Bleeding Prolapsed Hemorrhoids as a Presentation of Ruptured Internal Iliac Artery Aneurysm: Report...
3
Surg Today (2005) 35:893–895 DOI 10.1007/s00595-005-3019-2 Bleeding Prolapsed Hemorrhoids as a Presentation of Ruptured Internal Iliac Artery Aneurysm: Report of a Case Anjana Singh, Amit Amin, Amjid A. Riaz, Ramesh Nadarajah, and Jenny Ackroyd Princess Alexandra Hospital, Hamstel Road, Harlow, Essex CM20 1QX, UK Case Report A 79-year-old man presented to our casualty depart- ment with a 2-day history of right leg pain and swelling, which was initially thought to be sciatica. He had undergone an AAA repair 12 years earlier, but had no history of recent trauma. He was an ex-smoker of 40 years and his other medical history included hyperten- sion, a myocardial infarction, and noninsulin-dependent diabetes. On examination, he appeared well and comfortable. He was afebrile, with a pulse rate of 79 beats/min and a blood pressure of 108/76 mmHg. His chest was clear and his abdomen was not tender. No aneurysms were pal- pable, but the right leg had non-tender pitting edema extending to the groin. His femoral pulses were pal- pable and normal. Blood tests revealed high D-dimers of 2500 IU, hemoglobin (Hb) 13.6 g/dl, and creatinine of 173 mmol/l (Table 1). An electrocardiogram showed no acute changes. A clinical diagnosis of deep vein throm- bosis (DVT) was made, and he was given a therapeutic dose of tinzaparin and referred to the physicians. How- ever, 2 h after the injection he began to bleed from his rectum and his blood pressure dropped to 80/50 mmHg. Anorectal examination revealed a ring of tender pro- lapsing hemorrhoids, which were blue-black and oozing a small amount of fresh blood. These findings were attributed to the anticoagulation therapy. By a further 2 days later, the discoloration had expanded to the perineal region and the scrotum (Fig. 1), and it was noted that he had passed very little urine, with a re- sidual of only 300 ml on catheterization. Blood results now showed an Hb of 10.7 g/dl and acute renal failure (ARF), with urea 25.3 mmol/l and creatinine 500 mmol/ l. An urgent ultrasound scan showed bilateral mild renal pelvis dilatation, and probable retroperitoneal hematoma, as well as lack of flow in the right common femoral vein, suggesting iliac vein compression. A com- puted tomography scan showed a huge 16 ¥ 9.4-cm right Abstract Internal iliac artery aneurysms (IIAAs) are rare and their concealed location in the pelvis presents a diagnos- tic challenge. We report a case of a 79-year-old man who presented 12 years after an abdominal aortic aneu- rysm repair, with signs of prolapse, bleeding, hemor- rhoids, and a deep vein thrombosis. His condition rapidly deteriorated, with the development of acute renal failure and obvious perianal and perineal ecchy- moses, within a few days. Abdominal ultrasound and computed tomography showed a ruptured IIAA. His renal function returned to normal after surgical decom- pression of the aneurysm. Key words Internal iliac artery aneurysm Introduciton Internal iliac artery aneurysms (IIAAs) are an uncom- mon but well-described clinical entity. Between 1% and 2% of these aneurysms occur in association with ab- dominal aortic aneurysms (AAA), or after their surgical repair. 1,2,5 Internal iliac artery aneurysms are clinically important because their symptoms can mimic many intra-abdominal disorders causing difficulties and de- lays in diagnosis, and referrals to inappropriate medical specialities. 3,4,6 We report an unusual case of a ruptured IIAA in a patient whose referral to our surgical team was delayed because the initial signs of perianal ecchymoses were mistaken for prolapsing, bleeding hemorrhoids. Reprint requests to: A. Singh, 88 Harbut Road, London SW11 2RE, UK Received: March 29, 2004 / Accepted: November 16, 2004
-
Upload
anjana-singh -
Category
Documents
-
view
213 -
download
0
Transcript of Bleeding Prolapsed Hemorrhoids as a Presentation of Ruptured Internal Iliac Artery Aneurysm: Report...
Surg Today (2005) 35:893–895DOI 10.1007/s00595-005-3019-2
Bleeding Prolapsed Hemorrhoids as a Presentation of RupturedInternal Iliac Artery Aneurysm: Report of a Case
Anjana Singh, Amit Amin, Amjid A. Riaz, Ramesh Nadarajah, and Jenny Ackroyd
Princess Alexandra Hospital, Hamstel Road, Harlow, Essex CM20 1QX, UK
Case Report
A 79-year-old man presented to our casualty depart-ment with a 2-day history of right leg pain and swelling,which was initially thought to be sciatica. He hadundergone an AAA repair 12 years earlier, but had nohistory of recent trauma. He was an ex-smoker of 40years and his other medical history included hyperten-sion, a myocardial infarction, and noninsulin-dependentdiabetes.
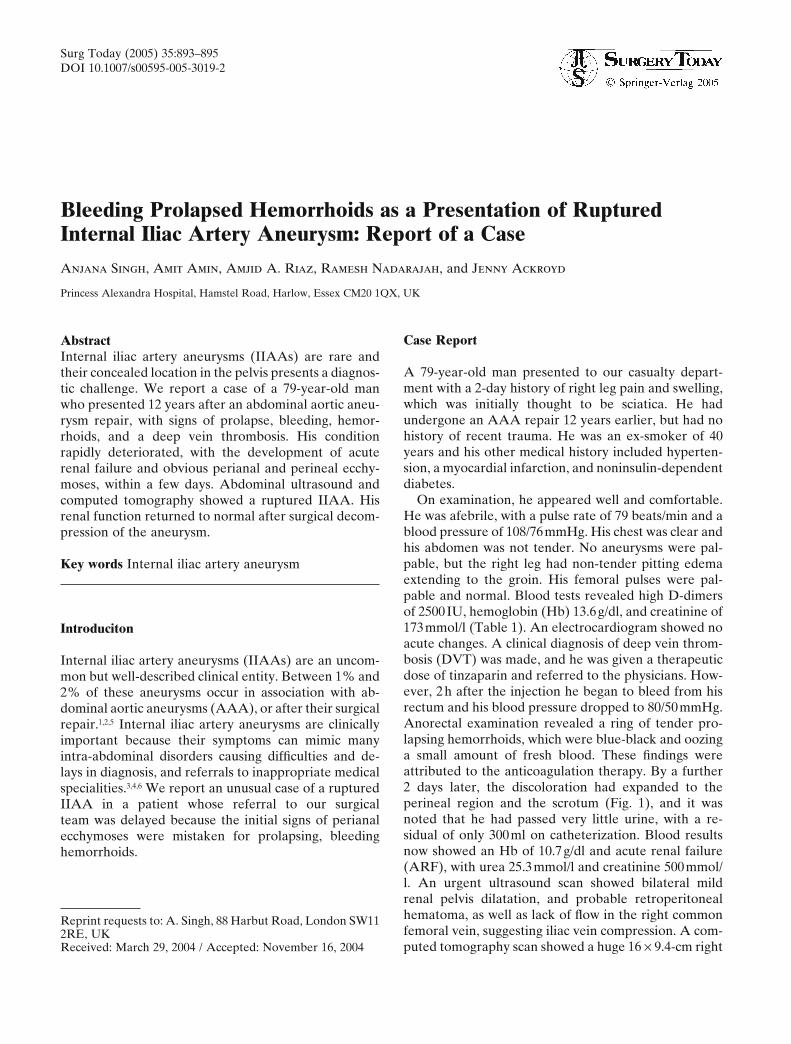
On examination, he appeared well and comfortable.He was afebrile, with a pulse rate of 79 beats/min and ablood pressure of 108/76mmHg. His chest was clear andhis abdomen was not tender. No aneurysms were pal-pable, but the right leg had non-tender pitting edemaextending to the groin. His femoral pulses were pal-pable and normal. Blood tests revealed high D-dimersof 2500IU, hemoglobin (Hb) 13.6g/dl, and creatinine of173mmol/l (Table 1). An electrocardiogram showed noacute changes. A clinical diagnosis of deep vein throm-bosis (DVT) was made, and he was given a therapeuticdose of tinzaparin and referred to the physicians. How-ever, 2h after the injection he began to bleed from hisrectum and his blood pressure dropped to 80/50mmHg.Anorectal examination revealed a ring of tender pro-lapsing hemorrhoids, which were blue-black and oozinga small amount of fresh blood. These findings wereattributed to the anticoagulation therapy. By a further2 days later, the discoloration had expanded to theperineal region and the scrotum (Fig. 1), and it wasnoted that he had passed very little urine, with a re-sidual of only 300ml on catheterization. Blood resultsnow showed an Hb of 10.7g/dl and acute renal failure(ARF), with urea 25.3mmol/l and creatinine 500mmol/l. An urgent ultrasound scan showed bilateral mildrenal pelvis dilatation, and probable retroperitonealhematoma, as well as lack of flow in the right commonfemoral vein, suggesting iliac vein compression. A com-puted tomography scan showed a huge 16 ¥ 9.4-cm right
AbstractInternal iliac artery aneurysms (IIAAs) are rare andtheir concealed location in the pelvis presents a diagnos-tic challenge. We report a case of a 79-year-old manwho presented 12 years after an abdominal aortic aneu-rysm repair, with signs of prolapse, bleeding, hemor-rhoids, and a deep vein thrombosis. His conditionrapidly deteriorated, with the development of acuterenal failure and obvious perianal and perineal ecchy-moses, within a few days. Abdominal ultrasound andcomputed tomography showed a ruptured IIAA. Hisrenal function returned to normal after surgical decom-pression of the aneurysm.
Key words Internal iliac artery aneurysm
Introduciton
Internal iliac artery aneurysms (IIAAs) are an uncom-mon but well-described clinical entity. Between 1% and2% of these aneurysms occur in association with ab-dominal aortic aneurysms (AAA), or after their surgicalrepair.1,2,5 Internal iliac artery aneurysms are clinicallyimportant because their symptoms can mimic manyintra-abdominal disorders causing difficulties and de-lays in diagnosis, and referrals to inappropriate medicalspecialities.3,4,6 We report an unusual case of a rupturedIIAA in a patient whose referral to our surgicalteam was delayed because the initial signs of perianalecchymoses were mistaken for prolapsing, bleedinghemorrhoids.
Reprint requests to: A. Singh, 88 Harbut Road, London SW112RE, UKReceived: March 29, 2004 / Accepted: November 16, 2004
894 A. Singh et al.: Internal Iliac Artery Aneurysm
was 8.8 ± 3.2 years.8 In our patient, IIAA was notpresent at the time of the original AAA repair, butmanifested 12 years later. The presentation of IIAA isoften atypical because of the concealed anatomicallocation of the aneurysm in the pelvis. Symptoms arecaused by compression of the surrounding structuresincluding the ureter, bladder, bowel, nerve roots, andpelvic veins. Signs are absent until the aneurysm is largeenough to compress the surrounding structures, or torupture producing a contained hematoma that subse-quently causes compression, shock, or both. Further-more, IIAAs are rarely palpable in the abdomen,although up to 55% are palpable per rectum.2 When anIIAA ruptures, patients may experience back, loin, or
Fig. 1. Perineal/buttock (a) and scrotal ecchymoses (b) just before the operation
Table 1. Laboratory results
Day 1 (on admission) Day 3
Hb (g/dl) 13.6 10.7Urea (mmol/l) 18.8 25.3Cr (mmol/l) 173 500D-dimer (IU) 2500 —
Hb, hemoglobin; Cr, creatinine
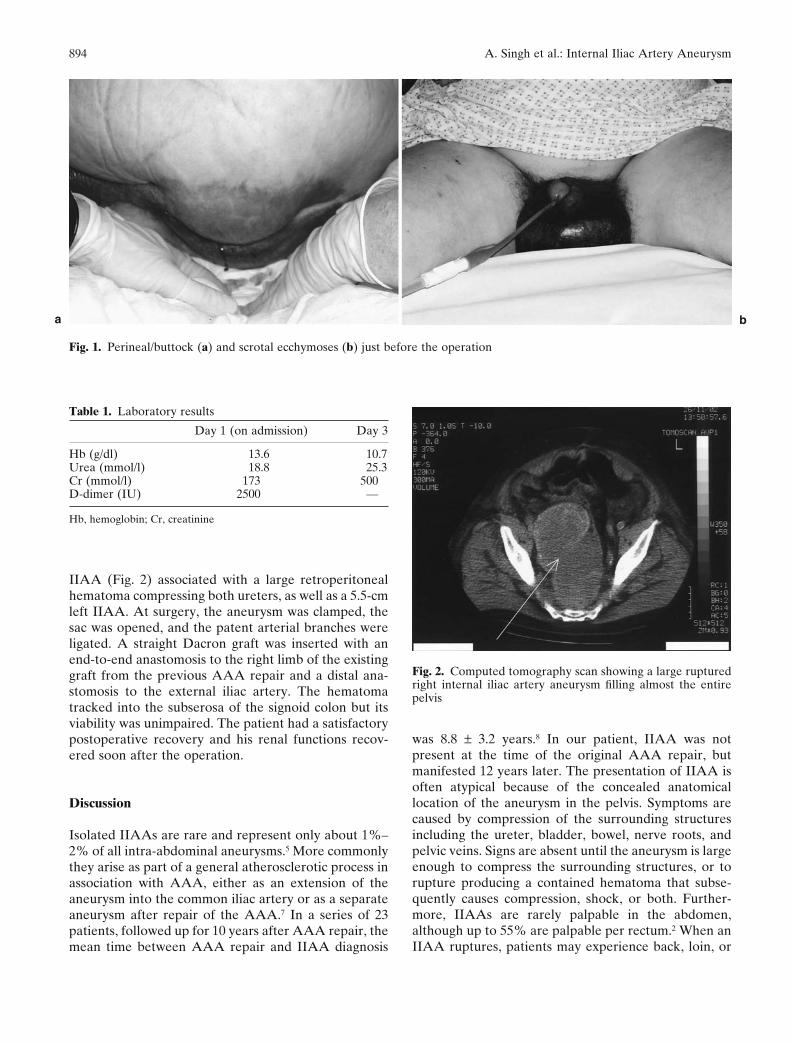
IIAA (Fig. 2) associated with a large retroperitonealhematoma compressing both ureters, as well as a 5.5-cmleft IIAA. At surgery, the aneurysm was clamped, thesac was opened, and the patent arterial branches wereligated. A straight Dacron graft was inserted with anend-to-end anastomosis to the right limb of the existinggraft from the previous AAA repair and a distal ana-stomosis to the external iliac artery. The hematomatracked into the subserosa of the signoid colon but itsviability was unimpaired. The patient had a satisfactorypostoperative recovery and his renal functions recov-ered soon after the operation.
Discussion
Isolated IIAAs are rare and represent only about 1%–2% of all intra-abdominal aneurysms.5 More commonlythey arise as part of a general atherosclerotic process inassociation with AAA, either as an extension of theaneurysm into the common iliac artery or as a separateaneurysm after repair of the AAA.7 In a series of 23patients, followed up for 10 years after AAA repair, themean time between AAA repair and IIAA diagnosis
Fig. 2. Computed tomography scan showing a large rupturedright internal iliac artery aneurysm filling almost the entirepelvis
a b

895A. Singh et al.: Internal Iliac Artery Aneurysm
abdominal pain. Rare presentations relate to the proxi-mity of the iliac system to the genitourinary system, thelumbosacral nerve roots, iliac veins, and the rectum asin our patient, whose symptoms were initially attributedincorrectly to sciatica by the general practitioner, andthen to a DVT complicated by bleeding hemorrhoids bythe physicians. The development of ARF finally led tothe “incidental” diagnosis of ruptured IIAA on the 3rdday after his admission. Apart from a single recordedfall in blood pressure, the fact that the patient remainedhemodynamically stable throughout despite anticoagu-lant therapy contributed to the delay in diagnosis. Thehigh mortality rate of 75%–90% associated with rup-ture of IIAA9,10 is partly attributed to the difficulty indiagnosis. Retrospectively, the perianal ecchymosesshould have been the main clue to the diagnosis, but thissign was mistaken as a complication of the anticoagula-tion therapy. Blood tracking through the levator ani andappearing around the anus is indicative of intra-abdominal or intrapelvic hemorrhage. Although thissign is rare, it can be extremely useful in establishing anearly diagnosis.11 The pelvic location of IIAA also oftencauses urinary tract symptoms. Acute renal failure wasprecipitated by bilateral compression of the ureters inour patient, whose renal function returned to normalafter decompression of the aneurysm. Nelson foundbilateral ureteral involvement in only 3 of 24 reportedcases of IIAA.12 Ileofemoral thrombosis occurs in only5% of IIAAs.13
The mean size of IIAAs varies between 4.5 and5.7cm.7 Internal iliac artery aneurysms greater than4cm in diameter should be repaired electively, which isassociated with operative survival reaching 90%.14 It isgenerally agreed that the best surgical treatment of aruptured IIAA is proximal ligation of the IIAA withobliterative endoaneurysmorrhaphy because proximalligation alone is associated with a high risk of recur-rence.9 We also performed a bypass graft in our patientbecause the common iliac artery was involved in theaneurysm. If bilateral IIAAs are repaired simulta-neously in elderly patients with atherosclerotic disease,revascularization of one internal iliac artery is recom-mended to prevent ischemic complications.15 Our pa-tient also had a left IIAA, but considering his poorgeneral condition we decided to leave the left sidealone. Embolization of the left IIAA at a later date is analternative possibility.16
In summary, this case illustrates some importantsalient features. First, careful rectal examination is
essential, because many IIAAs can be felt digitally as apulsation in the rectum. Second, bleeding, prolapsinghemorrhoids associated with perineal ecchymosis is animportant presenting feature of a ruptured IIAA.Finally, a high index of suspicion is essential in patientswith known vascular risk factors who present with atypi-cal symptoms and signs not fitting a definite diagnosis.Computed tomography should always be performedin these patients to allow for prompt diagnosis andtreatment.
References
1. Brunkwall J, Hauksson H, Bengtsson H, Berquist D, TakolanderR, Bergenz S-E. Solitary aneurysms of the iliac system: anestimate of their frequency of occurrence. J Vasc Surg 1989;10:381–4.
2. Richardson JW, Greenfield LJ. Natural history and managementof iliac aneurysms. J Vasc Surg 1988;8:165–71.
3. Ijaz S, Geroulakos G. Ruptured internal iliac artery aneurysmmimicking a hip fracture. Int Angiol 2001;20:187–9.
4. O’Driscoll D, Fitzgerald E. Isolated iliac artery aneurysms withassociated hydronephrosis. J R Coll Surg Edinb 1999;44:197–9.
5. Schuler JJ, Flanigan DP. Iliac artery aneurysms. In: Bergan J,Yao JST, editors. Aneurysms diagnosis and treatment. New York:Grune and Stratton; 1982. p. 469–85.
6. Ozergin U, Vatansev C, Durgut K, Ozulku M, Gormus N. Aninternal iliac artery aneurysm causing a colonic obstruction: re-port of a case. Surg Today 2001;31:839–41.
7. McCready R, Pairolero P, Gilmore J, Kazmier F, Cherry K,Hollier L. Isolated iliac artery aneurysms. Surgery 1983;93:688–93.
8. Dosluoglu HH, Dryjski ML, Harris LM. Isolated iliac arteryaneurysms in patients with or without previous abdominal aorticaneurysm repair. Am J Surg 1999;178:129–32.
9. Brin B, Bussutil R. Isolated hypogastric artery aneurysm. ArchSurg 1982;117:1329–33.
10. Brings HA, Murray JD, Light JT, Hemp JR, Ranbarger KR.Internal iliac artery aneurysm following aortic reconstruction.Ann Vasc Surg 1996;10:59–62.
11. Tamvakopoulos SK, Corvese WP, Vargas LL. Perianalhaematoma: a sign of leakage after rupture of aortic aneurysm.N Engl J Med 1969;280:548–9.
12. Nelson RP. Isolated internal iliac artery aneurysms and theirurological manifestations. J Urol 1980;124:300–3.
13. Rosenthal D, Matsuura JH, Jerius H, Clarke MD. Ileofemoralvenous thrombosis caused by compression of an internal iliacartery aneurysm: a minimally invasive treatment. J Endovasc Surg1998;5:142–5.
14. Sacks NP, Huddy SP, Wegner T, Giddings AE. Management ofsolitary iliac aneurysms. J Cardiovasc Surg (Torino) 1992;33:679–83.
15. Parry DJ, Kessel D, Scott DJA. Simplifying the internal iliacartery aneurysm. Ann R Coll Surg Engl 2001;83:302–8.
16. Melki J-P, Fichelle J-M, Cormier F, Marzelle J, Cormier J-M.Embolisation of hypogastric artery aneurysm: 17 cases. Am VascSurg 2001;15:312–20.