
Bleeding Disorders Haemostasis Hemorrhage in Oral Surgery.
72
Bleeding Disorders Bleeding Disorders Haemostasis Haemostasis Hemorrhage in Oral Hemorrhage in Oral Surgery Surgery
-
Upload
jordan-merritt -
Category
Documents
-
view
221 -
download
0
Transcript of Bleeding Disorders Haemostasis Hemorrhage in Oral Surgery.

Bleeding DisordersBleeding DisordersHaemostasisHaemostasis
Hemorrhage in Oral Hemorrhage in Oral SurgerySurgery
What is meant by Hemorrhage ?What is meant by Hemorrhage ?
Prolonged or Uncontrolled Bleeding Prolonged or Uncontrolled Bleeding
The amount of blood lost as a result of The amount of blood lost as a result of hemorrhage can range from hemorrhage can range from minimalminimal to to significant significant quantities.quantities.
Hemorrhage can occur to a greater or lesser Hemorrhage can occur to a greater or lesser degree during all surgical procedures and it’s degree during all surgical procedures and it’s management depends upon whether the management depends upon whether the patient is patient is hematologically normalhematologically normal or suffers or suffers from from some disturbance in the normal clotting some disturbance in the normal clotting mechanism.mechanism.
Hemorrhage in Oral SurgeryHemorrhage in Oral Surgery The overwhelming majority of patients who undergo The overwhelming majority of patients who undergo
oral surgical procedures are those who have normal oral surgical procedures are those who have normal haemostatic mechanism.haemostatic mechanism.
Therefore, significant or major hemorrhages are not Therefore, significant or major hemorrhages are not that common in oral surgery except in patients who that common in oral surgery except in patients who have a have a bleeding / clotting disorder or those who are on bleeding / clotting disorder or those who are on anticoagulants.anticoagulants.
However, uncontrolled and persistent bleeding can However, uncontrolled and persistent bleeding can occur in some healthy patients after dental extraction.occur in some healthy patients after dental extraction.
Therefore, it is still important to achieve proper Therefore, it is still important to achieve proper hemostasis in all patients during oral surgical hemostasis in all patients during oral surgical procedures, so as to prevent excessive post-operative procedures, so as to prevent excessive post-operative blood loss.blood loss.
Normal Mechanism of Normal Mechanism of HemostasisHemostasis
Hemostasis is a complicated process. Hemostasis is a complicated process. It involves a number of eventsIt involves a number of events 1. VASCULAR PHASE
2. PLATELET PHASE
3. COAGULATION PHASE
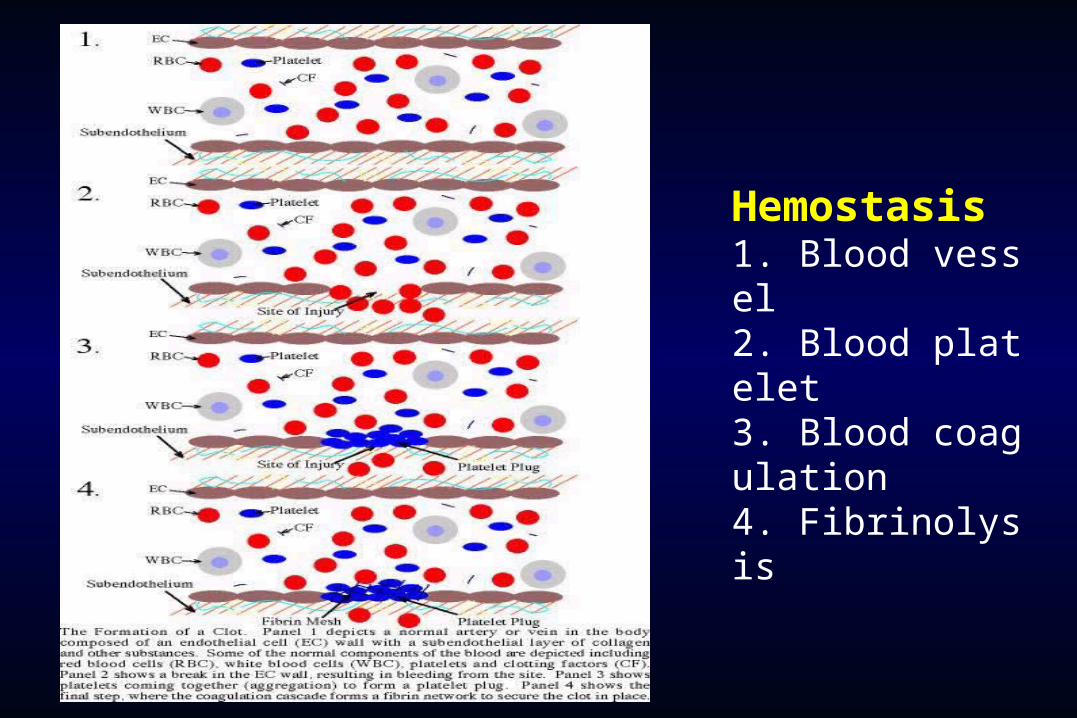
Hemostasis 1. Blood vessel
2. Blood platelet 3. Blood coagula
tttt 4. Fibrinolysis

Coagulation CascadeCoagulation Cascade
Vitamin K dependant factorsVitamin K dependant factors
XIIaXIIa
IIa
Intrinsic system Intrinsic system (surface contact)(surface contact)
XIIXII
XIXI XIa
Tissue factorTissue factor
IXIX IXa VIIa VIIVII
VIIIVIII VIIIaVIIIa
Extrinsic system (tissue damage)Extrinsic system (tissue damage)
XX
VV VaVa
IIII
FibrinogenFibrinogen FibrinFibrin
(Thrombin)(Thrombin)IIa
Xa
Normal Mechanism of HemostasisNormal Mechanism of Hemostasis VASCULAR PHASE :VASCULAR PHASE : When a blood vessel When a blood vessel
is damaged, is damaged, Vasoconstriction resultsVasoconstriction results.. PLATELET PHASE :PLATELET PHASE : Platelets adhere to Platelets adhere to
the damaged surface and form a the damaged surface and form a temporary plug.temporary plug.
COAGULATION PHASE :COAGULATION PHASE : Through two Through two separate pathways, the separate pathways, the IntrinsicIntrinsic and and ExtrinsicExtrinsic, the conversion of fibrinogen to , the conversion of fibrinogen to fibrin is complete. fibrin is complete. Fibrin tightly binds the Fibrin tightly binds the platelets to form a clotplatelets to form a clot
HEMOSTASISHEMOSTASISDEPENDENT UPON:DEPENDENT UPON:
Vessel Wall IntegrityVessel Wall Integrity
Adequate Numbers of PlateletsAdequate Numbers of Platelets
Proper Functioning PlateletsProper Functioning Platelets
Adequate Levels of Clotting FactorsAdequate Levels of Clotting Factors
Proper Function of Fibrinolytic PathwayProper Function of Fibrinolytic Pathway

HemostasisHemostasis
All component onset at same time and close All component onset at same time and close at different timeat different time
Primary(3-5 mins to onset)Primary(3-5 mins to onset) VesselVessel PlateletPlatelet
Secondary( 5-10 mins to onset)Secondary( 5-10 mins to onset) CoagulationCoagulation
Fibrinolysis( need 2-3 days to onset)Fibrinolysis( need 2-3 days to onset)
10
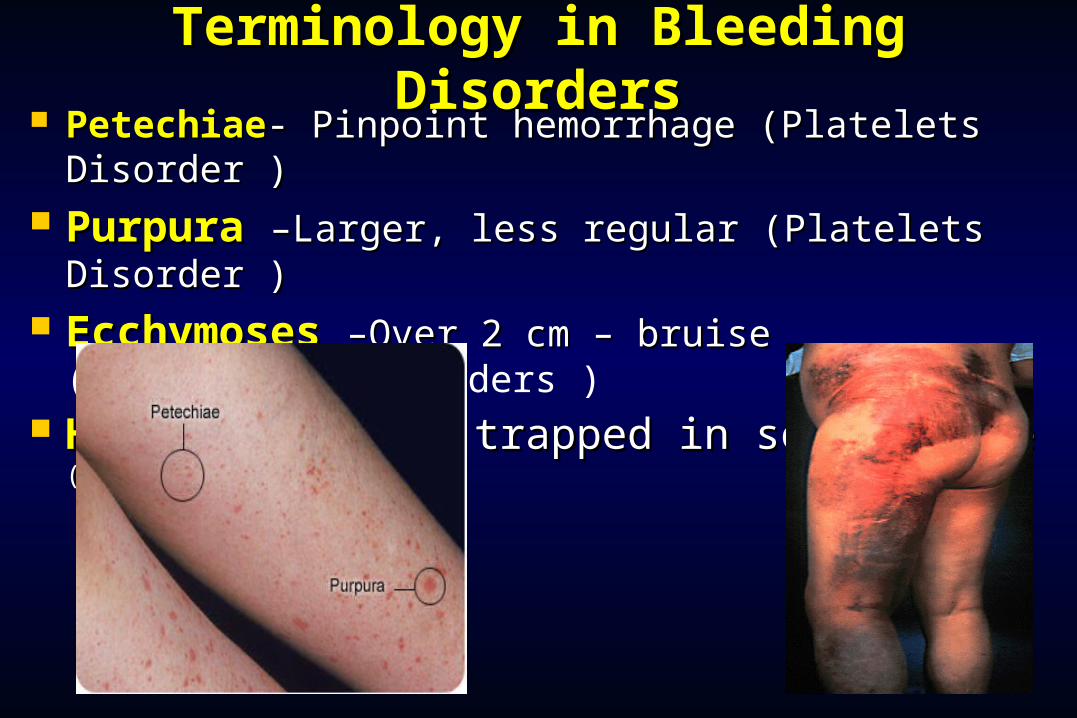
Terminology in Bleeding Terminology in Bleeding DisordersDisorders
PetechiaePetechiae- Pinpoint hemorrhage (Platelets - Pinpoint hemorrhage (Platelets Disorder )Disorder )
PurpuraPurpura –Larger, less regular (Platelets Disorder –Larger, less regular (Platelets Disorder ))
EcchymosesEcchymoses –Over 2 cm – bruise (–Over 2 cm – bruise (Coagulation disorders )
HematomaHematoma –Blood trapped in soft tissue –Blood trapped in soft tissue ((Coagulation disorders )

PetechiaePetechiae
Do not blanch with Do not blanch with pressurepressure
(cf. angiomas) (cf. angiomas)Not palpableNot palpable
(cf. vasculitis) (cf. vasculitis)
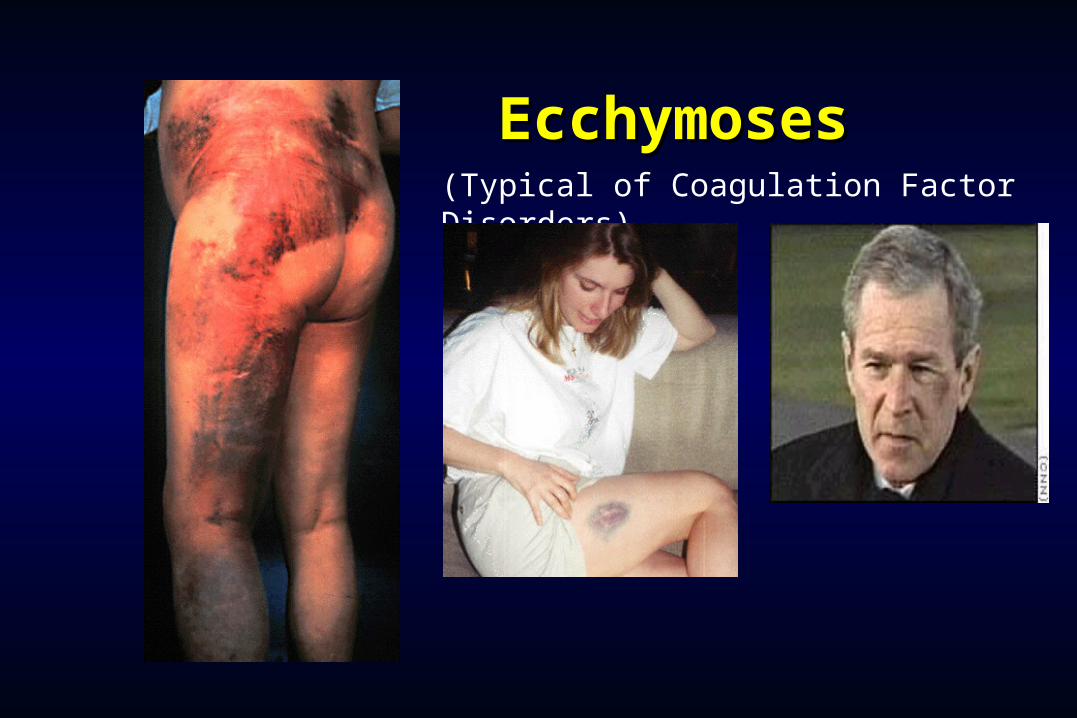
EcchymosesEcchymoses(Typical of Coagulation Factor Disorders)

HematomaHematoma
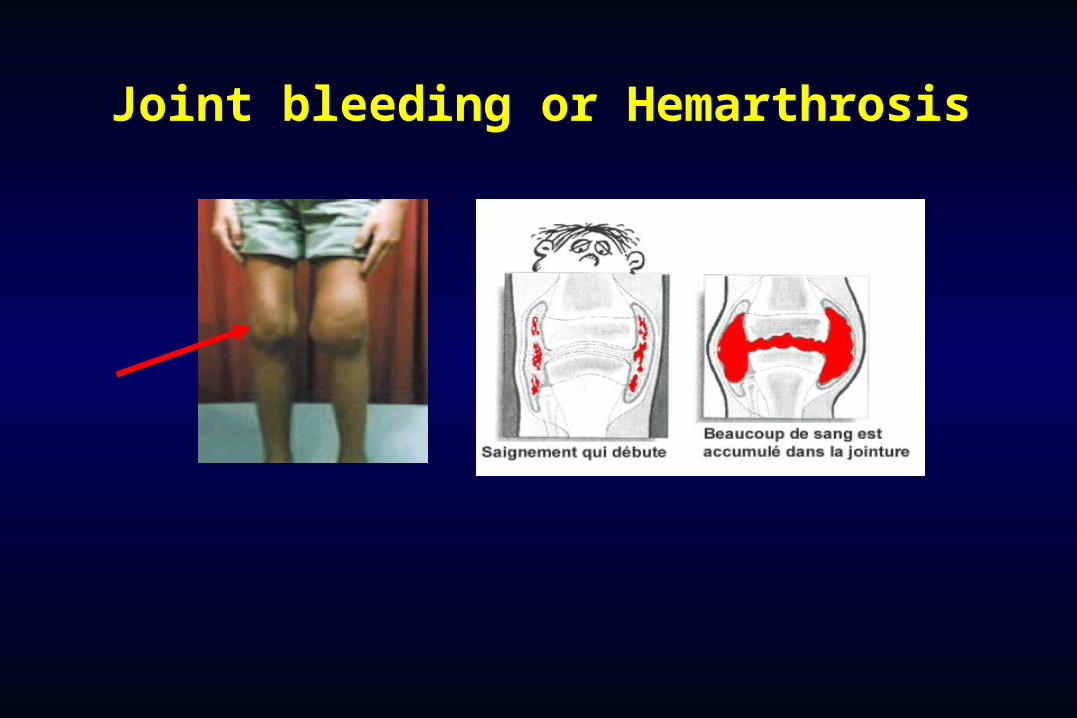
Joint bleeding or Hemarthrosis
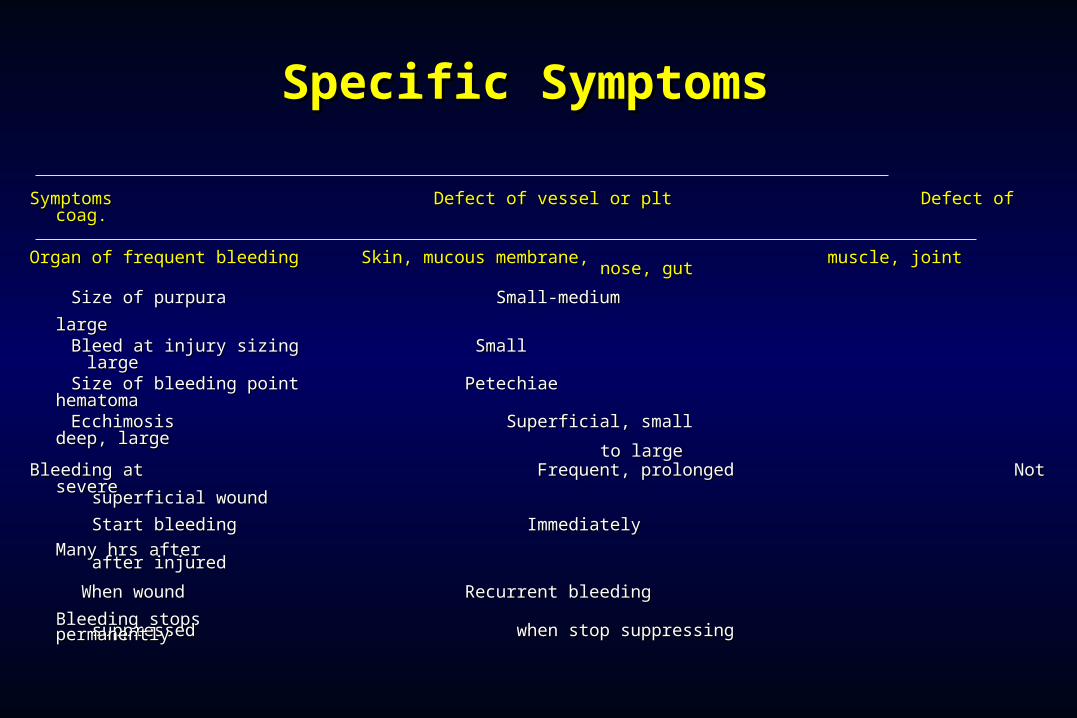
Specific Specific SSymptomsymptoms
Symptoms Defect of vessel or plt Defect of coag.Symptoms Defect of vessel or plt Defect of coag. Organ of frequent bleeding Skin, mucous membrane, muscle, jointOrgan of frequent bleeding Skin, mucous membrane, muscle, joint nose, gutnose, gut
Size of purpura Small-medium largeSize of purpura Small-medium large Bleed at injury sizing Small largeBleed at injury sizing Small large Size of bleeding point Petechiae hematomaSize of bleeding point Petechiae hematoma Ecchimosis Superficial, small deep, largeEcchimosis Superficial, small deep, large to largeto large Bleeding at Frequent, prolonged Not severeBleeding at Frequent, prolonged Not severe superficial woundsuperficial wound
Start bleeding Immediately Many hrs Start bleeding Immediately Many hrs
afterafter after injuredafter injured
When wound Recurrent bleeding Bleeding When wound Recurrent bleeding Bleeding
stopsstops suppressed when stop suppressing permanentlysuppressed when stop suppressing permanently
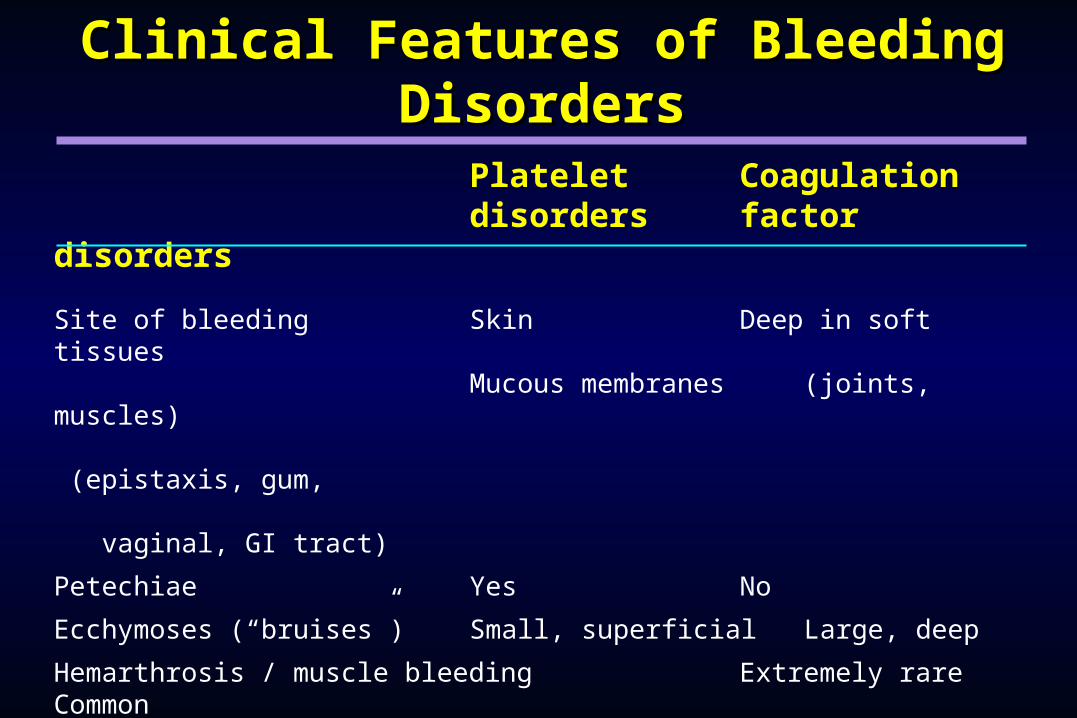
Clinical Features of Bleeding Clinical Features of Bleeding DisordersDisorders
Platelet Coagulation disorders factor
disorders
Site of bleeding Skin Deep in soft tissues Mucous membranes (joints, muscles) (epistaxis, gum, vaginal, GI tract)
Petechiae Yes No
Ecchymoses (“bruises”) Small, superficial Large, deep
Hemarthrosis / muscle bleeding Extremely rareCommon
Bleeding after cuts & scratches Yes No
Bleeding after surgery or trauma Immediate, Delayed
(1-2 days), Usually mild Often severe
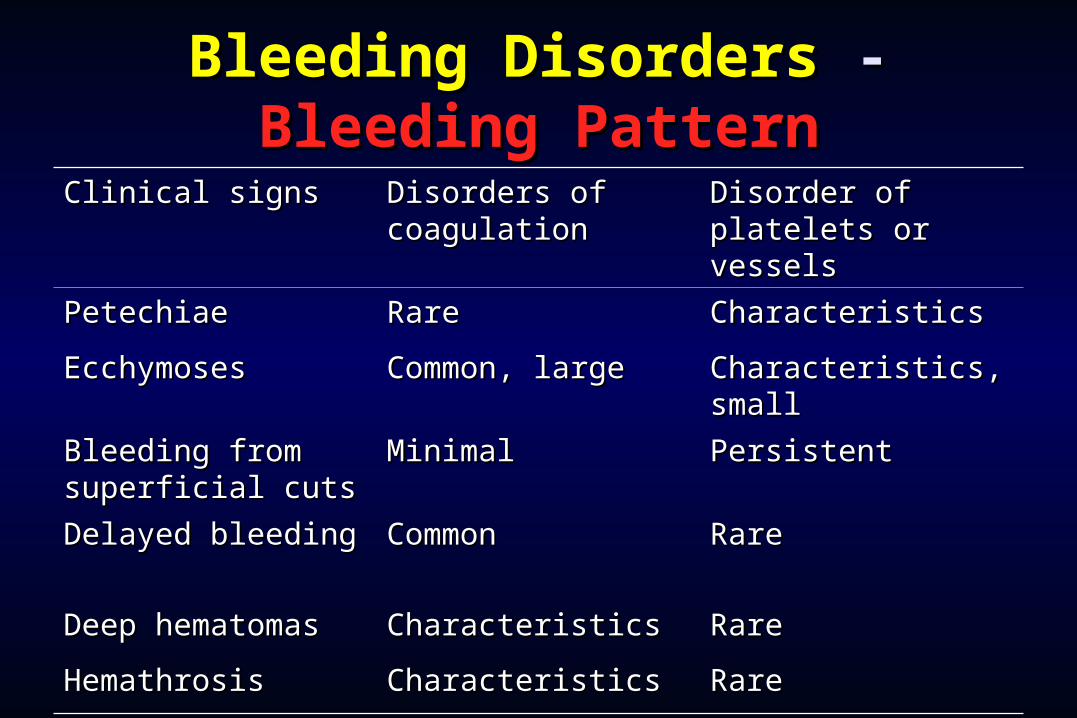
Bleeding DisordersBleeding Disorders - - Bleeding PatternBleeding Pattern
Clinical signsClinical signs Disorders of Disorders of coagulationcoagulation
Disorder of Disorder of platelets or vesselsplatelets or vessels
Petechiae Petechiae RareRare Characteristics Characteristics
Ecchymoses Ecchymoses Common, large Common, large Characteristics, Characteristics, smallsmall
Bleeding from Bleeding from superficial cuts superficial cuts
Minimal Minimal PersistentPersistent
Delayed bleedingDelayed bleeding Common Common RareRare
Deep hematomasDeep hematomas CharacteristicsCharacteristics Rare Rare
Hemathrosis Hemathrosis CharacteristicsCharacteristics Rare Rare
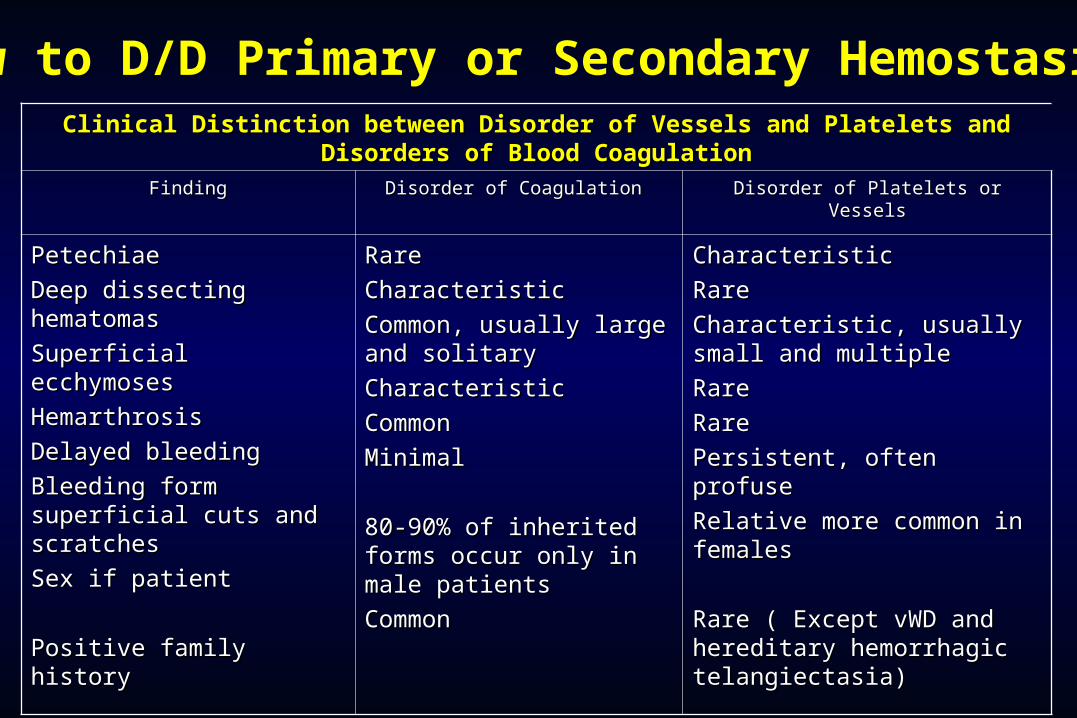
Clinical Distinction between Disorder of Vessels and Platelets and Clinical Distinction between Disorder of Vessels and Platelets and Disorders of Blood CoagulationDisorders of Blood Coagulation
FindingFinding Disorder of Coagulation Disorder of Coagulation Disorder of Platelets or VesselsDisorder of Platelets or Vessels
PetechiaePetechiae
Deep dissecting Deep dissecting hematomashematomas
Superficial ecchymosesSuperficial ecchymoses
HemarthrosisHemarthrosis
Delayed bleedingDelayed bleeding
Bleeding form superficial Bleeding form superficial cuts and scratchescuts and scratches
Sex if patientSex if patient
Positive family historyPositive family history
RareRare
CharacteristicCharacteristic
Common, usually large Common, usually large and solitaryand solitary
CharacteristicCharacteristic
CommonCommon
MinimalMinimal
80-90% of inherited 80-90% of inherited forms occur only in male forms occur only in male patientspatients
CommonCommon
CharacteristicCharacteristic
RareRare
Characteristic, usually small Characteristic, usually small and multipleand multiple
RareRare
RareRare
Persistent, often profusePersistent, often profuse
Relative more common in Relative more common in femalesfemales
Rare ( Except vWD and Rare ( Except vWD and hereditary hemorrhagic hereditary hemorrhagic telangiectasia)telangiectasia)
How to D/D Primary or Secondary Hemostasis
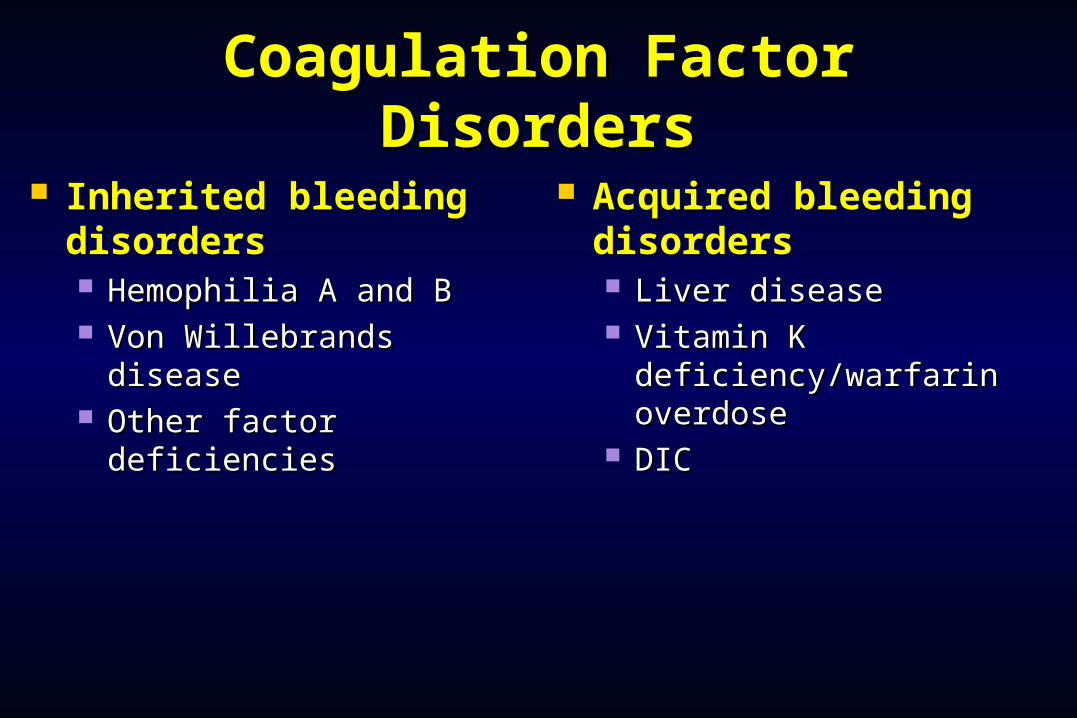
Coagulation Factor Coagulation Factor DisordersDisorders
Inherited bleeding Inherited bleeding disordersdisorders Hemophilia A and BHemophilia A and B Von Willebrands diseaseVon Willebrands disease Other factor deficienciesOther factor deficiencies
Acquired bleeding Acquired bleeding disordersdisorders Liver diseaseLiver disease Vitamin K Vitamin K
deficiency/warfarin deficiency/warfarin overdoseoverdose
DICDIC

Hemophilia A and BHemophilia A and B
Hemophilia AHemophilia B
Coagulation factor deficiency Factor VIII Factor IX
Inheritance X-linked X-linked
recessive recessive
Incidence 1/10,000 males1/50,000 males
Severity Related to factor level<1% - Severe - spontaneous bleeding1-5% - Moderate - bleeding with mild
injury5-25% - Mild - bleeding with surgery or
trauma
Complications Soft tissue bleeding
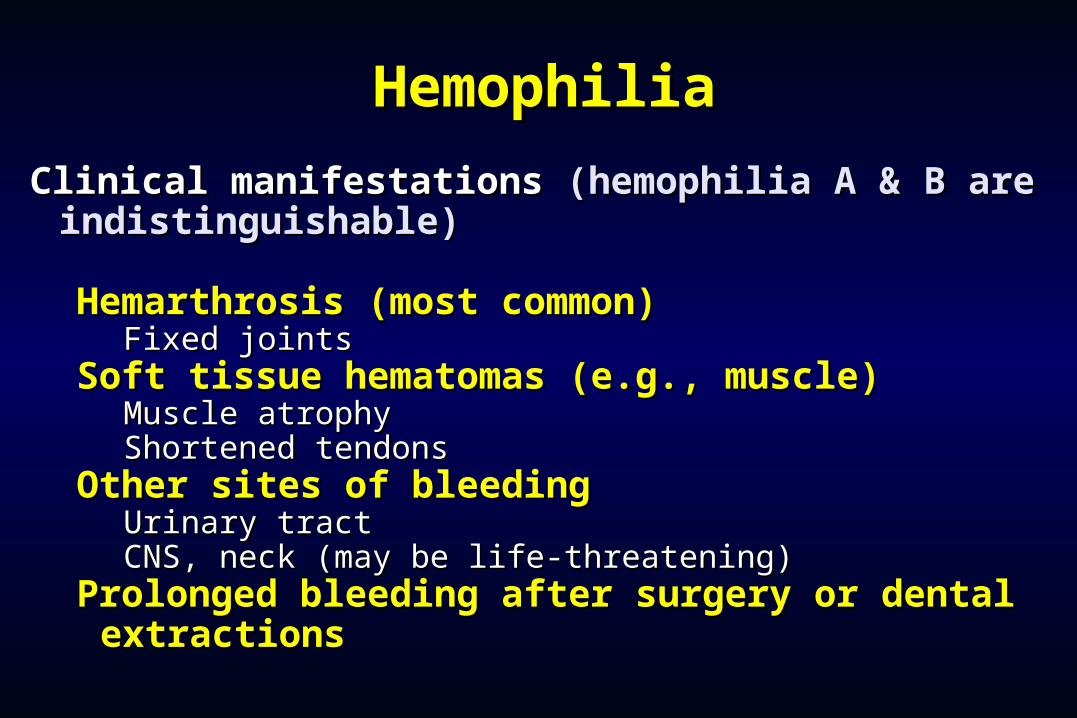
HemophiliaHemophilia
Clinical manifestations Clinical manifestations (hemophilia A & B are (hemophilia A & B are indistinguishable)indistinguishable)
Hemarthrosis (most common)Hemarthrosis (most common)Fixed jointsFixed joints
Soft tissue hematomas (e.g., muscle)Soft tissue hematomas (e.g., muscle)Muscle atrophyMuscle atrophyShortened tendonsShortened tendons
Other sites of bleedingOther sites of bleedingUrinary tractUrinary tractCNS, neck (may be life-threatening)CNS, neck (may be life-threatening)
Prolonged bleeding after surgery or dental Prolonged bleeding after surgery or dental extractionsextractions
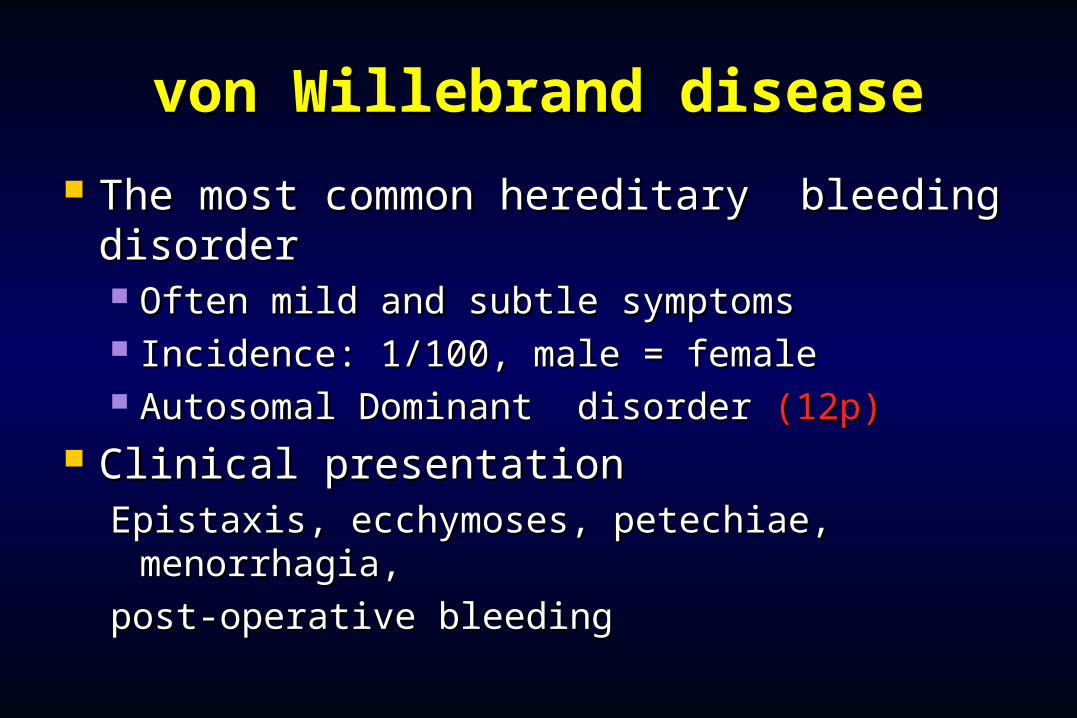
von Willebrand diseasevon Willebrand disease
The most common hereditary bleeding The most common hereditary bleeding disorderdisorder Often mild and subtle symptomsOften mild and subtle symptoms Incidence: 1/100, male = femaleIncidence: 1/100, male = female Autosomal Dominant disorder Autosomal Dominant disorder (12p)(12p)
Clinical presentationClinical presentationEpistaxis, ecchymoses, petechiae, Epistaxis, ecchymoses, petechiae,
menorrhagia, menorrhagia,
post-operative bleedingpost-operative bleeding
Treatment of von Willebrand Treatment of von Willebrand diseasedisease
CryoprecipitateCryoprecipitate Source of fibrinogen, factor VIII and VWFSource of fibrinogen, factor VIII and VWF Only plasma fraction that consistently contains VWF Only plasma fraction that consistently contains VWF
multimersmultimers Correction of bleeding time is variableCorrection of bleeding time is variable
DDAVP (Deamino-8-arginine vasopressin)DDAVP (Deamino-8-arginine vasopressin) Increases plasma VWF levels by stimulating secretion from Increases plasma VWF levels by stimulating secretion from
endotheliumendothelium Duration of response is variableDuration of response is variable Used for type 1 diseaseUsed for type 1 disease Dosage 0.3 µg/kg q 12 hr IVDosage 0.3 µg/kg q 12 hr IV
Factor VIII concentrate (Humate-P)Factor VIII concentrate (Humate-P) Virally inactivated productVirally inactivated product
Vitamin K deficiencyVitamin K deficiency
Source of vitamin K Source of vitamin K Green vegetablesGreen vegetablesSynthesized by intestinal floraSynthesized by intestinal flora
Required for synthesisRequired for synthesis Factors II, VII, IX ,XFactors II, VII, IX ,XProtein C and SProtein C and S
Causes of deficiencyCauses of deficiency MalnutritionMalnutritionBiliary obstructionBiliary obstruction
MalabsorptionMalabsorptionAntibiotic therapyAntibiotic therapy
TreatmentTreatment Vitamin KVitamin KFresh frozen plasmaFresh frozen plasma
25
Disorders of PlateletsDisorders of Platelets Thrombocytopenia – decreased numbers of platelets (below Thrombocytopenia – decreased numbers of platelets (below
100,000/mm100,000/mm33) ) Can lead to spontaneous bleeding, if low enough, and can be fatal Can lead to spontaneous bleeding, if low enough, and can be fatal
if bleeding occurs in the G.I. Tract, respiratory system or central if bleeding occurs in the G.I. Tract, respiratory system or central nervous system.nervous system.
Can be congenital or acquired; acquired is more common.Can be congenital or acquired; acquired is more common. Seen with:Seen with:
Generalized bone marrow suppressionGeneralized bone marrow suppression Acute viral infectionAcute viral infection Nutritional deficiencies of BNutritional deficiencies of B1212, folic acid and iron, folic acid and iron Bone marrow transplantBone marrow transplant drugs, especially heparin, and toxins, thiazide diuretics, gold, drugs, especially heparin, and toxins, thiazide diuretics, gold,
ethanol…ethanol… Immune reactionsImmune reactions

Sites of Bleeding in Sites of Bleeding in ThrombocytopeniaThrombocytopenia
Skin and mucous membranesSkin and mucous membranes PetechiaePetechiae EcchymosisEcchymosis Hemorrhagic vesiclesHemorrhagic vesicles Gingival bleeding and epistaxisGingival bleeding and epistaxis
MenorrhagiaMenorrhagia Gastrointestinal bleedingGastrointestinal bleeding Intracranial bleedingIntracranial bleeding
Classification of Platelet Classification of Platelet DisordersDisorders
Quantitative Quantitative disordersdisorders
Abnormal Abnormal distributiondistribution
Dilution effectDilution effect Decreased Decreased
productionproduction Increased Increased
destructiondestruction
Qualitative Qualitative disordersdisorders
Inherited disorders Inherited disorders (rare)(rare)
Acquired disordersAcquired disorders MedicationsMedications Chronic renal failureChronic renal failure Cardiopulmonary bypassCardiopulmonary bypass
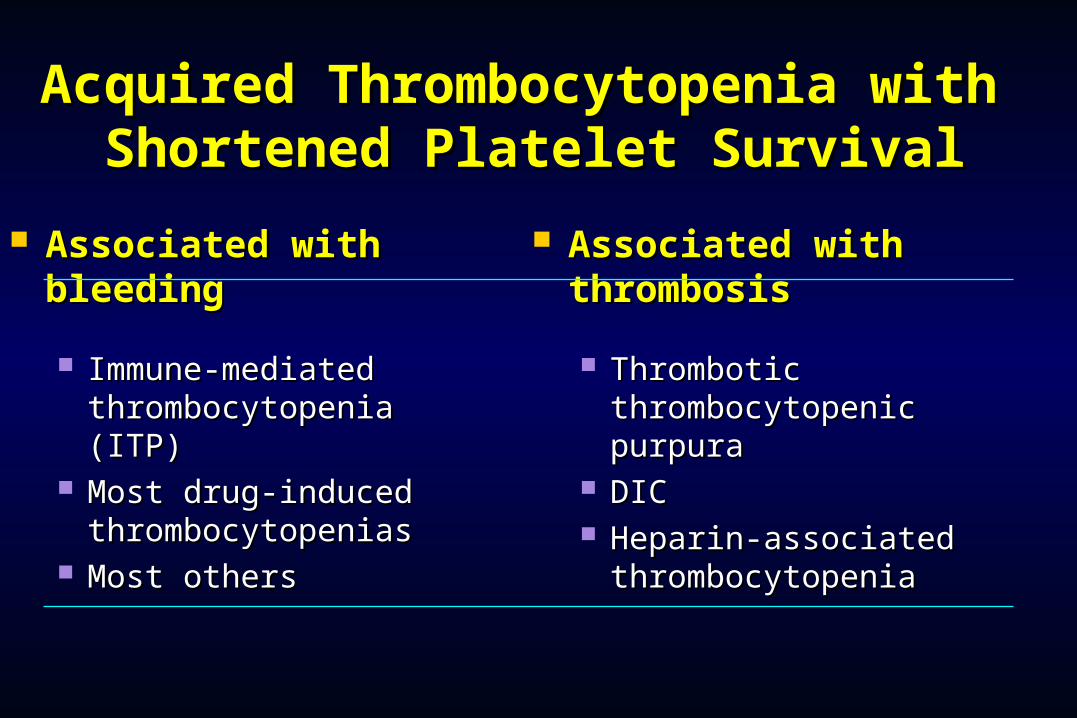
Acquired Thrombocytopenia with Acquired Thrombocytopenia with
Shortened Platelet SurvivalShortened Platelet Survival Associated with Associated with
bleedingbleeding
Immune-mediated Immune-mediated thrombocytopenia thrombocytopenia (ITP)(ITP)
Most drug-induced Most drug-induced thrombocytopeniasthrombocytopenias
Most othersMost others
Associated with Associated with thrombosisthrombosis
Thrombotic Thrombotic thrombocytopenic purpurathrombocytopenic purpura
DICDIC Heparin-associated Heparin-associated
thrombocytopeniathrombocytopenia
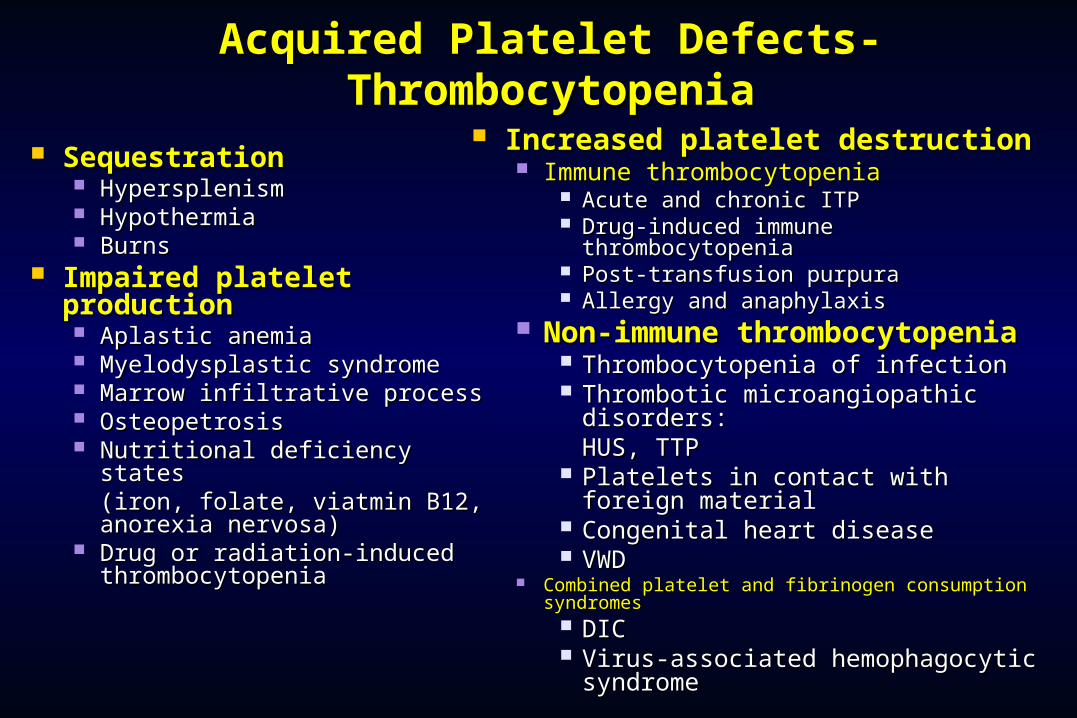
Acquired Platelet Defects-Acquired Platelet Defects-ThrombocytopeniaThrombocytopenia
SequestrationSequestration Hypersplenism Hypersplenism HypothermiaHypothermia BurnsBurns
Impaired platelet Impaired platelet productionproduction Aplastic anemiaAplastic anemia Myelodysplastic syndromeMyelodysplastic syndrome Marrow infiltrative processMarrow infiltrative process OsteopetrosisOsteopetrosis Nutritional deficiency states Nutritional deficiency states
(iron, folate, viatmin B12, (iron, folate, viatmin B12, anorexia nervosa)anorexia nervosa)
Drug or radiation-induced Drug or radiation-induced thrombocytopeniathrombocytopenia
Increased platelet destructionIncreased platelet destruction Immune thrombocytopeniaImmune thrombocytopenia
Acute and chronic ITPAcute and chronic ITP Drug-induced immune Drug-induced immune
thrombocytopeniathrombocytopenia Post-transfusion purpuraPost-transfusion purpura Allergy and anaphylaxisAllergy and anaphylaxis
Non-immune Non-immune thrombocytopeniathrombocytopenia
Thrombocytopenia of infectionThrombocytopenia of infection Thrombotic microangiopathic Thrombotic microangiopathic
disorders: disorders: HUS, TTPHUS, TTP
Platelets in contact with foreign Platelets in contact with foreign materialmaterial
Congenital heart diseaseCongenital heart disease VWDVWD
Combined platelet and fibrinogen consumption Combined platelet and fibrinogen consumption syndromessyndromes
DICDIC Virus-associated hemophagocytic Virus-associated hemophagocytic
syndromesyndrome
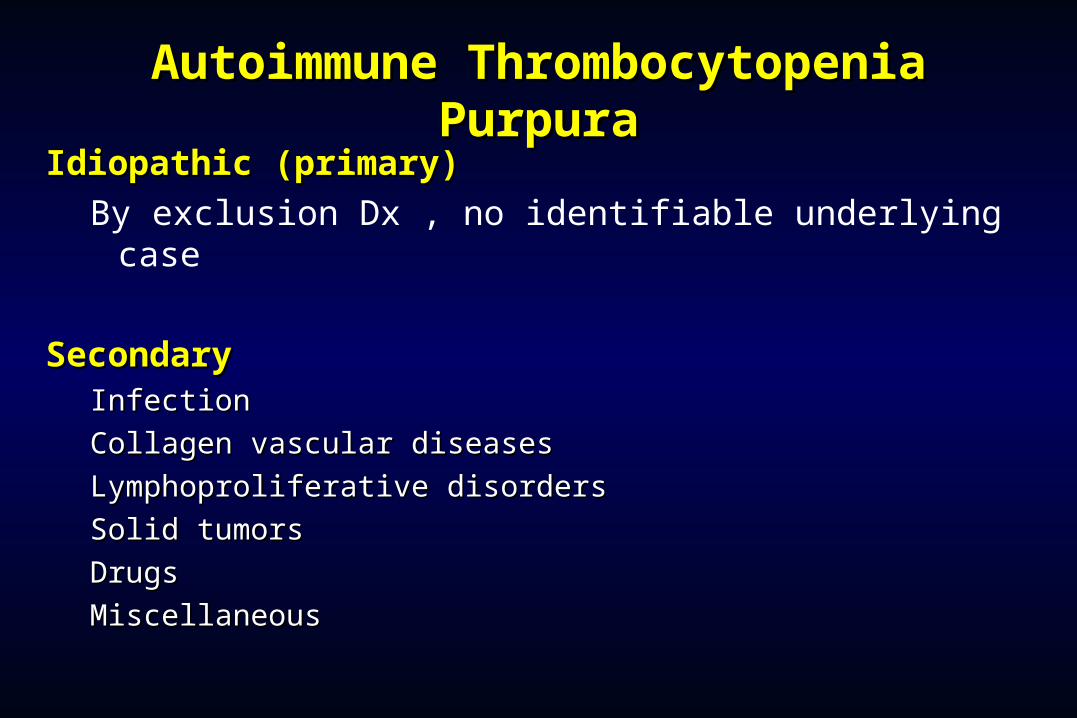
Autoimmune Thrombocytopenia Autoimmune Thrombocytopenia PurpuraPurpura
Idiopathic (primary)Idiopathic (primary)By exclusion Dx , no identifiable underlying case
SecondarySecondaryInfectionInfection
Collagen vascular diseasesCollagen vascular diseases
Lymphoproliferative disordersLymphoproliferative disorders
Solid tumorsSolid tumors
DrugsDrugs
MiscellaneousMiscellaneous

Features of Acute and Chronic ITPFeatures of Acute and Chronic ITP
Features AcuteITP Chronic ITP
Peak age Children (2-6 yrs)Adults (20-40 yrs)Female:male 1:1 3:1Antecedent infection Common RareOnset of symptoms AbruptAbrupt-indolentPlatelet count at presentation <20,000<50,000Duration 2-6 weeks Long-termSpontaneous remission Common(80%)Uncommon

Initial Treatment of ITPInitial Treatment of ITP
Platelet count Symptoms Treatment (per µl)
>50,000 None
20-50,000 Not bleeding NoneBleeding Glucocorticoids
IVIG
<20,000 Not bleedingGlucocorticoids
Bleeding GlucocorticoidsIVIGHospitalization
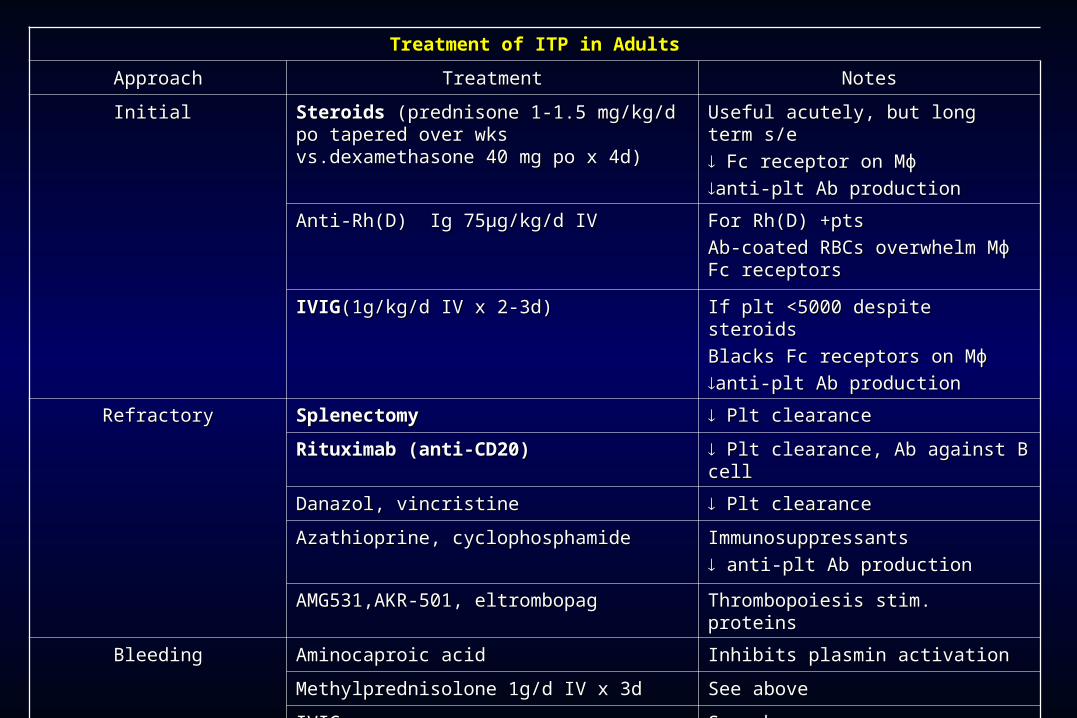
Treatment of ITP in AdultsTreatment of ITP in Adults
ApproachApproach TreatmentTreatment NotesNotes
Initial Initial Steroids Steroids (prednisone 1-1.5 mg/kg/d po (prednisone 1-1.5 mg/kg/d po tapered over wks vs.dexamethasone 40 tapered over wks vs.dexamethasone 40 mg po x 4d)mg po x 4d)
Useful acutely, but long term s/eUseful acutely, but long term s/e
Fc receptor on MɸFc receptor on Mɸ
anti-plt Ab productionanti-plt Ab production
Anti-Rh(D) Ig 75μg/kg/d IVAnti-Rh(D) Ig 75μg/kg/d IV For Rh(D) +ptsFor Rh(D) +pts
Ab-coated RBCs overwhelm Mɸ Ab-coated RBCs overwhelm Mɸ Fc receptorsFc receptors
IVIGIVIG(1g/kg/d IV x 2-3d)(1g/kg/d IV x 2-3d) If plt <5000 despite steroids If plt <5000 despite steroids
Blacks Fc receptors on MɸBlacks Fc receptors on Mɸ
anti-plt Ab productionanti-plt Ab production
RefractoryRefractory Splenectomy Splenectomy Plt clearancePlt clearance
Rituximab (anti-CD20)Rituximab (anti-CD20) Plt clearance, Ab against B cellPlt clearance, Ab against B cell
Danazol, vincristineDanazol, vincristine Plt clearancePlt clearance
Azathioprine, cyclophosphamideAzathioprine, cyclophosphamide ImmunosuppressantsImmunosuppressants
anti-plt Ab productionanti-plt Ab production
AMG531,AKR-501, eltrombopagAMG531,AKR-501, eltrombopag Thrombopoiesis stim. proteinsThrombopoiesis stim. proteins
BleedingBleeding Aminocaproic acid Aminocaproic acid Inhibits plasmin activationInhibits plasmin activation
Methylprednisolone 1g/d IV x 3dMethylprednisolone 1g/d IV x 3d See aboveSee above
IVIGIVIG See aboveSee above
Chronic refractoryChronic refractory Autologous HSCTAutologous HSCT InvestigationalInvestigational
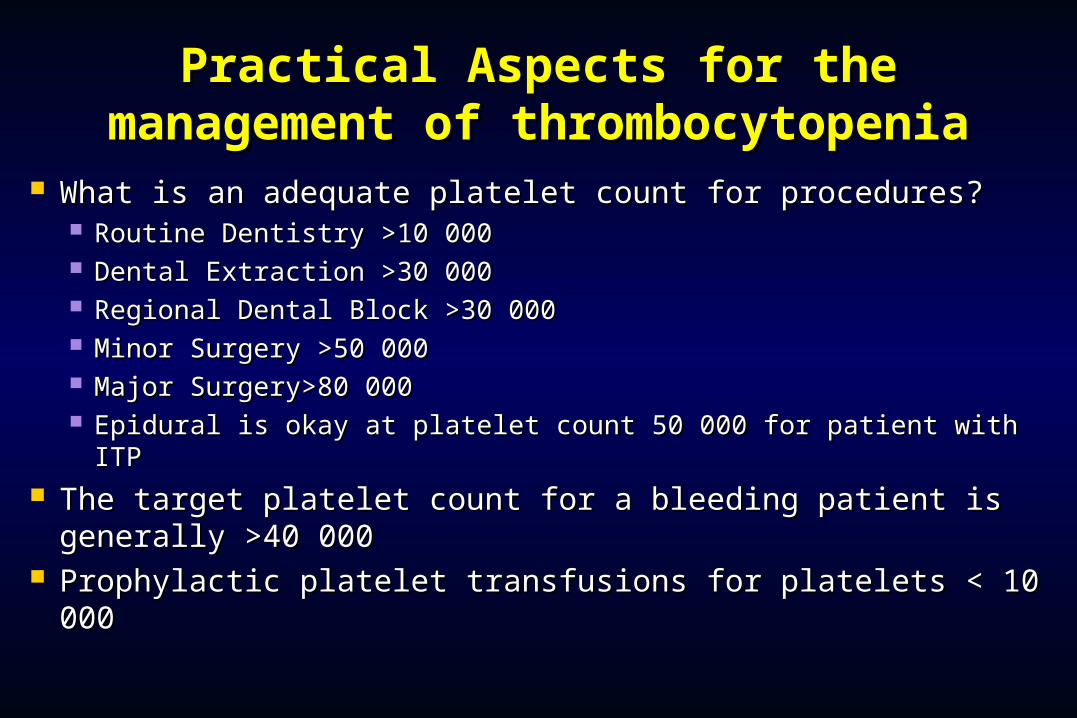
Practical Aspects for the Practical Aspects for the management of thrombocytopeniamanagement of thrombocytopenia
What is an adequate platelet count for procedures?What is an adequate platelet count for procedures? Routine Dentistry >10 000Routine Dentistry >10 000 Dental Extraction >30 000Dental Extraction >30 000 Regional Dental Block >30 000Regional Dental Block >30 000 Minor Surgery >50 000Minor Surgery >50 000 Major Surgery>80 000Major Surgery>80 000 Epidural is okay at platelet count 50 000 for patient with ITPEpidural is okay at platelet count 50 000 for patient with ITP
The target platelet count for a bleeding patient is The target platelet count for a bleeding patient is generally >40 000generally >40 000
Prophylactic platelet transfusions for platelets < 10 000Prophylactic platelet transfusions for platelets < 10 000

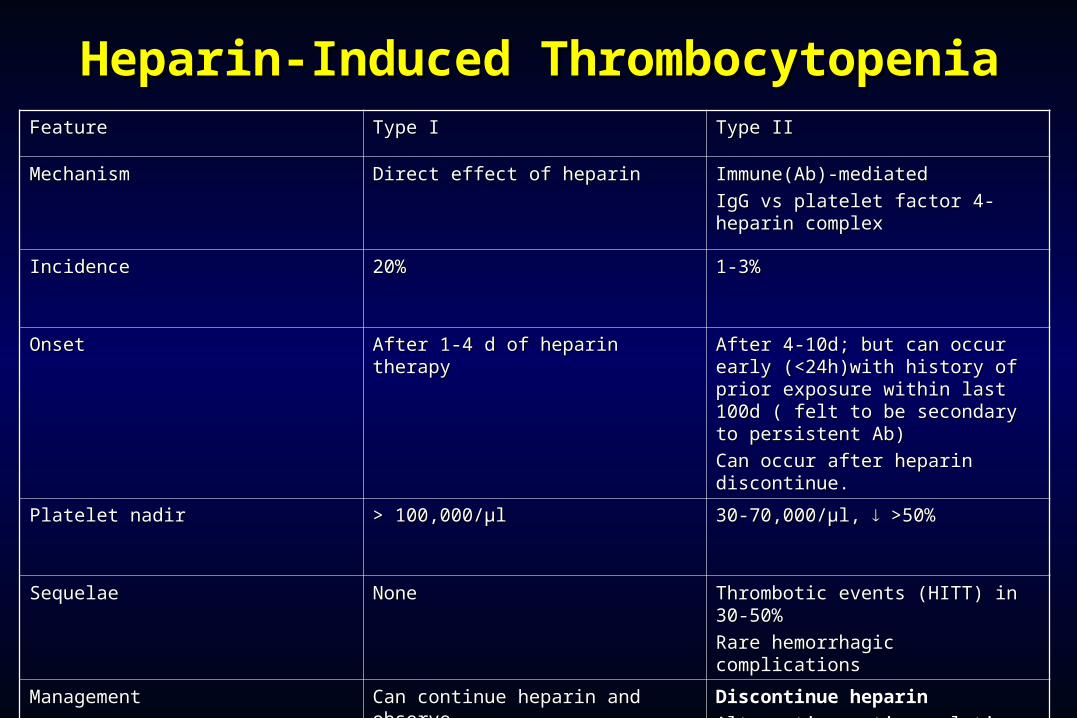
Heparin-Induced Heparin-Induced ThrombocytopeniaThrombocytopenia
FeatureFeature Type IType I Type IIType II
MechanismMechanism Direct effect of heparinDirect effect of heparin Immune(Ab)-mediatedImmune(Ab)-mediated
IgG vs platelet factor 4-heparin IgG vs platelet factor 4-heparin complexcomplex
Incidence Incidence 20%20% 1-3%1-3%
OnsetOnset After 1-4 d of heparin therapyAfter 1-4 d of heparin therapy After 4-10d; but can occur early After 4-10d; but can occur early (<24h)with history of prior (<24h)with history of prior exposure within last 100d ( felt to exposure within last 100d ( felt to be secondary to persistent Ab)be secondary to persistent Ab)
Can occur after heparin Can occur after heparin discontinue.discontinue.
Platelet nadir Platelet nadir > 100,000/μl> 100,000/μl 30-70,000/μl, 30-70,000/μl, >50% >50%
SequelaeSequelae NoneNone Thrombotic events (HITT) in 30-Thrombotic events (HITT) in 30-50%50%
Rare hemorrhagic complicationsRare hemorrhagic complications
ManagementManagement Can continue heparin and Can continue heparin and observeobserve
Discontinue heparinDiscontinue heparin
Alternative anticoagulation Alternative anticoagulation (lepirudin or arga)(lepirudin or arga)
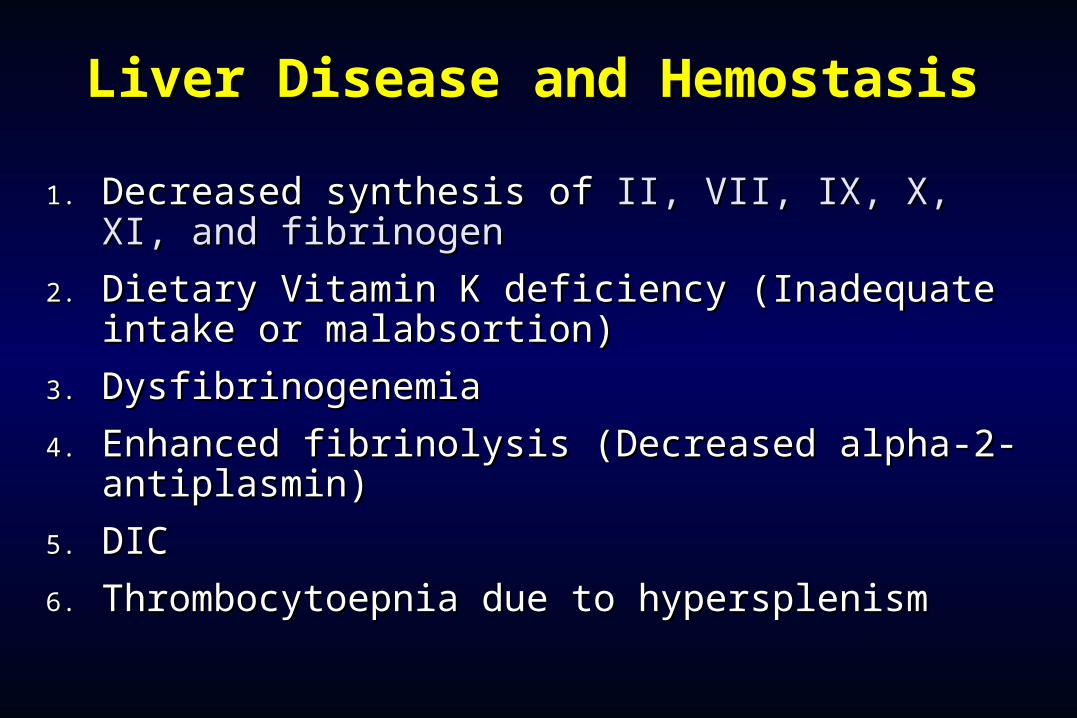
Liver Disease and HemostasisLiver Disease and Hemostasis
1.1. Decreased synthesis of Decreased synthesis of II, VII, IX, X, XI, and II, VII, IX, X, XI, and fibrinogenfibrinogen
2.2. Dietary Vitamin K deficiency (Inadequate intake Dietary Vitamin K deficiency (Inadequate intake or malabsortion)or malabsortion)
3.3. DysfibrinogenemiaDysfibrinogenemia
4.4. Enhanced fibrinolysis (Decreased alpha-2-Enhanced fibrinolysis (Decreased alpha-2-antiplasmin)antiplasmin)
5.5. DICDIC
6.6. Thrombocytoepnia due to hypersplenismThrombocytoepnia due to hypersplenism
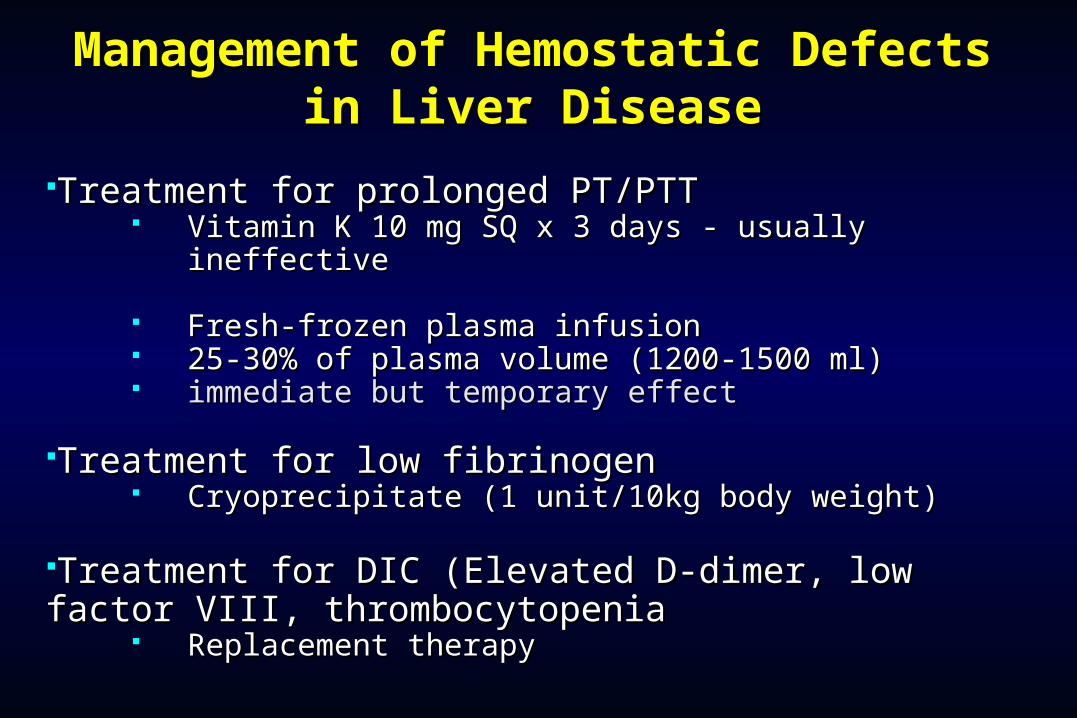
Management of Hemostatic Management of Hemostatic Defects in Liver DiseaseDefects in Liver Disease
Treatment for prolonged PT/PTTTreatment for prolonged PT/PTT Vitamin K 10 mg SQ x 3 days - usually ineffectiveVitamin K 10 mg SQ x 3 days - usually ineffective
Fresh-frozen plasma infusionFresh-frozen plasma infusion 25-30% of plasma volume (1200-1500 ml) 25-30% of plasma volume (1200-1500 ml) immediate but temporary effectimmediate but temporary effect
Treatment for low fibrinogenTreatment for low fibrinogen Cryoprecipitate (1 unit/10kg body weight)Cryoprecipitate (1 unit/10kg body weight)
Treatment for DIC (Elevated D-dimer, low factor Treatment for DIC (Elevated D-dimer, low factor VIII, thrombocytopeniaVIII, thrombocytopenia
Replacement therapyReplacement therapy

Vitamin K deficiency due to warfarin Vitamin K deficiency due to warfarin overdoseoverdose
Managing high INR valuesManaging high INR values
Clinical situation Guidelines
INR therapeutic-5 Lower or omit next dose;Resume therapy when INR is therapeutic
INR 5-9; no bleeding Lower or omit next dose;Resume therapy when INR is therapeutic
Omit dose and give vitamin K (1-2.5 mg po)
Rapid reversal: vitamin K 2-4 mg po (repeat)
INR >9; no bleeding Omit dose; vitamin K 3-5 mg po; repeat as necessaryResume therapy at lower dose when INR therapeutic
Chest 2001:119;22-38s (supplement)

Vitamin K deficiency due to Vitamin K deficiency due to warfarin overdosewarfarin overdose
Managing high INR values in bleeding Managing high INR values in bleeding patientspatients
Clinical situation Guidelines
INR > 20; serious bleeding Omit warfarinVitamin K 10 mg slow IV infusionFFP or PCC (depending on urgency)Repeat vitamin K injections every 12 hrs as needed
Any life-threatening bleeding Omit warfarinVitamin K 10 mg slow IV infusionPCC ( or recombinant human factor VIIa)Repeat vitamin K injections every 12 hrs as needed
Chest 2001:119;22-38s (supplement)
Hemorrhage in Oral SurgeryHemorrhage in Oral Surgery
Hemorrhage following Oral Surgical Hemorrhage following Oral Surgical procedures can occur due to procedures can occur due to Local Local or or SystemicSystemic causes. causes.
In healthy patients the postoperative In healthy patients the postoperative bleeding is mainly due to local causes. bleeding is mainly due to local causes.
Local causes of hemorrhage originate in Local causes of hemorrhage originate in either either Soft TissueSoft Tissue or or BoneBone..
Local causes of hemorrhage in oral Local causes of hemorrhage in oral surgery –surgery –Soft tissue bleedingSoft tissue bleeding
Soft tissue bleeding is either arterial, venous, or Soft tissue bleeding is either arterial, venous, or capillary in nature.capillary in nature.
Arterial bleedingArterial bleeding is bright red and spurting in nature. is bright red and spurting in nature. Arteries in the soft tissues at risk during oral surgical Arteries in the soft tissues at risk during oral surgical
procedures are the lies posterior portion of hard procedures are the lies posterior portion of hard palate) greater palatine artery and the buccal artery palate) greater palatine artery and the buccal artery (lies lateral to the retromolar pad) (lies lateral to the retromolar pad)
Venous bloodVenous blood is dark red in color and flows steadily is dark red in color and flows steadily and heavily especially if the vein is large.and heavily especially if the vein is large.
Capillary bleedingCapillary bleeding is bright red in color and is more is bright red in color and is more of a minimal ooze.of a minimal ooze.
Local causes –Local causes – Osseous (Bony) bleeding in Osseous (Bony) bleeding in oral surgeryoral surgery
Troublesome bone bleeding originates either Troublesome bone bleeding originates either from nutrient canals in the alveolar region, from nutrient canals in the alveolar region, central vessels, such as the central vessels, such as the inferior alveolar inferior alveolar artery,artery, or from central vascular lesions or from central vascular lesions (Hemangioma or Vascular malformation)(Hemangioma or Vascular malformation)
Systemic causes of hemorrhage in Systemic causes of hemorrhage in oral surgeryoral surgery
Some patients with heriditary conditions such as Some patients with heriditary conditions such as hemophilia, Von Willebrand’s disease are susceptible hemophilia, Von Willebrand’s disease are susceptible for hemorrhage following oral surgical procedures.for hemorrhage following oral surgical procedures.
Patients with thrombocytopenia, are at risk of Patients with thrombocytopenia, are at risk of prolonged bleeding after surgery.prolonged bleeding after surgery.
Patients with uncontrolled hypertension.Patients with uncontrolled hypertension. Patients with H/O prosthetic heart valve replacement, Patients with H/O prosthetic heart valve replacement,
Stroke (Cerebrovascular accidentStroke (Cerebrovascular accident) e.t.c., take oral ) e.t.c., take oral anticoagulants like Aspirin or Warfarinanticoagulants like Aspirin or Warfarin to prevent the to prevent the occurrence of a thromboembolic episode. occurrence of a thromboembolic episode.
These patients are also at risk of prolonged severe These patients are also at risk of prolonged severe bleeding during and after an oral surgical procedure.bleeding during and after an oral surgical procedure.
Types of Hemorrhage - Types of Hemorrhage - Primary Primary HemorrhageHemorrhage
This occurs during the surgery, as a result of This occurs during the surgery, as a result of injury like cutting or laceration of the artery injury like cutting or laceration of the artery or bleeding from bone.or bleeding from bone.
This also occurs when surgery is done in an This also occurs when surgery is done in an infected area with a lot of granulation tissue.infected area with a lot of granulation tissue.
It can also occur after a very short period of It can also occur after a very short period of time immediately after surgery. time immediately after surgery.
This type of bleeding is really normal and can This type of bleeding is really normal and can be controlled easily.be controlled easily.
Intermediate / Reactionary Intermediate / Reactionary HemorrhageHemorrhage
This type of bleeding occurs within a few hours after This type of bleeding occurs within a few hours after surgery.surgery.
This type of bleeding occurs as a result of failure of This type of bleeding occurs as a result of failure of coagulation to occur (as in patients with systemic coagulation to occur (as in patients with systemic bleeding problems or those on anticoagulants)bleeding problems or those on anticoagulants)
Patients who have unknowingly disturbed / dislodged Patients who have unknowingly disturbed / dislodged the clot are also prone for this type of bleeding.the clot are also prone for this type of bleeding.
Secondary HemorrhageSecondary Hemorrhage
This occurs after This occurs after 7 to 10 days7 to 10 days after surgery. after surgery. This is mainly due to partial division of blood This is mainly due to partial division of blood vessel in combination with infection of the vessel in combination with infection of the wound (Like patient’s who undergo radical neck wound (Like patient’s who undergo radical neck dissection e.t.c.,).dissection e.t.c.,).
This type of bleeding is not very frequently This type of bleeding is not very frequently encountered after oral surgery procedures.encountered after oral surgery procedures.
Management of Primary Hemorrhage in Management of Primary Hemorrhage in Normal patientsNormal patients
The management of bleeding during surgery The management of bleeding during surgery (Primary (Primary bleeding)bleeding) can be achieved by the following means, can be achieved by the following means,
(i)(i) Securing / ligation of blood vessels with silk sutures.Securing / ligation of blood vessels with silk sutures.
(ii)(ii) Use of pressure swab to achieve hemostasis.Use of pressure swab to achieve hemostasis.
(iii)(iii) Use of electrocautery to achieve hemostasis.Use of electrocautery to achieve hemostasis.
(iv)(iv) Use of hemostatic agents like bone wax, Use of hemostatic agents like bone wax, surgicel,e.t.c.,surgicel,e.t.c.,
(v)(v) Hypotensive anaesthesia (G.A) and use of Hypotensive anaesthesia (G.A) and use of vasoconstrictors in L.A.vasoconstrictors in L.A.
Local Measures Local Measures ( Synthetic ( Synthetic Materials)Materials)
There are several materials that are commercially There are several materials that are commercially available that are used locally for achieving available that are used locally for achieving adequate hemostasis.adequate hemostasis.
Surgical (Oxidised Regenerated Cellulose)Surgical (Oxidised Regenerated Cellulose) Gelfoam with activated thrombinGelfoam with activated thrombin Gelfoam with activated thrombinGelfoam with activated thrombin Avitene Avitene (Microfibrillar Collagen)(Microfibrillar Collagen) Etik Collagen Etik Collagen (Packed collagen)(Packed collagen) Tranexamic acid 5%Tranexamic acid 5% Tranexamic acid 5% in SyringeTranexamic acid 5% in Syringe Irrigation of wound with Tranexamic acidIrrigation of wound with Tranexamic acid Suturing the woundSuturing the wound Pressure with oral packsPressure with oral packs
Local Measures: Local Measures: Surgicel (Oxidised Surgicel (Oxidised Regenerated Cellulose)Regenerated Cellulose)

Local measures:Local measures: Gelfoam with Gelfoam with activated thrombinactivated thrombin
Local Measures: Local Measures: Avitene Avitene (Microfibrillar Collagen)(Microfibrillar Collagen)

Local Measures: Etik Collagen Local Measures: Etik Collagen (Packed collagen)(Packed collagen)
Local Measures: Local Measures: Tranexamic acid 5%Tranexamic acid 5%
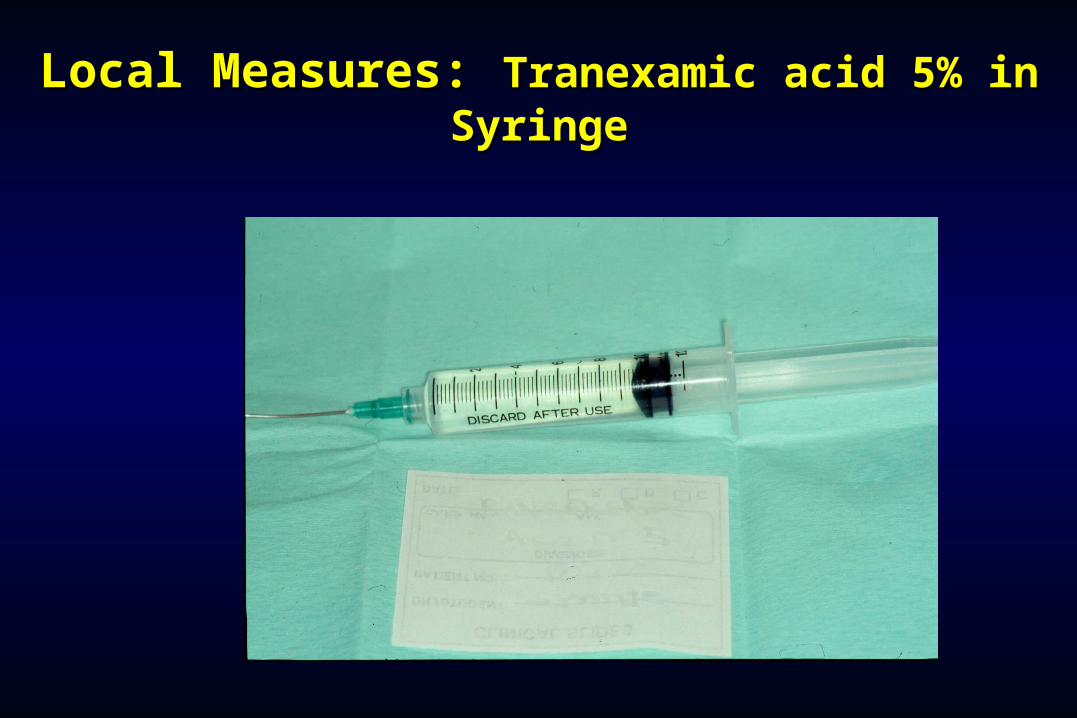
Local Measures:Local Measures: Tranexamic acid 5% in Tranexamic acid 5% in SyringeSyringe
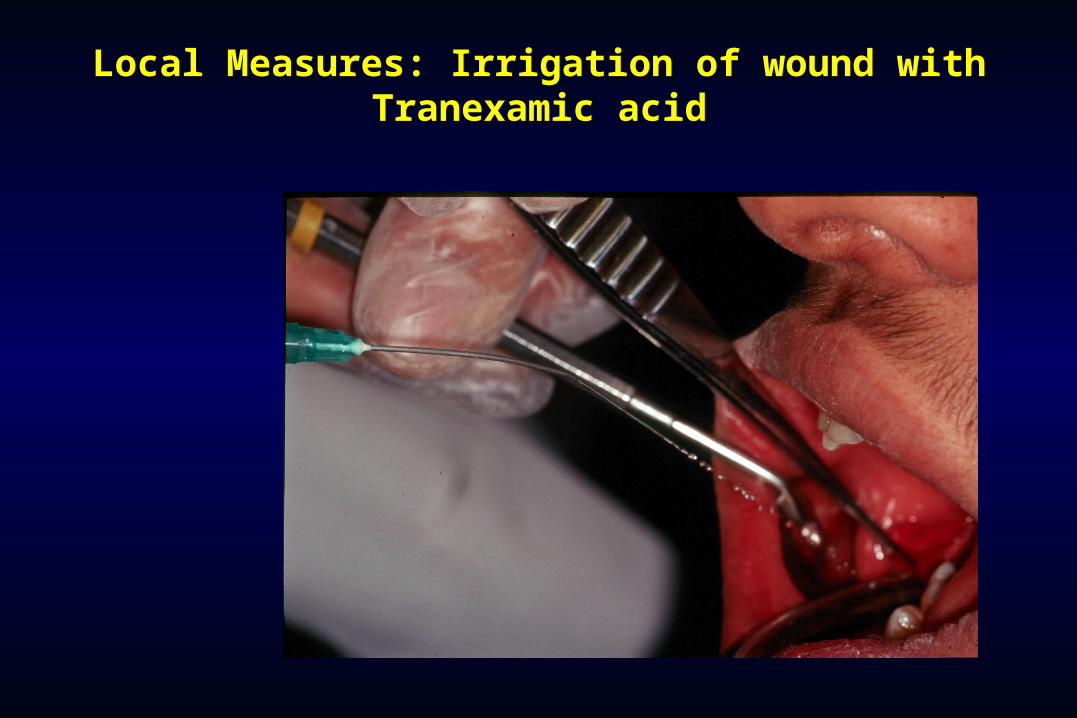
Local Measures: Irrigation of wound with Local Measures: Irrigation of wound with Tranexamic acidTranexamic acid
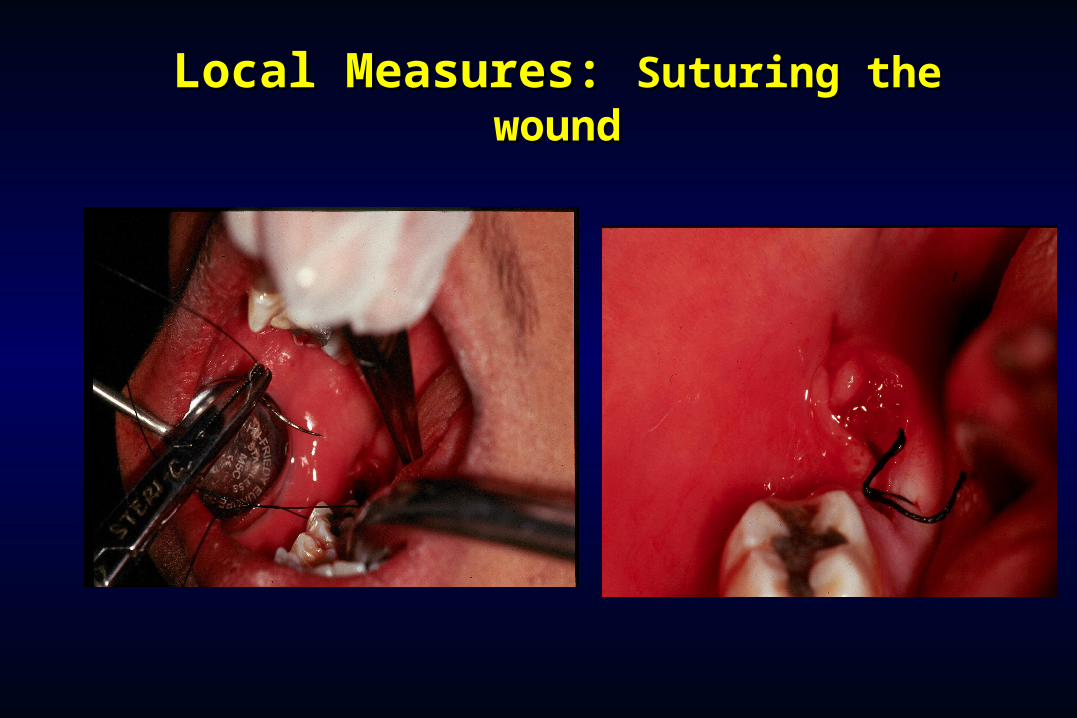
Local Measures:Local Measures: Suturing the Suturing the woundwound
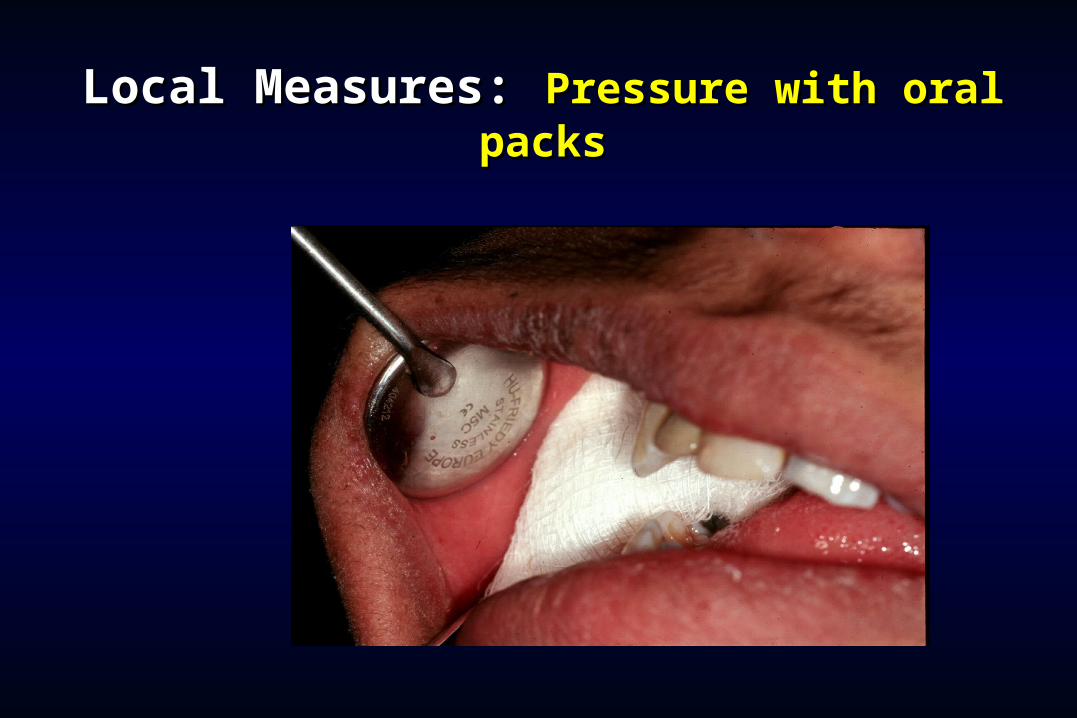
Local Measures:Local Measures: Pressure with oral Pressure with oral packspacks

Management of Intermediate Hemorrhage in Management of Intermediate Hemorrhage in Normal patientsNormal patients
The management of bleeding that occurs immediately The management of bleeding that occurs immediately after surgery (Reactionary bleeding) involves proper after surgery (Reactionary bleeding) involves proper examination of the surgical wound to identify the site examination of the surgical wound to identify the site of bleeding (i.e ) from bone or soft tissue.of bleeding (i.e ) from bone or soft tissue.
(i)(i) If bleeding is from bone then the hemostatic agents If bleeding is from bone then the hemostatic agents like bone wax or gelfoam is usually used.like bone wax or gelfoam is usually used.
(ii)(ii) If bleeding is from soft tissues then, ligation / If bleeding is from soft tissues then, ligation / cauterization of blood vessels along with the use of cauterization of blood vessels along with the use of hemostatic agents like surgicel and suturing of the hemostatic agents like surgicel and suturing of the wound is carried out.wound is carried out.
Management of Secondary Hemorrhage in Management of Secondary Hemorrhage in Normal patientsNormal patients
The management of this type of bleeding that occurs a The management of this type of bleeding that occurs a few days after surgery involves the removal of any few days after surgery involves the removal of any debris from the wound surface that promotes the debris from the wound surface that promotes the infection of the woundinfection of the wound..
Identify the source of bleeding and treat as would be Identify the source of bleeding and treat as would be done in a patient with secondary bleeding.done in a patient with secondary bleeding.
Surgical stents can be placed over extraction sockets Surgical stents can be placed over extraction sockets for stabilization of clot and prevention of wound for stabilization of clot and prevention of wound contamination.contamination.

Management of Hemorrhage in patients Management of Hemorrhage in patients with bleeding disorders / and those on with bleeding disorders / and those on
anticoagulant therapyanticoagulant therapy The usual protocol involved in the treatment of The usual protocol involved in the treatment of
this group of patients consists of pre-operative this group of patients consists of pre-operative blood investigations and preoperative correction blood investigations and preoperative correction of the underlying deficiency (Replacement of of the underlying deficiency (Replacement of Clotting factors / platelets) if any in these patients.Clotting factors / platelets) if any in these patients.
Subsequently, after this appropriate local Subsequently, after this appropriate local measures are used to decrease the chances of measures are used to decrease the chances of post-operative bleeding.post-operative bleeding.
Management of Hemorrhage in Management of Hemorrhage in patients with Uncontrolled patients with Uncontrolled
Hypertension.Hypertension. This group of patients need appropriate medical This group of patients need appropriate medical
consultation for initiation of medical treatment to consultation for initiation of medical treatment to decrease their Blood Pressure.decrease their Blood Pressure.
Thus once their B.P is controlled, then the bleeding Thus once their B.P is controlled, then the bleeding decreases and with local measures the hemorrhage decreases and with local measures the hemorrhage is controlled.is controlled.
Approach to Post-operative Approach to Post-operative bleedingbleeding
1.1. Is the bleeding local or due to a hemostatic failure?Is the bleeding local or due to a hemostatic failure?1.1. Local: Single site of bleeding usually rapid with minimal Local: Single site of bleeding usually rapid with minimal
coagulation test abnormalitiescoagulation test abnormalities2.2. Hemostatic failure: Multiple site or unusual pattern with Hemostatic failure: Multiple site or unusual pattern with
abnormal coagulation testsabnormal coagulation tests
2.2. Evaluate for causes of peri-operative hemostatic failureEvaluate for causes of peri-operative hemostatic failure1.1. Preexisting abnormalityPreexisting abnormality2.2. Special cases (e.g. Cardiopulmonmary bypass)Special cases (e.g. Cardiopulmonmary bypass)
3.3. Diagnosis of hemostatic failureDiagnosis of hemostatic failure1.1. Review pre-operative testingReview pre-operative testing2.2. Obtain updated testingObtain updated testing
Laboratory Evaluation of BleedingLaboratory Evaluation of BleedingOverviewOverview
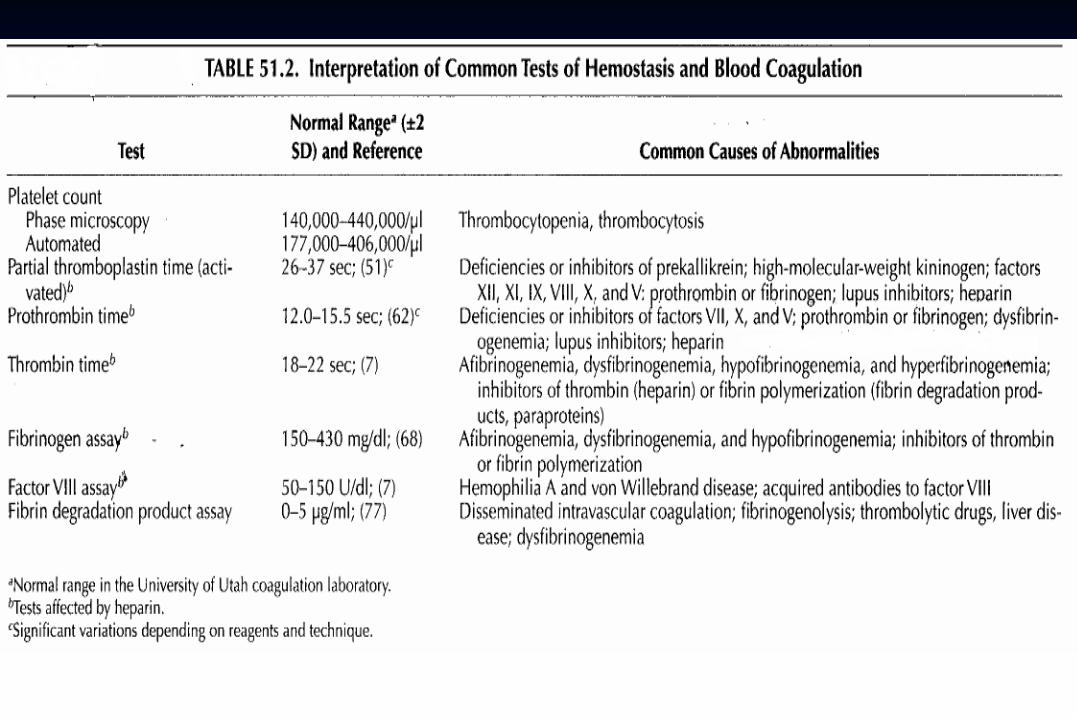
CBC and smearCBC and smear Platelet countPlatelet count ThrombocytopeniaThrombocytopeniaRBC and platelet morphologyRBC and platelet morphology TTP, DIC, etc.TTP, DIC, etc.
CoagulationCoagulation Prothrombin timeProthrombin time Extrinsic/common pathwaysExtrinsic/common pathwaysPartial thromboplastin timePartial thromboplastin time Intrinsic/common pathwaysIntrinsic/common pathwaysCoagulation factor assaysCoagulation factor assays Specific factor deficienciesSpecific factor deficiencies50:50 mix50:50 mix Inhibitors (e.g., antibodies)Inhibitors (e.g., antibodies)Fibrinogen assayFibrinogen assay Decreased fibrinogenDecreased fibrinogenThrombin timeThrombin time Qualitative/quantitativeQualitative/quantitative
fibrinogen defectsfibrinogen defectsFDPs or D-dimerFDPs or D-dimer Fibrinolysis (DIC)Fibrinolysis (DIC)
Platelet functionPlatelet function von Willebrand factorvon Willebrand factor vWDvWDBleeding timeBleeding time In vivoIn vivo test (non-specific) test (non-specific)Platelet function analyzer (PFA)Platelet function analyzer (PFA) Qualitative platelet Qualitative platelet
disorders disorders and vWD and vWDPlatelet function testsPlatelet function tests Qualitative platelet disordersQualitative platelet disorders
LABORATORY EVALUATIONLABORATORY EVALUATION
PLATELET COUNTPLATELET COUNT BLEEDING TIME (BT)BLEEDING TIME (BT) PROTHROMBIN TIME (PT)PROTHROMBIN TIME (PT) PARTIAL THROMBOPLASTIN TIME PARTIAL THROMBOPLASTIN TIME
(PTT)(PTT) THROMBIN TIME (TT)THROMBIN TIME (TT)
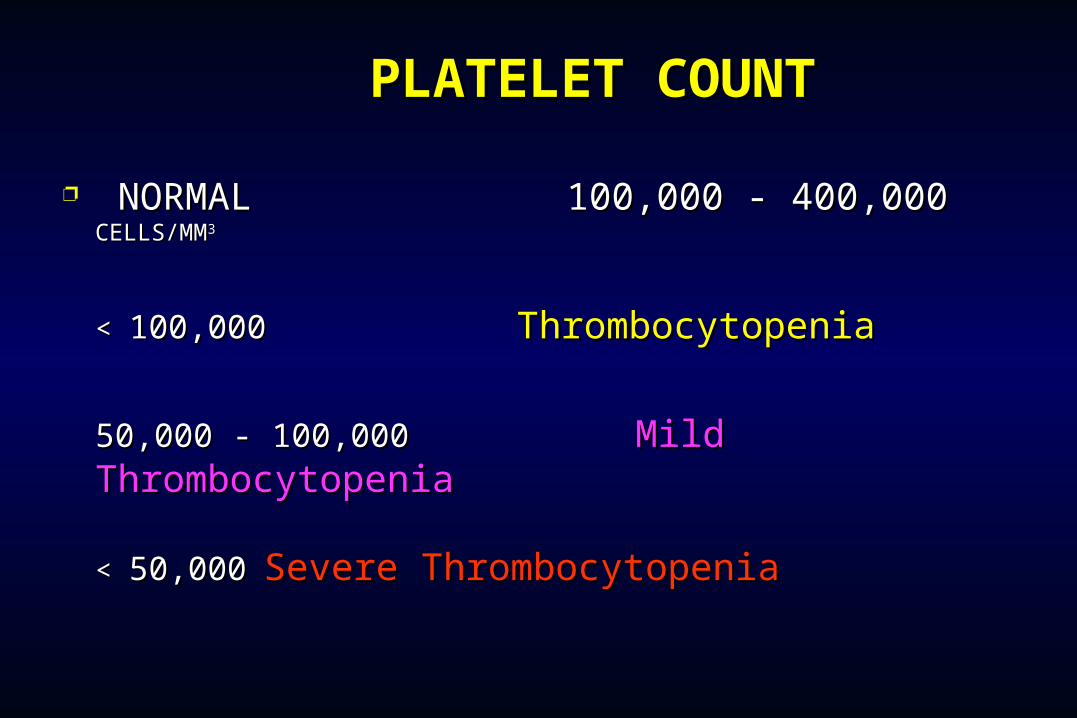
PLATELET COUNTPLATELET COUNT
NORMAL 100,000 - 400,000NORMAL 100,000 - 400,000 CELLS/MM CELLS/MM33
< < 100,000100,000 ThrombocytopeniaThrombocytopenia
50,000 - 100,00050,000 - 100,000 Mild Mild ThrombocytopeniaThrombocytopenia
< < 50,00050,000 Severe ThrombocytopeniaSevere Thrombocytopenia

BLEEDING TIMEBLEEDING TIME
PROVIDES ASSESSMENT OF PLATELET COUNT AND FUNCTION
NORMAL VALUENORMAL VALUE
2-8 MINUTES2-8 MINUTES

PROTHROMBIN TIME
Measures Effectiveness of the Extrinsic Measures Effectiveness of the Extrinsic PathwayPathway
NORMAL VALUENORMAL VALUE
10-15 SECS ( INR : 1 )10-15 SECS ( INR : 1 )

PARTIAL THROMBOPLASTIN PARTIAL THROMBOPLASTIN TIMETIME
Measures Effectiveness of the Intrinsic Measures Effectiveness of the Intrinsic PathwayPathway
NORMAL VALUENORMAL VALUE
25-40 SECS25-40 SECS
THROMBIN TIME
Time for Thrombin To Convert Fibrinogen Fibrin
A Measure of Fibrinolytic Pathway
NORMAL VALUENORMAL VALUE
9-13 SECS9-13 SECS









![Acute Gastrointestinal Hemorrhage: Radiologic Diagnosis ... · bleeding are peptic ulcer disease, variceal bleeding, Mallory-Weisstear,vascularlesions,andneoplasms(Table1) [2]. Lower](https://static.fdocuments.us/doc/165x107/6021c6749b53ea1a471bc940/acute-gastrointestinal-hemorrhage-radiologic-diagnosis-bleeding-are-peptic.jpg)








