Blue Cross Medicare Supplement Outline of Coverage
44
Blue Cross ® Medicare Supplement Outline of Medicare supplement coverage — Plans A, C, D, F, High-Deductible F, G, High-Deductible G and N 20 21 Medicare supplement coverage offered by Blue Cross Blue Shield of Michigan www.bcbsm.com/medicare-supplement
Transcript of Blue Cross Medicare Supplement Outline of Coverage
Blue Cross® Medicare SupplementOutline of Medicare supplement coverage — Plans A, C, D, F, High-Deductible F, G, High-Deductible G and N
20 21
Medicare supplement coverage offered by Blue Cross Blue Shield of Michigan
www.bcbsm.com/medicare-supplement


1
Now that you’re eligible for Medicare, you have new options for health care coverage. Blue Cross Medicare Supplement offers coverage that’s convenient and helps protect you from the high cost of health care.
Getting to know Medicare supplement coverageMedicare supplement coverage, also called Medigap coverage, is a health policy that works together with Original Medicare Part A (hospital) and Part B (medical) to help cover certain costs Original Medicare doesn’t. It offers great benefits and lowers your out-of-pocket costs. As your primary health care coverage, Original Medicare provides hospital and medical coverage, but it doesn’t cover all health care costs and has deductibles and coinsurances that must be paid before Medicare pays benefits. Medicare also limits coverage for certain services.
Medicare supplement works with Original Medicare coverage and, depending on the plan you’re eligible for, may cover all or a portion of your Medicare deductibles and coinsurances. Blue Cross Blue Shield of Michigan offers Blue Cross Medicare Supplement options for Plans A, C, D, F, High-Deductible F, G, High-Deductible G and N only. Other Michigan insurance carriers may offer other or additional plans, but supplement plans can be sold in only 10 standard plan options plus two high-deductible plans: Plans A, B, C, D, F, G, K, L, M and N.*
Every supplement insurer must make Plan A available. Plan A covers basic benefits:
Hospitalization: Medicare Part A coinsurance plus coverage for 365 additional days after Medicare benefits end
Medical expenses: Medicare Part B coinsurance (generally 20% of Medicare-approved expenses) or copayments for hospital outpatient services
Blood: First three pints of blood each calendar year
Blue Cross Medicare Supplement made easy
*Plans E, H, I and J are no longer available for sale.

21There are also two high-deductible plans, HD-F and HD-G. If you are eligible for either plan and decide to enroll, this means you must pay for Medicare-covered costs up to the deductible amount of $2,370 for 2021 before your supplement plan pays anything.2After you meet your out-of-pocket yearly limit and your yearly Part B deductible, the supplement plan pays 100% of covered services for the rest of the calendar year.
BenefitsAll nationwide plans
A B C1 D1 F2 G2 K L M N3
Medicare Part A coinsurance and hospital costs up to an additional 365 days after Medicare benefits are used up
4 4 4 4 4 4 4 4 4 4
Medicare Part B coinsurance or copay 4 4 4 4 4 4 50% 75% 4 43
Blood (first three pints) 4 4 4 4 4 4 50% 75% 4 4
Part A hospice care coinsurance or copay 4 4 4 4 4 4 50% 75% 4 4
Skilled nursing facility care coinsurance 4 4 4 4 50% 75% 4 4
Medicare Part A deductible 4 4 4 4 4 50% 75% 50% 4
Medicare Part B deductible 4 4
Medicare Part B excess charges 4 4
Foreign travel emergency (up to plan limits)
80% 80% 80% 80% 80% 80%
Out-of-pocket limit4
$6,220 in 2021
$3,110 in 2021
Medicare supplement plans across the country
How to read the chart:If a check mark appears in a column of this chart, the supplement policy covers 100% of the described benefit. If a row lists a percentage, the policy covers that percentage of the described benefit. If row is blank, the policy doesn’t cover that benefit. Note: The supplement policy covers coinsurance only after you’ve paid the deductible unless the supplement policy also covers the deductible.

3
BenefitsAll nationwide plans
A B C1 D1 F2 G2 K L M N3
Medicare Part A coinsurance and hospital costs up to an additional 365 days after Medicare benefits are used up
4 4 4 4 4 4 4 4 4 4
Medicare Part B coinsurance or copay 4 4 4 4 4 4 50% 75% 4 43
Blood (first three pints) 4 4 4 4 4 4 50% 75% 4 4
Part A hospice care coinsurance or copay 4 4 4 4 4 4 50% 75% 4 4
Skilled nursing facility care coinsurance 4 4 4 4 50% 75% 4 4
Medicare Part A deductible 4 4 4 4 4 50% 75% 50% 4
Medicare Part B deductible 4 4
Medicare Part B excess charges 4 4
Foreign travel emergency (up to plan limits)
80% 80% 80% 80% 80% 80%
Out-of-pocket limit4
$6,220 in 2021
$3,110 in 2021
3Plan N pays 100% of the Part B coinsurance, except for a copay of up to $20 for some office visits and up to a $50 copay for emergency room visits that don’t result in an inpatient admission.4Plans C, F, and HD-F are only available to those who have Medicare effective dates before January 1, 2020.
Blue Cross does not offer these plans.

4
Did you delay enrolling in a Medicare supplement plan, but were eligible for Medicare before Jan 1, 2020?As you consider your options with Medicare supplement, Blue Cross wants to make you aware of some federal law changes that could affect your health plan decision. The Medicare Access and CHIP Reauthorization Act of 2015, or MACRA, affects Medicare supplement plans nationwide that cover the Medicare Part B deductible. Medicare supplement plans that cover the Part B deductible (Plans C, F, and High-Deductible F) are no longer available for individuals who turned 65 or became eligible for Medicare on or after Jan. 1, 2020. Blue Cross offers Plan G, which is very comparable in benefits and available at a less expensive price than Plan F.
If you want to learn more about MACRA legislation, visit the Network for Regional Healthcare Improvement’s website at: www.nrhi.org/work/what-is-macra*.
Don’t delay
Learn about what MACRA means to you
*Blue Cross Blue Shield of Michigan doesn’t own or control this website.

5

6
Our new Dental Vision Hearing Package is both exciting and essential to your best health. So add it to your plan and watch the sunrise, listen to your music and smile all the while.
Yours at a low cost starting April 1, 2021• Your price will be just $15.25 per month, in addition to your
Blue Cross Medicare Supplement premium.1
• If you choose the Dental Vision Hearing Package, it will be added to your Blue Cross Medicare Supplement plan. The Dental Vision Hearing Package will be available starting Feb. 1, 2021, for a Apr. 1, 2021, start date.2
Available for new and existing members• The Dental Vision Hearing Package will be available to
new Blue Cross Medicare Supplement members as well as existing Blue Cross Medicare Supplement and Legacy Medigap members.
• New members will have the ability to add the Dental Vision Hearing Package to their Medicare supplement plan at the time of initial enrollment or within the first 30 days following the policy start date.3
1 Premium for the Dental Vision Hearing Package will be re-evaluated each year and is subject to change.
2Dental, vision or hearing benefits aren’t sold separately3 Existing members can add the Dental Vision Hearing Package to their current plan by reaching out to their agent or by applying electronically at www.bcbsm.com/medicare/help/forms-documents/enrollment.html
NEW for 2021Dental Vision Hearing Package
See Page 36 for more information about the Dental Vision Hearing Package.

7

8
Medicare Supplement Well-Being program
Real support for real life
You get great advantages to help you live a healthier, happier life
Our Well-Being program helps you live your best life. As a member, you have advantages that will let you experience life’s adventures with Blue Cross confidence. You choose the Medicare supplement plan you want, and we’ll supply the well-being support you need to fulfill your personal health goals.
You’ll notice that so much of this program can be taken advantage of virtually, so no matter what the world brings, you can stay healthy.

9
WelvieSM Surgery Decision-Support program We have an online surgery support program that helps you decide on, prepare for and recover from surgery. It can help you talk with your doctor about surgery and other treatment options. If you need surgery, the program can show you how to avoid common problems that may occur after surgery.
24-Hour Nurse Line Talk to a registered nurse when you have questions about an illness or injury. The nurse line can help you, day or night, determine how you can treat minor things at home. This may help you avoid unnecessary trips to the doctor or hospital.
Blue Cross® Virtual Well-Being You’ll get guidance and support on your journey to personal well-being. Short, high-energy, virtual webinars are available to watch on your computer, tablet or mobile phone each week. They focus on different topics, such as mindfulness, emotional health, financial security, physical wellness, preventive health care and more. The program also offers informational materials you can download to save and share with your family and caregivers.
Blue365® discounts When you show your member ID card, you get nationwide savings for health magazines, cooking classes, weight-loss programs and retail stores. You can even get discounts on hearing aids and eyewear, as well as exams. Get a list of current savings at www.blue365deals.com.
Included in your membership ...

10
Blue Cross Medicare Supplement premiumsFor Blue Cross Medicare Supplement plans, certain factors may affect your monthly premium. We base your premium on the area you live in and your age, gender and in certain situations, health status and whether you use tobacco. When we base your premium on health status and whether you use tobacco, this is called medical underwriting. The charts in this booklet show the monthly cost for Plans A, C, D, F, High-Deductible F, G, High-Deductible G and N based on these factors. The deductible, coinsurance and copay amounts listed in this brochure are based on the 2021 CMS-approved values and are subject to change in 2022.
Your premium won’t be affected by your tobacco use, health status (including body mass index value), claims experience, receipt of health care or medical condition, if you:
Are applying during your Medigap Open Enrollment Period (OEP)
Have a situation that qualifies as a guaranteed issue right(see Page 13 for additional details)
*CMS stands for Centers for Medicare & Medicaid Services
11
More members means more savingsWe’re happy to offer a household discount to Blue Cross Medicare Supplement members. If you’re a Blue Cross Medicare Supplement member, you may be eligible to save 5% on your monthly premium. Here’s what you need to do to become eligible for this discount and start saving:
If you’re a new member
Apply at the same time as another Medicare-eligible individual who lives in the same household and is applying for
a Blue Cross Medicare Supplement plan. You can also apply for this discount if a household member is currently covered by a Blue Cross Medicare Supplement
or Legacy Medigap plan.
If you’re an
existing member
You and any other household members who are currently enrolled in a
Blue Cross Medicare Supplement or Legacy Medigap plan can apply for the
discount1. Two or more existing Blue Cross Medicare Supplement or
Legacy Medigap members in the same household must complete an Application for Medicare Supplement Household Discount. You can get the form online at www.bcbsm.com/medicare/help/understanding-plans/
supplement/household-discounts.html.
You can also call Customer Service at 1-888-216-4858 from 8 a.m. to 5 p.m. Eastern time, Monday through Friday
(TTY users, call 711).
Please note: There does not need to be a spousal or familial relationship between the policy holders to make them eligible for the discount; however, you must reside in the same household. A household is defined as a single-family home, a condominium or an apartment. Assisted living facilities, group homes, adult day care facilities, nursing homes or any other health residential facilities are not included in the definition of household.1Members with Medicare Advantage plans are not eligible for this discount and cannot be used to make a Medicare supplement member eligible for the household discount.
12
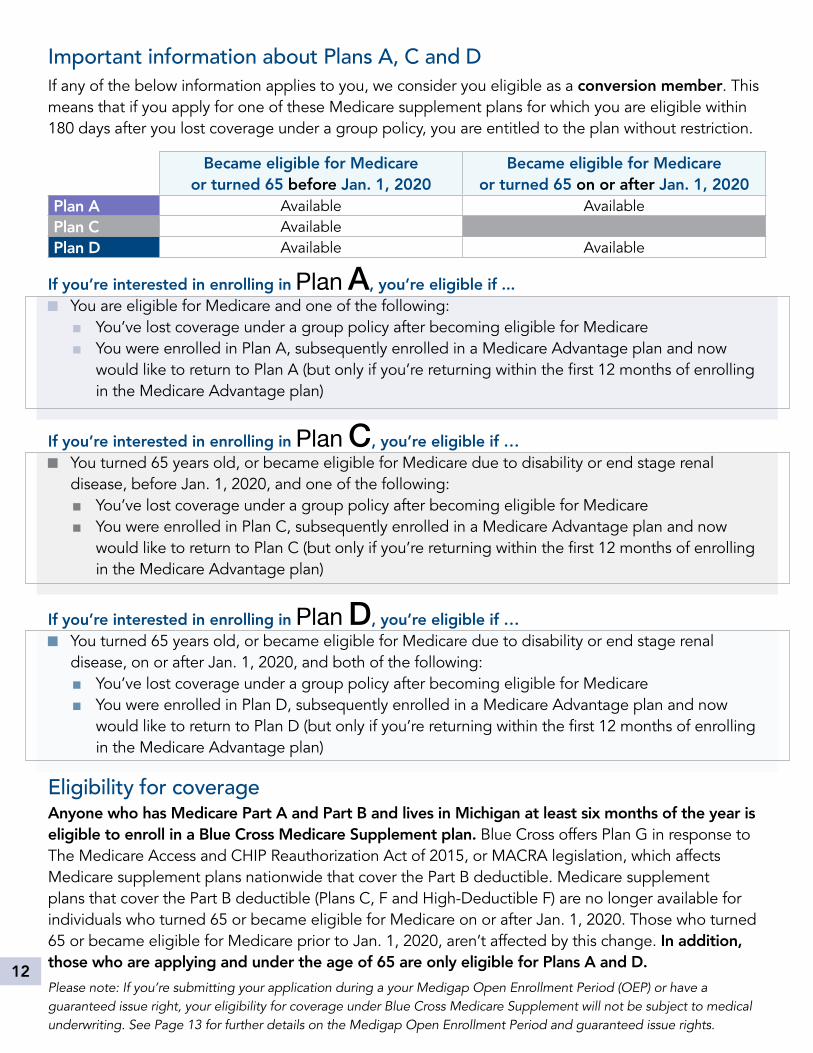
Important information about Plans A, C and DIf any of the below information applies to you, we consider you eligible as a conversion member. This means that if you apply for one of these Medicare supplement plans for which you are eligible within 180 days after you lost coverage under a group policy, you are entitled to the plan without restriction.
Became eligible for Medicare or turned 65 before Jan. 1, 2020
Became eligible for Medicare or turned 65 on or after Jan. 1, 2020
Plan A Available AvailablePlan C AvailablePlan D Available Available
If you’re interested in enrolling in Plan A, you’re eligible if ... You are eligible for Medicare and one of the following:
You’ve lost coverage under a group policy after becoming eligible for Medicare You were enrolled in Plan A, subsequently enrolled in a Medicare Advantage plan and now
would like to return to Plan A (but only if you’re returning within the first 12 months of enrolling in the Medicare Advantage plan)
If you’re interested in enrolling in Plan C, you’re eligible if … You turned 65 years old, or became eligible for Medicare due to disability or end stage renal
disease, before Jan. 1, 2020, and one of the following: You’ve lost coverage under a group policy after becoming eligible for Medicare You were enrolled in Plan C, subsequently enrolled in a Medicare Advantage plan and now
would like to return to Plan C (but only if you’re returning within the first 12 months of enrolling in the Medicare Advantage plan)
If you’re interested in enrolling in Plan D, you’re eligible if … You turned 65 years old, or became eligible for Medicare due to disability or end stage renal
disease, on or after Jan. 1, 2020, and both of the following: You’ve lost coverage under a group policy after becoming eligible for Medicare You were enrolled in Plan D, subsequently enrolled in a Medicare Advantage plan and now
would like to return to Plan D (but only if you’re returning within the first 12 months of enrolling in the Medicare Advantage plan)
Eligibility for coverageAnyone who has Medicare Part A and Part B and lives in Michigan at least six months of the year is eligible to enroll in a Blue Cross Medicare Supplement plan. Blue Cross offers Plan G in response to The Medicare Access and CHIP Reauthorization Act of 2015, or MACRA legislation, which affects Medicare supplement plans nationwide that cover the Part B deductible. Medicare supplement plans that cover the Part B deductible (Plans C, F and High-Deductible F) are no longer available for individuals who turned 65 or became eligible for Medicare on or after Jan. 1, 2020. Those who turned 65 or became eligible for Medicare prior to Jan. 1, 2020, aren’t affected by this change. In addition, those who are applying and under the age of 65 are only eligible for Plans A and D.
Please note: If you’re submitting your application during a your Medigap Open Enrollment Period (OEP) or have a guaranteed issue right, your eligibility for coverage under Blue Cross Medicare Supplement will not be subject to medical underwriting. See Page 13 for further details on the Medigap Open Enrollment Period and guaranteed issue rights.

13
Do you qualify for a guaranteed issue right?Insurance companies are required by law to offer a supplement policy without conditions or constraints on coverage to individuals who meet certain requirements. If you’re applying during your Medigap Open Enrollment Period, which lasts for six months and begins on the first day of the month in which you’re both 65 or older and enrolled in Medicare Part B (for example, you elect Part B upon retirement at age 70), you already have a guaranteed issue right and do not need any of the following to apply to you.
If you are not within your Medigap Open Enrollment Period, any of the following scenarios qualify you for a guaranteed issue right:
1. You were enrolled in an employer group health care plan (including retiree or COBRA coverage) that pays after Medicare pays and your employer group terminated that coverage within the past 63 days.
2. You were enrolled in a Medicare Advantage plan, Program of All Inclusive Care for the Elderly, Health Care Pre-Payment Plan, other Medicare demonstration project or Medicare Select plan, and within the past 63 days:
• The certification of the organization or plan was terminated.
• The plan terminated or discontinued providing coverage in the area in which you reside.
• You moved out of the plan’s service area and are no longer eligible to participate in the plan.
• You voluntarily disenrolled because the plan substantially violated a material provision of the organization’s contract with you. This includes:
– Failing to provide an enrollee, on a timely basis, medically necessary care for which benefits are available under the plan
– Failing to provide covered care in accordance with applicable standards
– The organization, agent or other entity acting on the organization’s behalf, materially misrepresented the plan’s provisions in marketing the plan to you
3. You voluntarily disenrolled from a Medicare Advantage plan within 12 months after the effective date of enrollment, upon first becoming eligible for benefits under Medicare Part A at age 65.
4. You were enrolled in a supplement policy within the past 63 days and one of the following:
• You involuntarily lost coverage due to insolvency of the insurer or bankruptcy of the organization offering the coverage.
• You voluntarily disenrolled because the plan violated a material provision of the policy or the insurer materially misrepresented the policy’s provisions in marketing the policy to you.
5. You terminated enrollment and subsequently enrolled, for the first time, in a Medicare Advantage plan, Medicare Select Plan, Medicare Cost Plan or Program of All Inclusive Care for the Elderly, and the subsequent enrollment was terminated by you within the first 12 months.

14
InstructionsTo find your estimated monthly premium cost, follow these steps:
1. Select a plan option: Plan A, C, D, F, High-Deductible F, G, High-Deductible G or N.
2. Using the following tables:
If you’re in a your Medigap Open Enrollment Period or have a guaranteed issue right, use the tables on Pages 15 through 18 to find your monthly premium.
If you’re not in your Medigap Open Enrollment Period and don’t have a guaranteed issue right, use the tables on Pages 19 through 25.
If you qualify for Conversion Plans A, C or D, use the table on Pages 28 and 29.
If you are younger than 65, use the tables on Pages 26 and 27.
3. Please note that if you turned 65 or became eligible for Medicare after Dec. 31, 2019, you’re not eligible to enroll in a plan that covers the Part B deductible (Plans C, F or High-Deductible F).
Find the plan option that’s right for you.
1. If you live in a ZIP code that begins with 480 through 485, you’re in Area 1.
2. If you live in any other ZIP code in Michigan, you’re in Area 2.
Once you find the correct table, scroll down the first column to find your age. Your premium will be shown at the right, based on whether you’re male or female, and whether you use tobacco if you’re applying outside of a Medigap OEP or have a guaranteed issue right.

15
Monthly premiums for individuals applying
during their Medigap OEP or have a guaranteed issue right(Effective April 1, 2021)
Blue Cross Medicare Supplement Plan A, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $118.64 $112.99 $114.60 $109.15
66 $125.71 $119.15 $121.43 $115.10
67 $132.84 $125.32 $128.32 $121.05
68 $138.93 $130.45 $134.20 $126.01
69 $145.08 $135.59 $140.14 $130.98
70 $150.87 $139.70 $145.74 $134.94
71 $156.75 $143.81 $151.42 $138.91
72 $162.71 $147.91 $157.17 $142.88
73 $168.75 $152.02 $163.00 $146.85
74 $174.87 $156.13 $168.92 $150.82
75 $178.75 $158.19 $172.67 $152.80
76 $182.67 $160.24 $176.46 $154.79
77 $186.64 $162.30 $180.29 $156.77
78 $190.65 $164.35 $184.16 $158.76
79 $194.69 $166.40 $188.07 $160.74
80 and older $198.78 $168.46 $192.02 $162.73
Please note that these rates don’t include the Dental Vision Hearing Package rate.

16
Monthly premiums for individuals applying during their Medigap OEP or have a guaranteed issue right (Continued)
*HD means high-deductible
Blue Cross Medicare Supplement Plan G, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $136.56 $130.06 $131.91 $125.63
66 $147.40 $139.72 $142.38 $134.96
67 $158.33 $149.37 $152.95 $144.29
68 $167.65 $157.42 $161.95 $152.06
69 $177.05 $165.47 $171.03 $159.84
70 $185.66 $171.91 $179.34 $166.06
71 $194.39 $178.34 $187.78 $172.28
72 $203.26 $184.78 $196.34 $178.49
73 $212.25 $191.22 $205.03 $184.71
74 $221.38 $197.66 $213.84 $190.93
75 $226.99 $200.88 $219.27 $194.04
76 $232.67 $204.10 $224.75 $197.15
77 $238.41 $207.32 $230.30 $200.26
78 $244.22 $210.53 $235.91 $203.37
79 $250.09 $213.75 $241.58 $206.48
80 and older
$256.03 $216.97 $247.32 $209.59
Blue Cross Medicare Supplement Plan HD-G*, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $66.72 $63.54 $64.45 $61.38
66 $72.02 $68.26 $69.57 $65.94
67 $77.36 $72.98 $74.73 $70.50
68 $81.91 $76.91 $79.12 $74.29
69 $86.50 $80.84 $83.56 $78.09
70 $90.71 $83.99 $87.62 $81.13
71 $94.98 $87.13 $91.74 $84.17
72 $99.31 $90.28 $95.93 $87.21
73 $103.70 $93.43 $100.17 $90.25
74 $108.16 $96.57 $104.48 $93.28
75 $110.90 $98.14 $107.13 $94.80
76 $113.68 $99.72 $109.81 $96.32
77 $116.48 $101.29 $112.52 $97.84
78 $119.32 $102.86 $115.26 $99.36
79 $122.19 $104.43 $118.03 $100.88
80 and older
$125.09 $106.01 $120.83 $102.40
Please note that these rates don’t include the Dental Vision Hearing Package rate.

17
Blue Cross Medicare Supplement Plan N, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $126.84 $120.80 $122.52 $116.69
66 $136.91 $129.77 $132.25 $125.35
67 $147.06 $138.74 $142.06 $134.02
68 $155.72 $146.21 $150.42 $141.24
69 $164.45 $153.69 $158.85 $148.46
70 $172.44 $159.67 $166.57 $154.23
71 $180.55 $165.65 $174.41 $160.01
72 $188.79 $171.63 $182.37 $165.79
73 $197.14 $177.61 $190.43 $171.56
74 $205.62 $183.59 $198.62 $177.34
75 $210.83 $186.58 $203.66 $180.23
76 $216.10 $189.57 $208.75 $183.12
77 $221.44 $192.56 $213.90 $186.00
78 $226.83 $195.55 $219.11 $188.89
79 $232.29 $198.53 $224.38 $191.78
80 and older
$237.80 $201.52 $229.71 $194.67
Blue Cross Medicare Supplement Plan D, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $147.63 $140.60 $142.61 $135.82
66 $159.35 $151.04 $153.93 $145.90
67 $171.17 $161.48 $165.35 $155.99
68 $181.24 $170.18 $175.08 $164.39
69 $191.40 $178.88 $184.89 $172.79
70 $200.71 $185.84 $193.88 $179.52
71 $210.15 $192.80 $203.00 $186.24
72 $219.74 $199.76 $212.26 $192.96
73 $229.46 $206.72 $221.65 $199.69
74 $239.32 $213.68 $231.18 $206.41
75 $245.39 $217.16 $237.04 $209.77
76 $251.53 $220.64 $242.97 $213.13
77 $257.74 $224.12 $248.97 $216.49
78 $264.02 $227.60 $255.03 $219.86
79 $270.36 $231.08 $261.16 $223.22
80 and older
$276.78 $234.56 $267.36 $226.58

18 *HD means high-deductible
Blue Cross Medicare Supplement Plan F, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $180.71 $172.10 $174.56 $166.25
66 $195.05 $184.88 $188.41 $178.59
67 $209.52 $197.66 $202.39 $190.94
68 $221.85 $208.31 $214.30 $201.22
69 $234.29 $218.96 $226.32 $211.51
70 $245.68 $227.48 $237.32 $219.74
71 $257.24 $236.00 $248.49 $227.97
72 $268.97 $244.52 $259.82 $236.20
73 $280.87 $253.04 $271.31 $244.43
74 $292.94 $261.56 $282.98 $252.66
75 $300.37 $265.82 $290.15 $256.77
76 $307.89 $270.08 $297.41 $260.89
77 $315.49 $274.34 $304.75 $265.00
78 $323.17 $278.60 $312.17 $269.12
79 $330.94 $282.86 $319.68 $273.23
80 and older
$338.80 $287.11 $327.27 $277.35
Blue Cross Medicare Supplement Plan HD-F*, guaranteed issue rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
65 $68.98 $65.69 $66.63 $63.46
66 $74.45 $70.57 $71.92 $68.17
67 $79.98 $75.45 $77.26 $72.88
68 $84.68 $79.52 $81.80 $76.81
69 $89.43 $83.58 $86.39 $80.74
70 $93.78 $86.83 $90.59 $83.88
71 $98.19 $90.08 $94.85 $87.02
72 $102.67 $93.34 $99.18 $90.16
73 $107.21 $96.59 $103.57 $93.30
74 $111.82 $99.84 $108.02 $96.44
75 $114.66 $101.47 $110.76 $98.01
76 $117.53 $103.09 $113.53 $99.58
77 $120.43 $104.72 $116.33 $101.16
78 $123.36 $106.34 $119.16 $102.73
79 $126.33 $107.97 $122.03 $104.30
80 and older
$129.32 $109.60 $124.92 $105.87
Monthly premiums for individuals applying during their Medigap OEP or have a guaranteed issue right (Continued)
Please note that these rates don’t include the Dental Vision Hearing Package rate.
19
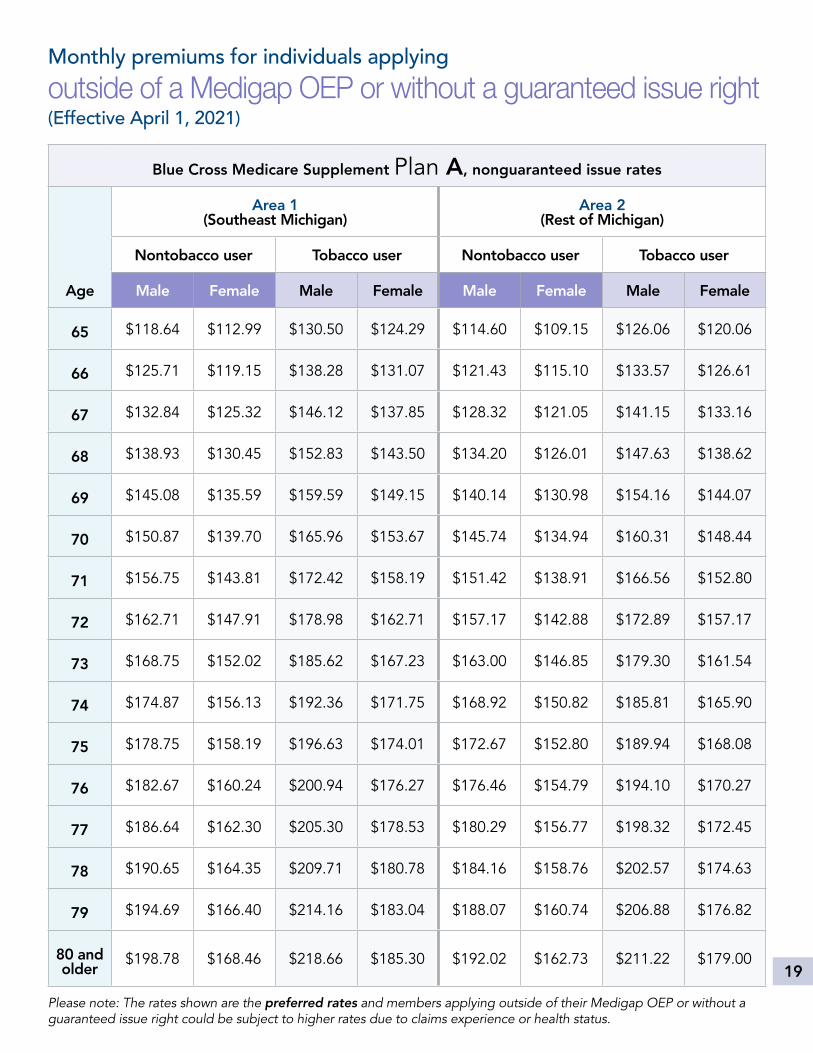
Blue Cross Medicare Supplement Plan A, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $118.64 $112.99 $130.50 $124.29 $114.60 $109.15 $126.06 $120.06
66 $125.71 $119.15 $138.28 $131.07 $121.43 $115.10 $133.57 $126.61
67 $132.84 $125.32 $146.12 $137.85 $128.32 $121.05 $141.15 $133.16
68 $138.93 $130.45 $152.83 $143.50 $134.20 $126.01 $147.63 $138.62
69 $145.08 $135.59 $159.59 $149.15 $140.14 $130.98 $154.16 $144.07
70 $150.87 $139.70 $165.96 $153.67 $145.74 $134.94 $160.31 $148.44
71 $156.75 $143.81 $172.42 $158.19 $151.42 $138.91 $166.56 $152.80
72 $162.71 $147.91 $178.98 $162.71 $157.17 $142.88 $172.89 $157.17
73 $168.75 $152.02 $185.62 $167.23 $163.00 $146.85 $179.30 $161.54
74 $174.87 $156.13 $192.36 $171.75 $168.92 $150.82 $185.81 $165.90
75 $178.75 $158.19 $196.63 $174.01 $172.67 $152.80 $189.94 $168.08
76 $182.67 $160.24 $200.94 $176.27 $176.46 $154.79 $194.10 $170.27
77 $186.64 $162.30 $205.30 $178.53 $180.29 $156.77 $198.32 $172.45
78 $190.65 $164.35 $209.71 $180.78 $184.16 $158.76 $202.57 $174.63
79 $194.69 $166.40 $214.16 $183.04 $188.07 $160.74 $206.88 $176.82
80 and older
$198.78 $168.46 $218.66 $185.30 $192.02 $162.73 $211.22 $179.00
Please note: The rates shown are the preferred rates and members applying outside of their Medigap OEP or without a guaranteed issue right could be subject to higher rates due to claims experience or health status.
Monthly premiums for individuals applying
outside of a Medigap OEP or without a guaranteed issue right(Effective April 1, 2021)
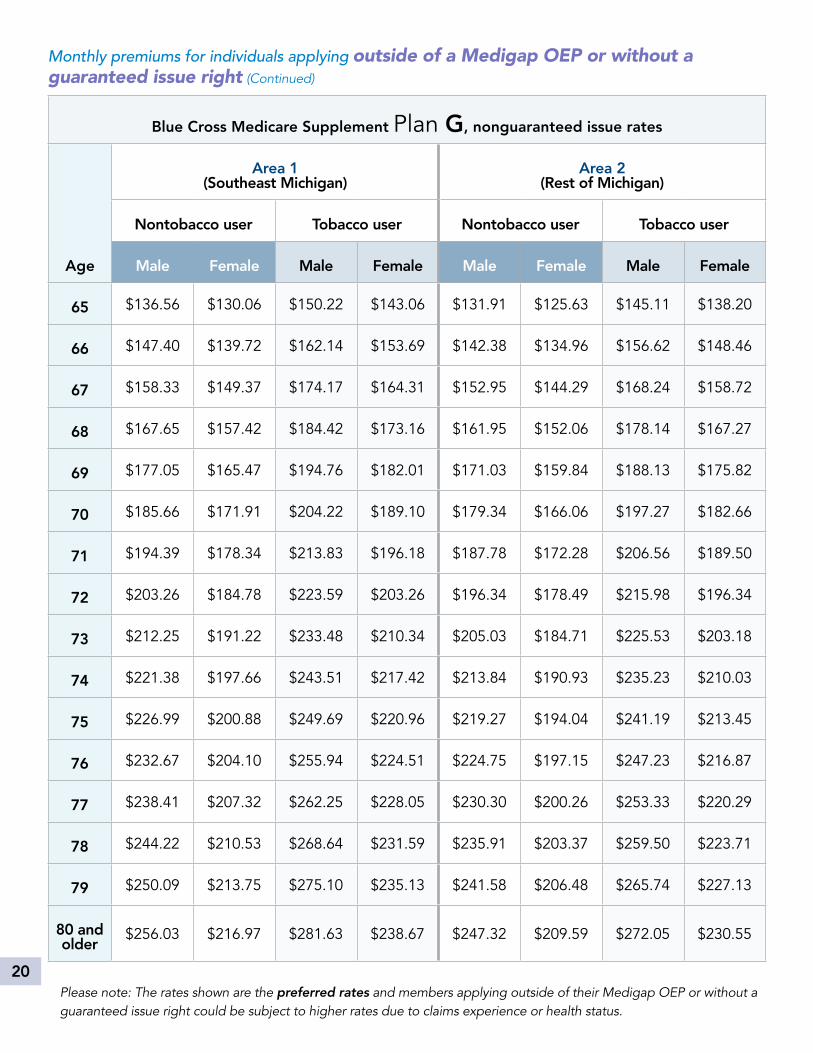
20Please note: The rates shown are the preferred rates and members applying outside of their Medigap OEP or without a guaranteed issue right could be subject to higher rates due to claims experience or health status.
Monthly premiums for individuals applying outside of a Medigap OEP or without a guaranteed issue right (Continued)
Blue Cross Medicare Supplement Plan G, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $136.56 $130.06 $150.22 $143.06 $131.91 $125.63 $145.11 $138.20
66 $147.40 $139.72 $162.14 $153.69 $142.38 $134.96 $156.62 $148.46
67 $158.33 $149.37 $174.17 $164.31 $152.95 $144.29 $168.24 $158.72
68 $167.65 $157.42 $184.42 $173.16 $161.95 $152.06 $178.14 $167.27
69 $177.05 $165.47 $194.76 $182.01 $171.03 $159.84 $188.13 $175.82
70 $185.66 $171.91 $204.22 $189.10 $179.34 $166.06 $197.27 $182.66
71 $194.39 $178.34 $213.83 $196.18 $187.78 $172.28 $206.56 $189.50
72 $203.26 $184.78 $223.59 $203.26 $196.34 $178.49 $215.98 $196.34
73 $212.25 $191.22 $233.48 $210.34 $205.03 $184.71 $225.53 $203.18
74 $221.38 $197.66 $243.51 $217.42 $213.84 $190.93 $235.23 $210.03
75 $226.99 $200.88 $249.69 $220.96 $219.27 $194.04 $241.19 $213.45
76 $232.67 $204.10 $255.94 $224.51 $224.75 $197.15 $247.23 $216.87
77 $238.41 $207.32 $262.25 $228.05 $230.30 $200.26 $253.33 $220.29
78 $244.22 $210.53 $268.64 $231.59 $235.91 $203.37 $259.50 $223.71
79 $250.09 $213.75 $275.10 $235.13 $241.58 $206.48 $265.74 $227.13
80 and older
$256.03 $216.97 $281.63 $238.67 $247.32 $209.59 $272.05 $230.55

21
Blue Cross Medicare Supplement Plan HD-G, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $66.72 $63.54 $73.39 $69.90 $64.45 $61.38 $70.89 $67.52
66 $72.02 $68.26 $79.22 $75.09 $69.57 $65.94 $76.52 $72.53
67 $77.36 $72.98 $85.09 $80.28 $74.73 $70.50 $82.20 $77.55
68 $81.91 $76.91 $90.10 $84.60 $79.12 $74.29 $87.04 $81.72
69 $86.50 $80.84 $95.15 $88.93 $83.56 $78.09 $91.91 $85.90
70 $90.71 $83.99 $99.78 $92.39 $87.62 $81.13 $96.38 $89.24
71 $94.98 $87.13 $104.47 $95.85 $91.74 $84.17 $100.92 $92.59
72 $99.31 $90.28 $109.24 $99.31 $95.93 $87.21 $105.52 $95.93
73 $103.70 $93.43 $114.07 $102.77 $100.17 $90.25 $110.19 $99.27
74 $108.16 $96.57 $118.97 $106.23 $104.48 $93.28 $114.93 $102.61
75 $110.90 $98.14 $121.99 $107.96 $107.13 $94.80 $117.84 $104.28
76 $113.68 $99.72 $125.04 $109.69 $109.81 $96.32 $120.79 $105.96
77 $116.48 $101.29 $128.13 $111.42 $112.52 $97.84 $123.77 $107.63
78 $119.32 $102.86 $131.25 $113.15 $115.26 $99.36 $126.79 $109.30
79 $122.19 $104.43 $134.41 $114.88 $118.03 $100.88 $129.83 $110.97
80 and older
$125.09 $106.01 $137.60 $116.61 $120.83 $102.40 $132.92 $112.64
Please note that these rates don’t include the Dental Vision Hearing Package rate.

22
Blue Cross Medicare Supplement Plan N, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $126.84 $120.80 $139.52 $132.88 $122.52 $116.69 $134.77 $128.36
66 $136.91 $129.77 $150.60 $142.74 $132.25 $125.35 $145.47 $137.89
67 $147.06 $138.74 $161.77 $152.61 $142.06 $134.02 $156.26 $147.42
68 $155.72 $146.21 $171.29 $160.83 $150.42 $141.24 $165.46 $155.36
69 $164.45 $153.69 $180.89 $169.06 $158.85 $148.46 $174.73 $163.30
70 $172.44 $159.67 $189.68 $175.63 $166.57 $154.23 $183.23 $169.66
71 $180.55 $165.65 $198.61 $182.21 $174.41 $160.01 $191.85 $176.01
72 $188.79 $171.63 $207.67 $188.79 $182.37 $165.79 $200.60 $182.37
73 $197.14 $177.61 $216.86 $195.37 $190.43 $171.56 $209.48 $188.72
74 $205.62 $183.59 $226.18 $201.94 $198.62 $177.34 $218.48 $195.07
75 $210.83 $186.58 $231.91 $205.23 $203.66 $180.23 $224.02 $198.25
76 $216.10 $189.57 $237.71 $208.52 $208.75 $183.12 $229.63 $201.43
77 $221.44 $192.56 $243.58 $211.81 $213.90 $186.00 $235.29 $204.60
78 $226.83 $195.55 $249.52 $215.10 $219.11 $188.89 $241.03 $207.78
79 $232.29 $198.53 $255.51 $218.39 $224.38 $191.78 $246.82 $210.96
80 and older
$237.80 $201.52 $261.58 $221.68 $229.71 $194.67 $252.68 $214.13
Monthly premiums for individuals applying outside of a Medigap OEP or without a guaranteed issue right (Continued)
Please note: The rates shown are the preferred rates and members applying outside of their Medigap OEP or without a guaranteed issue right could be subject to higher rates due to claims experience or health status.

23
Blue Cross Medicare Supplement Plan D, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $147.63 $140.60 $162.39 $154.66 $142.61 $135.82 $156.87 $149.40
66 $159.35 $151.04 $175.28 $166.14 $153.93 $145.90 $169.32 $160.49
67 $171.17 $161.48 $188.29 $177.63 $165.35 $155.99 $181.88 $171.58
68 $181.24 $170.18 $199.37 $187.20 $175.08 $164.39 $192.58 $180.83
69 $191.40 $178.88 $210.54 $196.77 $184.89 $172.79 $203.38 $190.07
70 $200.71 $185.84 $220.78 $204.42 $193.88 $179.52 $213.27 $197.47
71 $210.15 $192.80 $231.17 $212.08 $203.00 $186.24 $223.30 $204.86
72 $219.74 $199.76 $241.71 $219.74 $212.26 $192.96 $233.49 $212.26
73 $229.46 $206.72 $252.41 $227.39 $221.65 $199.69 $243.82 $219.66
74 $239.32 $213.68 $263.25 $235.05 $231.18 $206.41 $254.30 $227.05
75 $245.39 $217.16 $269.93 $238.88 $237.04 $209.77 $260.75 $230.75
76 $251.53 $220.64 $276.68 $242.70 $242.97 $213.13 $267.27 $234.45
77 $257.74 $224.12 $283.51 $246.53 $248.97 $216.49 $273.87 $238.14
78 $264.02 $227.60 $290.42 $250.36 $255.03 $219.86 $280.54 $241.84
79 $270.36 $231.08 $297.40 $254.19 $261.16 $223.22 $287.28 $245.54
80 and older
$276.78 $234.56 $304.46 $258.02 $267.36 $226.58 $294.10 $249.24
Please note that these rates don’t include the Dental Vision Hearing Package rate.

24
Blue Cross Medicare Supplement Plan F, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $180.71 $172.10 $198.78 $189.31 $174.56 $166.25 $192.02 $182.87
66 $195.05 $184.88 $214.56 $203.37 $188.41 $178.59 $207.26 $196.45
67 $209.52 $197.66 $230.47 $217.43 $202.39 $190.94 $222.63 $210.03
68 $221.85 $208.31 $244.04 $229.14 $214.30 $201.22 $235.73 $221.34
69 $234.29 $218.96 $257.72 $240.86 $226.32 $211.51 $248.95 $232.66
70 $245.68 $227.48 $270.25 $250.23 $237.32 $219.74 $261.05 $241.71
71 $257.24 $236.00 $282.96 $259.60 $248.49 $227.97 $273.33 $250.77
72 $268.97 $244.52 $295.87 $268.97 $259.82 $236.20 $285.80 $259.82
73 $280.87 $253.04 $308.96 $278.34 $271.31 $244.43 $298.45 $268.87
74 $292.94 $261.56 $322.24 $287.71 $282.98 $252.66 $311.27 $277.92
75 $300.37 $265.82 $330.41 $292.40 $290.15 $256.77 $319.17 $282.45
76 $307.89 $270.08 $338.68 $297.08 $297.41 $260.89 $327.15 $286.98
77 $315.49 $274.34 $347.03 $301.77 $304.75 $265.00 $335.23 $291.50
78 $323.17 $278.60 $355.49 $306.46 $312.17 $269.12 $343.39 $296.03
79 $330.94 $282.86 $364.03 $311.14 $319.68 $273.23 $351.65 $300.55
80 and older
$338.80 $287.11 $372.68 $315.83 $327.27 $277.35 $359.99 $305.08
Monthly premiums for individuals applying outside of a Medigap OEP or without a guaranteed issue right (Continued)
Please note: The rates shown are the preferred rates and members applying outside of their Medigap OEP or without a guaranteed issue right could be subject to higher rates due to claims experience or health status.1HD means high-deductible

25
Blue Cross Medicare Supplement Plan HD-F*, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Nontobacco user Tobacco user Nontobacco user Tobacco user
Male Female Male Female Male Female Male Female
65 $68.98 $65.69 $75.88 $72.26 $66.63 $63.46 $73.30 $69.81
66 $74.45 $70.57 $81.90 $77.63 $71.92 $68.17 $79.11 $74.99
67 $79.98 $75.45 $87.98 $83.00 $77.26 $72.88 $84.98 $80.17
68 $84.68 $79.52 $93.15 $87.47 $81.80 $76.81 $89.98 $84.49
69 $89.43 $83.58 $98.37 $91.94 $86.39 $80.74 $95.03 $88.81
70 $93.78 $86.83 $103.16 $95.52 $90.59 $83.88 $99.65 $92.27
71 $98.19 $90.08 $108.01 $99.09 $94.85 $87.02 $104.34 $95.72
72 $102.67 $93.34 $112.94 $102.67 $99.18 $90.16 $109.09 $99.18
73 $107.21 $96.59 $117.93 $106.25 $103.57 $93.30 $113.92 $102.63
74 $111.82 $99.84 $123.00 $109.82 $108.02 $96.44 $118.82 $106.09
75 $114.66 $101.47 $126.12 $111.61 $110.76 $98.01 $121.83 $107.82
76 $117.53 $103.09 $129.28 $113.40 $113.53 $99.58 $124.88 $109.54
77 $120.43 $104.72 $132.47 $115.19 $116.33 $101.16 $127.96 $111.27
78 $123.36 $106.34 $135.70 $116.98 $119.16 $102.73 $131.08 $113.00
79 $126.33 $107.97 $138.96 $118.77 $122.03 $104.30 $134.23 $114.73
80 and older
$129.32 $109.60 $142.26 $120.56 $124.92 $105.87 $137.42 $116.45
Please note that these rates don’t include the Dental Vision Hearing Package rate.
26
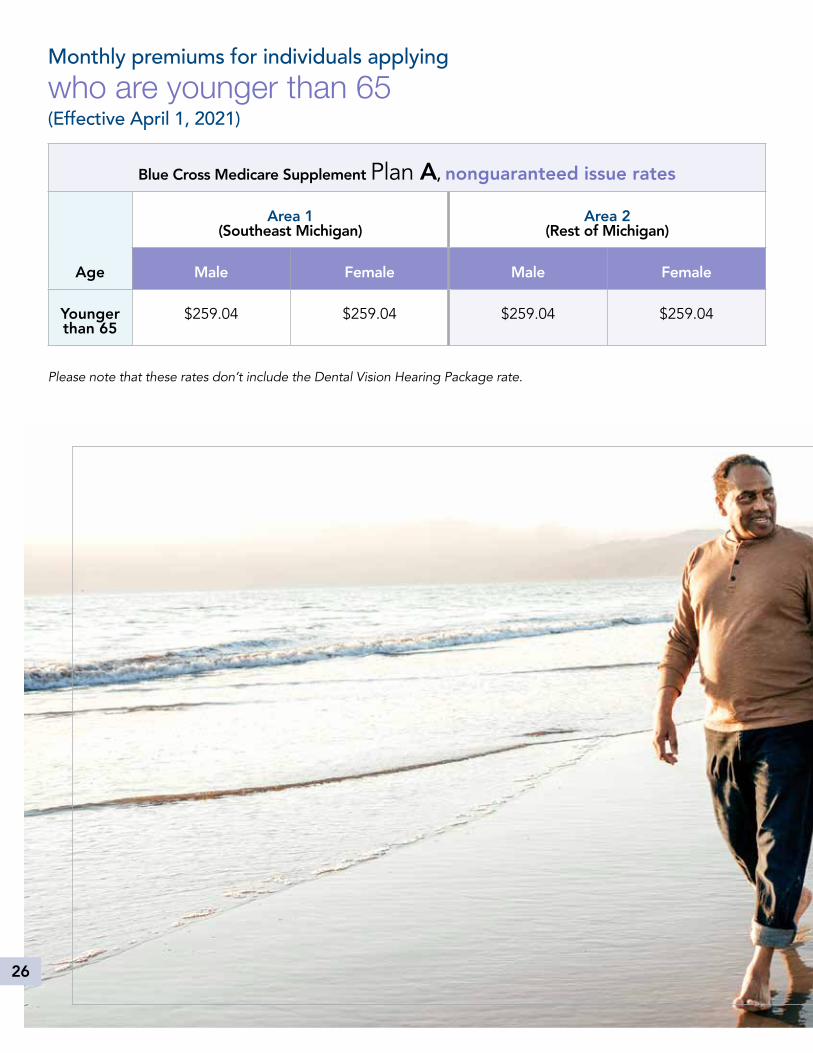
Monthly premiums for individuals applying
who are younger than 65 (Effective April 1, 2021)
Blue Cross Medicare Supplement Plan A, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Male Female Male Female
Younger than 65
$259.04 $259.04 $259.04 $259.04
Please note that these rates don’t include the Dental Vision Hearing Package rate.

27
Blue Cross Medicare Supplement Plan D, nonguaranteed issue rates
Age
Area 1 (Southeast Michigan)
Area 2 (Rest of Michigan)
Male Female Male Female
Younger than 65
$528.79 $528.79 $528.79 $528.79

28
Blue Cross Medicare Supplement Plan A, conversion rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
Under age 65 $259.04 $259.04 $259.04 $259.04
65 $118.64 $112.99 $114.60 $109.15
66 $125.71 $119.15 $121.43 $115.10
67 $132.84 $125.32 $128.32 $121.05
68 $138.93 $130.45 $134.20 $126.01
69 $145.08 $135.59 $140.14 $130.98
70 $150.87 $139.70 $145.74 $134.94
71 $156.75 $143.81 $151.42 $138.91
72 $162.71 $147.91 $157.17 $142.88
73 $168.75 $152.02 $163.00 $146.85
74 $174.87 $156.13 $168.92 $150.82
75 $178.75 $158.19 $172.67 $152.80
76 $182.67 $160.24 $176.46 $154.79
77 $186.64 $162.30 $180.29 $156.77
78 $190.65 $164.35 $184.16 $158.76
79 $194.69 $166.40 $188.07 $160.74
80 and older $198.78 $168.46 $192.02 $162.73
See important information about Plans A, C and D on page 12.
Blue Cross Medicare Supplement Plan D, conversion rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
Under age 65 $528.79 $528.79 $528.79 $528.79
65 $147.63 $140.60 $142.61 $135.82
66 $159.35 $151.04 $153.93 $145.90
67 $171.17 $161.48 $165.35 $155.99
68 $181.24 $170.18 $175.08 $164.39
69 $191.40 $178.88 $184.89 $172.79
70 $200.71 $185.84 $193.88 $179.52
71 $210.15 $192.80 $203.00 $186.24
72 $219.74 $199.76 $212.26 $192.96
73 $229.46 $206.72 $221.65 $199.69
74 $239.32 $213.68 $231.18 $206.41
75 $245.39 $217.16 $237.04 $209.77
76 $251.53 $220.64 $242.97 $213.13
77 $257.74 $224.12 $248.97 $216.49
78 $264.02 $227.60 $255.03 $219.86
79 $270.36 $231.08 $261.16 $223.22
80 and older $276.78 $234.56 $267.36 $226.58
Monthly premiums for individuals, who qualify for
conversion, applying for Plans A, D and C (Effective April 1, 2021)
If you were eligible for Medicare on or after January 1, 2020, you are not eligible for Plan C.
Refer to Page 12 for additional information on conversion members.

29
Blue Cross Medicare Supplement Plan C, conversion rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
Under age 65 $412.12 $412.12 $412.12 $412.12
65 $203.44 $193.75 $196.52 $187.16
66 $215.56 $204.32 $208.23 $197.37
67 $227.78 $214.89 $220.03 $207.58
68 $238.24 $223.70 $230.13 $216.09
69 $248.78 $232.50 $240.31 $224.59
70 $258.71 $239.55 $249.91 $231.40
71 $268.79 $246.60 $259.64 $238.21
72 $279.01 $253.64 $269.51 $245.01
73 $289.36 $260.69 $279.52 $251.82
74 $299.86 $267.73 $289.66 $258.62
75 $306.52 $271.26 $296.09 $262.03
76 $313.25 $274.78 $302.59 $265.43
77 $320.05 $278.30 $309.16 $268.83
78 $326.92 $281.82 $315.79 $272.23
79 $333.86 $285.35 $322.50 $275.64
80 and older $340.87 $288.87 $329.27 $279.04
Blue Cross Medicare Supplement Plan D, conversion rates
Age
Area 1(Southeast Michigan)
Area 2(Rest of Michigan)
Male Female Male Female
Under age 65 $528.79 $528.79 $528.79 $528.79
65 $147.63 $140.60 $142.61 $135.82
66 $159.35 $151.04 $153.93 $145.90
67 $171.17 $161.48 $165.35 $155.99
68 $181.24 $170.18 $175.08 $164.39
69 $191.40 $178.88 $184.89 $172.79
70 $200.71 $185.84 $193.88 $179.52
71 $210.15 $192.80 $203.00 $186.24
72 $219.74 $199.76 $212.26 $192.96
73 $229.46 $206.72 $221.65 $199.69
74 $239.32 $213.68 $231.18 $206.41
75 $245.39 $217.16 $237.04 $209.77
76 $251.53 $220.64 $242.97 $213.13
77 $257.74 $224.12 $248.97 $216.49
78 $264.02 $227.60 $255.03 $219.86
79 $270.36 $231.08 $261.16 $223.22
80 and older $276.78 $234.56 $267.36 $226.58

30
Premium informationFor Blue Cross Medicare Supplement plans, certain factors may affect your monthly premium cost. We base your premium on the area you live in and your age, gender, and in some situations, health status and whether you use tobacco. When we base your premium on health status and whether you use tobacco, this is called medical underwriting.
Please note: If you’re submitting your application during your Medigap OEP or have a guaranteed issue right, your rate won’t be affected by your tobacco use, health status, claims experience, receipt of health care or medical condition.
Your premium may change if you move into a different rating area. Other than premium adjustments due to age or relocation, we can only raise your premium if we raise the premium for all policies like yours. All premiums in this booklet are subject to change on April 1, 2022.
Disenrollment may occur if premium payments aren’t received by the due date. In such cases, there will be a six-month waiting period before you’re eligible to reapply.
Your payment options
You may make payments through authorized automatic deductions from your bank account or by personal check, money order, cashier’s check or credit card. See the enrollment application for details on payment methods. Premium payments are due the 25th of each month.
31
Choose a plan option that meets your needs.The chart on Pages 32 through 35 outlines the coverage options offered by Blue Cross plans A, C, D, F, High-Deductible F, G, High-Deductible G and N. This Outline of Coverage doesn’t give all the details of Medicare coverage. For information about your Medicare Part A and Part B coverage, contact your local Social Security office or consult Medicare & You (online at www.medicare.gov*). Medicare benefits are subject to change. Please consult the latest Choosing a Medigap Policy: Guide to Health Insurance for People with Medicare, which can be found online at www.medicare.gov*.
The Blue Cross Medicare Supplement plan may not fully cover all of your medical costs. When you receive covered services from a provider who doesn’t accept Medicare assignment, you’re responsible for the difference between the provider’s charge and the Medicare-approved amount, plus any deductible or coinsurance amounts required by the Blue Cross Medicare Supplement plan you select.
Once enrolled in Blue Cross Medicare Supplement, we’ll send you a member ID card and plan handbook that provides comprehensive details about your coverage. We’ll also give you a Certificate of Coverage. It’s your legal contract with Blue Cross. We encourage you to read the certificate to understand all of the rights and duties of both you and Blue Cross. For more information about Blue Cross Medicare Supplement coverage, call 1-888-563-3307 or contact an insurance agent authorized to sell Blue Cross policies. TTY users should call 711.
*Blue Cross Blue Shield of Michigan doesn’t own or control this website.

32
Outline of coverageThe Medicare deductibles, coinsurance and copay amounts listed are based upon the 2021 CMS-approved values and could change for 2022.
Covered service Plan option Plan A1 Plan C1 Plan D1
Medicare pays Plan pays You pay Plan pays You pay Plan pays You payMedicare Part A hospital coverage — Semi-private room, general nursing care, miscellaneous services and supplies2
Deductible $0 $0 $1,484 $1,484 $0 $1,484 $0First 60 days of care 100% $0 $0 $0 $0 $0 $0Days 61 to 90 All but the $371
daily copay$371 daily copay $0 $371 daily copay $0 $371 daily copay $0
Days 91 to 150 (lifetime reserve days)
All but the $742 daily copay
$742 daily copay $0 $742 daily copay $0 $742 daily copay $0
Day 151 and beyond (additional 365 days after lifetime reserve days used)
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0 100% of Medicare- eligible expenses
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Skilled nursing facility care — including having been in a hospital for at least three daysFirst 20 days of care 100% $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)Days 21 to 100 All but $185.50
daily skilled nursing facility copay
$0 $185.50 daily copay $185.50 daily copay $0 $185.50 daily copay $0
Hospice careAll but very limited
copay/coinsurance for outpatient drugs and inpatient respite care
Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0
Emergency care outside the U.S.No benefits for care
outside U.S.No benefits for care
outside U.S.All costs2 for services 80% of approved amount
for covered services after $250 deductible
is met. Lifetime maximum of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
Medicare Part B physician and outpatient services — In- or out-of-the-hospital and outpatient hospital physician’s services (such as tests), and durable medical equipment, per calendar yearDeductible (annual)3 $0 $0 $203 $203 $0 $0 $203Coinsurance 80% of the approved
amount after $203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Clinical laboratory services — tests for diagnostic services
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Home health care services — Medicare-approved servicesMedically necessary skilled care services and medical supplies
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Durable medical equipment 80% of the approved amount after the
$203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Excess charges $0 $0 All costs2 $0 All costs2 $0 All costs2
1See Important Information about Plans A, C and D on Page 12. 2Per benefit period. A benefit period begins on the first day you receive services as an inpatient in a hospital and ends after you’ve been out of the hospital and haven’t received skilled nursing care in any other facility for 60 consecutive days.3The Part B deductible needs to be met only once each calendar year (Jan. 1 through Dec. 31). After, Medicare makespayments up to the limiting charge established by law and shown on your Medicare explanation of benefits.

33
Covered service Plan option Plan A1 Plan C1 Plan D1
Medicare pays Plan pays You pay Plan pays You pay Plan pays You payMedicare Part A hospital coverage — Semi-private room, general nursing care, miscellaneous services and supplies2
Deductible $0 $0 $1,484 $1,484 $0 $1,484 $0First 60 days of care 100% $0 $0 $0 $0 $0 $0Days 61 to 90 All but the $371
daily copay$371 daily copay $0 $371 daily copay $0 $371 daily copay $0
Days 91 to 150 (lifetime reserve days)
All but the $742 daily copay
$742 daily copay $0 $742 daily copay $0 $742 daily copay $0
Day 151 and beyond (additional 365 days after lifetime reserve days used)
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0 100% of Medicare- eligible expenses
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Skilled nursing facility care — including having been in a hospital for at least three daysFirst 20 days of care 100% $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)Days 21 to 100 All but $185.50
daily skilled nursing facility copay
$0 $185.50 daily copay $185.50 daily copay $0 $185.50 daily copay $0
Hospice careAll but very limited
copay/coinsurance for outpatient drugs and inpatient respite care
Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0
Emergency care outside the U.S.No benefits for care
outside U.S.No benefits for care
outside U.S.All costs2 for services 80% of approved amount
for covered services after $250 deductible
is met. Lifetime maximum of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
Medicare Part B physician and outpatient services — In- or out-of-the-hospital and outpatient hospital physician’s services (such as tests), and durable medical equipment, per calendar yearDeductible (annual)3 $0 $0 $203 $203 $0 $0 $203Coinsurance 80% of the approved
amount after $203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Clinical laboratory services — tests for diagnostic services
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Home health care services — Medicare-approved servicesMedically necessary skilled care services and medical supplies
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Durable medical equipment 80% of the approved amount after the
$203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Excess charges $0 $0 All costs2 $0 All costs2 $0 All costs2
34
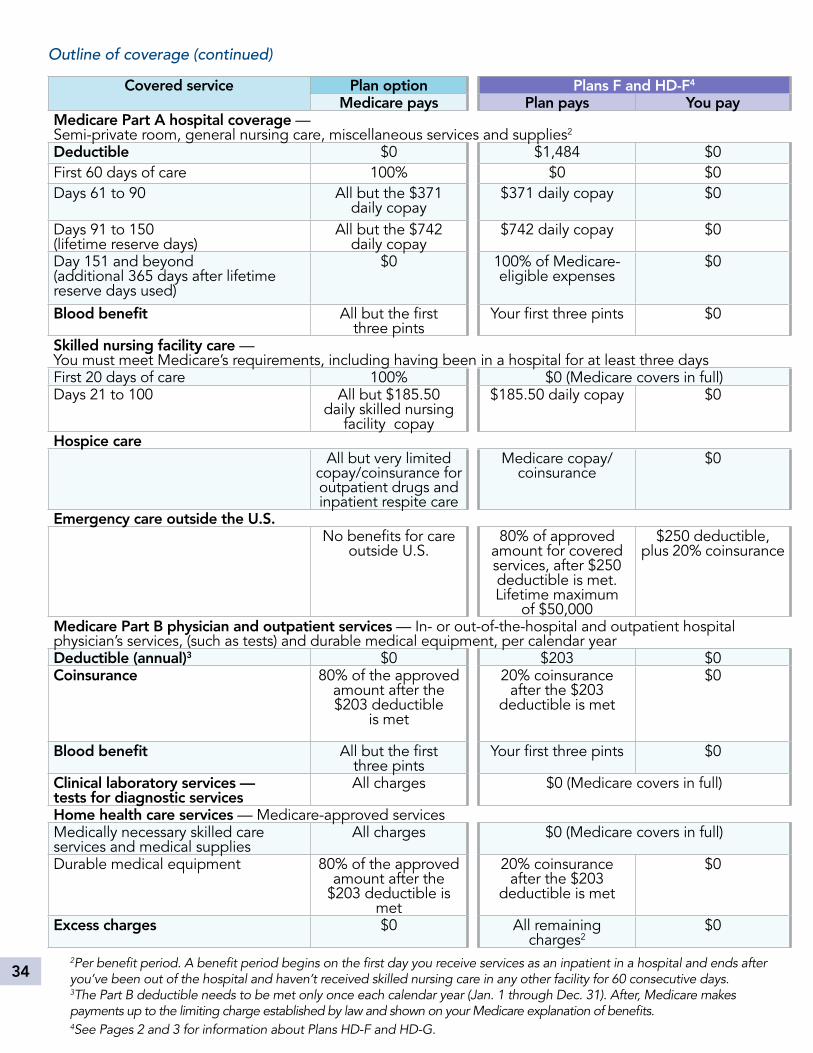
Outline of coverage (continued)
Covered service Plan option Plans F and HD-F4 Plans G and HD-G4 Plan NMedicare pays Plan pays You pay Plan pays You pay Plan pays You pay
Medicare Part A hospital coverage — Semi-private room, general nursing care, miscellaneous services and supplies2
Deductible $0 $1,484 $0 $1,484 $0 $1,484 $0First 60 days of care 100% $0 $0 $0 $0 $0 $0Days 61 to 90 All but the $371
daily copay$371 daily copay $0 $371 daily copay $0 $371 daily copay $0
Days 91 to 150 (lifetime reserve days)
All but the $742 daily copay
$742 daily copay $0 $742 daily copay $0 $742 daily copay $0
Day 151 and beyond (additional 365 days after lifetime reserve days used)
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Skilled nursing facility care — You must meet Medicare’s requirements, including having been in a hospital for at least three daysFirst 20 days of care 100% $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)Days 21 to 100 All but $185.50
daily skilled nursing facility copay
$185.50 daily copay $0 $185.50 daily copay $0 $185.50 daily copay $0
Hospice careAll but very limited
copay/coinsurance for outpatient drugs and inpatient respite care
Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0
Emergency care outside the U.S.No benefits for care
outside U.S.80% of approved
amount for covered services, after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services,
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services,
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
Medicare Part B physician and outpatient services — In- or out-of-the-hospital and outpatient hospital physician’s services, (such as tests) and durable medical equipment, per calendar yearDeductible (annual)3 $0 $203 $0 $0 $203 $0 $203Coinsurance 80% of the approved
amount after the $203 deductible
is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 Balance, other than up to $20 per office visit and
up to $50 per emergency room visit, after the $203
deductible is met
Up to $20 per office visit and up to $50 per emergency room visit
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Clinical laboratory services — tests for diagnostic services
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Home health care services — Medicare-approved servicesMedically necessary skilled care services and medical supplies
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Durable medical equipment 80% of the approved amount after the
$203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Excess charges $0 All remaining charges2
$0 All remaining charges2 $0 $0 All remaining charges2
2Per benefit period. A benefit period begins on the first day you receive services as an inpatient in a hospital and ends after you’ve been out of the hospital and haven’t received skilled nursing care in any other facility for 60 consecutive days.3The Part B deductible needs to be met only once each calendar year (Jan. 1 through Dec. 31). After, Medicare makes payments up to the limiting charge established by law and shown on your Medicare explanation of benefits.4See Pages 2 and 3 for information about Plans HD-F and HD-G.

35
Covered service Plan option Plans F and HD-F4 Plans G and HD-G4 Plan NMedicare pays Plan pays You pay Plan pays You pay Plan pays You pay
Medicare Part A hospital coverage — Semi-private room, general nursing care, miscellaneous services and supplies2
Deductible $0 $1,484 $0 $1,484 $0 $1,484 $0First 60 days of care 100% $0 $0 $0 $0 $0 $0Days 61 to 90 All but the $371
daily copay$371 daily copay $0 $371 daily copay $0 $371 daily copay $0
Days 91 to 150 (lifetime reserve days)
All but the $742 daily copay
$742 daily copay $0 $742 daily copay $0 $742 daily copay $0
Day 151 and beyond (additional 365 days after lifetime reserve days used)
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0 100% of Medicare-eligible expenses
$0
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Skilled nursing facility care — You must meet Medicare’s requirements, including having been in a hospital for at least three daysFirst 20 days of care 100% $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)Days 21 to 100 All but $185.50
daily skilled nursing facility copay
$185.50 daily copay $0 $185.50 daily copay $0 $185.50 daily copay $0
Hospice careAll but very limited
copay/coinsurance for outpatient drugs and inpatient respite care
Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0 Medicare copay/coinsurance
$0
Emergency care outside the U.S.No benefits for care
outside U.S.80% of approved
amount for covered services, after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services,
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
80% of approved amount for covered services,
after $250 deductible is met. Lifetime maximum
of $50,000
$250 deductible, plus 20% coinsurance
Medicare Part B physician and outpatient services — In- or out-of-the-hospital and outpatient hospital physician’s services, (such as tests) and durable medical equipment, per calendar yearDeductible (annual)3 $0 $203 $0 $0 $203 $0 $203Coinsurance 80% of the approved
amount after the $203 deductible
is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 Balance, other than up to $20 per office visit and
up to $50 per emergency room visit, after the $203
deductible is met
Up to $20 per office visit and up to $50 per emergency room visit
Blood benefit All but the first three pints
Your first three pints $0 Your first three pints $0 Your first three pints $0
Clinical laboratory services — tests for diagnostic services
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Home health care services — Medicare-approved servicesMedically necessary skilled care services and medical supplies
All charges $0 (Medicare covers in full) $0 (Medicare covers in full) $0 (Medicare covers in full)
Durable medical equipment 80% of the approved amount after the
$203 deductible is met
20% coinsurance after the $203
deductible is met
$0 20% coinsurance after the $203 deductible is met
$0 20% coinsurance after the $203 deductible is met
$0
Excess charges $0 All remaining charges2
$0 All remaining charges2 $0 $0 All remaining charges2

36
You can have dental, vision and hearing benefits added to your plan for a low cost of $15.251. Your benefits can begin as early as April 1, 2021, and include the following great coverage ...
Dental Vision Hearing Package
Basic dental services
In network Out of network
Waiting period None
Deductible $0 $0
Two routine exams Two cleanings
One X-ray (every two calendar years)
One of the following: - One set of up to four bitewings - Six periapicalFluorideBrush biopsy
0% coinsurance 50% coinsurance
Annual maximumCombined in and out of network. Applies to services below.
$1,500
Amalgam and resin fillings
Root canals
Simple extractions
Crown repairs
Crowns
50% coinsurance 50% coinsurance
Vision services
In network Out of network
Waiting period None
Frames or Elective contact lenses
$300 allowance for frames
or elective contact lenses
every 12 months
Frames reimbursed up to $70
orcontact lenses
reimbursed up to $105 every 12 months
LensesStandard lenses
are covered in full every 12 months
Reimbursement up to –Single vision lenses: $30
Bifocal lenses: $50Trifocal lenses: $65
Lenticular lenses: $100every 12 months
Exam Covered after $20 copay every 12 months
Reimbursed up to $45 every 12 months

37
Vision services
In network Out of network
Waiting period None
Frames or Elective contact lenses
$300 allowance for frames
or elective contact lenses
every 12 months
Frames reimbursed up to $70
orcontact lenses
reimbursed up to $105 every 12 months
LensesStandard lenses
are covered in full every 12 months
Reimbursement up to –Single vision lenses: $30
Bifocal lenses: $50Trifocal lenses: $65
Lenticular lenses: $100every 12 months
Exam Covered after $20 copay every 12 months
Reimbursed up to $45 every 12 months
Hearing services
TruHearing® network
Waiting period None
Hearing aidsYour payment (per ear)
$495 / $895 / $1,295 / $1,695
Hearing exam Included
Frequency One hearing aid per ear every 12 months
1Premium for the Dental Vision Hearing Package will be re-evaluated each year and is subject to change.

38
Enrolling is easyYou can apply for coverage for a Blue Cross Medicare Supplement plan online at www.bcbsm.com/medicare-supplement, by contacting a Blue Cross Blue Shield of Michigan agent, or by calling 1-888-563-3307. TTY users, call 711.
You can also complete a paper application and send it to one of the following:
Mail: Blue Cross Blue Shield of MichiganP.O. Box 44407 Detroit, MI 48244-0407
Fax: 1-866-392-7528
Use one application for each person. Be sure to answer truthfully and completely all questions about your medical and health history (if outside a Medigap OEP or you don’t have a guaranteed issue right). Blue Cross may increase your rates, cancel your policy or refuse to pay any claims if you leave out or falsify important medical information or information about your permanent residence, date of birth, health status or tobacco use. If applicable, indicate that you’re switching to a supplement plan from your current coverage. We’ll help you enroll and ensure that you have no lapse in coverage.
If you’re covered under a health policy from any other insurer, don’t cancel that coverage until you receive your Quick Start Guide from Blue Cross Medicare Supplement and are sure you want to keep your plan. We’ll mail a booklet when we enroll you in the plan. If you have questions, please call the number on the back of your Blue Cross member ID card or contact your agent. TTY users, call 711.
Whether you’re applying for coverage online or through an authorized insurance agent, it’s important to know that neither Blue Cross nor its authorized agents are connected with Medicare.
Blue Cross®
Medicare Supplement
Plans A, C, D, F, High-Deductible F,
G, High-Deductible G and N
Application
20 21

39
Changing your coverageYou may switch to a different Blue Cross Medicare Supplement policy at any time, but you may be subject to medical underwriting1. If you’re switching to a Medicare Advantage plan, you can enroll only during certain times of the year.
Important: If you’re currently enrolled in a Medicare Advantage plan and wish to enroll in Medicare supplement, you must separately disenroll in writing from Medicare Advantage. Submitting this application doesn’t automatically disenroll you from your current Medicare Advantage insurance carrier. Call your Medicare Advantage Customer Service department for information on how to disenroll from that plan and prevent duplication of coverage or a lapse in coverage. Medicare Advantage plans only allow disenrollment at certain times of the year.
Do you also need prescription drug coverage?You may purchase Medicare Part D drug coverage with Blue Cross Blue Shield of Michigan’s Prescription BlueSM PDP plan. Call 1-888-563-3307. (TTY users, call 711).
You may cancel this coverage if it’s not right for youIf you find that you aren’t satisfied with Blue Cross Medicare Supplement coverage, notify us by phone, fax or write to us at the address below within the first 30 days of your coverage. We’ll treat the coverage as if it had never been issued and return all of your payments, less the reasonable cost of any health services paid by Blue Cross during that time. You’ll be responsible for any deductibles or coinsurance for Medicare Part A and Part B claims, or any services not covered by Original Medicare incurred during that 30-day period.
If you choose to cancel your Blue Cross Medicare Supplement coverage after the first 30 days, the signature of the policy holder or legal representative is required.
Do one of the following:
Call the Customer Service number on the back of your Blue Cross member ID card. TTY users, call 711.
Mail:Blue Cross Blue Shield of MichiganP.O. Box 44407 Detroit, MI 48244-0407
Fax: 1-866-392-7528
1Please see Page 10 for more information on what medical underwriting is.

40
Notes

41
Notes

To enroll in a Blue Cross Medicare Supplement plan:
Contact your Blue Cross Blue Shield of Michigan agent.
Enroll online at www.bcbsm.com/medicare-supplement.
Call 1-888-563-3307 (TTY: 711) 8 a.m. to 9 p.m. Eastern time, Monday through Friday, with weekend hours from Oct. 1 through March 31.
DB 18494 JAN 21 W003381
www.bcbsm.com/medicare-supplement
This outline of Medicare Supplement coverage is a summary only. Specific provisions for coverage, limitations and exclusions are contained in certificates and, if applicable, riders to those certificates. Although every effort
has been made to accurately describe the benefits, if there is a discrepancy between this outline and applicable certificates and riders, the certificates and riders will govern.
This request for information is insurance related and if you respond you may be contacted in an attempt to sell you insurance. Blue Cross Medicare Supplement is not connected with or endorsed
by the U.S. government or the federal Medicare program.
Blue Cross does not control the third-party websites referred to in this publication and is not responsible for their content.
This document is the Blue Cross Medicare Supplement outline of coverage, and the details and exceptions of Blue Cross Medicare Supplement follow. The deductible, coinsurance and copay amounts listed in this brochure are based on the 2021 CMS-approved values and could change for 2022. Like Medicare, Blue Cross Medicare Supplement coverage is accepted nationwide and the plan is easy to use. There are no provider networks or referrals — just use any health care provider who accepts Medicare. Simply present your Blue Cross Medicare Supplement member ID card along with your red, white and blue Medicare health insurance card whenever you receive health care services. We’ll coordinate payment with Medicare and your health care providers. In most cases, you’ll never have to bother with claim filing or paperwork.