Bitten by Ophthalmology
26
Bitten by Bitten by Ophthalmology Ophthalmology Professor Helen Danesh-Meyer University of Auckland
description
Bitten by Ophthalmology. Professor Helen Danesh-Meyer University of Auckland. 5 Keys steps for assessment of optic nerve function. VA Colour Vision Relative afferent pupillary defect Visual Field Optic Nerve. 1. Visual Acuity. Best Corrected. Pinhole. Papillo -macular bundle. - PowerPoint PPT Presentation
Transcript of Bitten by Ophthalmology

Bitten byBitten byOphthalmology Ophthalmology
Bitten byBitten byOphthalmology Ophthalmology
Professor Helen Danesh-Meyer
University of Auckland

5 Keys steps for assessment 5 Keys steps for assessment of optic nerve functionof optic nerve function
5 Keys steps for assessment 5 Keys steps for assessment of optic nerve functionof optic nerve function
• VA
• Colour Vision
• Relative afferent
pupillary defect
• Visual Field
• Optic Nerve

1. Visual Acuity1. Visual Acuity1. Visual Acuity1. Visual Acuity
Best Corrected
Pinhole

Papillo-macular bundlePapillo-macular bundlePapillo-macular bundlePapillo-macular bundle

GlaucomaGlaucomaGlaucomaGlaucoma
• A collective term for group of potentially blinding ocular conditions
• Characterised by peripheral visual field loss and characteristic changes to the optic nerve head
• Can be:– primary (occur by themselves), or – secondary (other ocular condition causes it)

Primary Open Angle Primary Open Angle GlaucomaGlaucoma
Primary Open Angle Primary Open Angle GlaucomaGlaucoma
• Adult onset (> 40yrs)
• Angle normal and open
• Higher IOP greater risk
• Glaucomatous optic nerve head damage
• Visual Field loss
Normal
Glaucoma
cup disc
cup disc
c/d = 0.3
c/d = 0.8

Open Angle GlaucomaOpen Angle GlaucomaOpen Angle GlaucomaOpen Angle Glaucoma
• Asymptomatic
• Genetic
• Visual loss is irreversible
• Most common cause of preventable blindness
• Treatment is lifelong

2. Colour vision 2. Colour vision 2. Colour vision 2. Colour vision
• Optic nerve disease has decreased colour out of proportion to VA.
• Red desaturation classic for compressive optic neuropathies
• Tests:– Ishihara– Red target

3. Relative Afferent Pupillary 3. Relative Afferent Pupillary DefectDefect
3. Relative Afferent Pupillary 3. Relative Afferent Pupillary DefectDefect

3. Relative Afferent Pupillary 3. Relative Afferent Pupillary DefectDefect
3. Relative Afferent Pupillary 3. Relative Afferent Pupillary DefectDefect
• Objective sign of optic nerve compromise
• Can be used to monitor progression
• Provides a comparison of the two optic nerves

Relative Afferent Pupillary Defect Relative Afferent Pupillary Defect (RAPD)(RAPD)
Relative Afferent Pupillary Defect Relative Afferent Pupillary Defect (RAPD)(RAPD)
• Test in dim room with pt looking at the distance
• Use bright source of light about 30cm from pt’s eyes
• Swing light b/w the eyes (2-3 sec on each eye)
• Make your decision within 2-3 swings


ObserveObserveObserveObserve
Photopic illuminationScotopic illumination

Light responsesLight responsesLight responsesLight responses
Consensual responseDirect response

Light responsesLight responsesLight responsesLight responses
Direct responseConsensual response

Abnormal responseAbnormal responseAbnormal responseAbnormal response
Right Relative AfferentPupillary Defect


Circumstances when RAPD Circumstances when RAPD assessment difficultassessment difficult
Circumstances when RAPD Circumstances when RAPD assessment difficultassessment difficult
• Both pupils dilated
• Dark irides
• Elderly- small constricted pupils
• Damage to iris by surgery (cataract)
• Presybopic examiner

Surrogate Tests for RAPDSurrogate Tests for RAPDSurrogate Tests for RAPDSurrogate Tests for RAPD
• Brightness sense
• Red perception

Brightness senseBrightness senseBrightness senseBrightness sense
• Test in dim room with pt looking directly at the light
• Use bright source of light
• Ask:1. Is light equally bright in both eyes?2. If light is 100% bright in this eye (or worth
100 dollars) then how many percent (or how many dollars) is it in the other eye?

4. Visual Field Assessment4. Visual Field Assessment4. Visual Field Assessment4. Visual Field Assessment

Anatomy of visual pathwayAnatomy of visual pathwayAnatomy of visual pathwayAnatomy of visual pathway
Right eye Left eye
Temporal TemporalNasalNasal

Anatomy of visual pathwayAnatomy of visual pathwayAnatomy of visual pathwayAnatomy of visual pathway
Modified from Kahle W.Frotscher M: Color Atlas and Textbook of Human Anatomy. 5th ed. Stuttgart: Thieme. Vol.3 p.355, 2003
Optic nerve
Nasal retina
Optic chiasm
Optic tract
Optic radiation
Temporal retina Temporal retina
Lateral geniculate body
Striate cortex

Case 2Case 2Case 2Case 2
• 24 yr old male
• ~ 1 yr Hx of headaches, worse last 2-3/12• Examination: 6/6 OD 6/6 OS
No RAPD
Pallor + Pallor +
• CT head – pituitary adenoma

Visual Fields – 2/7 pre-op
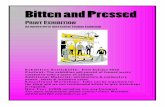
39 year old: 6/6 VA both eyes39 year old: 6/6 VA both eyes39 year old: 6/6 VA both eyes39 year old: 6/6 VA both eyes

Visual Acuity
Pupil Testing
Visual Fields
Colour vision
Fundus Examination