Blood Transfusion - Simply Revision - Home · 2018-09-06 · Blood products Packed Red Cells 1 unit...
42
Blood Transfusion Dr William Dooley
Transcript of Blood Transfusion - Simply Revision - Home · 2018-09-06 · Blood products Packed Red Cells 1 unit...

Blood Transfusion
Dr William Dooley

Plan
• Cases
• OSCE practice scenario
• Blood groups / Indications
• Monitoring / Reactions

CasesFor following cases: - Would you give them a blood transfusion? - How many units you would prescribe? - What other investigations/management would you consider?
1. Miss Irene Bleede, 23 yo asymptomatic, healthy woman with menorrhagia
Hb 84 g/l, MCV 73fl
2. Mr Oliver Negg, 86 yo asymptomatic man with occasional anginaHb 96 g/l, MCV 104fl
3. Mr Oscar Dere, 73 yo man presenting with acute upper GI bleedBP 80/60, Pulse 120 thready. Hb 82 g/dl, MCV 101fl
4. Mrs A Smith, 35yo woman post Caesarean Section, blood loss 2000mls. Seen on Day 1: obs stable. Hb 66 g/dl (pre op 112)

Cases1. Miss I Bleede, 23 yo asymptomatic, healthy woman with
menorrhagiaHb 84 g/l, MCV 73fl
Microcytic anaemia Iron deficiencyMx: Oral iron replacement (e.g. Ferrous Sulphate 200mg TDS)No transfusion requiredIx: If severe
2. Mr O Negg, 86 yo asymptomatic man with occasional anginaHb 96 g/l, MCV 104fl
Macrocytic anaemia Mx: Treat causeIx: ?cause: alcohol, meds, hypothyroidism, haemolysis

3. Mr O Dere, 73 yo man presenting with acute/severe upper GI bleed BP 80/60, Pulse 120 thready. Hb 82 g/l, MCV 101fl
Acute anaemia Mx: Stabilise (ABCDE)
Cross Match and transfuse 4-6 unitsUrgent OGD
Ix: Clotting screen
4. Mrs A Smith, 35yo woman post Caesarean Section, blood loss 2000mls. Obs stable. Day 1 Hb 66 g/dl (pre op 101)
Acute anaemia from blood lossMx: Advise blood transfusion
Cases

Indications for Blood Transfusion
Acute Anaemia (rarely chronic anaemia)Symptomatic anaemia and blood lossPeri-operative: ‘replacing losses’Haemolysis (treat underlying cause)
Case-case basisCo-morbidities SymptomsPatient choice
Threshold of Hb? Hb < 70 g/L transfusion is usually indicated (NICE 2015)Hb < 80 g/L if acute coronary syndrome
Alternatives? Iron transfusion or Oral iron replacement
Blood products
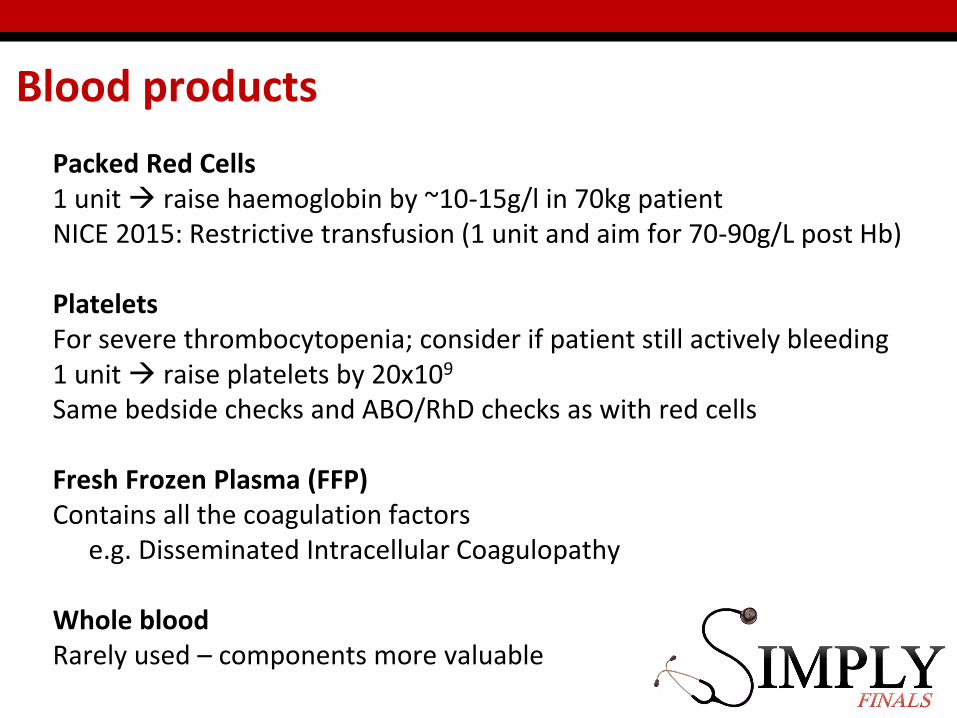
Packed Red Cells1 unit raise haemoglobin by ~10-15g/l in 70kg patientNICE 2015: Restrictive transfusion (1 unit and aim for 70-90g/L post Hb)
Platelets For severe thrombocytopenia; consider if patient still actively bleeding1 unit raise platelets by 20x109
Same bedside checks and ABO/RhD checks as with red cells
Fresh Frozen Plasma (FFP)Contains all the coagulation factors
e.g. Disseminated Intracellular Coagulopathy
Whole blood Rarely used – components more valuable
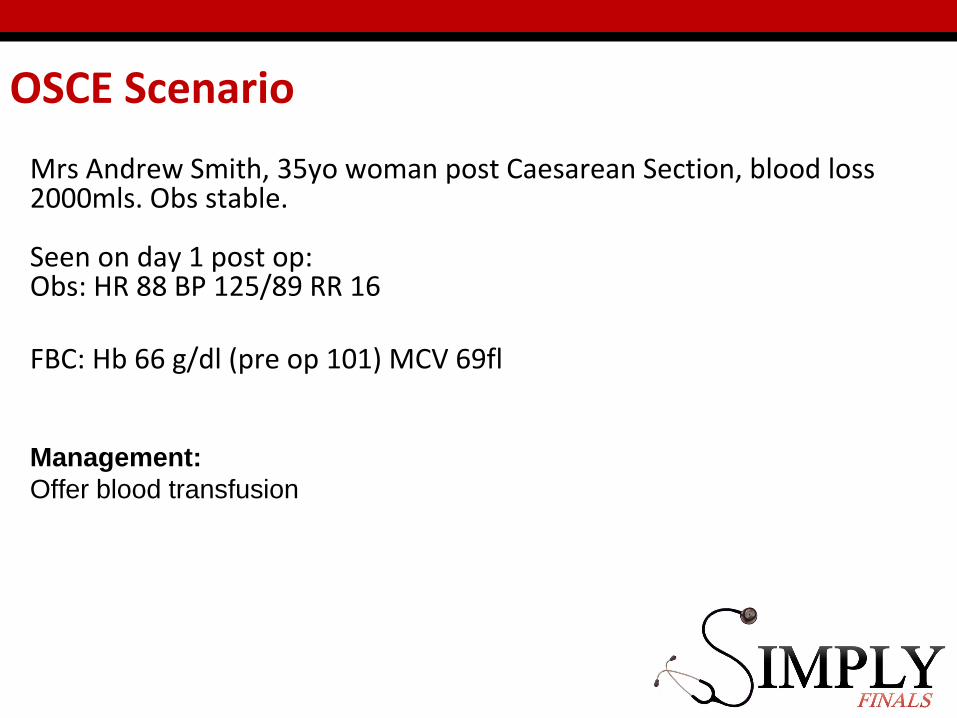
Mrs Andrew Smith, 35yo woman post Caesarean Section, blood loss 2000mls. Obs stable.
Seen on day 1 post op: Obs: HR 88 BP 125/89 RR 16
FBC: Hb 66 g/dl (pre op 101) MCV 69fl
Management:
Offer blood transfusion
OSCE Scenario

Transfusion discussion

1. Indication / Benefits
1. Risks (Inform patient that following a blood transfusion they can no longer be a blood donor)
2. Alternatives
3. How administered
4. Provide written information. Offer time to consider
5. Document discussion
Transfusion discussion

Chronic: Infections
Risk of HIV per unit transfused = 1 in 6 millionRisk of Hep B per unit transfused = 1 in 1.3 millionRisk of Hep C per unit transfused = 1 in 28 million
All tested for Hep B / Hep C / HIV 1&2 / Human T-cell lymphotropicvirus / syphilis +/- CMV and malaria
Risk = asymptomatic window period

Taking blood sample

Taking blood sample
Positive identification- Full name and DOBConfirm with ID wrist band and request form
Group and Save vs Cross Match
Write details on blood bottle after blood added and at bedside1. Who? Name/DOB/hospital number2. Where? Location3. When? Date/time4. Who?? Signature
Prescribing Blood
Prescribing Blood
Different at different Trusts – but principles the same
Usually on separate blood transfusion chart, prescribe:
“PACKED RED CELLS”
Timing: Needs to be complete in 4 hours (so logistically usually over 1-3 hours)
Same prescribing principles as with normal meds: Who? Sign/Print name/Contact numberWhen? Date/Time
Pre Transfusion Checks

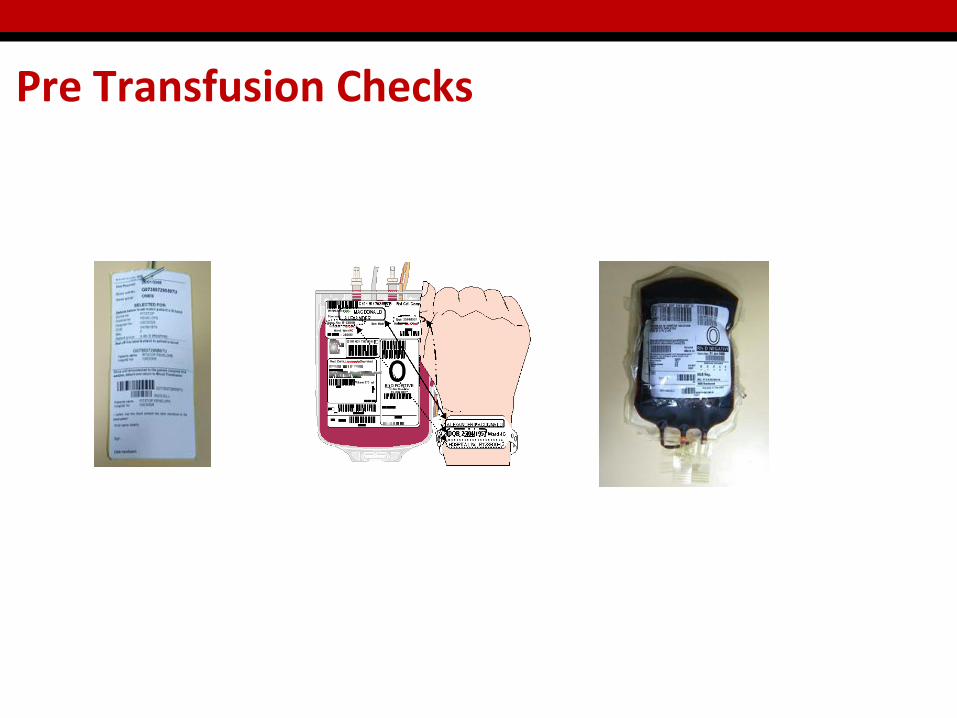
1. IDENTIFICATION CHECKSa) Positive identification with TWO STAFF: Ask patient full name / DOBb) Check against wristband on the patientc) Check against compatibility label on blood unit / request form
2. BLOOD UNIT CHECKa) Check blood unit expiry date / number and blood groupb) Check blood bag: ensure free from clots / leaks
3. DOCUMENTATIONa) Record- blood pack number, date/time and signature of both staffb) Send request label back to lab to monitor completion
Pre Transfusion Checks

Pre Transfusion Checks – what to check

Putting up the blood

Putting up the blood
1. PRE CHECKSAseptic technique – wash hands, gloves, apronGiving set: Double lumen, check expiryPatient observations (baseline)
2. CONNECT BAGConnect the giving set to the blood bagSqueeze blood into both chambersPrime the giving set with bloodAttach to cannula
3. GO!Set drip rate
4. DOCUMENTRecord when started / by who / checks done

During procedure checks

When should observations be checked?Initial/baseline observations15 minutes after startingHourly thereafterAt end of transfusion
What should you be checking for? TemperatureHeart rate/Blood PressureRespiratory rate/Saturation
What symptoms should you be advising the patient to report?ANY!
Chest/Abdo painSOBRestlessness/anxietyRashBlood in urine
Checks during procedure
… Mrs Smith
Baseline observations: Temperature: 36.5Blood pressure: 120/80Heart rate: 80Saturations: 99% OA
15 mins into transfusionPatient c/o difficulty breathing
What would you do?
… Mrs Smith ...
Baseline observations: Temperature: 36.5Blood pressure: 120/80Heart rate: 80Saturations: 99% OA
15 mins into transfusionPatient c/o difficulty breathing
1. ABCDE AssessmentA- patent, B- wheeze throughout, C- well perfused, good cap refill
2. Consider stopping transfusion
1. Repeat ObservationsTemperature: 36.7Blood pressure: 105/70Heart rate: 90Saturations: 94% OA

When to stop the transfusion

When to stop the transfusion
Temperature - Increase by 1 degree
Blood Pressure - Significant change (+/- 10mmHg)
Heart Rate - Significant rise
Symptoms
Complications – which one?
Acute haemolytic reaction
TRALI
Infections
TACO
Anaphylaxis
Iron overload
Allergic rxn
Post-transfusion purpura
Fluid overload
Bacterial contamination
Graft vs host disease
Non-haemolytic febrile transfusion rxn

Complications – which one?
Acute haemolytic reaction
TRALI
Infections
TACO
Anaphylaxis
Iron overload
Allergic rxn
Post-transfusion purpura
Fluid overload
Bacterial contamination
Graft vs host disease
Non-haemolytic febrile transfusion rxn

Transfusion Reactions
General management:STOP Transfusion
Send blood product to labMaintain line with IV FluidCall for help
New FBC/U+E/Clotting samplesClear history of symptomsDocument
Think specifics for management
Early vs Late reactions

Blood GroupsUNIVERSAL
DONORUNIVERSAL RECIPIENT
UK
Frequency42% 8% 3% 47%

Early vs. Delayed complications
Early (<24hrs)
Acute haemolytic reactionAnaphylaxisBacterial contaminationTRALI / TACONon-haemolytic febrile
transfusion rxnAllergic rxn
Late (>24hrs)
InfectionsIron overloadGraft vs host diseasePost-transfusion purpura

Early: Acute haemolytic reaction
e.g. ABO incompatibility – commonly clerical errors
Signs/symptoms:agitation, rapid onset fever, hypotension, flusing,
abdominal/chest pain, DIC +/- death
LARGELY PREVENTABLECOMMONEST CAUSE = HUMAN ERROR

Acute Lung Complications TRALI vs. TACO
Signs/symptoms
Transfusion Related Acute Lung Injury
Dysponea, cough
General principles
Oxygen
Treat as ARDS
Transfusion Associated Circulatory Overload
Dysponea, hypoxia, tachycardia, creps+/- echo/BNP
General principlesOxygenDiuretic (furosemide)
Management

Acute: Other reactions
Non-haemolytic febrile transfusion reactionShivering and fever (1-1.5hrs post starting)Unpleasant but not life threateningMx: Consider anti-pyretic (paracetamol)
Bacterial ContaminationFever, hypotension and rigorsMx: Urgent septic screen, Broad spec ABx
AnaphylaxisBronchospasm, cyanosis, hypotension, soft tissue swellingMx: Maintain airway + Oxygen. Call help/2222
Allergic reactionUrticaria and itchMx: Chlorphenamine

Chronic: Other
Post Transfusion Purpura5-7 days post transfusionPlatelets fall – can be lethal
Graft-versus-host diseaseRare. Fatal.Donor lympocytes mount an immune response against the immunocompromised hostPrevented by irradiation of donor blood

‘the life of all flesh is the blood thereof: whoever eat it shall be cut off’ (Lev. 17:10–16) ‘abstain from the meats offered to idols and from blood’ (Acts 15:28–29) (1–3).

Is blood transfusion necessary?
If so, ensure:
Right blood
Right patient
Right time
Right place
Summary
ANY QUESTIONS???
SMITH, Andrew01/10/19878765432

10/03/2016
SMITH, AndrewDOB: 01/10/1987Hospital Number: 8765432
20/01/2016

Fluid with food dye in
Giving sets – fluid and blood one
Gloves
Cannula
Prescription chart
Name badges












