“Biologics” and the spondyloarthropathies (for a busy GP) South/Sat_room10_0710_Grainger.pdf ·...
47
“Biologics” and the spondyloarthropathies (for a busy GP) Dr Rebecca Grainger Rheumatologist, Hutt Valley DHB Senior Lecturer, University of Otago Wellington GPCME South 2015
Transcript of “Biologics” and the spondyloarthropathies (for a busy GP) South/Sat_room10_0710_Grainger.pdf ·...

“Biologics” and the spondyloarthropathies
(for a busy GP)
Dr Rebecca GraingerRheumatologist, Hutt Valley DHB
Senior Lecturer, University of Otago WellingtonGPCME South 2015
Topics
• Overview of spondyloarthropathies
• Role of biologics in treatment
• Practical aspects of biologics
– Administration
– Adverse effects
– Collaborative management with secondary care
• Cardiovascular risk
• Vaccination

Learning outcomes
• Feel confident in providing for primary care needs of patients with inflammatory arthritis (esp SpA) on biologics funded in NZ






Psoriatic arthritis
• Arthritis in 20-40% PsO• Arthritis may predate PsO• May only be FHx PsO• Peak onset 20-40 yrs

Psoriatic Arthritis
• Monoarthritis (1) or
Oligoarthritis (2-4) or
Polyarthritis (>4)
• Small or large joints
• Spinal involvement
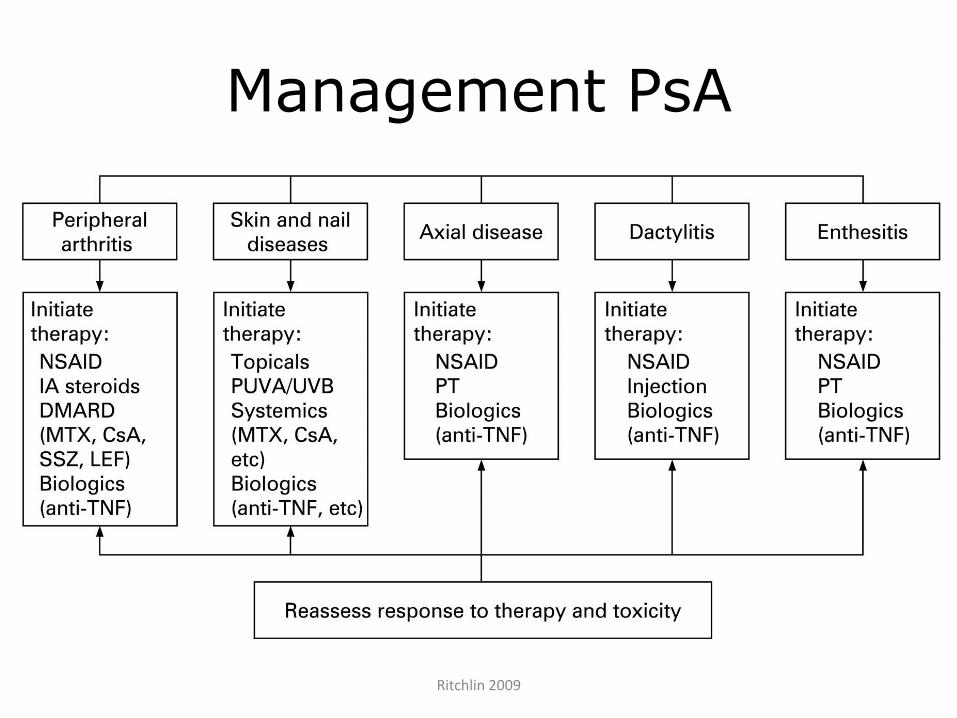
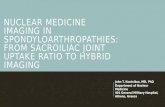
Management PsA
Ritchlin 2009



Biologic DMARDs
Bioengineered variants of endogenous proteins with specific inflammatory
targets

bDMARD – TNF inhibitors
Bioengineered variants of endogenous proteins targeting TNF-α

Inflammatory arthritis Funded bDMARDs (in NZ)
Name Target Administration
Adalimumab(Humira®)
TNF s/c fortnightly
Etanercept(Enbrel®)
TNF s/c weekly
Infliximab (Remicade®) TNF i/v 2 months
Rituximab (Mabthera®) CD-20 (B cell marker)
i/v >6 months
Tocilizumab (Actemra®) IL-6 i/v monthly

Inflammatory arthritis Funded bDMARDs (in NZ)
Name Target Administration
Adalimumab(Humira®)
TNF s/c fortnightly
Etanercept(Enbrel®)
TNF s/c weekly
Infliximab (Remicade®) TNF i/v 2 months
Rituximab (Mabthera®) CD-20 (B cell marker)
i/v >6 months
Tocilizumab (Actemra®) IL-6 i/v monthly

Inflammatory arthritis Funded bDMARDs (in NZ)
Name Target Administration
Adalimumab(Humira®)
TNF s/c fortnightly
Etanercept(Enbrel®)
TNF s/c weekly
Infliximab (Remicade®) TNF i/v 2 months
Rituximab (Mabthera®) CD-20 (B cell marker)
i/v >6 months
Tocilizumab (Actemra®) IL-6 i/v monthly





Lower back pain is common
• Lifetime prevalence 50-80%
• Point prevalence 15-30%

37 year old male
5 years of intermittent lower back pain
4 months buttock pain, especially in the
morning
Sleeping poorly due to pain
Painful heel
“I thought I should go back to see my GP cause my stiffness was just like car driver on tv”
NSAIDS from GP reduced night time pain

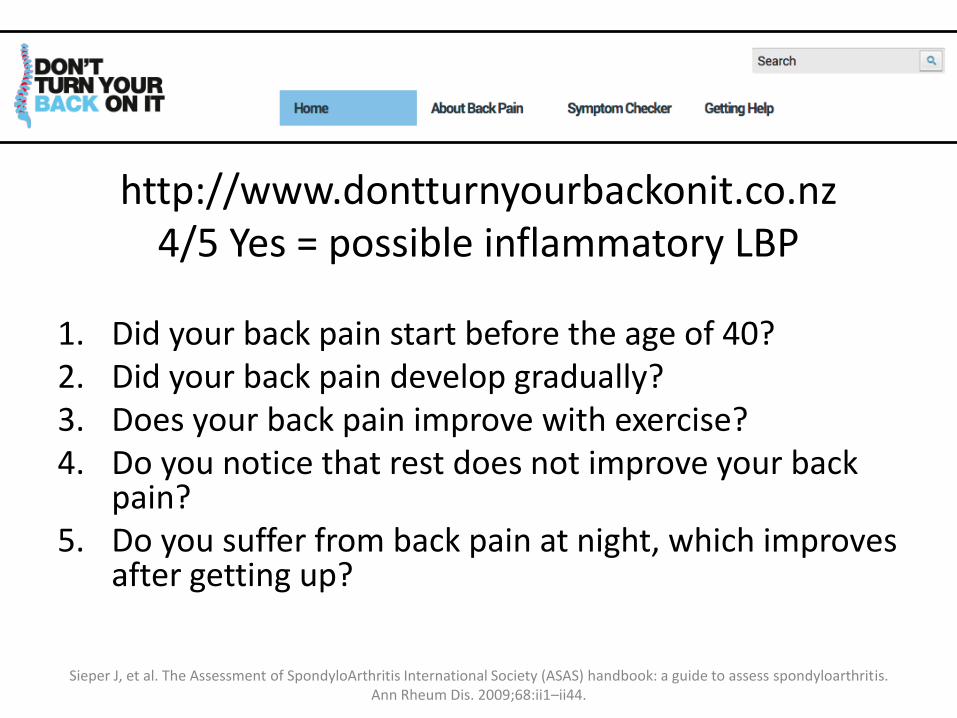
http://www.dontturnyourbackonit.co.nz4/5 Yes = possible inflammatory LBP
1. Did your back pain start before the age of 40?2. Did your back pain develop gradually?3. Does your back pain improve with exercise?4. Do you notice that rest does not improve your back
pain?5. Do you suffer from back pain at night, which improves
after getting up?
Sieper J, et al. The Assessment of SpondyloArthritis International Society (ASAS) handbook: a guide to assess spondyloarthritis.Ann Rheum Dis. 2009;68:ii1–ii44.

http://www.dontturnyourbackonit.co.nz/back-pain-symptom-checker/results.html?chk1=yes&chk2=yes&chk3=yes&chk4=yes&chk5=yes&quesnum=5

Further information required
• Any suggestions?

Further information required
• Personal or family history of Psoriasis
• Current ROM spine (Cx, axial, lumbar)
• HLA B27 status

37 year old male
5 years of intermittent lower back pain
Dx Ankylosing spondylitis

37 year old male
5 years of intermittent lower back pain
Dx Ankylosing spondylitis
Ongoing pain despite diclofenac then
naproxen
BASDAI 6.5
Rx Adalimumab (Humira©)

2 Kivitz 2006


TNFI Contraindications
• Active infections
• Malignancy within 5 years (x non-melanoma skin cancer)
• Inadequately treated prior Tb or latent Tb
• Co-morbidities
– CHF Grade III or IV
– Demyelinating disease

TNFI Pretreatment work up
• Measure of disease activity
• Hep B/C serology
• Screen for latent Tb (CXR, Quantiferon gold)
• HIV if risk factors
• Immunisations…….

TNFI Immunisation
• Avoid live vaccines
– Yellow fever, MMR, BCG, oral polio, oral typhoid
– Avoid Zostavax
• Annual influenza
• Vaccination against pneumococcus recommended before initiation
– Pneumovax vs Prevenar 13
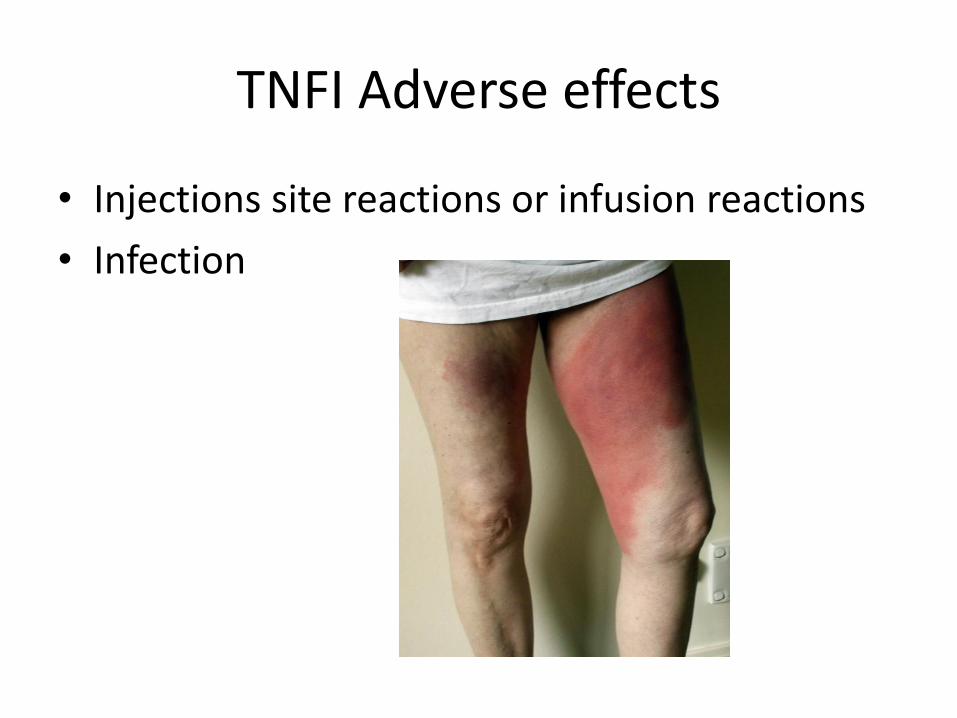
TNFI Adverse effects
• Injections site reactions or infusion reactions
• Infection

TNFI Infections
https://commons.wikimedia.org/wiki/File:Cellulitis3.jpg. https://en.wikipedia.org/wiki/File:PneumonisWedge09.JPG https://en.wikipedia.org/wiki/File:Pyuria2011.JPG
The usual suspects, AND opportunistic organisms
Tuberculosis screening in all pre treatment
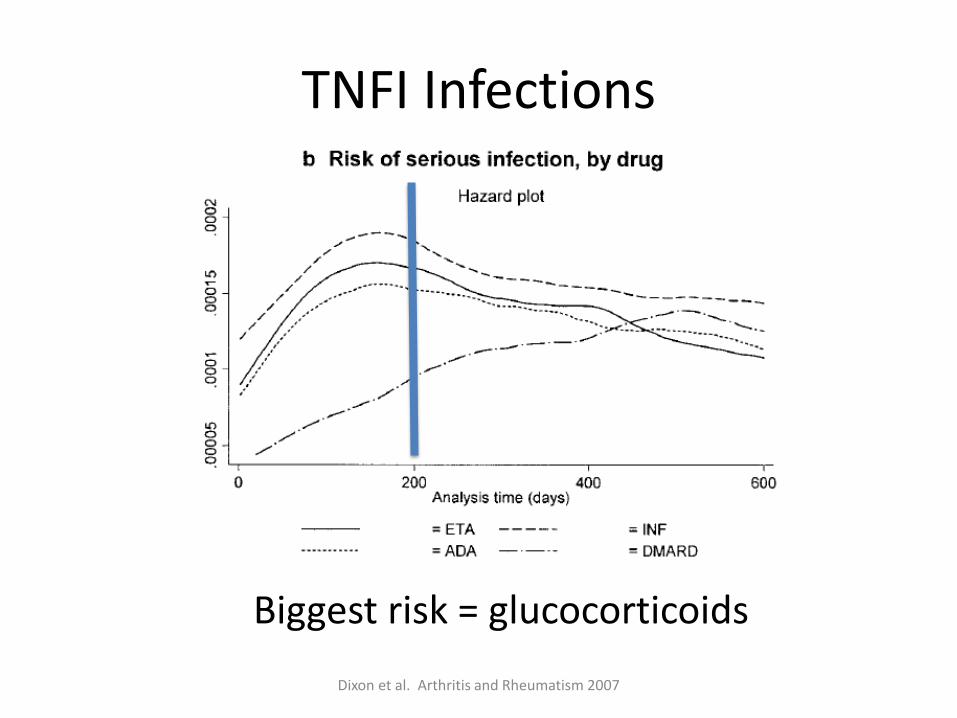
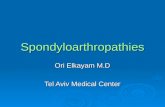
TNFI Infections
Dixon et al. Arthritis and Rheumatism 2007
Biggest risk = glucocorticoids
TNFI infection advice
• Patients are advised to seek medical advice early in the event of unexplained illness.
– Recommend medical review that day if temperature >38.5oC on one occasion or >38oC on two occasions more than one hour apart.
– Withhold any further doses of biologic until infection has been adequately assessed and if necessary treated.

TNFI Monitoring
• Seen every 6 months (special authority)
• Lab monitoring not specifically required for BDMARDs

TNFI FAQs
• Pregnancy and breastfeeding not recommended
• Contraception recommended
• Discontinue at confirmation of pregnancy
• No known drug interactions
• If misses s/c dose - inject asap when remembered then next dose as usual

TNFI Surgery and intercurrent illness
• Skip biologics week of surgery, restart once infection risk low
• Withhold if intercurrent infection

Take home messages
• <40 LBP ?inflammatory
– www.donturnyourbackonit.co.nz
• TNFI treatment
– Flu vaccination – the under 65s
– Intercurrent illness – THINK INFECTION