Blastocystis hominis
26
BLASTOCYSTIS HOMINIS
-
Upload
anady-eleccion -
Category
Health & Medicine
-
view
2.876 -
download
1
Transcript of Blastocystis hominis

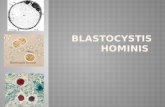
BLASTOCYSTIS HOMINIS

Wet mount

Initially described by Prowasek and Alexeieff, then named by Brumpt in 1912
Blastocystis hominis is an inhabitant of the lower intestinal tract of humans and other animals
Formerly classified as a yeast under the genus Schizosaccharomyces, while other taxonomists considered it to be related to Blastomyces

Lacks a cell wall but has a mitochondrion with protozoan morphology.
Capable of pseudopodial extension and retraction
Asexual reproduction by binary fission or sporulation under strict anaerobic conditions
Optimal growth= 37 oC in the presence of bacteria; does not grow on fungal media

Parasite Biology Multiplication of Blastocystis hominis is by
binary fission Transmitted by fecal-oral route Morphological forms:
1. Vacuolated
2. Ameba-like
3. Granular
4. Multiple fission
5. Cyst
6. Avacuolar

Vacuolated form Most predominant form in fecal specimen Spherical in shape, measuring 5-10 µm in
diameter Large central vacuole pushes the cytoplasm
and nuclei to the periphery of the cell Sometimes, very thick capsule surround them Prominent central vacuole has been found to be
a reproductive organelle Main type of Blastocystis causing diarrhea

Ameba-like forms
Occasionally observed in stool samples Exhibit active extension and retraction of
pseudopodia The nuclear chromatin, when visible,
characteristically shows peripheral clumping Appears to be an intermediate stage
between the vacuolar and pre-cystic form Allows the parasite to ingest bacteria to
enhance encystment

Granular forms
Mainly observed from old cultures Diameter of the cell varies from 10 -60
µm Granular contents develop into daughter
cells of the ameba-form when the cell ruptures

Multiple Fission
Arise from vacuolated forms It is believed that these multiple fission
forms produce many vacuolated forms.

Cystic form Size in about 3-55 µm Has a very prominent and thick osmophilic
electron dense wall Appears as a sharply demarcated polymorphic,
but mostly oval or circular, dense body surrounded by a loose outer membranous layer (seen in contrast microscopy)
Membranous layer corresponds to the fibrillar layer described around the cyst at ultrastructural level; easiest diagnostic feature

It is assumed that the thick-walled cyst might be responsible for external transmission while those cysts with thin walls might be the cause of re-infection within a host’s intestinal tract



Pathogenesis and Clinical Manifestation Blastocystosis- infection with Blastocystis
hominis Blastocystis hominis as a cause of
gastrointestinal pathology is controversial Several studies showed that the presence of
parasite in a majority of patients was not associated with symptoms, or is found with other organisms that are more likely to be cause of the symptoms

Other studies concluded that presence of Blastocystis in large numbers produce a wide variety of intestinal disorders: abdominal cramps, irritable bowel syndrome, bloating, flatulence, mild to moderate diarrhea without fecal leucocytes or blood, nausea, vomiting, low grade fever, and malaise
Symptoms usually last about 3-10 days, but may sometimes persist for weeks or months

It has been found out that in subjects suffering from Blastocystis showed a significant association with gastrointestinal symptoms
Other studies also provided evidence of cellular immune function changes in infected individuals

Diagnosis
Laboratory detection from stool is needed for confirmation
Stool samples should be collected more than once from patients showing signs and symptoms
Microscopic examination using direct fecal smear is useful but sensitivity is increased when concentration techniques are used

Hematoxylin or trichome staining offers a very convenient and easy method to differentiate the various stages of Blastocystis
Leukocytes are usually seen in fecal smears and stool eosinophilia may also be observed
The organism can be cultured using the Boeck and Drbohlav’s or the Nelson and Jones media

Treatment
Blastocystis is difficult to erradicate Hides in the intestinal mucus, sticks and
holds on the intestinal membranes Drug of choice is metronidazole given at
750 mg 3x daily for 10 days (Pedriatric dose: 35-50 mg per kg per day in 3 doses for 5 days) or iodoquinol given at 650 mg 3x daily for 20 days.

However, there are reported cases of resistance of Blastocystis to metronidazole
Trimethroprim-sulfamethaxazole (TMP-SMX) has been found to be highly effective against Blastocystis

Epidemiology
Reported practically worldwide, with infections common in tropical , subtropical and developing countries
In general, studies from developed countries report approx. 1.5% - 10% overall prevalence of Blastocystis hominis
All ages are affected but symptomatic cases are commonly found in children and in those with weakened immune systems

A prevalence of up to 11.6% was reported from Stanford University Hospital
Occurrence of parasite in temperate countries is generally associated with recent travel to the tropics and consumption of untreated drinking water, an indication that infection is possibly through the oral route and it is more likely to occur in crowded and unsanitary conditions

Outbreaks of Blastocystis hominis in day care centers were reported in Spain, Brazil and Canada
In the Philippines, results of 355 stools examined in 1997 by the Department of Parasitology, College of Public Health, University of the Philippines Manila, showed a prevalence of 22.8% with or without other intestinal parasites or organisms

In 1988, the prevalence was 20.7% in 772 stool samples examined.
Studies have shown prevalence rates of 40.6% among food service workers in a tertiary hospital and 23.6% among food handlers in selected school canteens in Manila

Several animals like the pig-tailed macaques, chicken, dogs, and ostriches harbor Blastocystis similar to those found in humans.
Evidence also shows that it is present in house lizards and cockroaches, thus implying that food and water contaminated by fecal droppings of these “home visitors” may transmit Blastocystis

Prevention and Control Disease can be prevented by consuming
safe drinking water Provisions for sanitary preparation may
be of value in efforts to prevent and control this infection
The cysts of Blastocystis hominis can survive up to 19 days in water at normal temperature and have shown resistance to chlorine at the standard concentrations