Why and How Migrate Informatica to ODI | Infa to ODI Migration | Infa to ODI Conversion

1
Biomechanical Evaluation of the ODI Hip Screw System
Research Report for Compression and Torsion Biomechanical Tests
February 23, 2000
Research Sponsor: Orthopedic Designs, Inc.
PO Box 7778
St. Petersburg, FL 33734
Phone: (888) 635-8535
Fax: (727) 344-3244
Research Institution: University of Florida
Department of Orthopaedics
Division of Research
1600 SW Archer Rd.
Box 100246
Gainesville, FL 32610
Investigators: Donna Wheeler, PhD
Alex Rose, BS
Bryan Conrad, BS
Andy Petrella, MD
Phone: (352) 392-4251
Fax: (352) 392-8637
e-mail: [email protected]

2
BIOMECHANICAL EVALUATION OF A NEW TYPE OF HIP COMPRESSION
SCREW WITH RETRACTABLE TANGS
Bramlet, Dale G. MD, Petrella, Andrew MD and Wheeler, Donna PhD
The advantages of treatment by open reduction and internal fixation for
intertrochanteric, subtrochanteric, and some femoral neck fractures of the proximal femur
has been well known to orthopedic surgeons for several decades25, 39, 49-51, 70, 84, 86, 87, 89, 100,
101. Rigid internal fixation with interfragmentary compression permits early mobilization
and reduces patient morbidity and mortality53, 66, 79, 99. Initial results with the Jewett
triflanged nails102 were dampened when long term reports revealed as high as a 26%
failure rate commonly associated with varus displacement and joint penetration with these
devices14, 57, 93. The introduction of a sliding hip compression screw lowered these
complications by allowing the fracture site to collapse upon itself as patients ambulated
rather that having the lag screw erode through the bone and penetrate into the hip joint1, 27,
31, 36, 37, 42-45, 69. Technical failure, defined as loss of fixation, loosening of the lag screw
and/or cut out of the screw with hip joint penetration has still been reported in from 4 -
19% of cases7, 26, 71, 95, 103.
Unstable fractures with a large posterior spike of bone and/or medial comminution are
particularly challenging and both medial displacement34, 41 and valgus osteotomies9, 17, 28,
88 have been proposed for restoring stability to this fracture pattern. Other authors have
advocated the use of methylmethacrylate as an adjunct to internal fixation with
intertrochanteric fractures in osteoporotic patients4, 12, 15, 16, 35, 80. Anatomic reduction and
rigid internal fixation with a compression screw – plate system is the preferred technique
by the majority of current authors13, 23, 29, 40, 93. Restoring a stable fracture pattern is
fundamental to obtaining a high union rate of these challenging fractures48, 67, 82 and
reoperation following nonunion of intertrochanteric fractures that fail to unite with
primary treatment is uniformly advocated62. In many series, from 30 to 65% of all
intertrochanteric fractures are classified as unstable52. With weak osteoporotic bone and
in unstable, comminuted 3 and 4 part intertrochanteric fractures of the proximal femur,
varus angulation of the fracture fragments and joint penetration rates of from 8 - 34%
have been reported58, 68. A high grade of osteoporosis or the presence of osteomyelitis
have been shown to be the important predisposing factors in the spontaneous
development of a subcapital femoral neck fracture after a healed intertrochanteric hip
fracture47, 54, 60, 63, 77.
While some authors have advocated the use of intramedullary nails5, 10, 18, 19, 46, 78, 96 instead of
hip compression screws for intertrochanteric fractures, the compression hip screw remains the
most popular method for treatment of these sometimes challenging fractures21, 24, 65, 74, 83, 106.
Intramedullary hip - screws have been shown to have significantly less sliding of the lag-screw,
effectively converting these into fixed angle devices with the attendant risks of cut-out, distal
cortical hypertrophy or fracture, and limb shortening, especially in unstable fractures33.
Furthermore, intramedullary devices are technically more demanding with higher intra-
operative and post-operative complications and inferior return of mobility38, 73, 90-92.
Several commercially available hip compression screw systems are “keyed” whereby
they have a design fit between the lag screw and side plate that minimizes torque or

3
rotation forces from occurring at the fracture site by limiting rotation between the lag
screw and the barrel of the side plate. These systems still allow sliding to occur between
the lag screw and side plate, enabling fracture fragments to settle into a stable pattern as
the patient walks. A compression screw at the time of internal fixation can be utilized to
apply compression forces across the fracture site. This minimizes the potential for
excessive lag screw slide and subsequent impingement of the threads of the lag screw
against the barrel, effectively converting a sliding screw into a fixed angle device8, 105.
Sliding occurs mainly during the first 2 weeks post-operatively and excessive sliding has
been associated with a delay in union of the fracture72 and lag screw cut-out105. In cases
of severe osteoporosis, excessive tightening of the compression screw can lead to a
stripping out of the thread “purchase” within the bone of the femoral head and a
subsequent loss of fixation. Increasing the strength of attachment of the lag screw within
the femoral head (or the “purchase” of the lag screw) can enable greater compressive
forces to be applied across the fracture site. With appropriate lag screw length choice,
initial compression at the fracture site should result in less settling of the lag screw, and
thus less chance of lag screw thread - barrel engagement61, 85.
We tested a new type of hip compression screw1 incorporating a reversibly deployable
series of four tangs (Figures 1 and 2) that protrude from the base of the threads of the lag
screw. The tangs are designed to engage into the cortical bone at the base of the femoral
head - neck junction in the inferior portion of the femoral head. We hypothesized that the
engagement of the tangs into the dense cortical bone serves three purposes. First, they
increase the “purchase strength” of the lag screw within the femoral head, enabling the
surgeon to tighten the compression screw with greater force without the lag screw
stripping out. Second, the tangs resist torque forces between the femoral head and the lag
screw by counteracting rotational forces occurring at this interface. Third, by increasing
the amount of bone engaged by the screw, particularly the dense cortical bone at the base
of the femoral neck, it theoretically should resist joint penetration by increasing the
column of bone necessary for a lag screw to penetrate through prior to perforating
through the femoral head and entering into the hip joint space. This paper reports the
results of testing the first two of our three hypotheses.
Because the final location of the lag screw relative to the femoral head geometry has been
shown to be significant in terms of failure2, 3, 20, 22, 32, 97, we chose to test the central versus
the inferior head position of the lag screw and its relationship to purchase within the
femoral head. Furthermore, we hypothesized that resistance to torque forces is a critical
factor leading to the failure of hip pins in osteoporotic bone. As the patient ambulates in
the early post-operative period, the repetitive torque and loading forces are paramount in
leading to a wedge effect of the lag screw in the minimally dense femoral head.
Therefore, we chose to test the torque or rotational strength of the talon hip pin.
Compression at the fracture site is critical to preventing subsequent excessive slide of the
lag screw as the patient ambulates in the post-operative period11. We therefore chose to
test compressive forces across the fracture site utilizing the Talon hip pin.
1 Talon Dynamic Compression Hip Pinning System (ODi: Orthopedic Designs Inc., P. O Box 7778 St. Petersburg, FL
33734)

4
Materials and Methods
A total of 25 matched pairs of embalmed adult cadaveric femurs were obtained
and the soft tissue removed. Radiographs were taken of each femur to assure symmetry
between right and left limbs, rule out bone pathology and assess femoral anatomy. Dual
energy x-ray absorptiometry (DEXA) (Lunar Corporation, Madison, WI) was used to
quantify the bone mineral density (BMD) of each femoral pair at the region of Ward’s
triangle. Femoral pairs were excluded from the study if there was: (1) assymetry between
right and left femurs; (2) a pathological condition; or (3) bone mineral density difference
greater than 15% between right and left femurs.
In order to maintain alignment and assist reduction, the femoral heads were
drilled and tapped for implantation of hip pins prior to creation of intertrochanteric
fractures. A pneumatic saw was used to score the femur in a circumferential manner
extending from the proximal superior aspect of the greater trochanter to the inferior
aspect of the femoral neck, just superior to the lesser trochanter. The fracture was then
completed with an osteotome.
In all studies, for one side of each pair of femurs, an ODI compression hip screw
system with a 4-hole side plate was surgically implanted using the procedure
recommended by the manufacturer. The tangs (Figure 2) of the ODI lag screw were
deployed in one femur from each pair (tang) while the tangs remained retracted in the
contralateral femur (screw). The femurs receiving the tang treatment were alternatively
placed in the higher BMD bone of a pair and then the lower BMD bone of the next pair.
All femurs were fixed with a standard barrel (38 mm)/standard barrel angle (135°) plate.
The lag screw length was determined by the femoral neck length and set as specified by
the manufacturer. Radiographs were taken after implantation to document tang
deployment and lag screw position. All surgical implantations were conducted by two
orthopaedic surgeons.
Torsional Stability Eight pairs of embalmed, adult cadaveric femora were used for this phase of the
investigation. All femoral pairs underwent cyclic torsional loading followed by a
torsional load to failure. Femoral heads were potted in dental stone (Snap Stone, Whip
Mix, Louisville, KY) in such a way that the fracture would be perpendicular to the axis of
rotation. Each femur was mounted on a custom made jig that held the shaft at
approximately 45° (Figure 3). A torsional load was applied to the femur using an Instron
materials testing system (Instron Corp, Canton, MA). The cyclic torsional load applied
to the femur was ramped between 1 and 11 N-m in a clockwise direction (tightening
action). Torsional loading was applied to the femurs at 1 Hz for 5000 cycles. Angular
displacement and torque were collected during cycling to determine rotational stability of
the construct. All femurs underwent cyclic testing prior to torque to failure.
After cycling, the compression screw was removed from the lag screw and the
femoral head fragment removed from the lag screw barrel of the side plate and the
femoral shaft. The lag screw was securely mounted to the materials testing equipment
using a 4-jaw Jacobs chuck. The femoral head, mounted in dental stone and reinforced
with k-wires, was mounted to the actuator of the materials testing equipment. The
construct was loaded to failure in torque at a loading rate of 1 degree/sec to a maximum
rotation of 90 degrees in a clockwise direction.

5
Statistical analyses involved an analysis of variance (ANOVA) with a complete
block design (paired samples) evaluating the effects of bone mineral density and
treatment (tang or screw). All statistical tests were run using SAS statistical software at a
significance level of α = 0.05.
Interfragment Compression
Seventeen pairs of embalmed, adult cadaveric femora were assigned for this phase
of the investigation. Intertrochanteric osteotomies were performed, instead of
ostectomies, to provide space between fracture fragments for the compression transducer.
Care was taken to assure parallel fragment surfaces for uniform load distribution to the
interposed ring load transducer. The load transducer placed between intertranchanteric
fragments is shown in Figure 4.
Four pairs of specimens were tested with the lag screw in the central aspect of the
femoral neck (center). The lag screw was placed in the inferior position (IP) for the
remaining femoral pair to provide better cortical purchase. Both center and IP positions
were tested to determine if lag screw position affected compressive characteristics.
A 4400 N (1000 lb) capacity ring load cell (Transducer Techniques, Inc,
Temacula, CA) was used to monitor the compression of intertrochanteric fragments. The
calibrated load cell was placed between the fracture fragments prior to insertion of the
device lag screw. For each quarter turn of the compression screw, the interfragment
compression and torque applied to the compression screw were recorded in a systematic
fashion. Compression force and torque were recorded for a total of 15 complete turns of
the compression screw. Failure was defined as a drop in compression of more than 50%
within one turn of the compression screw. Data was acquired 5 screw turns beyond peak
compression. Radiographs were acquired following testing to document the device
position at failure.
Statistical analyses involved an analysis of variance (ANOVA) with a complete
block design (paired samples) evaluating the effects of bone mineral density, lag screw
position (center or IP) and treatment (tang or screw). If a significant effect of position
was found, the effects of treatment by position were determined. Similarly, if a
significant effect of treatment was found, the effects of position by treatment were
determined. All statistical tests were run using SAS statistical software at a significance
level of α = 0.05.

6
Results
Torsional Stability
Table 1 summarizes the results of the cyclic torsional and torque to failure tests.
The relative rotational displacement during cyclic testing from preload to maximum load
was defined as amplitude. The absolute rotational displacement from beginning to end of
cycling (5000 cycles) was defined as migration. The amplitude during cyclic loading for
the tang and screw groups was not significantly different. However, the femurs fixed
with the tang treatment had significantly less rotational migration during 5000 torsional
cycles than the screw group (p = 0.023), with angular values of 1.59 ± 3.15 degrees and
2.11 ± 2.97 degrees, respectively. The peak torque for the tang device was significantly
greater than the torque for the screw device (p = 0.00016) with torque values of 6.48 ±
1.73 N-m and 1.92 ± 1.71 N-m, respectively. The average rotational displacement
occurring prior to peak torque was 27.13 ± 18.20 degrees for the tang group and 30.13 ±
19.38 degrees for the screw group. The rotational displacement at peak was not different
between the tang and screw groups. The torque at 15 degrees of rotation, a more
clinically relevant value, was also significantly greater for the tang compared to the
screw device (p=0.0028) with torque values of 4.185 ± 2.002 N-m and 1.21 ± 1.15 N-m,
respectively. Peak torque and torque at 15 degrees of rotation are presented graphically
in Figure 5.
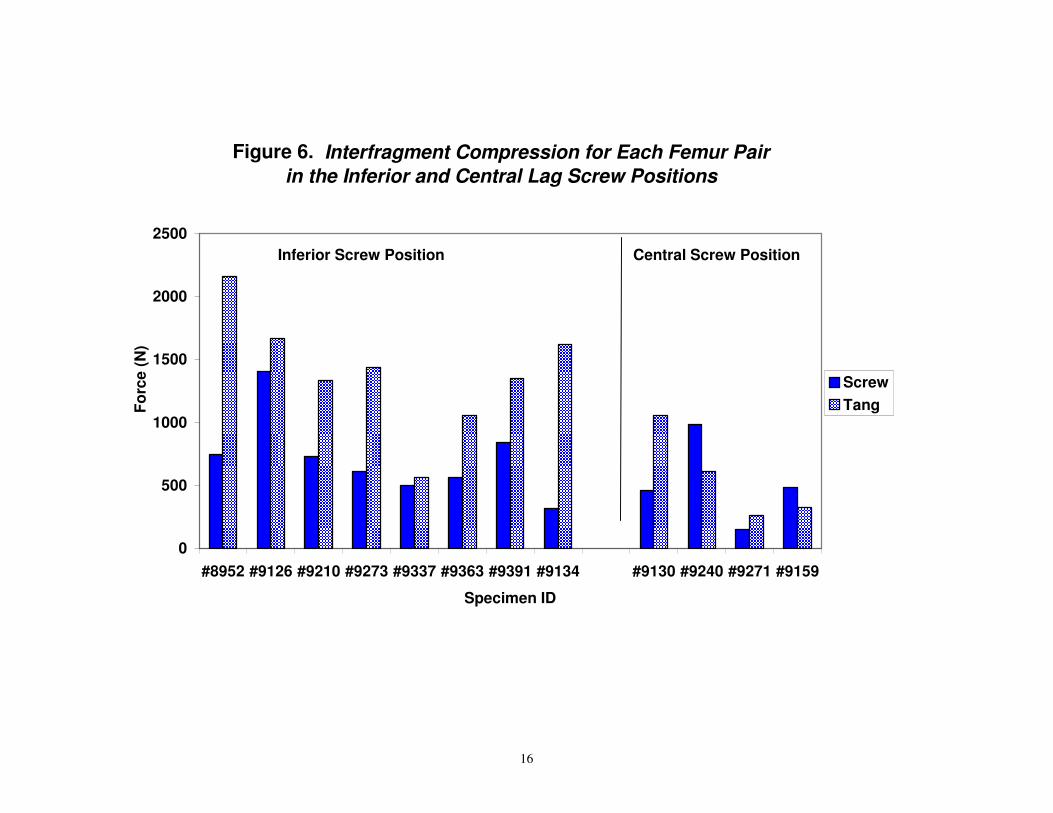
Interfragment Compression Of the 17 paired specimens assigned to compression testing, 5 pairs of specimens
were deleted from the analysis. The specimens were eliminated due to testing errors
(n=2), implantation errors (n=1), and BMD differences between contralateral femurs
greater than 15% (n=2). The remaining 12 femur pairs were evaluated for interfragment
compression as a function of compression screw rotation. Table 2 and Figures 6 – 9
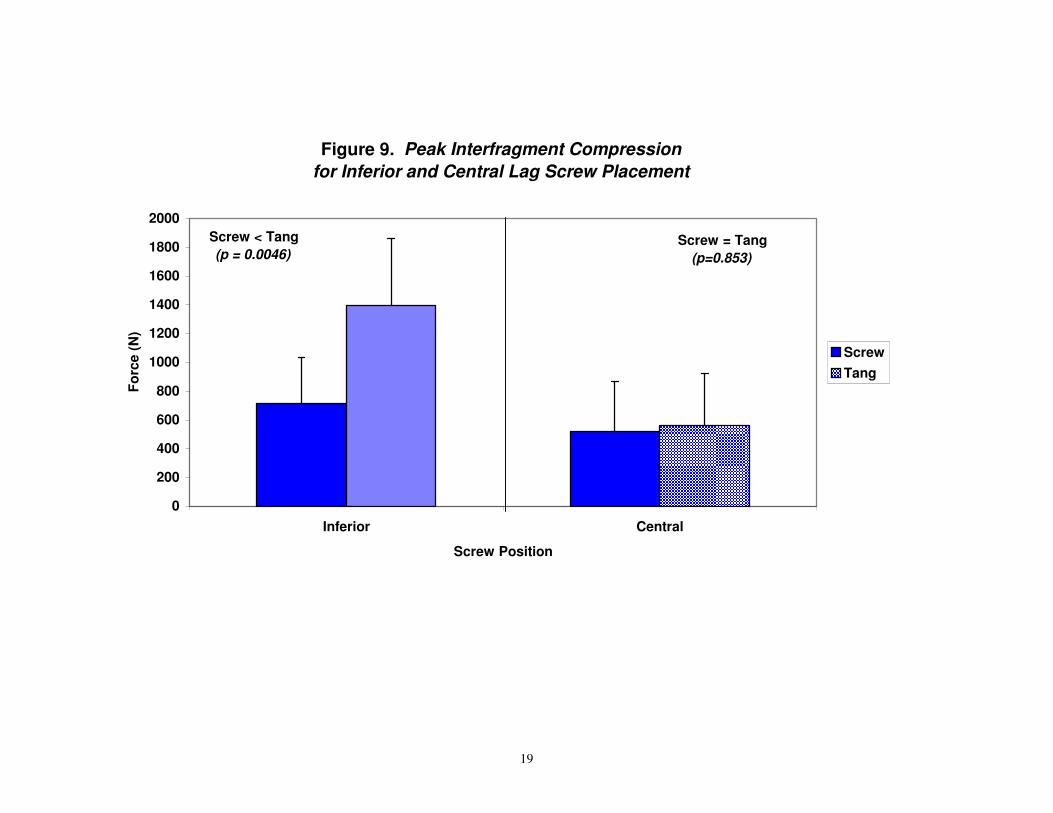
summarize the results from the compression test. The peak compressive forces generated
by the tang treatment group were significantly greater than the screw group in the inferior
position (p = 0.0046) with compression values of 1398.41 ± 466.84 N and 712.83 ±
322.77 N, respectively (Figures 7 & 9). No differences between tang and screw
treatments were noted when the device was implanted in the central position (Figures 8 &
9). The compression was significantly greater for the tang group when the lag screw was
placed in the inferior position compared to the central position (p=0.011) but no
difference in the screw group was noted (Figure 10). The tang group produced
significantly greater compression than the screw group in the inferior position (p=0.036)
but no difference in the central position (Figure 7). The BMD did not have a significant
effect on interfragment compression for the screw or tang group (p > 0.05).

7
Discussion
Numerous papers have addressed the ideal positioning of the lag screw within the
femoral head to maximize purchase of the screw and to minimize the risk of cut out59,
95, 104. Our data clearly demonstrates that an inferior placement of the lag screw within
the lower portions of the femoral head results in greater purchase of the lag screw
regardless of whether the tangs are deployed . However, with tang deployment, a 96%
greater peak compression strength is obtained prior to failure when compressive forces
are applied across the fracture site. These results were statistically significant [Figures
7 & 9; (p=0.0046)]
Our results show that one of the critical factors maximizing the purchase of the lag screw
within the femoral head is to engage the tangs within the dense cortical bone at the
junction between the femoral head and the neck. If a central location is chosen and the
bone is weak and osteoporotic, deployment of the tangs provides no further increase in
purchase resistance to compressive forces within the femoral head (Figure 8). If the
tangs are engaged within the dense cortical bone provided by an inferior lag screw axis,
then a statistically significant (p=0.036) increase in compressive force across the fracture
site can be produced (Figure 10) prior to lag screw failure.
Regardless of tang deployment, an inferior position is supported by this study. With both
the torque testing and the compression testing, at the extremes of testing, representing
non-physiologic loads, radiographs revealed gross tang deformity. In all instances, when
the actuator retrieval mechanism was utilized, the tangs fully retracted and no tangs broke
or failed to retract.
We believe that the mechanism of failure accounting for lag screw cut out and subsequent
pin penetration so commonly reported is multifactorial. Gill J. et al reported that high
streeses in the surrounding cancellous bone contribute to the failure of repairs30. Failure
to compress the fracture site fully has been noted clinically to be accompanied by
excessive slide of the lag screw, which has been shown to be associated with a poor
functional outcome6. The advantage of enhanced compression across the fracture site has
been advocated by numerous authors55, 56, 64, 75, 76, 98. Indeed, excessive slide, presumably
associated with poor initial compression has been shown to prolong time to union of
operatively treated intertrochanteric fractures72. Prior to the introduction of the talon hip
pinning system, few hip pinning systems were designed to prevent rotation forces
between the lag screw and the proximal femoral bone. While hip bolt procedures have
been advocated by some authors to increase the purchase of the device within the femoral
head, most authors have favored use of the hip compression screw81. Our results clearly
demonstrate an approximately three times greater peak rotational purchase of the Talon
lag screw within the femoral head compared to those lag screws wherein the tangs were
not deployed (Figure 5). There are no comparative studies to date testing different
commercially available hip pinning systems with the Talon hip pin. Thread length and
screw designs vary between manufacturers.

8
Most current hip pinning systems fail to adequately address rotational or torque forces
that occur between the femoral head and the lag screw as the patient ambulates and
arises from or resumes the sitting position. We postulate that with weakened
osteoporotic bone, the lag screw acts like a wedge, slowly working its way upward as
the patient ambulates and subjects their recently fractured hip to rotational forces. This
is particularly a problem in the non-compliant and slightly demented patients who
nevertheless remain ambulatory. Many authors have noted the extreme resorption of
bone in the femoral head and metaphyseal regions of the proximal femur and torsional
forces have been implicated in implant failure94. Enlarged threads patterns or expansile
devices such as molley-bolt designed hip lag screws fail to reach to the dense remaining
cortical bone that we believe holds the greatest promise for maximizing purchase of the
lag screw within the femoral head.
Our prior experience has shown great difficulty in experimental models for reproducing
“cut-out” of the femoral head. Investigators have difficulty obtaining only osteoporotic
femurs for testing, and many matched specimens vary in bone density even in the same
person. We alternated between most and least dense femurs for deployment of our tang –
deployed and control lag screws, but a better test design would be to have matched
controls that were tested in only osteoporotic femurs. Furthermore, our fracture design
was a stable model whereby a simple 2 part intertrochanteric fracture was created. This
insured a stable reconstruction of the fracture pattern simulating a reproducible construct
expected after open reduction internal fixation. Clinical experience dictates that unstable
and multipart fractures are those most at risk for cut-out, in addition to the extremely
osteoporotic. Furthermore, in vivo experience would suggest greater extremes of fracture
site bone interdigitation depending upon the extremes of fracture comminution and the
success of the fracture site reduction.
Our results clearly demonstrate that with a stable 2 part intertrochanteric fracture of the
proximal femur treated with a Talon lag screw with tangs fully deployed, the resistance to
torque forces (Table 1, p=0.0028) in our experimental model were greater with tangs
deployed that with comparable lag screws wherein the tangs were not deployed. Many
manufacturers and numerous studies have attempted to prevent or reduce the incidence of
cut out of the lag screw by enlarging the threads of the lag screw or by expanding a
molley-bolt type device within the head of the femoral head. An association with over-
reaming and weak osteoporotic bone have been shown to be significant risk factorsa.
We believe that the unique combination of deployable tangs within the femoral head has
been shown to be superior to resisting rotational forces than a comparable lag screw
without tangs deployed. Furthermore, the tangs deploy a full 1 inch at maximum
deployment. Most standard lag screws have an external thread diameter of
approximately ½ in. The column of bone that a lag screw must erode through to penetrate
through the superior cortex of the femoral head is thus doubled with the talon hip pin
with tangs deployed.

9
The peak compressive forces generated by the tang treatment group were significantly
greater than the screw group in the inferior position (p = 0.0046) with compression values
of 1398.41 ± 466.84 N and 712.83 ± 322.77 N, respectively (Figures 7 & 9). No
differences between tang and screw treatments were noted when the device was
implanted in the central position (Figures 8 & 9). The compression was significantly
greater for the tang group when the lag screw was placed in the inferior position
compared to the central position (p=0.011) but no difference in the screw group was
noted (Figure 10). The tang group produced significantly greater compression than the
screw group in the inferior position (p=0.036) but no difference in the central position
(Figure 7). The BMD did not have a significant effect on interfragment compression for
the screw or tang group (p > 0.05).
In summary, the talon hip pinning system in our matched cadaveric model provided a
two fold increase of purchase of the lag screw when tangs were deployed within the
femoral head when compressed to failure at the fracture site. Optimal location of any lag
screw with an axis inferior to the center of the femoral head as advocated by Wu, C. et
al104 in supported by our results in this study. This leads to greater purchase of the lag
screw within the femoral head in an area that presumably has more dense bone and thus
theoretically should resist cut-out. Deployment of the tangs into or through the cortical
endosteal surface increases the purchase strength of the lag screw in this inferior position.
Furthermore, tang deployment appears to be the critical factor in resisting rotational
torque forces about the femoral head in our test model. After cyclical testing of the
fracture construct, peak torque for the tang device was significantly greater than the
torque for the screw device (p = 0.00016) with torque values of 6.48 ± 1.73 N-m and
1.92 ± 1.71 N-m, respectively. Our results support our hypotheses that the Talon hip pin
system with tangs deployed provides significantly increased purchase of the lag screw
within the proximal femoral head and will allow greater compression forces to be applied
across the fracture site. The increased purchase afforded by the tangs within the femoral
head counteracts rotational forces and provides a greater column of bone that must be
eroded through prior to lag screw penetration in our model. While our results did not
address the degree of tang penetration into the dense cortical bone, we believe from our
experience with this device that engagement or penetration into or through the cortical
bone at the base of the femoral head-neck junction is the critical technical step to
maximize the tang purchase within the femoral head.

10
BMD
(g/cm3)
Amplitude (degrees)
Migration (degrees)
Peak Torque (N-m)
Torque at 15 degrees
(N-m)
Screw 0.516 ± 0.234 0.953 ± 0.409 2.11 ± 2.97 1.92 ± 1.71 1.21 ± 1.15
Tang 0.547 ± 0.243 1.07 ± 0.581 1.59 ± 3.15 6.476 ± 1.73 4.185 ± 2.002
Screw vs Tang
(p-value) p = 0.292 p = 0.723
Tang < Screw p = 0.023
Tang > Screw p = 0.00016
Tang > Screw p = 0.0028
Table 1. Results of Torsional Biomechanical Tests
Implantation Location
Measurement Screw Tang Screw vs Tang
(p-value)
Inferior
Peak Compression (N) (n = 8)
712.83 ± 322.77 1398.41 ± 466.84 *p = 0.0046
Peak + 1 turn (N) (n = 6)
380.88 ± 196.64 1033.47 ± 451.37 *p = 0.021
Peak + 3 turn (N) (n = 6)
343.90 ± 192.90 712.46 ± 384.01 *p = 0.024
Peak + 5 turn (N) (n = 6)
258.55 ± 132.22 472.99 ± 215.43 p = 0.078
Central
Peak Compression (N) (n = 4)
520.44 ± 346.22 562.70 ± 362.26 p = 0.853
Peak + 1 turn (N) (n = 4)
270.67 ± 204.61 286.91 ± 166.14 p = 0.905
Peak + 3 turn (N) (n = 4)
145.01 ± 108.25 205.73 ± 60.81 p = 0.396
Peak + 5 turn (N) (n = 4)
71.73 ± 55.42 180.15 ± 30.55 *p = 0.024
Table 2. Results of Interfragmentary Compression Tests
11
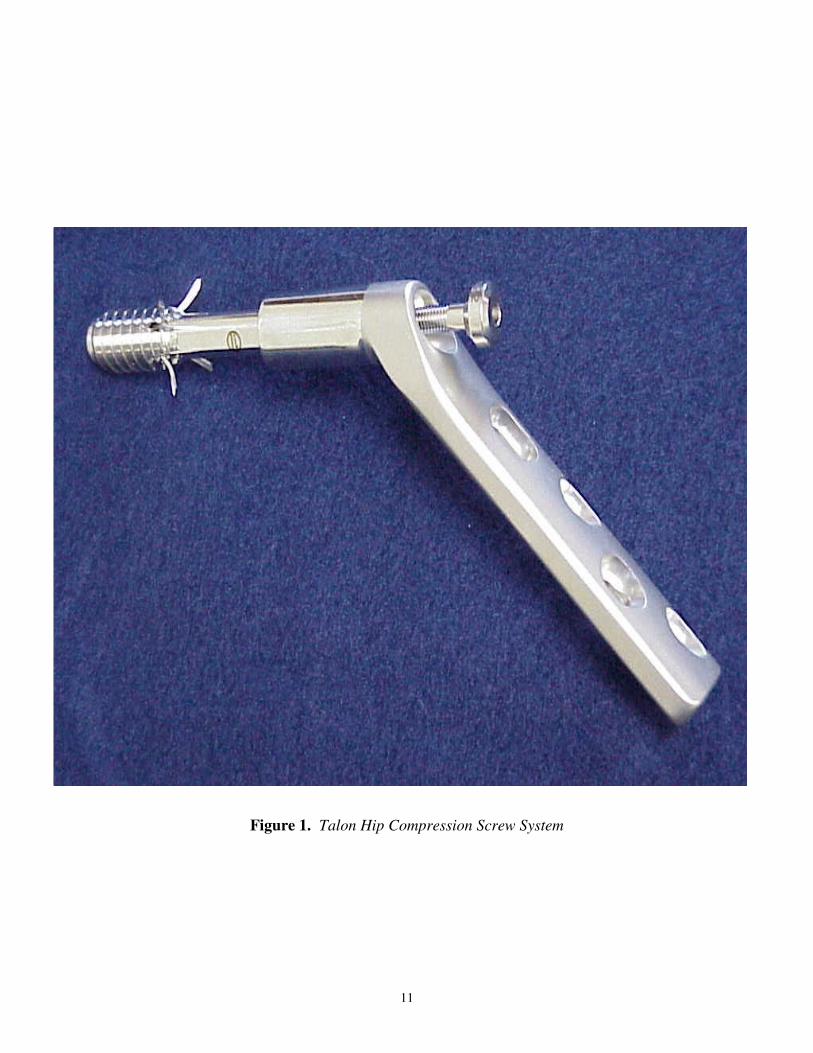
Figure 1. Talon Hip Compression Screw System

12
Figure 2. Talons fully deployed

13
Figure 3. Specimen in Test Fixture for Cyclic Torsional Loading

14
Figure 4. Specimen with Load Transducer Interposed between
Intertrochanteric Fragments to Measure Compression

15
Figure 5. Peak Torque and Torque at 15 Degress
0
1
2
3
4
5
6
7
8
9
Peak 15 degrees
To
rqu
e (
N-m
)
Screw
Tang
Tang > Screw
(p = 0.00016)
Tang > Screw
(p = 0.0028)
16
Figure 6. Interfragment Compression for Each Femur Pair
in the Inferior and Central Lag Screw Positions
0
500
1000
1500
2000
2500
#8952 #9126 #9210 #9273 #9337 #9363 #9391 #9134 #9130 #9240 #9271 #9159
Specimen ID
Fo
rce
(N
)
Screw
Tang
Inferior Screw Position Central Screw Position

17
Figure 7. Peak & Post-Peak Compressive Forces
Inferior Postion
0
500
1000
1500
2000
2500
Peak Peak + 1 turn Peak + 3 turn Peak + 5 turn
Fo
rce
(N
)
Screw
Tang
Screw < Tang
(p = 0.0046)
Screw < Tang
(p = 0.021)
Screw < Tang
(p = 0.024)
Screw = Tang
(p = 0.078)

18
Figure 8. Peak and Post-Peak Compressive Forces
Central Postiion
0
200
400
600
800
1000
1200
Peak Peak + 1 turn Peak + 3 turn Peak + 5 turn
Fo
rce (
N)
Screw
Tang
Screw = Tang
(p = 0.853)
Screw = Tang
(p = 0.905)Screw = Tang
(p = 0.396)
Screw < Tang
(p = 0.024)
19
Figure 9. Peak Interfragment Compression
for Inferior and Central Lag Screw Placement
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Inferior Central
Screw Position
Fo
rce
(N
)
Screw
Tang
Screw = Tang
(p=0.853)
Screw < Tang
(p = 0.0046)

20
Figure 10. Inferior versus Central Placement of Lag Screw
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Screw Tang
Treatment
Fo
rce
(N
)
Inferior
Central
Inferior > Central
(p = 0.0110)
Inferior = Central
(p = 0.3635)

21
Bibliography
1. Alho, A.; Molster, A.; Raugstad, T.; Medby, P.; and Stray, O.: Sliding of the
compression hip screw in femoral neck fractures. J Orthop Trauma , 1(4): 293-7, 1987.
2. Arrington, E.: Subcapital femoral neck fracture after closed reduction and internal
fixation of an intertrochanteric hip fracture: a case report and review of the literature. [In
Process Citation]. Am J Orthop , 28(9): 517-521, 1999.
3. Baker, D.: Fractures of the femoral neck after healed intertrochanteric fractures: a
complication of too short a nail plate fixation. Report of three cases. J Trauma , 15(1):
73-81, 1975.
4. Bartucci, E.; Gonzalez, M.; Cooperman, D.; Freedberg, H.; Barmada, R.; and
Laros, G.: The effect of adjunctive methylmethacrylate on failures of fixation and
function in patients with intertrochanteric fractures and osteoporosis. J Bone Joint Surg
[Am] , 67(7): 1094-107, 1985.
5. Baumgaertner, M.; Curtin, S.; and Lindskog, D.: Intramedullary versus
extramedullary fixation for the treatment of intertrochanteric hip fractures. Clin Orthop
,(348): 87-94, 1998.
6. Bendo, J.; Weiner, L.; Strauss, E.; and Yang, E.: Collapse of intertrochanteric hip
fractures fixed with sliding screws. Orthop Rev , Suppl: 30-7, 1994.
7. Benterud, J.; Husby, T.; Nordsletten, L.; and Alho, A.: Fixation of displaced
femoral neck fractures with a sliding screw plate and a cancellous screw or two Olmed
screws. A prospective, randomized study of 225 elderly patients with a 3-year follow-up.
Ann Chir Gynaecol , 86(4): 338-42, 1997.
8. Bonamo, J.; and Accettola, A.: Treatment of intertrochanteric fractures with a sliding
nail-plate. J Trauma , 22(3): 205-15, 1982.
9. Bong, S.; Lau, H.; Leong, J.; Fang, D.; and Lau, M.: The treatment of unstable
intertrochanteric fractures of the hip: a prospective trial of 150 cases. Injury , 13(2): 139-
46, 1981.
10. Bridle, S.; Patel, A.; Bircher, M.; and Calvert, P.: Fixation of intertrochanteric
fractures of the femur. A randomised prospective comparison of the gamma nail and the
dynamic hip screw. J Bone Joint Surg [Br] , 73(2): 330-4, 1991.
11. Cameron, H.; and Graham, J.: Retention of the compression screw in sliding screw
plate devices. Clin Orthop ,(146): 219-21, 1980.
12. Caudle, R.; Hopson, C.; and Clarke, R.: Unstable intertrochanteric fractures of the
hip. Orthop Rev , 16(8): 538-49, 1987.
13. Chang, W.; Zuckerman, J.; Kummer, F.; and Frankel, V.: Biomechanical
evaluation of anatomic reduction versus medial displacement osteotomy in unstable
intertrochanteric fractures. Clin Orthop ,(225): 141-6, 1987.
14. Chinoy, M.; and Parker, M.: Fixed nail plates versus sliding hip systems for the
treatment of trochanteric femoral fractures: a meta analysis of 14 studies. Injury , 30(3):
157-63, 1999.

22
15. Choueka, J.; Koval, K.; Kummer, F.; and Zukerman, J.: Cement augmentation of
intertrochanteric fracture fixation: a cadaver comparison of 2 techniques. Acta Orthop
Scand , 67(2): 153-7, 1996.
16. Chow, S.; Tang, S.; Pun, W., et al.: Treatment of unstable trochanteric fractures
with Dimon-Hughston osteotomy displacement fixation and acrylic cement. Injury ,
18(2): 123-7, 1987.
17. Clark, D.; and Ribbans, W.: Treatment of unstable intertrochanteric fractures of the
femur: a prospective trial comparing anatomical reduction and valgus osteotomy. Injury ,
21(2): 84-8, 1990.
18. Curtis, M.; Jinnah, R.; Wilson, V.; and Cunningham, B.: Proximal femoral
fractures: a biomechanical study to compare intramedullary and extramedullary fixation.
Injury , 25(2): 99-104, 1994.
19. Davis, T.; Sher, J.; Checketts, R.; and Porter, B.: Intertrochanteric fractures of the
femur: a prospective study comparing the use of the Kuntscher-Y nail and a sliding hip
screw. Injury , 19(6): 421-6, 1988.
20. Davis, T.; Sher, J.; Horsman, A.; Simpson, M.; Porter, B.; and Checketts, R.:
Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone
Joint Surg [Br] , 72(1): 26-31, 1990.
21. De, P. L.; Specchia, N.; Rizzi, L.; Gigante, A.; and Greco, F.: Critical analysis of
intramedullary nailing by the Ender method in the treatment of intertrochanteric fractures.
Ital J Orthop Traumatol , 19(1): 25-31, 1993.
22. Den, H. B.; Bartal, E.; and Cooke, F.: Treatment of the unstable intertrochanteric
fracture. Effect of the placement of the screw, its angle of insertion, and osteotomy [see
comments]. J Bone Joint Surg [Am] , 73(5): 726-33, 1991.
23. Desjardins, A.; Roy, A.; Paiement, G., et al.: Unstable intertrochanteric fracture of
the femur. A prospective randomised study comparing anatomical reduction and medial
displacement osteotomy. J Bone Joint Surg Br , 75(3): 445-7, 1993.
24. Doppelt, S.: The sliding compression screw--today's best answer for stabilization of
intertrochanteric hip fractures. Orthop Clin North Am , 11(3): 507-23, 1980.
25. Dresing, K.; and Sturmer, K. M.: [Comparison of the quality of life before and after
surgical management of pertrochanteric femoral fractures in elderly patients]. , 113: 983-
6, 1996.
26. Ecker, M.; Joyce, J.; and Kohl, E.: The treatment of trochanteric hip fractures using
a compression screw. J Bone Joint Surg [Am] , 57(1): 23-7, 1975.
27. Flores, L.; Harrington, I.; and Heller, M.: The stability of intertrochanteric
fractures treated with a sliding screw-plate. J Bone Joint Surg [Br] , 72(1): 37-40, 1990.
28. Fontanesi, G.; Costa, P.; Giancecchi, F.; and Tartaglia, I.: Intertrochanteric valgus
osteotomy and sliding compression hip screw in fractures of the femoral neck. Ital J
Orthop Traumatol , 17(3): 293-304, 1991.
29. Gargan, M.; Gundle, R.; and Simpson, A.: How effective are osteotomies for
unstable intertrochanteric fractures? J Bone Joint Surg Br , 76(5): 789-92, 1994.
30. Gill, J.; Johnson, G.; Sher, J.; and Kornjaca, N.: Biomechanical aspects of the
repair of intertrochanteric fractures. J Biomed Eng , 11(3): 235-9, 1989.
31. Greider, J. J.; and Horowitz, M.: Clinical evaluation of the sliding compression
screw in 121 hip fractures. South Med J , 73(10): 1343-8, 1980.

23
32. Gundle, R.; Gargan, M.; and Simpson, A.: How to minimize failures of fixation of
unstable intertrochanteric fractures. Injury , 26(9): 611-4, 1995.
33. Hardy, D.; Descamps, P.; Krallis, P., et al.: Use of an intramedullary hip-screw
compared with a compression hip-screw with a plate for intertrochanteric femoral
fractures. A prospective, randomized study of one hundred patients. J Bone Joint Surg
Am , 80(5): 618-30, 1998.
34. Harper, M.: The treatment of unstable intertrochanteric fractures using a sliding
screw-medial displacement technique. J Trauma , 22(9): 792-6, 1982.
35. Harrington, K.: The use of methylmethacrylate as an adjunct in the internal fixation
of unstable comminuted intertrochanteric fractures in osteoporotic patients. J Bone Joint
Surg [Am] , 57(6): 744-50, 1975.
36. Hegge, H.; Hatten, S.; Patka, P.; Van, M. J.; and Breederveld, R.: Results of
dynamic hip-screw osteosynthesis for intracapsular fractures of the femoral neck. Neth J
Surg , 41(2): 27-30, 1989.
37. Heyse-Moore, G.; MacEachern, A.; and Evans, D.: Treatment of intertrochanteric
fractures of the femur. A comparison of the Richards screw-plate with the Jewett nail-
plate. J Bone Joint Surg [Br] , 65(3): 262-7, 1983.
38. Hoffman, C.; and Lynskey, T.: Intertrochanteric fractures of the femur: a
randomized prospective comparison of the Gamma nail and the Ambi hip screw. Aust N
Z J Surg , 66(3): 151-5, 1996.
39. Hogh, J.: Sliding screw in the treatment of trochanteric and subtrochanteric fractures.
Injury , 14(2): 141-5, 1982.
40. Hopkins, C.; Nugent, J.; and Dimon, J. d.: Medial displacement osteotomy for
unstable intertrochanteric fractures. Twenty years later. Clin Orthop ,(245): 169-72,
1989.
41. Hunter, G.; and Krajbich, I.: The results of medial displacement osteotomy for
unstable intertrochanteric fractures of the femur. Clin Orthop ,(137): 140-3, 1978.
42. Jacobs, R.; McClain, O.; and Armstrong, H.: Internal fixation of intertrochanteric
hip fractures: a clinical and biomechanical study. Clin Orthop ,(146): 62-70, 1980.
43. Jensen, J.; Sonne-Holm, S.; and Tondevold, E.: Unstable trochanteric fractures. A
comparative analysis of four methods of internal fixation. Acta Orthop Scand , 51(6):
949-62, 1980.
44. Jensen, J.; Tondevold, E.; and Mossing, N.: Unstable trochanteric fractures treated
with the sliding screw-plate system. A biomechanical study of unstable trochanteric
fractures. III. Acta Orthop Scand , 49(4): 392-7, 1978.
45. Jensen, J.; Tondevold, E.; and Sonne-Holm, S.: Stable trochanteric fractures. A
comparative analysis of four methods of internal fixation. Acta Orthop Scand , 51(5):
811-6, 1980.
46. Juhn, A.; Krimerman, J.; and Mendes, D.: Intertrochanteric fracture of the hip.
Comparison of nail-plate fixation and Ender's nailing. Arch Orthop Trauma Surg ,
107(3): 136-9, 1988.
47. Kanai, H.; Igarashi, M.; Yamamoto, S.; and Oda, H.: Spontaneous subcapital
femoral neck fracture complicating a healed intertrochanteric fracture. Arch Orthop
Trauma Surg , 119(5-6): 271-5, 1999.
48. Kumar, M.; Sudhakar, G.; Shah, D.; and Pathak, R.: A study of the role of
osteotomy in unstable intertrochanteric fractures. J Postgrad Med , 42(1): 4-6, 1996.

24
49. Kyle, R.: Fixation of intertrochanteric hip fractures with sliding devices. Instr Course
Lect , 33: 197-203, 1984.
50. Kyle, R.; Cabanela, M.; Russell, T., et al.: Fractures of the proximal part of the
femur. Instr Course Lect , 44: 227-53, 1995.
51. Laros, G.: Intertrochanteric fractures. The role of complications of fixation. Arch
Surg , 110(1): 37-40, 1975.
52. Larsson, S.; Friberg, S.; and Hansson, L.: Trochanteric fractures. Influence of
reduction and implant position on impaction and complications. Clin Orthop ,(259): 130-
9, 1990.
53. Laskin, R.; Gruber, M.; and Zimmerman, A.: Intertrochanteric fractures of the hip
in the elderly: a retrospective analysis of 236 cases. Clin Orthop ,(141): 188-95, 1979.
54. Lombardi, L. J.; Cleri, D. J.; Goldhagen, P. R.; and Halligan, J. B.: Subcapital
fracture complicating fixation of an intertrochanteric fracture from osteomyelitis. , 23(3):
257-60, 1994.
55. Lunsjo, K.; Ceder, L.; Stigsson, L.; and Hauggaard, A.: One-way compression
along the femoral shaft with the Medoff sliding plate. The first European experience of
104 intertrochanteric fractures with a 1-year follow-up. Acta Orthop Scand , 66(4): 343-
6, 1995.
56. Lunsjo, K.; Ceder, L.; Stigsson, L.; and Hauggaard, A.: Two-way compression
along the shaft and the neck of the femur with the Medoff sliding plate: one-year follow-
up of 108 intertrochanteric fractures. J Bone Joint Surg Br , 78(3): 387-90, 1996.
57. MacEachern, A.; and Heyse-Moore, G.: Stable intertrochanteric femoral fractures.
A misnomer? J Bone Joint Surg [Br] , 65(5): 582-3, 1983.
58. Madsen, J.; Naess, L.; Aune, A.; Alho, A.; Ekeland, A.; and Stromsoe, K.:
Dynamic hip screw with trochanteric stabilizing plate in the treatment of unstable
proximal femoral fractures: a comparative study with the Gamma nail and compression
hip screw. J Orthop Trauma , 12(4): 241-8, 1998.
59. Mainds, C. C. a. N., R.J.: Implant Failures in Patients with Proximal Fractures of the
Femur Treated with a Sliding Screw Device. , 20: 98, 1989.
60. Malkani, A. L.; and Rand, J. A.: Subcapital femoral neck fracture following open
reduction and internal fixation of an intertrochanteric hip fracture using a sliding screw
and side plate. , 22(4): 469-72, 1993.
61. Manoli, A. d.: Malassembly of the sliding screw-plate device. J Trauma , 26(10):
916-22, 1986.
62. Mariani, E. M.; and Rand, J. A.: Nonunion of intertrochanteric fractures of the
femur following open reduction and internal fixation. Results of second attempts to gain
union. ,(218): 81-9, 1987.
63. Mariani, E. M.; and Rand, J. A.: Subcapital fractures after open reduction and
internal fixation of intertrochanteric fractures of the hip. Report of three cases [see
comments]. ,(245): 165-8, 1989.
64. Medoff, R.; and Maes, K.: A new device for the fixation of unstable pertrochanteric
fractures of the hip. J Bone Joint Surg [Am] , 73(8): 1192-9, 1991.
65. Meislin, R.; Zuckerman, J.; Kummer, F.; and Frankel, V.: A biomechanical
analysis of the sliding hip screw: the question of plate angle. J Orthop Trauma , 4(2):
130-6, 1990.

25
66. Miller, K.; Atzenhofer, K.; Gerber, G.; and Reichel, M.: Risk prediction in
operatively treated fractures of the hip. Clin Orthop ,(293): 148-52, 1993.
67. Moehring, H. D.; Nowinski, G. P.; Chapman, M. W.; and Voigtlander, J. P.:
Irreducible intertrochanteric fractures of the femur. ,(339): 197-9, 1997.
68. Moller, B.; Lucht, U.; Grymer, F.; and Bartholdy, N.: Instability of trochanteric
hip fractures following internal fixation. A radiographic comparison of the Richards
sliding screw-plate and the McLaughlin nail-plate. Acta Orthop Scand , 55(5): 517-20,
1984.
69. Mulholland, R.; and Gunn, D.: Sliding screw plate fixation of intertrochanteric
femoral fractures. J Trauma , 12(7): 581-91, 1972.
70. Mullaji, A.; and Thomas, T.: Low-energy subtrochanteric fractures in elderly
patients: results of fixation with the sliding screw plate. J Trauma , 34(1): 56-61, 1993.
71. Nagi, O.; Dhillon, M.; and Goni, V.: Open reduction, internal fixation and fibular
autografting for neglected fracture of the femoral neck. J Bone Joint Surg Br , 80(5): 798-
804, 1998.
72. Nakata, K.; Ohzono, K.; Hiroshima, K.; and Toge, K.: Serial change of sliding in
intertrochanteric femoral fractures treated with sliding screw system. Arch Orthop
Trauma Surg , 113(5): 276-80, 1994.
73. Nungu, S.; Olerud, C.; and Rehnberg, L.: Treatment of intertrochanteric fractures:
comparison of Ender nails and sliding screw plates. J Orthop Trauma , 5(4): 452-7, 1991.
74. O'Brien, P.; Meek, R.; Blachut, P.; Broekhuyse, H.; and Sabharwal, S.: Fixation
of intertrochanteric hip fractures: gamma nail versus dynamic hip screw. A randomized,
prospective study. Can J Surg , 38(6): 516-20, 1995.
75. Olsson, O.; Ceder, L.; Lunsjo, K.; and Hauggaard, A.: Biaxial dynamization in
unstable intertrochanteric fractures. Good experience with a simplified Medoff sliding
plate in 94 patients. Acta Orthop Scand , 68(4): 327-31, 1997.
76. Olsson, O.; Kummer, F.; Ceder, L.; Koval, K.; Larsson, S.; and Zuckerman, J.:
The Medoff sliding plate and a standard sliding hip screw for unstable intertrochanteric
fractures: a mechanical comparison in cadaver femurs. Acta Orthop Scand , 69(3): 266-
72, 1998.
77. Otsuka, N.; and Schatzker, J.: Subcapital fracture of the hip after internal fixation
of an intertrochanteric fracture. A case report. Arch Orthop Trauma Surg , 112(2): 69-70,
1993.
78. Park, S.; Kang, J.; Kim, H.; Lee, W.; and Kim, Y.: Treatment of intertrochanteric
fracture with the Gamma AP locking nail or by a compression hip screw--a randomised
prospective trial. Int Orthop , 22(3): 157-60, 1998.
79. Pitsaer, E.; and Samuel, A.: Functional outcome after intertrochanteric fractures of
the femur: does the implant matter? A prospective study of 100 consecutive cases. Injury
, 24(1): 35-6, 1993.
80. Pun, W.; Chow, S.; Chan, K., et al.: Treatment of unstable intertrochanteric
fractures with Sarmiento valgus osteotomy and acrylic cement augmentation. Injury ,
18(6): 384-9, 1987.
81. Rao, J.; Alber, G.; and Gutteling, E.: Clinical evaluation of the Alta hip bolt in
peritrochanteric hip fractures. Am J Orthop , 27(9): 612-6, 1998.

26
82. Rao, J.; Banzon, M.; Weiss, A.; and Rayhack, J.: Treatment of unstable
intertrochanteric fractures with anatomic reduction and compression hip screw fixation.
Clin Orthop ,(175): 65-71, 1983.
83. Rao, J.; Hambly, M.; King, J.; and Benevenia, J.: A comparative analysis of
Ender's-rod and compression screw and side plate fixation of intertrochanteric fractures
of the hip. Clin Orthop ,(256): 125-31, 1990.
84. Rau, F.; Manoli, A. d.; and Morawa, L.: Treatment of femoral neck fractures with
the sliding compression screw. Clin Orthop ,(163): 137-40, 1982.
85. Rha, J.; Kim, Y.; Yoon, S.; Park, T.; and Lee, M.: Factors affecting sliding of the
lag screw in intertrochanteric fractures. Int Orthop , 17(5): 320-4, 1993.
86. Ruff, M.; and Lubbers, L.: Treatment of subtrochanteric fractures with a sliding
screw-plate device. J Trauma , 26(1): 75-80, 1986.
87. Sahlstrand, T.: The Richards compression and sliding hip screw system in the
treatment of intertrochanteric fractures. Acta Orthop Scand , 45(2): 213-9, 1974.
88. Sarathy, M.; Madhavan, P.; and Oomen, M.: Modified medial displacement and
valgus osteotomy for unstable intertrochanteric fractures. Injury , 28(9-10): 601-5, 1997.
89. Sartoris, D.; Kerr, R.; Goergen, T.; and Resnick, D.: Sliding-screw plate fixation
of proximal femoral fractures: radiographic assessment. Skeletal Radiol , 14(2): 104-10,
1985.
90. Sernbo, I.; Johnell, O.; Gentz, C.; and Nilsson, J.: Unstable intertrochanteric
fractures of the hip. Treatment with Ender pins compared with a compression hip-screw.
J Bone Joint Surg [Am] , 70(9): 1297-303, 1988.
91. Sherk, H.; and Foster, M.: Hip fractures: condylocephalic rod versus compression
screw. Clin Orthop ,(192): 255-9, 1985.
92. Stark, A.; Brostrom, L.; Barrios, C.; Walheim, G.; and Olsson, E.: A prospective
randomized study of the use of sliding hip screws and Ender nails for trochanteric
fractures of the femur. Int Orthop , 16(4): 359-62, 1992.
93. Steinberg, G.; Desai, S.; Kornwitz, N.; and Sullivan, T.: The intertrochanteric hip
fracture. A retrospective analysis. Orthopedics , 11(2): 265-73, 1988.
94. Swiontkowski, M.; Harrington, R.; Keller, T.; and Van, P. P.: Torsion and
bending analysis of internal fixation techniques for femoral neck fractures: the role of
implant design and bone density. J Orthop Res , 5(3): 433-44, 1987.
95. Thomas, A. P.: Dynamic Hip Screws That Fail. , 22(1): 45-46, 1991.
96. Tigani, D.; Laus, M.; Bettelli, G.; Boriani, S.; and Giunti, A.: The Gamma nail,
sliding-compression plate. A comparison between the long-term results obtained in two
similar series. Chir Organi Mov , 77(2): 151-8, 1992.
97. Walsh, M.; Wilkinson, R.; and Stother, I.: Biomechanical stability of four-part
intertrochanteric fractures in cadaveric femurs fixed with a sliding screw-plate. Injury ,
21(2): 89-92, 1990.
98. Watson, J.; Moed, B.; Cramer, K.; and Karges, D.: Comparison of the
compression hip screw with the Medoff sliding plate for intertrochanteric fractures. Clin
Orthop ,(348): 79-86, 1998.
99. Wellin, D. E.; Galloni, L.; and Gelb, R. I.: Ipsilateral intertrochanteric and
diaphyseal femoral fractures. Four patients treated by one technique. ,(183): 71-5, 1984.

27
100. Whitelaw, G.; Segal, D.; Sanzone, C.; Ober, N.; and Hadley, N.: Unstable
intertrochanteric/subtrochanteric fractures of the femur. Clin Orthop ,(252): 238-45,
1990.
101. Wile, P.; Panjabi, M.; and Southwick, W.: Treatment of subtrochanteric fractures
with a high-angle compression hip screw. Clin Orthop ,(175): 72-8, 1983.
102. Wilson, H. J.; Rubin, B.; Helbig, F.; Fielding, J.; and Unis, G.: Treatment of
interotrochanteric fractures with the Jewett nail: experience with 1,015 cases. Clin
Orthop ,(148): 186-91, 1980.
103. Wolfgang, G.; Bryant, M.; and O'Neill, J.: Treatment of intertrochanteric fracture
of the femur using sliding screw plate fixation. Clin Orthop ,(163): 148-58, 1982.
104. Wu, C.; Shih, C.; Lee, M.; and Tai, C.: Biomechanical analysis of location of lag
screw of a dynamic hip screw in treatment of unstable intertrochanteric fracture. J
Trauma , 41(4): 699-702, 1996.
105. Yoshimine, F.; Latta, L.; and Milne, E.: Sliding characteristics of compression hip
screws in the intertrochanteric fracture: a clinical study. J Orthop Trauma , 7(4): 348-53,
1993.
106. Zukor, D.; Miller, B.; Hadjipavlou, A.; and Lander, P.: Hip pinning, past and
present: Richards' compression-screw fixation versus Ender's nailing. Can J Surg , 28(5):
391-5, 1985.