
Biological targeted agents for mGC · Biological targeted agents for mGC. ... Better drugs, better...
39
Sun Young RHA Yonsei Cancer Center Yonsei University College of Medicine ESMO GI preceptorship 2019 Biological targeted agents for mGC
Transcript of Biological targeted agents for mGC · Biological targeted agents for mGC. ... Better drugs, better...

Sun Young RHAYonsei Cancer Center
Yonsei University College of Medicine
ESMO GI preceptorship 2019
Biological targeted agents for mGC
Disclosures
• Research grants and research support: MSD, BMS, GSK, Eli Lilly, Boehringer Ingelheim
• Consultation/advisory role: MSD, Celltrion, Ipsen, Daiichi Sankyo, Eisai
• Speaker bureau: Eli Lilly, Ipsen
Agenda
• Molecular subgrouping
• Her-2 +
• Angiogenesis
• Others

5-fluorouracil/platinum(+/- docetaxel) 5-7 Mo
Paclitaxel or Irinotecan (3-5 Mo)
+ Trastuzumab in Her-2 + + Ramucirumab
Current treatment of metastatic GC (median 16-18m)
90 % 60-65% 30-40%
Supportive2nd line Tx (3rd - 4th line Tx)1st line Tx
Chemotherapy
Apatinib?
Pembrolizumab in MSI-H/dMMR
� Asians vs westerns
� Chemotherapy is the main treatment
� Doublet vs triplet
� Various doublets are similar
� Sequential treatment improved survival
� Angiogenesis inhibitor showed benefit in 2nd line and more
� Role of molecular targeted agents?
� IO showed the potential benefit in subgroup
� New strategy: Conversion surgery, IP chemotherapy
Nivolumab, Pembrolizumab in PD-L1 +

Multiple combination
with next generation
precision medicine
1970s 1980s 1990s 2000s 2015s~2010s
Surgery/
Radiotherapy
Combination
Chemotherapy
Targeted
Agents
Various
combinations
Targeted
Agents
Precision medicine
with targeted
agents
Immunotherapy
Trastuzumab
in Her-2+ GCRamucirumab
in 2nd line GC
GCNivolumab
Pembrolizumab
Lung ca
mOS 6months ----------------------------------------------------- ---------------------------� 38-52months
mOS 6months ----------------------------------------------------- ---------------------------� 16 months
Different treatment development and outcome in Lung Ca and Gastric Ca

1) Development of high-technology2) Genomic dissection3) Understanding biology4) Translating into clinical/patient biology : Dependency?
-> novel targets-> novel drugs
5) Clinical feasibility: heterogeneity-> proper patient selection : Biomarker!!
Genomic Dissection -> Improving Treatment Outcome
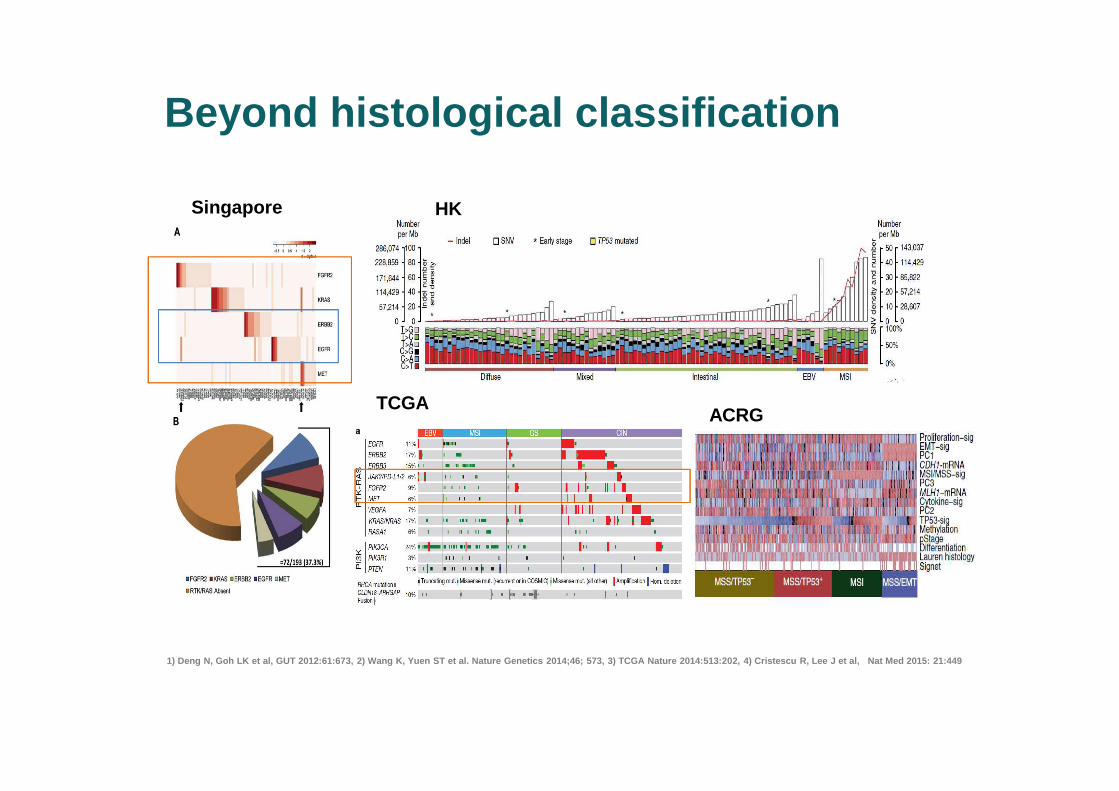
Beyond histological classification
1) Deng N, Goh LK et al, GUT 2012:61:673, 2) Wang K , Yuen ST et al. Nature Genetics 2014;46; 573, 3) T CGA Nature 2014:513:202, 4) Cristescu R, Lee J et a l, Nat Med 2015: 21:449
Singapore HK
TCGAACRG

� Many negative trials • Bevacizumab• Cetuximab• Panitumumab• Lapatinib• Everolimus (mTORi)• Rilotumumab• Onartuzumab• AMG337(Met i)• AZ4547 (FGFRi)• MK2206 (AKTi)• Etc ..
Deng N, Goh LK et al, GUT 2012:61:673
� Not a genomic-driven disease?� Hit the proper target with proper biomarker/assay for patient
enrichment?
� Heterogeneity and genomic evolution? � Immunogenic tumor? Role of IO Tx?
Adding molecular targeted agents-> Genomics and precision medicine in mGC
Adding trastuzumab in Her-2 + patients(1st line): 2010

Gastric cancerLung ca
NRAS 1%
US Lung Cancer Mutation Consortium(N = 733 for 10 genes)
EGFR(sensitizing)
17%
HER2 3%
ALK 8%MEK1 <1%
MET 1%
Mut >1 gene 3%
No oncogenicdriver detected
36%
PIK3CA 1%
KRAS 25%
EGFR (other)4%
BRAF 2%
Oncogenic driver 466/733 (64%)
TCGA 30.6% -> real world <10% Her-2 10%
• Utility of molecular subtype in clinical practice: ~20%
So many differences among tumor types
� Different genomic dependency� More heterogeneity and genomic evolution? � Different TMEs� Etc …
Genomic dissection of Gastric cancer did not transl ate to the clinical practice
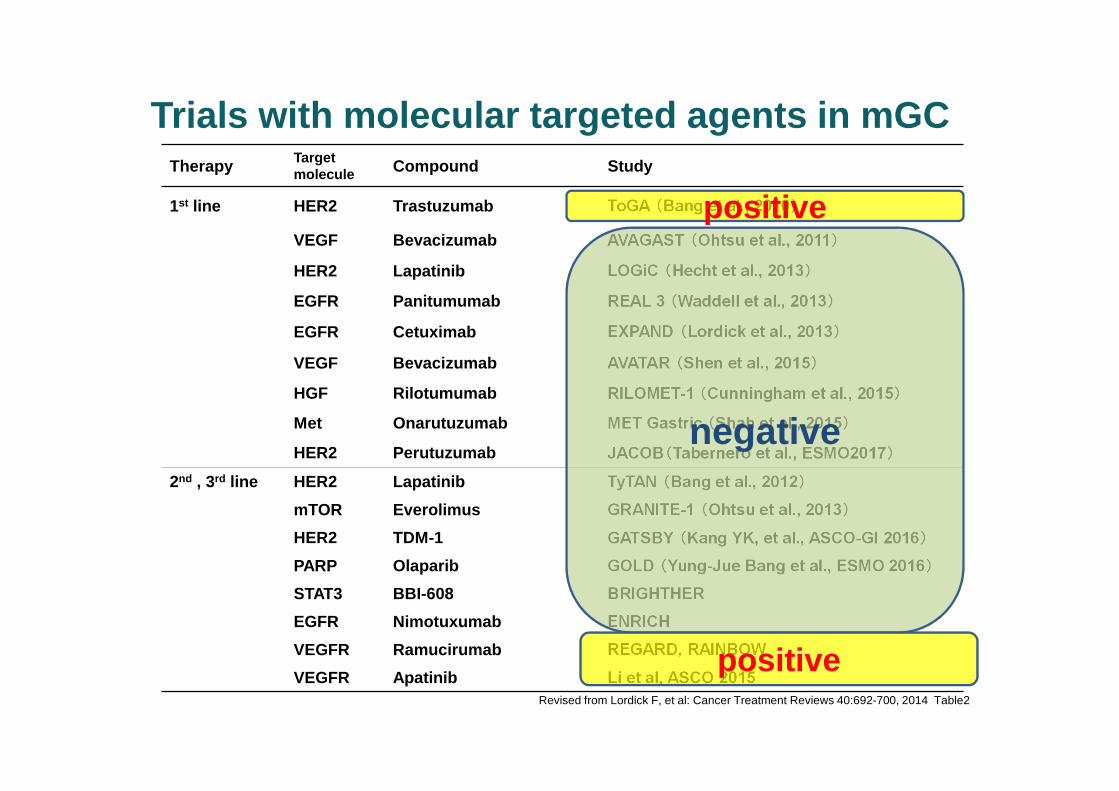
Therapy Target molecule Compound Study
1st line HER2 Trastuzumab ToGA (Bang et al., 2010 )
VEGF Bevacizumab AVAGAST (Ohtsu et al., 2011 )
HER2 Lapatinib LOGiC (Hecht et al., 2013 )
EGFR Panitumumab REAL 3 (Waddell et al., 2013 )
EGFR Cetuximab EXPAND (Lordick et al., 2013 )
VEGF Bevacizumab AVATAR (Shen et al., 2015 )
HGF Rilotumumab RILOMET-1 (Cunningham et al., 2015 )
Met Onarutuzumab MET Gastric (Shah et al., 2015 )
HER2 Perutuzumab JACOB (Tabernero et al., ESMO2017 )
2nd , 3rd line HER2 Lapatinib TyTAN (Bang et al., 2012 )
mTOR Everolimus GRANITE-1 (Ohtsu et al., 2013 )
HER2 TDM-1 GATSBY (Kang YK, et al., ASCO-GI 2016 )
PARP Olaparib GOLD (Yung-Jue Bang et al., ESMO 2016 )
STAT3 BBI-608 BRIGHTHER
EGFR Nimotuxumab ENRICH
VEGFR Ramucirumab REGARD, RAINBOW
VEGFR Apatinib Li et al, ASCO 2015Revised from Lordick F, et al: Cancer Treatment Reviews 40:692-700, 2014 Table2
positive
negative
positive
Trials with molecular targeted agents in mGC
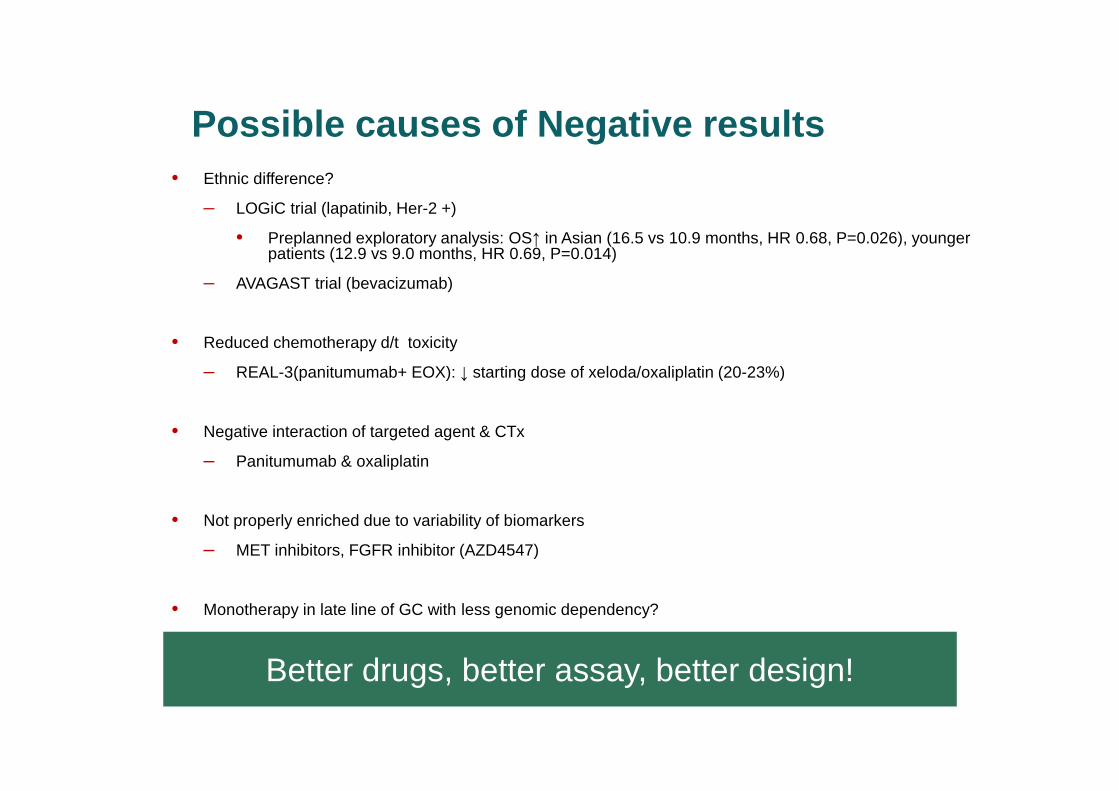
• Ethnic difference?
– LOGiC trial (lapatinib, Her-2 +)
• Preplanned exploratory analysis: OS↑ in Asian (16.5 vs 10.9 months, HR 0.68, P=0.026), younger patients (12.9 vs 9.0 months, HR 0.69, P=0.014)
– AVAGAST trial (bevacizumab)
• Reduced chemotherapy d/t toxicity
– REAL-3(panitumumab+ EOX): ↓ starting dose of xeloda/oxaliplatin (20-23%)
• Negative interaction of targeted agent & CTx
– Panitumumab & oxaliplatin
• Not properly enriched due to variability of biomarkers
– MET inhibitors, FGFR inhibitor (AZD4547)
• Monotherapy in late line of GC with less genomic dependency?
Better drugs, better assay, better design!
Possible causes of Negative results

Comprehensive molecular characterization of gastric adenocarcinoma. 2014. Nature
�The Cancer Genome Atlas - GC
� Reliable molecular subgrouping of mGC
� Multiple targets with multiple potential drugs/Tx
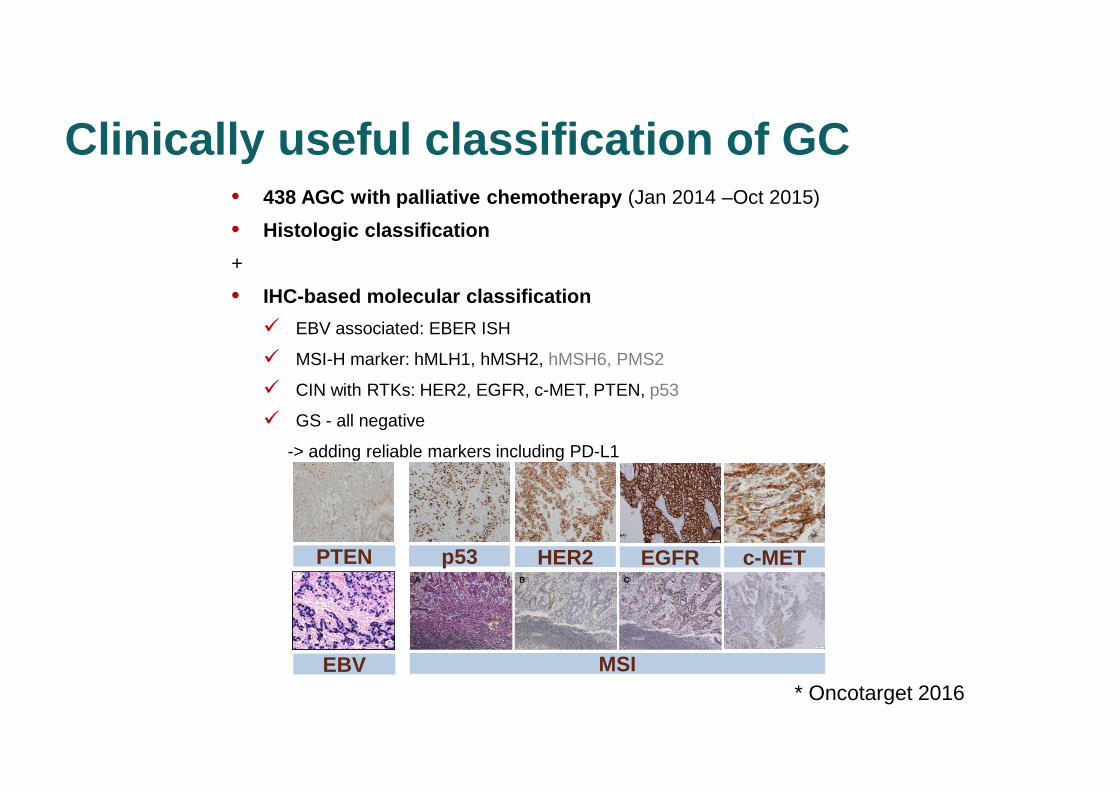
Clinically useful classification of GC• 438 AGC with palliative chemotherapy (Jan 2014 –Oct 2015)
• Histologic classification
+
• IHC-based molecular classification
� EBV associated: EBER ISH
� MSI-H marker: hMLH1, hMSH2, hMSH6, PMS2
� CIN with RTKs: HER2, EGFR, c-MET, PTEN, p53
� GS - all negative
-> adding reliable markers including PD-L1
EBV EBV MSIMSI
PTENPTEN p53p53 HER2HER2 EGFREGFR c-METc-MET
* Oncotarget 2016
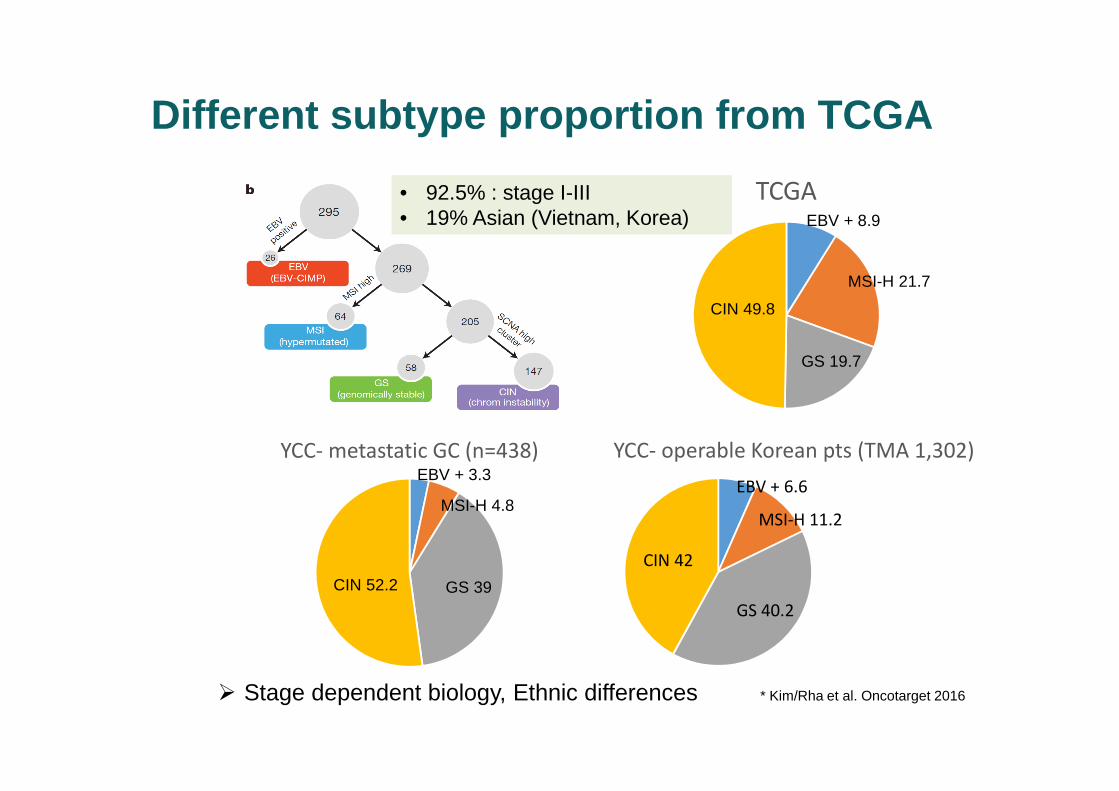
� Stage dependent biology, Ethnic differences * Kim/Rha et al. Oncotarget 2016
Different subtype proportion from TCGA
TCGAEBV + 8.9
MSI-H 21.7
GS 19.7
CIN 49.8
YCC- metastatic GC (n=438)EBV + 3.3
MSI-H 4.8
GS 39CIN 52.2
YCC- operable Korean pts (TMA 1,302)
MSI-H 11.2
EBV + 6.6
GS 40.2
CIN 42
• 92.5% : stage I-III • 19% Asian (Vietnam, Korea)

• Most common (~40%)• With druggable targets • HER2 negative group (~90%)
-> in need of drug development
Triple Negative Gastric Cancer (EBV negative, MSI negative, HER2 negative)
-> Proper screening and new drug development!
• Most common in Korea/ Asia(30~40%)• No druggable targets• Necessity of new targets/drugs
• Potential for Immune Tx• Less incidence( ~12%)
PD-L1 / CD2747
6
5
4
3
2
1
0
mR
NA
Exp
ress
ion
(RN
A S
eq R
PK
M)(
log2
)
CIN EBV GS MSIMolecular Subtype
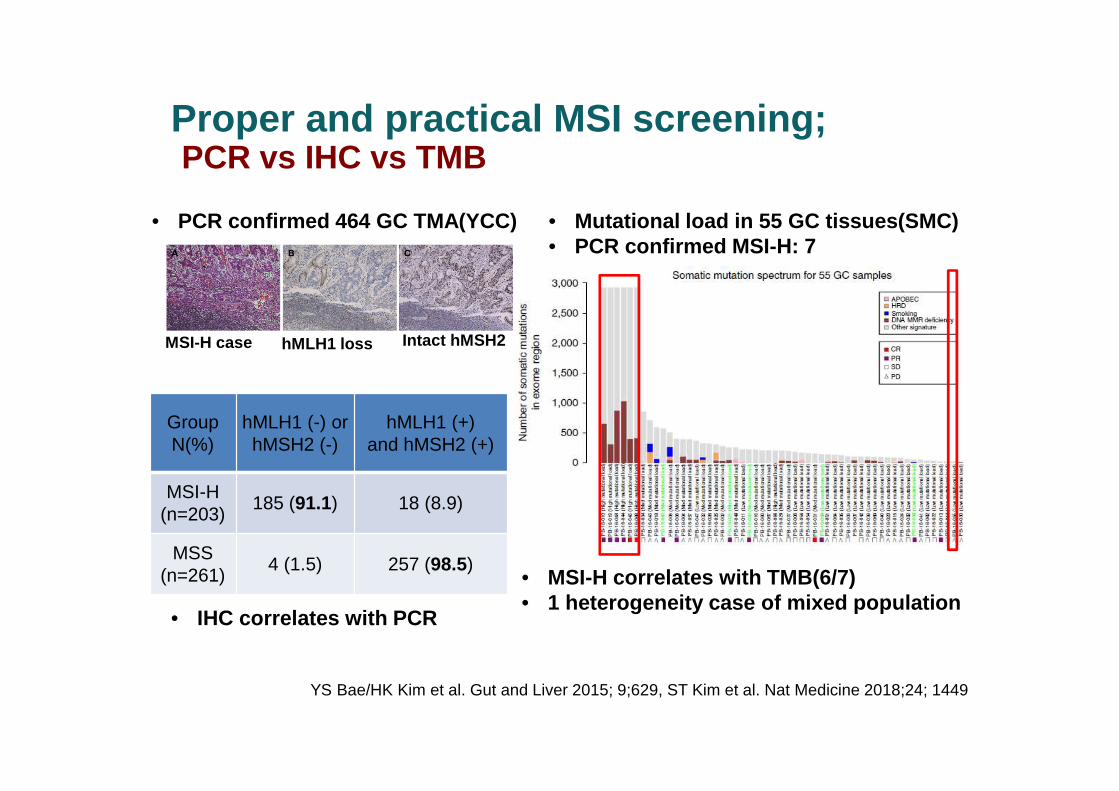
GroupN(%)
hMLH1 (-) or hMSH2 (-)
hMLH1 (+) and hMSH2 (+)
MSI-H (n=203)
185 (91.1) 18 (8.9)
MSS (n=261)
4 (1.5) 257 (98.5)
hMLH1 loss Intact hMSH2
YS Bae/HK Kim et al. Gut and Liver 2015; 9;629, ST Kim et al. Nat Medicine 2018;24; 1449
Proper and practical MSI screening; PCR vs IHC vs TMB
• PCR confirmed 464 GC TMA(YCC)
MSI-H case
• Mutational load in 55 GC tissues(SMC)• PCR confirmed MSI-H: 7
• MSI-H correlates with TMB(6/7)• 1 heterogeneity case of mixed population
• IHC correlates with PCR

0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
F/X + C
F/X + C + Trastuzumab
Months
294290
277 266
246223
209185
173143
147117
11390
9064
7147
5632
4324
3016
2114
137
126
65
40
10
00
No. at risk
Probability of survival
Events
167182
HR
0.74
95% CI
0.60, 0.91
p value
0.0046
MedianOS
13.811.1
11.1 13.8
F, 5-FU; X, Xeloda®; C, cisplatin Bang et al. Lancet 2010
� HER2-positive : IHC 3+ or HER2 FISH (+)
Targeting HER -2 in GC: TOGA trial

Soularue et al, Bull Cancer. 2015 Apr;102(4):324-31..
Ryu et al, Eur J Cancer. 2015 Mar;51(4):482-8.Gong et al, BMC Cancer. 2016 Feb 8;16:68.
N Chemotherapy
partner
ORR mPFS mOS
Soularue et al* 34 FOLFOX/XELOX 41% 9m 17.3m
Ryu et al 55 XELOX 67% 9.8m 21.0m
Gong et al 55 XELOX 68% 9.2m 19.5m
*retrospective
Outcomes appear similar to cisplatin and 5FU in TOGA
Caveat: Phase II, uncontrolled data
NCCN Gastric Cancer Guidelines 2018
Trastuzumab + cisplatin/5FU – Category 1
Trastuzumab + other chemotherapy – Category 2B
Alternative chemotherapy regimens: Oxaliplatin -based + trastuzumab

Treatment naïve advanced HER2 positive* gastric
cancer
S-1 80-120 mg
D1-14
Cisplatin 60
mg2 D1 q21D
+
Trastuzumab
n=55
HERBIS-1
Median OS and PFS were 16.0 months and 7.8 months
Kurokawa et al, Br J Cancer. 2014 Mar 4;110(5):1163-8.
*IHC 3+ or FISH positive
ORR 68%
Alternative chemotherapy regimens: Cisplatin + S1 (SP) + trastuzumab
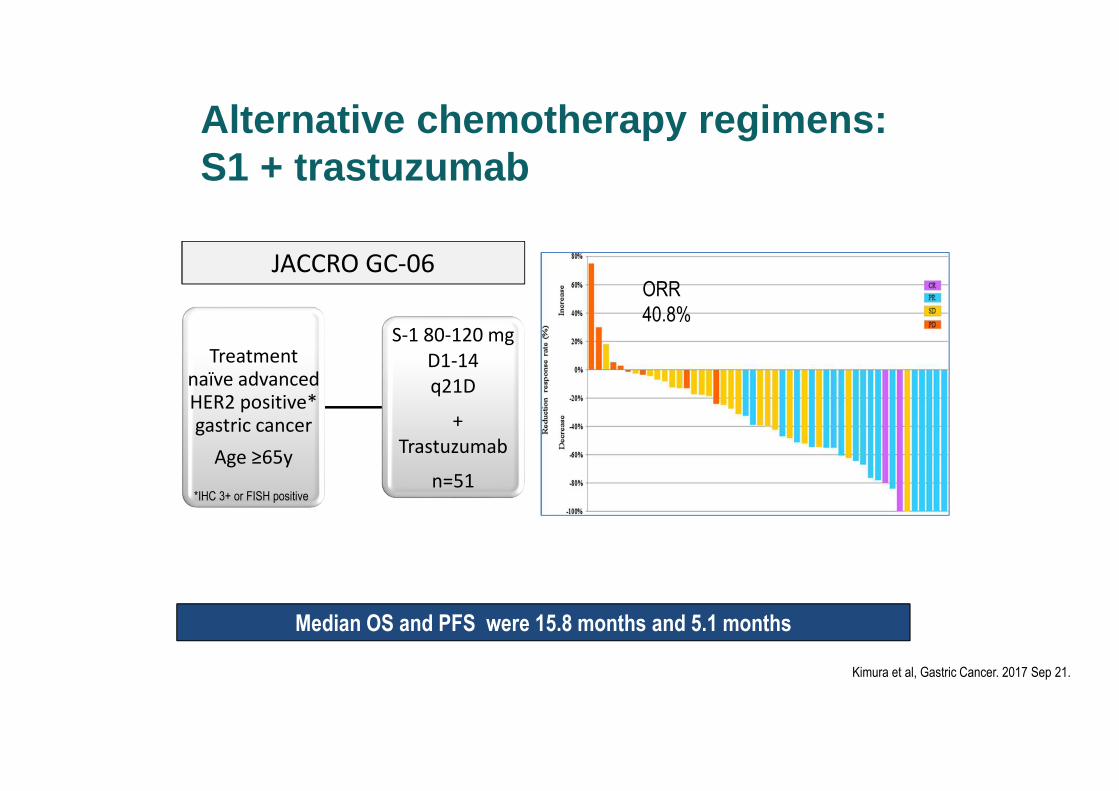
Treatmentnaïve advanced HER2 positive* gastric cancer
Age ≥65y
S-1 80-120 mg
D1-14
q21D
+
Trastuzumab
n=51
JACCRO GC-06
Median OS and PFS were 15.8 months and 5.1 months
Kimura et al, Gastric Cancer. 2017 Sep 21.
*IHC 3+ or FISH positive
ORR
40.8%
Alternative chemotherapy regimens: S1 + trastuzumab

HER2 positive treatment naïve
GEJ/ GC
CF/X + Trastuzum
ab
(n=388)
CF/X + Trastuzumab +
Pertuzumab
(n=392)
International multicentre trial
Primary endpoint = OS
Tabernero et al, ESMO 2017
Objective response rate (ORR) in evaluable
patients
CF/X + T CF/X + T + P
ORR (%) 56.7 48.3
Duration of
ORR (m)
10.2 8.4
Progression free survival
CF/X + T CF/X + T + P
PFS (months) 7.0 8.5
HR 0.73 (95%CI 0.62 -0.86)
CF/X, cisplatin, 5-fluorouracil or capecitabine
Despite 3.3 month absolute benefit in OS, no statistically
significant benefit in OS for addition of pertuzumab
Pertuzumab & Trastuzumab in HER + GC: JACOB trial
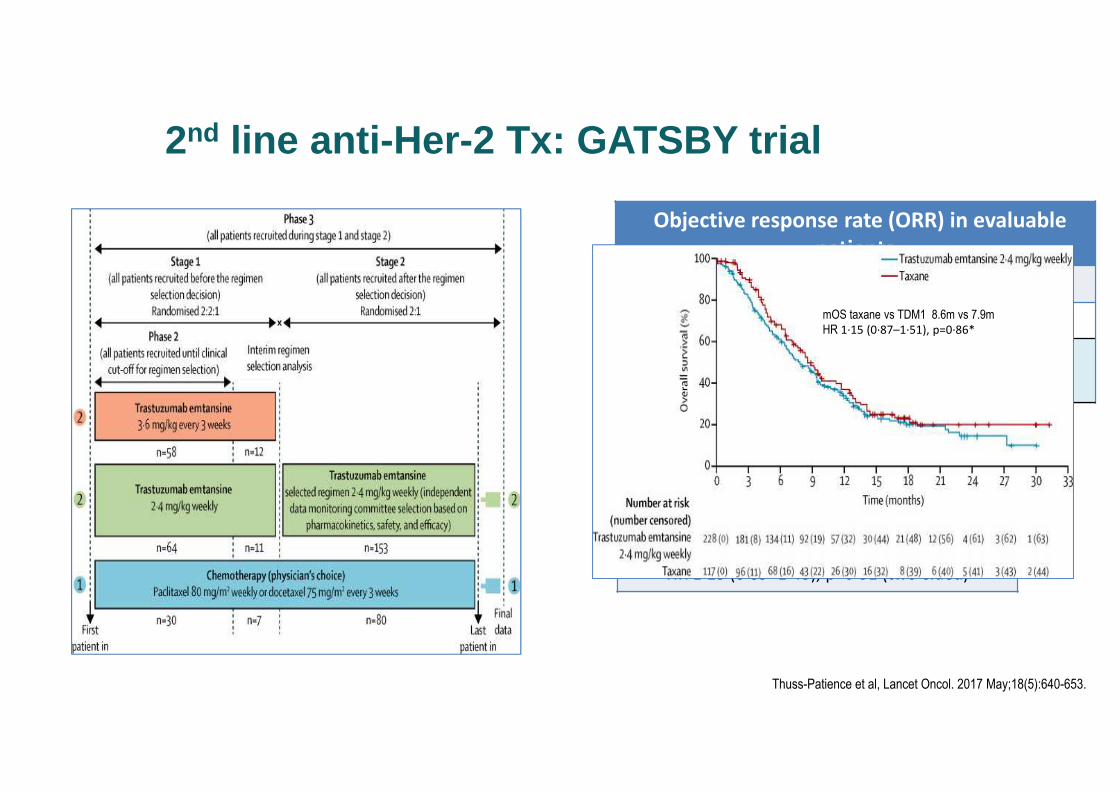
Objective response rate (ORR) in evaluable
patients
Taxane TDM1
ORR (%) 19.6 20.6
Duration of
response
3.7m 4.3m
Progression free survival
Taxane TDM1
PFS
(months)
2.9 2.7
HR 1·13 (0·89–1·43), p=0·31 (two-sided)
Thuss-Patience et al, Lancet Oncol. 2017 May;18(5):640-653.
mOS taxane vs TDM1 8.6m vs 7.9m
HR 1·15 (0·87–1·51), p=0·86*
2nd line anti-Her-2 Tx : GATSBY trial

Iwata H et al. ASCO 2018 (Abst 1031)
• ORR 43.2% (19/44)
• DCR 79.5% (35/44)
• PFS 5.6 months
DS-8201a: A novel HER2 ADC
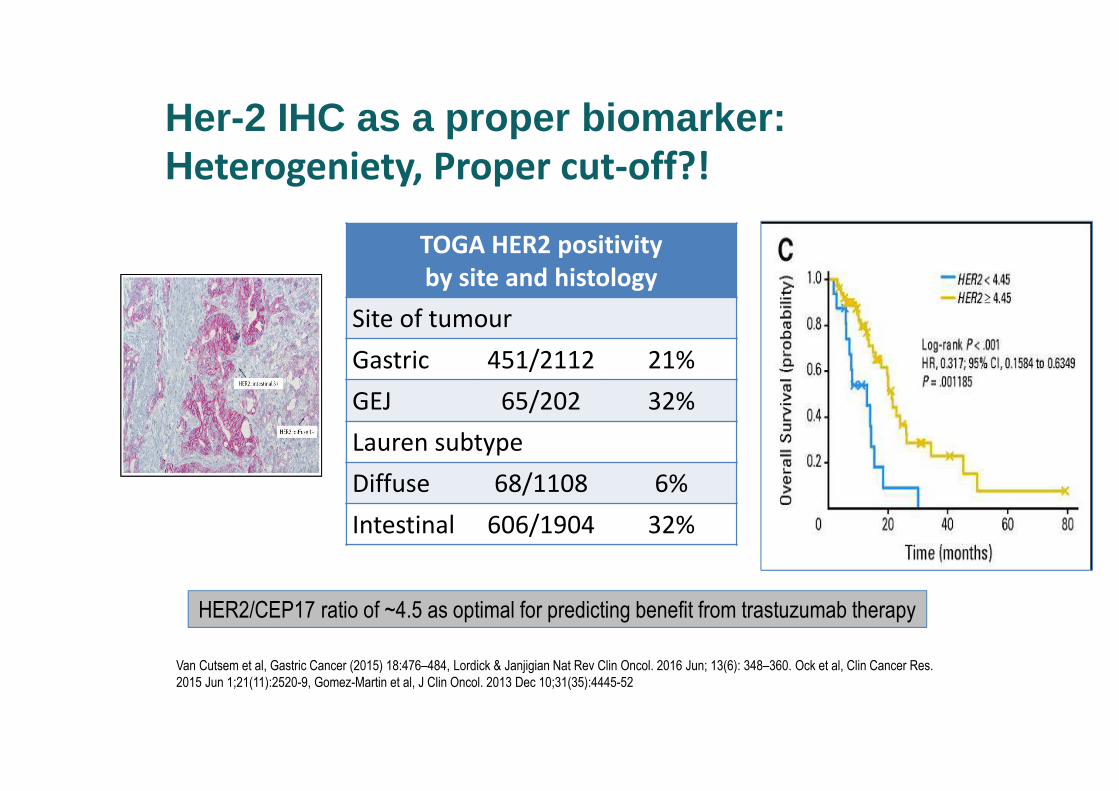
TOGA HER2 positivity
by site and histology
Site of tumour
Gastric 451/2112 21%
GEJ 65/202 32%
Lauren subtype
Diffuse 68/1108 6%
Intestinal 606/1904 32%
Van Cutsem et al, Gastric Cancer (2015) 18:476–484, Lordick & Janjigian Nat Rev Clin Oncol. 2016 Jun; 13(6): 348–360. Ock et al, Clin Cancer Res.
2015 Jun 1;21(11):2520-9, Gomez-Martin et al, J Clin Oncol. 2013 Dec 10;31(35):4445-52
Her-2 IHC as a proper biomarker: Heterogeniety, Proper cut-off?!
HER2/CEP17 ratio of ~4.5 as optimal for predicting benefit from trastuzumab therapy
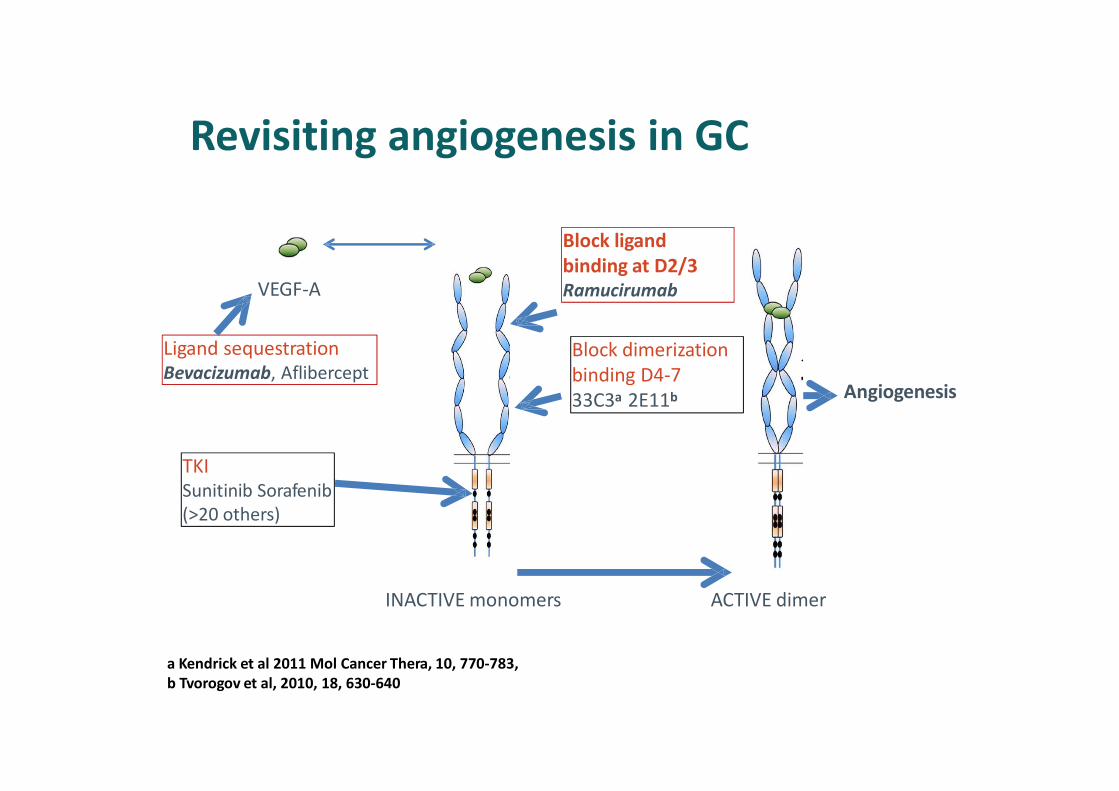
INACTIVE monomers ACTIVE dimer
VEGF-A
Ligand sequestration
Bevacizumab, Aflibercept
Block ligand
binding at D2/3
Ramucirumab
Block dimerization
binding D4-7
33C3a 2E11b
TKI
Sunitinib Sorafenib
(>20 others)
Angiogenesis
a Kendrick et al 2011 Mol Cancer Thera, 10, 770-783,
b Tvorogov et al, 2010, 18, 630-640
Revisiting angiogenesis in GC
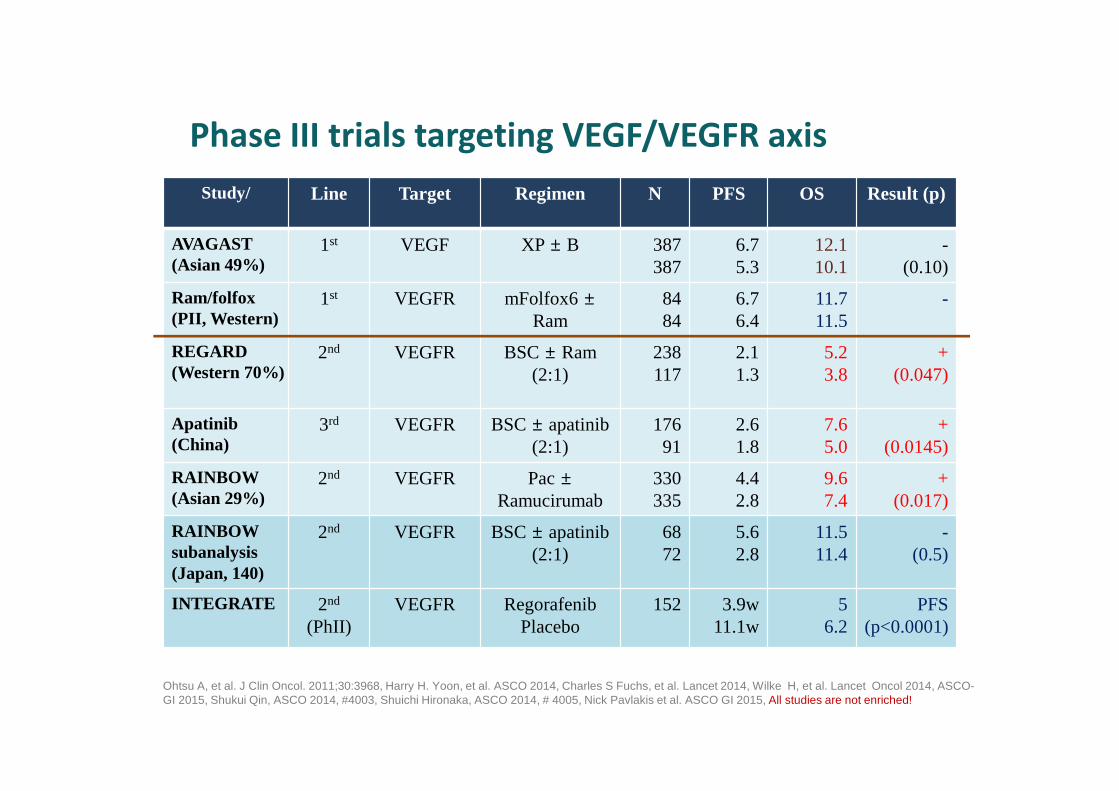
Study/ Line Target Regimen N PFS OS Result (p)
AVAGAST(Asian 49%)
1st VEGF XP ± B 387387
6.75.3
12.110.1
-(0.10)
Ram/folfox(PII, Western)
1st VEGFR mFolfox6 ±Ram
8484
6.76.4
11.711.5
-
REGARD(Western 70%)
2nd VEGFR BSC ± Ram(2:1)
238117
2.11.3
5.23.8
+(0.047)
Apatinib(China)
3rd VEGFR BSC ± apatinib(2:1)
17691
2.61.8
7.65.0
+(0.0145)
RAINBOW(Asian 29%)
2nd VEGFR Pac ±Ramucirumab
330335
4.42.8
9.67.4
+(0.017)
RAINBOW subanalysis(Japan, 140)
2nd VEGFR BSC ± apatinib(2:1)
6872
5.62.8
11.511.4
-(0.5)
INTEGRATE 2nd
(PhII) VEGFR Regorafenib
Placebo152 3.9w
11.1w5
6.2PFS
(p<0.0001)
Ohtsu A, et al. J Clin Oncol. 2011;30:3968, Harry H. Yoon, et al. ASCO 2014, Charles S Fuchs, et al. Lancet 2014, Wilke H, et al. Lancet Oncol 2014, ASCO-GI 2015, Shukui Qin, ASCO 2014, #4003, Shuichi Hironaka, ASCO 2014, # 4005, Nick Pavlakis et al. ASCO GI 2015, All studies are not enriched!
Phase III trials targeting VEGF/VEGFR axis

RAM+PTX RAM mono100
90
80
70
60
50
40
30
20
10
00 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Ramucirumab+paclitaxel
Placebo+paclitaxel
Censored
No. at riskRamuciruamb+ paclitaxel
Placebo+ paclitaxel
330 308 267 228 185 148 116 78 60 41 24 13 6 1 0
335 294 241 180 143 109 81 64 47 30 22 13 5 2 0
Time from randomization (months)
(%)
Overall survival
Censored
(%)
No. at riskRamucirumab
Placebo
238 154 92 49 17 7 3 0 0
117 66 34 20 7 4 2 1 0
Time (months)
Overall survival
PlaceboRamucirumab
100
80
60
40
20
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 26 27 28
Wilke H, et al: Lancet Oncol 15: 1224-1235, 2014 Fuchs CS, et al: Lancet 383: 31-39, 2014
(RAINBOW study) (REGARD study)
Ramucirumab 9.6 monPlacebo 7.4 mon
HR=0.807 [0.678-0.962]P=0.017
Ramucirumab 5.2 monPlacebo 3.8 mon
HR=0.776 [0.603-0.998]P=0.047
Prolonged survival in two Phase III studies
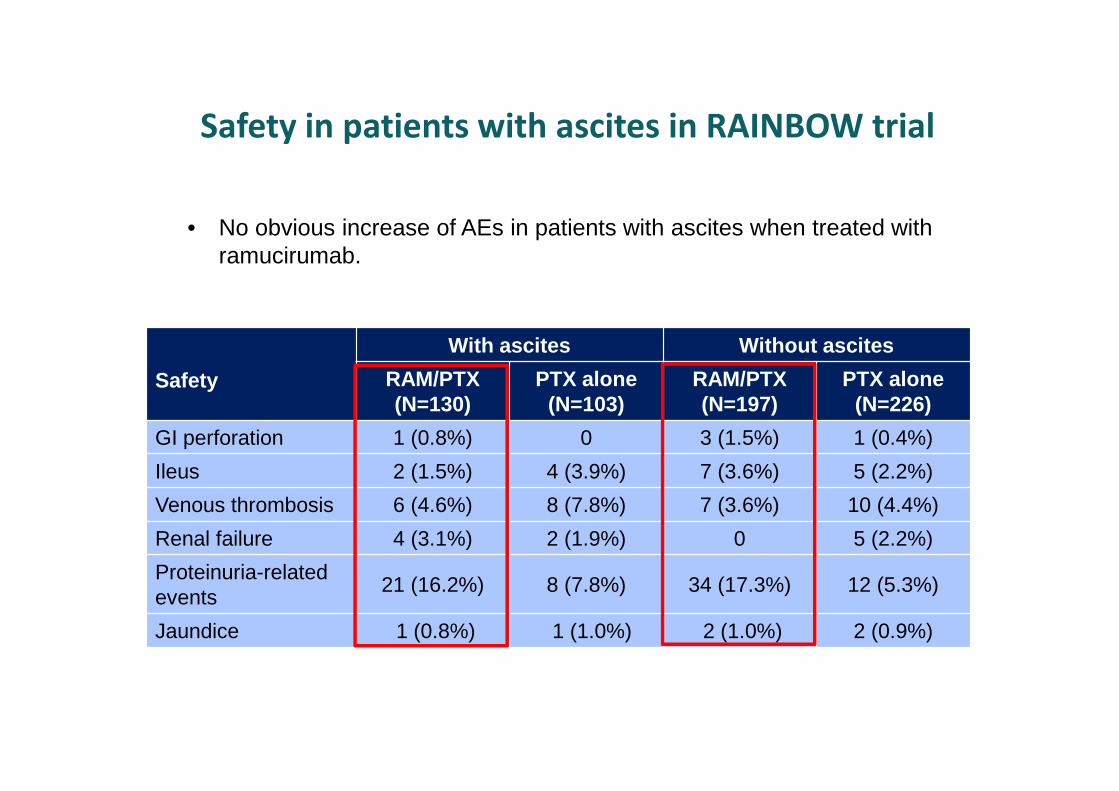
• No obvious increase of AEs in patients with ascites when treated with ramucirumab.
Safety
With ascites Without ascites
RAM/PTX(N=130)
PTX alone(N=103)
RAM/PTX(N=197)
PTX alone(N=226)
GI perforation 1 (0.8%) 0 3 (1.5%) 1 (0.4%)
Ileus 2 (1.5%) 4 (3.9%) 7 (3.6%) 5 (2.2%)
Venous thrombosis 6 (4.6%) 8 (7.8%) 7 (3.6%) 10 (4.4%)
Renal failure 4 (3.1%) 2 (1.9%) 0 5 (2.2%)
Proteinuria-related events
21 (16.2%) 8 (7.8%) 34 (17.3%) 12 (5.3%)
Jaundice 1 (0.8%) 1 (1.0%) 2 (1.0%) 2 (0.9%)
Safety in patients with ascites in RAINBOW trial
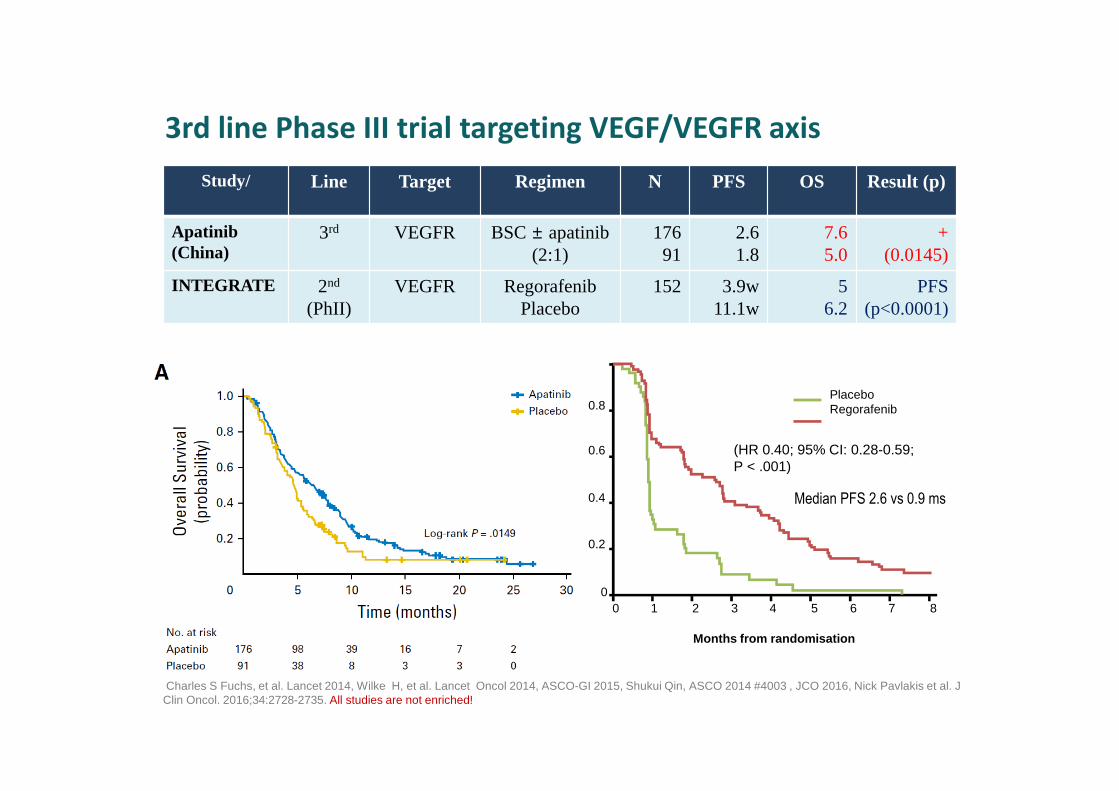
Study/ Line Target Regimen N PFS OS Result (p)
Apatinib(China)
3rd VEGFR BSC ± apatinib(2:1)
17691
2.61.8
7.65.0
+(0.0145)
INTEGRATE 2nd
(PhII) VEGFR Regorafenib
Placebo152 3.9w
11.1w5
6.2PFS
(p<0.0001)
Charles S Fuchs, et al. Lancet 2014, Wilke H, et al. Lancet Oncol 2014, ASCO-GI 2015, Shukui Qin, ASCO 2014 #4003 , JCO 2016, Nick Pavlakis et al. J Clin Oncol. 2016;34:2728-2735. All studies are not enriched!
3rd line Phase III trial targeting VEGF/VEGFR axis
0.8
0.6
0.4
0.2
00 1 2 3 4 5 6 7 8
Months from randomisation
PlaceboRegorafenib
(HR 0.40; 95% CI: 0.28-0.59; P < .001)
Median PFS 2.6 vs 0.9 ms

LBA43: Randomized phase 3 ANGEL study of rivoceranib (apatinib) + best supportive care (BSC) vs placebo + BSC in patients with advanced/metastat ic gastric cancer who failed ≥2 prior chemotherapy regimens – Kang Y-K, et al
Study objective• To investigate the efficacy and safety of rivoceranib (apatinib) + BSC in patients with previously treated advanced or
metastatic gastric cancer
Kang Y-K, et al. Ann Oncol 2019;30(suppl):abstr LBA43
PRIMARY ENDPOINT• OS
R2:1
PD*/toxicity
Stratification• Geographic region (Asia vs. North America/Europe)• Disease measurability• Prior ramucirumab use• Line of therapy (3L vs. ≥4L)
Rivoceranib 700 mg/day po+ BSC (n=308)Key patient inclusion criteria
• Advanced/metastatic gastric or GEJ cancer
• Failed ≥2 prior lines of chemotherapy
• ECOG PS ≤1
(n=460) PD/toxicity
Placebo + BSC (n=152)
SECONDARY ENDPOINT
• PFS, ORR, DCR, QoL, safety
*Patients permitted to continue treatment beyond PD at the investigators’ discretion

LBA43: Randomized phase 3 ANGEL study of rivoceranib (apatinib) + best supportive care (BSC) vs placebo + BSC in patients with advanced/metastat ic gastric cancer who failed ≥2 prior chemotherapy regimens – Kang Y-K, et al
Key results
Kang Y-K, et al. Ann Oncol 2019;30(suppl):abstr LBA43
OS
Time from randomisation, months
Sur
viva
l pro
babi
lity
100
80
60
40
20
00 3 6 9 12 15 2418 21
Rivo 308 239 8 5143 74 32 16 1
Placebo 152 108 5 262 30 16 6 0
No. at risk
Median follow-
up, mo
Pts with event,
n (%) mOS, mo
HR
(95%CI) p-value
Rivoceranib 13.7 250 (81.2) 5.8 0.93
(0.74, 1.15)0.4850
Placebo 12.1 119 (78.3) 5.1
5.8 months
5.1 months

RAMN=16
RAMN=80
PLN=5
PLN=46
Ove
rall
Surv
ival
(mon
ths)
HER2-NegativeHER2-Positive
• Patients with Her-2 positive or who received prior trastuzumab were not excluded
from REGARD and RAINBOW.
• REGARD: among 147 pts tested for Her-2 status, 21 were HER2+ve
-> 16 patients received Ram; no different efficacy of ram in HER2+ve patients
• RAINBOW: 39 out of 665 patients received 1st line trastuzumab
-> 20 in the ramucirumab plus paclitaxel arm; 19 in the paclitaxel arm
-> similar efficacy to Her-2 negative patients
OS by HER2 Status
RAMN=16
RAMN=80
PLN=5
PLN=46
Pro
gres
sion
-free
Sur
viva
l (m
onth
s)
HER2-NegativeHER2-Positive
RAM
N=16
PL
N=5
RAM
N=80
PL
N=46
RAM
N=16
PL
N=5
RAM
N=80
PL
N=46
(Fuchs CS et al. ASCO 2015. Abastrct 4029)
PFS by HER2 Status
Ramucirumab as a 2nd line Tx in Her-2 + GC?

HER2+ve: OS 8.6 months, PFS 3.7 months
could be considered as future reference for 2nd line studies in HER2+ve GC
Jung et at. Gastric Cancer 2018
P=0.605P=0.321
Korean EAP evidence with Ram+ Paclitaxel (N=228, 14% (n=32) Her-2 +)

Dynamic changes in HER2 expression
HER status changes post trastuzumab therapy
22 pairs pre and post treatment biopsies.
7/22 (32%) HER2 negative following treatment.
More common in IHC2+ vs IHC3+ !
Pietrantonio et al, Int J Cancer. 2016 Dec 15;139(12):2859-2864.
Janjigian et al, ESMO 2016
Continue anti-her-2 treatment in Her-2 + GC?
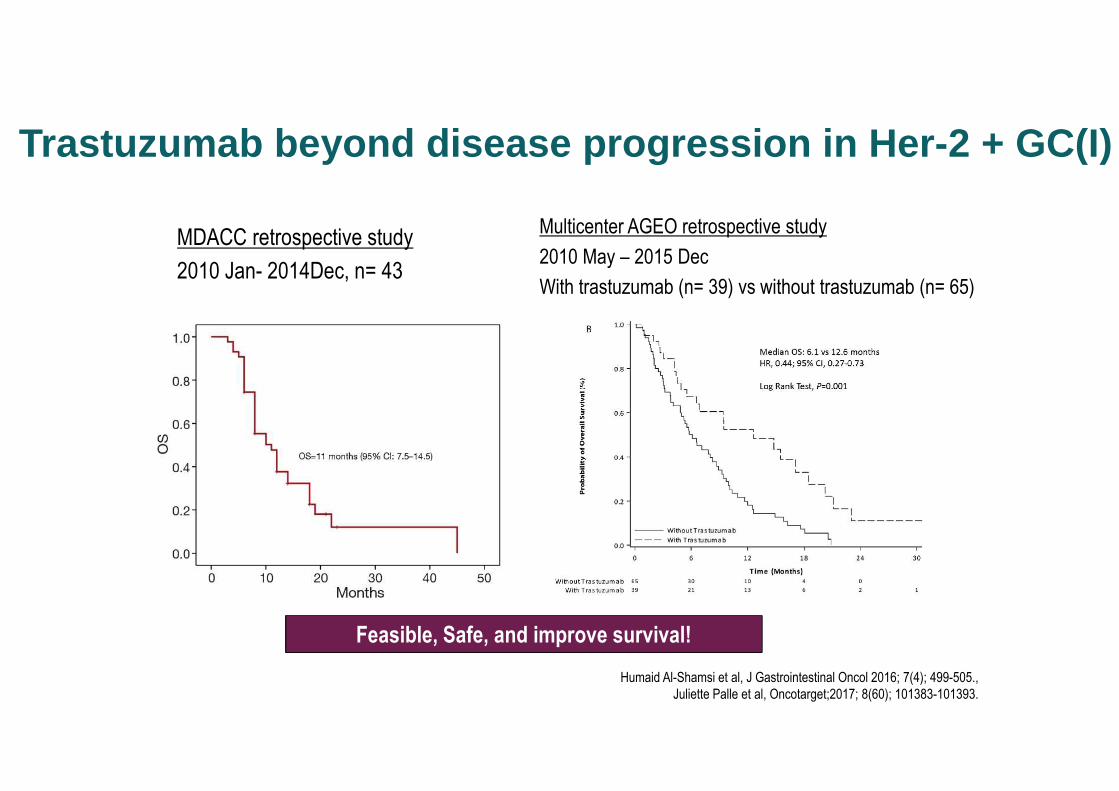
MDACC retrospective study
2010 Jan- 2014Dec, n= 43
Humaid Al-Shamsi et al, J Gastrointestinal Oncol 2016; 7(4); 499-505.,
Juliette Palle et al, Oncotarget;2017; 8(60); 101383-101393.
Feasible, Safe, and improve survival!
Trastuzumab beyond disease progression in Her-2 + GC(I)
Multicenter AGEO retrospective study
2010 May – 2015 Dec
With trastuzumab (n= 39) vs without trastuzumab (n= 65)

Chinese 3 sites retrospective study
2012 Sep – 2015 Oct
With trastuzumab (n= 32) vs without trastuzumab (n= 27)
Qian Li et al., Oncotarget 2016;7(31); 50656-50665.
Feasible, Safe, and improve survival!
Trastuzumab beyond disease progression in Her-2 + GC(II)

Chaganty et al. Cancer Letters; 43:47, 2018, Ott PA, et al. Front Oncol 2015;5:202, Motz GT et al. Nat Rev Immunol. 2011:11:702, Huang Y et al. Blood. 2007;110:624.
Crosstalk between cancer cells – endothelial cells – immune suppression
Trastuzumab
IO: Nivolumab/Pembrolizumab etc.
� Promotes inhibitory immune cells
• Tregs
• MDSCs
• TAMs
� Compromises APC and T effector cell function
� Impairs lymphocyte development and trafficking
Currently, 2nd line phase Ib/II trial with Paclitaxel + Ramucirumab + Trastuzumab
combination at YCC
Dual blocking tumor with
oncogenic driver and
angiogenesis
Dual blocking Immune
suppressive aniogenesis and
immune checkpoints
(Ramucirumab + Pembrolizumab)
Dual blocking tumor with oncogenic driver and immune checkpoints?
-> YCC 1st line PANTHERA trial (HXP + pembrolizumab), MSKCC, KN 811 tria
Ramucirumab

� New agents in development
• New agents targeting known targets: Her-2, MET, FGFR, angiogenesis
• Ab-drug conjugates
• DDR targeting in combination with IOs
• GS-5745 (MMP-9 inhibitor)
• Napabucasin(BBI608) – stemness inhibitor
• IMAB362: Anti-CLDN18.2 antibody
• Anetumab- targeting mesothelin
• CDK4/6 inhibitors
• Epigenetics modulators: BET inhibitor
• TGF-b inhibitor
• Etc …
• Immunotherapy
� Proper patients selection: Precision Medicine



















