Blood pressure reduction with statins Meta-analysis of randomised controlled trials P. Strazzullo 1,...
16
Blood pressure reduction with statins Meta-analysis of randomised controlled trials P. Strazzullo 1 , S.M. Kerry 2 , A. Barbato 1,2 , M. Versiero 1 , L. D’Elia 1 & F.P. Cappuccio 3 1 Department of Clinical & Experimental Medicine, Federico II Medical School, University of Naples, Italy; 2 Division of Community Health Sciences, St George’s University of London, UK; 3 Clinical Sciences Research Institute, Warwick Medical School, Coventry, UK
-
Upload
curtis-flynn -
Category
Documents
-
view
213 -
download
0
Transcript of Blood pressure reduction with statins Meta-analysis of randomised controlled trials P. Strazzullo 1,...

Blood pressure reduction with statinsMeta-analysis of randomised controlled trials
P. Strazzullo1, S.M. Kerry2, A. Barbato1,2, M. Versiero1, L. D’Elia1 & F.P. Cappuccio3
1 Department of Clinical & Experimental Medicine, Federico II Medical School, University of Naples, Italy; 2 Division of Community Health Sciences, St George’s University of London, UK; 3 Clinical Sciences Research Institute, Warwick Medical School, Coventry, UK

2
Conflict of Interest
• FPC has received honoraria and refund of expenses from Pfizer

3
Background
• Possible anti-HPT effect of statins investigated by very few studies in patients with HPT and hypercholesterolemia.
• Additional information from several other studies, not specifically aimed at the evaluation of the statins’ anti-HPT effect.
• Present knowledge hampered by severe limitations (inadequate design, small sample size, too short Rx period, modification of concomitant anti-HPT Rx during the trial).
• Nevertheless, effect of statins on BP plausible given their impact on endothelial function, interaction with RAS and influence on large artery compliance.

4
Objectives
• To carry out a systematic review of the literature to identify all studies reporting BP data during treatment with statins.
• To carry out a meta-analysis of the effect of statins on BP including all trials which met strict predefined inclusion criteria.

5
Design and Methods• Meta-analysis of randomised controlled trials
comparing statins vs placebo (or control)• Medline (1966 to Oct 2005), Embase (1980 to Oct
2005), Databases (Cochrane, Clinical Effectiveness, HTA, NHS Economic Evaluation, TRIP, CRD, AHRQ) identified 175 trials.

6
Flow DiagramRCTs identified
(n=175)
RCTs retrieved(n=156)
RCTs suitable(n=20)
RCTs included(n=20)
No control group (n=19) BP treatment
not constant (n=26)
Incomplete data(n=97)
Other (n=13)
Placebo-controlled (n=20)High TC pts (n=19) High BP pts (n=11)
Pravastatin (n=8) Simvastatin (n=6) Fluvastatin (n=3)Atorvastatin, Cerivastatin (n=2) Lovastatin (n=1)

7
Design and Methods• Meta-analysis of randomised controlled trials
comparing statins vs placebo (or control)• Medline (1966 to Jan 2003), Embase (1980 to Jan
2003), Databases (Cochrane, Clinical Effectiveness, HTA, NHS Economic Evaluation, TRIP, CRD, AHRQ) identified 175 potential trials
• Outcome measures: difference in SBP and DBP between patients taking statins and those taking placebo (or control Rx)
• 889 patients studied (324 on statins, 303 on Control, 262 in cross-over trials, age 41-70 yrs)
• Duration: from 4 weeks to 1 year

8
Statistical Analysis• Random effects model• Difference in BP (95% CI)• Publication bias by funnel plot and
Egger’s test• ‘Trim and fill’ method• Heterogeneity by chi-square• Meta-regression to assess the possible
association of the BP effect of statin with age, baseline BP, duration, HPT status, T2D, TChol response to statin

9
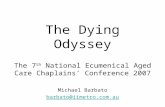
Effect of Statins on Systolic BP
Heterogeneity p<0.01
Intervention effect (mmHg) -20 0 20 40
Combined
Koh,2004
Ikeda,2004 Fogari ,2004 Ferrier,2002
Shige,2001 Glorioso,1999
Tonolo,1997 Straznicky,1995
Kool,1995 Balletshofer,2005
Jenkins,2003 De Rosa(2),2003 De Rosa(1),2003
Lee,2002 Nakamura,2001
Bak (2),1998
Bak (1),1998 O'Callaghan,1994
Hommel,1992 McDowell,1991 -4.0 ( -19.1,11.1)
-8.0 ( -25.5,9.5) 0.0 ( -14.7,14.7)
1.9( -4.8,8.6) -2.3 ( -8.8, 4.2)
-6.0 ( -13.0,1.0) -1.0 ( -6.5,4.5) -2.0 ( -9.5,5.5)
-3.0 ( -10.4,4.4) 5.2 ( -2.7,13.1)
-10.0 ( -21.8,1.8) 3.0 ( -4.3,10.3) 0.5 ( -4.0, 5.0) 0.0 ( -2.0,2. 0)
-7.0 ( -10.0, -4.0) 1.0 ( -5.6,7.6)
-6.0 ( -11.1, -0.9) -4.2 ( -7.3,1.1)
-4.9 ( -7.2, -2.6) 5.0 (0.2,9.9)
-1.9 (-3.8 ÷ -0.1)
STATIN better CONTROL better

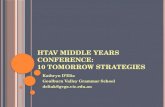
10Heterogeneity p<0.01
Effect of Statins on Diastolic BP
Intervention effect (mmHg)
-10 0 10 20
Combined
Koh,2004 Ikeda,2004
Fogari,2004
Ferrier,2002
Shige,2001
Glorioso,1999
Tonolo,1997
Straznicky,1995
Kool,1995 Balletshofer,2005
Jenkins,2003
De Rosa(2),2003
De Rosa(1),2003
Lee,2002 Nakamura,2001
Bak (2),1998
Bak (1),1998 O'Callaghan,1994
Hommel,1992
McDowell,1991 -6.0 ( -14.2,2.2)
-5.0 ( -14.9,4.9)
4.0 ( -2.9,10.9)
1.1 ( -2.1,4.3)
-1.0 ( -4.2,2.2)
-2.0 ( -7.3,3.3)
-1.0 ( -3.8,1.8)
-2.0( -7.2,3.2)
-2.0 ( -7.1,3.1)
-0.9 ( -6.0,4.2)
-5.0 ( -11.3,1.3)
1.0 ( -3.1,5.1)
1.0 ( -2.0,4. 0)
-0.5 ( -1.7,0.7) -4.0 ( -6.0, -2.0)
1.0 ( -1.8,3.8)
-2.0 ( -4.0, -0.0)
-3.4 ( -4.7, -2.1)
-0.2 ( -2.2,1.8) 4.0 (1.0,7.0)
- 0.9 (- 2.0 ÷ 0.2)
STATIN better CONTROL better

11
Funnel plots for systolic and diastolic BP 1/
SE
(in
terv
enti
on e
ffec
t)
Systolic blood pressure Diastolic blood pressure
Intervention effect (mmHg)
-10 -5 0 50
0.5
1
Intervention effect (mmHg)
-10 -5 0 50
0.5
1
1.5
2
1/S
E (
inte
rven
tion
eff
ect)
Egger’s test, p=0.58 Egger’s test, p=0.48

12
Effect of Statins on Systolic BP in studies with average baseline BP >130 mmHg
Heterogeneity p=0.26
-4.0 (-19.1,11.1)
-8.0 (-25.5,9.5)
0.0 (-14.7,14.7)
1.9 (-4.8,8.6)
-2.3 (-8.8, 4.2)
-2.0 (-9.5,5.5)
-3.0 (10.4,-4.4)
-10.0 (-21.8,1.8)
0.5 (-4.0, 5.0)
-7.0 (-10.0,-4.0)
-6.0 (-11.1,-0.9)
-4.9 (-7.2,-2.6)
Intervention effect (mmHg)
-20 0 20 40
Combined
Ikeda,2004
Ferrier,2002
Glorioso,1999
Straznicky,1995
Balletshofer,2005
De Rosa(2),2003
De Rosa(1),2003
Bak (2),1998
Bak (1),1998
O'Callaghan,1994
Hommel,1992
McDowell,1991
-4.0 (-5.8 ÷ -2.2)
STATIN better CONTROL better

13
Effect of Statins on Diastolic BP in studies with average baseline BP >80 mmHg
Heterogeneity p=0.069
STATIN better CONTROL better
Intervention effect (mmHg)
- 10 0 10 20
Combined
Ikeda,2004
Ferri er,2002
Glorioso,1999
Straznicky,1995
Balletshofer,2005
De Rosa(2),2003
De Rosa(1),2003
Bak (2),1998
Bak (1),1998
O'Callaghan,1994
Hommel,1992 -5.0 ( -14.9,4.9)
4.0 ( -2.9,10.9)
1.1 ( -2.1,4.3)
-1.0 ( -4.2,2.2)
-2.0 ( -7.2,3.2)
-2.0 ( -7. 1,3.1)
-5.0 ( -11.3,1.3)
1.0 ( -2.0,4.0)
-4.0 (-6.0,-2.0)
-2.0 (-4.0,0.1)
-0.2 (-2-2,1.8)
-1.2 (- 2.6 ÷ 0.1)

14
Meta-regression of intervention effect on
systolic and diastolic BP
Inte
rven
tion
eff
ect
(SB
P)
Average baseline systolic BP (mmHg)
(p=0.066)
120 130 140 150 160 -10
-5
0
5
Inte
rven
tion
eff
ect
(DB
P)
Average baseline diastolic BP (mmHg)
70 80 90 100
-5
0
5
(p=0.023)
-5
0
5

15
Limitations• Small n° of studies, small total sample size.• Much larger studies not included to avoid
potential bias of BP treatment (e.g. WOSCOPS, ASCOT, ALLHAT, etc)
• Between-studies heterogeneity.• Most studies NOT specifically designed to
evaluate the effect of statins on BP.• Most studies carried out in hypercholesterolemic
patients.• Publication bias impossible to rule out
completely.• Intra-class differences not discernible.

16
Summary and Conclusions• Small but statistically significant effect of statins on
BP, more prominent on systolic BP• Effect greater in those with higher baseline BP, BUT
unrelated to age, duration of treatment, BP Rx, T2D and cholesterol response,
• Class effect difficult to detect• Possible mechanisms – increased NO bioavailability,
reduced ET1 production, improved endothelial function, inhibition of ROS production, reduction in large arteries stiffness, improved systemic arterial compliance, down-regulation of AII type 1 receptor and reduced vasoconstrictor response to AII.
• Potential importance for controlling high BP in patients with CV co-morbidities