but must look at how we work together to enable and support the development of the new arrangements. The Board: Requested that the paper is reviewed and comes back to a future meeting giving Board members the Greater Manchester context and assurance around protecting business critical functions.
11/54 Trafford Programme Board
19

Dr Burrows introduced the report, updating the Board that following the announcement of Central Manchester University Hospitals NHS Foundation Trusts as the preferred acquisition partner for Trafford Healthcare NHS Trust, there is a requirement to develop a governance structure that, in parallel with the completion of the acquisition process will ensure the development of a commissioner led, clinically designed vision for the provision of healthcare in Trafford and the implementation of a safe and sustainable health system for Trafford. Consultation will take place with stakeholders and the public. Dr Burrows explained that the acquisition group had met earlier on the day of this Board meeting and a number of small amendments to the document had been agreed to include:
• An emphasis on a continuation of the work already completed with this programme representing the next step.
• The proposed governance structures to include the Trafford Health and Wellbeing Board
• Key stakeholders in section 2.3 to include University Hospital South Manchester and Trafford Provider Services, currently in a holding arrangement with Bridgwater Trust.
Mr Greenwood expressed concern with regards to the development of the service provision for Trafford taking place separately from the wider Greater Manchester wide Safe and Sustainable strategy work. Dr Burrows acknowledged Mr Greenwood’s concern but stated that the acquisition process is time bound and, as such, the Trafford proposal must take place speedily to ensure that the service provision is in line with commissioning intention rather than be provider driven. The Board, acting as the Board of NHS Trafford, endorsed the recommendations:
• To approve the creation of Trafford Strategic Programme Board as a task and finish sub committee of NHS Greater Manchester Board.
• To appoint a dedicated project lead. • To support the appointment of an independent Chair for the
strategic Programme Board. • That the Programme Board develops a Terms of reference for
formal approval at the November Board Meeting.
MINUTES AND REPORTS
11/55 Locality Board Summary Documents Mr Bellingham introduced this item. Professor Fairhurst asked the Non Executive Directors to ensure that the Locality Board Summaries fully represent the discussions taking place around performance and risk management at the locality Board meetings.
20

Mrs Garratt added that it was important that the summaries make explicit that the recommendations from the Francis Report are tested against governance arrangements locally. Mrs Yarwood explained that the external auditors will use the reports to test risks and as such Board will need some assurance that they are being discussed. Mrs Yarwood asked that the Chairman send a communication to Locality Board Chairs to highlight what assurance is required arising from issues discussed at Locality Board meetings. The Board noted the Locality Board Summary Documents.
11/56 NHS Greater Manchester Remuneration Committee Minutes – 22 June 2011 The minutes were agreed and the contents noted.
FOR INFORMATION
11/57 Reflections Mrs Senior asked that consideration be given to the length of the Board papers, and whether some papers could be more succinct, with additional background or detailed information available if required. Mr Atherton indicated he was conscious that having bi monthly meetings may mean that information was not received in a timely manner. Some thought to be given to how important information can be disseminated to Board without it becoming unmanageable.
11/58 Date and Time of Next Meeting 10th November at 2 pm Exclusion of Press and Public To resolve that publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted and that the public be excluded.
21

22
NHS GREATER MANCHESTER BOARD MEETING MATTER ARISING 4a 10th November 2011 REPORT OF:
Director of Finance
DATE OF PAPER:
20th October 2011
SUBJECT:
Information Governance update – Minute 11/41
IN CASE OF QUERY, PLEASE CONTACT
Claire Yarwood 0161 212 6135
PURPOSE OF PAPER: To update the Board on progress with implementing NHS Greater Manchester wide Information Governance Toolkit reporting, the approach taken to provide assurance and the timetable for gaining assurance on locality performance.
23

Information Governance Update The Board were made aware of the Department of Health Informatics Directorate “Guidance for Boards: Information Governance” published in August 2011, at the Board meeting in September 2011. The guidance advises Boards to ask themselves: 1. “What have we done, as an organisation, to ensure we have implemented adequate policies and procedures and are addressing the responsibilities and key actions required to support effective Information Governance?” 2. “What were the outcomes of our most recent annual Information Governance assessment, and what measures (if any) have been put in place to address any identified deficiencies?” 3. “What plans do we have in place to ensure our organisation remains compliant with national standards for Information Governance? 4. “Do we as an organisation have the capacity and capability to guarantee our plans for Information Governance can be implemented?” 5. “Do our information governance arrangements adequately encompass all teams and work areas that we are legally accountable for?” This paper outlines the plan put in place by NHS Greater Manchester to provide assurance that adequate measures have been put in place. 1 Introduction and Background 1.1 Information governance aims to support the delivery of high quality care by promoting the
effective and appropriate use of information. The Information Governance framework for Health and Social Care is formed by those elements of law and policy from which applicable information governance standards are derived, and the activities and roles which individually and collectively ensure that these standards are clearly defined and met.
1.2 Since 2008, concerns about public sector data protection have resulted in the Cabinet Office mandating a range of standards for managing information risk, an important element of information governance. These standards are reflected within the NHS Information Governance Toolkit. The NHS Chief Executive, in his communications to NHS Chief Executives, has made it clear that the ultimate responsibility for information governance in the NHS rests with the Board of each organisation.
1.3 The NHS Greater Manchester Cluster Chief Executive briefed the September Board on the
Information Governance performance of each locality as at the end of March 2011. This paper outlines the plan put in place by NHS Greater Manchester to provide assurance that adequate measures have been put in place to ensure Information Governance standards would be met by the end of March 2012.
2 Further Information 2.1 Further information can be found at https://www.igt.connectingforhealth.nhs.uk or by contacting
the cluster Information Governance workstream lead [email protected].
24

3 Action Plan 3.1 The NHS Greater Manchester IM&T Programme has put in place a dedicated workstream to
oversee Cluster wide Information Governance and to develop standardised policy based on best practice. An initial self assessment of dedicated Information Governance capacity has been undertaken and this will feed into the broader review of IM&T support across NHS Greater Manchester due to report to the IM&T Programme Board in November.
3.2 The Director of Finance has met with Internal Auditors to ensure that a consistent scope is
developed for the annual Information Governance audit and that independent assurance will be available to support the completion of a Cluster return by the 31st March 2012.
3.3 The Information Governance workstream has been briefed by Internal Auditors on the mandatory
audit scope and process for 2011/12. The workstream lead reports to the Director of Finance on progress and issues.
3.4 The timetable for this is: 31st October 2011
1. All localities to complete their own interim Information Governance (IG) return, supported by local evidence, to provide NHS Greater Manchester with a baseline IG Toolkit score.
2. NHS Greater Manchester to submit an interim return to the Department of Health based on the lowest score within the Cluster for each element.
November 2011 3. Internal Auditors will provide an initial review to each locality on the robustness of their October return and local improvement plans to achieve a satisfactory rating by March 2012.
4. Prior to feeding back to localities, Internal Auditors will undertake an informal peer review exercise ensuring that interpretations are common, that evidence requirements have been equally defined and met and that outcomes are consistent.
November 2011 to February 2012
5. NHS Greater Manchester IG Workstream to monitor progress against locality improvement plans and to provide to localities should the need arise.
6. IG workstream to determine future IG Shared Service arrangements and the approach to standardisation and improvement.
February 2012 to March 2012
7. Internal Audit to provide their formal assessment of locality performance. 8. All localities to provide NHS Greater Manchester with final 2011/12 IG Toolkit
rating.
March 2012 9. GM Cluster to submit IG Toolkit return. 4 Recommendations 4.1 The Board of NHS Greater Manchester are asked to note progress made to date. Claire Yarwood Director of Finance
25

26
NHS GREATER MANCHESTER BOARD MEETING MATTER ARISING 4b 10th November 2011 REPORT OF:
Raj Patel, Medical Director
DATE OF PAPER:
26th October 2011
SUBJECT:
Recruitment of two Associate Directors of Service Redesign – Minute 11/42
IN CASE OF QUERY, PLEASE CONTACT
Raj Patel 0161 212 6134
PURPOSE OF PAPER: Following the successful appointment of Dr David Valentine as Associate Director of Performance & Regulation, the purpose of this paper is to update Board members in respect of the progress made in the recruitment of two additional Associate Directors who will be appointed to support QIPP, clinical leadership and service design.
27

Recruitment of Associate Directors 1. Update 1.1 With regard to the recruitment and appointment of two additional Associate Directors to
support QIPP, clinical leadership and service design, Board members are asked to note that interviews for these posts are scheduled to take place between the 25th October and 1st November.
1.2 A further update report to announce the successful candidates will be presented to the
January Board, at which time the recruitment process should be complete. Dr Raj Patel Medical Director
28

NHS GREATER MANCHESTER BOARD MEETING MATTER ARISING 4c 10th November 2011 REPORT OF:
Director of Finance
DATE OF PAPER:
3rd November 2011
SUBJECT:
Locality Board Summary Documents – Minute 11/50
IN CASE OF QUERY, PLEASE CONTACT
Claire Yarwood 0161 212 6135
PURPOSE OF PAPER: To update the Board
29
Locality Board Summary Documents 1 Board Update 1.1 A paper was shared with Governance Leads and Managing Directors. The paper set out the next
stages in the governance development programme, and included the rationale and requirement for the further development of Locality Board Summary Documents.
1.2 A letter has been issued from the NHS Greater Manchester Chair to localities to underpin this
requirement. Claire Yarwood Director of Finance
30

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 6 10 November 2011 REPORT OF:
Chief Executive
DATE OF PAPER:
1 November 2011
SUBJECT:
Report of the Chief Executive
IN CASE OF QUERY, PLEASE CONTACT
Dr Mike Burrows 0161 212 4821
PURPOSE OF PAPER: The NHS Greater Manchester Board are asked to note and minute its acceptance of the contents of:
• Section 1: Personal Liability of Non Executive Directors The NHS Greater Manchester Board are asked to approve the recommendations outlined in the following sections:
• Section 2: Public Health Annual Report • Section 3: Home Oxygen Service Contract for the North West • Section 4: Greater Manchester Health Protection
The NHS Greater Manchester Board are asked to note the content of the report, in particular to note the actions ongoing in the following sections:
• Section 5: North West Surgical Taskforce • Section 9: Industrial Action Ballot • Section 13: Nurse and Allied Health Professional Leadership in Commissioning • Section 14: Extending Patient Choice of Provider – Progress Update. • Section 21: Greater Manchester Effective Use of Resources – Establishing New
Arrangements
31

Report of the Chief Executive
1. Personal Liability of Non Executive Directors - Indemnity 1.1 Non Executive Directors can technically be considered as personally liable for the
consequences of board decisions. The threat of legal action against a chair or non executive director personally, rather than the NHS organisation they serve is very small but legally, chairs or non executive directors are personally liable for their actions and decisions whether acting as individuals or as members of a board.
1.2 To provide protection it is usual for NHS organisations to provide an indemnity for decisions
taken properly in the normal course of board business. The indemnity advised to the NHS in HSC 1999/104 is still relevant and should be issued to the chair and non executive directors of any NHS Boards:
1.3 ‘A chairman or non executive member or director who has acted honestly and in good faith
will not have to meet out of his or her own personal resources any personal civil liability which is incurred in the execution or purported execution of his or her board function, save where the person has acted recklessly.’
1.4 The above indemnity will be activated by minuting its acceptance in the minutes of the
meeting of the NHS Greater Manchester Board, (acting in its capacity as the Board of the 10 Greater Manchester PCTs).
1.5 Executive Directors are not required to be issued with the above indemnity as the employing
organisation is always liable for the actions of its employees in the course of their employment.
2. Public Health Annual Report 2.1 Directors of Public Health have a statutory responsibility to report on the health of their
population on an annual basis. The Public Health Annual Report has usually been presented to PCT Boards, Councils and other bodies by the Director of Public Health and is often used to influence commissioning decisions and the development of the local health strategy. As a consequence of the clustering of the PCTs and preparation for the new commissioning arrangements via CCGs, and the emergence of Health and Wellbeing Boards in each local authority, it would seem sensible for the Board of NHS Greater Manchester to delegate its responsibility for receiving the Public Health Annual Report to the Board of the shadow CCGs and Health and Wellbeing Boards in each locality.
2.2 Recommendation:
The Board are asked to delegate its responsibility for receiving the Public Health Annual Report for each of the 10 Greater Manchester Localities to their respective shadow CCG Boards and Health and Wellbeing Boards.
32
3. Home Oxygen Services Contract for the North West Region 3.1 In May 2011 the 24 North West Primary Care Trust’s delegated lead responsibility for the
re-procurement of Home Oxygen Services to the Cheshire, Warrington and Wirral PCT Cluster. The project has now progressed and the existing contract has been extended until the 26th June 2012. A procurement exercise has taken place across the summer months and as a result the procurement team is recommending entering into a contract with the preferred provider, Air Liquide (Homecare) Ltd. It is estimated that the value of the contract for the 10 Greater Manchester PCTs will be £1.76 million and this should result in savings of £2.63 million to the 10 Greater Manchester PCTs on a full year basis.
3.2 The Board is asked to provide delegated authority to the Chief Executive to sign the
contract on behalf of the 10 Greater Manchester PCTs. 4. Greater Manchester Health Protection 4.1 Greater Manchester Directors of Public Health have been reviewing the PCT health
protection/infection control function as part of the transition work programme. 4.2 Increasing risks have now been highlighted as part of this work stream; the workforce was
small when first reviewed a few months ago but has reduced even more due to:- • Vacancies not being filled in some PCTs • Vacant posts/budgets being given up for cost savings or lost as part of MARS
arrangements • Loss of staff to provider organisations without appropriate service specifications to
deliver key functions across the community. 4.3 Risks to resilience arising from this are that there is reduced capacity across GM to deliver
essential health protection/infection control functions during this winter and in the longer term, these include:-
a) Inability for PCTs and DPHs to discharge their core functions or emergency responses
relating to health protection/infection control
b) Inadequate capacity:- • to investigate or provide advice during outbreaks • to undertake essential surveillance and root cause analysis (RCAs) of Health Care
Associated Infections e.g. C Diff and MRSA bacteraemia • to undertake enhanced surveillance programmes e.g. E.Coli bacteraemia, MSSA
bacteraemia. • to provide advice to health care professionals, partner agencies, and the public
c) Inability to deliver core functions that ensure the health economy work force is equipped
to maintain high standards of infection prevention and control such as:- i. Education and training ii. Audit iii. Implementation of findings from RCAs iv. Policy development and support
4.4 The GM DPH Group recommends that an interim shared commissioning and support
service is put in place immediately to increase resilience in the short term. These steps will also have the added benefit of testing relationships and working arrangements and be able to inform the longer term transition project. The transitional arrangement will not affect the working arrangements with GM Health Protection Unit and will also help to test out longer
33
term relationships and models of working with a view to becoming an “early adopter” site for PH transition.
4.5 The interim structure will ensure that a resilient and responsive service is available to
respond to outbreaks/incidents during the winter months. It will also ensure commissioning support is available for a range of commissioning organisations including clinical commissioning groups, the local level of the NHS commissioning board and local authority commissioning functions. It is planned that the interim structure will be in place by December 2011 and a consultation exercise including an away day will be held through November.
4.6 Two PCTs have moved all their infection control resource into provider services as part of the transforming community services agenda. Service Level Agreements are in place but it is not clear whether this provides an adequate service for commissioners. This will require further consideration.
4.7 As noted above the current available resource (staff/budget) is not sufficient to maintain
resilience. Maintaining a shared resilient service will require PCTs to recommit resources that have been removed from infection prevention control in the last twelve months.
4.8 Recommendation
To ensure that there is resilience across GM as we face the winter, NHS Manchester Board is asked to:- • Support the development of an interim shared service across the 8 PCTs who
have not moved their resources to provider services • To mandate those PCT’s to recommit resources that have been removed from
infection prevention control in the last twelve months. 5. North West Surgical Taskforce 5.1 The Northwest Paediatric Surgery and Anaesthesia Taskforce are seeking support for
developing additional standards for paediatric surgical specialties. 5.2 The PCT Cluster Chief Executives have been asked to support the following
recommendations:
• To receive and endorse the first outputs of the Northwest Paediatric Surgical Taskforce. • To agree a process for ensuring local providers comply with the standards and
undertake a self assessment/ audit of the standards and submit their data to AQuA for benchmarking.
• Agree in principle to ongoing support to the North West Paediatric Surgery Taskforce and the resources required.
• Support the work on developing NW Standards for other paediatric surgical specialities. 6. Cooperation and Competition Panel Conclusion re North West Continuing Health
Care Procurement 6.1 Members will recall being provided with an overview of this issue at the July Board meeting.
The Co-operation and Competition Panel, (CCP), conducted an investigation into this procurement following a complaint made by the Lancashire Care Association. The CCP is a national body which was set up to help ensure that the Principles and Rules of Co-operation and Competition for the provision of NHS-funded services support the delivery of high
34

quality care for patients and value for money for taxpayers. The Panel investigates potential breaches of the Principles and Rules, and makes independent recommendations to the Department of Health and Monitor on how such breaches should be resolved.
6.2 Following the investigation, a report was published on the 12th September indicating that
the framework developed is consistent with the principles and rules for cooperation and competition. In particular, the CCP found that procurement processes for putting in place the new framework agreements were transparent and non-discriminatory. Further, the CCP has found that the PCTs’ payment regimes are transparent and fair. The CCP also considered that the framework agreements are flexible enough to ensure that individual PCTs will be able to commission sufficient Continuing Healthcare places for their local populations from the best placed providers. In the light of these conclusions, the CCP decided not to progress to a detailed Phase II investigation.
.. 7. HealthWatch Programme Board 7.1 To inform the development of HealthWatch, the Care Quality Commission and Department
of Health have jointly established the HealthWatch Programme Board and its advisory group.
7.2 HealthWatch England and Local HealthWatch will be established as the new independent
consumer champions for health and social care from October 2012. 7.3 The HealthWatch Programme Board provides strategic oversight and ensures readiness for
the launch of both Local HealthWatch and HealthWatch England. The HealthWatch advisory group provides expert guidance to the programme board so it can advise ministers on the implementation of the government’s proposals for HealthWatch. The group also works with the Department of Health and Care Quality Commission to look at practical ways of ensuring the transition to HealthWatch runs smoothly.
8. Consultation on Increase to NHS Pension Scheme Contributions 8.1 The Department of Health has launched a consultation on proposed changes to the level of
contributions made by NHS Pension Scheme members towards their pension. 8.2 The Spending Review 2010 sets out plans to secure £2.8bn savings per year by 2014/2015
through increasing public service employee pension contributions by an average of 3.2%, phased in from April 2012.
The consultation is available: http://www.dh.gov.uk/en/Consultations/Liveconsultations/DH_128710 9. Industrial Action Ballot 9.1 A letter has been received from the Regional Secretary of Unison indicating that they
intend to hold an official industrial action ballot with ballot papers being issued on the 11th October 2011. The ballot is in relation to a trade dispute over changes to NHS pensions. The ballot paper will ask whether staff are prepared to take part in industrial action in the form of strike action. NHS Greater Manchester will ensure contingency plans are developed to respond to any future possible strike action within the 10 PCTs.
35
10. Voluntary Redundancy and Retirement Scheme 10.1 This Scheme as proposed under Section 16 of Agenda for Change will be reconsidered in
January 2012. At this point work on shared services in a number of areas will have progressed. Workforce plans, targets for running cost reductions and details of emergent organisations will also have developed further. If there is a continued requirement to run the Voluntary Redundancy and Retirement Scheme then this can be administered and run to ensure maximum payback within the financial year 2012/13.
11. Safeguarding Leads in Greater Manchester 11.1 Greater Manchester Safeguarding Leads will move into a single management structure for
GM under direct line management of the Executive Director of Nursing, Quality and Performance. This is to provide a clear line of sight on the issues and workstreams that protect our most vulnerable clients during this period of transition and will strengthen the resilience across the system. The staff affected by this will continue to work locally and within the partnership arrangements established with local agencies. They will be supported by local commissioners and Directors of Public Health. The line of management will be aligned to the accountability, which is through to the NHS Greater Manchester Executive Nurse.
12. Whistleblowing 12.1 Following the recent (June 2010) guidance on whistleblowing, NHS Greater Manchester will
be developing a confidential contact system for all NHS staff working in Greater Manchester to use where they have been unable to progress issues within local organisations. It is important for CCGs to have their own whistleblowing issues being raised and managed within shadow GPCCs. However, given the pace of transition underway from locality boards to GPCCGs during the next few months, it is important that NHS Greater Manchester demonstrates the ability to be able to listen to staff and patients as part of the early warning system described in last month’s board papers on Quality and Safety.
13. Nurse and Allied Health Professional Leadership in Commissioning 13.1 Nurse and Allied Health Professional leadership in the Clinical Commissioning landscape is
seen as vital by the GP Community and NHS Greater Manchester in ensuring we maximise the clinical talent available to develop effective safe services for our population.
13.2 The Executive Director of Nursing, Quality and Performance is currently identifying Nurses and Allied Health Professionals who have the potential to support Shadow GP Clinical Commissioning Groups and Health and Well Being Boards, both during transition and in the future. Once identified, these individuals will form part of a clinical community and will be supported to enhance and develop clinical commissioning skills with our GP commissioning colleagues.
13.3 Meanwhile, the Executive Director of Nursing, Quality and Performance and the Executive Director of Commissioning Development will work together to ensure that local authorisation processes reflect the importance and requirement to have Nurses and Allied Health Professionals on the governing body of Clinical Commissioning Groups and involved within wider commissioning activities.
36
14. Extending patient choice of provider – progress update 14.1 The Department of Health issued guidance on Extending patient choice of provider on 19
July 2011, which set proposals for a phased implementation of the policy, treating 12/13 as a transitional year, starting with a limited set of community and some Mental Health services.
14.2 The guidance required commissioners (to be led by PCT Clusters) to identify 3 or more
community or mental health services in which to implement patient choice of any qualified provider from April 2012. Commissioners were asked to meet the following deadlines to progress the policy:
• September 30th – outline local processes for public and professional engagement on
local priorities for extending choice of provider.
• October 31st - the identification of three or more community or mental health services to implement patient choice of Any Qualified Provider from April 2012.
14.3 The Greater Manchester wider leadership team discussed the policy and agreed that this
should be implemented through the GM Directors of Commissioning group. Each locality undertook locality engagement and prioritisation processes to identify stakeholder preferences for implementation of the policy.
14.4 A stock take was presented to the Locality Managing Directors on 16th September 2011 and a collective approach to implementation across GM was proposed and endorsed for 2 services allowing locality flexibility for the other choice(s). Directors of Commissioning were also asked to ensure the risks inherent in the roll out of the policy were mitigated, to seek support of the Directors of Finance and ensure processes are led by Clinical Commissioning Groups.
14.5 As at the 13th October 2011, all localities have completed their engagement and prioritisation and 2 priorities have emerged as the majority choice across GM: Podiatry and Diagnostics. Directors of Commissioning have convened a working group to develop a risk management plan. The next step will be for weekly operations meeting (21/10/11) of NHS Greater Manchester to consider the priorities to agree the approach of the GM Cluster.
15. National Audit of Intermediate Care 15.1 The first ever national audit of intermediate care is to take place over the next three years,
headed up by NHS Benchmarking. It invites PCTs to participate at a cost, expressing interest by the 18th November 2011. Further information on the project can be document ‘Proposal for a National Audit of Intermediate Care’, a copy of which can be provided to Board Members on request.
16. Care Quality Commission Annual Report 16.1 The Care Quality Commission (CQC) has published its second annual report, which has
been laid before Parliament. The report covers the period April 2010 to March 2011, during which 12,000 organisations running services such as care homes, care in the home agencies and private hospitals were brought into a new system of regulation. There was a large increase in the scale of the CQC’s regulatory work as 9,000 dentists and independent ambulance services were brought into this same system.
37

16.2 The annual report and annual accounts are available at: http://www.cqc.org.uk/publications.cfm?fde_id=18566 17. National Standards for Senior NHS Leaders 17.1 The Department of Health has commissioned the Council for Healthcare Regulatory
Excellence (CHRE) to develop national standards of probity, behaviour and competence for senior NHS leaders to provide a clearer understanding of what is expected of them.
17.2 This programme of work arises from the government’s commitment in the recent command
paper, Enabling Excellent – Autonomy and Accountability for Healthcare Workers, Social Workers and Social Care Workers.
17.3 CHRE aim to consult on draft standards in November 2011 and will report to Ministers in
March 2012. Further information is available at http://www.chre.org.uk/media/18/408 18. Annual Report of the Parliamentary and Health Service Ombudsman 2010/11 18.1 The Parliamentary and Health Service Ombudsman, Ann Abraham, has published the
annual report for 2010/11, which details the Ombudsman’s work in responding to complaints about the NHS in England and government departments and other public bodies across the UK.
18.2 The report includes research findings from the Ombudsman’s customers, including their
views on the service they receive. The report also provides high level data on the complaints received, as well as where complaints originate from.
18.3 In 2010/11, the Ombudsman published Listening and Learning, a review of complaint
handling by the NHS in England. A second review of complaint handling in the NHS and a new publication reviewing complaint handling by government departments and other public bodies will be published by the Ombudsman in autumn 2011.
The report is available to download from www.ombudsman.org.uk 19. Response to the Consultation on Value-Based Pricing 19.1 Between 16 December 2010 and 17 March 2011, the government undertook a public
consultation on proposals for a new value-based system of pricing medicines. 19.2 The government has published a document that provides a summary of the responses
received to the consultation, highlights the key themes and sets out the government’s response and actions to be taken.
19.3 The full document is available at: http://www.dh.gov.uk/en/Consultations/Responsestoconsultations/DH_128226
38

20 Government to publish new data on health, schools, courts and transport 20.1 The Prime Minister has announced his commitment to publishing key data on public
services, including the NHS, as part of the government’s continuing commitment to open public services in advance of the Open Public Services White Paper.
20.2 The new data on the NHS will include:
• Data on comparative clinical outcomes and prescribing practice by GP practice from December 2011;
• Complaints data by NHS hospital from October 2011; • Clinical audit data detailing the performance of publicly funded clinical teams in treating key
healthcare conditions from April 2012; • Data on staff satisfaction and engagement from December 2011; • Data on the quality of post-graduate medical education from April 2012.
20.3 Further information can be found at:
http://www.cabinetoffice.gov.uk/news/government-publish-new-data-health-schools-courts-and-transport
21 Greater Manchester Effective Use of Resources (EUR) – Establishing New
Arrangements
21.1 The aim of an EUR policy is to maximise the value the NHS can provide to patients by restricting provision of interventions when they are unlikely to be clinically or cost effective. EUR policies are implemented in a variety of ways including ‘exceptional case panels’.
21.2 The initial mapping phase of the EUR project found each locality has a small EUR team and
they have all developed their own approaches in response to local issues and capacity. Options for the future have been discussed at a variety of forums. A consensus has emerged that a Hub & Spoke model should be implemented. This model aims to develop Greater Manchester EUR policies, support and monitor how they are being implemented locally and reduce current duplication of EUR work; it will also support local differences in approaches where these can be explained.
21.3 The project’s second phase, establishing the new Hub & Spoke arrangements, is
commencing and will report as part of the Commissioning Support Service programme.
Mike Burrows Chief Executive November 2011
39

40

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 7 10 November 2011 REPORT OF:
Medical Director
DATE OF PAPER:
10 November 2011
SUBJECT:
Report of the Medical Director
IN CASE OF QUERY, PLEASE CONTACT
Dr Raj Patel 0161 212 4821
PURPOSE OF PAPER: To update the NHS Greater Manchester Board on the activities of the medical directorate.
41

Report of the Medical Director 1 Clinical Commissioning Board 1.1 Further to the Board’s September decision to establish an executive committee to
provide clinical leadership to its commissioning business, I can confirm that board is now fully established.
1.2 The Clinical Commissioning Board (CCB) has drawn its membership from the local
Clinical Commissioning Group nominations and enjoys a clear clinical majority. It receives managerial support from NHS Greater Manchester Executive Directors and also from locality directors with deep knowledge of, in particular collaborative and tertiary commissioning.
1.3 A detailed report of the CCB’s commissioning activities is provided elsewhere on the
Board’s agenda. Forthcoming work will include:
• Oversight of the review of the model of stroke care; • Oversight of the work informing improvements in dementia care; • Commissioning for harm free care; • The introduction of 111; and • Commissioning Major Trauma care.
2 Clinical Networks and Clinical Senates 2.1 Further to the Board’s decision in September setting the course for Clinical Networks,
NHS Greater Manchester has commissioned immediate work to support the next stage development of Greater Manchester’s Clinical Networks. The work will seek to inform Dr Kathy McLean’s work on behalf of the Future Forum to lead the development of proposals for the future of networks and senates.
2.2 The principal objectives for the project include:
• Defining and initiating a model for Integrated Network Support – As the networks move to hosting by the National Commissioning Board it will be necessary to take a consolidating step to gather network support together into a single integrated arrangement. The project should propose a target future model of network support which will realise savings at least sufficient to support the establishment and maintenance of a GM Clinical Senate.
• Creation of the Clinical Senate – The project should support the intention to build the GM Senate in advance of any national work and ensure that approach positively influences national direction. In the short term the project should ensure the proposal responds to our ambitions for Safe & Sustainable clinical services across Greater Manchester and underpins appropriate cross-specialty linkages from the individual service networks.
42

• Ensuring workstream alignment, oversight & governance – There are a number of workstreams underway across networks with direct relevance to QIPP/Service Transformation. It is necessary to map all current network workstreams and plot in relation to QIPP, Service Transformation and Collaborative Commissioning and clarify leadership, oversight and governance of each workstream in relation to EDs, MDs, the Clinical Commissioning Board and Service Transformation Board.
3 Recommendation 3.1 The NHS Greater Manchester Board is asked to note the contents of this report. Dr Raj Patel Medical Director
43

44

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 8 10 November 2011 REPORT OF:
Director of Policy & External Relations
DATE OF PAPER:
20 October 2011
SUBJECT:
Public Service Reform
IN CASE OF QUERY, PLEASE CONTACT
Warren Heppolette 0161 212 4815
PURPOSE OF PAPER: This paper describes the initial proposal for the Health & Social Care Exemplar supporting the Association of Greater Manchester Authorities’ Public Service Reform (PSR) work. It follows consideration by senior participants across NHS commissioners, NHS providers, local government and social care.
The NHS Greater Manchester Board is asked to confirm its support for the Health and Social Care Exemplar described within the report.
45
Public Service Reform Executive Summary The purpose of this paper is to describe the work to date defining the NHS engagement in the Association of Greater Manchester Authorities’ (AGMA) public service reform work. The Public Service Reform work aims to improve productivity and outcomes across the range of public services by providing the means to test and adopt at scale specific proposals for new ways of working. The work envisages a series of thematic exemplars (Health, Complex Families, Early Years, Transforming Justice) connected by a series of cross cutting enabling themes. The Health exemplar proposes to work with emerging major change programmes driven principally at borough level in localities. It will engage with localities participating in the AQUA/Kings Fund Integrated Care Discovery Community supporting large scale integrated care models. It will support NHS Greater Manchester’s work through demonstrator sites to introduce new models of care for dementia, and joint work with the GM Directors of Adult Services to improve urgent care. It will also tap into external expertise where necessary to identify and assess new investment models for integrated commissioning and care. The NHS Greater Manchester Board is asked to confirm its support for the health and social care exemplar described in the report. 1 Purpose 1.1 This note describes the initial proposal for the Health & Social Care Exemplar supporting the
Association of Greater Manchester Authorities’ Public Service Reform (PSR) work. It follows consideration by senior participants across NHS commissioners, NHS providers, local government and social care.
2 Background 2.1 This is a challenging time for all public services, with sharp cuts in spending, difficult choices
about priorities and sluggish growth in the economy. The vision for Public Service Reform is to develop a response to these issues.
2.2 To create viable and effective public services in the future, we need a radical new pan-public sector approach. This will sit alongside tactical, shorter term reform which is required to address the immediate reductions in funding. Successfully delivered, the PSR agenda will radically shift the way in which Public Service resources are used across the conurbation, enabling returns on investment to be reused to support broader demand reduction. Ultimately, public service spending will be reduced across the sub-region, making this a critical programme of work aligned to the Local Government Resource Review. In turn, this will lead to a strong proposition for a different form of devolution for Greater Manchester in comparison to other parts of the Country.
2.3 PSR aims to reduce demand for public services, and to improve productivity and outcomes, to move beyond a local authority driven programme and develop a programme with organisations
46

from across the public service spectrum. The programme aims to establish a series of 'exemplar' projects that will illustrate and underpin this vision. These exemplars will provide a powerful basis for dialogue with Government, and will deliver public service reform on a size and scale that will be able to test real options at pace – they will focus on mainstream implementation, rather than pilots. PSR will put in place models and approaches that through a reduction in demand, will improve growth and outcomes and enable new funding and investment models to influence the next Comprehensive Spending Review. It is proposed to develop the exemplars from the areas where the best reform has taken place to date, and to create new examples in pan-public service arenas.
2.4 The exemplars will consider the impact of pathway and whole system reform at a pan-Greater
Manchester, pan-organisation and neighbourhood level. They are all interlinked around people and neighbourhoods but offer an opportunity to demonstrate GM approach to PSR. These are not “projects” but themes that reform is based around.
2.5 Based on context and principles, 4 exemplars are proposed alongside a set of acknowledged
cross-cutting workstreams
Exemplar Themes Cross Cutting Workstreams • Complex Families, • Transforming Justice • Health and Social Care • 0-5’s Early Years.
• New investment models, • Information, intelligence &
technology • Skills & workforce development • Place.
3 Health & Social Care Exemplars 3.1 The approach to health sought to do two things: develop the engagement of stakeholders
reflecting the complexity of the health and wellbeing system; and identify an appropriate and deliverable focus for the exemplar projects. A Think Tank session was held on the 23rd September building on initial discussions involving a broad range of stakeholders. Participants in the discussions shaping the exemplar so far have included:
• Joyce Redfearn, Chief Exec, Wigan MBC • Sean Harris, Chief Exec, Bolton Council • Stuart Cowley, Director, Personalisation & Partnerships, Wigan Council • Jan Hutchinson, Director of Public Health, Bolton • Warren Heppolette, Director of Policy & External Relations, NHS Greater Manchester • Andrew Foster, Chief Exec, Wrightington, Wigan & Leigh NHS Foundation Trust • Jack Sharp, Director of Strategy, Salford Royal NHS Foundation Trust • Michael McCourt, Director of Operations & Nursing, Pennine Care NHS Foundation Trust • David Fillingham, Chief Exec, AQUA • Mike Burrows, Chief Exec, NHS Greater Manchester • Julie Higgins, Director of Commissioning Development, NHS Greater Manchester
47

• Anne Higgins, Director of Adult Social Care, Trafford Council • Tracy Minshull, Head of Commissioning and Strategy, Bury MBC • Dr Raj Patel, Chair, Clinical Commissioning Group Tameside & Glossop
3.2 The starting point for the discussion recognised three key drivers for radical change in health and
social care. These included:
• A much stronger likelihood of Integration and the creation of new delivery vehicles. This will impact both at the service level in rethinking pathways and between organisations in aligning service and financial incentives;
• Large scale adoption of new technologies & treatments enabling much greater degrees of self care and care at or close to home; and
• Much greater personalisation of care with individual citizens directing service responses through idiosyncratic commissioning.
3.3 Across these areas of work the exemplar will look to consider integration at three levels:
• The macro level – integrated care across a spectrum of services as part of models emerging inspired by international models of Healthcare Management Organisations. There was a strong view that integration needs to be taken forward at speed and at scale;
• The meso level – integrating care for people with the same disease or conditions. This reflects a key focus to promote clinical and service integration for populations such as frail elderly people with complex needs; and
• The micro level – integrating care for individuals through care planning, case management etc.
3.4 Across each of these areas the need to scale up prevention, early detection of disease and early
intervention will inform the approach Greater Manchester takes to developing its new public health system. Primary and secondary prevention will be essential strategies in preventing or slowing the progression of disease. The approach must, therefore, ensure changes are made across the whole of the pathway and take new approaches to prevention, screening and early detection targeting specific areas such as alcohol harm, tobacco control, obesity, physical activity, sexual health, heart disease, and cancer.
3.5 Whichever aspect of reform we view we see opportunities for radical reform in relation to
personalisation, integration and the possibilities of new technologies. Commissioning will change as expectations shift to establish a future of shared decision making between citizen and clinician. We will see integration across commissioner and provider lines to a degree not previously imagined. Finally, opportunities for new technologies will make care outside hospital the default setting in the vast majority of circumstances.
3.6 Proposal
To use a range of exemplars to generate step changes in relation to the integration of services; personalized care & choice for individuals; technology supporting care at home; and the quality & consistency of care across hospitals, general practice, social care and community services. The exemplars will operate across three tiers:
48

• Place - The health and social care exemplar will take very current opportunities to illustrate these changes at scale. It will benefit from the recent announcement of the AQUA/Kings Fund Integrated Care Discovery community which has already engaged 5 of Greater Manchester's localities (Salford, Bolton, Trafford, Oldham, Central Manchester) and through that inform the blueprints for new models of care which better enable us to support people with complex long term health needs in their own homes and local communities.
• Service – It will provide a focus for engagement across the NHS and Social Care for improvements we want to see in dementia care, urgent care and reablement. And it will support us in exploring better ways of ensuring we deliver the best outcomes for the resources available across the whole of the public sector. We will seek to develop blueprints for new models of care in these selected service areas (dementia care, urgent care and services for complex families); and
• Investment Models – assessing and testing new approaches to align financial and organisational incentives. We will investigate options to establish payment systems which map to outcomes and continuity of care rather than activity. This will inform our discussions with Government where the case can be made for changed arrangements to address current barriers to integration and with Monitor to ensure we are able to harness the benefits of co-operation.
3.7 Intended Outcomes
Whilst the work is at a very early stage and focused consideration of outcomes yet to occur, the following key aims might initially be set:
Integrated Care • Clear and robust ‘blue print’ for a borough
level integrated care system • Started to deliver targeted changes within
the specific client groups / populations • Developed common standards and
governance arrangements for integrated care system
• Organisational development / capability building across demonstrator sites
• Implementation of common measurement systems
• assessing and testing new approaches to align financial and organisational incentives.
Dementia Care Four levels of outcome:
i. Outcomes based on ADASS/AQuA outcomes for frail elderly, linked to savings e.g. reduced non-elective admissions, or admissions to residential care.
ii. Outputs in line with local priorities– e.g QOF data on identification and assessment, staff trained, prescriptions antipsychotics, advanced care plans, legal and financial planning.
iii. Patient defined outcomes iv. Reduction in ratio of acute spend on
dementia patients to investment in community based identification, early intervention and management.
Urgent Care The work here is still to be scoped and its target outcomes defined.
Financial Models
• Identification of options for new models of reimbursement, based on international evidence;
• Assessment of relationship between investment models and service/organisational incentives.
49

3.8 Next Steps The immediate next stage work will require:
• Development of a project brief defining the approach to the exemplar; • Consideration within that of the intended products and outcomes; • Consideration also of the means of successfully building on the emergent work to ensure
effective delivery; and • Identification of internal and external capacity to support the work.
4 Recommendation 4.1 The NHS Greater Manchester Board is asked to confirm its support for the Health and Social
Care Exemplar described within the report. Warren Heppolette Director of Policy & External Relationships
50

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 9a 10 November 2011 REPORT OF:
Executive Director of Nursing, Quality and Performance
DATE OF PAPER:
1 November 2011
SUBJECT:
Greater Manchester Performance
IN CASE OF QUERY, PLEASE CONTACT
Hilary Garratt 0161 304 5169
PURPOSE OF PAPER: 1) The report is structured in two sections:
• At a glance (main report) • Analysis of the related information. (Appendix 1)
2) To provide the board with an overview of key performance areas across its areas of responsibility:
• The non FT providers • The FT providers • Operating framework headline measures • Diagnostics • Ambulance performance • Collaborative commissioning • Mental health performance
3) NHS Greater Manchester Board are asked to accept the areas of underperformance set out in this report and support the direct action needed to be taken by the Executive Team
51

Executive Summary This report summarises performance by exception and has placed reliance on July 2011 published data. NHS Performance Framework: This shows that there is one GM Trust (Trafford Healthcare) who is categorised as “underperforming” on Finance and one GM Trust who is categorised as “under performing” on quality of services. Monitor Risk Rating: Finance risk ratings have changed for a number of Providers however the majority are maintaining a rating of 3 and above with the exception of Tameside FT. This Trust has had its Finance rating reduced to 1 and maintains a red governance rating and is subject to enhanced monitoring by Monitor. Healthcare Acquired Infection: CDiff actions are being taken across the affected Providers (Tameside and Stockport) to improve performance and ensure that detailed forensic and root cause analysis is done for each case together with engaging clinicians on primary and secondary care pathways around anti-biotic prescribing. AWL and North East sector have produced turnaround plans and HPA have been asked to support a comprehensive review of this. Referral To Treatment (RTT): Four Providers are working to improve RTT performance and it is expected that both Pennine Acute and Stockport (Stepping Hill) will be back on track by end of October. Bolton NHS Trust is anticipated to be back on target by end of November although NHS GM is still awaiting a revised action plan. CMFT continues to make steady progress and should be on target from 1 January 2012. Mixed Sex Accommodation Breaches (MSA) – There are two localities with underperformance and these are Salford and Bolton. Each has arrangements in place to either build assurances with Provider or seek to reach a resolution either via negotiations (Salford) or the use of contract levers (Bolton). Performance on Cancer: Performance against the 62 days Treatment Target is worsening across GM and patients continue to receive treatment outside the national standard. The key reason for this underperformance has been the inability of the GM network to efficiently manage inter provider transfers (ITT) and only 59% of patients are treated within 62 days where there is an ITT. NHS GM has submitted a collective recovery plans to NHS North of England. NHS GM has been actively engaged with the Acute sector Chief Executive’s and their relevant Directors to agree and implement a revised breach allocation policy for GM and Cheshire Cancer Network; performance manage and improve referrals and communications form local hospital cancer teams to specialist tertiary providers and ensure that agreements are built into contracts for 2012-13. A Memorandum of Understanding between all Acute Providers and the Cluster is now being pursued to secure further commitment to this performance area. A&E: Four Providers have experienced failures to meet the 95% target in October. Central Manchester Foundation Trust and Wrightington, Wigan and Leigh Foundation Trust experienced dips in performance and have put in remedial actions to maintain performance. Stockport’s A&E performance has reduced during October and has been variable (year to date) and further assurances are required from the Urgent Care Strategy. Pennine Acute continues to struggle to maintain a consistent and
Greater Manchester Performance Report
52
resilient services across all sites and continues to have significant challenges particularly in North Manchester General Hospital. Pennine Acute acknowledge that the main reason for this has been recruiting the A&E staff into the department and as a result presents issues with supervision and a higher number of patients being admitted rather than assessed and discharged. There is a risk that Pennine Acute will fail the annual target. Diagnostics: Pennine Acute is steadily clearing the diagnostic backlog, however, the backlog at Central Manchester is proving to be more challenging and an initial trajectory suggests it will be March 2012 before the backlog is cleared. Further work is being undertaken to improve this position. NWAS: 8 minute performance across GM was 75.33% in September 2011 bringing the cumulative position for Greater Manchester to 73.68%. The challenge in Greater Manchester will now be to maintain performance above 75% with constituent PCTs working with NWAS to support performance. Further work is required in relation to quality indicators as NWAS continues to have the highest conveyance rates nationally with 80% of calls being conveyed to A&E departments and one of the lowest rate for closing calls with telephone advice and the highest re-contact rate following a call being closed with telephone advice. Mental Health: NHS GM will be undertaking further work in the next quarter to understand the Improving Access to Psychological Therapies (IAPT) service and put in place recovery plans where performance continues to remain below the nationally agreed performance indicators. NHS GM will be undertaking an assessment of the performance of Mental Health services in terms of outreach service and gatekeeping services to identify areas for improvement in the quality of the services.
53

54
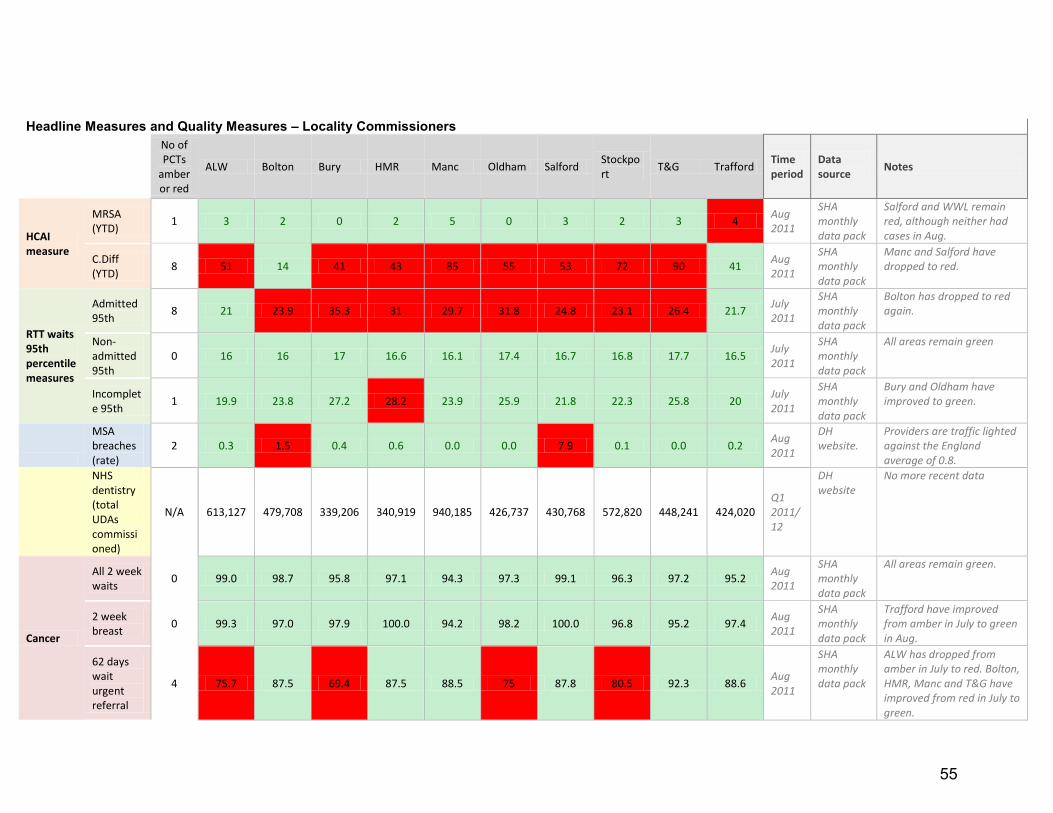
Headline Measures and Quality Measures – Locality Commissioners
No of PCTs
amber or red
ALW Bolton Bury HMR Manc Oldham Salford Stockport
T&G Trafford Time period
Data source
Notes
HCAI measure
MRSA (YTD)
1 3 2 0 2 5 0 3 2 3 4 Aug 2011
SHA monthly data pack
Salford and WWL remain red, although neither had cases in Aug.
C.Diff (YTD)
8 51 14 41 43 85 55 53 72 90 41 Aug 2011
SHA monthly data pack
Manc and Salford have dropped to red.
RTT waits 95th percentile measures
Admitted 95th
8 21 23.9 35.3 31 29.7 31.8 24.8 23.1 26.4 21.7 July 2011
SHA monthly data pack
Bolton has dropped to red again.
Non-admitted 95th
0 16 16 17 16.6 16.1 17.4 16.7 16.8 17.7 16.5 July 2011
SHA monthly data pack
All areas remain green
Incomplete 95th
1 19.9 23.8 27.2 28.2 23.9 25.9 21.8 22.3 25.8 20 July 2011
SHA monthly data pack
Bury and Oldham have improved to green.
MSA breaches (rate)
2 0.3 1.5 0.4 0.6 0.0 0.0 7.9 0.1 0.0 0.2 Aug 2011
DH website.
Providers are traffic lighted against the England average of 0.8.
NHS dentistry (total UDAs commissioned)
N/A 613,127 479,708 339,206 340,919 940,185 426,737 430,768 572,820 448,241 424,020 Q1 2011/12
DH website
No more recent data
Cancer
All 2 week waits
0 99.0 98.7 95.8 97.1 94.3 97.3 99.1 96.3 97.2 95.2 Aug 2011
SHA monthly data pack
All areas remain green.
2 week breast
0 99.3 97.0 97.9 100.0 94.2 98.2 100.0 96.8 95.2 97.4 Aug 2011
SHA monthly data pack
Trafford have improved from amber in July to green in Aug.
62 days wait urgent referral
4 75.7 87.5 69.4 87.5 88.5 75 87.8 80.5 92.3 88.6 Aug 2011
SHA monthly data pack
ALW has dropped from amber in July to red. Bolton, HMR, Manc and T&G have improved from red in July to green.
55

62 days screening
1 87.5 100 100 100 92.3 100 100 100 100 100 Aug 2011
SHA monthly data pack
Central Manc, Pennine Acute and South Manc have dropped to red. Tameside has improved to green.
62 days consultant
5 100 50 50 25 60 60 100 88.9 100 93.3 Aug 2011
SHA monthly data pack
Bolton and Oldham have dropped from green in July to red. T&G has improved from red to green.
Emergency Readmissions
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
A&E Quality Indicators (5 measures)
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Patient experience survey
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A Reported by Provider
Quality
Stroke - 90% of time on stroke unit
9 73.4% 59.8% 76.2% 77.5% 72.2% 69.8% 82.6% 72.0% 50.6% 75.3% Q1 2011/12
DH website
Traffic lighted against the national standard of 80%
Overall Performance P PUR UP PUR PUR UP P PUR PUR P
Overall NHS GM Cluster Performance – Under
Performing
P = Performing (Green), PUR = Performance Under Review (Amber), UP = Underperforming (Red)
56

Headline Measures and Quality Measures - Provider
Trusts amber or red
Central Manc
The Christie
Pennine Acute
Royal Bolton
Salford Royal
South Manc
Stockport Tameside Trafford Healthcare
Wrightington Wigan and Leigh
Time period
Data source
Notes
HCAI measure
MRSA (YTD) 2 1 0 2 0 4 1 0 1 0 1 Aug 2011
SHA monthly data pack
Salford and WWL remain red, although neither had cases in Aug.
C.Diff (YTD) 2 42 3 47 9 28 27 30 43 1 24 Aug 2011
SHA monthly data pack
Central Manc has dropped to red. Tameside remains red
Referral to Treatment waits (95th percentile measures)
Admitted 95th
4 43.5 14.9 33.6 23.6 22 22.6 23.1 21.8 17.9 21.4 July 2011
SHA monthly data pack
Royal Bolton has dropped back to red. WWL has improved.
Non-admitted 95th
0 17 15.8 17.6 16.1 17.2 14.9 17.9 18 16.6 15.9 July 2011
SHA monthly data pack
All trusts remain green
Incomplete 95th
1 31.7 14.5 27.2 21.6 18.6 20.7 23.4 25.8 15.4 18.9 July 2011
SHA monthly data pack
Pennine Acute has improved to green.
MSA breaches (rate)
2 0.0 0.0 0.2 2.1 7.2 0.5 0.0 0.0 0.0 0.2 Aug 2011
DH website.
Providers are traffic lighted against the England average of 0.8.
Cancer
All 2 week waits
1 92.2
96.5 98.8 97.4 94.7 96.4 97.3 96.7 99.2 Aug 2011
SHA monthly data pack
Central Manc has dropped from green in July to amber.
2 week breast
0
98.5 97.3 100 94.6 97.9 95.3
99.2 Aug 2011
SHA monthly data pack
All trusts remain green
62 days urgent referral
5 84.8 52.8 81.6 92.1 89.1 89 84.9 92 93.8 78.8 Aug 2011
SHA monthly data pack
Central Manc and Stockport have improved from
57
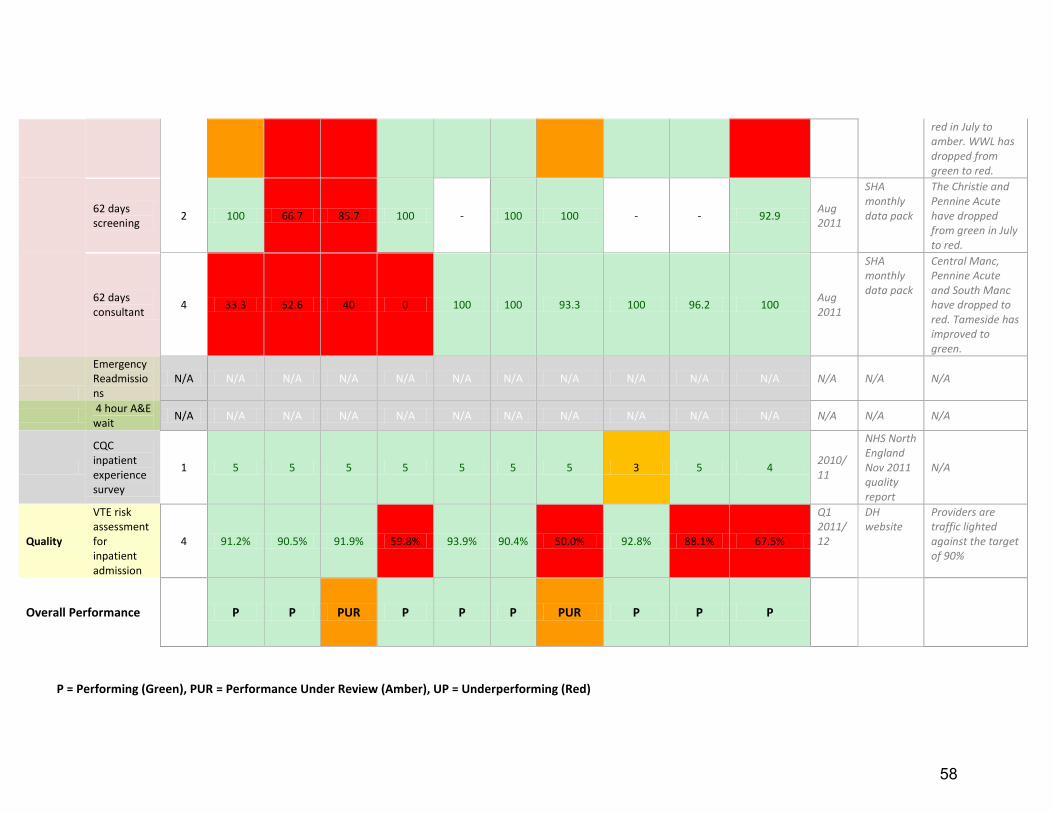
red in July to amber. WWL has dropped from green to red.
62 days screening
2 100 66.7 85.7 100 - 100 100 - - 92.9 Aug 2011
SHA monthly data pack
The Christie and Pennine Acute have dropped from green in July to red.
62 days consultant
4 33.3 52.6 40 0 100 100 93.3 100 96.2 100 Aug 2011
SHA monthly data pack
Central Manc, Pennine Acute and South Manc have dropped to red. Tameside has improved to green.
Emergency Readmissions
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
4 hour A&E wait
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
CQC inpatient experience survey
1 5 5 5 5 5 5 5 3 5 4 2010/11
NHS North England Nov 2011 quality report
N/A
Quality
VTE risk assessment for inpatient admission
4 91.2% 90.5% 91.9% 59.8% 93.9% 90.4% 50.0% 92.8% 88.1% 67.5%
Q1 2011/12
DH website
Providers are traffic lighted against the target of 90%
Overall Performance P P PUR P P P PUR P P P
P = Performing (Green), PUR = Performance Under Review (Amber), UP = Underperforming (Red)
58

Appendix 1
Executive Summary The purpose of this section is to highlight the detail that sits behind our crucial performance targets. Each locality is required to address all poor performance areas urgently, with action plans and trajectories that achieve marked improvements by January 2012. The locality Commissioning Board will be held accountable for performance with Managing Directors personally accountable for improvements to NHS Greater Manchester. 1 NHS Performance Framework for NHS Trusts – Quarter 1 2011/12 1.1 Background 1.1.1 The NHS Performance Framework is an assessment of NHS providers (that are
not foundation trusts) against minimum standards in finance and quality. The framework sets clear thresholds for intervention in underperforming organisations and a rules-based process for escalation. The categories are performing, performance under review or underperforming.
1.2 Current Performance 1.2.1 The most recent data was published 30 September 2011 and covers the first
quarter of 2011/12. Four NHS trusts are covered by the NHS Performance Framework and this is shown in Table 1. The Table shows that there has been an overall drop in quality to “performance under review” for standards and integrated measures at Pennine Acute. NHS GM is working with local Commissioners and Providers to improve this position. Trafford HealthCare Trust (underperforming) and Manchester Mental Health and Social Care Trust (Performing) maintain their previous rating. NWAS has improved their rating on overall quality to performing status.
Greater Manchester Performance Report
59
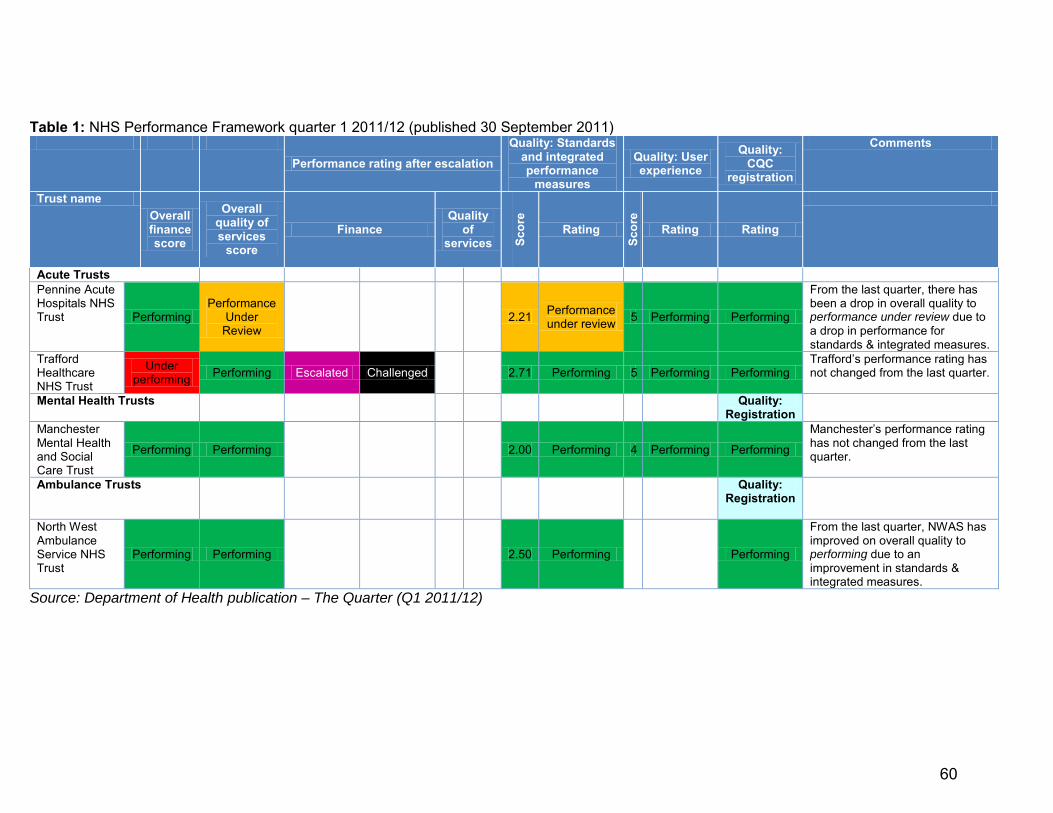
Table 1: NHS Performance Framework quarter 1 2011/12 (published 30 September 2011)
Performance rating after escalation
Quality: Standards and integrated performance
measures
Quality: User experience
Quality: CQC
registration
Comments
Trust name Overall finance score
Overall quality of services
score Finance
Quality of
services Scor
e
Rating
Scor
e
Rating Rating
Acute Trusts Pennine Acute Hospitals NHS Trust Performing
Performance Under
Review 2.21 Performance
under review 5 Performing Performing
From the last quarter, there has been a drop in overall quality to performance under review due to a drop in performance for standards & integrated measures.
Trafford Healthcare NHS Trust
Under performing Performing Escalated Challenged 2.71 Performing 5 Performing Performing
Trafford’s performance rating has not changed from the last quarter.
Mental Health Trusts Quality: Registration
Manchester Mental Health and Social Care Trust
Performing Performing 2.00 Performing 4 Performing Performing
Manchester’s performance rating has not changed from the last quarter.
Ambulance Trusts
Quality: Registration
North West Ambulance Service NHS Trust
Performing Performing 2.50 Performing
Performing
From the last quarter, NWAS has improved on overall quality to performing due to an improvement in standards & integrated measures.
Source: Department of Health publication – The Quarter (Q1 2011/12)
60

2 Monitor Risk Ratings for Foundation Trusts - Quarter 1 2011/12 2.1 Quarter 1 2011/12 Performance
2.1.1 Monitor is the independent regulator of NHS foundation trusts and undertakes a
risk based approach to regulation. Foundation trusts are asked to assess their own compliance with the terms of their authorisation and Monitor then publishes quarterly reports covering the performance and risk ratings on finance and governance for NHS foundation hospitals.
2.1.2 Stockport FT, Salford Royal FT, WWL and the Christie each had their Finance score reduced although they remain at an acceptable level of 3 or above. However, Tameside FT has had its finance rating reduced from 2 to 1 and remains red on governance. The Trust is subject to enhanced monitoring until Monitor determines that it is no longer in significant breach of its authorisation.
61

Table 2: NHS Foundation Trust Performance – Review of 3 months to 30 June 2011 (Published 29 September 2011) Name Finance Governance Change from previous quarter Tameside Hospital NHS FT
1 Red
Finance has dropped from 2 to 1. Governance remains red. In February 2011, the trust was found in significant breach of two terms of its authorisation: the general duty to exercise its functions effectively, efficiently and economically and its governance duty. This was as a result of the trust delivering an unplanned financial risk rating of 2 at quarter two.
In May 2011, as a result of a planned review, CQC found one moderate and four minor concerns about how the trust was meeting essential standards of quality and safety. The trust will be subject to enhanced monitoring until Monitor determines that it is no longer in significant breach of its authorisation.
Stockport NHS FT 3 Red
Finance has dropped from 4 to 3. Governance has dropped from green to red, because at quarter one the trust breached the 95th percentile total time in A&E target and 95th percentile 18 weeks admitted pathways target. The trust also has outstanding Care Quality Commission compliance actions.
Salford Royal NHS FT 3 Amber – green Finance has dropped from 4 to 3. Governance has dropped from green to amber-green, because at quarter one the trust breached its MRSA target.
Wrightington, Wigan and Leigh NHS FT 3 Amber – green
Finance has dropped from 4 to 3. Governance has dropped from green to amber-green because, the trust breached its 95th percentile 18 weeks admitted pathways target at quarter one.
Royal Bolton Hospital NHS FT 3 Amber – green No change
Central Manchester University Hospitals NHS FT 3 Amber – green
Finance remains 3. Governance has improved from amber-red to amber-green, because at quarter one, the trust was found to no longer be in breach of the 31-day wait for second or subsequent surgery target or the 62-day wait for first treatment from consultant screening service referral
The Christie NHS FT 4 Amber – green Finance has dropped from 5 to 4. University Hospital of South Manchester NHS FT 3 Green No change
Greater Manchester West Mental Health NHS FT 4 Green No change
Pennine Care FT 4 Green No change Source: Monitor’s website. The framework for Monitor’s risk rating is shown in the appendix.
62

3 Operating Framework 2011/12 Headline Measures 3.1 Background 3.1.1 The Operating Framework 2011/12 targets were published in December 2010 and
were divided into headline measures and supporting measures. The information on the performance of the headline measures is taken from the monthly information pack produced by the strategic health authority and from data produced by the Department of Health. All information has been validated and signed off by commissioners.
3.1.2 Details of performance for the following headline measures are provided in this report: • Healthcare acquired infections
• MRSA • C. Difficle
• Referral to treatment times • Admitted 95th percentile • Non-admitted 95th percentile • Incomplete 95th percentile
• Mixed sex accommodation breaches • Cancer
• All 2 week waits • week breast symptoms • 62 day wait from urgent referral • 62 day wait from the Cancer Screening Service • 62 day wait from a consultant upgrade
• A&E quality indicators
63

3.2 MRSA and C Difficile August 2011 – Four providers are under performing and nine localities are underperforming
3.2.1 Salford Royal had no MRSA cases in August, but remains red against plan year to
date. 3.2.2 Trafford has 4 cases of MRSA against a year to date trajectory of 2. NHS GM will
continue to monitor this against the agreed Action Plan.
3.2.3 Ashton, Wigan and Leigh are above their planned position for MSRA and have recently submitted and Action Plan outlining the steps that will be taken to improve the position. This Action Plan is being reviewed by HPA colleagues to ensure its’ actions are comprehensive.
3.2.4 Eight localities are over trajectory and each have submitted an Action Plan which has
been scrutinised by HRA 3.2.4 During October, Stepping Hill experienced four C Diff cases. NHS GM has responded by taking following actions:
• liaising with public health colleagues to set out the standards required • engaging clinicians in antibiotic stewardship across primary and secondary care
pathways • requiring each case to be forensically examined until each case is fully explained • issuing communication to GP about this type of infection
3.2.5 From 2 November 2011, E.coli data will be published on a monthly basis and will cover the first four months of surveillance (June to September 2011) E. coli data will thus be included in the next scheduled report.
64

3.3 18 weeks RTT July 2011 – Four providers are underperforming
Graph 1: Royal Bolton - RTT admitted adjusted by speciality July 11
Issue: • Underperforming on
RTT admitted 95th percentile in July 2011 Royal Bolton continues to fail to meet this target. An action plan is in the process of being agreed and the Local Commissioner is agreeing increased level of activity.
Graph 2: Pennine Acute – RTT admitted adjusted by speciality July 11
Issue: • Underperforming on
RTT admitted 95th percentile in July 2011 October’s weekly performance is currently 88.4% and is expected to reach the It is anticipated that the target will be achieved in October 2011. Detailed trajectories are being prepared by speciality to ensure that the target is managed at speciality and aggregate level.
Graph 3: Central Manchester – RTT admitted adjusted by speciality July 11
Issue: • Underperforming on
RTT admitted 95th percentile in July 2011 The backlog is continuing to reduce and is on trajectory for achievement at 1 January 2012. The backlog of patients at 23 October is1475. Small numbers of urology patients are
65

now being seen at Alder Hey although some time was lost as a result of delays in contacting patients.
Graph 4: Stockport – RTT admitted adjusted by speciality July 2011
Issue: Underperforming on RTT admitted 95th
percentile in July 2011 Stockport is making steady progress to clear the backlog. On 17 October, 183 backlog cases with a forecast target of 89.9% for that week.
3.3.1 The August RTT data confirms this position and Providers and Commissioners continue to
work towards ensuring patients are treated. The Table below shows the predicted achievement date for GM’s four Providers under pressure with RTT.
Table 3: Forecast Referral To Treatment times from September 2011 to January 2012
Projected Projected Projected Projected Projected
90% Admitted RTT Sep-11 Oct-11 Nov-11 Dec-11 Jan-12
Pennine Acute Hospitals NHS Trust 84.00% >90% >90% >90% >90%
Central Manchester University Hospitals NHS FT 78.40% 76.53% 76.53% 82.14% >90%
Stockport NHS FT <90% <90% >90% >90% >90%
Royal Bolton Hospital NHS FT <90% <90% <90% >90% >90%
3.4 MSA Breaches August 2011 – Salford and Bolton localities are underperforming 3.4.1 There are two localities underperforming - NHS Salford’s Performance and NHS Bolton.
Bolton continues to work with Royal Bolton to determine the number of breach days and are applying the penalty on a quarterly basis.
3.4.1.1 NHS Salford’s MSA breach rate in August 2011 was significantly higher than the England
average. Salford Royal Foundation NHS Trust (SRFT) has an action plan to eliminate mixed sex accommodation which is on track and in some instances being delivered before the expected date. SRFT are nearing completion on the PFI and NHS Salford negotiated that where breaches were within emergency admission unit (EAU)/admission wards (until
66

November 2011) that these breaches are not subject to sanctions but were still reported. The move to the new facilities for EAU is now complete and early reports suggest no breaches from these areas although October’s position will not be confirmed until early November 2011.
3.4.1.2 Regular meetings are held between SRFT and NHS Salford and this is building assurance
between Provider and Commissioner that the necessary steps are being taken to eliminate mixed sex accommodation.
3.4.1.4 SRFT is breaching the step down of patients from the intensive treatment unit (ITU) and
high dependency unit (HDU). The movement of critical care/HDU and the rationalisation of some of these speciality beds will impact on the elimination of mixed sex accommodation in these areas.
3.4.1.5 The one potential problem area remaining is the step-down from neuro-HDU to rehab,
then onto repatriation to the referring trust, where the referring trust has no vacant beds. NHS GM Director of Policy and External Relations and the Greater Manchester Neurosciences Director has a meeting with Acute Trusts to agree a way forward.
3.5 Cancer - July 2011 3.5.1 Overview of Commissioner Performance
3.5.1.1 Ashton, Leigh & Wigan; Bury and Oldham are the poorest performing localities in August
2011, underachieving or failing two of the five cancer headline measures. Table 4 on the following pages shows the performance for all nine cancer targets, including the five headline measures).
3.5.2 Overview of Provider Performance 3.5.2.1 The Christie, Pennine Acute and Central Manchester are the poorest performing
providers in August 2011, underachieving or failing three of the five cancer headline measures. Table 5 on the following pages shows the performance for all nine cancer targets, including the five headline measures
67

Table 4 – Commissioner Performance in August 2011
Headline Headline
Headline Headline Headline
= service not provided
Total Total Total Drug
Treatments Surgery
Radiotherapy Treatments
Total Total Total
Suspected Cancer - Two Week Wait
Breast Symptom - Two Week
First Treatment -
31 Day
Subsequent Treatment -
31 day
Subsequent Treatment -
31 day
Subsequent Treatment - 31
day
Urgent Referrals -
62 day
Screening - 62 day
Upgrade - 62 day
A’ton, Leigh and Wigan 99.0 99.3 98.1 100.0 96.3 100.0 75.7 87.5 100.0 Bolton 98.7 97.0 100.0 100.0 100.0 100.0 87.5 100.0 50.0 Bury 95.8 97.9 95.6 100.0 100.0 100.0 69.4 100.0 50.0 Hey’d, M’ton & R’dale 97.1 100.0 95.1 95.7 100.0 100.0 87.5 100.0 25.0 Manchester 94.3 94.2 100.0 100.0 100.0 100.0 88.5 92.3 60.0 Oldham 97.3 98.2 100.0 100.0 100.0 100.0 75.0 100.0 60.0 Salford 99.1 100.0 94.3 100.0 100.0 100.0 87.8 100.0 100.0 Stockport 96.3 96.8 99.1 100.0 100.0 100.0 80.5 100.0 88.9 Tameside and Glossop 97.2 95.2 100.0 100.0 100.0 100.0 92.3 100.0 100.0 Trafford 95.2 97.4 95.6 100.0 100.0 100.0 88.6 100.0 93.3
Table 5 – Provider performance in August 2011
Headline Headline
Headline Headline Headline
Total Total Total
Drug Treatments
Surgery Radiotherapy Treatments
Total Total Total
Suspected Cancer - Two Week Wait
Breast Symptom - Two Week
First Treatment -
31 Day
Subsequent Treatment -
31 day
Subsequent Treatment -
31 day
Subsequent Treatment -
31 day
Urgent Referrals - 62
day
Screening - 62 day
Upgrade - 62 day
Central Manchester 92.2
100.0 100.0 100.0
84.8 100.0 33.3
Christie
98.3 100.0 100.0 100.0 52.8 66.7 52.6
Pennine Acute 96.5 98.5 97.1 94.7 100.0
81.6 85.7 40.0
Royal Bolton 98.8 97.3 98.9 100.0 100.0
92.1 100.0 0.0
Salford Royal 97.4 100.0 94.0 100.0 100.0
89.1 - 100.0
South Manchester 94.7 94.6 98.3 100.0 100.0
89.0 100.0 100.0
Stockport 96.4 97.9 98.9 100.0 100.0
84.9 100.0 93.3
Tameside 97.3 95.3 100.0 100.0 100.0
92.0 - 100.0
Trafford 96.7
94.1 - 100.0
93.8 - 96.2
W’ton, Wigan and Leigh 99.2 99.2 100.0 100.0 93.3 - 78.8 92.9 100.0
68

3.5.3 62-Day Treatment Target (Urgent Referrals) 3.5.3.1 Performance against the 62 day treatment standard represents the greatest
concern for NHS GM as year to date performance is worsening. It is unacceptable that patients within the network continue to receive treatment outside the national standard.
3.5.3.2 A key reason for this failure is the inability of the network to efficiently manage
inter provider transfers (ITTs) with only 59% of patients being treated within 62 days where there is an ITT.
3.5.3.3 A critical failure is to ensure the timely onward referral of patients where ITTs are
required as part of the cancer care pathway. The percentage of communication and referral proformas (CaRPs) sent by day 42, the minimum acceptable standard to achieve this target (see Table 8) is unacceptably low (56%). NHS GM is setting this as a priority for the coming months.
3.5.3.4 Monitor has clarified its regulatory position in relation to the achievement of the 62
day standard. In future, Monitor will apply a score of 1.0 to the governance risk rating of all the foundation trusts in Greater Manchester and Cheshire Cancer Network (GMCCN) that are breaching the standard after re-allocating breaches, where the patient was referred after 42 days by the referring provider. Trusts will continue to be scored in this way until it is clear that this issue has been resolved. As with all other 1.0 rated targets, a failure of this target for three consecutive quarters will result in a trust being considered for escalation to determine whether it is in significant breach of its terms of authorisation.
3.5.3.5 Based on Quarter 1 performance, the NHS North of England requested recovery
plans from the following commissioning localities within the network: Bury, Oldham, Manchester, Stockport, Tameside, Salford, Bolton and Central & East Cheshire. A recovery plan has subsequently been requested by NHS GM from NHS Ashton, Leigh & Wigan.
3.5.3.6 NHS GM has used these plans and meetings with local Commissioning leads to
develop a recovery plan which includes:
• specific guidance and instructions to locality (clinical commissioning group) commissioning managers and highlights the risks that they must address with trust provider colleagues;
• recommendations of the Helen Bellair’s review (as endorsed by the NHS GM Board in August 2011).
3.5.3.7 During October and November 2011, NHS GM ensure actions are taken to
address the fundamental short term risks that will prevent local achievement of this target. This will include action to:
• agree and implement a revised breach allocation policy for the Greater
Manchester & Cheshire Cancer Network area; • performance manage and significantly improve the communication of cancer
referrals from local hospital cancer multidisciplinary teams (MDTs) to specialist (tertiary provider) MDTs;
• ensure more robust performance management arrangements are put into place by providers and commissioners;
69

• ensure that agreements are reflected in contracts and formal regulatory arrangements.
3.5.3.8 The NHS GM recovery plan is designed is to achieve the 62 day cancer wait
target across GM and Cheshire by the end of the 2011/12 financial year. NHS GM are working to include the achievement of the percentage of CaRPs sent by 42 days to a contractual minimum standard for 2012-13.
3.6 A&E Performance 3.6.1 A&E Quality Indicators 3.6.1.1 There are five A&E quality indicators, which were introduced in the 2011/12
Operating Framework. These are listed below:
• HQU09 – Unplanned reattendance rate; • HQU10 – Total time in the A&E department; • HQU11 – Left without being seen rate; • HQU12 – Time to initial assessment; • HQU13 – Time to treatment.
3.6.1.2 Commissioning Business Service has prepared an analysis on HQU10, HQU11,
HQU12 and HQU13 using the 2011-12 Secondary Uses Services (SUS) extract mart data extracted on 14 October 2011. Data from the NHS Information Centre report is available for comparison for April and May 2011 and in some areas this shows a small amount of variation to the SUS data.
3.6.2 HQU09 – Unplanned Reattendance Rate 3.6.2.1 The NHS Operating Framework 2011/12 states that unplanned reattendance
rates should be between 5% and 1%. DoH is currently re-visiting the definition of this indicator and may decide to amend it in due course.
3.6.3 HQU10 – Total Time in the A&E Department
This indicator is broken down into three parts: • median time to departure, • 95th percentile of times (the time by which 95% of patient departed A&E) • single longest time.
3.6.3.1 This indicator is also broken down into admitted and non-admitted patients,
however, only the admitted data is reported in this report. The 2011/12 Operating Framework states that a 95th percentile wait of above four hours may trigger intervention. There are A&E concerns at a number of GM Providers as shown in the Table below:
70

Table 6: A&E Departments failing to meet 95% target during October
Pennine Acute Issue: • Rated red against target of 95% year to date.
Pennine Acute continues to struggle to maintain a consistent and resilient service across all sites and has experienced significant challenges at the North Manchester General Hospital. Site performance at NMGH however remains below the target and this poor performance is only compensated for by performance on the other sites. Pennine Acute have been finding it difficult to recruit to A&E and are having to rely on agency doctors which presents issues with supervision and higher number of patients being admitted rather than being assessed and discharged in A&E. Until a reasonable level of consultant staff are working from 8am – 12pm each weekday and 12 hours on a Saturday and Sunday there will continue to be volatility across all of the sites. Pennine Acute continues to look fragile in securing a satisfactory patient experience in A&E. Stockport Issue:
• Rated red against target of 95% year to date. Stockport’s A&E performance has reduced during October (four weeks below the target) and further action is being put in place to improve performance to enable achievement of the target for the year. NHS GM has requested further assurance that the Urgent Care Strategy engages with the whole local economy to ensure that it is resilient.
CMFT Issue: • Failure to perform in October
October saw a performance at MRI dip below the target for three consecutive weeks in October. CMFT MRI Emergency Department saw increased attendances over and the age profile of these has been in the 18-25 yr category as a result of ‘Fresher’s Week’ and despite the Trust being actively involved with the University around the ‘Choose Well’ campaign and staff from the emergency department attending events. IST is working with the Trust on flow issues and performance is being monitored by a Health Economy wide including weekly teleconference calls. As at 23 October, target is being achieved. Wrightington, Wigan and Leigh
Issue: • Performance dipping in October
WWL experienced a dip in performance for two weeks in October and actions are being put in place to ensure the performance is improved. 3.6.4 HQU11 - Percentage of Patients Attending A&E That Left Before Treatment 3.6.4.1 The target for the percentage of patients attending A&E that left before treatment
is 5% or less. Only one Provider (Tameside) has a year to date figure above the target of 5.1%.
71

3.6.5 HQU12 - Time to Initial Assessment 3.6.5.1 This indicator is broken down into three parts: median time, 95th percentile of
times (the time by which 95% of attendances were assessed) and single longest time. The 2011/12 Operating Framework states that it is good practice to have all patients assessed within 20 minutes of arrival and a 95th percentile time of above 15 minutes may trigger intervention.
3.6.6 HQU13 - Time to Treatment 3.6.6.1 This indicator is broken down into three parts: median time, 95th percentile of
times (the time by which 95% of attendances were treated) and single longest time. The 2011/12 Operating Framework states that a median time of above 60 minutes may trigger intervention.
3.6.7 Conclusion 3.6.7.1 NHS GM will be working with local Commissioners and Trusts to collate the
published indicators and validate in a more timely way. Overall, the results of the A&E Quality Indicators suggest that there is further work to be undertaken with Providers in GM and Commissioners to ensure a better patient journey through A&E services and robust data collection methods.
72

4 Diagnostics for the 15 key diagnostic tests and procedures - August 2011 4.1 This information taken from the SHA monthly data pack, which is sourced from
Unify2. Table 7: Diagnostics by Provider Organisation – August 2011 Provider Organisation Total
waiting Number waiting
6+ weeks
% waiting 6+ weeks
Number waiting 13+
weeks
% waiting 13+
weeks
Central Manchester University Hospitals NHS Foundation Trust 4,764 810 17.0% 214 4.5% Christie NHS Foundation Trust 315 0 0.0% 0 0.0% Pennine Acute Hospitals NHS Trust 8,077 975 12.1% 60 0.7% Royal Bolton Hospital NHS Foundation Trust 1,679 44 2.6% 0 0.0% Salford Royal NHS Foundation Trust 3,670 7 0.2% 0 0.0% Stockport NHS Foundation Trust 2,167 0 0.0% 0 0.0% Tameside Hospital NHS Foundation Trust 2,609 148 5.7% 3 0.1% Trafford Healthcare NHS Trust 1,923 5 0.3% 0 0.0% University Hospital of South Manchester NHS Foundation Trust 2,280 142 6.2% 4 0.2% Wrightington, Wigan and Leigh NHS Foundation Trust 3,386 141 4.2% 6 0.2% 4.2 Central Manchester Foundation Trust 4.2.1 Work continues in Manchester to improve the performance against the six week
diagnostic indicator with weekly teleconferences held with NHS GM, local Commissioners and CMFT. The number of diagnostics waiting longer than 6 weeks as at 23 October is 708 (admitted and non admitted pathways) with the majority of the diagnostics relating to Gastroenterology.
4.2.2 A revised trajectory has been submitted for diagnostics which indicates that the backlog
will be cleared by the end of February (for adults) and by end of March 2012 for children. Commissioners are working to pull this trajectory forward by sourcing alternative provision within GM for adults and looking to identify availability of geographically wider diagnostic provision for children.
4.3 Pennine Acute 4.3.1 Work continues across the North East Sector to improve performance against the six
week diagnostic indicator. Robust governance is in place, with weekly meetings with the
73

Pennine Acute Hospitals NHS Trust taking place to assess improvement and ensure actions within the agreed recovery plan are being undertaken as agreed. There has been a significant reduction in the number waiting and it has reduced to approximately 80 at the end of October. Therefore, there is further work to do to improve this situation further and to ensure adequate surveillance so that the situation does not represent itself.
4.3.2 NHS Heywood, Middleton & Rochdale also intends to review associate PCT
relationships with NHS Manchester in order to assess the position with Central Manchester University Hospitals NHS Foundation Trust and implement appropriate actions to mitigate any underperformance.
5 Ambulance Performance 5.1 NHS Blackpool, as lead commissioner for North West Ambulance Service (NWAS) has
prepared an update on current performance and developments for the ambulance service for the Greater Manchester area. A table detailing the new categorisations for ambulance calls is contained in the appendix. Category A calls are now categorised as red 8 and 19 minute.
5.2 Greater Manchester Performance & Activity 5.2.1 Red 8 minute performance across Greater Manchester was 75.33% in September 2011,
bringing the cumulative position for Greater Manchester to 73.68%. 5.2.2 This position has improved from a low point of 69.94% in June 2011 following the
implementation of the new dispatch system (CAD) at the end of May 2011. Performance over recent months has been 73.56% in July and 79.01% in August 2011.
5.2.3 Performance in Greater Manchester has historically not been as high as the other sub
regions and NWAS are addressing this through the work being undertaken by the turnaround team. The challenge in Greater Manchester will now be to maintain performance above 75% with constituent PCTs working with NWAS to support performance. One of the ways this can be supported is through management of handover and turnaround delays at acute trusts via monitoring of the information held in the online reporting system.
5.2.4 Cumulative red 19 minute response performance at the end of September 2011 was
96.12% for NWAS and 95.46% across Greater Manchester. This continues to remain above the national target of 95%.
5.2.5 A summary of red 8 minute performance for Greater Manchester, NWAS and the other
sub regions is shown in table 8, together with red activity across Greater Manchester, which is currently 4.3% above plan (2,787 incidents).
74

Table 8: Greater Manchester Red Performance and Activity
Primary Care Trust 8 mins Plan Actual Actual % 8 minsAshton Leigh & Wigan PCT 74.05% 6,955 7,166 211 3.03% 75.43%Bolton PCT 70.42% 6,123 6,158 35 0.57% 69.99%Bury PCT 72.22% 4,001 4,423 422 10.55% 71.40%Heywood, Middleton & Rochdale PCT 71.11% 5,186 5,401 215 4.15% 68.70%Manchester PCT 81.35% 15,522 16,442 920 5.93% 80.10%Oldham PCT 73.00% 4,999 5,547 548 10.96% 71.93%Salford PCT 77.59% 5,963 5,769 (194) (3.25%) 74.81%Stockport PCT 74.74% 5,993 6,169 176 2.94% 69.39%Tameside & Glossop PCT 73.87% 5,926 6,244 318 5.37% 70.74%Trafford PCT 73.72% 4,186 4,331 145 3.46% 71.28%OOA / Unknown 0.00% 19 10 (9) (47.62%) 50.00%
Greater Manchester 75.33% 64,873 67,660 2,787 4.30% 73.68%Cheshire & Mersey 79.03% 56,910 56,895 (15) (0.03%) 77.10%Lancashire 81.40% 34,127 36,177 2,050 6.01% 80.66%Cumbria PCT 77.03% 9,472 10,262 790 8.34% 77.15%
Grand Total 77.97% 165,382 170,994 5,612 3.39% 76.50%
September 2011 RedMonthly Cumulative
Performance Activity Variation to Plan Performance
5.3 Paramedic Emergency Services (PES) Financial Projections & Impacts for the
North West 5.3.1 At the end of September the cumulative cost of over activity associated with the PES
contract was £1.45m at full cost. The projected full year effect of this over performance amounts to £4.24m across the North West. This projection allows for expected additional demand over the winter period.
5.3.2 The first £1.3m of additional activity is charged at full cost with anything thereafter
charged at a marginal rate of 50%. The £1.3m is already paid by PCTs as part of the regular monthly payment made to NHS Blackpool. Allowing for this adjustment in relation to the projected over performance, the projected year end cost for PES is £2.77m leaving a projected pressure of £1.47m across the North West.
5.4 NWAS Recovery Plan 5.4.1 A detailed implementation plan has been produced by the internal performance
turnaround team, which is used to monitor progress on a weekly basis. The key elements of the plan include:
• Increasing the use of rapid response vehicles (RRVs) in responding to red
responses; • Use of demand analysis and other information to support improvements in
production/efficiency; • Improving hospital turnaround times; • Enhancing the urgent care desk and urgent care service to support appropriate
response to 999 calls; • Strengthening of local operational management and accountability.
5.4.2 The turnaround team is currently focused on finalising winter plans to ensure that
response time performance can be optimised throughout the winter period and commissioners are engaged with NWAS in this process.
75

5.5 Accountability Agreement 5.5.1 The 2011/12 Accountability Agreement lays out the principles and process by which
NHS North West will receive assurance that NWAS will reach foundation trust status, as determined within the formal tripartite agreement document between NWAS, NHS North West and NHS Blackpool, as lead commissioner.
5.5.2 This agreement provides the framework within which NWAS can clearly demonstrate its
progress and, therefore, maintain their present operational and strategic independence. It sets out the project milestones and covenant tests against which NHS North West will performance manage NWAS.
5.5.3 The agreement is clearly linked to the recovery trajectories. It is closely monitored via
the Finance & Contracting Group, with escalation to the Strategic Partnership Board, if required. The trajectories against plan are classified as green and on track. There are no issues to report.
5.6 Commissioning for Quality and Innovation (CQUIN) 5.6.1 Following agreement with NWAS on CQUIN for 2011/12, the trust submitted scheme
outlines supported by project plans for the five PES CQUIN schemes listed below:
• Acute Myocardial Infarction (Regional scheme as part of Advancing Quality); • Development of an urgent care service to provide more appropriate disposition of
calls (particularly green category calls through usage of ‘Hear & Treat’); • Development of a Paramedic Emergency Service (PES) emergency contact centre
to support future management of calls and care pathways and rationalise existing call centres;
• Collation of the information required for clinical quality outcome indicators; • Development of complementary resources to support access to defibrillation in the
event of cardiac arrest, including access to community first responders. 5.6.2 CQUIN schemes for patient transport services (PTS) that focus on improving patient
experience have also been agreed. The scheme outlines for the PTS elements of CQUIN have also been received.
5.6.3 Evidence has been provided by NWAS regarding work that has been undertaken to
meet the milestones set out in the project plans. The first milestones were reviewed by the ambulance commissioning team and a recommendation made to the Ambulance Strategic Partnership Board to approve payment for the quarter 1 milestones.
5.7 Quality 5.7.1 The national ambulance clinical quality indicators continue to be published on the
Department of Health website. Data has now been published up to August 2011 NWAS is now the top performing ambulance trust for 8 minute response times.
5.7.4 August reporting also showed that NWAS had one of the lowest call abandonment rates
nationally (at 0.8% of calls abandoned before being answered) and that calls were
76

answered on average in one second, placing them second nationally compared to other ambulance trusts.
5.7.5 Further work is needed by the trust in relation to other quality indicators as NWAS have:
• the highest conveyance rate nationally, with 80% of calls being conveyed to A&E departments;
• One of the lowest rates for closing calls with telephone advice and the highest re-contact rate following a call being closed with telephone advice (38%).
5.7.6 NWAS are also one of six trusts that currently do not have a frequent caller protocol in
place. A procedure has been produced but this has not yet been agreed. NHS GM will work with the lead Commissioner to ensure that this is formalised and implemented.
5.7.7 The remaining clinical quality outcome indicators were expected to be reported towards
the end of October 2011 and collation of information for these quality indicators has been supported through CQUIN.
6 Collaboratively Commissioned Contracts 6.1 Collaboratively Commissioned Contracts – Month four position (September 2011) 6.1.2 The collaboratively commissioned and managed contracts across Greater Manchester
and the lead commissioners are: The Christie (NHS Oldham); district and tertiary cardiac (NHS Stockport); hyper acute stroke (NHS Stockport); neurology (NHS Salford) and cervical cytology (NHS Salford).
6.2 Finance and activity – Greater Manchester summary 6.2.1 As at month four, the majority of the GM collaborative contracts are performing against
plan. 6.2.2 The exception is the cardiac contract which continues to underperform with a month four
position is £345k (under). However, this is a reflection of the implementation of the Cardiac Strategy.
6.2.3 Some potential pressures have been identified in The Christie contract due to an
expected increase in transplant activity, which is being managed through the Cancer Commissioning Advisory Group and in the district/cardiac contract due to a potential need to increase the agreed activity. Any increase in activity will be met through the planned inter hospital transfer tariff adjustments.
6.2.4 As at month four, there is forecasted year end over performance of £704k in The Christie
contract and underperformance of £1.5m in the district/tertiary cardiac contracts. Clinical Quality – Greater Manchester Last month, Board agreed the key KPI’s to be collected on the Cardiac and Neurology
contracts. Progress against the delivery will be reported to NHS GM through the bi-annual lead Commissioning to CCB in February 2012 for Cardiac and March 2012 for Neurology.
77

6.3 Quality, Innovation, Productivity and Prevention (QIPP) and Commissioning for Quality and Innovation (CQUIN) plans 2011/12
6.3.1 The QIPP and CQUIN plans have been agreed for district/tertiary cardiac, tertiary cancer, neurology and NWAS.
6.3.2 The monthly lead commissioner report identifies the planned financial QIPP and CQUIN outcomes and lead commissioners have been asked to provide monthly progress updates. The 2011/12 QIPP plans have been achieved through the 2011/12 contract for cardiac and for cancer and neurology implementation plans are being developed.
6.3.3 As at month four, NWAS plans are in the process of being ratified by the Strategic Partnership Board and stroke QIPP plans are still to be developed following the 12 month review. Stroke CQUINs are covered in the main report.
6.3.4 The Clinical Commissioning Board requested that clinical risk profiling is applied to lead commissioner QIPP and CQUIN plans and this will be progressed over the next few months.
7 Mental Health Performance – Quarter 1 2011/12 7.1 This section begins a review of the key performance indicators available for Mental
Health focusing on Care Pathways and access to psychological therapies (IAPTs). The interim board report will look at the performance of Mental Health outreach services and gatekeeping to prevent inappropriate admissions.
7.2 Care Pathways 7.2.1 Graph 5 showing the Care Pathway Approach (where each patient is issued with a CPA)
shows that GM is achieving above the threshold. Graph 6 shows the % of patients who are referred to psychological therapies receiving therapy.
Graph 5: Care Pathway Approach - Quarter 1 2011/12
78

Graph 6: Percentage referred for psychological therapies receiving therapy - Quarter 1 2011/12
Plan set at zero
7.3 Improving Access to Psychological Therapies 7.3.1 There are a small number of performance issues which have been identified in GM
locality relating to IAPT services. It has identified the following issues: • Manchester as a having poor performance, based on their performance above
their agreed trajectory although low numbers of patients entering treatment programmes;
• Bolton, HMR; Tameside and Trafford appear to be below optimum prevalence rates
• Salford and Bolton appear to be performing below optimum performance levels for recovery rates;
• Ashton, Wigan and Leigh, Bury, Salford, Stockport and Trafford appear to waiting times exceeding the nationally agreed key performance indicators.
7.3.2 NHS GM will undertake further work during the next quarter to understand these
variances and to put in place recovery actions where performance continues to remain below the nationally agreed key performance indicators (when Quarter 2 information is available).
7.3.3 NHS GM will be undertaking an assessment of the performance of Mental Health services in terms of outreach service and gatekeeping services and designing an action plan to improve the quality of services where necessary.
Hilary Garratt Executive Director of Nursing, Quality and Performance
79

80

Page 1 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 9B 10 November 2011
REPORT OF:
Executive Director of Nursing, Quality and Performance
DATE OF PAPER:
28 October 2011
SUBJECT:
Greater Manchester Quality and Safety report.
IN CASE OF QUERY, PLEASE CONTACT
Hilary Garratt, Director of Nursing, Quality and Performance. Tel: 0161 212 6132
PURPOSE OF PAPER: This is the second quality and safety update report to the NHS Greater Manchester Board. It covers the following areas:
Care Quality Commission (CQC) inspections of dignity and nutrition of older people in acute settings
2011/12 CQUIN schemes Castlebeck, and Southern Cross Ofsted inspection at Manchester Children’s Services Indicative work programme for quality and safety
81
Page 2 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
Greater Manchester Quality and Safety Issues
Executive Summary This is the second Quality and Safety Report for the NHS Greater Manchester (GM) Board. It updates Board members on several quality issues: The first section informs the Board of the recent final report of the Care Quality Commission’s (CQC) inspections of dignity and nutrition standards in the care of older people in acute hospitals. Five GM hospitals were part of the review earlier this year. The second section updates the Board on Commissioning for Quality and Innovation (CQUIN) schemes defined locally with providers (national and regional schemes were covered by the previous paper). NHS GM is considering some Cluster-wide CQUIN schemes for 2012/13. The third section provides updates on how the safety of residents is assured in the homes of two care home providers which have caused concern recently: Castlebeck and Southern Cross. The fourth section reports the findings of a recent annual unannounced inspection of Manchester Social Care Services by Ofsted. The results are in line with those of neighbouring local authorities. The fifth and final section reports on the NHS Greater Manchester outline programme for quality and safety.
1. CQC Inspection on Dignity and Nutrition 2011 1.1 Throughout March-June 2011, the Care Quality Commission (CQC) inspected the standards of
dignity and nutrition in the care of older people in 100 acute hospitals; the final report was published in October.
1.2 The national picture arising from presents that of the 100 hospitals inspected:
45 hospitals met both standards (‘fully compliant’). 35 met both standards but needed to improve in one or both (‘fully compliant, with
improvements suggested’). 20 hospitals did not meet one or both standards (‘non-compliant, with improvements
required’). (based on the poorest performance found within any hospital) 1.3 The final report includes the Chair’s reflections on the findings of the inspection and draws
attention to three key themes underpinning poor care (and be reverse, good care): firstly, hospital leaders must create a culture in which good care can flourish, secondly, staff attitudes are critical, and thirdly, resources play a role. These are important messages for providers as well as commissioners concerned about quality of care in acute, but also community, and residential care organisations. Six Greater Manchester hospitals were part of the inspection, and NHS GM is monitoring the required improvements taking place. The findings relating to GM trusts can be seen in the dashboard in Appendix 1; only Stockport NHS Foundation Trust had ‘moderate’
82

Page 3 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
concerns identified against the nutrition standard; for other trusts, the CQC recorded ‘minor’ or no concerns.
2. 2011/12 CQUIN schemes 2.1 We have undertaken an exercise to gather all existing local 2011/12 CQUIN (Commissioning for
Quality and Innovation) schemes which localities agreed with their acute, mental health, or community provider organisations. The information gives an indication of which areas the local CQUINs currently cover (beyond those defined nationally and regionally). Areas most frequently covered in acute CQUIN schemes are discharge letters, end-of-life care, urgent care, safeguarding children and adults, and stroke care. Only some localities have included public health-focused schemes.
2.2 Having this information gives the GM community an opportunity to work with clinical commissioning groups (CCGs) to consider areas for developing potential Cluster-wide CQUIN schemes for 2012/13. NHS Greater Manchester (GM) has started work on this within the current contracting process, and is considering schemes on harm-free care, dementia care, dignity and nutrition, workforce, as well as potentially a GM-wide public health scheme. This is in response to a national focus on patient safety, and we know that harm causes unnecessary suffering to patients, demoralises staff, and is costly to the NHS.
2.3 The next Board paper will be able to report achievements against the regional CQUIN schemes on the Advancing Quality programme, and the Trauma Audit and Research Network (mentioned in the last paper).
3. Castlebeck, and Southern Cross 3.1 Castlebeck
3.1.1 Following the Board report in June 2011, the following provides an update in respect of the
strategies put in place by Greater Manchester localities to monitor individuals whose care has been commissioned from Castlebeck Care providers.
3.1.2 Localities across Greater Manchester continue with implementing a robust review process for
service users receiving their care package from Castlebeck Care. Many localities have taken the decision to repatriate a number of Service Users and are exploring procurement/ commissioning of care packages to meet individual need.
3.1.3 This work is ongoing and relates to many service users who have complex care needs and the
most appropriate care packages may take some time to arrange, however the Cluster has received assurances that frequent and robust monitoring systems are in place.
3.2 Southern Cross 3.2.1 Most of the Southern Cross homes in Greater Manchester have now transferred to their new
operator/ organisation. 3.2.2 Each locality has been monitoring Southern Cross care homes and there have been regular
communications with the emerging organisations. 3.2.3 Initially there was confusion from the new operators in respect of how many service users and
which locality funded the residents within their care homes. However, with effective partnership working this generally appears to have been resolved with a variety of payment arrangements being made to ensure continuity of business.
83
Page 4 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
3.2.4 Generally, localities have seen an improvement in the environment of many care homes with new
operators identifying programmes of refurbishment and update, all of which appear to have had a positive impact on patient outcomes.
3.2.5 Whilst it is acknowledged that it is ‘early days’ in respect of this transfer of responsibility, localities
are not reporting concerns that appear to be impacting on patient care. However, regular monitoring is continuing in the form of routine visits and ad-hoc unannounced visits.
3.2.6 Joint working with local authorities is continuing and where any issues are identified appropriate
action will be taken following established pathways e.g. Adult Safeguarding procedures. NHS GM will continue to actively monitor and feedback on improvements made.
4. Unannounced Ofsted inspection of Manchester City Council Children’s Services 4.1 Local Authorities are lead agencies for safeguarding children. Ofsted undertook an unannounced
inspection within Manchester City Council children’s services on 23 and 24 August 2011. The inspection sampled the quality and effectiveness of contact, referral, and assessment arrangements and their impact on minimising any child abuse and neglect; the inspection focussed mainly on Local Authority services.
4.2 The inspection identified no priority action, one area of strength (good multi-agency working),
several areas of practice that met the requirements of statutory guidance, as well as five areas for development. These included the need for greater rigor, and involvement of all family members in assessments, the need to embed the Common Assessment Framework, and to reduce some social worker case loads.
4.3 A recruitment and training initiative for qualified social workers is underway. Also, work on
complex families funded through the Community Budgets in two pilot areas of the city will bring evidence-based interventions to hard-to-reach families. Teams in these pilot areas are working with single assessments; a rollout across the city is being considered.1
5. Greater Manchester work programme for quality and safety 5.1 NHS GM is undertaking a number of initiatives to ensure that a clear line of sight remains on
quality and safety at both central and local level via CCGs. To this end we are working on a programme of work to ensure quality drives our corporate agenda and that we support and and assist in the development of CCGs. An outline of the work is given below:
1. The further development of an early warning system for Greater Manchester providers to
ensure GM commissioners are informed about quality and safety in provider organisations and any serious quality concerns can be detected and dealt with early.
2. Work on processes to support the prevention and management of Never Events is outlined in a separate Board paper. The intention is to make sure we minimise and ultimately eliminate the occurrence of Never Events, and when they do happen, we maximise learning from them across the system.
3. An assessment of commissioners’ and providers’ implementation of the recommendations from the Francis report (following events in Mid-Staffordshire NHS Foundation Trust), and from recent National Quality Board reports will provide assurance of relevant systems and thus support CCG authorisation.
1 More detail can be found in the Manchester City Council Children and Young People Overview and Scrutiny
Committee paper of 18 October 2011, which is available here: http://secure.manchester.gov.uk/egov_downloads/6_Results_of_he_Unnannounced_Inspection.pdf
84

Page 5 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
4. Working with contracting colleagues, we are developing a smaller number of Greater Manchester CQUIN schemes in a number of priority areas where we want to ensure we commission for safety right across the GM geography.
5. Developing harm-free care as an organisational culture as we move through the transition phase has never been more important. This will involve enabling the building of commissioning relationships between CCGs and providers of care to ensure a systematic approach to keeping patients safe develops.
6. We are working on developing the nursing and allied health professional leadership (AHP) capacity and capability for commissioning. Within a community of integrated practice across nursing and AHPs, we will develop professionals to serve effectively as CCG Board members as well as on other CCG functions.
7. We are developing a framework for ensuring that quality and safety are central to the QIPP (Quality Innovation, Productivity, and Prevention) programmes, and that clear quality and safety benefits can be measured.
8. We will be working with Strategic Health Authority and locality/CCG colleagues on developing our current quality reporting and monitoring processes further.
5.2 The North of England has recently developed an active quality dashboard, covering patient
experience, effectiveness, and safety. Appendix 1 reproduces the Greater Manchester section of the dashboard. This is a welcome starting point for our own quality monitoring, and we will be working with the Strategic Health Authority on strengthening this, avoiding duplication. In future reports we will include Mental Health and Community Services in the dashboard.
5.3 As raised in previous Board reports, NHS GM is ensuring that venous thromboembolism (VTE)
action plans are being produced and implemented and that necessary actions are being undertaken around the application of contract levers for Mixed Sex Accommodation.
5.4 The quality dashboard does highlight that NHS GM needs to look to secure improvements in
understanding the results from the staff survey as an indicator of quality and safety and we will support our local commissioners to do this. Healthcare acquired infections have been reported in the performance report.
5.5 NHS GM will work with NHS Tameside and Glossop to understand the significance and potential
impact of the current HSMR Figures. We will report back to Board in January at the latest. Hilary Garratt Executive Director of Nursing, Quality and Performance
85
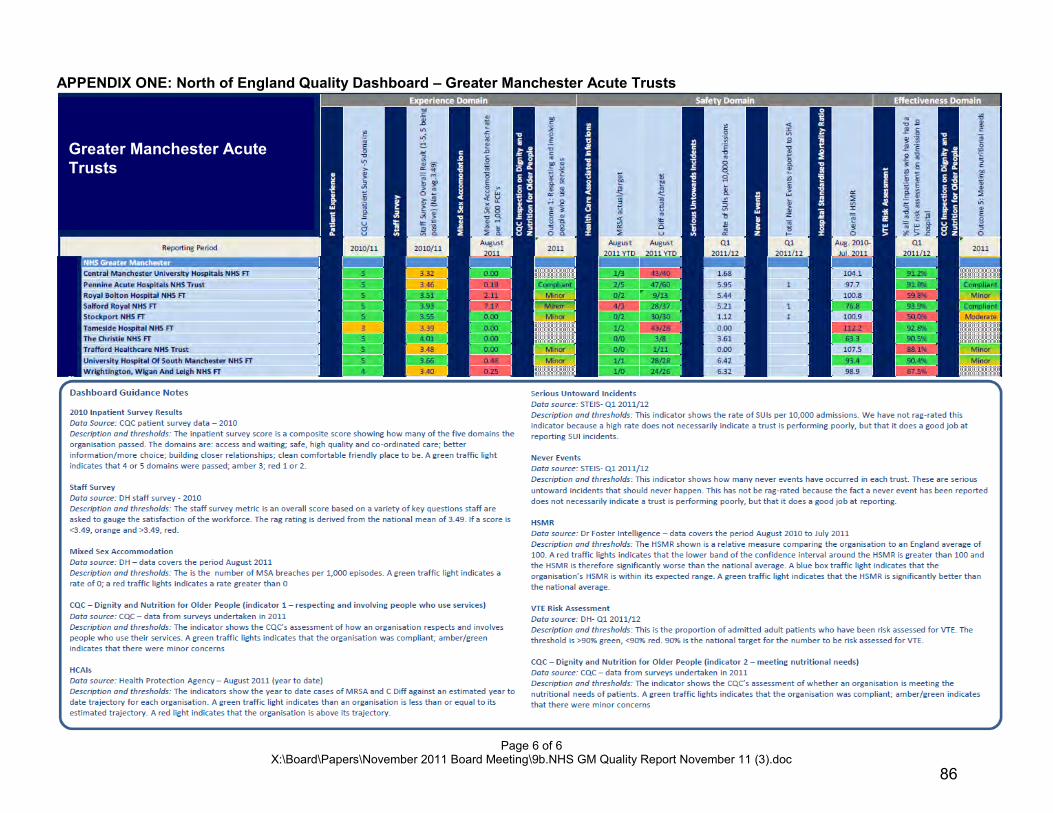
Page 6 of 6 X:\Board\Papers\November 2011 Board Meeting\9b.NHS GM Quality Report November 11 (3).doc
APPENDIX ONE: North of England Quality Dashboard – Greater Manchester Acute Trusts
Greater Manchester Acute Trusts
86

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 9c 10 November 2011 REPORT OF:
Director of Human Resources and Organisational Development
DATE OF PAPER: 28 October 2011
SUBJECT:
Human Resources Performance
IN CASE OF QUERY, PLEASE CONTACT
Andrea Anderson 0161 212 6138
PURPOSE OF PAPER: This paper provides an update on the performance of Human Resources across the PCTs in the NHS Greater Manchester cluster.
87

Human Resources Performance Executive Summary This paper provides an update on the performance of Human Resources across the PCTs in the NHS Greater Manchester Cluster. 1 Reporting Information 1.1 This report summarises the performance of Human Resources across NHS Greater Manchester,
by exception, and is based upon a snapshot of the workforce information recorded in the Electronic Staff Record (ESR) as at 30 September 2011.
1.2 Local intelligence has been collated and used to enhance the report in the following areas:
• Financial Information • Active Recruitment • ‘At risk’ Registrations • VSM Contract Holders
Local Information is also accurate as at 30 September 2011. 1.3 Reported financial information - The figures presented only account for the activity that has
taken place as at the reporting date (30 September 2011 for this report) and does not include predictions or known costs in the next period. Cumulative redundancy figures, for example, will only include the costs of those individuals who have actually left the organisation as at the reporting date and will not account for any known potential redundancies expected in the near future. It is important to note that for NHS Tameside & Glossop, the redundancy and MARS leavers are within this financial year and, therefore, their costs have been included, but the associated costs have been incurred in the previous financial year.
2 Exception Headlines 2.1 This section of the report focuses on the elements of HR performance that are either
recommended for urgent performance review or should be noted as well within target:
88

HOTSPOT / INFORMATION DETAILS 2.1 Bank & Agency Spend According to the financial information submitted by the localities for this exercise, total Agency and Bank costs for the month of September 2011 are £650,739 and £28,313 respectively. Total Expenditure on Bank and Agency for the period 01 April 2011 to 30 September 2011 are Agency £2,862,480 and Bank, £515,283.
2.1.1 NHS Manchester: The highest spender on Agency is NHS Manchester, with a spend for the month of September 2011 of £507,930 (78% of the total spend across the NHS Greater Manchester PCT Cluster that month) and £1,842,163 for the period 01 April 2011 to 30 September 2011 (64% of the total NHS Greater Manchester spend for the same period). NHS Manchester have not reported any spend on Bank working, although they do have 28 members of their locality work bank recorded in ESR. It is worth noting that NHS Manchester for the month of September have an active vacancy rate of 0.94% and, excluding their use of agency, are operating at 93% of their funded establishment FTE. 2.1.2 NHS Bolton & NHS Tameside & Glossop: Other comparatively high spenders across the 10 locality PCTs’ on Agency are NHS Bolton at £47,658 (7%) and NHS Tameside & Glossop £42,650 (6.5%) for the month of September. Both NHS Bolton and NHS Tameside & Glossop report a small spend on Bank working. In the absence of Actual Spent Establishment financial data for this period, the Agency spend for each organisation cannot be presented in this report as a percentage of the paybill. An indicative measure of spend on Agency against the FTE employed highlights the following trends in the three highest spending localities: NHS Manchester £1000 spent per FTE NHS Bolton £237 spent per FTE NHS Tameside & Glossop £225 spent per FTE
2.2 Performance Targets The setting of targets for HR would facilitate the identification of problem areas and indicators of organisational strength (potential ability to provide support to struggling localities).
2.2.1 Hotspot Areas Three key areas have been highlighted initially as ‘Hot Spots’ and are recommended for further investigation, monitoring and Management. Once objectives have been agreed targets can be proposed for the consideration and approval of the NHS Greater Manchester Board: Bank expenditure Agency expenditure Active Vacancies
89

2.3 Assignment Status
Programme Update The Assignment programme in NHS Greater Manchester Cluster was halted in July 2011. An update of the position of each locality in ‘assigning’ to Clinical Commissioning Groups (CCG’s) has been obtained by the Business Services Team. Please see Appendix 2 for a status update on Assignment to CCG’s from the NHS Greater Manchester Cluster
Up to the date that the assignment programme was halted for NHS Greater Manchester, seven out of the ten NHS Greater Manchester Localities have confirmed formal assignment to CCG’s. 2.3.1 Assignment Confirmed The following organisations have confirmed formal assignment of staff to a CCG: NHS Manchester *NHS Stockport NHS Ashton Wigan & Leigh NHS Bolton NHS Oldham NHS Bury NHS Tameside & Glossop *Please note that NHS Stockport report that they were mid the assignment process when the instruction to halt the process was given. 2.3.2 No Assignment The following PCT’s have reported that no assignments have been made. Three of these (asterixed) have made arrangements to ensure support to the CCG has been allocated to one or all of the four key roles determined by the Department of Health: *NHS Salford *NHS HMR NHS Trafford
2.4 Sickness Absence The Sickness Absence percentage for NHS Greater Manchester is an average of the percentages reported by each of the ten NHS Greater Manchester Organisations. Using this as the formula, NHS Greater Manchester is reporting an average monthly sickness of 3.24% for the month of September 2011 and an annual average sickness absence rate of 3.58%. Both average statistics for NHS Greater Manchester are below the QIPP Target of 3.6%
2.4.1 Organisations reporting RED or AMBER (above target) for sickness absence: NHS Manchester NHS Oldham NHS Bolton NHS Stockport NHS Trafford 2.4.2 Organisations reporting GREEN (on or below target) for Sickness Absence: NHS Bury NHS HMR NHS Salford NHE Ashton Wigan & Leigh NHS Tameside and Glossop
90

3 Improvements underway for the next Board Report 3.1. The next Board report will compare the current month banding tree with the banding structure in
place as at 01 April 2011. This information will be presented for NHS Greater Manchester as a whole, but will be available by locality also, should this be required. Using the structure as at 01 April 2011 as a benchmark, this will provide NHS Greater Manchester Board members with useful information about the changing shape of the organisation. Once a future structure and shape for the NHS Greater Manchester workforce has been determined along with any incremental staffing level changes, this tool will provide a visual track, by band, of the progress being made toward the desired organisational shape.
3.2. For the next reporting period, the Agency and Bank Spend will be available as a percentage of
the spent Paybill for the current comparable month. Agency figures will also be clarified as to what they represent (i.e. true Agency, Independent Contractors etc..) to ensure that the figures reported are truly comparable across organisations and are fully reflective of the actual costs being incurred in the use of peripheral workforce.
** Where the NHS Greater Manchester Board would like to investigate an anomaly within the
Human Resources key performance indicators (KPIs) in more detail, this can be requested and will be prepared by the Business Services Team in time for the next Report.
4 Recommendation 4.1 The NHS Greater Manchester Board is asked to note the Greater Manchester workforce
information and proposed future development. Andrea Anderson Director of Human Resources and Organisational Development
91

TRENDRED Movement away from Target
AMBER No Change (may be on target and green)
GREEN Movement toward Target
Measure Period Measure Period Position as @ 01 april 2011
Cumulatiive Fig. from 1st April
2011
2899 Aug-11 2875 Sep-11 N/A GREEN 2970 Not Applicable
2428.11 Aug-11 2410.34 Sep-11 N/A AMBER 2490.6 Not Applicable
2582 Aug-11 2559 Sep-11 N/A AMBER 2653 Not Applicable
231 Aug-11 233 Sep-11 N/A AMBER 240 Not Applicable
87 Aug-11 88 Sep-11 N/A GREEN 78 Not Applicable
30 Aug-11 39 Sep-11 N/A N/A Not Applicable 239
No. 1 1 N/A N/A N/A Not Applicable 16
Cost £60,953.69 £53,542.56 N/A N/A N/A Not Applicable £1,011,577.94
No. 0 0 N/A N/A N/A Not Applicable 2
Cost £0.00 £0.00 N/A N/A N/A Not Applicable £57,674.02
No. 3 4 N/A N/A N/A Not Applicable 20
Cost £48,556.00 £0.00 N/A N/A N/A Not Applicable £286,605.00
19 Aug-11 7 Sep-11 N/A N/A Not Applicable 90
15.76% Aug-11 15.67% Sep-11 13.6% National Avg. AMBER Incomplete data
set Not Applicable NOTES:The NHSGM overall % for Sickness Absence is the mean of all % returned by NHSGM Cluster PCT's.
59 Aug-11 51 Sep-11 N/A N/A Not Applicable Not Applicable
2.12% Aug-11 11.47% Sep-11 To Be Established AMBER Incomplete data set Not Applicable NOTES: The NHSGM overall % for Sickness Absence is the mean of all %
returned by NHSGM Cluster PCT's.
£434,396.55 Aug-11 £650,739.79 Sep-11 To Be Established RED Not Applicable £2,862,480.51 HOTSPOTS: HIGHEST THREE SPENDERS = NHS MANCHESTER, NHS BOLTON, NHS TAMESIDE & GLOSSOP
£49,479.13 Aug-11 £32,313.28 Sep-11 To Be Established AMBER Not Applicable £515,283.62
N/A N/A N/A
N/A N/A N/A
3.34% Jul-11 3.24% Aug-11 3.6% QIPP GREEN Incomplete data set Not Applicable
3.59% Jul-11 3.58% Aug-11 3.6% QIPP GREEN Incomplete data set Not Applicable
Future Reporting Working toward
Future Reporting Working toward
TRIDRANT 3 Organisational BehaviourSickness Absence Rate
(Average Calculation Month)NOTES: The NHSGM overall % for Sickness Absence is the mean of all % returned by NHSGM Cluster PCT's. HOTSPOTS: Following organisations are above the QUPP Sickness Absence Target: NHS Manchester, NHS Oldham, NHS Bolton, NHS Stockport, NHS Trafford
Annual Sickness Absence Trend(Average Calculation 12 Months)
Seco
nd-
men
ts In Future Reporting
Working towardFuture Reporting Working toward
Out Future Reporting Working toward
Future Reporting Working toward
Active Vacancy Rate
Bank
&
Agen
cy
Spen
d Agency
Bank
Sep-11
Total No. New Starters
Turnover Rate(Average Calculation)
Total No. Staff Registered 'At Risk'
Sep-11
Voluntary Redundancy Aug-11 Sep-11
Total No. Leavers
of w
hich
Rea
son
for L
eavi
ng is
Re
dund
ancy
/MAR
S
Compulsory Redundancy Aug-11
MARS Aug-11
TRIDRANT 1 Organisational Profile
Indicator
Previous Month Current Month
Trend
Comparison
CommentsHotspots
NHS Greater Manchester (Cluster)Reporting Period: SEPTEMBER 2011
PERFORMANCE STATUS
Funded Establishment (FTE)) 2479.92 Actual Spent Establishment
(FTE)) 2255.48Performance is above Target
Performance is slightly above target.
Performance is on or below Target
TRIDRANT 2 Organisational Movement
NHS GM Target
(Where Appropriate)
Performance Against Target
Against NHS GM Target or Comparison Position
Empl
oym
ent
Com
posi
tion
Total Headcount
Total Staff in post (FTE)
Substantive
FTC
Bank
92

FTE by Pay Scale / Band
Not AssimilatedConsultant
Dental AdhocDental Scale
Medical AdhocBand 1Band 2Band 3Band 4Band 5Band 6Band 7
Band 8aBand 8bBand 8cBand 8d
Band 9VSM
FTE Banding Tree - NHS Greater Manchester PCT Cluster
Pay Band NHSBury
NHSHMR
NHS Manchester NHS Oldham NHS Salford NHS
AWL NHS Bolton NHS Stockport NHS Tameside & Glossop NHS Trafford NHSGM
TOTAL
Not Assimilated 5.01 0.00 3.31 22.38 19.97 12.68 8.62 2.00 0.72 5.58 80.27Consultant 1.00 1.60 3.23 1.00 0.60 2.00 1.00 1.90 2.70 1.80 16.83
Dental Adhoc 0.00 0.00 0.00 0.00 0.30 0.45 0.73 0.35 0.30 0.00 2.13Dental Scale 0.00 0.00 1.37 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1.37
Medical Adhoc 0.00 5.50 2.30 0.00 0.45 0.23 0.00 0.51 0.17 0.00 9.16Band 1 1.55 0.00 51.86 0.50 52.72 0.00 0.00 0.00 0.00 0.00 106.63Band 2 15.93 2.10 20.15 34.14 20.96 7.31 7.61 12.26 8.72 1.00 130.18Band 3 22.10 9.99 73.01 22.03 28.65 18.81 16.29 13.83 23.45 15.07 243.23Band 4 32.36 20.25 74.57 26.09 34.90 26.36 19.66 17.14 21.56 15.41 288.31Band 5 27.87 28.61 74.68 23.41 45.17 38.37 27.79 24.72 29.64 22.20 342.46Band 6 41.22 25.13 47.86 28.70 34.91 26.85 39.71 18.32 24.51 16.00 303.20Band 7 23.65 34.09 63.80 30.64 42.88 29.73 36.88 25.89 31.91 31.83 351.29Band 8a 15.79 21.77 35.49 17.58 40.98 26.88 14.25 20.74 13.80 18.53 225.81Band 8b 10.65 11.40 33.29 11.79 18.14 17.13 12.36 3.00 11.64 13.18 142.58Band 8c 8.81 9.93 4.60 9.00 13.10 6.00 5.80 6.00 7.00 2.80 73.04Band 8d 7.22 5.11 17.70 4.80 5.00 6.00 7.30 5.00 4.00 3.00 65.13Band 9 2.32 0.00 0.00 2.00 1.40 1.00 1.30 1.00 0.00 2.00 11.02
VSM 4.00 0.00 4.00 5.00 0.00 0.00 0.00 4.00 7.00 0.00 24.00Totals 219.47 175.48 511.21 239.07 360.13 219.80 199.29 156.67 187.12 148.40 2416.64
FTE
Comments: A comparison Banding Tree presenting the organisational structure, by band, as at 01 April 2011 will be available for the next Board Report to provide a benchmark from which changes in the shape of the workforce can be identified. Please note that this information is available by locality if required.
93

94

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 10 10 November 2011 REPORT OF:
Jan Hutchinson - Lead Greater Manchester Director of Public Health, and Director of Public Health Bolton
DATE OF PAPER:
20 October 2011
SUBJECT:
GM Public Health Performance Report
IN CASE OF QUERY, PLEASE CONTACT
Will Blandamer Director, GM Public Health Network
PURPOSE OF PAPER: To inform the NHS Greater Manchester Board on the current performance on key performance indicators for Public Health for Greater Manchester. The paper is in three parts
1) performance on all age all cause mortality in Greater Manchester at a City Region and Local Authority level 2) the introduction of a “dashboard” approach to presentation of Key Public Health Indicators 3) An overview of the Adult health screening programmes in Greater Manchester.
The board is advised information on ante-natal and new born health screening will be presented in the January report in the context of a specific focus in that report on child and maternal health.
95

Greater Manchester Public Health Performance Report – November 2011 Executive Summary 1) All Age All Cause Mortality: Whilst Greater Manchester continues to perform well on progress to achieving the 2010 trajectory, this masks differential PCT performance. 2) Public Health Performance Dashboard: The information presented in the previous performance report is presented here in dashboard format for consideration. This will be updated as and when new information is available. 3) Health Screening – Adults: Greater Manchester has a strong collective understanding of its position and performance on key indicators for health screening programmes as a consequence of the co-ordinating role of the GM Screening Programme and the production of a 6 monthly detailed report from the programme is routinely considered by the GM Directors of Public Health Group. Overall performance on screening programmes is relatively good. Where there are local or GM actions required to address particular issues of concern a note of ‘actions for improvement’ is included in each section. The board are advised these actions are reported to the GM Directors of Public Health Group and will be reviewed in the context of the next GM Screening Programme report due early in the new year. Appendix 1 – All Age All Cause Mortality Reporting by PCT. 1 All Age All Cause Mortality 1.1 Whilst Greater Manchester continues to perform well on progress to achieving the 2010
trajectory, this masks differential PCT performance. 1.2 Areas of particular concern are Ashton Leigh and Wigan (although significant progress is
being made at pace to catch up from a low base), Tameside (where the locality board have signed off a detailed plan to strengthen and improve primary care management and engagement in accordance with the NST for Health Inequalities recommendations) and Oldham (where the reported position was adversely affected by the mid year population estimates and further work is being done to understand the position in more detail).
1.3 The very positive position of Stockport and the encouraging position of Manchester,
HMR, and Salford should be recognised. 1.4 NHS North West have identified 5 PCTs in the North West causing particular concern
and the GM PCT identified is ALW, on the grounds that as at April 2011 it is off trajectory for both male and female. The board will note the reported progress for males since April 2011 for that PCT.
96

1.5 Appendix one sets out the detailed times series analysis for each PCT.
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Greater Manchester. Source: NHS North West
Greater Manchesterestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09 jun
09au
g09
oct'0
920
09feb
10ap
r10 jun10
aug1
0oc
t10 2010
feb11
apr11 jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Commentary Overall the GM wide position appears positive although care should be taken to recognise the confidence limits of the reported position. The reported position of individual PCTs and action being taken is in Appendix I. NHS Greater Manchester, through the GM Public Health Network, continues to prioritise CVD, Cancer, Tobacco, Alcohol and Healthy Weight, and suicide prevention, as well as engaging with partners on wider determinants of health: worklessness, fuel poverty, ambition, crime, transport etc.
97
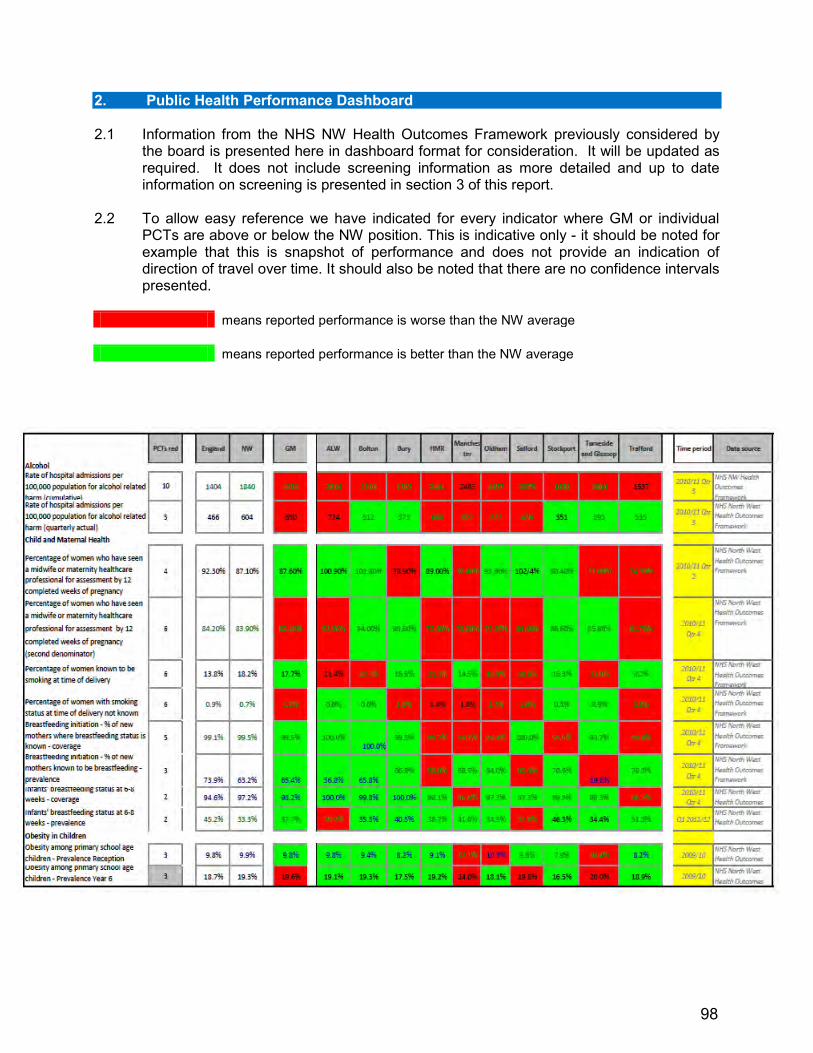
2. Public Health Performance Dashboard 2.1 Information from the NHS NW Health Outcomes Framework previously considered by
the board is presented here in dashboard format for consideration. It will be updated as required. It does not include screening information as more detailed and up to date information on screening is presented in section 3 of this report.
2.2 To allow easy reference we have indicated for every indicator where GM or individual
PCTs are above or below the NW position. This is indicative only - it should be noted for example that this is snapshot of performance and does not provide an indication of direction of travel over time. It should also be noted that there are no confidence intervals presented.
means reported performance is worse than the NW average means reported performance is better than the NW average
98

*NB - some data in the above is based on quarterly data not cumulative data which may provide a better position. Further work is underway to present cumulative data in this format
99
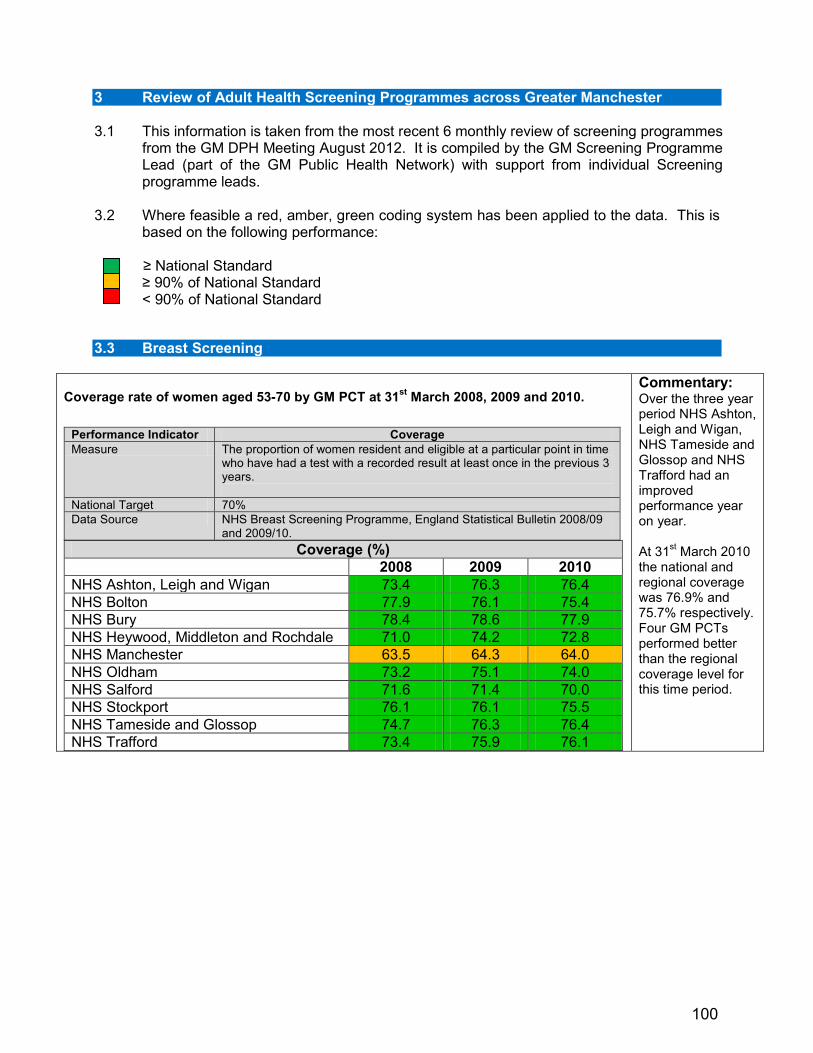
3 Review of Adult Health Screening Programmes across Greater Manchester 3.1 This information is taken from the most recent 6 monthly review of screening programmes
from the GM DPH Meeting August 2012. It is compiled by the GM Screening Programme Lead (part of the GM Public Health Network) with support from individual Screening programme leads.
3.2 Where feasible a red, amber, green coding system has been applied to the data. This is
based on the following performance: ≥ National Standard ≥ 90% of National Standard < 90% of National Standard 3.3 Breast Screening
Coverage rate of women aged 53-70 by GM PCT at 31st March 2008, 2009 and 2010.
Performance Indicator Coverage Measure The proportion of women resident and eligible at a particular point in time
who have had a test with a recorded result at least once in the previous 3 years.
National Target 70% Data Source NHS Breast Screening Programme, England Statistical Bulletin 2008/09
and 2009/10. Coverage (%)
2008 2009 2010 NHS Ashton, Leigh and Wigan 73.4 76.3 76.4 NHS Bolton 77.9 76.1 75.4 NHS Bury 78.4 78.6 77.9 NHS Heywood, Middleton and Rochdale 71.0 74.2 72.8 NHS Manchester 63.5 64.3 64.0 NHS Oldham 73.2 75.1 74.0 NHS Salford 71.6 71.4 70.0 NHS Stockport 76.1 76.1 75.5 NHS Tameside and Glossop 74.7 76.3 76.4 NHS Trafford 73.4 75.9 76.1
Commentary: Over the three year period NHS Ashton, Leigh and Wigan, NHS Tameside and Glossop and NHS Trafford had an improved performance year on year. At 31st March 2010 the national and regional coverage was 76.9% and 75.7% respectively. Four GM PCTs performed better than the regional coverage level for this time period.
100

GM Breast Screening Programmes Quarterly Round Length, % ≤ 36 months, October - December 2010, January - March and April - June 2011.
Performance Indicator Round Length Measure The percentage of eligible women whose first offered appointment is
within 36 months of their previous screen. National Minimum Standard
≥ 90%
National Target 100% Data Source NHS Breast Screening Programme, Quality Assurance Reference
Centre, North West Region. Quarterly Round Length % ≤ 36 Months
Oct – Dec Jan - Mar Apr - Jun Bolton 88% 89% 78% East Cheshire and Stockport 96% 86% 98% GM (Nightingale) 95% 90% 99% South Lancashire 96% 99% 96%
Commentary: Bolton programme narrowly missed this target in October – December and January – March but fell considerably below during April – June. East Cheshire and Stockport achieved the target in October – December and April - June but fell short for the period January – March.
GM Breast Screening Programmes Screening to Routine Recall, % ≤ 2 weeks, October to December 2010 and January to March 2011.
Performance Indicator Screening to Routine Recall Measure The percentage of women who are sent their
results within two weeks. National Minimum Standard ≥ 90% National Target 100% Data Source NHS Breast Screening Programme, Quality
Assurance Reference Centre, North West Region.
Screening to Routine Recall % ≤ 2 weeks
Oct – Dec Jan - Mar Bolton 97% 77% East Cheshire and Stockport 98% 99% GM (Nightingale) 97% 96% South Lancashire (formerly Wigan) 97% 94%
Commentary: With the exception of Bolton all screening programmes exceeded the minimum standard for both quarters.
101
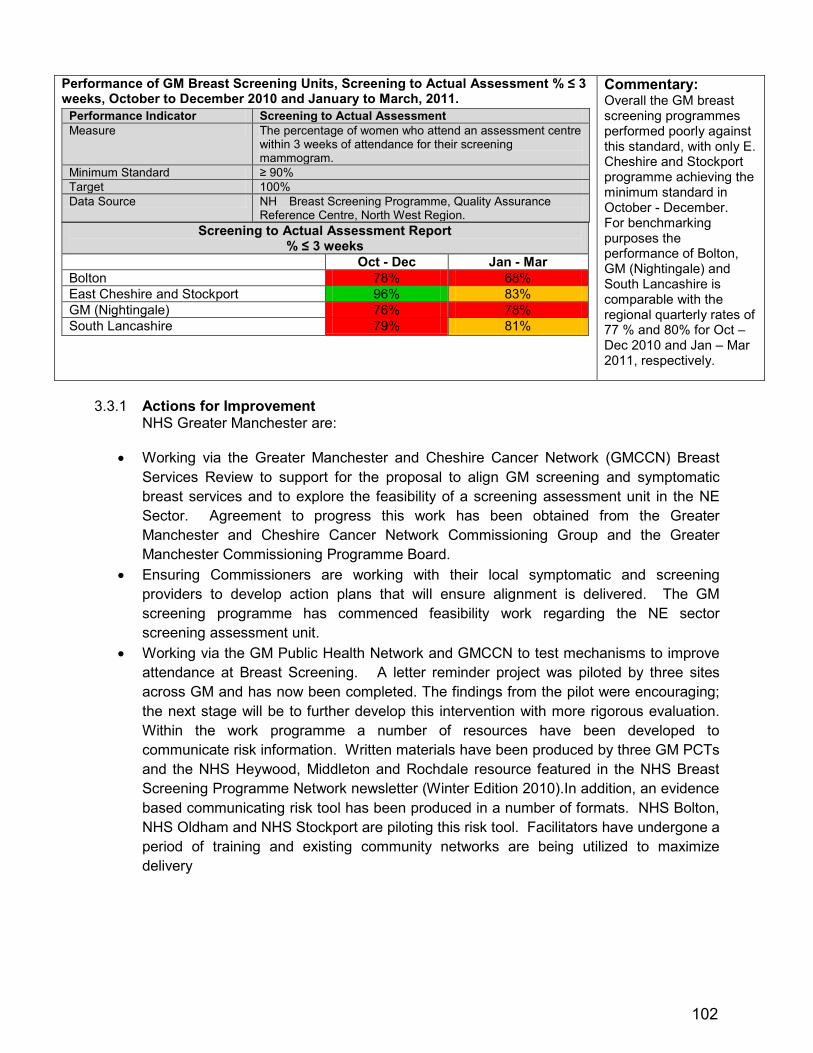
Performance of GM Breast Screening Units, Screening to Actual Assessment % ≤ 3 weeks, October to December 2010 and January to March, 2011.
Performance Indicator Screening to Actual Assessment Measure The percentage of women who attend an assessment centre
within 3 weeks of attendance for their screening mammogram.
Minimum Standard ≥ 90% Target 100% Data Source NH Breast Screening Programme, Quality Assurance
Reference Centre, North West Region. Screening to Actual Assessment Report
% ≤ 3 weeks Oct - Dec Jan - Mar Bolton 78% 68% East Cheshire and Stockport 96% 83% GM (Nightingale) 76% 78% South Lancashire 79% 81%
Commentary: Overall the GM breast screening programmes performed poorly against this standard, with only E. Cheshire and Stockport programme achieving the minimum standard in October - December. For benchmarking purposes the performance of Bolton, GM (Nightingale) and South Lancashire is comparable with the regional quarterly rates of 77 % and 80% for Oct – Dec 2010 and Jan – Mar 2011, respectively.
3.3.1 Actions for Improvement
NHS Greater Manchester are:
• Working via the Greater Manchester and Cheshire Cancer Network (GMCCN) Breast Services Review to support for the proposal to align GM screening and symptomatic breast services and to explore the feasibility of a screening assessment unit in the NE Sector. Agreement to progress this work has been obtained from the Greater Manchester and Cheshire Cancer Network Commissioning Group and the Greater Manchester Commissioning Programme Board.
• Ensuring Commissioners are working with their local symptomatic and screening providers to develop action plans that will ensure alignment is delivered. The GM screening programme has commenced feasibility work regarding the NE sector screening assessment unit.
• Working via the GM Public Health Network and GMCCN to test mechanisms to improve attendance at Breast Screening. A letter reminder project was piloted by three sites across GM and has now been completed. The findings from the pilot were encouraging; the next stage will be to further develop this intervention with more rigorous evaluation. Within the work programme a number of resources have been developed to communicate risk information. Written materials have been produced by three GM PCTs and the NHS Heywood, Middleton and Rochdale resource featured in the NHS Breast Screening Programme Network newsletter (Winter Edition 2010).In addition, an evidence based communicating risk tool has been produced in a number of formats. NHS Bolton, NHS Oldham and NHS Stockport are piloting this risk tool. Facilitators have undergone a period of training and existing community networks are being utilized to maximize delivery
102
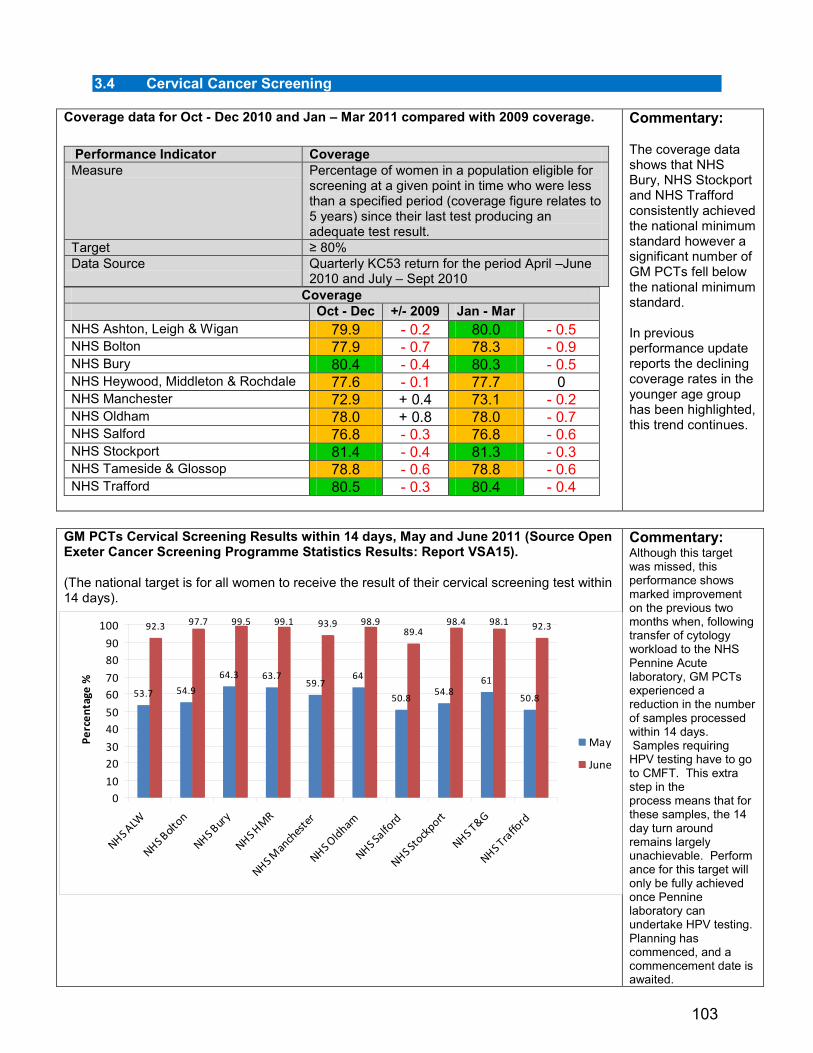
3.4 Cervical Cancer Screening
Coverage data for Oct - Dec 2010 and Jan – Mar 2011 compared with 2009 coverage.
Performance Indicator Coverage Measure Percentage of women in a population eligible for
screening at a given point in time who were less than a specified period (coverage figure relates to 5 years) since their last test producing an adequate test result.
Target ≥ 80% Data Source Quarterly KC53 return for the period April –June
2010 and July – Sept 2010 Coverage
Oct - Dec +/- 2009 Jan - Mar NHS Ashton, Leigh & Wigan 79.9 - 0.2 80.0 - 0.5 NHS Bolton 77.9 - 0.7 78.3 - 0.9 NHS Bury 80.4 - 0.4 80.3 - 0.5 NHS Heywood, Middleton & Rochdale 77.6 - 0.1 77.7 0 NHS Manchester 72.9 + 0.4 73.1 - 0.2 NHS Oldham 78.0 + 0.8 78.0 - 0.7 NHS Salford 76.8 - 0.3 76.8 - 0.6 NHS Stockport 81.4 - 0.4 81.3 - 0.3 NHS Tameside & Glossop 78.8 - 0.6 78.8 - 0.6 NHS Trafford 80.5 - 0.3 80.4 - 0.4
Commentary: The coverage data shows that NHS Bury, NHS Stockport and NHS Trafford consistently achieved the national minimum standard however a significant number of GM PCTs fell below the national minimum standard. In previous performance update reports the declining coverage rates in the younger age group has been highlighted, this trend continues.
GM PCTs Cervical Screening Results within 14 days, May and June 2011 (Source Open Exeter Cancer Screening Programme Statistics Results: Report VSA15). (The national target is for all women to receive the result of their cervical screening test within 14 days).
Commentary: Although this target was missed, this performance shows marked improvement on the previous two months when, following transfer of cytology workload to the NHS Pennine Acute laboratory, GM PCTs experienced a reduction in the number of samples processed within 14 days. Samples requiring HPV testing have to go to CMFT. This extra step in the process means that for these samples, the 14 day turn around remains largely unachievable. Performance for this target will only be fully achieved once Pennine laboratory can undertake HPV testing. Planning has commenced, and a commencement date is awaited.
53.7 54.9
64.3 63.759.7
64
50.854.8
61
50.8
92.3 97.7 99.5 99.1 93.9 98.989.4
98.4 98.1 92.3
010
2030
4050
6070
8090
100
NHS ALW
NHS Bolt
on
NHS Bur
y
NHS HM
R
NHS Man
ches
ter
NHS Oldham
NHS Salfo
rd
NHS Sto
ckport
NHS T&G
NHS Tra
fford
Perc
enta
ge %
May
June
103

3.4.1 Actions for Improvement
NHS Greater Manchester have: 3.4.2 Reconvened the GM cervical screening group under the leadership of Helen Lewis-
Parmar (Consultant in Public Health, HMR). Terms of reference and membership have been amended to reflect the new GM laboratory arrangements and the changing NHS context for commissioning & delivery of screening. Issues currently being addressed through the group include: • HPV Immunisation recording on Exeter and associated data sharing issues • Transfer to GMC/ NMC smear taker code • Alignment of direct referral to colposcopy across Greater Manchester
3.4.3 Ensured concerted focus on improving attendance at Cervical Screening. The Improving
Attendance Work Programme includes an intervention that specifically targets the 25 -29 year age group. The pilot involves sending a text message reminder to women that are due a cervical screen. The findings from the pilot project will be shared across GM at the end of 2011.
3.4.4 Working to improve the arrangements for nurse cervical smear taker training. The North
West Cervical Screening Quality Assurance Reference Centre (NWCSQARC) proposal for a centralised administration function for nurse cervical smear taker training has not progressed and communication from the SHA clearly states PCTs should take ownership. There is consensus that a GM approach should be developed for future sample taker training and the GM Screening Programme is coordinating this work. A task and finish group has been formed to develop a GM model and will report to the GM Cervical Screening Group, Directors of Public Health and the Clinical Commissioning Board.
3.4.5 GM is seeking DH approval to roll out implementation of HPV Triage and Test of Cure to
remaining GM PCTs. A co-ordinated approach across Greater Manchester via a Task and Finish Sub-Group of the Greater Manchester Cervical Screening Group has been agreed. Local Cervical Screening Leads would be responsible for ensuring that there is the capacity to deliver the key aspects of the programme locally and also for briefing the local Clinical Commissioning Groups and Locality Board.
3.4.6 The financial and contracting arrangements will be initially scoped as part of the contact
for population cytology with NHS Salford as Lead Commissioner. Central funding is available which in the first year to cover all implementation costs including laboratory costs; test kits; training and increased histology and colposcopy. In the second year of implementation costs will reduce as the peak of colposcopy activity is in the first year. By year three saving accrue.
104
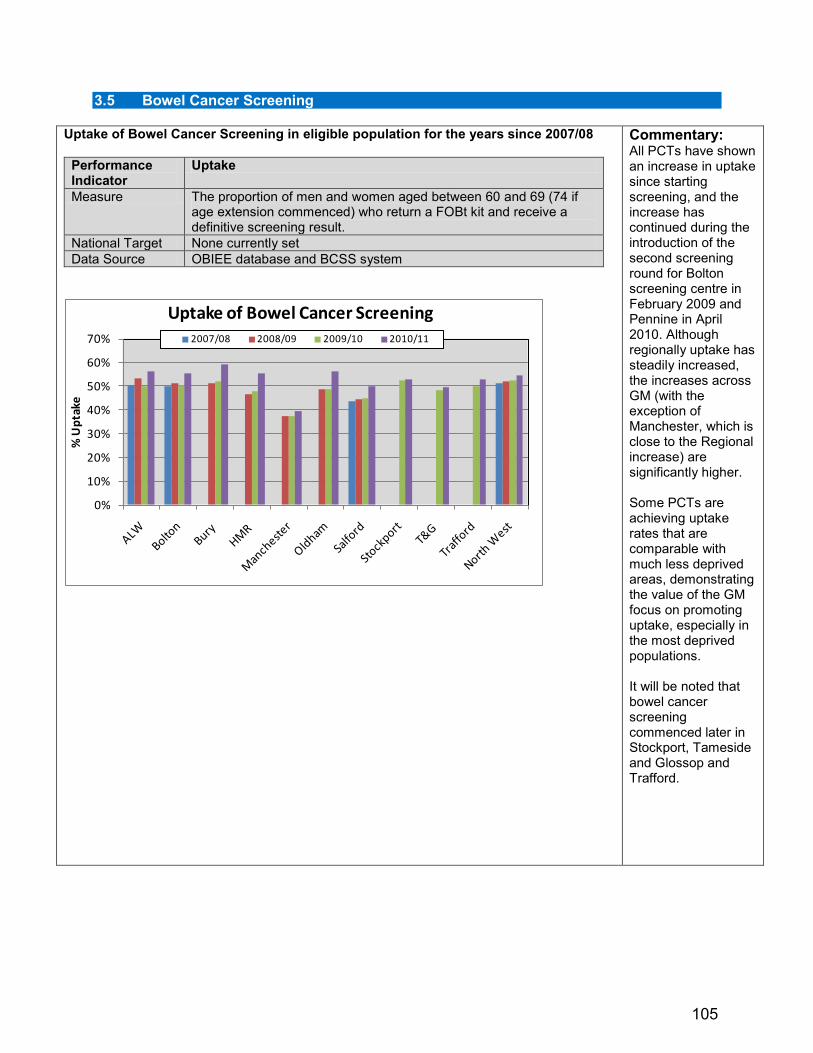
3.5 Bowel Cancer Screening
Uptake of Bowel Cancer Screening in eligible population for the years since 2007/08
Performance Indicator
Uptake
Measure The proportion of men and women aged between 60 and 69 (74 if age extension commenced) who return a FOBt kit and receive a definitive screening result.
National Target None currently set Data Source OBIEE database and BCSS system
0%
10%
20%
30%
40%
50%
60%
70%
% U
ptak
e
Uptake of Bowel Cancer Screening2007/08 2008/09 2009/10 2010/11
Commentary: All PCTs have shown an increase in uptake since starting screening, and the increase has continued during the introduction of the second screening round for Bolton screening centre in February 2009 and Pennine in April 2010. Although regionally uptake has steadily increased, the increases across GM (with the exception of Manchester, which is close to the Regional increase) are significantly higher. Some PCTs are achieving uptake rates that are comparable with much less deprived areas, demonstrating the value of the GM focus on promoting uptake, especially in the most deprived populations. It will be noted that bowel cancer screening commenced later in Stockport, Tameside and Glossop and Trafford.
105
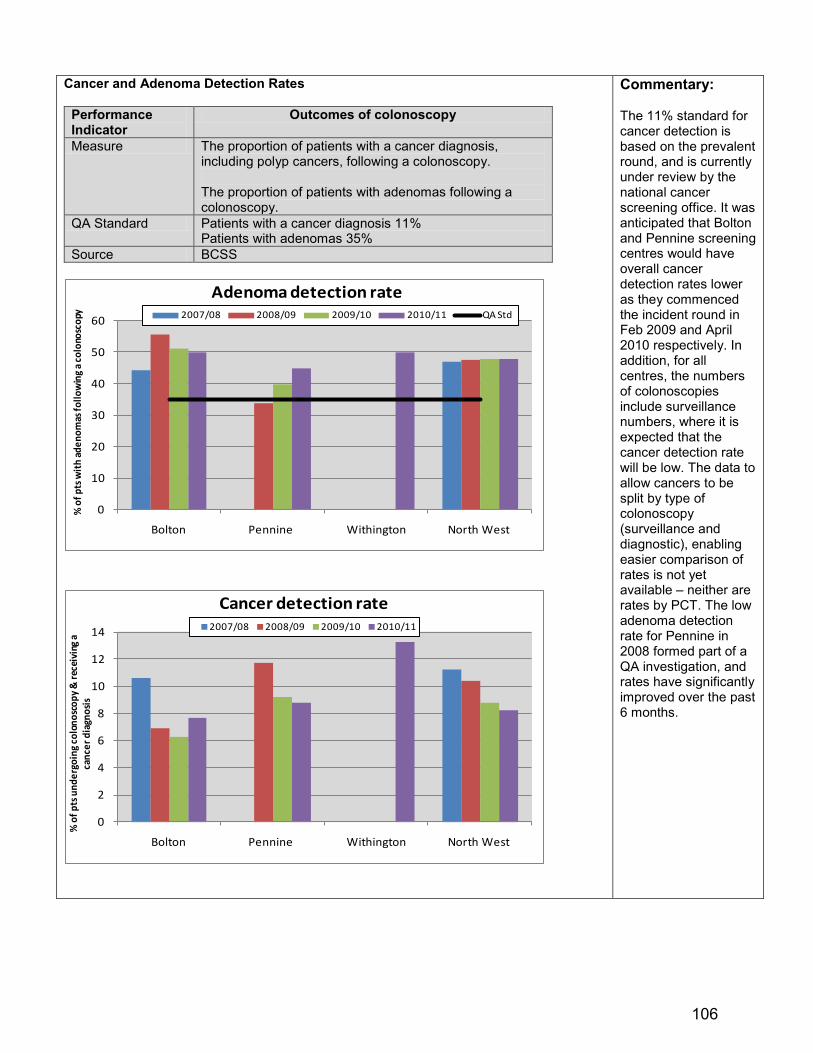
Cancer and Adenoma Detection Rates
Performance Indicator
Outcomes of colonoscopy
Measure The proportion of patients with a cancer diagnosis, including polyp cancers, following a colonoscopy. The proportion of patients with adenomas following a colonoscopy.
QA Standard Patients with a cancer diagnosis 11% Patients with adenomas 35%
Source BCSS
0
10
20
30
40
50
60
Bolton Pennine Withington North West
% o
f pts
wit
h ad
enom
as fo
llow
ing
a co
lono
scop
y
Adenoma detection rate 2007/08 2008/09 2009/10 2010/11 QA Std
0
2
4
6
8
10
12
14
Bolton Pennine Withington North West
% o
f pts
und
ergo
ing
colo
nosc
opy
& re
ceiv
ing
a ca
ncer
dia
gnos
is
Cancer detection rate 2007/08 2008/09 2009/10 2010/11
Commentary: The 11% standard for cancer detection is based on the prevalent round, and is currently under review by the national cancer screening office. It was anticipated that Bolton and Pennine screening centres would have overall cancer detection rates lower as they commenced the incident round in Feb 2009 and April 2010 respectively. In addition, for all centres, the numbers of colonoscopies include surveillance numbers, where it is expected that the cancer detection rate will be low. The data to allow cancers to be split by type of colonoscopy (surveillance and diagnostic), enabling easier comparison of rates is not yet available – neither are rates by PCT. The low adenoma detection rate for Pennine in 2008 formed part of a QA investigation, and rates have significantly improved over the past 6 months.
106

Waiting Times for SSP and First colonoscopy
% of SSP appointments within 14 days % of colonoscopies within 14 days
10/11 Qtr 2
10/11 Qtr 3
10/11 Qtr 4
11/12 Qtr 1
10/11 Qtr 2
10/11 Qtr 3
10/11 Qtr 4
11/12 Qtr 1
Bolton 100 98.8 100 100 100 97.1 95.9 62.3 Pennine 100 100 100 100 98.7 96.2 98.6 90.9 Withington 94.18 88.31 100 100 54.9 38.0 99.2 94.9
Performance Indicator
Waiting times
Measure The time from the date of booking an SSP appointment to first offered SSP appointment The time from attending an SSP appointment to first offered colonoscopy appointment
QA Standard Abnormal result to SPP 14 days SSP to colonoscopy 14 days
Source OBIEE
Commentary: There have been colonoscopy capacity issues at Withington screening centre, due to staff shortages and a high number of abnormal screening results in Oct and November 2010. Waiting times improved in January, and there are now four fixed colonoscopy lists per week, enabling targets to be more easily achieved. Bolton is struggling at present to cope with meeting waiting times for colonoscopy within 14 days. This is due to a combination of lack of accredited colonoscopists (one of their team has been involved in a serious accident) and issues around mixed sex accommodation. An action plan has been developed and its impact is being assessed currently.
3.5.1 Actions for Improvement
The GM Bowel Cancer Screening Programme is co-ordinated on behalf of NHS Greater Manchester by Bolton PCT. NHS Greater Manchester board should note the following:
3.5.2 Quality Assurance: Bolton screening centre had a formal QA visit in December 2010.
There were no major concerns highlighted, with the main recommendation being to ensure increased capacity to accommodate age extension. Both Withington and Pennine will have formal QA visits in 2012, although a preliminary QA visit took place at Withington in June 2011.
3.5.3 Future Challenges and Initiatives: The Cancer Reform Strategy (2007) and the
subsequent NHS Operating Framework 2009-10 outlined the age extension of bowel screening to include 70-74 year olds over a four year period. Bolton screening centre started age extension in October 2010, Pennine are waiting for QA and National Office sign off, and Withington will be eligible for age extension from December 2011. Due to issues around waiting times for symptomatic endoscopy services, both screening centres are not likely to begin age extension until early 2012.
3.5.4 Improving Outcomes: A strategy for Cancer (2011) confirms the intention to introduce
flexible sigmoidoscopy screening for men and women aged 55. This will be a phased roll out, and further guidance will be issued by the National Cancer Screening Office later in the year.
107
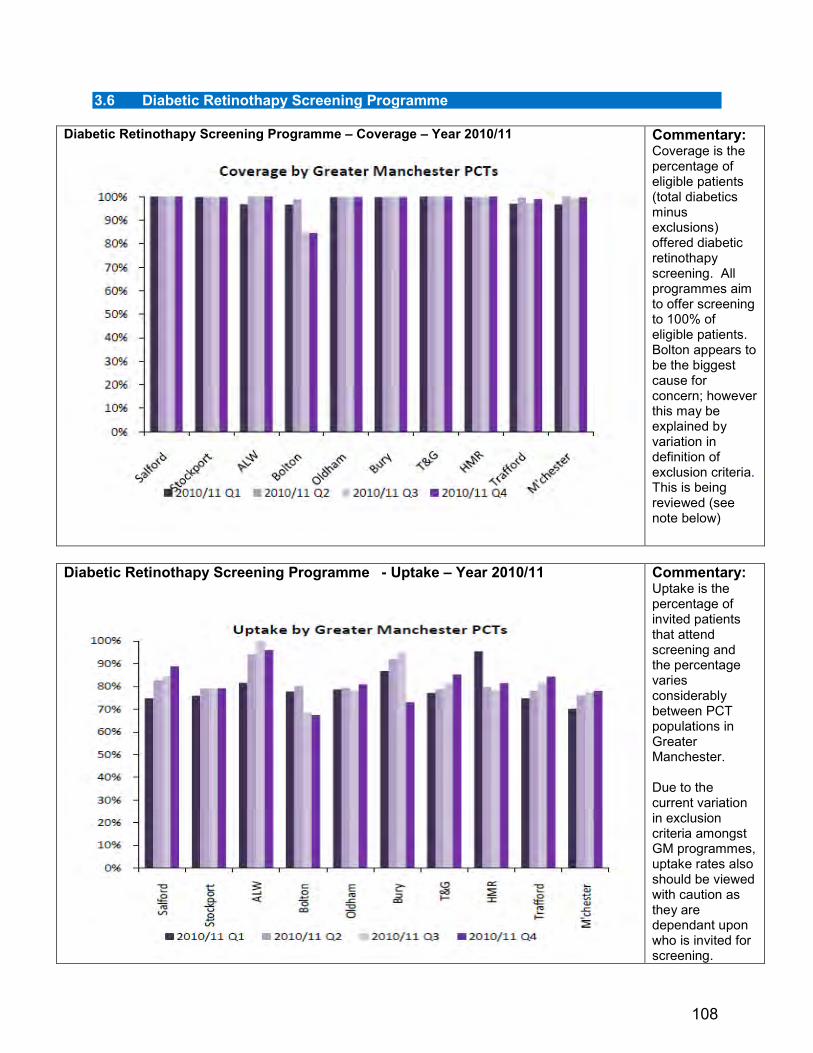
3.6 Diabetic Retinothapy Screening Programme
Diabetic Retinothapy Screening Programme – Coverage – Year 2010/11
Commentary: Coverage is the percentage of eligible patients (total diabetics minus exclusions) offered diabetic retinothapy screening. All programmes aim to offer screening to 100% of eligible patients. Bolton appears to be the biggest cause for concern; however this may be explained by variation in definition of exclusion criteria. This is being reviewed (see note below)
Diabetic Retinothapy Screening Programme - Uptake – Year 2010/11
Commentary: Uptake is the percentage of invited patients that attend screening and the percentage varies considerably between PCT populations in Greater Manchester. Due to the current variation in exclusion criteria amongst GM programmes, uptake rates also should be viewed with caution as they are dependant upon who is invited for screening.
108

3.6.1 Actions for Improvement 3.6.2 The GM Directors of Public Health Group at their October 2012 meeting received a
mapping exercise of the 4 Diabetic Retinothapy Screening Programmes in GM each of which operate on different models with governance in individual sectors. It has been recognized that comparative data would be beneficial across the DRSP programmes in GM. The population eligible for screening has increased since the introduction of the programme and is expected to go on increasing in coming years. Locally individual programmes are addressing challenges specific to their population; these are similar to all programmes. However comparisons across the programmes cannot be made with assurance and reliability of the data is questionable due to different measures being used for the indicators. This has consequences for individuals who are accessing the programmes and causes inequity of service provision across GM which has a direct impact on reported uptake and coverage of the service. Nationally there is a fitness for purpose review of the programme in progress with plans for a single service specification and single pathway underway and anticipated before the end of the year.
3.6.3 The GM Directors of Public Health Group agreed to a stepped process for change by
initially maintaining the four programmes with added GM collaboration & oversight but with the view that this should be a step along the path to a single combined managed programme for GM. This would both strengthen assurance, potentially generate cost savings by economies of scale and at the very least ensure the programme is robust enough within current costs to meet an increasing population cohort
3.7 Abdominal Aortic Aneurysm Programme 3.7.1 The NHS Abdominal aortic aneurysm screening programme aims to reduce deaths from
abdominal aortic aneurysms through early detection. Men in the year of their 65th birthday are offered an ultrasound screen.
ALW Bolton Bury CEC HMR Mancheste Oldham Salford Stockport T&G Trafford Total0 0 0 1388 0 589 0 0 1599 1365 1152 6093
attendance 1043 360 1248 1005 838 4494% 75.1 61.1 78.0 73.6 72.7 73.8requires appt 0 0 0 0 0 0% 0.0 0.0 0.0 0.0 0.0 0.0appt booked/planned 3 1 0 2 2 8% 0.2 0.2 0.0 0.1 0.2 0.1inactive - missed appts 182 146 187 181 163 859% 13.1 24.8 11.7 13.3 14.1 14.1
in-active - screen clear 1030 347 1229 983 825 4414% 98.8 96.4 98.5 97.8 98.4 98.2active - surveillance 13 12 18 20 13 76% 1.2 3.3 1.4 2.0 1.6 1.7referred 0 1 1 2 0 4% 0.0 0.3 0.1 0.2 0.0 0.1total number of AAA found 13 13 19 22 13 80% 1.2 3.6 1.5 2.2 1.6 1.8
ALW Bolton Bury CEC HMR Mancheste Oldham Salford Stockport T&G Trafford Total1748 1292 968 1238 984 1713 1169 1071 1508 1223 1078 13992
attendance 203 921 297 570 112 404 789 268 958 858 790 6170% 11.6 71.3 30.7 46.0 11.4 23.6 67.5 25.0 63.5 70.2 73.3 44.1requires appt 1119 0 304 213 614 886 2 577 119 0 2 3836% 64.0 0.0 31.4 17.2 62.4 51.7 0.2 53.9 7.9 0.0 0.2 27.4appt booked/planned 319 18 252 324 195 194 78 110 108 12 6 1616% 18.2 1.4 26.0 26.2 19.8 11.3 6.7 10.3 7.2 1.0 0.6 11.5inactive - missed appts 37 190 26 42 21 92 150 39 153 192 154 1096% 2.1 14.7 2.7 3.4 2.1 5.4 12.8 3.6 10.1 15.7 14.3 7.8
in-active - screen clear 198 899 289 554 107 387 764 262 933 838 764 5995% 97.5 97.6 97.3 97.2 95.5 95.8 96.8 97.8 97.4 97.7 96.7 97.2active - surveillance 3 20 7 15 4 16 23 5 24 20 22 159% 1.5 2.2 2.4 2.6 3.6 4.0 2.9 1.9 2.5 2.3 2.8 2.6referred 2 2 1 1 1 1 2 1 1 0 4 16% 1.0 0.2 0.3 0.2 0.9 0.2 0.3 0.4 0.1 0.0 0.5 0.3total number of AAA found 5 22 8 16 5 17 25 6 25 20 26 175% 2.5 2.4 2.7 2.8 4.5 4.2 3.2 2.2 2.6 2.3 3.3 2.8
Early Implementation Group
Screening Year 01.04.2009 - 31.03.2010, data correct as of 14.06.2011
All GM PCTS & part CEC PCT
Screening Year 01.04.2010 - 31.03.2011, data correct as of 14.06.2011
Outcome
Outcome
109

3.7.2 Actions for Improvement The GM AAA screening programme was reviewed by the GM Commissioning Programme Board in September 2011. The Board “noted that the GM AAASP has been successfully rolled out to all GM PCTs. The uptake of screening in the completed cohort in the South Sector of GM is 73%. This is very positive and was achieved without proactive promotion of the service. Current uptake in the roll out PCTs is 44%, however this cohort is only partially completed and increases in attendance/uptake are expected. The detection rate of aneurysms is currently 2.8%; this is in line with national figures. The Board also noted the positive national feedback for the GM programme. The National Screening Committee has described GM AAA screening Programme as a model of best practice and the Public Health Network has been requested to support other regions to replicate the model. The Board was satisfied that the review data on uptake, detection, patient experience and outcomes indicated supported continuation of the programme as recommended by DPHs. The Board confirmed its ongoing support for the GM AAA Screening Programme until the anticipated transfer of screening responsibilities to Public Health England in 2013”.
3.7.3 The GMAAASP will be transferred from NHS Bury to a new provider by April 2012. A GM AA Screening Procurement Project Steering Group has been formed & is leading this work.
Jan Hutchinson Lead Greater Manchester Director of Public Health
110

Appendix 1
All Age All Cause Mortality - Progress by PCT The chart uses the monthly provisional deaths counts for local areas, published by ONS. (Cross-checking these provisional counts of local deaths with the subsequent definitive deaths extract shows that they rarely differ by more than one or two over a 12 month period). For the purposes of the chart, the most recent twelve months’ deaths have been aggregated for each locality. Male and female deaths are not distinguished in the published data. Care should be taken in interpreting performance within the confidence intervals indicated.
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for ALW PCT. Source: NHS North West
Ashton, Wigan and Leigh PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: ALW has been off trajectory for some time but progress is being made at pace particularly for males. Action is being taken via the Health and Wellbeing Board and CCG, including the ‘Find and Treat’ CVD risk assessment programme expansion, inclusion of relevant CQUIN targets in acute and community contracts and a wide ranging programme of capacity building for public health across all frontline staff in key agencies “Make Every Contact Count” and in the community (over 900 Community Health advocates).Participation in the DH Healthy Living Pharmacy programme to increase the role of pharmacists in disease risk management. Wigan has one of the highest smoking quit rates in the NW and the alcohol active case management programme in A+E is starting to make significant progress in reducing repeat admissions and attendances for chronic alcohol harm.
111
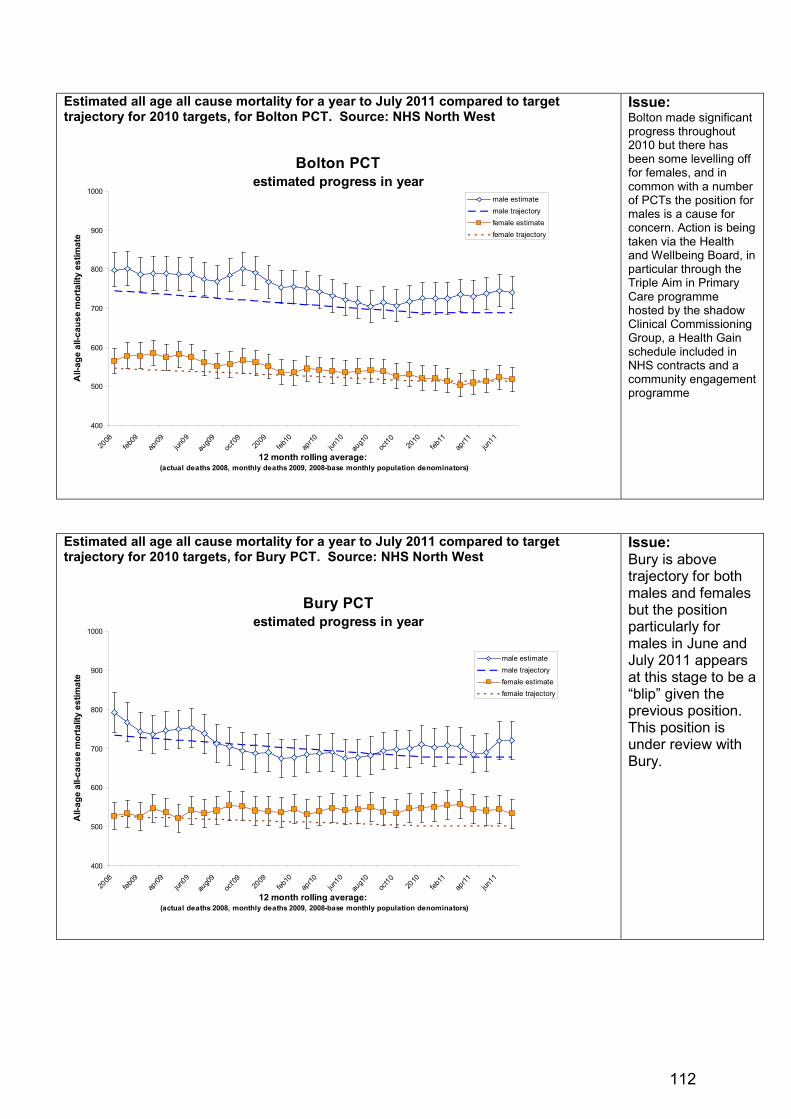
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Bolton PCT. Source: NHS North West
Bolton PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: Bolton made significant progress throughout 2010 but there has been some levelling off for females, and in common with a number of PCTs the position for males is a cause for concern. Action is being taken via the Health and Wellbeing Board, in particular through the Triple Aim in Primary Care programme hosted by the shadow Clinical Commissioning Group, a Health Gain schedule included in NHS contracts and a community engagement programme
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Bury PCT. Source: NHS North West
Bury PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: Bury is above trajectory for both males and females but the position particularly for males in June and July 2011 appears at this stage to be a “blip” given the previous position. This position is under review with Bury.
112
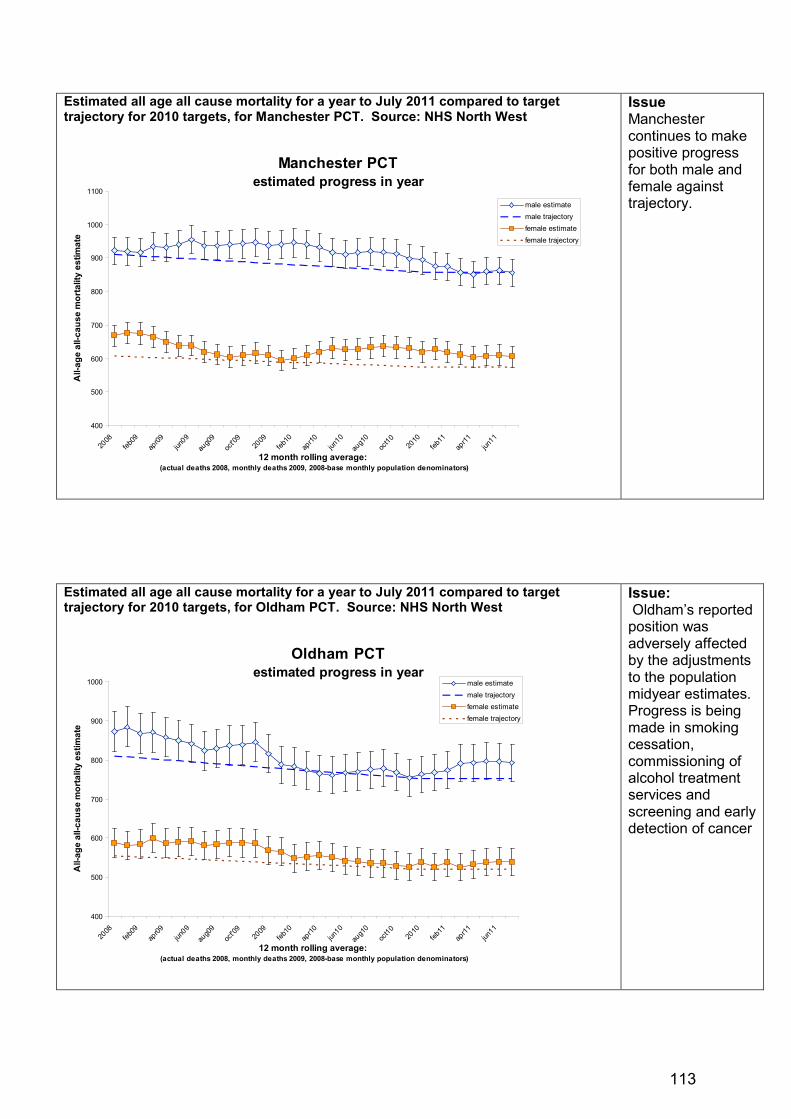
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Manchester PCT. Source: NHS North West
Manchester PCTestimated progress in year
400
500
600
700
800
900
1000
1100
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue Manchester continues to make positive progress for both male and female against trajectory.
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Oldham PCT. Source: NHS North West
Oldham PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: Oldham’s reported position was adversely affected by the adjustments to the population midyear estimates. Progress is being made in smoking cessation, commissioning of alcohol treatment services and screening and early detection of cancer
113

Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for HMR PCT. Source: NHS North West
Heywood, Middleton and Rochdale PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09 jun
09au
g09
oct'0
920
09feb
10ap
r10 jun10
aug1
0oc
t10 2010
feb11
apr11 jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue HMR continue to make good progress particularly for females and are the third best GM PCT in terms of distance for target for consolidated position for males and females. The relative plateau for males is of concern and HMR have identified male AAACM as at risk and have developed a recovery plan. .
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Salford PCT. Source: NHS North West
Salford PCTestimated progress in year
400
500
600
700
800
900
1000
1100
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: Salford continues to make good progress for both genders.
114

Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Stockport PCT. Source: NHS North West
Stockport PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e male estimatemale trajectoryfemale estimatefemale trajectory
Issue Stockport continues to outperform the trajectory for both genders and makes a relatively large contribution to the overall GM position.
Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Tameside and Glossop PCT. Source: NHS North West
Tameside and Glossop PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09
jun09
aug0
9oc
t'09
2009
feb10
apr10
jun10
aug1
0oc
t1020
10feb
11ap
r11jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: Tameside position is beginning to show cause for concern However, the Health &Wellbeing Board and CCG have both agreed that action on CVD continues as a priority – leading cause of the gap. The NST approach will be more firmly embedded in relation to action on tobacco and alcohol plus a specific focus on primary care quality for CVD.
115

Estimated all age all cause mortality for a year to July 2011 compared to target trajectory for 2010 targets, for Trafford PCT. Source: NHS North West
Trafford PCTestimated progress in year
400
500
600
700
800
900
1000
2008
feb09
apr09 jun
09au
g09
oct'0
920
09feb
10ap
r10 jun10
aug1
0oc
t10 2010
feb11
apr11 jun
11
12 month rolling average: (actual deaths 2008, monthly deaths 2009, 2008-base monthly population denominators)
All-
age
all-c
ause
mor
talit
y es
timat
e
male estimatemale trajectoryfemale estimatefemale trajectory
Issue: The Trafford position has been mostly positive but the trend for females is beginning to show some cause for concern. Action is being taken via the Health and Wellbeing Board and shadow CCG
116

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 11 10 November 2011 REPORT OF:
Jan Hutchinson Lead GM Director of Public Health
DATE OF PAPER:
19 October 2011
SUBJECT:
Re-emergence of a Public Health Issue - TB
IN CASE OF QUERY, PLEASE CONTACT
Debra Malone Consultant in Public Health, NHS Bolton [email protected]
PURPOSE OF PAPER: To raise awareness of the increased incidence of TB in adults and children in Greater Manchester. To update NHS Greater Manchester Board members on plans to tackle the increased incidence of TB across Greater Manchester and the North West. To highlight key challenges to reducing TB incidence and prevalence, particularly in children. NHS Greater Manchester Board is asked to approve recommendations relating to the development of a work stream and delivery plan to reduce TB transmission in children. The Board is also asked to support the recommendation that dedicated commissioning/contracting support is made available to the GM TB Commissioning Plan Implementation Group and the GM Paediatric TB Task Group.
117

Re-emergence of a Public Health Issue - TB Executive Summary TB (tuberculosis), which was once thought to have been eradicated in the UK, has now re-emerged following its lowest recorded prevalence in 1987. Over the past 20 years there has been a gradual increase in the number of cases in the UK, with approximately 9,000 cases of TB being notified each year. In 2009 the largest numbers of TB notifications were in London residents with the West Midlands and the North West reporting the second and third greatest incidences respectively. In 2009 there were 816 cases of TB in the North West, which was a 10% rise from the preceding year. Greater Manchester currently has the highest annual TB incidence in the North West. Across GM there are large differences in incidence with the city of Manchester recording the highest rates and Ashton, Leigh and Wigan recording the lowest. In response to the increasing incidence of overall TB a GM TB Commissioning Plan was developed in 2010 and is currently being implemented. Most recently, however, further concerns have been raised relating to the increasing incidence of paediatric TB across GM with Manchester again, recording the largest increase in incidence. The incidence of paediatric TB is inextricably linked to the prevalence of adult TB, particularly undiagnosed, multi drug resistant or latent disease. Therefore it is imperative that additional work is carried out to ensure a co-ordinated approach is developed to tackling the overall increasing incidence of TB across GM. This paper offers an overview of progress to date in relation to the implementation of the GM Commissioning Plan but also highlights some of the challenges facing health care professionals and commissioners in terms of responding to the issue as effectively as possible. 1 Introduction 1.1 TB, which was once thought to have been eradicated in the UK, has now re-emerged following its
lowest recorded prevalence in 1987. Over the past 20 years there has been a gradual increase in the number of cases in the UK, with approximately 9,000 cases of TB being notified each year. In 2009 the largest numbers of TB notifications were for London residents with the West Midlands and the North West reporting the second and third greatest incidences respectively.
1.2 In 2009 there were 816 cases of TB in the North West, which was a 10% rise from the preceding
year. At that time there were 536 confirmed cases of TB in Greater Manchester; two-thirds of the North West total. Across GM there are large differences in incidence with the city of Manchester recording the highest rates (up to 40 cases per 100,000 population) and Ashton Leigh and Wigan recording the lowest rates (less than 5 cases per 100,000 population).
1.3 Nationally, the highest incidence rates of TB are found in people from South Asia and Sub
Saharan Africa. This is true for the North West as a whole and for Greater Manchester the largest increase in TB diagnoses has most recently been observed in Black African and South Asian
118

communities in that order. Nevertheless, across the North West, 20% of TB diagnoses are also found in the white population indicating that it is a disease that crosses the broad spectrum of ethnicity.
2 Background 2.1 There has been an increase in the incidence and prevalence of adult and paediatric cases of TB
across GM and the North West over the past 10 years. NHS Manchester records the highest incidence rates but TB rates for NHS HMR, NHS Bolton and NHS Oldham are also relatively high. Consequently the burden on the NHS across GM in relation to TB treatment and care is also increasing. This is particularly significant for paediatric specialist services as these services often treat children from across the North West. The specialist nature of TB treatment and care, particularly for individuals with Multi Drug Resistant TB, means that increasing rates of the disease pose major challenges to public health and to health care services.
2.2 This paper notes that currently, there are two separate but related work streams focusing on
reducing TB incidence across GM. The first work stream relates to the implementation of the GM TB Commissioning Plan which was approved by the GM Commissioning Programme Board in May 2010 with the aim of reducing the overall incidence and prevalence of TB. The most substantial piece of work within this work stream has been the development of an adult TB service specification to be implemented by all GM Acute Hospital Trusts in 2012/13. The service specification addresses the issue of TB nursing capacity and contains Key Performance Indicators that will result in improved skill mix and more formalised cross boundary working. The specification will reinforce the need for a cohesive approach to Continuing Professional Development for TB nurses, which has recently been kick-started via the development of the GM TB Nurse Network which over the next year will be linked to the establishment of a TB Cohort Review process for GM.
2.3 The second work stream is relatively new and focuses on TB in children but is inextricably linked
to the implementation of the GM TB Commissioning Plan. A Paediatric TB Task Group has been established to specifically act on data indicating an increased incidence of TB in children and to review BCG uptake rates in eligible children. The Task Group will report to the GM TB Commissioning Plan Implementation Group. From November 2011, both Groups will be chaired by Alan Higgins who has recently become the lead GM DPH for TB.
2.4 To date there has only been one meeting of the Paediatric TB Task Group and currently there is
no delivery plan in place. However it is expected that the Group will:
• verify data relating to the current uptake of BCG vaccination • make recommendations relating to the development of improved care pathways and methods
of delivery of BCG vaccination • ensure that the data relating to the increased incidence of paediatric TB is fully understood
and shared appropriately to inform service re-design • review the impact on the Manchester based paediatric TB services as a result of the
increasing number of cases of TB in children from across the North West as a whole • make recommendations relating to the most effective models of delivery of paediatric TB
services across the North West in the future • develop new service specification(s) for new models of paediatric TB services across the
North West. 2.5 It is possible that as a result of service re-design there may be a need for additional investment to
facilitate the effective delivery of paediatric TB services across the North West but especially in Manchester.
119

3 Overview of Greater Manchester TB Commissioning Plan 3.1 Following the approval of the GM TB Commissioning Plan by the Greater Manchester
Commissioning Programme Board, NHS Bolton was identified as lead commissioner and the multi-disciplinary, multi-agency, GM TB Commissioning Plan Implementation Group was established. The Group predominantly comprises clinicians and there has been no dedicated commissioning input to the Group for some months now.
3.2 The aim of the Commissioning Plan is to drive up the quality of TB treatment services across the
conurbation, increase awareness, improve equity in terms of access to services and, ultimately to reduce TB prevalence. There are several strands to the work programme, which seeks to:
• develop standard service specifications, protocols and quality indicators. • establish a GM TB Nurse Network to facilitate the sharing of good practice. • establish new referral and care pathways between the TB workforce, healthcare professionals
and third sector organisations in contact with those most at risk of TB. • support the local implementation of TB Alert’s “The Truth About TB” campaign by developing
resources that are specifically targeted towards third sector organisations working with Black African communities.
• develop a GM wide TB incident and outbreak plan and develop and deliver TB education and awareness initiatives.
• improve service user engagement and involvement. • develop a GM wide TB population prevention and awareness plan to include the
implementation of NICE guidance relating to the (BCG) immunisation of targeted neonates prior to hospital discharge.
4 Current Position GM TB Commissioning Plan and New Adult Service Specification 4.1 As a result of excellent partnership working across the TB workforce, good progress has been
made against all of the elements of the GM TB Commissioning Plan outlined above.
4.2 During 2011 the GM TB Commissioning Plan Implementation Group’s main focus has been on developing the new service specification for adult TB services across Greater Manchester. A final draft document was submitted to the Greater Manchester Contracting and Finance Sub-Group by Bolton’s Senior Contracts Manager in July 2011. However, further work is required to clarify inpatient, outpatient and community based activity in order to establish baselines and inform contract values. The intention is for each one of GM PCT’s commissioning teams to take this specification forward with their respective hospital trusts well in advance of the new financial year.
4.3 The GM Contracting and Finance Sub-group have asked the GM TB Commissioning Plan Implementation Group to attempt to establish activity baselines. This is proving difficult as the Group does not have any dedicated commissioning/contracting support and providers have been reluctant to participate in a data trawl in this respect. Consequently progress in terms of finalising the specification has been hampered. There is concern within the GM TB Commissioning Plan Implementation Group that there needs to be stronger support from locality commissioning and contracting teams to champion the service specification within each PCT and to ensure that it is firmly embedded in contracts for 2012/13. The nomination of a GM commissioning/contracting lead for TB would assist in driving this issue forward with locality colleagues. There will be a need for liaison with commissioning colleagues in Lancashire as patient flows, especially for paediatrics, tends to be from Lancashire into Manchester.
120

5 TB in Children 5.1 The existing GM TB Commissioning Plan does not specifically refer to paediatric TB services
because when the Plan was written the available epidemiological data was not suggestive of a significant trend in the increase of TB in children. Now, however, the epidemiological data very clearly indicates that, since 2004, TB rates amongst children in GM have risen substantially (Fig.1); a trend which has not been reported anywhere else in the country. In 2009 there were 42 cases of TB in children in GM and, of these, 66% were born in the UK.
Fig. 1 Trends in TB incidence in children aged 0 - 14
0.0
2.0
4.0
6.0
8.0
10.0
2002 2003 2004 2005 2006 2007 2008 2009
Cru
de T
B i
ncid
ence
rat
e pe
r 10
0,00
0 po
pula
tion
Year
Trend in TB Incidence for those aged 0-14 years - North West
Cheshire & Merseyside Cumbria & Lancashire Greater Manchester North West Region
Source: ETS, HPA & ONS 5.2 TB incidence and prevalence in children is a matter for concern as it is indicates that recent
transmission has taken place and is suggestive of a lack of effectiveness in relation to prevention and control interventions. Children have a higher risk of morbidity and mortality from TB than adults and the literature suggests that between 40-60% of children hospitalised with TB could have been diagnosed earlier.
5.3 There is clearly a great deal of work to be carried out to tackle the rise in paediatric TB in GM. It
should also be noted that due to cross boundary flows Paediatric TB is not just an issue for GM but for the North West as whole. Depending on their place of residence children living in the North West are known to access services provided by a number of hospitals across the area. Whilst the majority of children are cared for, at least initially, by Central Manchester NHS Foundation Trust, the increasing incidence of paediatric TB is also likely to impact on other North West hospitals. This is likely to add additional layers of complexity in terms of paediatric TB service re-design.
121
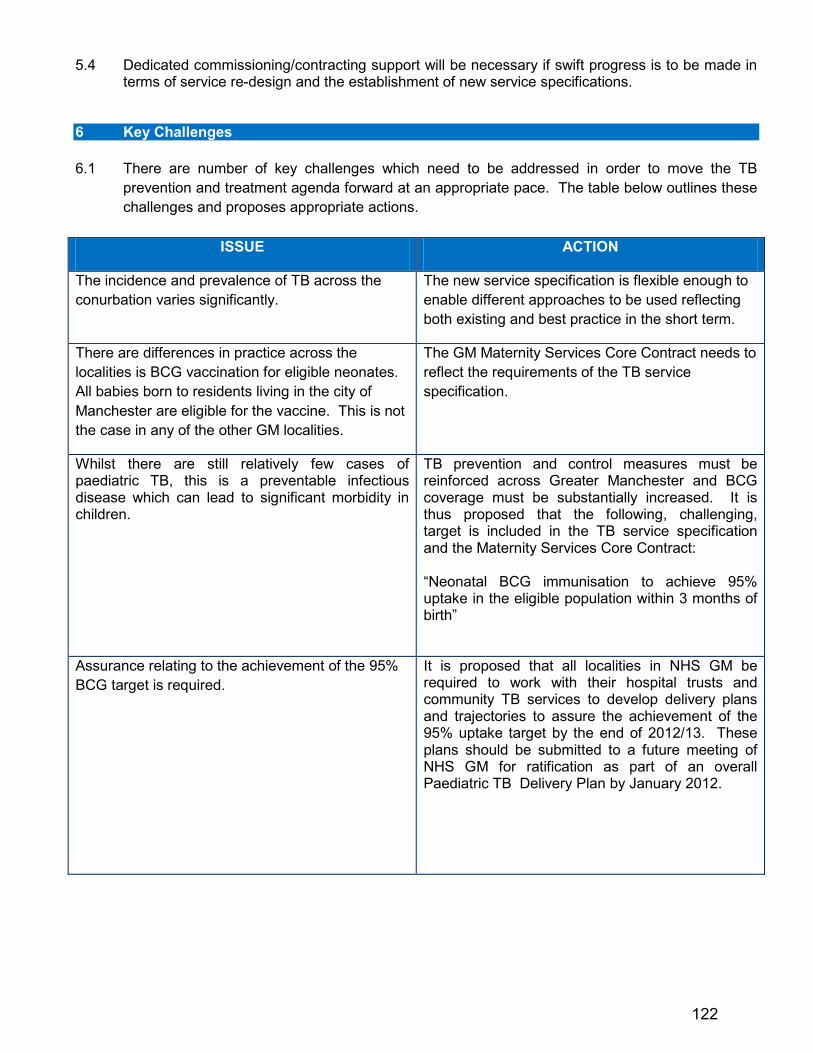
5.4 Dedicated commissioning/contracting support will be necessary if swift progress is to be made in terms of service re-design and the establishment of new service specifications.
6 Key Challenges 6.1 There are number of key challenges which need to be addressed in order to move the TB
prevention and treatment agenda forward at an appropriate pace. The table below outlines these challenges and proposes appropriate actions.
ISSUE ACTION
The incidence and prevalence of TB across the conurbation varies significantly.
The new service specification is flexible enough to enable different approaches to be used reflecting both existing and best practice in the short term.
There are differences in practice across the localities is BCG vaccination for eligible neonates. All babies born to residents living in the city of Manchester are eligible for the vaccine. This is not the case in any of the other GM localities.
The GM Maternity Services Core Contract needs to reflect the requirements of the TB service specification.
Whilst there are still relatively few cases of paediatric TB, this is a preventable infectious disease which can lead to significant morbidity in children.
TB prevention and control measures must be reinforced across Greater Manchester and BCG coverage must be substantially increased. It is thus proposed that the following, challenging, target is included in the TB service specification and the Maternity Services Core Contract: “Neonatal BCG immunisation to achieve 95% uptake in the eligible population within 3 months of birth”
Assurance relating to the achievement of the 95% BCG target is required.
It is proposed that all localities in NHS GM be required to work with their hospital trusts and community TB services to develop delivery plans and trajectories to assure the achievement of the 95% uptake target by the end of 2012/13. These plans should be submitted to a future meeting of NHS GM for ratification as part of an overall Paediatric TB Delivery Plan by January 2012.
122

ISSUE ACTION
The early diagnosis of TB, particularly in children, can be difficult. Central Manchester Foundation NHS Trust currently provides this service to children predominantly from GM but also from across the North West. This is an historical arrangement and commissioning processes are not in place to assess the appropriateness and impact of the existing arrangements.
The Paediatric Task Group will need to explore ways of establishing an improved model of clinical care for children with TB across the North West. It is proposed that this piece of work is scoped out by the end of 2011 and included in a Paediatric TB Delivery Plan.
The Paediatric TB work stream is new and a great deal of effort is required to effect necessary changes. In addition there is a need to ensure that the new service specification is rigorously implemented across GM.
The nomination of a dedicated GM TB commissioning/contracting lead is required to facilitate support for the implementation and delivery of the new TB service specification across all 10 GM localities.
7 Recommendations 7.1 The NHS Greater Manchester Board is asked to approve: 7.1.1 The inclusion of the 95% uptake target for neonatal BCG in both the new TB service specification
and the GM Maternity Services Contract. 7.1.2 The proposal for NHS GM to assure the delivery of 95% BCG coverage for eligible neonates in
conjunction with appropriate health care providers by the end of 2012/13, through the development of delivery plans, milestones and trajectories.
7.1.3 The proposal that the Paediatric TB Task Group be asked to produce a comprehensive Paediatric
TB Delivery Plan to be submitted to a future meeting of NHS GM for ratification by January 2012 and, where appropriate, implement key actions with immediate effect.
7.1.4 The nomination of a dedicated GM TB commissioning/contracting lead to facilitate support for the
implementation and delivery of the new TB service specification across all 10 GM localities and influence the effective re-design of Paediatric TB services across the North West.
Jan Hutchinson Lead GM Director of Public Health
123

124
REPORT OF: Director of FinanceDATE OF PAPER: 24 October 2011SUBJECT: Finance Report for the six months
ended 30 September 2011IN CASE OF QUERY, PLEASE CONTACT
Mrs Claire Yarwood0161 212 4835
PURPOSE OF PAPER:This paper provides an update to the Cluster Board on the financial position for the ten Greater Manchester PCTs for the first six months of 2011-12.
NHS GREATER MANCHESTER BOARD MEETINGAGENDA ITEM 12
10 November 2011
125

Contents
1. Key Financial Performance Dashboard
2. Summary Financial Position
3. Risks
4. QIPP Performance
5. PCT Performance Exception Report
6. 2% Recurrent Headroom
7. Contract Performance Report
8. Running Costs Analysis
9. Capital Investment Programme
10. Recommendations
126

1 Key Financial Performance Dashboard
Review Commentary Year to Date Rating
Year End Rating
RevenuePCTs are forecasting achievement of the planned surpluses for 2011-12 although this is dependent on the achievement of significant levels of QIPP savings. NHS Bolton and NHS Oldham are reporting year to date positiions which are behind plan.
CapitalTo date there has been minimal spend of £2,578k against a total net capital resource limit of £13,753k. Whilst plans are profiled towards the second half of the year, there is an underspend against the plan to date of approximately £3m.
CashPCTs are largely drawing down cash in accordance with their plans, with the exception of NHS Oldham (0.02% ahead of plan). No PCTs are currently indicating a requirement for cash in excess of their allocation.
Provider Breakeven
NHS Stockport is the only PCT with a provider arm. NHS Stockport has reported a year to date surplus of £589k due to lower than planned pay costs and procurement savings. NHS Stockport is forecasting a breakeven position for the year and is planning to transfer provider services to an Acute Trust on or after 1 April 2012.
127
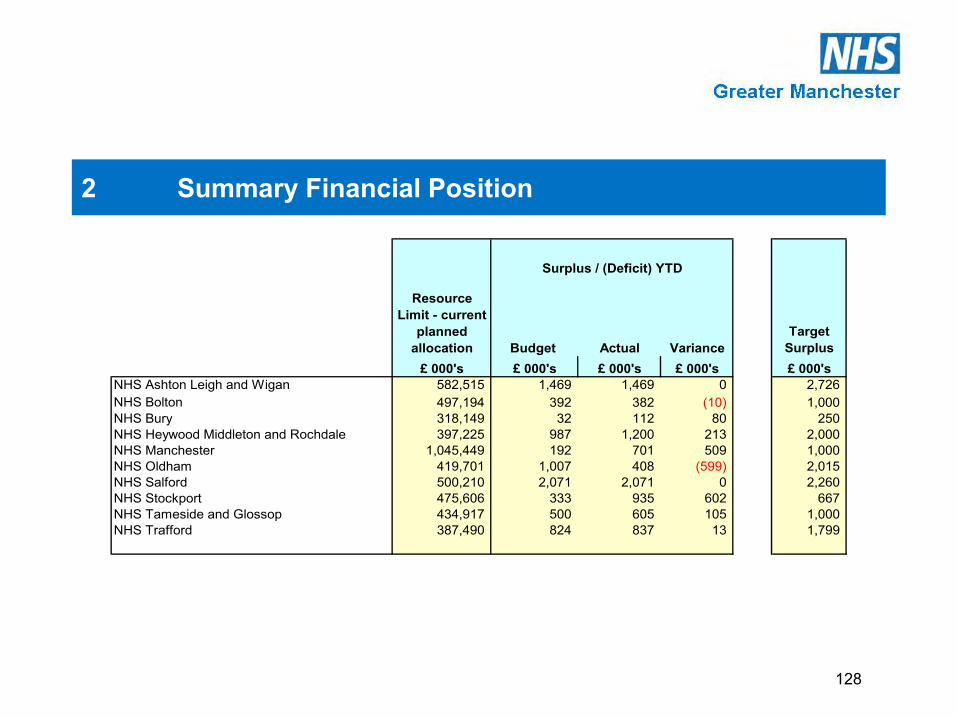
2 Summary Financial Position
Budget Actual VarianceTarget
Surplus£ 000's £ 000's £ 000's £ 000's £ 000's
NHS Ashton Leigh and Wigan 582,515 1,469 1,469 0 2,726NHS Bolton 497,194 392 382 (10) 1,000NHS Bury 318,149 32 112 80 250NHS Heywood Middleton and Rochdale 397,225 987 1,200 213 2,000NHS Manchester 1,045,449 192 701 509 1,000NHS Oldham 419,701 1,007 408 (599) 2,015NHS Salford 500,210 2,071 2,071 0 2,260NHS Stockport 475,606 333 935 602 667NHS Tameside and Glossop 434,917 500 605 105 1,000NHS Trafford 387,490 824 837 13 1,799
Surplus / (Deficit) YTD
Resource Limit - current
planned allocation
128
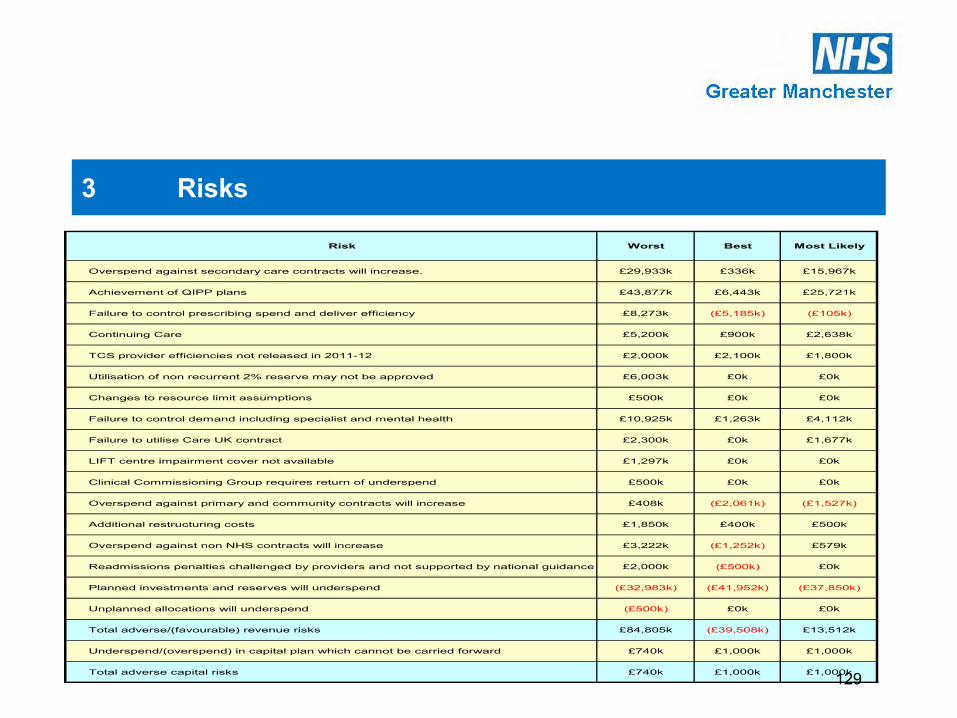
3 Risks
Risk Worst Best Most Likely
Overspend against secondary care contracts will increase. £29,933k £336k £15,967k
Achievement of QIPP plans £43,877k £6,443k £25,721k
Failure to control prescribing spend and deliver efficiency £8,273k (£5,185k) (£105k)
Continuing Care £5,200k £900k £2,638k
TCS provider efficiencies not released in 2011-12 £2,000k £2,100k £1,800k
Utilisation of non recurrent 2% reserve may not be approved £6,003k £0k £0k
Changes to resource limit assumptions £500k £0k £0k
Failure to control demand including specialist and mental health £10,925k £1,263k £4,112k
Failure to utilise Care UK contract £2,300k £0k £1,677k
LIFT centre impairment cover not available £1,297k £0k £0k
Clinical Commissioning Group requires return of underspend £500k £0k £0k
Overspend against primary and community contracts will increase £408k (£2,061k) (£1,527k)
Additional restructuring costs £1,850k £400k £500k
Overspend against non NHS contracts will increase £3,222k (£1,252k) £579k
Readmissions penalties challenged by providers and not supported by national guidance £2,000k (£500k) £0k
Planned investments and reserves will underspend (£32,983k) (£41,952k) (£37,850k)
Unplanned allocations will underspend (£500k) £0k £0k
Total adverse/(favourable) revenue risks £84,805k (£39,508k) £13,512k
Underspend/(overspend) in capital plan which cannot be carried forward £740k £1,000k £1,000k
Total adverse capital risks £740k £1,000k £1,000k129
6
3 Risks
•There are a number of financial risks that are included in the PCTs’ forecast financial position however the magnitudeand certainty of these risks is variable. The table on the previous page lists the major risks and the potential best andworst cases. Currently the most likely positions are included in the forecast outturns and are mitigated by contingencies,under spends on developments and strategic initiatives.
•Each PCT has assessed the risks applicable to their financial position and commissioned services. Whilst some risksare specific to particular PCTs, the risks relating to secondary care contracts, QIPP delivery and prescribing spend arecommon to most PCTs. It should be noted that the most likely position for prescribing has improved for a number ofPCTs, with six out of ten PCTs now predicting breakeven or an underspend for the year.
•Overall, the worst and best case positions have improved compared to those identified in the month three report. Themost likely position has improved for a number of risks – achievement of QIPP £25,721k (£28,720k at month 3),prescribing underspends £105k (£3,244k overspends at month 3) and utilisation of contingencies. The most likelyposition regarding secondary care overspend risk has deteriorated slightly but the worst case position has improved; thisis largely due to firmer forecasts based on more comprehensive information from providers.
130

4 QIPP Performance
Resource Limit ; Opening in-year
allocation QIPP PlanQIPP Plan as %
of Resource LimitQIPP plan to M6 QIPP achieved to
M6 QIPP Forecast
£ 000's £ 000's £ 000's £ 000's £ 000's NHS Ashton Leigh and Wigan 573,073 12,681 2.2 6,342 6,083 12,681 NHS Bolton 488,691 9,300 1.9 4,650 2,357 6,677 NHS Bury 316,152 25,653 8.1 12,628 9,364 25,653 NHS Heywood Middleton and Rochdale 396,762 10,939 2.8 5,076 6,288 10,939 NHS Manchester 1,032,509 23,237 2.3 6,462 9,487 24,849 NHS Oldham 422,179 18,902 4.5 7,766 3,317 12,490 NHS Salford 476,052 2,258 0.5 1,015 1,374 3,738 NHS Stockport 482,475 8,180 1.7 3,522 7,838 7,888 NHS Tameside and Glossop 429,940 10,200 2.4 3,340 7,175 10,200 NHS Trafford 379,322 16,106 4.2 5,741 7,523 15,295
Greater Manchester PCTs 4,997,155 137,456 2.8 56,542 60,806 130,410
131
4 QIPP Performance
•NHS Bolton are currently highlighting a potential under achievement against their QIPP plans of £2.6m, of which £600k is relatedto prescribing schemes and based on holding spend to 2010-11 levels, and £2m is for demand management schemes. Howeverthis is expected to improve as the programme takes effect but will be closely monitored; until there is more certainty the PCT hasforecast slippage on investments and non recurrent expenditure to ensure it delivers the target surplus.
•NHS Bury has the highest QIPP target as a percentage of revenue resource limit, at £25.6m. To month six, financial recoveryschemes have slipped by £3.27m although full delivery in year would have delivered a 1% surplus. On this basis, if this slippagecontinues to yearend an under achievement against QIPP of £6.54m will result – 50% of which represents the 1% contingencyand 50% to be supported by non-recurrent measures.
• NHS Manchester set an initial QIPP target of £20.2m and then added a further 50% to allow for slippage on schemes, optimismbias, and to provide a potential contingency for any deterioration in the underlying financial position. Detailed plans have beendrawn up by consortia leads and other budget holders to address £25m of the revised £30m target and although they are currentlyworking on proposals to achieve the balance it is unlikely that further savings will be achieved in 2011-12. The QIPP team is nowfocussing on the certainty of the delivery of existing plans; the proportion of red rated schemes has reduced from 30% at monththree to 17% at month six.
•NHS Oldham initially identified a non recurrent revenue gap of £11.9m, and added a further £7m to the target to provideadditional recurrent headroom. Evidence based savings to date indicate a forecast outturn of £12.5m in savings, of which £11.5mare recurrent. Programmes of concern are those with the largest QIPP target; urgent care (achieved £528k against forecast of£3.1m) and planned care (achieved £655k against forecast of £3.9m).
132

5 PCT Performance Exception Report• PCTs are currently forecasting achievement of the planned surpluses. These aggregate to the surplus control total agreed withthe Strategic Health Authority to achieve the planned 2% recurrent headroom target. Further detail on this target is given insection six of this report.
•At month six, two PCTs are under achieving against their planned year to date surpluses, with the main under achievement inNHS Oldham. Most PCTs have incorporated month five activity from their main provider and month four activity from the NorthWest Specialist Commissioning Team into their forecasts.
• NHS Bury is experiencing pressures in acute activity, specialist commissioning and continuing health care. However, the PCT isforecasting achievement of the target surplus on the basis that non-recurrent savings and measures will be put in place to mitigatein year slippage on savings relating to the various financial recovery schemes.
•NHS Manchester has identified forecast overspends of £5.8m, mainly within acute contracts (£1.8m), secure mental healthcontracts (£985k), and management budgets (£3m). Within the management budgets overspend, there is a pressure of £839krelated to Transforming Community Services, where a number of non recurrent costs have been agreed with the new providers.In addition, pressures are forecast for legal fees and settlements, reduced income streams and resignation/redundancy schemes.There are ongoing negotiations between NHS Manchester and Manchester City Council regarding the settlement of mental healthnon secure over performance for 2009-10, the 2010-11 mental health pool contribution and pooling resources for 2011-12.
133

5 PCT Performance Exception Report•NHS Oldham is reporting a year to date surplus behind plan and this is mainly due to slippage on QIPP schemes,pressures due to secondary care and specialist services over performance, and overspends in prescribing. The PCTcontinues to forecast achievement of the target surplus on the basis that QIPP plans will be achieved later in the year andthat contingency reserves will be utilised, although this target is becoming increasingly challenging.
•NHS Stockport is reporting a year to date surplus significantly above plan, largely as a result of lower than planned paycosts due to staff vacancies, and non pay procurement savings within the provider arm of the PCT. The forecast has beenmaintained at the target surplus of £667k as non recurrent transition and equipping costs will be funded from the providerunderspend.
134
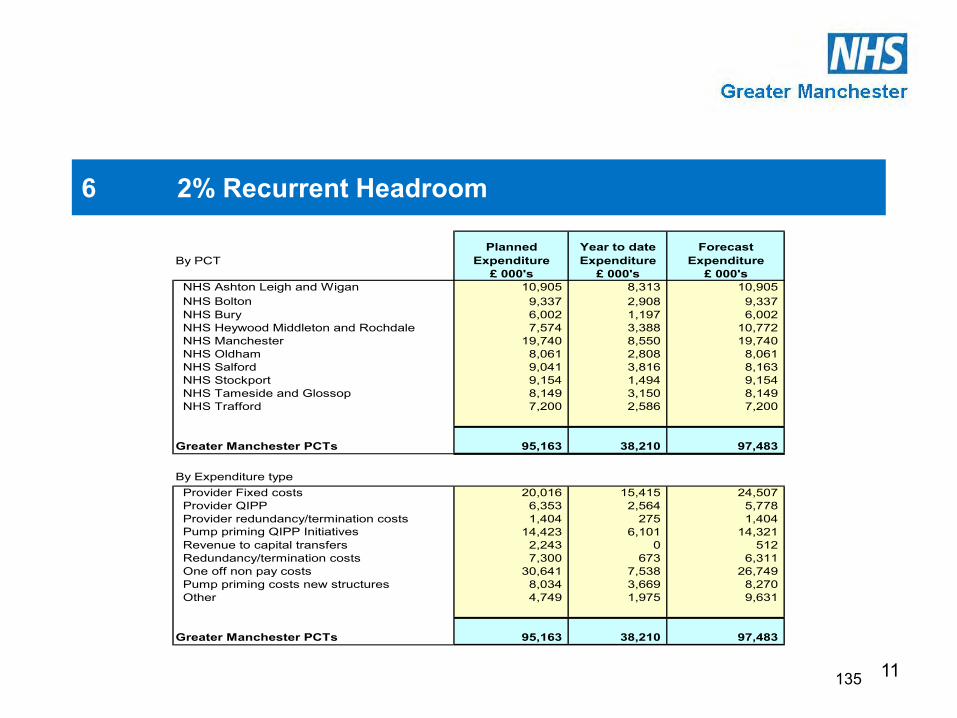
11
6 2% Recurrent Headroom
By PCTPlanned
Expenditure Year to date Expenditure
Forecast Expenditure
£ 000's £ 000's £ 000's NHS Ashton Leigh and Wigan 10,905 8,313 10,905 NHS Bolton 9,337 2,908 9,337 NHS Bury 6,002 1,197 6,002 NHS Heywood Middleton and Rochdale 7,574 3,388 10,772 NHS Manchester 19,740 8,550 19,740 NHS Oldham 8,061 2,808 8,061 NHS Salford 9,041 3,816 8,163 NHS Stockport 9,154 1,494 9,154 NHS Tameside and Glossop 8,149 3,150 8,149 NHS Trafford 7,200 2,586 7,200
Greater Manchester PCTs 95,163 38,210 97,483
By Expenditure type Provider Fixed costs 20,016 15,415 24,507 Provider QIPP 6,353 2,564 5,778 Provider redundancy/termination costs 1,404 275 1,404 Pump priming QIPP Initiatives 14,423 6,101 14,321 Revenue to capital transfers 2,243 0 512 Redundancy/termination costs 7,300 673 6,311 One off non pay costs 30,641 7,538 26,749 Pump priming costs new structures 8,034 3,669 8,270 Other 4,749 1,975 9,631
Greater Manchester PCTs 95,163 38,210 97,483
135

12
6 2% Recurrent Headroom
•The 2011-12 Operating Framework advised that 2% of each PCT’s recurrent revenue allocation would be topsliced andheld by the Strategic Health Authority, and that PCTs would be required to submit business cases to access the fundingto demonstrate the non recurrent nature of the expenditure. This process has now been completed and the funds havenow been returned to each PCT to spend in accordance with approved plans.
•To date, £38.2m has been spent against the planned expenditure of £95.2m, and forecasts are largely in line with plans.NHS Salford is forecasting spend of £878k less than plan, mainly due to lower clinical commissioning groupdevelopment costs (already fully funded recurrently) and termination costs less than forecast. NHS Heywood Middletonand Rochdale is forecasting additional costs of £3.2m, related to the Healthy Futures acute sector service redesign.
•One off non pay costs include expenditure related to transition such as dilapidations costs, estates and legal costs andCCG development.
136
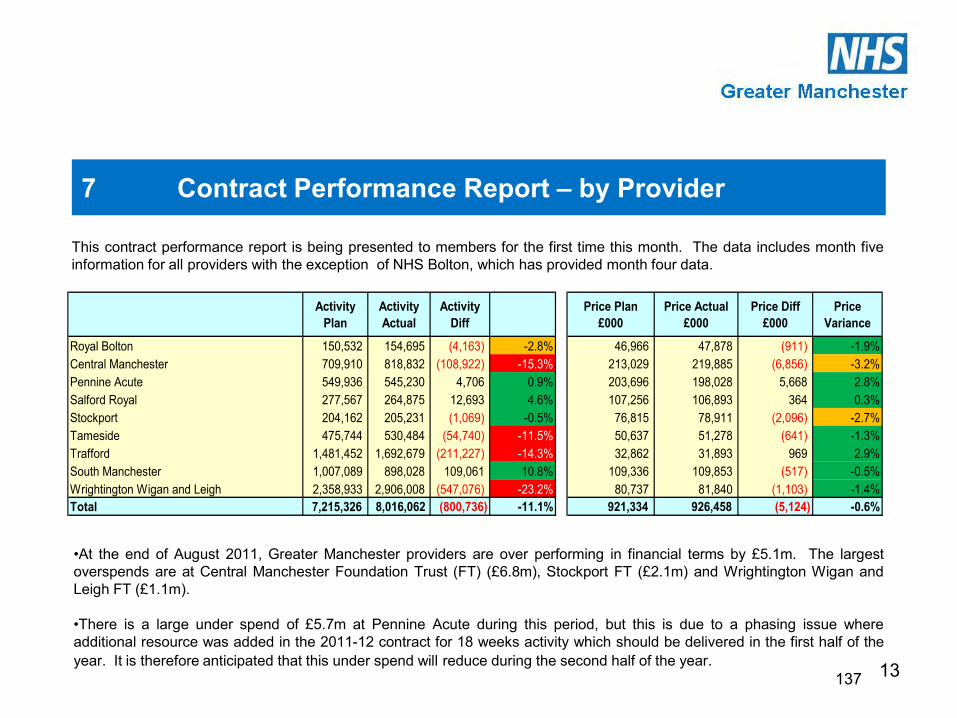
13
7 Contract Performance Report – by Provider
•At the end of August 2011, Greater Manchester providers are over performing in financial terms by £5.1m. The largestoverspends are at Central Manchester Foundation Trust (FT) (£6.8m), Stockport FT (£2.1m) and Wrightington Wigan andLeigh FT (£1.1m).
•There is a large under spend of £5.7m at Pennine Acute during this period, but this is due to a phasing issue whereadditional resource was added in the 2011-12 contract for 18 weeks activity which should be delivered in the first half of theyear. It is therefore anticipated that this under spend will reduce during the second half of the year.
This contract performance report is being presented to members for the first time this month. The data includes month fiveinformation for all providers with the exception of NHS Bolton, which has provided month four data.
Activity Plan
Activity Actual
Activity Diff
Price Plan £000
Price Actual £000
Price Diff £000
Price Variance
Royal Bolton 150,532 154,695 (4,163) -2.8% 46,966 47,878 (911) -1.9%Central Manchester 709,910 818,832 (108,922) -15.3% 213,029 219,885 (6,856) -3.2%Pennine Acute 549,936 545,230 4,706 0.9% 203,696 198,028 5,668 2.8%Salford Royal 277,567 264,875 12,693 4.6% 107,256 106,893 364 0.3%Stockport 204,162 205,231 (1,069) -0.5% 76,815 78,911 (2,096) -2.7%Tameside 475,744 530,484 (54,740) -11.5% 50,637 51,278 (641) -1.3%Trafford 1,481,452 1,692,679 (211,227) -14.3% 32,862 31,893 969 2.9%South Manchester 1,007,089 898,028 109,061 10.8% 109,336 109,853 (517) -0.5%Wrightington Wigan and Leigh 2,358,933 2,906,008 (547,076) -23.2% 80,737 81,840 (1,103) -1.4%Total 7,215,326 8,016,062 (800,736) -11.1% 921,334 926,458 (5,124) -0.6%
137

14
7 Contract Performance Report – by Commissioner
•PCT performance ranges from £1.4m under spend (NHS Bury) and £2.5m overspend (NHS Stockport). In terms ofpercentage variance from plan, the range is 2.9% under plan (NHS Bury) and 3.7% over plan (NHS Tameside andGlossop).
Activity Plan
Activity Actual
Activity Diff
Price Plan £000
Price Actual £000
Price Diff £000
Price Variance
Ashton Leigh and Wigan 2,255,708 2,736,426 (480,718) -21.3% 82,897 84,164 (1,266) -1.5%Bolton 159,072 148,314 10,758 6.8% 46,280 47,963 (1,683) -3.6%Bury 137,611 141,203 (3,592) -2.6% 48,387 46,963 1,424 2.9%Heywood Middleton and Rochdale 155,323 156,895 (1,572) -1.0% 57,131 56,262 869 1.5%Manchester 1,419,351 1,412,528 6,823 0.5% 155,483 154,848 635 0.4%Oldham 174,370 172,579 1,791 1.0% 57,663 58,235 (572) -1.0%Salford 178,286 182,613 (4,326) -2.4% 65,306 64,877 429 0.7%Stockport 263,476 276,540 (13,065) -5.0% 75,981 78,490 (2,510) -3.3%Tameside and Glossop 503,486 559,493 (56,007) -11.1% 64,661 67,056 (2,395) -3.7%Trafford 1,499,662 1,674,335 (174,673) -11.6% 66,669 67,848 (1,179) -1.8%All Other PCTs - Core Services 239,381 342,499 (103,118) -43.1% 55,214 54,260 953 1.7%Core Total 6,985,727 7,803,427 (817,699) -11.7% 775,673 780,966 (5,294) -0.7%
Collaborative Contracts 49,406 43,765 5,641 11.4% 41,810 41,020 789 1.9%North West Specialist services commissioned by NWSCT 180,192 168,870 11,322 6.3% 103,851 104,471 (620) -0.6%Total Other Contracts (Specialist and Collab)
229,598 212,635 16,963 7.4% 145,661 145,491 170 0.1%
Grand Total Provider Income 7,215,326 8,016,062 (800,736) -11.1% 921,334 926,458 (5,124) -0.6%
138

15
7 Contract Performance Report – by Care Group
•Elective admissions and day cases are under spent by £1.5m. Pennine Acute is £5m under spent due to phasing ofwaiting list activity and it is anticipated that this under spend will reduce. Providers that are over activity are StockportFT £1.8m and Central Manchester FT £1.8m.•Outpatients are over spent by £1.8m, the majority of which is at Central Manchester FT £1.6m.•Non Elective admissions are £1m over spent. Central Manchester FT is £3m over spent although there is a risk shareagreement with the provider and some PCTs, where block agreements have been made and PCTs will receive a rebateagainst over performance. Salford Royal FT and Trafford Healthcare are reporting under performance to date on nonelective of £0.8m and £1.0m respectively.All other points of delivery £4.5m over spent - the main issues are Critical Care at University Hospitals South Manchester£1.6m, high cost drugs at Wrightington Wigan and Leigh FT £1.0m and Pennine FT drugs £0.5m.
Activity Plan
Activity Actual
Activity Diff
Price Plan £000
Price Actual £000
Price Diff £000
Price Variance
Elective Admissions and Planned Same Day 149,496 147,951 1,545 1.0% 171,058 169,572 1,486 0.9%Elective Excess Beddays 12,426 11,158 1,268 10.2% 3,118 2,801 316 10.2%Outpatients (include procedures, radiology and ward attenders) 1,325,064 1,348,084 (23,020) -1.7% 152,328 154,131 (1,803) -1.2%Sub Total Planned Care 1,486,986 1,507,193 (20,207) -1.4% 326,504 326,504 0 0.0%
A&E 406,591 409,408 (2,817) -0.7% 38,042 38,680 (638) -1.7%Non Elective Admissions 158,949 159,084 (135) -0.1% 254,495 255,572 (1,077) -0.4%Non Elective Excess Beddays 72,086 60,783 11,303 15.7% 16,842 14,667 2,175 12.9%Sub Total Unplanned Care 637,627 629,275 8,352 1.3% 309,378 308,919 459 0.1%
All Other Points of Delivery 4,839,173 5,566,777 (727,604) -15.0% 222,972 227,565 (4,592) -2.1%Grand Total 6,963,785 7,703,245 (739,460) -10.6% 858,854 862,988 (4,134) -0.5%
139

16
7 Contract Performance Report - Independent Sector
Annual Annual
Plan Plan Actual Variance Plan PlanGuaranteed
FixedValue
GuaranteedFixedValue
Reduction
NETGuaranteed
FixedValue
Actual Variance
GM Pct's@ Guaranteed
Levels
`Ashton, Leigh & Wigan 2,164 1,076 691 (385) 351 174 148 (8) 140 127 (13) 12 127 139Bolton 17,848 8,899 4,787 (4,112) 2,836 1,413 1,201 (59) 1,142 830 (312) 289 830 1,119Bury 9,829 4,860 3,354 (1,506) 1,572 768 653 (48) 605 568 (37) 34 568 602Heywood, Middleton & Rochdale 28,194 13,942 9,327 (4,615) 4,758 2,323 1,975 (86) 1,889 1,577 (312) 289 1,577 1,866Manchester 40,149 19,882 14,529 (5,353) 6,493 3,188 2,709 (122) 2,587 2,243 (344) 319 2,243 2,562Oldham 15,835 7,738 5,035 (2,703) 2,389 1,150 977 (60) 917 817 (100) 93 817 910Salford 25,137 12,489 10,091 (2,398) 3,997 1,974 1,678 (100) 1,578 1,726 148 0 1,726 1,726Stockport 11,383 5,540 2,510 (3,030) 1,889 898 764 (6) 758 486 (272) 252 486 738Tameside & Glossop 20,349 9,826 4,841 (4,985) 3,315 1,553 1,320 (44) 1,275 806 (470) 435 806 1,240Trafford 20,993 10,133 5,938 (4,195) 3,407 1,594 1,355 (114) 1,242 1,090 (152) 141 1,090 1,230
Total 191,882 94,384 61,111 (33,273) 31,007 15,034 12,779 (646) 12,133 10,270 (1,863) 1,863 10,270 12,133
Utilisation Adjustment
Actual Cost of activity
Current YTD Amount Due
EXPENDITURE (£000)ACTIVITY
Year to Date Position @ Month 6Year to Date Postion @ Month 6
140

17
7 Contract Performance Report - Independent Sector
•The table on the previous page illustrates the month six position for PCTs, detailing performance against planned activity,amount due from each PCT, the value of actual activity and the adjusted shortfall. Utilisation of the contract has seensignificant year on year improvement. The current year to date shortfall is £1,863k, where as the month six position in2010-11 was a shortfall of £3,991K, a significant improvement of £2,128K.
•Utilisation and Performance –Since May referrals have increased by just over 1% per month. As with previous monthsalthough utilisation performance has seen a continued increase, due to the sustained higher monthly plan percentageutilisation remains fairly static. Year to date referrals received equate to 70% utilisation (82% of guaranteed levels).However following re-energised engagement, referral levels increased in September to the highest since servicecommencement. This increase should result in increased financial utilisation through the remaining months.
•The financial position at month six shows actual spend at £10,207k against a guaranteed payment of £12,779k. Howeverthe actual guarantee payments have been reduced by £646k due to the application of penalties relating toperformance. The overall shortfall at the end of month six is £1,863k, equating to an overall percentage utilisation of 85%.
•Currently NHS Salford is the only PCT performing at the required level. The under-performing PCTs gain benefit from anyover-utilisation. Any PCTs who over-perform against the guarantee levels, are charged for their actual usage however, anyPCT overspend is prorated between the under-performers, by apportioning the value of any over-utilisation to all other
PCTs.
141

18
8 Running Costs Analysis
* The original management costs target issued by the Strategic Health Authority in March 2010** The new definition of running costs as set out in the 2011-12 Operating Framework
Original Target to 2013-14 *
£000
Planned Reduction by 2011-12
£000
Actual Reduction by 2010-11
£000
Forecast reduction
running costs 2011-12 **
£000
Total reduction
forecast to 2011-12
£000
Under/(over) achieved to
date £000
% of total reduction
NHS Ashton Leigh and Wigan 7,738 5,548 908 3,561 4,469 1,079 58NHS Bolton 1,840 1,319 500 717 1,217 102 66NHS Bury 2,203 1,580 (82) 1,788 1,706 (126) 77NHS Heywood Middleton and Rochdale 3,581 2,568 1,016 2,378 3,394 (826) 95NHS Manchester 7,445 5,338 1,838 3,487 5,325 13 72NHS Oldham 3,143 2,253 860 1,210 2,070 183 66NHS Salford 5,128 3,677 1,547 1,981 3,528 149 69NHS Stockport 743 533 355 208 563 (30) 76NHS Tameside and Glossop 2,785 1,997 1,173 1,700 2,873 (876) 103NHS Trafford 3,125 2,240 962 919 1,881 359 60
37,731 27,053 9,077 17,949 27,026 27 72
142

19
8 Running Costs Analysis
•The management costs target reduction issued by the Strategic Health Authority in March 2010 totalled £37.7m for the tenGreater Manchester PCTs, and was to be achieved by 2013-14. Over 70% of the reduction was to be achieved by 2011-12.At the end of 2010-11, a £9.1m saving in management costs was reported in the PCTs’ annual accounts and thisrepresented a shortfall of £1.4m against the 2010-11 target. This shortfall was mainly contributed by NHS Ashton Leigh andWigan (£1.2m) and NHS Bury (£0.7m).
•The Strategic Health Authority has suggested that there will be no changes to the running costs target for 2011-12, for theremainder of this financial year. The cumulative forecast savings are £27,026k against a target of £27,053k, so it can beconcluded that overall, PCTs in Greater Manchester are on target.
•There needs to be a recognition that there are significant additional costs being incurred to support the transition to the neworganisational structure from 1 April 2013; it is hoped that the 2012-13 Operating Framework will reflect this and amend thephasing of target running cost reductions. The Operating Framework is expected to be published in November 2011.
143

9 Capital Investment Programme
Actual YTD
ExpenditureDisposals /Grants
/IFRIC-12 Net CRL ExpenditureDisposals /Grants
/IFRIC-12 Net CRL ExpenditureDisposals /Grants
/IFRIC-12 Net CRL
NHS Ashton Leigh and Wigan 2,068 (1,633) 435 78 0 78 1,356 (715) 641NHS Bolton 16,130 (11,925) 4,205 114 0 114 15,180 (11,725) 3,455NHS Bury 1,558 (592) 966 393 (135) 258 1,558 (592) 966NHS Heywood Middleton and Rochdale 925 (340) 585 130 (6) 124 779 (366) 413NHS Manchester 3,718 0 3,718 380 0 380 3,718 0 3,718NHS Oldham 15,346 (16,942) (1,596) 1,231 (895) 336 13,620 (13,410) 210NHS Salford 3,954 (831) 3,123 63 0 63 1,801 (831) 970NHS Stockport 2,092 (427) 1,665 17 0 17 2,092 (427) 1,665NHS Tameside and Glossop 1,105 (340) 765 37 (225) (188) 1,105 (340) 765NHS Trafford 1,900 (1,050) 850 135 0 135 950 0 950
48,796 (34,080) 14,716 2,578 (1,261) 1,317 42,159 (28,406) 13,753
ForecastPlan
144
21
9 Capital Investment Programme
•All PCTs are forecasting to remain within the net Capital Resource Limit for 2011-12, although there has been verylittle expenditure to date on the capital programmes. Whilst PCTs have profiled the majority of their planned capitalexpenditure for the second half of the year, actual expenditure to date of £2,578k is still £3m behind plan.
•NHS Bolton have indicated that the equipping costs of Bolton One are less than expected and consequently there aresurplus capital funds of £1m available for reprioritisation across the North West.
•Approximately £6.3m of planned capital expenditure was dependent on the disposal of assets, all to non NHS bodies,and PCTs have programmed capital schemes to commence only when disposals are certain. PCTs have now revisedtheir forecasts of disposals and the likely resource available in 2011-12 will be £4.7m.
•IT schemes total £4.4m and work is currently being undertaken to review the nature of planned expenditure anddetermine whether efficiencies in procurement and/or implementation are possible across the Greater Manchesterfootprint.
•Approximately £23m of the proposed capital expenditure relates to the capitalisation of two LIFT schemes at NHSOldham and NHS Bolton. The Oldham scheme has now been handed over at a likely value of £11.3m and theamount charged against the Capital Resource Limit for NHS Bolton will depend on the final build costs of the schemesat the handover date of February 2012.
145
10 Recommendations
10.1 The NHS Greater Manchester Board are asked to note the contents of the report.
10.2 The NHS Greater Manchester Board is asked to recognise the risks associated with the delivery of the control totals in each PCT, which the locality management are required to deliver.
146

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 13 10 November 2011 REPORT OF:
Executive Director of Commissioning Development and Deputy Chief Executive
DATE OF PAPER:
25 October 2011
SUBJECT:
Development of Commissioning Support Service (CSS) Governance Arrangements
IN CASE OF QUERY, PLEASE CONTACT
Dr Julie Higgins, 0161 212 4821
PURPOSE OF PAPER: The NHS Greater Manchester Board is asked to support the establishment of the CSS Development Board and support the delegated authority to progress necessary legal, human resources and financial steps to progress successful completion.
147

Development of Commissioning Support Service (CSS) Governance Arrangements Executive Summary The purpose of this paper is to update the Board on current progress on CSS; provide a summary of recent draft guidance, support the establishment of the CSS Development Board and support the delegated authority to progress necessary legal, human resources and financial steps to progress successful completion. 1 Background and progress to date 1.1 This paper further updates the Board following the July 2011 paper. Work has progressed in
relation to building a case for change principally through conversation and use of the ready reckoner to facilitate understanding of how CCGs will use their budgets to deliver their accountabilities and commission CSS. A series of discussions with CCG Chairs has produced a long list of possible services for CSS and gained commitment for design of back office functions. Consideration is also being given to CSS offer to NCB and other potential customers. Ongoing development of the shared service pipe line has continued and is now populated with 25 services. The critical path for services is the development of high level service specifications, detailed service specification and HR plans. A detailed programme plan is in development and the DH Gateway Review Team have assessed our governance and made recommendations.
1.2 Draft guidance was issued by DH this month outlining the Departments of Health’s vision for commissioning support. Key messages were: • A strategic approach is required to develop commissioning support services towards a market
system and should build on the needs of CCGs
• Significant savings can be made in sharing back office functions and a model has been developed that groups commissioning support functions into six categories and gives an indication of what can be delivered at scale, nationally, at cluster and in house
• Running costs are likely to be within £25-35 per head and CCGs will buy commissioning support from this budget
• Transition to commissioning support is complicated as we have to continue the day job; current and new models may be very different and require a different culture; CCGs will need to demonstrate they have adequate support for authorisation; if CCGs go to the market, procurement will take them beyond 2013. Consequently, the period of NHS development has been extended by allowing the NCB to host viable arms length commissioning support services until 2016 at the latest after which commissioning support will become fully commercial
148

• From 2013, CCGs will be able to get their commissioning support from whomever they wish and will use NHS services until they are ready to go to the market following formal procurement processes. TUPE is expected to apply
• Potential commissioning support including those hosted by CCGs will be fully assessed to ensure NCB and CCGs are not taking on unacceptable risk
• The roadmap for development includes: a prospectus by December 2011, an outline business case by March 2012 and full business case by August 2012
1.3 In order to successfully deliver the milestones as outlined above, the development of an arms length arrangement to manage the CSS is proposed. This arrangement is more closely aligned to the proposed temporary hosting arrangement by the NCB and will better support the freedoms and flexibility to operate the commercial relationship that will be in place in the future with CCGs, NCB and other customers.
2 Proposed Establishment of a CSS Development Board 2.1 The proposed terms of reference for NHS Greater Manchester’s CSS Development Board is
attached in Appendix 1 and these capture the breadth and complexity of the various work streams.
2.2 The CSS Development Board will have three aims:
• To oversee the establishment of Greater Manchester CSS
• Describe the governance and delegated powers of the arms length arrangement (ALA) which will be established by March 2012 to fit in with the production of the outline business case
• Programme management of the various work streams that will lead to the CSS such as shared service development and commercial readiness
2.3 It is proposed that the CSS Development Board will be chaired by a lay representative from the former community of Non-Executive Directors in NHS Greater Manchester with a further two-three lay representatives and the Executive making up the membership.
2.4 Reporting to the Board will be a number of Operational Sub-Committees, in particular a Commissioning Support Steering Group which will ensure the development of the shared services of CSS.
2.5 The CSS Board will meet monthly and report through the DCD to each Cluster Board.
2.6 CSS will be hosted by NHS Greater Manchester via the arms length agreement until 2013 when it will transfer to the National Commissioning Board. Prior to this date, staff who are seconded to CSS will be hosted by NHS Salford.
2.7 Development of the CSS will be taken forward by a Chief Operating Officer who will be semi-autonomous when the ALA is in place. Recruitment to this post has commenced.
2.8 The Board is asked to grant delegated authority to the Executive Team to progress necessary legal, human resources and financial steps to progress successful transition to the ALA.
149

3 Recommendation 3.1 The NHS Greater Manchester Board is asked to:
• Support the establishment of the CSS Development Board • Support the delegated authority to progress necessary legal, human resources and financial
steps to progress successful completion to progress successful completion
Dr Julie Higgins Executive Director of Commissioning Development/ Deputy Chief Executive Appendix One
150
CSS Development Board Draft Terms of Reference 1 Scope
1.1 Those services that can possibly be part of the CSS offer in shadow and after 2013.
2 Purpose
2.1 To oversee the establishment of Greater Manchester CSS.
2.2 To describe the governance and delegated powers of the arms length arrangement (ALA), which will be established by March 2012 to fit in with the production of the outline business case.
2.3 To programme manage the various work streams that will lead to the CSS such as shared service development and commercial readiness.
3 Membership
3.1 The membership shall comprise of: • Lay member* (Chair of CSS Development Board) • Two Lay members* • Chief Executive • Director of Commissioning Development • Director of Finance • Director of Human Resources • Two CCG Chair Council Reps • AGMA Rep • Public Health Rep • Commissioning Support Service Chief Operating Officer • Lay members from the former community of Non-Executive Directors in NHS Greater
Manchester
4 Accountability
4.1 To ensure that there is a full engagement process including the case for change and that this is shared and developed with staff and CCGs and other potential customers.
4.2 To manage emergent strategy and translate policy into tangible actions.
4.3 To manage a gateway process and programme of delivery to set up shared services that migrate to CSS.
4.4 To identify and manage dependencies between the shared service lines.
4.5 To identify and manage financial and resource targets for service lines.
4.6 To ensure staff are supported and manage high quality HR processes.
4.7 To prepare the CSS for commercial readiness.
151

4.8 To ensure delivery of key milestones as laid out in DH roadmap – prospectus, OBC and FBC.
4.9 To describe the governance and delegated powers of the arms length arrangement (ALA).
5 Term of Delegated Powers
5.1 To be reviewed in six months.
6 Frequency of meetings
6.1 Meetings should normally be held on a monthly basis, and not less than four times in six months.
7 Reporting
7.1 The CSS Development Board should report to the Trust Board through the Director of
Commissioning Development at each Trust Board meeting.
152
NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 14 10 November 2011 REPORT OF:
Board Secretary
DATE OF PAPER:
28 October 2011
SUBJECT:
Terms of Reference – Board Committees
IN CASE OF QUERY, PLEASE CONTACT
Rob Bellingham 0161 212 6141
PURPOSE OF PAPER: This paper sets out the Terms of Reference for two committees reporting directly to the NHS Greater Manchester Board. Additionally, Terms of Reference for the Audit Committee and Locality Audit Groups have been provided for approval as part of the report of the Audit Committee. The NHS Greater Manchester Board is asked to:
• Approve the Terms of Reference for the Clinical Commissioning Board, (this committee will fulfil the statutory function of the Professional Executive Committee, (PEC))
• Approve the Terms of Reference for the Service Transformation Board
153

Terms of Reference – Board Committees
Executive Summary The purpose of this paper is to set out the Terms of Reference for two committees reporting directly to the NHS Greater Manchester Board.
GREATER MANCHESTER CLINICAL COMMISSIONING BOARD TERMS OF REFERENCE
1 Purpose of the Group
1.1 To provide NHS Greater Manchester with strong clinical leadership which will shape and deliver
NHS GM’s Business Plan and key objectives. To stimulate and lead innovation in care pathway re-design, securing active clinical engagement from a broad range of clinicians, in order to improve outcomes for patients. To promote clinical quality and safety in all services commissioned by NHS Greater Manchester, and give an independent clinical view on PCT clinical policies and protocols.
2 Objectives of the Group 2.1 The Clinical Commissioning Board will support NHS GM’s central roles of tackling health
inequalities and improving health through commissioning and work with partners. This will be achieved through strong clinical leadership and active clinical engagement.
2.2 The Clinical Commissioning Board will actively support the delivery of NHS GM’s Business Plan
objectives to:- Tackle inequality Deliver financial balance Improve clinical standards Engage with the public and patients Improve health and well being Work in partnership with others Increase choice Ensure safe and effective services Ensure robust emergency plans To identify emerging clinical leaders and support their development To support existing clinical leaders to develop their skills and to provide advice and
mentorship to them as required
Within these objectives the Clinical Commissioning Board will:- Provide strong clinical leadership to NHS GM; Support NHS GM in developing and delivering its commissioning strategy; Support business continuity of GM level commissioning business; Lead clinical communications with partners and stakeholders on behalf of NHS GM; Providing clinical scrutiny of service innovation: safety, quality and appropriateness;
154

Support the creation of and ultimately relate to the establishment of Clinical Senate(s) within Greater Manchester;
Provide oversight of commissioning reform across Greater Manchester ensuring that local decisions are coherent and that pace of change is aligned;
Provide leadership and direction to the Greater Manchester Clinical Networks; Provide commissioning authority for Clinical Networks work programmes; and Provide a mechanism to support effective engagement with the developing Clinical
Commissioning Groups through routine engagement (and, where possible, common membership) with the Greater Manchester GP Commissioning Council.
2.3 The Clinical Commissioning Board will scrutinise clinical protocols and pathways and recommend
approval where appropriate. 2.4 Clinical Commissioning Board members will work with GP Commissioning partners to develop
new pathways and business cases for innovation. The Chair(s) will contribute to the approval process when cases and projects are brought to NHS GM’s Executive Team for approval. Where a conflict of interest or financial benefit could occur the relevant CCB member must declare their interest and absent themselves from any discussion or decision in that case.
2.5 The Clinical Commissioning Board will ensure that it develops mechanisms to hear from and
represent the views of local clinicians. 2.6 The Clinical Commissioning Board will support the delivery of NHS GM’s communications
strategy, by providing clinical input to any relevant media campaigns, public education and reactive responses to media enquiries.
2.7 The Clinical Commissioning Board will produce an annual work plan, supported by a published
Forward Plan with clearly identified priorities, timescales and identified leads which will align to NHS GM’s Business Plan and strategy.
3 Membership 3.1 Membership will comprise:
NHS Greater Manchester Medical Director (Chair) Representatives from each of the GM CCGs, (1 per CCG) NHS Greater Manchester Director of Quality & Performance (Nurse Member) NHS GM Finance and Public Health Representation
4 Quorum 4.1 The quorum will be seven Clinical Commissioning Board members. This must include a minimum
of five clinicians/professional members and one officer member. 5 Frequency of Meetings 5.1 Clinical Commissioning Board meetings will be held monthly and all members as described above
will be expected to attend, wherever possible. Formal agendas and minutes will be produced which will be public documents; minutes will be reported to the Board.
6 Accountability 6.1 The Clinical Commissioning Board is formally constituted as a committee of the NHS Greater
Manchester Board and will submit written updates to the board at least bi-monthly. 6.2 The Clinical Commissioning Board Chair (s) will work closely with Chief Executive of NHS GM
and report to the NHS GM Chairman and will have an appraisal at least annually
155

6.3 The Clinical Commissioning Board Chair (s) and members will work closely with the NHS Greater
Manchester Board and Executive Team 6.4 The NHS Greater Manchester Board will delegate decision making to the Clinical Commissioning
Board according to the NHS Greater Manchester Scheme of Delegation of Powers. 6.5 Performance, roles and responsibilities will be regularly reviewed with a formal annual report to
the NHS Greater Manchester Board.
156

GREATER MANCHESTER SERVICE TRANSFORMATION BOARD TERMS OF REFERENCE
1 Purpose and Objectives 1.1 To ensure a Greater Manchester programme is in place to meet the requirements of QIPP, as set
by national policy and direction.
1.2 To ensure the QIPP programme will both support a viable and sustainable provider system and recognises the role of partner organisations through the alignment and integration of health, social care and public health.
1.3 To oversee the development and agree the “level 3” Greater Manchester QIPP programme which will include a “Greater Manchester Strategy for Service Redesign” – a strategic redesign of key areas of secondary and tertiary healthcare to achieve high quality, safe, accessible hospital services across Greater Manchester.
1.4 To ensure co-ordination and oversight of the development and delivery of supra-local (level 2+) plans is achieved, without competing or conflicting developments.
1.5 To ensure oversight, reporting and assurance processes are in place to provide the DH and other key stakeholders that GM QIPP plans are robust and meet the defined objectives.
1.6 To assess progress and performance against key tasks and key milestones contained with QIPP plans and within the GM Strategy for Service Redesign. If and where underperformance is identified, implications are explored and corrective action is identified and direction given.
1.7 To ensure a comprehensive and robust programme management approach to service transformation is developed and implemented coherently by the GM Programme Management Office (PMO) for all projects within the work programme.
1.8 To ensure that there is a robust and effective clinical assurance process in place that is robustly applied to all service transformation projects.
1.9 To ensure that all service transformation projects have clearly identified quality benefits.
1.10 To ensure that there is an effective risk management strategy and following that, following analysis, appropriate action is taken.
2 Membership 2.1 Membership will comprise:
Non Executive Director – Chair Representatives from Clinical Commissioning Groups across Greater Manchester Director of Service Transformation, NHS Greater Manchester Director of Finance, NHS Greater Manchester Director of Performance & Quality, NHS Greater Manchester Medical Director, NHS Greater Manchester Director of Commissioning, NHS Greater Manchester Reconfiguration Lead, NHS North SHA
157

2.2 At certain points in the development and implementation of the service transformation programme
the Board’s membership will be extended to other key stakeholders including providers and local authorities.
2.3 In attendance:-
Service Transformation project leads as required.
3 Quorum 3.1 The quorum will be five members, including at least two CCG representatives, an Executive
Director and the Chair (or a nominated vice-chair) 4 Frequency of Meetings 4.1 Clinical Commissioning Board meetings will be held at least quarterly and all members as
described above will be expected to attend, wherever possible. Formal agendas and minutes will be produced which and will be reported to the Board. As some of the business to be transacted will be confidential in its nature, it may be necessary for reporting to take place at part 2 of the Board. This will be kept under review, with a commitment to report outcomes to part 1 at the earliest opportunity.
5 Accountability 5.1 The Service Transformation Board is formally constituted as a committee of the NHS Greater
Manchester Board. Robert Bellingham Board Secretary
158

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 15 10 November 2011 REPORT OF:
Board Secretary
DATE OF PAPER:
1 November 2011
SUBJECT:
Board Assurance Framework
IN CASE OF QUERY, PLEASE CONTACT
Rob Bellingham 0161 212 6141
PURPOSE OF PAPER: This paper builds on the paper presented to the September Board meeting relating to risk management arrangements, providing a high level summary of the position of each of the Greater Manchester localities. A depiction is provided of the top strategic risks forming part of the NHS Greater Manchester Assurance Framework and their status in each of the 10 localities.
159

Board Assurance Framework
Executive Summary The paper describes the following key elements of the assurance work taking place in NHS Greater Manchester as follows: The risk management development process Assurance derived with regard to locality risk management arrangements The development of a Board Assurance Framework and the assessment of the top risks facing NHS Greater Manchester in the context of the Delivery Plan agreed at the September Board meeting. 1 INTRODUCTION
1.1 This paper builds on the Greater Manchester Risks paper presented at the September Board meeting as an introduction to the development of a risk assurance system for NHS Greater Manchester.
1.2 The risk management approach of NHS Greater Manchester has been developed through the
Cluster Governance Leads Group and Risk Sub-Group, with review from Mersey Internal Audit Agency.
2. RISK MANAGEMENT DEVELOPMENT PROCESS 2.1 Following the report to the September Board meeting, the following actions have been completed,
in line with the resolutions made at the meeting:
Stage One - The Risk Sub-Group convened to discuss an approach to the delivery of the actions mandated by the Board. Stage Two - A letter was sent to all Locality Managing Directors from the Chief Executive detailing the approach to be taken. Subsequently a Localities Risk Management request was issued requiring;
• A self-assessment to be completed on the risk management approach undertaken at each Locality
• Information on any risk management package or in-house system in use • The latest reported Locality Board Assurance Framework and Corporate Risk Register to
be provided
160
• Any Internal Audit reports for the period 2008-11 concerning the risk management arrangements at each Locality to be provided
• Assurance that a risk assessment had been conducted against the themes reported at the September Board meeting, ie financial, performance, quality, IM&T, transition/organisational change and health improvement. (This requirement was designed to address the issue raised at the September Board meeting, where there was an apparent significant variation in the themes being reported by localities).
Stage Three - The Risk Sub-Group re-convened and finalised the development of a NHS Greater Manchester Board Assurance Framework (BAF). The approach described in this paper bases the NHS GM Assurance Framework on the objectives set out in the Delivery Plan agreed at the September Board meeting. It is intended that this NHS GM Assurance framework complements, rather than duplicates, the ten Locality Board Assurance Frameworks. A reporting dashboard of the top risks for the BAF was compiled to provide robust and user friendly Board reporting. This approach has been supported by the NHS Greater Manchester Executive Team for presentation to the Board for approval. Further detail with regard to this process is contained within section 5 of this report. Stage Four - The NHS Greater Manchester risks were then issued to each locality for self-assessment. This supports the concept of a proportionate approach to risk and performance management, allowing focus to be placed on those localities where particular issues are being experienced.
3 LOCALITIES RISK MANAGEMENT ARRANGEMENTS 3.1 The key highlights of the Localities Risk Management Request submissions described at stage 2
in section 2.1 above are as follows:
• Self-Assessment – All ten localities provided responses to ten assessment questions as requested. Of the 100 responses, (ie 10 x 10), only three ‘red’ responses were received. These have each been individually followed up, with assurance gained that has reduced these initial assessments to amber ratings. As a next stage, each of the amber assessments received will be further reviewed but at the current stage of the process it is felt that there is reasonable assurance with regard to the systems and processes in place in each locality, (utilising a combination of the self-assessment returns, the content of the Locality Board Assurance Frameworks/ Corporate Risk Registers and the Internal Audit Assurances). These assessments will be kept under review and best practice shared and mandated across Greater Manchester with the aim of delivering further improvements across all localities.
• Risk Management Systems Used – Five Localities used Safeguard (with one also using
Covalent), two using Datix and one each using Performance Manager, EBMS and Performance Plus.
• Risk Strategies and Policies – All Localities provided their current risk strategy and/or
policy in place at their Locality.
161

• Locality Board Assurance Framework/Corporate Risk Registers – All Localities provided their latest Locality Board Assurance Framework and Corporate Risk Register.
• Internal Audit Assurances – The majority of Localities provided internal audit reports over
the period 2008-11 covering for example risk management, assurance frameworks and statements of internal control. Where internal audit reports have yet to be provided or where these reports have highlighted issues requiring further assurance or confirmation that actions have been carried out, further validation will take place in conjunction with the local governance leads.
3.2 Each locality confirmed that it had conducted assessments against each of the themes contained
within the Risk Report presented at the September Board meeting. Where some gaps initially appear against the risk themes, further validation and clarification is to take place in conjunction with the local risk leads.
4 INTERNAL AUDIT INPUT 4.1 A meeting has taken place with the Mersey Internal Audit Agency (MIAA) with regard to this work.
The approach described in this paper was presented and discussed, with an agreement that the MIAA would review and feedback accordingly. Any such feedback received ahead of the Board meeting will be verbally reported.
5 2011/12 NHS GREATER MANCHESTER BOARD ASSURANCE FRAMEWORK 5.1 Those risks currently outlined as being the most significant to achievement of the NHS Greater
Manchester Delivery Plan are contained at appendix 1. The risks are presented in a format which it is hoped provides a useful summary for Board members.
5.2 The respective elements of the dashboard are described below:
• Rank/Move - The initial rank of risk in number order, with the movement since the last reporting period.
• Objective Area - The area of the Greater Manchester Delivery Plan from which the risk has been identified.
• High Level Risk Description - The description of the risk in the context of the Greater Manchester Delivery Plan.
• Risk Assessment - The assessment of the risk based on likelihood multiplied by impact on a current basis (with controls applied) and on a target basis (when all mitigating actions have been completed).
• GM/Locality Position - The position based on a red, amber or green rating. For the majority of risks, the position in each locality is shown. For those risks which sit at a Greater Manchester level, a single indicator is shown to represent the GM position.
• Risk rating – The overall NHS Greater Manchester likelihood multiplied by impact assessment of the risk at the current time.
• Owner – The NHS Greater Manchester Board member accountable for the risk. • Oversight – Where the risk is reported and challenged as assurance of its management.
162

5.3 The Risk sub-group continues to meet to develop the next stages of this process. The current priority is to capture further detail to support the initial high level assessments received from localities. This process will incorporate all elements of the delivery plan, including those top level risks described in appendix 1.
6 RECOMMENDATIONS 6.1 The NHS Greater Manchester Board is requested to:
• Approve the content and format of the Board Assurance Framework Top Risks document shown at appendix 1
• Mandate the further development of the Greater Manchester Board Assurance Framework to complement the existing locality Assurance Frameworks
• Require the bi-monthly reporting of top risks at the NHS Greater Manchester Board meeting
Robert Bellingham Board Secretary
163

164
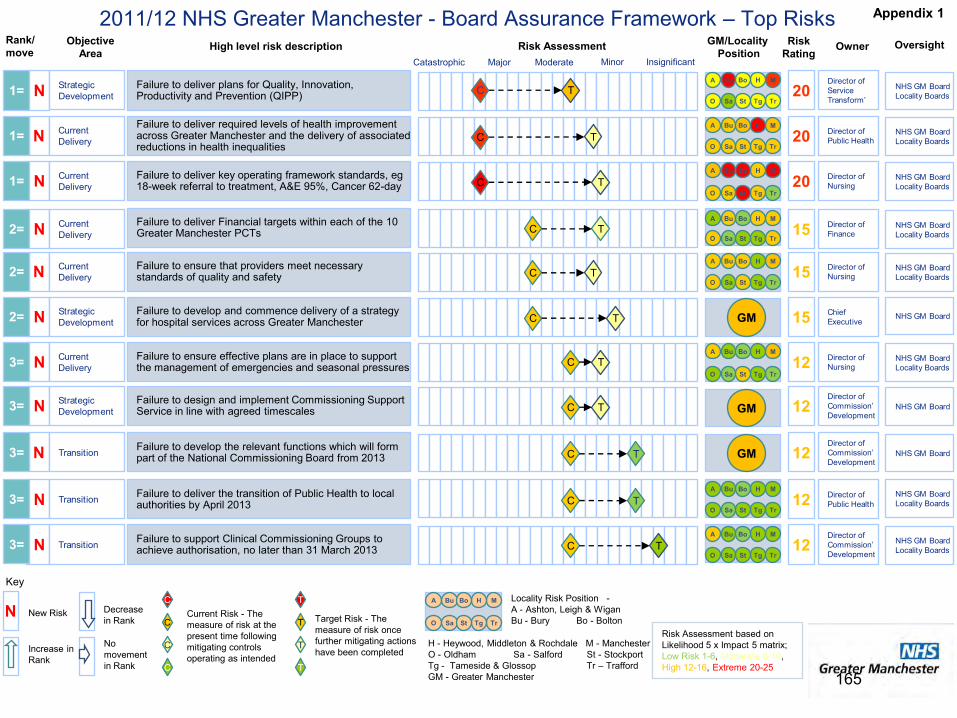
N
2011/12 NHS Greater Manchester - Board Assurance Framework – Top RisksRank/move OwnerObjective
AreaRisk Assessment Risk
RatingOversightHigh level risk description
MinorModerateMajorCatastrophic Insignificant
NHS GM Board Locality Boards12
Director of Commission’ Development
C T
NHS GM Board Locality Boards12 Director of
Public HealthC
NHS GM Board Locality Boards20
Director of Service Transform’
C T
C
CNew Risk Current Risk - The
measure of risk at the present time following mitigating controls operating as intended
T
T Target Risk - The measure of risk once further mitigating actions have been completed
T
T
C
C
Increase in Rank
Decrease in Rank
No movement in Rank
N
NHS GM Board12Director of Commission’ Development
T
NHS GM Board Locality Boards15N Director of
NursingT
NHS GM Board Locality Boards20 Director of
Nursing
Failure to ensure effective plans are in place to support the management of emergencies and seasonal pressures
NHS GM Board Locality Boards123= Director of
NursingT
Key
N
N
N
N
N
Failure to ensure that providers meet necessary standards of quality and safety 2=
3= Failure to design and implement Commissioning Support Service in line with agreed timescales
3=
Failure to support Clinical Commissioning Groups to achieve authorisation, no later than 31 March 2013
1= Failure to deliver key operating framework standards, eg 18-week referral to treatment, A&E 95%, Cancer 62-day
3=
Failure to deliver plans for Quality, Innovation, Productivity and Prevention (QIPP)
T
TTransition
Strategic Development
Strategic Development
Current Delivery
Current Delivery
Current Delivery
Transition
Failure to deliver the transition of Public Health to local authorities by April 2013
C
C
C
C
GM/Locality Position
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
O
A Bu
Sa
M
Tr
H
TgSt
Bo
H - Heywood, Middleton & Rochdale M - Manchester O - Oldham Sa - Salford St - Stockport Tg - Tameside & Glossop Tr – Trafford GM - Greater Manchester
Locality Risk Position -A - Ashton, Leigh & Wigan Bu - Bury Bo - Bolton
Risk Assessment based on Likelihood 5 x Impact 5 matrix; Low Risk 1-6, Moderate 8-10, High 12-16, Extreme 20-25
NHS GM Board Locality Boards15 Director of
FinanceC TN2= Failure to deliver Financial targets within each of the 10 Greater Manchester PCTs
Current Delivery O
A Bu
Sa
M
Tr
H
TgSt
Bo
NHS GM Board15 Chief ExecutiveC TN2= Failure to develop and commence delivery of a strategy
for hospital services across Greater Manchester Strategic Development
NHS GM Board12NDirector of Commission’ Development
Failure to develop the relevant functions which will form part of the National Commissioning Board from 2013 3= TTransition C
NHS GM Board Locality Boards20N Director of
Public HealthTFailure to deliver required levels of health improvement across Greater Manchester and the delivery of associated reductions in health inequalities
1=
Current Delivery C
O
A Bu
Sa
M
Tr
H
TgSt
Bo
1=
GM
GM
GM
Appendix 1
165

166

NHS GREATER MANCHESTER AGENDA ITEM NO 16 10 November 2011 REPORT OF:
Board Secretary
DATE OF PAPER:
1November 2011
SUBJECT:
Governance – Managing the Transition
IN CASE OF QUERY, PLEASE CONTACT
Rob Bellingham 0161 212 6141
PURPOSE OF PAPER: This paper builds on the Delivering Effective Governance paper agreed at the September Board meeting. It considers consequent changes in accountability arrangements at local level, a proposal for the governance of the Commissioning Support Service and describes the changing role of Locality Non-Executive and Managing Directors. Proposals are made to support the delivery of the transition process over the period to March 2013
167

Governance in NHS Greater Manchester – Managing the Transition Executive Summary This paper builds on the Delivering Effective Governance paper agreed at the September Board meeting. It considers consequent changes in accountability arrangements at local level, a proposal for the governance of the Commissioning Support Service and describes the changing role of Locality Non-Executive and Managing Directors. Proposals are made to support the delivery of the transition process over the period to March 2013. 1 Introduction 1.1 This document builds on the “Delivering Effective Governance in Greater Manchester” paper,
which was approved at the September 2011 Board meeting. The September paper described the current governance arrangements and defined the existing relationships between the NHS Greater Manchester Head Office and the 10 Localities. The Board formally approved these arrangements but mandated that further developmental work be done in the light of the ongoing development of Clinical Commissioning Groups.
1.2 The paper covers a range of governance related issues as set out below: • Setting out the changes to governance arrangements required in the context of the
development of Clinical Commissioning Groups, the transfer of Public Health to local authorities and the emergence of the National Commissioning Board
• The governance of the Commissioning Support Service • Describing the considerations in ensuring a smooth and safe transition to the new
arrangements • Considering the changing nature of existing key locality roles
1.3 The paper is framed in the context that it will be possible for Clinical Commissioning Groups to be
authorised from October 2012, with the objective for all to be authorised by March 2013. 1.4 Since the last Board meeting in September, further national developments have taken place as
follows: • A letter was issued on 29th September by Jim Easton, the National Director for
Improvement and Efficiency, relating to PCT Cluster Governance. The paper indicated that the “model 2” governance arrangement, as already implemented in NHS Greater Manchester, would be mandated for all PCT clusters to be in place by December 2011.
The characteristics of this arrangement are as follows: a single board meeting transacting, as far as is practicable, the board business
of all of the constituent PCTs; a single executive team with single chief executive;
168

a single individual as chair of the cluster, therefore excluding shared or rotating arrangements.
• The arrangements for Strategic Health Authority clustering are now in place, with NHS
North West now forming part of NHS North of England. The former chair of NHS North West is now one of two NHS North of England vice chairs and two former NHS North West Non Executive Directors are now Non Executives of NHS North of England. The remaining Non Executive Directors from the former NHS North West no longer hold Non Executive appointments
2 Changing Accountability Arrangements 2.1 Direct Line of reporting 2.1.1 Following the mandate given at the September Board meeting for governance models to “develop
and evolve in the light of the implementation of Clinical Commissioning Groups”, the NHS Greater Manchester Board has given further consideration to the next stage of the process. Much of this thinking took place at a Board Development session which was held on the 15th September. This paper sets out proposals based on the outcomes of these discussions. The proposals are designed to help ensure that Clinical Commissioning Groups are in a position to develop the track record which will be required to support the authorisation process.
2.1.2 To ensure clarity of accountability and reporting arrangements, each CCG will be required to
agree an Accountability Agreement with NHS Greater Manchester. This agreement will set out the key duties and responsibilities of the CCG and include the following key principles:
• Lead locality responsibility to be transferred from Locality Boards to CCGs no later than 31
March 2012. • The CCG will be the single reporting line from the area they serve to NHS Greater
Manchester, with the CCG Chair and shadow/interim Chief Officer assuming lead management accountability
• The membership of the CCG Governing Body should reflect the relevant guidance to include at least two lay members, "one with a lead role in championing patient and public involvement, the other with a lead role in overseeing key elements of governance such as audit, remuneration and managing conflicts of interest". Additionally, there should be plans in place to recruit “at least one registered nurse and one doctor who is a secondary care specialist".
• Appropriate leadership, management and management development arrangements will be in place to discharge the responsibilities set out in the Accountability Agreement
• Arrangements will be in place for the appropriate consideration and management of Quality and Safety issues. The Francis Report standards (drawn from the initial report into events at Mid Staffordshire Hospitals Trust), represent the minimum criteria that NHS Greater Manchester will require CCGs to meet prior to the handover taking place.
• Arrangements will be in place for the consideration and active management of performance. This focus on performance will be an ongoing priority for NHS Greater Manchester and NHS North of England and will therefore represent a key element of the accountability agreement.
169

• Arrangements will be in place for the management of a devolved budget including delivery of the local Quality, Innovation, Productivity and Prevention, (QIPP), programme, (there will be a requirement for the NHS Greater Manchester Scheme of Reservation and Delegation to be amended to take this into account)
• Arrangements will be in place to ensure active monitoring and management of patient experience indicators.
2.2 National Commissioning Board and Local Authority Functions 2.2.1 It is recognised that not all functions discharged by PCTs will transfer to Clinical Commissioning
Groups, ie those functions which will transfer to the National Commissioning Board or to Local Authorities.
2.2.2 It is anticipated that the transition to these new arrangements should take place as soon as
possible and wherever possible, in line with the timings for the transition described in 2.1 above. The National Commissioning Board functions would transfer to NHS Greater Manchester, pending the establishment of the NCB.
2.2.3 Where the transition has not all taken place in parallel, responsibility for the residual functions will
temporarily be held by the Clinical Commissioning Group pending their transfer. This may be achieved by a variety of means including the retention of a locality based committee, reporting to the Clinical Commissioning Group
2.3 NHS Greater Manchester Assurance 2.3.1 Delivery of the above transition represents a significant change and assurance needs to be in
place that locality arrangements are robust. The development and signing off of the Accountability Agreement referred to in Section 2.1.2 represents a major element of this assurance process.
2.3.2 Assurance will also be required that the appropriate operational and financial clarity is in place
prior to formally splitting existing PCT functions into the respective Clinical Commissioning Group, Local Authority, NHS Commissioning Board and Commissioning Support Service elements. A pre-cursor to any such financial or operational transitions being made will be for the necessary arrangements to have been identified, agreed and signed off by all parties, including NHS Greater Manchester.
3 Commissioning Support Service (CSS) 3.1 The arrangements described in this paper are underpinned by a parallel requirement to develop a
Commissioning Support Service. A Commissioning Support Service has been defined as “the assistance which commissioners (both CCGs and the NHSCB) can draw on to help them deliver their functions” and will incorporate the delivery of a wide range of support services and functions.
3.2 Arrangements to develop a Greater Manchester Commissioning Support Service are well
advanced, with the following high level timeline in place:
• November 2011 – Development of high level specification
170

• February 2012 – Development of Outline Business Case
• September 2012 – Development of Full Business Case
• November 2012 onwards – mobilisation
3.3 In order to successfully deliver the milestones described in 3.2 above, the establishment of an arms length arrangement to manage the CSS has been proposed. This organisation would initially sit within NHS Greater Manchester, (pending transfer to the National Commissioning Board), but would sit at arms length with its own Board and management team. This management board would include lay (Non-Executive) representation. (A recent parallel was observed in PCTs with the operation of Provider Services Units at arms length from the Commissioning PCT, prior to the Transforming Community Services process).
4 Role of Locality Non-Executive Directors and Managing Directors 4.1 Role of Locality/ Associate Non-Executive Directors – The role of the locality Non-Executive
Directors has changed significantly since May 2011 and the arrangements set out in this paper have major implications for the role. For clarity, the timeline below sets out the key dates and changes:
4.1.1 May 2011 - NHS Greater Manchester established as the embodiment of the 10 Greater
Manchester PCTs. Board appointed. Existing Non-Executive Directors role amended to that of Associate Non-Executive Director, with accountability held by members of the NHS Greater Manchester Board. Board meetings of NHS Greater Manchester are therefore meetings of the Board of each of the ten Greater Manchester PCTs.
4.1.2 October 2011 to March 2012 - Clinical Commissioning Groups becoming accountable to NHS Greater Manchester, taking over role from Locality Boards. Within this model there is a requirement for two lay members to sit on the CCG Board. It is suggested that these could be drawn from the existing locality Non-Executive cohort for the period to April 2013.
4.1.3 Additionally, the Chairman is expecting correspondence from Kathryn Riddle, the chair of NHS
North of England to indicate that with the adoption of model 2 governance arrangement, there will be a review of the number of Non Executive Directors in the North of England region.
4.1.4 April 2012 onwards – Remaining Locality Non-Executives will either:
• Serve as the 2 lay members on shadow CCG Boards • Serve as non-executive members of shadow CSS Board • Support transition in localities via membership of residual committees and/ or
provision of specific coaching/ development support to CCGs • Input to the developing Health and Well Being Boards
4.1.5 April 2013 – PCTs disestablished 4.2 Role of Managing Directors – Managing Directors have been in place in each of the localities,
since the establishment of NHS Greater Manchester in May 2011. The transfer of responsibility
171

from the locality Board to the CCGs as described in this paper will require a number of further changes in localities, including to the role of the Managing Directors.
4.3 This paper describes a model where the senior officer within localities would be the
shadow/interim Chief Officer of the CCG. In this context, a number of options apply to the future role of existing Managing Directors, including:
• Becoming the shadow/interim Chief Officer of a Clinical Commissioning Group • Retiring from or assuming a different role within the service • In areas with more complex configurations, retention in supra-Locality MD role
5 Recommendations 5.1 It is recommended that:
• Accountability to NHS Greater Manchester should transfer from Locality Boards to Clinical Commissioning Groups no later than 31 March 2012
• That each Clinical Commissioning Group must sign off an Accountability Agreement with NHS Greater Manchester no later than 29 February 2012
• That transfer of functions to Local Authorities and NHS Greater Manchester, (pending the establishment of the National Commissioning Board) should, wherever possible, take place in parallel with the transfer of responsibilities to the Clinical Commissioning Groups. Where this is not possible, these residual functions would temporarily become the responsibility of the relevant Clinical Commissioning Group(s).
• An arms length arrangement is established to manage the development and mobilisation of the Commissioning Support Service.
• The changes to the role of the Managing Director are approved by the Board
• The Board notes the process to be outlined by NHS North of England in relation to changes in the roles of locality Non Executive Directors
Rob Bellingham Board Secretary November 2011
172

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 17 10 November 2011 REPORT OF:
Director of Finance
DATE OF PAPER:
21 October 2011
SUBJECT:
Audit and Integrated Governance Committee Report
IN CASE OF QUERY, PLEASE CONTACT
Claire Yarwood – 0161 212 4835
PURPOSE OF PAPER: This paper updates the Board on decisions made and risks identified at the first Audit and Integrated Governance Committee meeting held on 15 September 2011. The terms of reference for the Committee are presented for approval by the Board.
173

NHS Greater Manchester
Audit and Integrated Governance Committee Report
Executive Summary This paper updates the Board on decisions made and risks identified at the first Audit and Integrated Governance Committee meeting held on 15 September 2011. Future reports will append approved minutes. 1 Role of Audit Committee 1.1 As this was the first Audit Committee meeting of NHS Greater Manchester, the first part of the
meeting was focused on discussion on the role of the Audit Committee. Mr Tim Crowley from Mersey Internal Audit Agency (MIAA) provided an overview of first principles, general best practice, challenges facing the committee and the potential solutions to those challenges.
1.2 The discussion highlighted the need for Locality Audit Groups to understand what information is
needed by the Cluster Audit Committee to provide a good level of assurance. It was agreed that correspondence would be sent on behalf of Mr Ahmad to explicitly inform Local Audit Group Chairs of what is expected in terms of consistent mechanisms for reporting the required information.
1.3 Mr Ahmad asked colleagues from External Audit to consider the principles for talking with each
other about individual organisations. All agreed that confidence would be maintained at all times and that if required the opportunity to have a separate private meeting to convey concerns would be beneficial.
1.4 The committee agreed that External Auditors should attend every meeting, both sets of auditors
should attend the financial year end meeting and that a Internal Audit colleagues should provide a standardised integrated report to highlight any issues for every Audit Committee meeting.
2 Reports presented to the Audit Committee 2.1 Members had received the draft Terms of Reference of the Audit and Integrated Governance
Committee and the Locality Audit Groups for comment prior to the meeting. Members debated delegation of authority for signing off financial statements and timing of meetings associated with the year end process. There was recognition that Local Audit Groups must have an opportunity to discuss matters with their Locality Boards. Both Terms of Reference were approved.
2.2 Mrs Vermeulen introduced the Audit and Integrated Governance Committee/Locality Audit Group
Work Plans and informed members that by the next committee both plans will be dovetailed. Mrs Yarwood noted that duplication of performance reports must be avoided but all can be assured that scrutiny will be robust. Members approved the draft work plans and noted the dates of future meetings.
2.3 Locality Audit Group reports were reviewed by members. Members discussed the required
format for reporting of issues at the Local Audit Groups going forward and highlighted areas of
174

concern. The committee noted the contents of the reports and welcomed the link between the Local Audit Groups and the Cluster Audit Committee that External Auditors could provide. It was agreed that the minutes of Locality Audit Group meetings, along with an exceptions report should be presented to Locality Boards to provide assurance of matters considered. The Committee agreed that it should receive a short concise standardised report that provides a record of matters considered by each organisation. The reports must also provide assurance that any issues highlighted are being addressed within Localities.
2.4 Mrs Vermeulen presented summary reports from Localities on the progress against
implementation of audit recommendations. Members agreed that in future the detail and format of the reports should be maintained at Locality Audit Group level, with only red ratings linking to failure of management action being undertaken being reported to Audit Committee.
2.5 Mrs Vermeulen introduced the Locality Losses and Special Payments Registers for the four
months to 31 July 2011 for the committee’s approval. NHS Bury and NHS Trafford have incurred no losses or special payments in this period. Members approved the entries in the Registers.
3 Recommendation 3.1 The NHS Greater Manchester Board is asked to note the contents of this report.
3.2 The NHS Greater Manchester Board is asked to approve the terms of reference for the Audit and Integrated Governance Committee, as set out in Appendix One.
Mrs Claire Yarwood Director of Finance
175

176
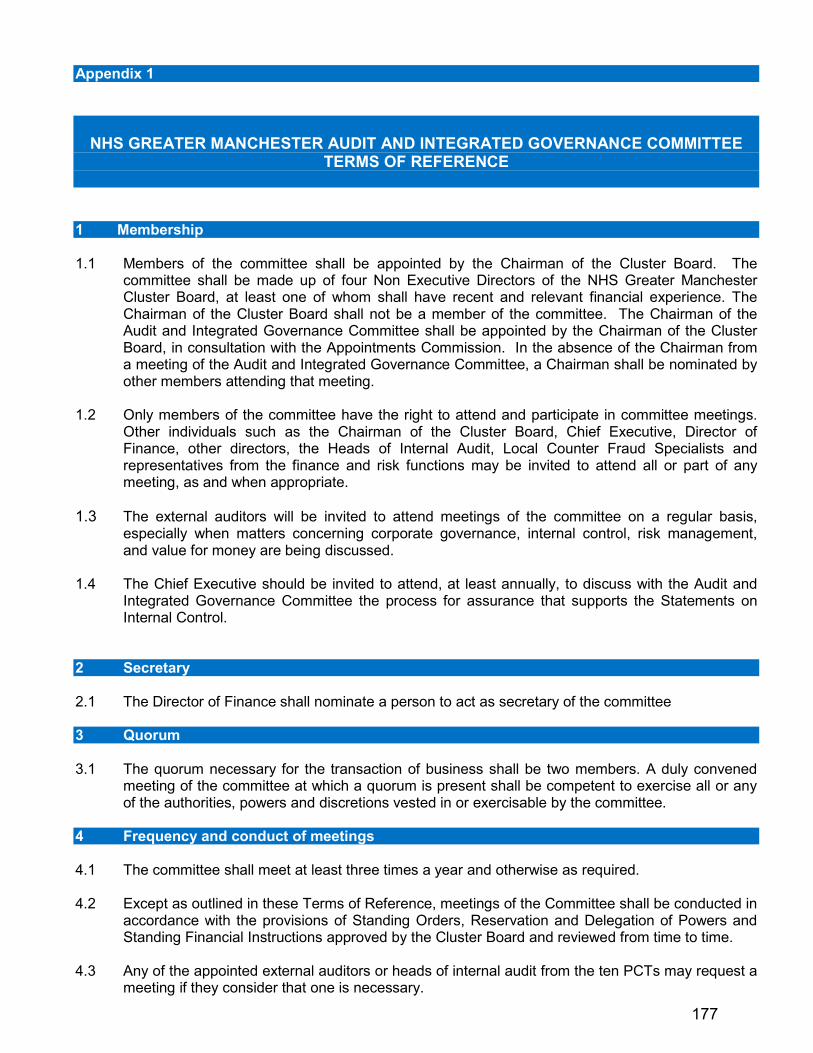
Appendix 1
NHS GREATER MANCHESTER AUDIT AND INTEGRATED GOVERNANCE COMMITTEE
TERMS OF REFERENCE
1 Membership 1.1 Members of the committee shall be appointed by the Chairman of the Cluster Board. The
committee shall be made up of four Non Executive Directors of the NHS Greater Manchester Cluster Board, at least one of whom shall have recent and relevant financial experience. The Chairman of the Cluster Board shall not be a member of the committee. The Chairman of the Audit and Integrated Governance Committee shall be appointed by the Chairman of the Cluster Board, in consultation with the Appointments Commission. In the absence of the Chairman from a meeting of the Audit and Integrated Governance Committee, a Chairman shall be nominated by other members attending that meeting.
1.2 Only members of the committee have the right to attend and participate in committee meetings.
Other individuals such as the Chairman of the Cluster Board, Chief Executive, Director of Finance, other directors, the Heads of Internal Audit, Local Counter Fraud Specialists and representatives from the finance and risk functions may be invited to attend all or part of any meeting, as and when appropriate.
1.3 The external auditors will be invited to attend meetings of the committee on a regular basis,
especially when matters concerning corporate governance, internal control, risk management, and value for money are being discussed.
1.4 The Chief Executive should be invited to attend, at least annually, to discuss with the Audit and
Integrated Governance Committee the process for assurance that supports the Statements on Internal Control.
2 Secretary 2.1 The Director of Finance shall nominate a person to act as secretary of the committee 3 Quorum 3.1 The quorum necessary for the transaction of business shall be two members. A duly convened
meeting of the committee at which a quorum is present shall be competent to exercise all or any of the authorities, powers and discretions vested in or exercisable by the committee.
4 Frequency and conduct of meetings 4.1 The committee shall meet at least three times a year and otherwise as required. 4.2 Except as outlined in these Terms of Reference, meetings of the Committee shall be conducted in
accordance with the provisions of Standing Orders, Reservation and Delegation of Powers and Standing Financial Instructions approved by the Cluster Board and reviewed from time to time.
4.3 Any of the appointed external auditors or heads of internal audit from the ten PCTs may request a
meeting if they consider that one is necessary.
177
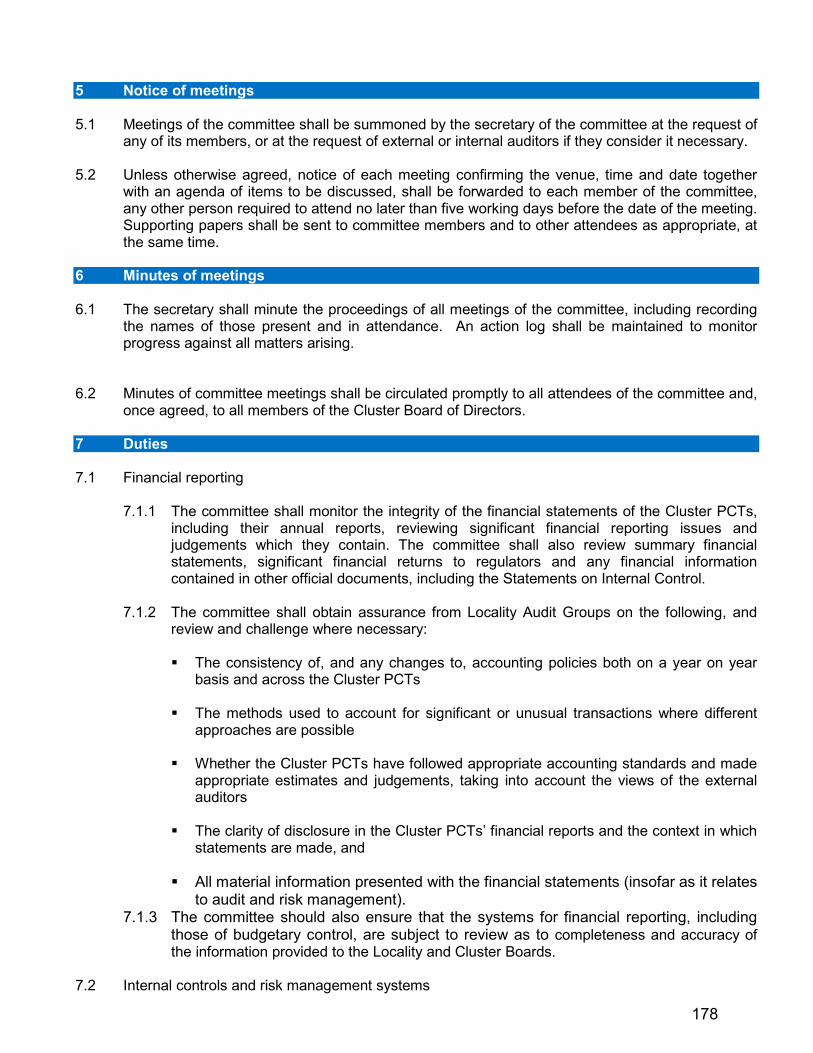
5 Notice of meetings 5.1 Meetings of the committee shall be summoned by the secretary of the committee at the request of
any of its members, or at the request of external or internal auditors if they consider it necessary. 5.2 Unless otherwise agreed, notice of each meeting confirming the venue, time and date together
with an agenda of items to be discussed, shall be forwarded to each member of the committee, any other person required to attend no later than five working days before the date of the meeting. Supporting papers shall be sent to committee members and to other attendees as appropriate, at the same time.
6 Minutes of meetings 6.1 The secretary shall minute the proceedings of all meetings of the committee, including recording
the names of those present and in attendance. An action log shall be maintained to monitor progress against all matters arising.
6.2 Minutes of committee meetings shall be circulated promptly to all attendees of the committee and,
once agreed, to all members of the Cluster Board of Directors. 7 Duties 7.1 Financial reporting
7.1.1 The committee shall monitor the integrity of the financial statements of the Cluster PCTs, including their annual reports, reviewing significant financial reporting issues and judgements which they contain. The committee shall also review summary financial statements, significant financial returns to regulators and any financial information contained in other official documents, including the Statements on Internal Control.
7.1.2 The committee shall obtain assurance from Locality Audit Groups on the following, and
review and challenge where necessary:
The consistency of, and any changes to, accounting policies both on a year on year basis and across the Cluster PCTs
The methods used to account for significant or unusual transactions where different
approaches are possible Whether the Cluster PCTs have followed appropriate accounting standards and made
appropriate estimates and judgements, taking into account the views of the external auditors
The clarity of disclosure in the Cluster PCTs’ financial reports and the context in which
statements are made, and All material information presented with the financial statements (insofar as it relates
to audit and risk management). 7.1.3 The committee should also ensure that the systems for financial reporting, including
those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Locality and Cluster Boards.
7.2 Internal controls and risk management systems
178

The committee shall review the implementation and ongoing quality of integrated governance, risk management and internal control, across the whole of the Cluster PCTs’ activities (both clinical and non-clinical), that supports the achievement of its objectives. In particular the committee shall:
7.2.1 Review the effectiveness of the Cluster PCTs’ internal controls, Cluster Board assurance
framework, integrated governance and risk management systems (the committee shall review the Cluster Corporate Risk Register at each of its meetings).
7.2.2 Review the adequacy of all risk and control related disclosure statements (in particular the
Statements on Internal Control), together with any reports from internal or external audit or other appropriate independent assurances, before making recommendations to the Cluster Board. The Audit and Integrated Governance Committee has the power to request individual PCTs to submit interim Statements on Internal Control at any point during the year, where it deems this necessary.
7.2.3 Approve the statements to be included in the annual report concerning internal controls
and risk management. 7.2.4 Review the underlying assurance processes that indicate the degree of the achievement
of corporate objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements.
7.2.5 Monitor the policies and procedures relating to counter-fraud and anti-corruption activities
as set out in the Secretary of State Directions and performed by NHS Protect. 7.2.6 Review the policies for ensuring compliance with relevant regulatory, legal and code of
conduct requirements. 7.2.7 Review compliance with relevant regulatory, legal and code of conduct requirements
including those listed in appendix one.
7.2.8 Review and approve instances where the Cluster PCTs’ Standing Orders and Standing Financial Instructions are waived and investigate those issues that present a risk to the internal control functions of the Cluster PCTs.
7.2.9 Review at least annually the Cluster Board’s register of gifts, hospitality and sponsorship,
and declaration of Cluster Board members’ interests. 7.2.10 Review Standing Orders and Standing Financial Instructions at least annually.
7.3 Internal audit
To monitor the effectiveness of the internal audit functions established by management, which meet mandatory NHS Internal Audit Standards and provide appropriate independent assurance to the Audit and Integrated Governance Committee, Chief Executive and Cluster Board, the committee shall:
7.3.1 Monitor and review the quality and effectiveness of the Cluster PCTs’ internal audit
function in the context of the Cluster PCTs’ overall risk management system as identified in the Cluster Board assurance framework.
7.3.2 Consider and approve the remit of the internal audit function and ensure it has adequate
resources and appropriate access to information to enable it to perform its function effectively and in accordance with the relevant professional standards. The committee
179

shall also ensure the function has adequate standing and is free from management or other restrictions.
7.3.3 Approve the appointment and removal of the heads of the internal audit function in the
cluster PCTs. 7.3.4 Review and assess the annual internal audit plans, ensuring these are consistent with the
audit needs of the organisations as identified in the Assurance Framework. 7.3.5 Ensure that all reports which provide limited or no assurance on the Cluster PCTs from the
internal auditors are evaluated promptly. 7.3.6 Assess and monitor management’s responsiveness to the findings and recommendations
of the internal auditors. 7.3.7 Meet the heads of internal audit at least once a year, without management being present,
to discuss their remit and any issues arising from the internal audits carried out. In addition, the heads of internal audit shall be given the right of direct access to the Chairman of the Cluster Board and to the committee.
7.4 Counter Fraud The committee shall ensure that there is effective review of the work of the Local Counter Fraud
Officers as set out by the Secretary of State Directions and as required by the Director of NHS Protect. This will be achieved by:
7.4.1 Approval of the appointment of Local Counter Fraud Officers either directly or through the
appointment of the internal audit services.
7.4.2 Review and approval of the Counter Fraud Policy, operational plans and detailed programme of work ensuring this is considered with the needs of the cluster PCTs.
7.4.3 Ensure that the Counter Fraud functions are adequately resourced and have appropriate
standing within the cluster PCTs.
7.4.4 Conduct of an annual review of the effectiveness of Local Counter Fraud work. 7.5 External audit
The committee shall:
7.5.1 Review the work and findings of the external auditor(s) appointed by the Audit Commission and consider the implications and management’s responses to their work.
7.5.2 Oversee the relationship with the external auditor(s) including (but not limited to):
Consideration of the appointment and performance of the external auditors and make recommendations to the Cluster Board, as far as the Audit Commission’s rules permit. External audit assessment will be undertaken by Locality Audit Groups and reported to the committee for review.
Discussion and agreement with the external auditors, before the audits commence, of
the nature and scope of the audits as set out in the annual plan, and ensure coordination, as appropriate, with other external auditors in the local health economy.
180

Discussion with the external auditors of their local evaluation of audit risks and
assessment of the Cluster PCTs and associated impact on the audit fees. Review all external audit reports, including agreement of the annual audit letter before
submission to the Cluster Board and any work carried outside the annual audit plan, together with the appropriateness of management responses.
7.5.3 The committee shall meet the external auditors at least once a year, without management
being present; to discuss their remit and any issues arising from the cluster PCT audits. 7.5.4 Ensure the cluster PCTs receive an effective service.
7.6 Assurance
7.6.1 The committee shall review the findings of other significant assurance functions, both internal and external, and make recommendations to the Cluster Board on matters affecting the governance of the Cluster PCTs. These will include, but not be limited to, any reviews by Department of Health arms length bodies or regulators/inspectors, or professional bodies with responsibility for the performance of staff or functions.
7.6.2 The committee will review the work of other committees of the Cluster Board or Cluster
PCTs, whose work can provide relevant assurance to the committee’s own scope of work. 7.6.3 The committee shall request and review reports and positive assurances from directors
and managers on the overall arrangements for governance, risk management and internal control, and may request specific reports from individual functions within the cluster PCTs as they may be appropriate to the overall arrangements.
7.6.4 The committee has oversight of the Locality Audit Groups in terms of consistency of
operation and performance. The Locality Audit Groups will be required to:
• Self assess their performance on an annual basis and report the results to the committee.
• Provide regular reports on their proceedings to ensure that the committee is notified of significant control issues and risks in a timely manner.
7.7 Annual report
7.7.1 The terms of reference of the Audit and Integrated Governance Committee, including its role and the authority delegated to it by the Cluster Board and its membership shall be made publicly available. A separate section of the cluster PCTs’ annual reports should describe the work of the committee in discharging those responsibilities.
7.7.2 Where an external auditor’s contract is terminated in disputed circumstances the removal
process and the underlying reasons for that action must be set out in the annual report. 7.8 Whistle-blowing
The committee shall review the Cluster PCTs’ arrangements for their employees to raise concerns, in confidence, about possible wrongdoing in financial reporting or other matters. The committee shall ensure that these arrangements allow proportionate and independent investigation of such matters and appropriate follow up action.
181

8 Reporting responsibilities
8.1 The committee will report to the Cluster Board annually on its work in support of the Statements on Internal Control, specifically commenting on the fitness for purpose of the Cluster Board assurance framework, the completeness and degree of integration of risk management in the organisation, and the holistic nature of governance arrangements.
8.2 The committee Chairman shall report formally to the Cluster Board on its proceedings after each meeting on all matters within its duties and responsibilities.
8.3 The committee shall make whatever recommendations to the Cluster Board it deems appropriate
on any area within its remit where action or improvement is needed. 8.4 The committee shall compile a report to the Cluster Board on its activities to be included in the
Cluster PCTs’ annual reports. This will include any recommendations by the committee that were not approved, and the reasons for their non-acceptance.
8.5 The Chairman of the committee shall write to the NHS Strategic Health Authority in those
instances where the services of the external auditor are terminated in disputed circumstances. 9 Other matters
The committee shall: 9.1 Have access to sufficient resources in order to carry out its duties, including access to the Cluster
secretariat for assistance as required. 9.2 Be provided with appropriate and timely training, both in the form of an induction programme for
new members and on an ongoing basis for all members. 9.3 Give due consideration to laws and regulations impacting on the work of the committee. 9.4 Be responsible for co-ordination of the internal and external auditors, and promote co-operation
between the groups of internal and external audit providers to provide an efficient and cost effective service for the ten PCTs.
9.5 Oversee any investigation of activities which are within its terms of reference and act as a court of
the last resort. 9.6 At least once a year, review its own performance and terms of reference to ensure it is operating
at maximum effectiveness and recommend any changes it considers necessary to the Cluster Board for approval.
10 Authority
The committee is a non executive committee of the Cluster Board and has no powers, other than those specifically delegated in these terms of reference. The committee is authorised:
10.1 To seek any information it requires from any employee of the Cluster PCTs in order to perform its
duties. 10.2 To obtain, at the Cluster PCTs’ expense, outside legal or other professional advice on any matter
within its terms of reference within a limit determined by the Director of Finance. 10.3 To call any employee to be questioned at a meeting of the committee as and when required.
182

APPENDIX ONE – CURRENT RELEVANT LEGISLATION • Civil Contingencies Act (Emergency Planning and Business Continuity) • Bribery Act 2010 • Health and Safety • Information Governance (including Data Protection, Confidentiality, Information Security etc) • NHS Act 2006 (Section 242 – Consultation, Engagement and Involvement and Health Overview and
Scrutiny Committee) • Human Rights Act, 1998, Race Relations Act, 2000 and Equality Act 2010 (Equality Impact
Assessments, Equality Diversity and Human Rights) • Employment law • Access to Health Records Act, 1990 • Freedom of Information Act, 2000 • Local Authority Social Services and NHS Complaints Regulations (England), 2009 • Procurement • Equality Act 2010
183

184

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 18 10 November 2011 REPORT OF:
Director of Finance
DATE OF PAPER:
31 October 2011
SUBJECT:
Annual Audit Letters
IN CASE OF QUERY, PLEASE CONTACT
Claire Yarwood 0161 212 4835
PURPOSE OF PAPER: The NHS Greater Manchester Board members are asked to note the Annual Audit Letters prepared by the external auditors of each of the ten Greater Manchester PCTs. Please note that these documents were circulated electronically to members by 31 October, in accordance with external audit requirements, and accordingly are not reprinted in these Board papers. The full documents will however be made available on PCTs’ websites.
185

186

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 19 10 November 2011 REPORT OF:
Chief Executive
DATE OF PAPER:
12 October 2011
SUBJECT:
Healthy Futures Report
IN CASE OF QUERY, PLEASE CONTACT
Mike Burrows 0161 212 4821
PURPOSE OF PAPER: The NHS Greater Manchester Board is asked to note the content of the report.
187
Healthy Futures Report
Executive Summary The purpose of this report is to provide an update around the further aspects of Healthy Futures consultation within the North East Sector of Greater Manchester. 1 Introduction 1.1 The purpose of this report is to update the Board on the progress which has been made in
preparation for the launch of the public consultation on the disposition of elective cardiology and stroke rehabilitation services within the North East Sector of Greater Manchester. The Joint Committee is a sub-committee of the Board of NHS Greater Manchester established to oversee the consultation process.
2 Background 2.1 The Board will be aware that the consultation is required following a review of the Healthy Futures
Programme as part of the Secretary of State’s national review of reconfiguration in 2010. As part of this review the National Clinical Assessment Team recommended a review of cardiology services across the North East sector. As a result the Strategic Health Authority commissioned a review of cardiology by Professor Sir Roger Boyle. His report recommended that specialist interventional cardiology services should be moved off the Rochdale Infirmary site and relocated to Fairfield General Hospital.
2.2 In addition it became clear to specialist stroke clinicians that the proposals in the 2006
consultation for patients who had suffered stroke, were post 48 hours and stable, to be transferred from the specialist stroke unit to inpatient beds at Rochdale Infirmary was no longer reflective of best practice and would not be compliant with the national stroke strategy.
2.3 The Joint Committee has met monthly since its first meeting in May and has followed the
requirements for consultation laid down in the North West Strategic Health Authority Service Reconfiguration Assurance Framework to guide its preparation for the consultation.
2.4 At the meeting of the Joint Committee held on the 21st September 2011 a number of key
decisions were made which moved the process to the next step. 3 Pre-consultation Engagement 3.1 The Committee received evidence of the pre-consultation engagement activity which had been
undertaken during August and the first part of September. The outcome of this work was incorporated into the business cases which were submitted for approval at the same meeting. The pre-consultation engagement findings were used to inform the public consultation document which was also submitted to the Committee for approval.
188
3.2 In total, 183 participants attended 15 focus groups with 20% identified as cardiology service users and 31% as stroke service users. Six members of the public responded via the internet survey, and one group representative responded via email. In addition presentations were made to the Joint Overview and Scrutiny Committee, Clinical Commissioning Groups, Locality PCT Boards, Local Authority officers and local MP’s.
3.3 A detailed paper is available describing this process is available from the Joint Committee
Secretariat. 4 Business Cases 4.1 Two Business Cases were considered at the meeting, one each for cardiology and stroke
rehabilitation. Both Business Cases were approved unanimously by the four voting members who were present at the meeting. The Business Cases were immediately submitted to the North West Strategic Health Authority for submission to their Board meeting on the 26th September 2011.
4.2 The Business Cases are available on request from the Joint Committee Secretariat. 5 Public Consultations 5.1 The final draft of the Public Consultation document was submitted to the Committee and
approved unanimously by the four voting members subject to minor typographical changes requested by communication leads in the North East Sector.
5.2 This to was submitted to the North West Strategic Health Authority Board meeting on the 26th
September 2011. 5.3 The consultation process commenced on the 17th October 2011 for a three month period. The
process itself is being monitored by an external stakeholder panel Chaired by Kathy Cowell. 6 North West Strategic Health Authority Board Meeting – 26th September 2011 6.1 The Strategic Health Authority Board approved the Business Cases and Consultation document
at this meeting. As this is the last stage of the pre-consultation assurance process approval was given for the public consultation to begin on the 17th October 2011.
6.2 Before the 17th October 2011 a series of stakeholder briefing events will be held. In addition a
formal press briefing will be held. The first week of the consultation is taken up with three public meetings in Bury, Rochdale and Oldham. Public meetings in Whitworth (for Rossendale) and North Manchester will be held soon after. A significant number of road shows, focus groups and other public and patient consultation meetings will be held during the three months of the consultation.
7 External Stakeholder Panel 7.1 The first meeting of the External Stakeholder Panel was held on the 30th September 2011 Chaired
by Kathy Cowell, Chair of NHS Cheshire, Warrington and Wirral. The Panel will be meeting monthly throughout the remainder of the consultation period in order to scrutinise consultation activity. Regular reports will be submitted to the Panel and panel members will be attending consultation events in order to ensure compliance with the assurance process. The Panel will feed back their observations to the Healthy Futures team and the Joint Committee. At the end of the consultation period the Chair will be required to write a report on the consultation process for the Joint Committee as part of the final decision making process.
189

7.2 The membership and terms of reference for the External Stakeholder Panel is available from the
Joint Committee Secretariat. Mike Burrows Chief Executive 12 October 2011
190

NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 20 10 November 2011 REPORT OF:
Medical Director
DATE OF PAPER:
20 October 2011
SUBJECT:
Clinical Commissioning Board
IN CASE OF QUERY, PLEASE CONTACT
Warren Heppolette 0161 212 4815
PURPOSE OF PAPER: To inform the NHS Greater Manchester Board of the recent Business of the Clinical Commissioning Board The NHS Greater Manchester Board is asked to note the content of the report.
191
Clinical Commissioning Board (CCB) Executive Summary The purpose of this paper is to inform the Board of the recent business of the Clinical Commissioning Board (CCB). The Board approved the establishment of the CCB at its September meeting and since then the CCB has met twice, initially to establish its membership and accept its terms of reference. The membership of the CCB now incorporates a clinical majority nominated by the Greater Manchester Clinical Commissioning Groups (CCGs). The CCB has immediately accepted and is leading the commissioning of collaboratively commissioned services, directing the work of the GM clinical networks, and providing a clear clinical ‘engine room’ for the work of NHS Greater Manchester in addition to the clinical leadership provided by CCGs on their own patch. 1 Purpose 1.1 This paper informs the NHS Greater Manchester Board of the business of its Clinical
Commissioning Board following its establishment in September. 2 Establishment of the Clinical Commissioning Board 2.1 The CCB adopted at its first meeting the proposed terms of reference for its operation which had
previously been supported by the Board of NHS Greater Manchester. 2.2 The CCB now incorporates a clinical majority drawn from the nominees of Greater Manchester’s
Clinical Commissioning Groups. The CCB is additionally supported by NHS Greater Manchester Executives and locality Directors with significant experience of collaborative and lead commissioning arrangements.
3 Business and Decisions 3.1 Atrial Fibrillation 3.1.1 The GM Clinical Commissioning Board received a verbal update outlining the current position in
relation to the introduction of the new oral anticoagulation therapies (NOACs), the first of which, dabigatran, has been licensed for stroke prevention in AF in August. A position statement has been agreed by both the GM Medicines Management Group and the GM Cardiac & Stroke Network.
3.1.1 The Board: (i) Confirmed in principle support for the interim position outlined prior to the finalisation of
NICE guidance.
192

(ii) Requested that the Statement be circulated for distribution to local leads to inform actions in localities.
(iii) Supported the withdrawal of co-operation at this stage to the industry launch event pending further discussion.
3.2 Collaborative Commissioning - Neurology 3.2.1 The CCB outlined the collaborative spend on neurology services across Greater Manchester
(GM) PCTS. The CCB investigated spend on neurology services at secondary and tertiary levels and highlighted the need for an integrated approach to commissioning of neurosciences services. The CCB also received an update on key aspects of joint work on pathway redesign, QIPP and service developments.
3.2.2 The Board: (i) Emphasised the need to develop a clear strategic commissioning framework for
neuroscience services. (ii) Agreed that the incorporation of Stockport to the work rolling out the headache
protocol be considered in the locality. (iii) Requested that Claire Yarwood be invited to review the intentions around the
neurology outpatient tariff to support an effective prioritisation of the proposal (iv) That a further paper on neuro-rehabilitiion be brought back presenting the service
specification and the timeline and issues for implementation (including commissioning and contracting; workforce; and provider engagement)
3.3 Vascular Services Review 3.3.1 The CCB received an update on the progress to date of the review of Vascular Surgery. The case
for change was outlined to the Board and referenced both the opportunities to ensure activity volumes at inpatient sites are co-ordinated to improve outcomes and the implications of GM being identified as 1 of 6 national screening early implementer sites for Abdominal Aortic Aneurysm (AAA) screening.
3.3.2 The clinical network recommended that the most suitable short term solution would be to have only three inpatient vascular centres. It was highlighted in the recommendations and options appraisal that although the three centre model could meet most of the required quality standards, it is not the ‘perfect’ solution and therefore a two centre model (one level four centre and one level three centre) should be pursued within agreed and well defined timescales.
3.3.3 The CCB considered the information in the presentation and supporting paperwork and highlighted a series of issues to guide the further commissioning aspects of the review. These included: • Assurance as to the robustness of the site selection or procurement process including the
rationale for not pursuing formal tender; • Engagement of GM PCT locality DOFs on the implications of the financial and activity
modelling contained in the Impact Assessment; • Assurance as to the robustness of the governance of the proposed Multi- Disciplinary Team
arrangements underpinning the ‘virtual level 4’ centre; and • Engagement with locality commissioners to ensure that trusts losing activity are planning to
withdraw vascular capacity appropriately. 3.4 Aortic Abdominal Aneurysm Screening Programme 3.4.1 The CCB received a paper outlining the recent review of the Programme to date including activity
and outcome data, patient experience findings and estimated funding requirements. In addition, related national screening policy and developments are outlined.
193

3.4.2 The CCB noted that the GM AAASP has been successfully rolled out to all GM PCTs. The uptake of screening in the completed cohort in the South Sector of GM is 73%. This is very positive and was achieved without proactive promotion of the service. Current uptake in the roll out PCTs is 44%, however this cohort is only partially completed and increases in attendance/uptake are expected. The detection rate of aneurysms is currently 2.8%; this is in line with national figures.
3.4.3 The CCB also noted the positive national feedback for the GM programme. The National Screening Committee has described GM AAA screening Programme as a model of best practice and the Public Health Network has been requested to support other regions to replicate the model.
3.4.4 The CCB was satisfied that the review data on uptake, detection, patient experience and outcomes indicated supported continuation of the programme as recommended by DPHs.
3.4.5 The CCB (i) Confirmed its ongoing support for the GM AAA Screening Programme until the anticipated
transfer of screening responsibilities to Public Health England in 2013. 3.5 Business Planning Round 2012/13 3.5.1 The CCB received a paper detailing the Cluster Assurance requirements for the 2012/13 business
planning process. The paper outlined the requirements for the process for 2012/13 and proposed the establishment of a time limited Contract Steering Group to ensure delivery of the key milestones in the timetable for delivering signed contracts.
3.5.2 The CCB: i. Approved the paper and the draft terms of reference for the GM Contract Steering Group. ii. Requested that consideration is given as to how to align workforce plans at the CCG/PCT
level with the process and then triangulate the localities plans across GM to understand the system-level impact.
iii. Acknowledged the importance of CCG involvement in the process proposed in the paper to manage collation and presentation of evidence towards CCG authorisation.
iv. Requested that quality requirements and CQUINs for inclusion in 12/13 contracts are developed through the Quality leads meeting (a sub-group of the Contract Steering Group) and that DPH and CCG quality representatives are invited.
v. Recognised that the GM Contract Steering Group will ensure consistency of contractual processes to be applied to 12/13 contracts, it will only hold responsibility for delivery of contractual process requirements for 12/13 for collaborative contracts and that localities remain responsible for the agreement of local commissioning intent and priorities to be included in 12/13 contracts.
3.6 Cervical Cytology Services 3.6.1 The CCB received an interim review of the Cervical Cytology Service, looking at previous
mobilisation issues; current performance and future developments.
3.6.2 The paper detailed a couple of issues that require consideration for development and implementation - electronic ordering and HPV testing. The Board:
(i) Received and noted the report. (ii) Supported the principle of the development of a single electronic ordering system to
include a consistent approach to electronic ordering, but requested that the Greater Manchester IM&T Review Board undertake a review of the implications of developing a single system in terms of workload and financial impact on GP practices for presentation to future Board to inform a decision on the way forward.
194
(iii) Noted the developments on HPV testing and that these will be progressed through the Greater Manchester DPH group.
(iv) Noted that the Quality Assurance visit planned for Pennine in October has been postponed until January 2012 and a report will come back to Board once visit and review is complete.
3.7 Patient Transport for GM CATS 3.7.1 The CCB received a verbal report on an emergent issue regarding the provider of patient
transport services for ISCATS. The current contract expired in March 2011 and was extended on a temporary basis. The current provider has indicated that they want to pull out of the Manchester operation and Board was asked to advise on the next steps.
3.7.2 CCB received 3 options: • Do nothing; • Award a 3 month contract and then tender for 12 months; • Award an 18 month contract and then align with the NW tender for PTS services planned
in 2012.
3.7.3 The CCB: (i) Requested that the current service specification is reviewed to see if it could be
aligned to the specification for general PTS (ii) Invite NWAS and non NHS providers to bid for an interim contract to deliver PTS to
Care UK. This interim contract would run up to 18 months until 31/3/2013. The procurement route would be done through a mini completion process, in line with GM Cluster SFIs
(iii) Include PTS for ISCATS in the North West procurement exercise on PTS which will be undertaken in 2012/13.
3.8 Collaborative Commissioning 3.8.1 The CCB received the monthly lead commissioner report for the collaboratively contracted
services of The Christie, district/tertiary cardiac, NWAS, neurology, stroke and cervical cytology.
3.8.2 A draft summary paper was presented in the meeting to assist with the management of the contents of the report by exception and this outlined any significant in-month or forecasted over or under performance, QIPP and CQUIN plans and progress towards achievement.
3.8.3 The CCB: (i) Noted the month 4 report and the draft summary paper and approved the summary sheet
for inclusion in future reports. (ii) Noted its concern at the gaps in information regarding QIPP and CQUIN plans and
updates and requested that lead commissioners routinely provide this information. (iii) Requested that clinical risk profiles are included into the QIPP plans for these services to
ensure that whilst savings are being delivered, that the services remain safe and sustainable to deliver the required patient outcomes.
3.9 Hepatitis C Programme 3.9.1 The CCB received a paper with the proposed clinical service specification for Hepatitis C for
Board approval to be included in contract intentions for 12/13 with the 4 main providers (CMFT, PAHT, WWL and UHSM). The specification has been developed in conjunction with NHS HMR and has been subject to numerous consultations with Directors of Commissioning and there was a final clinical meeting to sign off the specification.
3.9.2 The Board
195

(i) Approved the sign off of this phase of the project to agree the service specification in 12/13 contracts.
(ii) Approved the next stage for the project to return to Board in 2012 with activity data to inform the contact activity levels for 13/14.
(iii) Requested that additional work is undertaken to understand the health economic impact of screening the undiagnosed for Hepatitis C across Greater Manchester to ensure treat the appropriate cohort of patients where an activity cap is put in place through the contracts. Board acknowledged that this work should be considered in the context of QIPP and other treatment priorities.
(iv) Recognised the value in future work to review tariffs for hepatitis C services. 3.10 Improving Outcomes Guidance - Urological Cancer Services
3.10.1 The CCB received a paper updating on the current position with urological cancer services, and
the need to procure a service which meets national Urology Improving Outcomes Guidance (IOG) and national cancer quality measures for one part of the Greater Manchester conurbation.
3.10.2 The CCB was asked to recommend that the GM PCT Cluster proceeds with procurement of a single urology cancer specialist MDT operating at either one or two surgical sites, covering a population of at least 1 million. Specifically the SMDT is to cover the populations of Ashton, Wigan and Leigh, Bolton, Salford, South Manchester and Trafford.
3.10.3 The Board (v) Endorsed the approach described to secure an IOG compliant model through a
managed escalation process to procurement. (vi) Acknowledged discussions that were currently in progress with providers to confirm
the necessity for a procurement stage. (vii) Confirmed that the November Board would receive and consider a timeline for
procurement (01/11/11) in the event that provider discussions are not productive. 3.11 Specialised Commissioning 3.11.1 The CCB received a briefing from the North West Specialist Commissioning Group.
3.11.2 The CCB noted potential impact on the North West of the outcome of the national paediatric
cardiac surgery review, the national procurement of ECMO (Extra corporeal membrane oxygenation) beds and the pilot stock take undertaken by Ernst and Young at NWSCT and some other PCTs to map the future location for contracting functions from 2013.
3.11.3 The CCB (i) Requested an issues briefing on the outcomes of the Ernst and Young stock take to be
provided jointly by Jon Develing, Claire Yarwood and Kate Ardern. (ii) Briefing to be considered by the GM GP Council on the future migration path of
specialist services and the reset of national definition set and approach to top slicing of CCGs for services in the new definition set to be sighted on at relevant level.
3.12 Sequential biologics in the treatment of plaque psoriasis 3.12.1 The CCB received a refresh to the paper that was presented to the Commissioning Programme
Board in July. The Commissioning Programme Board did not support the adoption of an algorithm for the switching of biologics in the treatment of plaque psoriasis, as Board were not clear on the costs and the costs effectiveness of agreeing a formal switching policy across GM assessment of the affordability of the proposal for the different localities, as well as consideration of the broader implications for GMMMG and Individual Funding Request arrangements
3.12.2 The CCB
196

(i) Endorsed the recommendation of the new therapies sub group of GMMMG (GM Medicines Management Group).
The group recommends that a second or third biological therapy may be tried after a first has failed. It is recommended that patients are treated according to the Salford Royal NHS Foundation Trust algorithm for patients requiring biological therapy and should fulfil the NICE criteria for initiation and continuing therapy (ii) Recommended the future role and governance of the GMMMG was considered and
options presented back to Board for approval. 4. Recommendation 4.1 The NHS Greater Manchester Board is asked to note the content of the report. Dr Raj Patel Medical Director
197

198
NHS GREATER MANCHESTER BOARD MEETING AGENDA ITEM NO 21 10 November 2011 REPORT OF:
Director of Finance
DATE OF PAPER:
10 November 2011
SUBJECT:
Locality Board Summary Documents
IN CASE OF QUERY, PLEASE CONTACT
Claire Yarwood: 0161 212 4835
PURPOSE OF PAPER: Attached are a series of Locality Board Summary documents, covering the following Locality Board meetings: NHS Ashton, Wigan and Leigh – 24th August 2011 & 28th September 2011 NHS Bolton – 28th September 2011 NHS Bury – 21st September 2011 & 11th October 2011 NHS Heywood Middleton and Rochdale – 28th September 2011 NHS Manchester – 7th September 2011 NHS Oldham – 1st September 2011 & 6th October 2011 NHS Salford – 28th September 2011 NHS Stockport – 29th September 2011 NHS Tameside and Glossop - 7th September 2011 & 5th October 2011 NHS Trafford – 27th September 2011 & 25th October 2011 The NHS Greater Manchester Board is asked to note the content of the reports.
199

Locality Board Summary Document NHS Ashton, Leigh and Wigan Meeting Date: 24TH August 2011 Chaired by: Alan Stephenson Part I – Public Section Subject
Summary Actions
Draft Annual Report Draft annual report was presented to the Board. Approved subject to the amendments that had been supplied by Maurice Smith and Frank Costello.
Finance Report The Finance Director provided a report on the current position. At present the situation is stable with the PCT being on target to meet its planned surplus of £2.7m with an £871k surplus at month 4. These figures include QIPP requirements. The main pressure area is out of area contracts. The Board discussed how the cluster may get involved to get a degree of standardisation across the Greater Manchester area for Out of Hours. The Chief Operating Officer briefed the meeting on the sale of Grasmere Street. The Chief Operating Officer also advised the meeting that the dilapidation costs for Bryan House were in the plan with recurrent savings of c£250k following the move to the Life Centre. Financially the PCT is in a good position but still highly dependent on the achievement of QIPP targets. The 2% lodgement from the SHA has been returned; the
Agreed to raise degree of standardisation for Out of Hours at GM contract meeting next week. The Finance report was agreed.
200

spend will be monitored by the SHA.
Performance Report The Assistant Director of Finance took the meeting through the report. Of the 10 targets, 7 are green and 3 are red. MRSA is Red due to 2 breaches in the last period which have had a significant effect on the figures. C Diff is similar with 32 occurrences to date which is 9 above target; the PCT will not be able to achieve this target. It was confirmed that these are not all from a common source but from across the community. Antibiotic prescribing is a key aspect in the management of this area.
Board agreed the report.
Public Health Work is taking place linked to healthy lives and the legal changes which are part of the NHS transformation. The local public health work was linked to the LA and the cluster and response to the developments at national level. A public health engagement group has been formed to coordinate the input into this process. Wigan is the host for the GM public health network; the PCT Managing Director is the chair.
Board agreed the report.
Governance Local arrangements are being developed which show an increasing role for the 2 CCGs during transition. The structure proposed has a revised committee structure and link with the cluster. It shows how assurance will be provided in the transition. The authorisation process is being developed nationally and more details will become available. A report will be submitted to NHS Greater Manchester to provide further information on the next steps. It was confirmed that PEC members would leave at the end of September and that the Director of Public Health would be an additional member on the Residual Functions group.
Further discussion required with the 2 CCGs WB and ULC to support further development on their constitution and governance support structures.
Recommendations The NHS Greater Manchester Board is asked to: Note the above Locality Board summary
201

Locality Board Summary Document NHS Ashton, Leigh and Wigan Meeting Date: 28TH September 2011 Chaired by: Alan Stephenson Part I – Public Section Subject
Summary Actions
Information Governance The Chair said he had asked for this report following discussions at the Cluster Board as ALW was one of the 7 GM cluster PCT’s who were classified as requiring further improvement despite achieving the target of 70%. A discussion took place and an action plan has been put in place to deals with the issues. In future all submissions will go to the cluster where they will be correlated for final submission. The individual returns will be subject to audit. The CCG’s will be required to comply with the IG requirements and therefore complete the IG toolkit.
Action plan to be monitored by Management Group with report to Locality Board
Finance Finance headline indicators are green in all areas except QIPP and capital which are currently amber. The annual surplus is predicted at £2.7M and at month 5 the current surplus is £1.5M. The key messages are:
NHSALW QIPP It is essential that the QIPP savings for the PCT as identified are achieved and this is subject to regular review by the Executive team. We have currently achieved £5M of the £12M budget requirement
The main areas that need added attention are GPCC re-
QIPP plans to be standard item on Board and Exec agendas Out of area spend to continue to be actively monitored
202
design and Primary Care. Concern was raised about the reporting of stoke at Amber. It was explained that whilst it was achieving the savings it was not meeting the project milestones due to contractual challenges. Out of Area Acute The overspend in this area is beginning to stabilise but there is a risk around collaborative contracts.
Capital There is a resource of £616k but there may be more due to the property sales. The situation with Bridgewater Community Healthcare has been clarified with transfers and sales being agreed. It was confirmed that Grasmere Street surgery will be disposed of.
Stroke Care Commissioning Plan
This is a joint report with WWL and advised the board on the proposed actions in this area. This report shows variable performance against the set targets and WWL recognise that this is an issue to be addressed.
Meetings to continue with input from the CCG’s being taken into account
Vascular Review This is a GM review with feedback going to Salford PCT. Suitable sites have been identifies across GM. It was noted that Wigan was part of the Lancs. and Cumbria review
The meeting agreed that there needed to be further input to ensure the needs of the Wigan population were met.
Neuro Rehab Service The Locality Director of Commissioning took the meeting through the report which had been approved by the GM Commissioning Board with NHS Salford being the lead organisation. A discussion took place on relocating the unit at Leigh whilst the development work takes place on the infirmary site
The meeting agreed the proposal needs further examination to ensure that the provider makes decisions that meet the needs of the local population.
Recommendations The NHS Greater Manchester Board is asked to: Note the above Locality Board summary
203

Locality Board Summary Document NHS Bolton: 28th September 2011 Chaired by: Pam Senior Subject Summary Action
NHS Bolton Estate Strategy Review
Four work streams to address local estates issues :
- Hold and review Building Better Health for Bolton and establish a revised strategy group for a 12 month period
- Undertake estates utilisation review - Review outline business case for next
tranche - Stocktake of current HQ estate
The Locality Board noted the report agreeing to the recommendations aligned to the four work streams
Finance report The PCT’s revenue position as at the end of September 2001 shows a year to date surplus of £382k and a break even position for capital. The PCT is expecting to deliver against key statutory duties and financial performance indicators. The PCT is forecasting to deliver 1% reported surplus of £5m and a 2% recurrent surplus of £10m. For the year end 2011/12 the PCT is forecasting a break even position for revenue and capital expenditure. Significant risks highlighted within the position are as follows:
• Secondary care - £2.1m over spend in respect of over performance in NHS contracts and high costs drugs
The Locality Board:
• recognised the risks in relation secondary care, prescribing and continuing care and await further progress updates at the next meeting
• noted the revenue position and forecast break even position
204

• Specialist Commissioning – Overall for the North West £300k under spend but details for individual PCTs still awaited
• GM Collaborative Commissioning – Underspend of £1,158k
• Continuing Care – Overspend of £994k due to increased volume of patients meeting the criteria
• Prescribing – Overspend of £598k based on PPA data as at month 5
• Financial Recovery – Overall financial gap of £9.3m, of which the PCT is forecasting to achieve £6.7m. The gap of £2.6m will be delivered non recurrently
• Capital – Opening CRL was £16.1m and the PCT has identified surplus of £1.75m and is expected to be adjusted by the SHA
Performance report
Reported performance against the indicators highlighting exceptions
- 18 weeks – admitted remains a real problem to the health economy. Bolton NHS Foundation Trust are on weekly updates to both Cluster and SHA. Joint working to review action plan and consider additional non recurrent funding outside of the contract
- A&E – August/September showing signs of improvement
- 62 day cancer referral to treatment – local action plan developed for tracking individual patients
- VTE – remains an area for concern.
Members noted the report and expressed their real concern in relation to the poor performance of Bolton NHS Foundation Trust Members requested that all contract penalties were fully implemented
205

Requested action plan from Trust. Trust have appointed a fixed term VTE nurse specialist to work towards embedding the changes
Human Resources Performance Report
The dashboard reported against Quarter 1 performance indicators in relation to staff costs, staff composition, equality and diversity and development Members were informed of a change in personnel staff due to the recent integration and Alex Prescott, HR Business Manager will produce and present future reports
Members noted the report
Bolton Hospice Quality Account
Margaret Evans, Chief Executive at Bolton Hospice presented the Quality Account highlighting how the Hospice are performing and were any improvements are required against patient safety, clinical effectiveness, audit and quality and complaints and outlined the priorities for 2011-12. The Hospice intends to continue to ensure that quality is at the centre of everything they do, systems and processes are in place to maintain the highest possible standards and utilise both positive and negative feedback on all aspects of service provision.
Members noted the update
Quality and Safety Report
The report summarised how clinical quality is monitored by NHS Bolton and provides additional information on patient safety and elements of clinical quality:
- Hospital electronic discharge summaries communicated to GP practices
- CQC inspection of care home
Members noted the report Members requested that Mike write to BMI informing them that the Locality Board would be delighted to invite them or received a copy of the Quality Account at the next formal meeting in November
206

- SUI – bowel screening - Readmission rate reduction - Care maps prioritisation and development
of pathways - Repeat prescribing work
Mike Robinson informed members that the PCT had not as yet received a copy of BMI Healthcare Quality Account.
Cluster update
Update on the ‘Big Conversation’ listening event which had a clear intent to develop and keep contact with PCTs and CCGs
Members noted the update
Consortia update
Bolton Health Consortium and Bolton Collaborative Consortium – Position Statement on Gateway One The report detail the current position against the draft guidance for authorisation acknowledging that a single CCG for Bolton is the best way forward
- Recognition of how the PCT have engaged with primary care and the achievements
- Both consortia continue to work collaboratively
- Negotiations to take place in respect of a merger of the two consortia
-
Members noted the reports and were very keen that Gateway is met and authorisation process is achieved and welcome further negotiations in respect of a single CCG establishment
Complaints Policy and Procedure
In line with NHS Complaints Regulation the complaints and policy and procedure is reviewed and updated on an annual basis. There is no change in the way that NHS Bolton
The Locality Board approved the revised Policy
207

handle complaints, however, the policy has been amended to reflect changes following the transfer of services to the integrated provider and recent changes in roles and responsibilities within NHS Bolton
Minutes of meetings
The Board received minutes from recent meetings for information
The Minutes of the meetings were noted
Recommendation The NHS Greater Manchester Board is asked to:
• Note the above locality Board summary Pam Senior Chair NHS Bolton
208

NHS Bury Locality Board Summary Document NHS Bury: 21st September 2011 Chaired by: Paul Horrocks Subject Summary Action
Locality Directors Report
Detailed update and discussion on Organisational Change including:
• Confirmation of North East Manchester “sub-cluster” management arrangements
• Confirmation of the appointment of Dr Kiran Patel as Chair of the Bury Clinical Commissioning Group
• Update on the work and priorities of the Bury Health and Well Being Board
• Confirmation of the work being done relating to the transition of Public Health to the Local Authority and plans to bring a detailed proposal to the October Locality Board
Proposal for next phase of the “Care About the Cost” programme with the focus to be on flu immunisation, including via the development of a series of hard hitting public messages. Update on the Healthy Futures programme and progress towards public consultation on the next phase.
The Locality Board received the report and approved the next phase of the Care About the Cost programme.
NHS Greater Manchester Update
A detailed update was provided on the outcomes of the NHS Greater Manchester Board meeting which took place on 8th September.
The Locality Board received and noted the NHS Greater Manchester update.
Finance Report (including Financial Recovery Update
The PCT showed a slight surplus within revenue position for period to end of July 2011 and a break even capital position A breakeven position for 2011/12 is being forecast from a revenue and capital perspective, with the revenue position adjusted for an agreed additional financial allocation within the current financial year.
The Locality Board:
• Recognised the risks attached to the revenue position, therefore requiring the delivery of agreed savings targets in all areas in order to achieve financial balance in
209
Significant risk noted in sustaining the position, with particular risks highlighted as follows:
• Secondary care - £3.538m overspend • Specialist commissioning – Additional pressures anticipated but more
detailed activity data awaited to allow assessment of the precise implications
• Continuing care – Overspend of £0.84m to month 4. External support has been sourced to assist in this area with a recovery plan being developed and expected to be in place by month 6.
• Financial Recovery – Actions taken to date have reduced the monthly run rate deficit by £0.4m. Overall financial gap of £25.62m identified to in Financial Plan. Addressing this gap in full would provide a 1% surplus in the current financial year and a 3% surplus recurrently.
• Capital – NHS Bury plan received SHA approval with a breakeven position forecast.
2011/12. • Noted the specific risks identified in
the report, particularly those relating to Secondary Care and Continuing Care, requiring further detailed updates and assurances relating to progress at the next Locality Board meeting in October.
• Noted the breakeven capital position
Clinical Commissioning Group Development
Dr Kiran Patel, the Clinical Commissioning Group Chair, provided a detailed update on the Bury CCG development programme. The update incorporated:
• The process to appoint clinical members of the CCG • The next steps in the process towards authorisation
The Locality Board • Received and noted the report
Integrated Performance Report
The paper presented a thematic, risk based summary of performance issues, highlighting those areas with a risk score greater than or equal to 15. Particular focus was given to the following areas:
• 18-week referral to treatment – It was reported that Pennine Acute Hospitals were scheduled to deliver a return to national performance standards by 23rd September
• A&E – Performance issues being experienced with regard to the 95% standard, particularly in Oldham and North Manchester
• Cancer 62-day wait – Performance issues identified and required significant future focus
• Alcohol – A detailed discussion took place on the plans to deliver improvements with regard to alcohol related deaths in Bury and other alcohol related issues.
The Locality Board:
• Received the action plans described to manage risks, requiring updates on delivery at future meetings and mandating the required levels of improvement set out in the plans
210
Safeguarding Children and Adults at Risk
A paper was presented, designed to provide the Board with assurances that the organisation is undertaking its Statutory Safeguarding responsibilities as outlined in Working Together to Safeguarding Children (2010) in respect of multi agency working to safeguard children and adults at risk. The paper summarised the Annual Reports for both Safeguarding Adults and Children.
The Locality Board: • Accepted the report as
assurance of evidence of NHS Bury’s contribution to the wider safeguarding agenda in Bury.
• Agreed that a more detailed update should be provided to a future meeting of the Quality and Risk Committee.
Minutes of formal meetings
The Board received minutes from the Quality and Risk Committee held on 7th June for ratification. Items considered included
• Update on the development of the Corporate Assurance Framework and Risk Register
• Quality Update – including an update on the Quality Accounts for Pennine Acute Hospitals and Pennine Care Foundation Trust
• Equality and Diversity – An update on the EPIT process • Legacy Document – Process to develop the NHS Bury Legacy
Document • Patient Experience report – Report covered quarter 4 of 2010/11 and
included details of the complaints and PALS activity during the quarter, and engagement activity
• Volunteer policy – Approval of this policy • Receipt and approval of Risk Annual Report 2010/11 and workplan
2011/12 • Feedback from a quality meeting held with Pennine Acute Hospitals
Trust • Freedom of Information – received the quarter 4 report
The Locality Board • ratified the minutes of the Quality
and Risk Committee 7th June 2011
211

NHS Bury: 11th October 2011 Chaired by: Paul Horrocks Subject Summary Action
Locality Directors Report
Detailed update and discussion on Organisational Change including:
• Plans to recruit to four key Clinical Commissioning Group management posts as soon as possible
• Plans for CCGs to become directly accountable to the NHS Greater Manchester Board, (recognising implications for Locality Boards)
• Proposals for CCGs to become owners of NHS “Local” branding and confirmation of support to this approach from CCG Chair.
• Confirmation of the functional review of staff required for CCGs and the default position of assignment to NHS Greater Manchester
• References made to key clinical appointments to the CCG and progress re the Public Health Transition, (both of which were substantive items elsewhere on the agenda)
The Locality Board received the report, recognising the milestones set out in the update and requiring monthly updates on progress against plan.
Finance Report (including Financial Recovery Update
The PCT showed a slight surplus within revenue position for period to end of August 2011 and a break even capital position A breakeven position for 2011/12 is being forecast from a revenue and capital perspective, with the revenue position adjusted for an agreed additional financial allocation within the current financial year. Progress towards financial recovery continues positively with the recurrent monthly run-rate within the range of breakeven to £0.19 deficit, representing a significant improvement from the £0.6m per month deficit at the start of the financial year and a £1.3m per month deficit as at September 2010. Significant risk noted in sustaining the position, with particular risks highlighted as follows:
• Secondary care - £3.93m overspend with overspend relating to NHS Trusts totalling £3.02m
The Locality Board:
• Recognised the risks attached to the revenue position, therefore requiring the delivery of agreed savings targets in all areas in order to achieve financial balance in 2011/12.
• Noted the specific risks identified in the report, particularly those relating to Secondary Care and Continuing Care, requiring further detailed updates and assurances relating to progress at the next
212

• Specialist commissioning – Noted that overall breakeven is focussed for the North West but detail relating to individual PCTs is still awaited
• Continuing care – Overspend of £0.91m to month 5, although rate of increase is reducing. External support has been sourced to assist in this area with a recovery plan being developed.
• Financial Recovery – Overall financial gap of £25.62m identified to in Financial Plan. Addressing this gap in full would provide a 1% surplus in the current financial year and a 3% surplus recurrently.
• Capital – NHS Bury plan received SHA approval with a breakeven position forecast. Plan adjusted to take into account additional wheel chair and appliance costs. Completion achieved on sale of Talbot Grove site.
Locality Board meeting in November.
• Noted the breakeven capital position and associated actions taken.
Clinical Commissioning Group Development
Dr Kiran Patel, the Clinical Commissioning Group Chair, confirmed three clinical appointments to the CCG and plans to recruit an additional clinical member. Noted that four senior management posts to be filled on an interim basis, (subject to NHS Greater Manchester approval), as follows:
• Chief Operating Officer • Director of Finance • Head of Commissioning • Head of Operations and Engagement
(proposal for the Director of Finance post to be shared across North East Sector CCGs) Interim Non-Executive/ Lay member arrangements to be determined during October to allow the Shadow CCG Board to be established by 1 November. Appointment of Hospital Doctor, nurse and patient champion to be considered on receipt of further guidance from the Department of Health. Existing Locality Board Committees, ie Quality and Risk and Locality Audit
The Locality Board • Approved the proposals set out in
the report as described in this summary document
213

Group will continue pending further detailed review of future CCG requirements. Proposal for the CCG to report to the Locality Board from November, with the agreement to handover reporting to NHS Greater Manchester from the Locality Board to the CCG no later than 1 April 2012. Confirmation of the CCGs intent and plans to fully engage in the 2012/13 contracting round. Discussion and agreement that as part of the handover process, the CCG will need to establish robust arrangements to consider:
• Management of Quality and Safety • Performance • Finance
Public Health Transition
The paper set out a proposal for the transfer of the Public Health Function from NHS Bury to Bury Metropolitan Borough Council. (The same paper was to be considered by the Council Executive at its meeting on the 12th October). The paper outlined:
• The scope of the functions to be transferred, (subject to further national policy guidance)
• The employees to be aligned to the Local Authority in the transitional phase
• The plans to incorporate the Public Health function into the Local Authorities’ organisational structure
• Issues to be addressed in the context of the emerging policy guidance and the continuing transition process
The Locality Board:
• Approved the content of the paper, agreeing that the proposed transition arrangements should take place from 1 November
• Agreed that the Public Health team’s office base would move to Knowsley Place in Bury, (council facility)
• Gave delegated authority to the Managing Director and the CCG Chair to sign of the Memorandum of Understanding, (a document providing more detailed terms of agreement)
• Agreed that the overall transition
214

arrangements should be reviewed prior to April 2013
Integrated Performance Report
The paper presented a thematic, risk based summary of performance issues, highlighting those areas with a risk score greater than or equal to 15. Particular focus was given to the following areas:
• 18-week referral to treatment – Noted improved 18-week performance at Pennine Acute Hospitals but highlighted issues still in Orthopaedics and the need to focus on sustained delivery of the improved performance levels
• A&E – Issues still remain with regard to the 95% standard, particularly in Oldham and North Manchester and significant risk of non-achievement of this standard for 2011/12
• Cancer 62-day wait – Recovery plan in place and being managed using similar process to that used to oversee the 18-week recovery plan
Discussion also took place with regard to achievement of vaccination and immunisation targets, specifically plans to improve the uptake for school leaver’s immunisation.
The Locality Board:
• Received the performance report and in the light of the risks described, required a further detailed progress update on the three key issues described in this summary at the next meeting and each meeting thereafter until required performance levels have been achieved.
Board Secretaries Report
This paper provided updates on the following aspects of corporate governance:
• Performers List Management –additions and removals from medical list, dental list and Ophthalmic list
• Application of the Common Seal – no applications to report this month
• Compliance with Pharmaceutical Regulations – no pharmacy applications to report this month
The Locality Board:
• Noted changes to the Performers List
Minutes of formal meetings
The Board received minutes from recent committee meetings for ratification. Commissioning Board
The Locality Board • ratified the minutes of the
Commissioning Board (PEC) 3rd August 2011
215

Items considered included:
• Consideration of business cases for stroke rehabilitation at Rochdale and Cardiology services in the North East Sector, (both forming part of proposed future Healthy Futures consultation). This was in line with the resolution made at the July NHS Greater Manchester Board meeting and with the agreement of the Bury CCG Development Team.
• List inflation project report • Midwifery Led Unit update – confirming support of the NHS Bury
Locality Board recommendation • Update on North East Sector Effective Use of Resources process
Quality and Risk Committee Items considered included
• Corporate Assurance Framework and Risk Register Update • Quality Update – including confirmation of projected achievement of
MRSA target and discussions with regard to controlled drug incidents • Annual Audit Letter – 2009/ 10 – Confirmation of quality related actions
being addressed • Equality and Diversity – Noted NHS Bury’s improved EPIT
performance and requirements to migrate to the Equality Delivery System during 2011. Agreed the content of an Equality Charter for Bury
• Patient Experience report – Report covered quarter 1 of 2011/12 and included details of the approach to the management of patient experience in providers, patient engagement activity in the period, complaints and freedom of information activity
• Legacy Document – current version considered and noted that the document would be subject to ongoing development and review
• ratified the minutes of the Quality and Risk Committee 25th August 2011
216

NHS Heywood, Middleton and Rochdale Locality Board Summary Document NHS HMR: 28th September 2011 Chaired by: David Edwards Subject Summary Action
Governance Updates received on : • Register of Interests • Use of the Corporate Seal
• Performers list update
• Locality Governance Framework
• Transfer of Premises to Pennine Care
Contents noted. The Locality Board agreed to approve the use of corporate seal for:
• Counterpart Deed of Surrender relating to Dr I K Babar, Dr S K Morijawala and Dr K Mahmood at Croft Shifa Health Centre
• Underlease plus agreement for an additional room at GP Surgery premises for Dr I K Babar, Dr S K Morijawala and Dr K Mahmood at Croft Shifa Health Centre.
The full Performers List was reviewed due to the number of significant changes. The Locality Board agreed to note the content of the report. The Locality Board received an update. Discussions took place around the delegation of funding to the Best Value Service Review Panel. The Locality Board agreed to note the content of the report and approved the Locality Scheme of Delegation. Subject to final revision. The Locality Board reviewed the paper following guidance from the Department of Health.
217
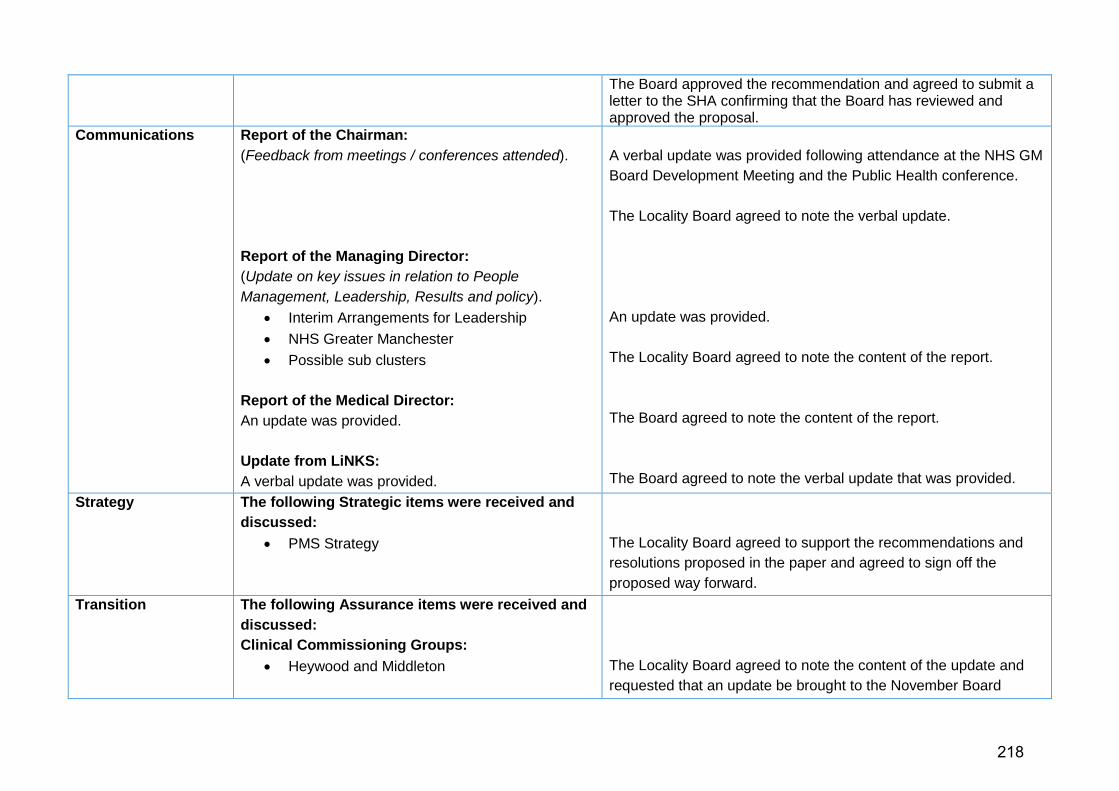
The Board approved the recommendation and agreed to submit a letter to the SHA confirming that the Board has reviewed and approved the proposal.
Communications
Report of the Chairman: (Feedback from meetings / conferences attended). Report of the Managing Director: (Update on key issues in relation to People Management, Leadership, Results and policy).
• Interim Arrangements for Leadership • NHS Greater Manchester • Possible sub clusters
Report of the Medical Director: An update was provided. Update from LiNKS: A verbal update was provided.
A verbal update was provided following attendance at the NHS GM Board Development Meeting and the Public Health conference. The Locality Board agreed to note the verbal update. An update was provided. The Locality Board agreed to note the content of the report. The Board agreed to note the content of the report. The Board agreed to note the verbal update that was provided.
Strategy The following Strategic items were received and discussed:
• PMS Strategy
The Locality Board agreed to support the recommendations and resolutions proposed in the paper and agreed to sign off the proposed way forward.
Transition The following Assurance items were received and discussed: Clinical Commissioning Groups:
• Heywood and Middleton
The Locality Board agreed to note the content of the update and requested that an update be brought to the November Board
218

• GP Care CIC
• Rochdale West
• CCG Options Paper Update on the Health and Wellbeing Board An update was provided on the current position regarding to the development of the Health and Wellbeing Board for the Borough. High Level Transition Plan The Locality Board discussed the Plan.
around the wind down and closing the LLP. The Locality Board agreed to note the content of the update and requested that an update be brought to the November Board around the wind down and closing the LLP. The Locality Board agreed to note the content of the update and requested that an update be brought to the November Board around the wind down and closing the LLP. The Locality Board received an update on the current footprint. The CCG Clinical Leads have recommended one CCG. Early feedback has indicated that the preferred option is likely to be this. Clinical Commissioning Group footprints and next steps will be discussed at the October strategy session. The Locality Board agreed to note the content of the report. The Locality Board agreed to note the content of the report. The Locality Board approved the proposed plan for management of transition and requested that a report be provided at every Locality Board.
Assurance Financial: • Locality Finance Report
Performance:
The Locality Board received an update on the current financial position and the current QIPP savings. The Locality Board agreed to note the content of the report.
219
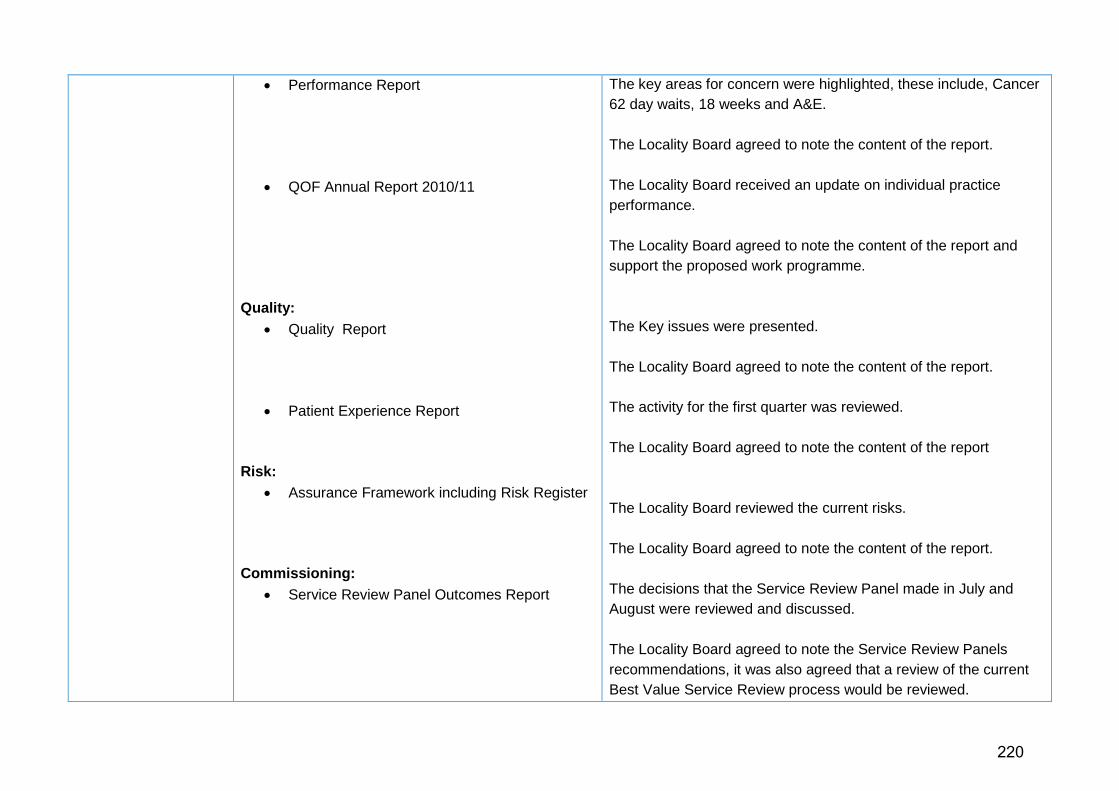
• Performance Report
• QOF Annual Report 2010/11
Quality: • Quality Report
• Patient Experience Report
Risk:
• Assurance Framework including Risk Register Commissioning:
• Service Review Panel Outcomes Report
The key areas for concern were highlighted, these include, Cancer 62 day waits, 18 weeks and A&E. The Locality Board agreed to note the content of the report. The Locality Board received an update on individual practice performance. The Locality Board agreed to note the content of the report and support the proposed work programme. The Key issues were presented. The Locality Board agreed to note the content of the report. The activity for the first quarter was reviewed. The Locality Board agreed to note the content of the report The Locality Board reviewed the current risks. The Locality Board agreed to note the content of the report. The decisions that the Service Review Panel made in July and August were reviewed and discussed. The Locality Board agreed to note the Service Review Panels recommendations, it was also agreed that a review of the current Best Value Service Review process would be reviewed.
220
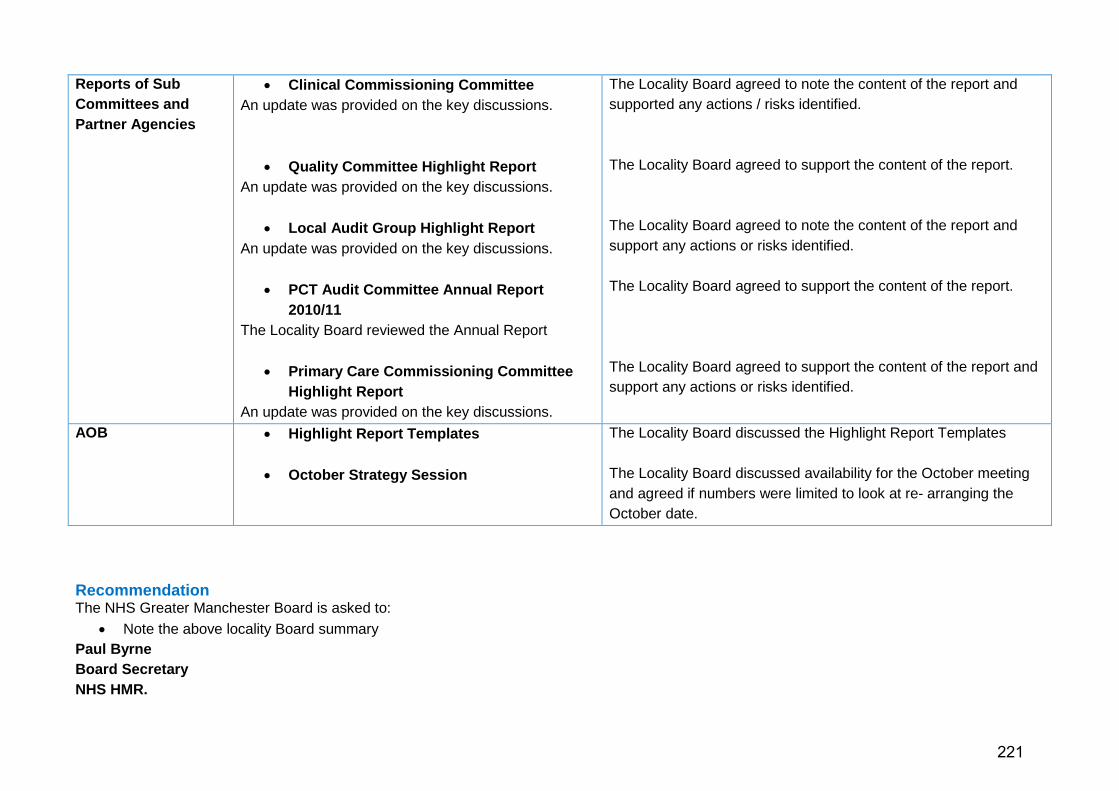
Reports of Sub Committees and Partner Agencies
• Clinical Commissioning Committee An update was provided on the key discussions.
• Quality Committee Highlight Report An update was provided on the key discussions.
• Local Audit Group Highlight Report An update was provided on the key discussions.
• PCT Audit Committee Annual Report 2010/11
The Locality Board reviewed the Annual Report
• Primary Care Commissioning Committee Highlight Report
An update was provided on the key discussions.
The Locality Board agreed to note the content of the report and supported any actions / risks identified. The Locality Board agreed to support the content of the report. The Locality Board agreed to note the content of the report and support any actions or risks identified. The Locality Board agreed to support the content of the report. The Locality Board agreed to support the content of the report and support any actions or risks identified.
AOB • Highlight Report Templates • October Strategy Session
The Locality Board discussed the Highlight Report Templates The Locality Board discussed availability for the October meeting and agreed if numbers were limited to look at re- arranging the October date.
Recommendation The NHS Greater Manchester Board is asked to:
• Note the above locality Board summary Paul Byrne Board Secretary NHS HMR.
221

Locality Board Summary Document NHS Manchester: 7 September 2011 Chaired by: Evelyn Asante-Mensah Subject Summary Action
Chair’s Report Update provided on: • North Manchester Locality Annual General
Meeting • Appointments to NHS North of England
The Locality Board noted the content of the Chair’s verbal report.
Managing Director’s Report
Update provided on Board Risk Register and the decision to put forward an application for 3 CCGs in Manchester at the first stage of the authorisation process.
The Locality Board agreed input was required from Clinical Commissioning Groups prior to approval at the November Locality Board meeting.
Local Public Health Transformation Project
The report provided an update on the public health transformation project which aimed to deliver a public health system for Manchester that was fit for purpose for delivering current and future public health priorities and provided information on the Manchester health profile 2011
The Locality Board requested that in terms of benchmarking, historical comparisons be provided against similar cities regarding pace of progress. The Locality Board noted the report.
Finance Report The report provided a summary of NHS Manchester’s financial performance. NHS Manchester’s financial position at the end of month 4 was an underspend of £35k. Board members were made aware of a number of pressure areas which included a forecast overspend against the Central Manchester contract (£4.2m); Specialist Commissioning (£2.8m) and management costs (£1.6m). Board members were made aware of additional pressures that had been identified such as legal costs, cluster resource and transitional costs. The report concluded that NHSM was in a challenging position and certainty of delivering financial targets was limited.
The Locality Board noted NHS Manchester’s current financial position.
QIPP Update Board members were updated on the current forecast as at 2 September 2011. The financial forecast for savings had decreased from £20.7 to £20m, however the confidence rating for delivery of savings plans had
The Locality Board noted the update on NHS Manchester’s QIPP programme.
222

improved. Members were informed that the QIPP Board would refocus to target specific areas, apply greater scrutiny and hold budget holders to account in order to drive forward savings.
Scheme of Delegation The paper provided an update of NHS Manchester’s Locality Scheme of Delegation in view of the Cluster Board’s approved Governance Manual, including scheme of delegation. Board members were advised that governance arrangements had been restructured to meet the transitional needs from PCT Commissioner to Clinical Commissioning Groups to bean organisation fit for purpose.
The Locality Board noted the Scheme of Delegation
Performance Report The report informed the locality board about key performance issues impacting on NHS Manchester, these included: MRSA - two main providers below trajectory; RTT waiting times at CMFT and PAHT below target (recovery plans established) and Stroke Care. Progress with the new A&E indicators was explained. The paper outlined NHS Manchester’s activity (inpatient, daycase, elective, non-elective and outpatients) against it plans. In total UHSMFT and PAHT activity was below plan (12.6% and 1.8% respectively) and CMFT 22.3% above plan. Key elective specialities overperforming at CMFT were: ophthalmology, gynaecology, oral surgery, trauma and orthopaedics, obstetrics. hepatology, orthodontics, anticoagulant service, gastroenterology, general surgery, urology, and transplantation surgery. Key non-elective specialties overperforming were: general medicine, paediatrics, paediatric surgery, respiratory medicine and gastroenterology.
The Locality Board noted that additional capacity could be obtained from Alder Hey Hospital to assist CMFT in achieving compliance of RTT 18 week target. They acknowledged that CMFT were on the right trajectory to deliver the action plan by December. The Locality Board acknowledged that North West was worst performing area in England for delivering diagnostic work by 6 weeks and confirmed that everything should be done locally to improve these accesses times consistent with achieving good value for money and meeting its financial duties. The Locality Board noted the performance report.
Recommendation The NHS Greater Manchester Board is asked to:
• Note the above locality Board summary Catherine Regan Assistant to Chair/Managing Director NHS Manchester
223

Locality Board Summary Document NHS Oldham: 1 September 2011 Chaired by: Riaz Ahmad (Chair, NHS Oldham) Subject Summary Action
NHS Oldham Locality Board Briefing
Update provided on: • NHS Greater Manchester developments • Clinical Commissioning Group developments • Delivery of the existing Healthy Futures
programme • Shared options model for PCT clusters • Werneth Primary Care Centre • Talking Leaflets
The Locality Board noted the content of the NHS Oldham Board Briefing
2011-12 Quality, Innovation, Productivity and Prevention (QIPP) Delivery Progress
The report confirmed that at Month 4 QIPP financial efficiencies of £5.5m full year effect was reported against target and forecast delivery was circa £13.6m efficiency savings. Programme areas of particular concern were NHS Oldham’s biggest risk areas, which included • Urgent Care • Planned Care
Governance arrangements focus for 2011/12 was very much on implementation of schemes, with internal assurance controls designed and established. Overall strategic monitoring of material QIPP risks was achieved through the Board Assurance Framework, together with appropriate action plans, which was reported to Locality Board on a quarterly basis.
The Locality Board • Acknowledged the progress on QIPP delivery for 2011-12 • Acknowledged the risk associated with full delivery of 2011-12
QIPP plan • Acknowledged the governance arrangements in place to
ensure delivery
224

Twice monthly finance and investment committees and week QIPP meetings would continue to be held to ensure full understanding of progress and timely decision-making and issue resolution. Main risks continued to be addressed through the established governance arrangements, structured engagement and communication plans, contract and performance monitoring and demand management mechanisms.
NHS Oldham Forecast Financial Position – July 2011
The report outlined the forecast financial position for NHS Oldham as at 31 July 2011, highlighting the impact of the continuing financial pressures, and performance against the PCT’s financial duties. Members discussed the in-year budget pressures and the corrective action being taken to address these. Some of the benefits of these improvements made in the last quarter of 2010/11 were now flowing through the system, and these would be closely monitored and evaluated. QIPP plans being implemented would also impact in these areas. Risk to delivering a balanced position were discussed in detail.
The Locality Board received and noted the report with members acknowledging the historic financial performance and continued financial pressures and the likelihood of NHS Oldham achieving the reported forecast balanced position.
North East Sector Scheduled Care Update
The report outlined progress made to date in relation to the North East Sector Scheduled Care QIPP programme, including updates on: • 2010/2011 performance • Implementation of 2011/2012 EUR Policy • Surgical activity thresholds
The Locality Board received and noted the report
225

• 18 week position • Risks • Next steps
North East Sector Unscheduled Care Update
The paper outlined progress made to date in relation to the North East Sector Unscheduled Care QIPP programme
The Locality Board resolved: • To note the contents of the report; • To note the financial risk associated with reliance on the North
East Sector Urgent Care QIPP Programme; • To take local action to address clinical and financial
management issues at the Royal Oldham Hospital Minutes of the Finance, Investment & Performance Committee Meetings held on 21 July 2011, 4 August 2011 and 18 August 2011
The Board received minutes from recent Finance, Investment & Performance Committee meetings for ratification
The Locality Board • Ratified the minutes of the Finance, Investment & Performance
Committee Meetings held on 21.07.11, 04.08.11 and 18.08.11
The Development of the Oldham NHS Clinical Commissioning Group
The report outlined the progress made in establishing a Clinical Commissioning Group (CCG) within Oldham
The Locality Board received and noted the report
Minutes of Oldham NHS Clinical Commissioning Group Meetings held on 1 July 2011 and 29 July 2011
The Board received minutes from recent Oldham NHS Clinical Commissioning meetings for ratification
The Locality Board received and noted the minutes
PCT Transition Governance Arrangements
The report set out the implications of the implementation of PCT Cluster arrangements with regard to NHS Oldham Board Governance. Following the establishment of the Greater Manchester PCT Cluster on 3 May 2011 there was a need to review
The Locality Board resolved: • To receive and note the information provided and progress
made to date; • To agree and endorse the proposed revised governance
arrangements for NHS Oldham in relation to the Locality Board
226

and modify NHS Oldham’s governance arrangements. The paper outlined the requirements for the PCT Board during 2011/12 and 2012/13 in complying with statute and the future responsibilities of the PCT Locality Board
and associated structures for submission to the GM PCT Cluster for approval
Corporate Performance Report – June 2011
The report provided an update on the latest corporate performance for the period ended 31 March 2012 Members were reminded that delivery of key performance targets remained an important part of delivering improved services to the population of Oldham. The report identified the risks and actions to maintain and improve performance and the Locality Board was reminded that this would be underpinned by future improved performance governance arrangements and performance improvement plan for areas of risk. The Locality Board were requested to:
• Ensure that they were aware of the key performance risks in this year;
• Discuss whether the actions identified were sufficient to improve performance
• Discuss and provide feedback with regard to the new content and format of this report
The Locality Board received and noted the report
Board Assurance Framework
The report advised the Board: • That further work had been undertaken to refine
the Board Assurance Framework to ensure it was in line with recommended good practice and reflected material organisational risks;
The Locality Board resolved: • To receive and note the contents of the report • To agree and endorse the 2011/12 Q2 Board Assurance
Framework as providing sufficient assurance around the
227

• Of the principal risks in respect of NHS Oldham delivering their strategic objectives, and the effectiveness of actions taken to manage these via the Board Assurance Framework attached (Appendix 1)
• Progress on actions to rectify identified gaps in assurance and in internal controls (Appendix 2)
management of strategic risks • To agree and endorse the delivery progress of the Assurance
Framework Action Plan
Readiness for Revalidation
The report provided an update for the Board on the GP Appraisal scheme and the steps taken to date to ensure NHS Oldham continued to strengthen and refine its approach to appraisal and performance management in General Practice. The policy should be read in conjunction with the policy relating to Performance Management in Primary Care.
The Locality Board received and noted the report, and acknowledged the progress made to date in readiness for revalidation
Individual Patient Review Panel and Process Review Panel Terms of Reference
The report described the responsibilities of the Individual Patient Review Panel (IPRP) and the Process Review Panel (PRP). The two terms of reference were used within the same document due to the interactions between the two.
The Locality Board resolved: • To receive and note the contents of the report • To endorse and agree the terms of reference
Minutes of the North East Sector Commissioning Board 27 July 2011
The Board received minutes from the recent North East Sector Commissioning Board for ratification
The Locality Board received and noted the minutes
Q1 Infection Prevention & Control Performance Summary 2011/12
The report informed the Board of current Infection Prevention & Control issues and reported on progress against the associated Work Plan. It provided assurance to the Board that NHS Oldham was meeting its statutory and NHS obligations.
The Locality Board received and noted the report
NHS Complaints The report provided a summary of the complaints, The Locality Board received and noted the report
228
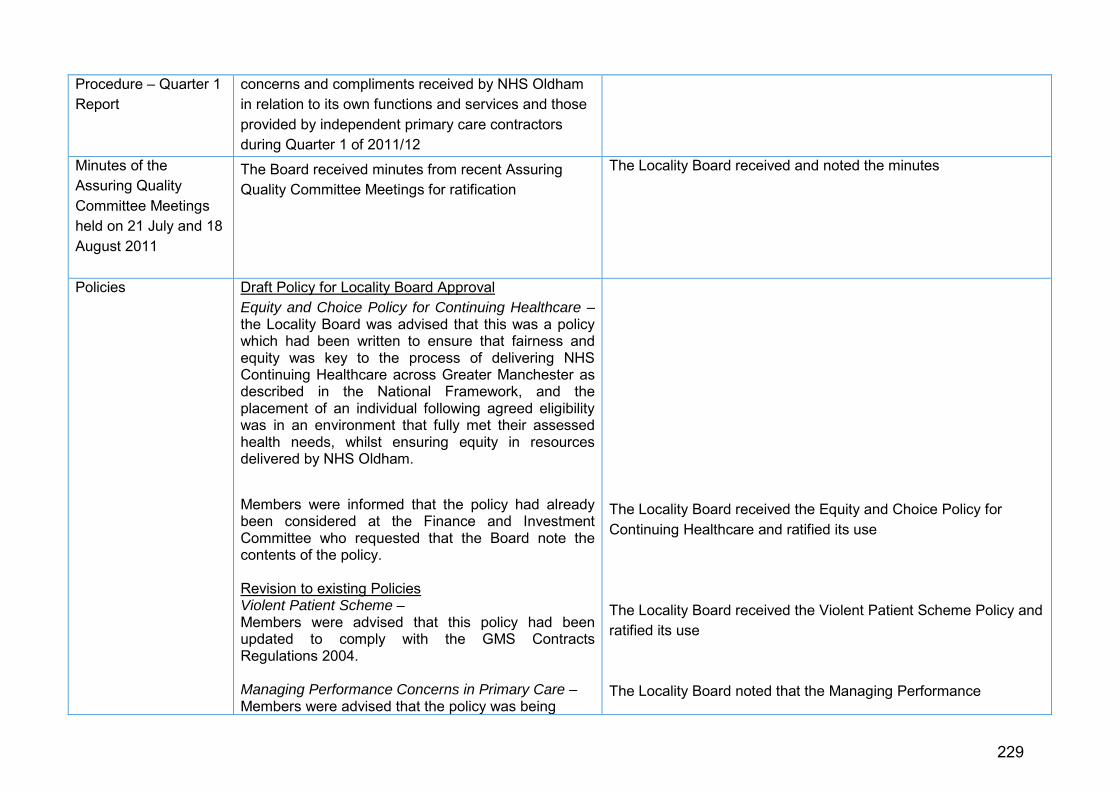
Procedure – Quarter 1 Report
concerns and compliments received by NHS Oldham in relation to its own functions and services and those provided by independent primary care contractors during Quarter 1 of 2011/12
Minutes of the Assuring Quality Committee Meetings held on 21 July and 18 August 2011
The Board received minutes from recent Assuring Quality Committee Meetings for ratification
The Locality Board received and noted the minutes
Policies Draft Policy for Locality Board Approval Equity and Choice Policy for Continuing Healthcare –the Locality Board was advised that this was a policy which had been written to ensure that fairness and equity was key to the process of delivering NHS Continuing Healthcare across Greater Manchester as described in the National Framework, and the placement of an individual following agreed eligibility was in an environment that fully met their assessed health needs, whilst ensuring equity in resources delivered by NHS Oldham.
Members were informed that the policy had already been considered at the Finance and Investment Committee who requested that the Board note the contents of the policy. Revision to existing Policies Violent Patient Scheme – Members were advised that this policy had been updated to comply with the GMS Contracts Regulations 2004. Managing Performance Concerns in Primary Care – Members were advised that the policy was being
The Locality Board received the Equity and Choice Policy for Continuing Healthcare and ratified its use The Locality Board received the Violent Patient Scheme Policy and ratified its use The Locality Board noted that the Managing Performance
229

presented at the Locality Board for information and comments, and was being withdrawn to enable more work to be done on it. Antibiotic Policy – Members were advised that the Antibiotics Policy had been reviewed and updated to reflect changes in clinical practice and that it had been already reviewed by the PCT Medicines Management Committee and the Quality Assurance Forum. A copy of the full policy was tabled for information.
Concerns in Primary Care Policy was for information only and would be withdrawn subject to more work being completed on it. The Locality Board received the Antibiotic Policy and ratified its use
Recommendation The NHS Greater Manchester Board is asked to:
• Note the above locality Board summary Nikki Boaler Board Secretary and Corporate Affairs Lead NHS Oldham
230
Locality Board Summary Document NHS Oldham: 6 October 2011 Chaired by: Riaz Ahmad (Chair, NHS Oldham) Subject Summary Action
NHS Oldham Locality Board Briefing
Update provided on: • Big conversation event • Clinical Commissioning Group (CCG)
developments • General Developments
o Final NHS Oldham Annual General Meeting
o Appointments to the new NHS North board o Developments in Oldham o Summary Care Records (SCR)
The Locality Board noted the content of the NHS Oldham Board Briefing
NHS Oldham Forecast Financial Position and QIPP Delivery – August 2011
The report outlined the forecast financial position as at 31 August 2011 (Month 5), and highlighted the impact of QIPP delivery and management of continuing financial pressures, in relation to performance against the PCT’s financial duties. In accordance with the 2011/12 Operating Framework, NHS Oldham planned to deliver a 0.5% recurrent surplus of £2m, after: • topslicing 2% (£8m) lodged with SHA to fund the
reversal of non-recurrent 2010/11 revenue adjustments
• the return to the SHA of £9m relating to 2010/11 support
• a further (recoverable) lodgement with the SHA of
The Locality Board resolved: • To acknowledge the historic financial performance and
continue financial pressures • To acknowledge the risk associated with full delivery of 2011-
12 QIPP plan • To acknowledge the governance arrangements in place to
ensure delivery
231

£2m The Locality Board discussed in depth the various risks to delivering a balanced position
Minutes of the Finance, Investment & Performance Committee Meetings held on 1 September 2011, and 29 September 2011
The Board received minutes from recent Finance, Investment & Performance Committee meetings for ratification
The Locality Board • Ratified the minutes of the Finance, Investment & Performance
Committee Meetings held on 01.09.11 and 29.09.11
Clinical Commissioning Group (CCG) Authorisation Process
The report outlined the progress made in establishing a Clinical Commissioning Group (CCG) within Oldham, and to obtain approval on the evidence to be submitted to the Cluster and the SHA in relation to the initial configuration gateway.
The Locality Board resolved: • To note the latest guidance in relation to CCG authorisation • To approve the position statement, supporting evidence and
risk assessment for each of the criteria required for the initial configuration phase
• To note the next steps to be undertaken in relation to the developments phase of CCG
Clinical Commissioning Group (CCG) Governance Structure (verbal)
Ian Wilkinson, Chair of the Clinical Commissioning Group, updated the Locality Board on the governance structures in place, both across Greater Manchester and locally in Oldham, and progress made by the CCG
The Locality Board received and noted the verbal update
Clinical Commissioning Group (CCG) Commissioning Intentions
The paper informed the Locality Board of the commissioning intentions developed for 2012/13 by the Oldham NHS Clinical Commissioning Group (CCG), which had been informed by the CCG clinical programme priority areas, and the NHS Greater Manchester commissioning intentions
The Locality Board resolved: • To note and agree the contents of the intentions for 2012/13
232
Minutes of Oldham NHS Clinical Commissioning Group Meeting held on 23 September 2011
The Board received minutes from the Oldham NHS Clinical Commissioning meeting held on 23 September 2011 for ratification
The Locality Board received and noted the minutes
Board Assurance Framework
The report advised the Locality Board: • that further work had been undertaken to refine the
Board Assurance Framework to ensure it was in line with recommended good practice and reflected material organisational risks;
• of the principal risks in respect of NHS Oldham delivering its strategic objectives, and the effectiveness of actions taken to manage these via the Board Assurance Framework attached as appendix 1
The Locality Board resolved: • To note the contents of the report • To receive and agree the 2011/12 Q2 Board Assurance
Framework as providing sufficient assurance around the management of strategic risks
Corporate Performance Report – August 2011
The report provided an update on the latest corporate performance for the period ended 31 March 2012, with key achievements and risks highlighted for the Locality Board’s attention. There was in depth discussion around key performance risks in year, including:
• Referral to Treatment (RTT) Waiting Times
• A&E Quality
• Cancer Waiting Times
• Stroke Indicator
• Coverage of NHS Health Checks Main achievements in the month was an improvement in the elimination of mixed sex accommodation, with
Following discussion around whether the actions identified were sufficient to improve performance, the Locality Board received and noted the report
233

no cases in August 2011; and a marked improvement in Health Care Associated Infection measure with regard to MRSA bacteraemia.
Vital Signs Performance – 2010/11
Members were advised that vital signs were an approach to planning and managing some of the most important areas of health services locally and nationally. These had been developed by the Department of Health to help organisations like NHS Oldham to set a framework to allow more decision making to take place locally and help develop healthcare in Oldham to better meet the needs of local people. The Locality Board was informed that despite not achieving all national and local targets in 2010/11, NHS Oldham continued to improve in many key areas such as cancer waiting times where they had surpassed the national targets for all the indicators except for the percentage of patients receiving first treatment within 62 days. Of the remaining indicators, members were advised that NHS Oldham’s performance was stronger than the average for North West PCTs and national averages in four out of five cases. The Locality Board was reminded that some of the targets NHS Oldham did not achieve in 2010/11 were particularly challenging at both a national and regional level, for example Chlamydia Screening and Stroke Care.
The Locality Board resolved: • To note the performance of NHS Oldham for the last financial
year, and to agree that these were the expected performance measures;
• To recognise the positive performances highlighted in the report and the continued performance challenges faced by NHS Oldham and its Clinical Commissioners
234
Implementing The Cluster Corporate Governance Manual
The paper set out the implications of the implementation of PCT Cluster arrangements with regard to Oldham Locality Board Governance. Following adoption of a Cluster Corporate Governance Manual in July 2011 there was a need to review the locality arrangements for ensuring compliance with new Standing Orders, Standing Financial Instructions and the Scheme of Reservation and Delegation. The paper outlined the work undertaken thus far and remaining work to ensure full implementation
The Locality Board resolved: • To agree that the Cluster Governance manual be provided to
all locality board and sub-committee members and be drawn to the attention of staff via the weekly Friday Bulletin;
• To review and note the content of appendix 1 to the Standing Orders and delegate the Director of Finance to implement the changes required, subject to clarification being sought where necessary;
• To review and note the content of appendix 2 relating to the Standing Financial Instructions and delegate the Director of Finance to implement the changes required, subject to clarification being sought where necessary;
• To review and note the powers that have been reserved to the Cluster Board;
• To formally re-confirm that NHS Oldham locality board members subscribe to the Codes of Conduct and Accountability and to require the Director of Finance to issue a reminder to this effect to all staff;
• To agree that the Locality Managing Director arrange for the preparation of a locality scheme of delegation for review by the locality board prior to submission to the next available cluster board
Minutes of the Audit and Integrated Governance Sub Committee meeting held on 28 September 2011
The Board received minutes from the recent Audit and Integrated Governance Sub Committee for ratification
The Locality Board received and noted the minutes
235

Locality Board Summary Document NHS Salford: 28 September 2011 Chaired by: Edward Vitalis Subject Summary Action
Constitution and Membership of the New Locality Board
Revised governance arrangements for Salford PCT in relation to the Locality Board and associated structures were presented, which had been submitted to the GM PCT Cluster for approval. Appended to the paper were the standing orders, standing financial instructions, and scheme of reservation and delegation.
The Locality Board endorsed the revised governance arrangements.
Chairman’s Communication
The Chairman presented his communication. He commented on the recent successful AGM and read extracts from recently rediscovered Salford Royal ledgers from the 1950s/60s.
The Locality Board noted the Chairman’s communication.
Report of the Managing Director
The report provided a summary of key issues facing the organisation or points relevant to the organisation. This covered:
• Staff figures • National policy, strategy or guidance detailing the impact
for Salford where relevant • Operational issues and updates at national, Greater
Manchester or Salford level • Hundreds Health – Salford Board update • Other matters of local interest
The Managing Director highlighted staff headcount changes, the consultation on a new value-based system of pricing medicines and future ownership of PCT estate in particular.
The Locality Board noted the Managing Director’s Report.
Report of the Medical Director
The report provided an update on the key activities of the Medical Directorate. It covered medical appointments to the Cluster, transition to Clinical Commissioning Groups and NICE guidelines for adult hypertension.
The Locality Board noted the Medical Director’s Report.
Report of the Director of Finance
The Finance Report showed a strong position overall, presenting the following more detailed information:
Discussion clarified that the lodgement this year will help the PCT next year when we expect to make a
236

• Revenue position at month 5 is an underspend of £1.668m, making planned surplus of £2.260m achievable (after accounting for lodgements)
• Capital expenditure plan on track with the majority of the spend weighted towards the latter end of the financial year
• Cash is being drawn down in accordance with the plan • The forecast provider revenue position is breakeven. The 6
degree social enterprise organisation was formed on 1 August and therefore expenditure is only reported to July 2011
• Performance against the Better Payment Practice Code is rated green
The Locality Director of Finance reported that the £2.5m lodgement approved by the Locality Board at its last meeting has been increased to £2.9m. In part due to reduced prescribing costs and corporate budget underspends. A stock take is currently being undertaken across Greater Manchester which will help determine whether the lodgement should be further increased. Local actions have been agreed to minimise the surplus.
contribution to the “Safe and Sustainable” programme of 1% of our budget. The Locality Board noted the Finance Report.
Performance Report a) Performance Information
The Performance Report presented information about performance against targets and the corporate risk register to the Board. The 2011/12 balanced scorecard contains Strategic Plan outcomes, the outcome measures in the Operating Framework and local targets.
There has been an improvement in performance against the 62 day wait for first treatment target for referrals from the NHS Cancer Screening Service.
The report highlighted the following targets (high and extreme risks) which may under-perform in 2011/12, based on previous year’s performance and action plans were received: • Operating Framework outcome – Incidence of MRSA
(HQU01_SRFT) • Operating Framework outcome – Incidence of C Difficile
infections (HQU02_SRFT)
The Locality Board challenged Executive Directors about how realistic smoking targets were, cancer mortality performance (and in particular asked for data about whether late presentation was an issue) and teenage pregnancy performance.
The Locality Board recognised the progress in achieving targets and approved the actions set out for the targets currently rated red.
The Locality Board confirmed as part of the assurance process that the risks reported were being addressed adequately and that the level of risk is acceptable to the PCT.
237

• Operating Framework outcome – Mixed sex accommodation breach (HQU08)
• Operating Framework outcome – Two week wait for breast symptoms (HQU14_B)
• Operating Framework outcome – All cancer two month urgent referral to treatment wait (HQU15_A)
• Operating Framework outcome – Access to NHS dentistry (SQU09)
• Operating Framework outcome – Smoking quitters (SQU18) • Operating Framework outcome – Breastfeeding prevalence
(SQU19) • Strategic Plan outcome area - Male and female mortality rates
(VSB01) • Strategic Plan outcome area - Cancer mortality (VSB03) • Strategic Plan outcome area - Teenage conception rates
(VSB08)
Particular action was noted in relation to patients with MRSA at Salford Royal Foundation Trust (SRFT) getting extra treatments (skin treatment and nasal spray) with no new cases since the end of July, Greater Manchester level work ongoing for the cancer two month urgent referral to treatment wait, dental performance being measured against a target that we set which is extremely high with two new practices to be launched in October and an imminent meeting with SRFT regarding breastfeeding.
Performance Report b) Performance on Quality
The Performance on Quality report presented the following to the Board: • The quality and performance indicators that are contained
within the Salford Royal Foundation Trust (Acute and Community) contracts. A summary of further action and assurance was provided for those indicators that are either not being achieved year to date or the most current month’s performance has not been achieved
• At the time of preparing the paper quality and performance
The Locality Board noted the contents of this paper which provided assurance of the progress of quality measures that were improving the outcomes for Salford patients in terms of experience, effectiveness and safety.
238

indicator information was not available for Greater Manchester West Mental Health Foundation Trust
• Advancing Quality data which shows that SRFT is performing well against standards
• Care Quality Commission Compliance highlighting that the one service (immunisations) will remain registered in a single location from St James’s House
• Advancing Quality Alliance (AQuA) update • Collaboration for Leadership in Applied Health Research
(CLAHRC) update with a possible impaired glucose tolerance Carecall project
• QOF Improvement Project outlining refreshed project objectives and scope
• Health, Safety and Risk Group report • Safeguarding adults report • Safeguarding children report • Complaints, Litigation and Patient Advice and Liaison Service
report • A positive commentary from NHS Salford to the Quality Account
from Oakland’s for 2010/11
Health Gain – Behaviour Change Programme Delivery Plan
The Health Gain – Behaviour Change programme (BCP) is a citywide scheme, to industrialise and make systematic the delivery of behaviour change interventions by front line staff. The aim is to make and sustain a population shift in health and wellbeing, through early engagement and support for people to change their own and their family’s wellbeing behaviour through early intervention, self care and brief interventions where there is an identified need. The BCP is designed for adults, families and young people. The programme will engage the Salford workforce to deliver behaviour change interventions as part of their everyday day work and be integrated into the commissioning process. A new training package will be developed and delivered involving service managers, as well as training a core team for further phases of delivery. The programme is being developed and delivered in
Board member questions resulted in assurance regarding evaluation, launch event and sufficient local provider interest.
The Locality Board: • Noted the current position in the development
phase of the Health Gain – Behaviour Change Programme
• Endorsed the key milestones for the implementation of the Behaviour Change Programme
• Endorsed adoption of the ‘Service Offer’ for those services commissioned by NHS Salford
• Agreed the proposed governance arrangements
239

partnership with Salford City Council, who will project manage the delivery system.
NHS Salford Board previously approved the proposal for the programme. This paper described the development plans, progress to date, deliverables, governance arrangements and alignment with strategic plans.
and the interim proposal to provide strategic leadership
• Supported the proposal for a launch event of the programme
Report from the Commissioning Board
The paper provided a summary for the July and August 2011 Commissioning Board meetings. With the new governance arrangements, the Commissioning Board no longer exists.
The Locality Board noted the Report from the Commissioning Board.
Report from the Health and Wellbeing Board July Meeting
The paper provided a summary for the July 2011 Health and Wellbeing Board meeting. With the new governance arrangements, this was the last meeting of the current Board.
The Locality Board noted the Report from the Health and Wellbeing Board.
Pathfinder Health and Wellbeing Board Terms of Reference
This paper presented the final Terms of Reference for Salford’s Pathfinder Health and Wellbeing Board (Salford HWB). The Health and Social Care Bill identifies that from 2013 the Board will be a statutory requirement for all local authorities. The Terms of Reference and proposed membership were set out, together with proposed routes for organisational governance and partnership reporting. A summary of comments taken from the consultation on the Terms of Reference and the suggested changes were shown. These transitional Terms of Reference have been approved by Salford City Council Cabinet for the pathfinder period until the Board is operational in 2013, prior to which a further review of Terms of Reference will be required.
Board members expressed concern about the size of the Pathfinder health and Wellbeing Board. Some Board members also expressed discomfort with the Chief Executive of a provider organisation (SRFT) being on the Board and potential conflicts of interest. These concerns were noted and it was agreed that they would be considered through the Board’s development programme. It was stressed that initially the Board would not be making any decisions, but would be offering guidance and developing relationships.
The Locality Board noted the Pathfinder Health and Wellbeing Board Terms of Reference and associated information.
Report from the PCT Transition Board
The paper provided an update from the PCT Transition Programme Board (August meeting) which was established to ensure continuance of PCT activity during transition and the safe transfer of PCT business to successor organisations. It provided a policy update and a summary of recent local activity (namely legacy document production, communication and engagement with staff, and career management support to staff).
The Locality Board noted the recent developments in the PCT Transition Programme; confirmed it was satisfied with the progress made and signed off the current version of the NHS Salford Legacy Document.
240

Locality Audit Group Report
The following were presented to the Audit Group in September, however as the meeting was not quorate it did not approve the minutes of the meeting held in June: • Teenage pregnancy strategy refresh report • Performance report • Unscheduled Care Board update report • Risk assurance framework and risk register report • Commissioning Board quality report • Internal Audit progress report • Local Counter Fraud Specialist Progress Report • Charitable Fund accounts • Audit Recommendations Progress Report • Losses and Special Payments report
The Locality Board noted the contents of the report.
Information Governance Annual Report
This report covered the Information Governance (IG) Steering Group arrangements, IG Toolkit workplans and submissions (70% score), new national initiatives, local policy and procedure approvals, information sharing agreements and research approvals. It summarised the risk, current status and forward look relating to the 7 major IG issues reviewed by the IG Steering Group during the year. It concluded with planned developments for 2011/12.
The Board discussed the requirements associated with IG moving through transition and obligations on future CCGs. Suggestions were also made for the Council, PCT and voluntary sector to work in a more coordinated way on IG.
The Locality Board confirmed it was satisfied with the work undertaken by the Information Governance Steering Group during 2010/11.
Charitable Fund Accounts
The paper presented the 2010/11 charitable funds annual report and accounts. As at March 2011 the balance of funds was £82,201 which is £2,759 less than the opening balance. The transfer of charitable funds from NHS Salford to Salford Royal Foundation Trust has been approved by the Secretary of State however this is unlikely to be completed until late in 2011. As an interim measure, the PCT has agreed to manage the funds on behalf of service providers.
The Locality Board approved the annual accounts and report for the year ended 31 March 2011 and noted the transfer of funds to Salford Royal NHS Foundation Trust.
Minutes from Delegated
The Board received the following minutes for information which relate to delegated arrangements:
The Locality Board noted the minutes.
241

Arrangements • NHS Greater Manchester Cluster Board (July 2011) • NW Specialist Commissioning Group (June 2011) • Children and Young People’s Trust Board (June 2011) • Manchester Academic Health Science Centre (MAHSC)
(April 2011) Recommendation The NHS Greater Manchester Board is asked to:
• Note the above Locality Board summary Hannah Dobrowolska Associate Director of Policy NHS Salford
242

Locality Board Summary Document NHS Stockport: 29 September 2011 Chaired by: Michael Greenwood Subject Summary Action
1 Matters Arising from the previous minutes
Confirmation has been received from NHS Greater Manchester that they support the principle of recharging for ‘looked after’ children. Work is underway to put this into practice. SFT has missed a deadline for supplying information on glaucoma patients.
The Locality Board agreed that responsibility for these actions should be retained by the Stockport Clinical Commissioning Pathfinder (SCCP) Executive Committee. They expressed their total dissatisfaction with the failure by SFT to produce the agreed information, and requested that the SCCP Executive Committee continues to monitor progress in this area and to look into how GPs could be supported to help address the situation. They resolved to write to C Burke and J Catania at SFT to express their dissatisfaction.
2 Report of the Chair There was a detailed discussion in the pre-Locality Board meeting of the proposal for developing the Stockport Clinical Commissioning Group. The Chair also provided updates on the following: - NHS Stockport’s commitment to the immunisation of workers against seasonal ‘flu
- He has received a letter from Andrew Gwynne, MP regarding the withdrawal of funding to George House Trust
The Locality Board noted the contents of the update, and stated its expectation that all NHS staff will have the ‘flu vaccine, and for this matter to be raised in communications to NHS Stockport and Community Health Stockport staff, to Stockport Foundation Trust and to General Practice.
243

) - He attended the September meeting of the NHS Greater Manchester Board
- The creditor team from the Finance Directorate have been nominated for Payments Team of the Year in the North-West Awards.
3 Report of the Managing Director
The Managing Director provided updates on the following: - He has discussed the decommissioning plans for CALL with its Operational Manager - Following on from responsibility delegated at the last Locality Board the ‘flu Local Enhanced Service has now been agreed - He has invited the former Professional Executive Committee Chair to take on the now-vacant position of Medical Director.
The Locality Board noted the contents of the report. The Locality Board endorsed the appointment of the former Professional Executive Committee Chair to the position of Medical Director.
4 Report from the Stockport Clinical Commissioning Pathfinder Executive Committee
The Chair of the SCCP Executive Committee provided the following key messages from the following meetings: 10 August 2011 - Any Qualified Provider: the proposed engagement and consultation process were discussed. Suggestions made for additional services to be considered were neuro-physiotherapy and dermatology - EUR policy changes were discussed and ratified - Interim Committee Structure: the proposals were agreed with the requirement to identify appropriate Local Authority involvement on the SCCP Executive Committee - Performance: the committee noted the progress being made against the action plan for reducing the
The Locality Board received the report, noting that its contents are in line with the approved Scheme of Delegation between the Locality Board and the Stockport Clinical Commissioning Pathfinder, and approved the actions being taken, in particular those to address the performance against 18 weeks and A&E, and the Clostridium Difficile outbreak.
244

18 weeks backlog and moving to a sustainable position. Work is ongoing for a reduction in referrals. The committee acknowledged the likely non-achievement against the Chlamydia screening target. Performance against the A&E target was discussed, with emphasis on the pathway redesign work underway by the Urgent Care board - Finance: the overall financial position with the forecast of financial balance was noted. 14 September 2011 - Strategy. The committee approved the eleven strategic themes and identified the three areas of focus for the next three months as being Authorisation/Organisational Development, Long Term Conditions, and Complex Elderly. - New Effective Use of Resources policies were agreed - The committee approved the programme management arrangements for delivering authorisation by October 2012. The capacity issues and time constraints were noted. - The committee approved the new Consultation Policy - Performance: the committee noted that further progress is being made on improving 18 week performance. A&E performance has improved but the committee requested assurance that this can be sustained. - The committee discussed the actions being taken to address the Clostridium Difficile outbreak at SFT.
245
5 Performance and Contract Report Month 4
The members were presented with the Contractor and Provider Performance report (previously discussed by the SCCP Executive Committee). The following key points were discussed: - 18 weeks performance. The number of patients at SFT in the backlog has reduced from 625 to 301 which is 160 ahead of the action plan trajectory. Significant issues remain at CMFT and Pennine Acute. - A&E. Quarter one performance was 92.6% against a target of 95%. There has been an improvement in recent weeks but it is not yet known if this is sustainable. - The action plan for the Clostridium Difficile outbreak will be brought to the next meeting. - There is a financial risk concerning access to urgent care and the implementation of the readmissions policy. Approximately £1.6M of readmissions charges have been challenged with the providers under this new guidance. - The report detailed the negotiation positions for the 2012/13 contracts.
The Locality Board noted the detail of this report and the actions being taken by the SCCP Executive Committee as provided within item 4.
6 Finance Report Month 4
The members were presented with a detailed finance report which included the following key points: - At month 4 we are reporting a year-to-date surplus of £554K against a full-year target of £667K. - Over the first four months £7,838K of the cost improvement target has been delivered. - By month 4 there has been £659K of over-performance by local Foundation Trusts. - Prescribing costs for June 2011 are showing a 6.7%
The Locality Board noted the detail of this report and the discussions of the SCCP Executive Committee as provided within item 4.
246

decrease against June 2010’s cost. The financial priorities looking ahead are to: - ensure revenue spend is maintained and delivery of the planned £667K surplus - achieve in-year financial balance against the capital plan - maintain cash spending within the allocation - process a minimum of 95% of bills by volume and value within the agreed payment terms.
7 Community Health Stockport Performance Report Month 5
The members were presented with a report detailing the performance of Community Health Stockport for the period ending 31 August 2011. The key messages were: - a reported underspend of £457K for this period - activity levels are currently showing an over-achievement of 2,000 contacts against benchmark - while the overall waiting list has increased to 3112 patients there are only 16 waiting for 18 weeks or longer. The average wait for patients remains at 5 weeks.
The Locality Board noted the contents of the report and asked for assurance regarding the work underway in the community regarding MRSA infection rates. They also requested assurance from the SCCP that the community contracting work is underway.
8 Pharmacy Services Quality and Performance Report
The members received a report on Stockport pharmacy services to provide assurance that providers are compliant with national indicators. The report provided detail of the essential and advanced services, and the local enhanced services. Thirty pharmacies have been audited, and four required urgent actions and support. The audit showed that all pharmacies were providing
The Locality Board noted the contents of the report and encouraged the focusing of appropriate amounts of effort to the different aspects of pharmaceutical activity to maximise the public health benefit for the available resource.
247
adequate standards of service in dispensing prescriptions.
9 Pharmacy Application
The members received a report informing them of the recommendation from the Pharmacy Contracts Panel for two 100 hour pharmacies.
The Locality Board endorsed the recommendation of the Pharmacy Contract Panel to accept both applications.
10 Effective Use of Resources Scheme of Delegation
The members received a report stating the changes to the Effective Use of Resources Scheme of delegation. .
The Locality Board received the report and noted the changes.
11 Audit Committee Minutes of 10 May 2011
The Locality Board were presented with the confirmed minutes of the Audit Committee of 10 May 2011. The minutes included the following key points: - the committee reviewed the operational risk register. They requested assurance that, as staff members leave the organisation, risks are reallocated in a timely manner. They also discussed in detail the current arrangements for the movement of patient identifiable data - the committee received and approved the 2011/12 Board Assurance Framework - a revised process for managing corporate policies was agreed - the committee agreed the new audit fee rates - progress against the internal audit plan was reviewed - the draft Annual Report was reviewed.
The Locality Board ratified the minutes of the Audit Committee of 10 May 2011. An update on the occupancy of a new health centre was requested and provided.
248
Recommendation The NHS Greater Manchester Board is asked to note the above NHS Stockport September 2011 Locality Board meeting summary. Paul Pallister Head of Corporate Governance and Risk NHS Stockport
249

Locality Board Summary Document NHS TAMESIDE AND GLOSSOP: 7th September 2011. Chaired by: Kailash Chand Subject Summary Action
Chair’s News Items
Staff Announcements Tim Riley’s CEO of PCT departure – October 20th 2011. Sue Maymon, Interim Director of HR departure - October 28th. Two new interim Appointments to CCG (Kathy Roe, Associate Director of Finance and Steve Allinson Associate Director of Programmes). National CIMA Award NHS Tameside & Glossop had been shortlisted for a national CIMA award – Unlocking Business Intelligence.
For Information
250

Locality Board Minutes
Agreed as a correct record of the meeting
Matters Arising
Performance HCAI Locality Board reiterated that the health care acquired infection Clostridium Difficile remains a high priority for the health economy in Tameside and Glossop. Locality Board further noted that CCG had received the full performance report at its meeting on August 24th.
Locality Board noted the actions being taken forward by the PCT and TFT clinicians, who had also signed-up to the following:-
a) The importance of inappropriate prescribing as being the main cause of CDI in the economy, leading to the majority of infections being designated as avoidable.
b) That every action is being taken to address inappropriate prescribing through clinical leadership that challenges aberrant practice; governance systems that were being put in place to monitor improvements in clinical prescribing performance, and where relevant, disciplinary action will be taken.
Locality Board consensus was that, although the paper provided a clear analysis, there was a need for an action plan with clear, specific and measurable outcomes with time-related targets. It was further agreed that the Locality Board would receive monthly updates (particularly on ‘avoidable’ cases), in order for the Locality Board to continue to monitor progress on a regular basis.
Locality Board particularly noted and discussed the areas of known high level risks, and were assured that these were reviewed and monitored through the monthly QIPP and Performance Board monthly meetings.
251

Scheme of Management
Locality Board approved the Scheme of Management arrangements.
Finance and QIPP
Locality Board received the Finance and
QIPP Report for month 4.
Locality Board noted the PCT’s annual control total for 2011-12 was a £1,000k surplus which is forecast to be achieved by year end. Locality Board also noted that the year to date position was a surplus of £480k which was £147k above the year to date control total. Locality Board were assured that the risks, previously reported (mainly secondary care and continuing care), were reducing, giving confidence that the PCT will achieve its QIPP target, due to the strengthening of the PCT’s financial position.
Draft Finance Committee Minutes
Board received the draft Finance Committee Minutes.
Board noted the key issues that were discussed at the meeting:-
- Secondary Care Performance Report
- Finance Report as at month 4
- QIPP Report
- In Year Financial Position
Draft Clinical Commissioning Group Minutes
Board received the draft CCG Minutes
Board noted the key discussions, actions and decisions held at the meeting on August 24th.
252
Tameside Safeguarding Children’s Board (presentation from the Local Authority)
Health Economy Position on C. Diff (actions being taken)
Scheme of Management (CCG gave approval)
Transition Planning – (noting the unanimous and strong support from CCG for a Tameside and Glossop CCG)
Transition Planning
Board focussed on the following issues:- • The pace of devolution/earned
autonomy for the CCG (completion by December 2011). This was agreed.
• The geography of the CCG to be authorised with the Cluster PCT and SHA’s (October 2011), noting that in the next month the Locality Board and the CCG would need to work through four test areas:-
1. Member practices
Locality Board noted that the CCG, at its meeting on August 24th unanimously and strongly supported a Tameside and Glossop Clinical Commissioning Group. Locality Board discussed the boundary issue at length reflecting on the PCT Reconfiguration Consultation that took place in 2006 and the scale of interest that the PCT had received at that time (in excess of 1,500 responses in favour, with only 11 in favour of Glossop moving to Derbyshire PCT). Tim Riley had also written to Nick Hodgson, Chief Executive of Derbyshire CCG outlining that after a wide ranging set of discussions with GP’s it was clear that the current T & G footprint was overwhelmingly preferred for the newly formed CCG, and that it was on this footprint that the shadow CCG achieved pathfinder status of a viable footprint for achieving authorisation.
253

2. Geography – boundary population
3. Geography – Local Authority boundaries
4. Impact of size
Locality Board also noted that there was one T & G practice in Mossley currently being administered by NHS Oldham. Negotiations were currently taking place with NHS Oldham and the practice in question. Raj Patel would keep Locality Board apprised of developments. In summary Locality Board strongly supported a Tameside and Glossop CCG and noted the on-going discussions with the Mossley practice.
Investment in Health Proposals
Locality Board received the proposals.
It was noted that the governance route going forwards was for individual schemes to now be worked into specific business cases and for these to be considered at the Executive Management Team for final approval. It was noted that CCG were now represented on EMT via Raj Patel, Steve Allinson and Kathy Roe. Decisions would be regularly reported to the CCG and the financial progress reported to the Finance Committee.
Locality Board agreed the proposals.
Telehealth Business Case
Locality Board agreed the Business Case
Any Qualified Provider
Locality Board agreed the proposals
254

PCT Estate
Locality Board received an update from Tom Wilson, outlining the DH Guidance issued on 4th August instructing PCTs to offer to transfer all estate that is ‘integral to the provision of community services’ to the relevant provider organisation – Stockport NHS FT in the case of NHS Tameside & Glossop
Locality Board supported the proposals and agreed to delegate authority to the PCT Executive Team should any interim decisions need to be made, prior to the next Locality Board.
Draft Quality Committee Minutes
Locality Board received the draft minutes.
Locality Board discussed the following key issues at length:-
• Quality Dashboards Report – particularly noting the four domains, patient safety; patient experience; service effectiveness and health outcomes.
• Learning Disability Self Assessment • Safeguarding • Late Discharges • Complaints and Incidents • Enter and Review CQUIN
Locality Board noted that a presentation had been made from the Learning Disability Service, where excellent practice had been commended, particularly in relation to the close working with user groups.
255

NHS Tameside and Glossop Locality Summary Document – October 5th 2011 Chaired by: Kailash Chand Subject Summary Action
Chair’s Report
• Tameside FT were shortlisted for two HSJ Awards
–Nursing Times and ‘Everyone Matters’.
• PEAT Scores 100% achievement for annual assessment of how well the NHS T & G maintain their building and physical environment.
Minutes of the Meeting Held on September 7th
Approved, with one minor typographical amendment. .
PCT Transition Plan
Locality Board approved the Transition Plan.
Locality Board made the following comments:-
• Wished to meet with CCG on October 19th to discuss enabling safe transition (ie. to devolve responsibilities, quickly but safely)
• Requested a Joint Executive Management
Team to support both Boards
• Requested retaining existing Chairmanship of Committees and CCG members to shadow Committee Chairs
• That both Boards formally receive each others minutes.
256
Locality Board noted that in the light of the Locality Board’s strategic priorities and decisions at previous meetings, which were supportive of the direction of travel, work is now taken forward between the PCT and CCG during October 2011 in order to agree a draft formal timetable for the transition process.
Locality Board agreed that at the November 2011 meeting a Transition Plan informed by that work will be considered for approval, together with associated governance structures.
Finance and QIPP
Locality Board noted the PCT’s funding allocation, 2011-12 budgets, the total operating costs and the PCT’s annual control total for 2011-12 which is a £1,000k surplus of £576k which is £159k above the year to date control total.
Locality Board noted that the NHS T & G’s financial risks were reducing, which gave confidence in achieving the QIPP target, due to the strengthening of our financial position. Locality Board noted that in order to achieve this position by the year end, there were still a number of risks that would need to be managed ie. there was a £10.2m QIPP savings target to achieve in 2011/12; secondary care may present a financial pressure to the PCT if activity continues to increase from the 2010/11 outturn position; continuing care caseloads could increase in number or complexity and required further detailed updates and assurances at the next Locality Board meeting in November.
Business Cases
Locality Board agreed two Business Cases – Re-location of the Stroke Unit at Tameside FT, and TFT Service Development (in line with SFI’s, ie. over £150k) General Note from Non Exec Director:-
al Malcolm Sugden asked for assurance that our
257
population is receiving the best possible service in terms of Mental Health Provision across Tameside and Glossop.
Naomi Duggan offered Locality Board assurance, stating that the PCT has recently submitted a return to NHS Greater Manchester outlining ‘’no significant issues’’ for Mental Health services. Tom Wilson also agreed to send Locality Board a briefing on our current position (via Clare Symons, Mental Health Commissioning Lead).
Finance Sub Committee Minutes August 22nd
Locality Board received updates on the following key issues:-
• Secondary care performance report
• Finance Report
• QIPP Report
Secondary Care A brief on Best Practice Tariffs would be circulated to members, after the meeting. Finance and QIPP Report Month 4 position was reporting a £1m surplus at year-end, which was on target. Locality Board noted that Ian Currell would confirm whether or not the PCT could offer ‘brokerage’ by November.
Corporate Performance/QIPP
The areas of known high risks were discussed. Board received the Minutes.
Locality Board were assured that the QIPP and Performance Board minutes gave an overview on corporate performance, highlighting areas of known risk; performance under review; DH and SHA updates. Locality Board were assured that QIPP and Performance Board members now receive weekly updates on C.Diff and improvements were now also
258

being realised. Locality Board also requested monthly updates (discussed further down the agenda, as substantive item). Areas identified as requiring further review and discussion were SATOD, Stroke, Cancer waits and Chlamydia screening. These would be presented to CCG in October, and presented to Locality Board via the CCG minutes in November. Locality Board also discussed issues around extra capacity that might be required in early 2012 to deal with bowel screening, as a result of the national awareness campaign. Tom Wilson assured Locality Board that robust plans had been put in place both at TFT and NHS Tameside and Glossop..
Draft Audit Committee Minutes
Locality Board noted the contents of the minutes and key
issues discussed around:-
• Training Reports • Register of Interests • Internal Audit Report • Audit Committee Handbook • Governance Issues • Cluster Governance • Bribery Act • Standards of Business Conduct • Information Governance Minutes • IM&T Sub Committee • Health and Safety Committee • Corporate Risk Register • StEIS • Incidents Report
Graham Curtis highlighted two issues:- A letter that had been received from NHS Greater Manchester to all Audit Committee Chair’s outlining their Terms of Reference. This would be presented to the next Locality Audit Committee for ratification.
Locality Board noted that Internal, and, External Auditors had paid the PCT a compliment, outlining the efficient running of the Committee and how well it covered diverse topics. Locality Board congratulated the Audit Committee members.
259
Locality Board received the Audit Committee Minutes held on 20th July 2011
Clinical Commissioning Group verbal update
Locality Board received a verbal update from Steve
Allinson. It was noted that an Away Day had taken place on September 20th Graham Curtis and Lynn Travis (NEDS) stated that there had been a great deal of enthusiasm and positive outcome from the CCG session. The key areas covered were – How are we doing as team leaders; Do groups deliver more; Being transformational; Assessing my activity; Transformational competencies; Developing Trust; The Impact of Trust; Four Cores of Credibility; Insight into Ourselves and Others; The Qualities of a Super Team; MOST plans; Avoiding Self Deception; How could we do as a Team of Leaders?
It was noted that a 90 Day Plan, based on the outputs of the session, could be obtained via Raj Patel’s office.
Next Steps:- The Locality Board and CCG were scheduled to meet jointly on October 19th to discuss transitional arrangements. Locality Board requested that a document, based on the discussions to be held and actions to be proposed, be presented to the November Locality Board meeting.
Public Health Transition Plan
The paper summarised the direction of travel for public health into Tameside MBC. It outlined the need for a transition plan to support an organized, safe and effective transition of functions and responsibilities.
The Locality Board supported the initiation of a transition planning group to ensure an effective transfer of public health staff supported by ensuring effective governance around the full transition of functions and the shift in responsibilities to local authorities by April 2013, specifically to:- Locality Board endorsed the development of a Transition Group to oversee the process jointly with Tameside MBC.
260

Locality Board agreed to the development of a Memorandum of Understanding to enable staff to transfer to the local authority by March 2012.
Locality Board supported collaborative working with Derbyshire CC and Derbyshire County PCT to enable the transfer of public health responsibilities for Glossopdale residents in April 2013
C. Diff
Standing/substantive item
Locality Board noted the progress against the HCAI reduction plans for Tameside FT and Community, noting that there had been an improvement in C.Diff infections. Locality Board received an informative presentation on GP prescribing of antibiotics. Locality Board noted that the DH has asked for the C.Diff plans, as exemplary practice. Board requested monthly updates but were assured that the rates of C.Diff were improving.
261
Locality Board Summary Document NHS Trafford: 27th September 2011 Chaired by: Terry Atherton Subject/Agenda Item Summary Action
Chair’s Report The Chair updated members on issues since the last meeting.
The Board were advised about the availability of the NHS Greater Manchester (Cluster) Board papers on the PCT website. The Chair highlighted that the papers for the 8th September 2011 included the Safe and Sustainable Report, which outlined a process to assist with service redesign to achieve a configuration of hospital services across Greater Manchester that provide safe, high-quality services delivered by sustainable, viable organisations.
The Locality Board noted the Chair’s report.
Managing Director’s Report
This is the monthly paper from the Managing Director outlining key issues since the last Board meeting across three key areas namely locality specific issues, NHS Greater Manchester and national issues. The report included locality updates in respect of the Trafford Shadow Health & Wellbeing Board, PCT Governance, Urmston Cottage, Manor Hey Care Homes and the Walk in Centre. In terms of the NHS Greater Manchester update, information was included in relation to the work being undertaken regarding EUR, information governance, risk management and procurement. Nationally, the Board noted that the Department of Health had published several documents in relation to developing a shared operating model for clusters, extending patient choice for providers and ownership of current PCT properties. Other key national documents were also referred to
The Locality Board noted the Managing Director’s report.
262
within the report.
Feedback from the NHS Greater Manchester Cluster Board
The Managing Director and Chair presented a report providing feedback from the meeting of the NHS Greater Manchester Board held on the 8th September 2011.
The Locality Board noted the feedback report.
Verbal Report of the Clinical Executive Committee Chair including Minutes of the Clinical Executive Committee meetings held on the 9th August and 13th September 2011
The CEC Chair provided a verbal overview of the recent discussions of the CEC referring to the minutes of the CEC meeting of the 9th August and 13th September 2011.
The Locality Board noted: - i) the verbal update from the CEC Chair. ii) the minutes of the CEC meetings held on 9 August and 13 September 2011
Finance and Contracting Update
The paper provided an update to the Board on the financial position of the PCT as at 31st August 2011 and the likely forecast out-turn to 31st March 2012. The paper showed that as at the 31st August 2011, the PCT was under spending by £500K and the year end forecast remains a surplus of £1.8M. In terms of CRES and QIPP savings, the PCT had delivered £5.5M of savings against a full year savings requirement of £15.3M. It was noted that some saving schemes carry greater financial risk than others and some schemes are scheduled to deliver savings in the second half of the year. The Executive Team and the Trafford Commissioning Consortium are closely monitoring delivery of the CRES/QIPP schemes and exploring opportunities to identify and agree additional schemes that can be implemented in 2011/12. It was reported that the PCT was experiencing pressures in the areas of
The Locality Board noted the content of this report and the risks therein and actions being taken to deliver the QIPP/CRES for 2011/12.
263

acute NHS, predominantly Central Manchester University Hospitals NHS Foundation Trust (CMFT), and independent providers. The Executive Team and the Trafford Commissioning Consortium are taking actions with providers to bring spending back in line with plans. It was noted that the University Hospital of South Manchester NHS Foundation Trust (UHSM) contracts were underspent as at 31 July 2011. The CMFT contract was overspent partly as a result of increased activity in relation to achievement of the 18 Weeks target.
Performance report (including risk)
The paper provided an overview of the progress made towards achieving the Integrated Performance Measures for 2011/12 and an in depth look at the work underway to reduce the number of delayed transfers of care. It was highlighted that the headline integrated performance measures showing concern are MRSA, A&E 95th percentile performance for admitted patients (time spent in the department), and mixed sex accommodation. These areas of concern and mitigating actions were discussed in detail with the Locality Board. An overview of the work underway across the Trafford health economy to reduce the number of delayed transfers of care was provided. It can be noted that this is a priority area for the PCT as delayed discharges adversely affect many other IPMS including, length of stay, the proportion of a patients stay on a stroke unit, A&E quality indicators and patient experience. It was highlighted that in terms of quarter 1 performance, the rate of delayed transfers was 15.75. This was a rate per 100,000 of the adult population across all providers. It was noted that the two providers causing most concern were THT and UHSM. THT had a consistently high level of delayed transfers of care, although a slight reduction can be seen in Q1 of 2011/12 over the previous 3 quarters in 2010/11. UHSM has seen a sharp rise in the number of delays and the Trust is working with PCT and social services colleagues to bring this down. It is important to
The Locality Board: - (i) noted the report and appended Scorecard. (ii) supported the work to achieve national Integrated Performance Measures and the reduction in delayed discharges (iii) noted that the Locality Director of Finance, Contracting and Performance would provide a further, detailed, report on work in respect of delayed transfers of care.
264
note that detailed action plans have been developed to improve performance within this area.
Locality Board Assurance Framework Report
The purpose of the report was to update the Board on the status of the 2011/12 Locality Board Assurance Framework.
The Locality Board noted the current position of the 2011/12 Locality Board Assurance Framework and the update on the current status of the Corporate Risk Register.
Annual Review of the Audit Committee
This paper summarised the main activities of the Audit Committee from the 1st April 2010 to 31st March 2011. This included details in relation to the Committee Membership, Attendance, Role of the Committee, Performance Against Duties, Key Achievements/highlights in addition to any comments deemed as relevant by the Chair.
The Locality Board noted the Committee review undertaken in respect of the Audit Committee performance for 2010/11.
Quality in Commissioned Services
This paper provided an update on the assurances the PCT has in relation to the quality of commissioned services and highlighted current issues and actions. The report provided statistical information from the Quality Dashboards along with a narrative of any issues and actions a summary of information considered by the June and July Clinical Quality meetings relating to the quality of commissioned service providers and other areas of work being undertaken by the Quality Team. It was highlighted that the stroke activity indicator, which shows the percentage of patients who spend more than 90% of time on a stroke unit was a concern. The PCT is working with NHS Manchester, the lead commissioner for CMFT and UHSM, on this indicator and will report back to a future Board meeting.
That the Locality Board: - (i) noted the issues raised in relation to the quality commissioned services. (ii)endorsed the approach which is being taken to manage the issues raised.
Workforce Information and Organisation Development Update Report
The report highlighted key aspects of the PCT’s workforce performance and the progress made to date on the OD commitments made to assist the PCT through the changes being made to the NHS. These included
The Locality Board noted the content of the paper and the progress made on the OD elements.
265

commitments made for the development of the Clinical Commissioning Group and the development of a comprehensive support package for staff..
Improving The Strategic Partnership & Governance Arrangements For The Joint Trafford Children And Young People’s Service (CYPS).
This report outlined the joint Local Authority and PCT proposal for improving partnership governance arrangements in regards to CYPS given the current proposed structural changes to the NHS and the need to strengthen local arrangements following audit and review.
The Locality Board approved the strategic partnership agreement and the new governance structure outlined within the body of the paper and requested that clarity be sought on whether this required ratification by NHS Greater Manchester.
Integrated Care Trust and Integrated Care Service Update
This was a verbal update from the Managing Director on the latest developments in relation to ICT and ICS.
The Locality Board noted the update.
Transformational Change Group Update
The report provided an update on the recent work stream meetings and the progress of the Transformational Change Group. The key risks, highlights and progress made during the last period in relation to the Master Assurance Plan were outlined.
The Locality Board noted the progress made over the last period.
266

Minutes of the Integrated Governance Committee held on the 21st July 2011
Members received the minutes from the Integrated Governance Committee held on the 21st July 2011. .
The Locality Board noted the minutes.
Minutes of the Finance and Performance Committee held on the 25th July 2011
Members received the minutes from the Finance and Performance Committee held on the 25th July 2011.
The Locality Board noted the minutes.
267

Locality Board Summary Document NHS Trafford: 25th October 2011 Chaired by: Terry Atherton Subject/Agenda Item Summary Action
Chair’s Report
The Chair’s verbal report included the following: The Chair congratulated Mr P Connellan, Non Executive Director on his appointment as the new Chairman of Tameside Hospital NHS Foundation Trust. On behalf of the Board, the Chair thanked Mr Connellan for his valuable contributions during his time as Non Executive Director at the PCT and wished Mr Connellan every success for the future. The Board were updated on the NHS Greater Manchester Cluster Strategy Day that had taken place on the 13th October 2011. It was noted that Whistleblowing has been raised at a Greater Manchester level and discussions are now proceeding as to how best to implement this across this wider health economy. It is possible, following an Announcement by the Secretary of State that this might become a statutory responsibility within the NHS Constitution.
The Locality Board noted the Chair’s report.
Managing Director’s Report
This is the monthly paper from the Managing Director outlining key issues since the last Board meeting across three key areas namely locality specific issues, NHS Greater Manchester and national issues. The report included locality updates in respect of Information Governance assurance, the Communications Team being shortlisted for further awards, the refresh of the Equality and Diversity Trafford Action Plan, the Winter Communications Plan, Walk in Centre and recent use of the Corporate Seal. In terms of the NHS Greater Manchester update, information in relation to
The Locality Board noted the Managing Director’s report and approved the use of the Seal.
268

agreement of the principles for assignment and Equitix and Community Solutions acquiring Primary Plus are included. Nationally, the Managing Director referred members to a number of publications that had been issued including the draft National Planning Policy Framework, a document concerning ‘Protecting Children and Young People: The Responsibilities of Doctors’ and other key documents.
Verbal Report of the Clinical Executive Committee Chair including Minutes of the Clinical Executive Committee meeting held on the 11th October 2011
The Medical Director provided a verbal overview on the recent discussions of the CEC referring to the minutes of the CEC meeting of the 11th October 2011. It was reported that issues were raised at the October CEC regarding the approval of the Leg Ulcer and Catheter Prescription Invest to Save proposals at the September meeting. This was in light of the apparent lack of consultation with pharmacies and potential for legal challenge which was evident following discussions with the LPC. A meeting with the CEC Pharmacy Lead and the LPC took place on the 20th October 2011 in an attempt to resolve these issues and a further update would be provided at the November CEC and Locality Board meetings.
The Locality Board noted: -
(i) the verbal update from the Medical Director (ii) the minutes of the CEC meeting held on 11th October 2011.
Finance and Contracting Update including QIPP Update
The paper provided an update to the Board on the financial position of the PCT as at 30th September 2011 and the likely forecast out-turn to 31st March 2012. The paper showed that as at the 30th September 2011, the PCT was under spending by £837K and the forecast was a surplus of £1.8M. It was highlighted that the actual under spending to month six was marginally above the surplus of £824K included within the plans with NHS North West and was principally as a result of a favourable variance against acute provider budgets in the month of September.
The Locality Director of Finance, Contracting and Performance informed
The Locality Board noted the content of this report and the risks therein and agreed the actions being taken to deliver the QIPP/CRES for 2011/12 and manage the risks.
269

members that the current overspend on secondary care contracts was £584K. This expenditure had been broken down to Trust level. The appropriate actions were being taken to address any areas of overspend.
It was noted that significant progress was being made in relation to prescribing in realising savings of £1,335k however members were reminded that the PCT was displaying a similar trajectory at the same time last year which was adversely affected by winter prescribing pressures. The Locality Director of Finance, Contracting and Performance highlighted that a reduction of £582K had been factored into the expected deduction to be made for patients readmitted within 30 days at UHSM in line with the guidance on readmissions as outlined in the Operating Framework.
It was reported that improvements had been achieved regarding elective activity at CMFT and the Trust has indicated that they do not expect the overspend to increase significantly. In terms of QIPP/CRES savings, £7.5M of savings have been delivered to the end of September however actual savings for the PCT are £555K behind plan and £150k behind the pro-rata savings target of £7.65M. It was reported that a review of the existing savings schemes had been undertaken and any areas of slippage had been identified. It was noted that a number of the schemes were planned to take place in the second half of the year which mainly relied upon actions from clinicians to deliver savings. The Locality Director of Finance, Contracting and Performance assured Locality members that a mitigation plan for any CRES slippage was being developed and meetings are taking place with saving scheme sponsors and clinical leads to ensure that plans are on target for achievement. It was agreed that this plan would be submitted to the next QIPP Committee (former Finance and Performance Committee) and the next Locality Board meeting.
Performance report (including Risk)
The paper provided an overview of the progress made towards achieving the Headline Integrated Performance Measures for 2011/12 and also
The Locality Board noted the contents of the report and agreed the work identified
270

examined the position on delayed discharges and plans to improve the current performance. It was reported that there were 30 headline measures (including 12 A&E measures to account for site based reporting) and as at August 2011, the PCT was rated ‘red’ against two of these measures. It was noted that this meant that performance was outside of trajectory by more than 10% in two areas namely the areas of MRSA and Eliminating Mixed Sex Accommodation (EMSA). It was highlighted that in respect of MRSA, this included two reported cases from the community as outlined at 2.3 of the report. It was noted that Healthcare Acquired Infection was a fixed agenda item on the commissioner/provider quality meetings and an economy wide plan was in place to address this issue.
In terms of EMSA, the PCT monitors the experience of Trafford patients at all providers. It was reported that between April-August 2011, there were 35 breaches including 33 at UHSM, 1 at Pennine Acute Trust and 1 at Barts and the London Trust. It was noted that the NHS Greater Manchester Cluster have been closely monitoring mixed sex accommodation across Greater Manchester and were keen to address any underperforming areas. The Locality Director of Finance, Contracting and Performance referred to the work being undertaken to address the delayed transfers of care to understand the underlying factors affecting performance within this area. It was reported that different methodologies were used by each Trust to capture this data making it difficult to make inferences about the number of patients waiting for discharge. Despite these difficulties, key actions were being taken to reduce the number of delays which was detailed at paragraph 3.9 of the report.
to deliver the integrated performance measures and reductions in delayed discharges.
Locality Board Assurance Framework Report
The purpose of the report was to update the Board on the status of the 2011/12 Locality Board Assurance Framework. It was reported that the top rated risk continued to be the ‘Lack of clarity
The Locality Board noted the current position of the 2011/12 Locality Board Assurance Framework and update of the status of the Corporate Risk Register.
271

about future direction for the NHS resulting in delays in local implementation plans for radical transformation and re design of clinical models of care and financially viable service models’. It was noted that the assignment process for staff was now becoming clearer and discussions had commenced at the Executive Team and Board which should positively impact on the rating for this risk over time.
Trafford Safeguarding Children Board Annual Report 2010/11 and Business Plan 2011/12
The report included the Trafford Safeguarding Children Board Annual Report 2010/11 and Business Plan 2011/12 which covered the governance arrangements, achievements and future plans. It was reported that Dr B Postlethwaite, Independent Chair, Trafford Safeguarding Children Board, would be attending the next Locality Board meeting in November 2011 and there would be a broader discussion in relation to this report at that meeting.
The Locality Board noted the Trafford Safeguarding Children Board Annual Report 2010/11 and Business Plan 2011/12.
The Munro Review of Child Protection: Final Report – A Child Centred System
The report updated the Locality Board on the Munro review of child protection, the Government response to the review and the Trafford implications and recommended actions from the review.
The Locality Board noted: - (i) Trafford implications and
recommended actions of the Munro Review of Child Protection as outlined in the paper that are being taken forward by CYPS governance arrangements;
(ii) Trafford Safeguarding Children Board (LSCB) preliminary action plan agreed at the September 2011 meeting for LSCB specific recommendations as outlined in Appendix 2.
Locality Governance Arrangements – Committee Terms of Reference
The purpose of the report was to update the Locality Board on the changes to the Committee Structure in preparedness for shadow Clinical Commissioning arrangements.
The Locality Board: - (i) approved the Terms of Reference for the Clinical Commissioning Committee,
272

This included the relevant revisions that have been made to the Committee Terms of Reference ensuring Non Executive Director input is maintained as part of the transition process.
Locality Audit Group, QIPP Committee and Clinical Quality Committee subject to any proposed comments/amendments being made by members of the Locality Board. (ii)noted the further actions being taken by the Corporate Support Team to support Committee leads and Chairs within their respective areas. (iii) approved the recommendation that task and finish group previously constituted to assist with the details of the revised governance arrangement be reconvened to enable further review of the draft scheme of accountability/delegation to these committees and that the group’s work should support the detailed operation of these new committees with their mandated terms of reference.
Trafford Healthcare Trust Acquisition and Integrated Care Service Update
This item was a verbal and written update from the Managing Director on the latest developments in relation to ICS and THT Acquisition. In addition to the regular locality update, two reports had been included for the Board’s information which were a report in respect of governance that was submitted to the NHS Greater Manchester Board on the 8th September 2011 and the Integrated Care System Programme Directors report of the 18th October 2011.
The Locality Board noted the reports.
Transformational Change Group Update
This was a written update on the recent work stream meetings and the progress of the Transformational Change Group. It was reported that the ‘one page programme manager’ tool was being utilised to track progress on each of the Transformational Change Workstreams with the use of a RAG rating system.
The Locality Board noted the progress made over the last period.
273

The Director of Corporate Affairs, Partnerships & Compliance informed members that plans were now in place to address the one area of red status within the plan which related to the reaffirmation of GP constitutional matters.
Commissioning Strategic Plan Year End report
The Deputy Director of Commissioning was in attendance to provide a presentation on the progress made in relation to the CSP initiatives for 2010/11. The Medical Director provided a patient story to demonstrate how initiatives from the CSP had benefited patients.
The Locality Board noted the report and presentation.
Minutes of the Locality Audit Group held on the 21st September 2011
Members received the minutes from the Locality Audit Group held on the 21st September 2011.
The Locality Board noted the minutes from the Locality Audit Group held on the 21st September 2011.
274

Remuneration and Terms of Service Committee Date: 14 July 2011 Venue: Cornerstone Centre, Beswick Present: Mr Terry Atherton – Non-Executive Director (Chair)
Professor Eileen Fairhurst - Chairman Mr Paul Horrocks – Non-Executive Director
Mr David Edwards – Non-Executive Director Dr Kailash Chand – Non-Executive Director Mr Riaz Ahmad – Non-Executive Director Mrs Pam Senior – Non-Executive Director Mr Alan Stephenson – Non-Executive Director
In Attendance: Dr. Mike Burrows - Chief Executive
Mrs Andrea Anderson – Associate Director of Human Resources Mr Rob Bellingham - Board Secretary
Agenda Item No Item
11/4 Apologies for Absence Ms Evelyn Asante-Mensah – Non-Executive Director Mr Michael Greenwood – Non-Executive Director
11/5 Notes from the Previous Meeting These were accepted as a correct record.
11/6
Terms of Reference The updated Terms of Reference were received by the Committee, noting they had been approved at the NHS Greater Manchester Board meeting which preceded this meeting.
11/7 Date and Time of Next Meeting To be confirmed
275


















