Biofuel: An Alternative Energy Source - COSMOS - Home
12
Review Trial Designs for Personalizing Cancer Care: A Systematic Review and Classification Parvin Tajik 1,2 , Aleiko H. Zwinderman 1 , Ben W. Mol 2 , and Patrick M. Bossuyt 1 Abstract There is an increasing interest in the evaluation of prognostic and predictive biomarkers for personalizing cancer care. The literature on the trial designs for evaluation of these markers is diverse and there is no consensus in the classification or nomenclature. We set this study to review the literature systematically, to identify the proposed trial designs, and to develop a classification scheme. We searched MEDLINE, EMBASE, Cochrane Methodology Register, and MathSciNet up to January 2013 for articles describing these trial designs. In each eligible article, we identified the trial designs presented and extracted the term used for labeling the design, components of patient flow (marker status of eligible participants, intervention, and comparator), study questions, and analysis plan. Our search strategy resulted in 88 eligible articles, wherein 315 labels had been used by authors in presenting trial designs; 134 of these were unique. By analyzing patient flow components, we could classify the 134 unique design labels into four basic patient flow categories, which we labeled with the most frequently used term: single-arm, enrichment, randomize-all, and biomarker-strategy designs. A fifth category consists of combinations of the other four patient flow categories. Our review showed that a considerable number of labels has been proposed for trial designs evaluating prognostic and predictive biomarkers which, based on patient flow elements, can be classified into five basic categories. The classification system proposed here could help clinicians and researchers in designing and interpreting trials evaluating predictive biomarkers, and could reduce confusion in labeling and reporting. Clin Cancer Res; 19(17); 1–11. Ó2013 AACR. Introduction Recent progress in understanding the molecular basis of cancer has redefined the landscape for achieving stratified and personalized medicine for patients with cancer. Ongo- ing efforts concentrate on the translation of these molecular insights into biomarkers that can reliably guide application of existing and new cancer treatments. Biomarkers that are informative for selecting treatment can be broadly classified as prognostic or predictive bio- markers. Prognostic biomarkers classify patients treated with standard therapies—including no treatment, if that is standard practice—into subgroups with distinct expected clinical outcomes. Predictive biomarkers identify patients whose tumors are likely to be sensitive or resistant to a specific agent (1). Valid and definitive evidence showing the clinical use of these biomarkers can be obtained by conducting well-designed clinical trials with adequate sam- ple size (1–3). These clinical trials are planned to evaluate biomarker-based treatment strategies. Their design often differs from the more conventional comparative clinical trials of interventions. Following the recent dramatic devel- opments in the technologies for identifying potential novel biomarkers and the huge increase in the number of claimed biomarkers, there has also been a great expansion in the number of trial designs proposed for validation of biomar- kers for treatment selection purposes. A rapid review of the biomarker trial designs in the oncology literature suggests substantial variability in the designs, as well as in the terms proposed by authors for labeling them. This makes retrieval, interpretation, com- parison, and critical appraisal of these types of studies complicated for consumers of trial results, who can be practicing physicians, researchers, or policymakers. The variability in labeling is a phenomenon typical for many rapidly developing areas of science. However, now that the field is maturing, and experts in other fields of medicine, such as cardiovascular diseases and infectious diseases, have started to apply the methodologic achievements of the oncology biomarker trials, it is time for harmonizing the terminologies in use and framing a classification of the designs. A harmonized terminology for describing bio- marker clinical trials and a simple classification scheme may help in speeding up the translation process of the Authors' Affiliations: Departments of 1 Clinical Epidemiology, Biostatistics and Bioinformatics and 2 Obstetrics and Gynaecology, Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). Corresponding Author: Parvin Tajik, Department Clinical Epidemiology, Biostatistics and Bioinformatics, Academic Medical Center, University of Amsterdam, Room J1b-210, PO Box 22700, 1100 DE Amsterdam, the Netherlands. Phone: 31-20-56-66-877; Fax: 31-20-69-12-683; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-12-3722 Ó2013 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org OF1 Research. on April 13, 2019. © 2013 American Association for Cancer clincancerres.aacrjournals.org Downloaded from Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722
Transcript of Biofuel: An Alternative Energy Source - COSMOS - Home

Review
Trial Designs for Personalizing Cancer Care: A SystematicReview and Classification
Parvin Tajik1,2, Aleiko H. Zwinderman1, Ben W. Mol2, and Patrick M. Bossuyt1
AbstractThere is an increasing interest in the evaluation of prognostic and predictive biomarkers for personalizing
cancer care. The literature on the trial designs for evaluation of these markers is diverse and there is no
consensus in the classification or nomenclature. We set this study to review the literature systematically, to
identify the proposed trial designs, and todevelop a classification scheme.We searchedMEDLINE, EMBASE,
Cochrane Methodology Register, and MathSciNet up to January 2013 for articles describing these trial
designs. In each eligible article, we identified the trial designs presented and extracted the term used for
labeling the design, components of patient flow (marker status of eligible participants, intervention, and
comparator), study questions, and analysis plan. Our search strategy resulted in 88 eligible articles, wherein
315 labels had been used by authors in presenting trial designs; 134 of these were unique. By analyzing
patient flow components, we could classify the 134 unique design labels into four basic patient flow
categories, which we labeled with the most frequently used term: single-arm, enrichment, randomize-all,
and biomarker-strategy designs. A fifth category consists of combinations of the other four patient flow
categories. Our review showed that a considerable number of labels has been proposed for trial designs
evaluating prognostic and predictive biomarkers which, based on patient flow elements, can be classified
into five basic categories. The classification system proposed here could help clinicians and researchers in
designing and interpreting trials evaluating predictive biomarkers, and could reduce confusion in labeling
and reporting. Clin Cancer Res; 19(17); 1–11. �2013 AACR.
IntroductionRecent progress in understanding the molecular basis of
cancer has redefined the landscape for achieving stratifiedand personalized medicine for patients with cancer. Ongo-ing efforts concentrate on the translation of thesemolecularinsights into biomarkers that can reliably guide applicationof existing and new cancer treatments.Biomarkers that are informative for selecting treatment
can be broadly classified as prognostic or predictive bio-markers. Prognostic biomarkers classify patients treatedwith standard therapies—including no treatment, if that isstandard practice—into subgroups with distinct expectedclinical outcomes. Predictive biomarkers identify patientswhose tumors are likely to be sensitive or resistant to aspecific agent (1). Valid and definitive evidence showing
the clinical use of these biomarkers can be obtained byconducting well-designed clinical trials with adequate sam-ple size (1–3). These clinical trials are planned to evaluatebiomarker-based treatment strategies. Their design oftendiffers from the more conventional comparative clinicaltrials of interventions. Following the recent dramatic devel-opments in the technologies for identifying potential novelbiomarkers and the huge increase in the number of claimedbiomarkers, there has also been a great expansion in thenumber of trial designs proposed for validation of biomar-kers for treatment selection purposes.
A rapid review of the biomarker trial designs in theoncology literature suggests substantial variability in thedesigns, as well as in the terms proposed by authors forlabeling them. This makes retrieval, interpretation, com-parison, and critical appraisal of these types of studiescomplicated for consumers of trial results, who can bepracticing physicians, researchers, or policymakers. Thevariability in labeling is a phenomenon typical for manyrapidly developing areas of science. However, now that thefield is maturing, and experts in other fields of medicine,such as cardiovascular diseases and infectious diseases,have started to apply the methodologic achievements ofthe oncology biomarker trials, it is time for harmonizingthe terminologies in use and framing a classification of thedesigns. A harmonized terminology for describing bio-marker clinical trials and a simple classification schememay help in speeding up the translation process of the
Authors' Affiliations: Departments of 1Clinical Epidemiology, Biostatisticsand Bioinformatics and 2Obstetrics and Gynaecology, Academic MedicalCenter, University of Amsterdam, Amsterdam, the Netherlands
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Parvin Tajik, Department Clinical Epidemiology,Biostatistics and Bioinformatics, Academic Medical Center, University ofAmsterdam, Room J1b-210, PO Box 22700, 1100 DE Amsterdam, theNetherlands. Phone: 31-20-56-66-877; Fax: 31-20-69-12-683; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-12-3722
�2013 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org OF1
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

biomarker findings and could assist in paving the way formaking personalized medicine a reality.
Here, we report on a systematic review of literature ontrial designs for evaluating biomarkers for treatment selec-tion. The review is based on a comprehensive and system-atic search in multiple databases. We propose a classifica-tion scheme based on the flowof patients in these trials. Theclassification system is presented using recent biomarkerclinical trials in oncology as examples, along with the mainquestions each category of designs can answer.
Materials and MethodsLiterature search
We searched MEDLINE, EMBASE, Cochrane Methodol-ogy Register, and MathSciNet up to 15 January 2013, andhand searched references and cited articles of all includedstudies using theWeb of Science database. The search filtersthat we developed and used in collaboration with a clinicallibrarian are presented in the Supplementary Materials andMethods. Eligible for inclusion were methodologic articlesthat described one or more trial designs for identificationand/or validationof prognostic or predictive biomarkers fortreatment selection. The searchwas not limited to oncology.No language restrictions were applied.
One author (P. Tajik) independently identified poten-tially eligible articles by reading titles and abstracts, whereasa second author (P.M. Bossuyt) independently screened arandom sample of 400 abstracts to ensure that no abstractsweremissed. Therewas a 99%agreement on the selection ofabstracts and disagreements were resolved in consensusdiscussions. Thereafter, full text copies of all potentiallyeligible articles were obtained and read in full. Articles wereincluded if they satisfied the inclusion criteria.
Data extractionFrom all included articles and for each proposed trial
design, we extracted detailed data on the proposed designlabel, trial objectives, patient flow elements, and the analysisplan. Our definition of patient flow is composed of the bio-markerstatusofparticipantsdeemedeligible for thestudy, theintervention participants are assigned to (whether or notbiomarker status is used for assigning study participants tothe experimental treatment) and the comparator (standardtreatment or both standard and experimental treatments).
AnalysisWe started our analysis by developing the list of study
labels from all included studies. For each label in the list, weexplored the participant–intervention–comparator compo-nents of patient flow.We then clustered all study labels withidentical components into disjoint categories. The mostcommonly used label for describing designs of each cate-gory was selected for labeling the corresponding category.
ResultsSearch results
Our initial search yielded 2,506 abstracts, of which 136were deemed eligible based on title and abstract. After
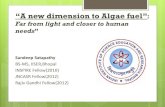
assessing the full texts of these 136 articles, 71 wereincluded. Seventeen other articles were added by handsearching references and citing articles, resulting in atotal of 88 articles in the final analysis (SupplementaryTable S1). A summary of the search process is outlinedin Fig. 1.
Trial design labelsFrom the included articles, we could extract 315 design
labels. The identified labels and the definitions as pre-sented in the studies are listed in the SupplementaryTable S2. By analyzing the extracted labels along withtheir patient flow components, we found 134 uniquecombinations of label and patient flow elements. Therewere many trial designs with the very same patientflow elements, which had received different labels. Therewere also a few labels used for describing designs withcompletely different patient flows. The 134 unique labeland patient flow combinations are presented in Table 1.By comparing the patterns of all the included designs,we could distinguish four basic and distinct patientflow categories, as well as a fifth category, consisting ofcombinations of two or more of the four basic patientflow elements (Table 1). In a later section, we discussthese categories in more detail.
CCR Reviews
© 2013 American Association for Cancer Research
Databases searched using keywords
Abstracts read and 136 found to be relevant
2,056 Abstracts identified 1680 PubMed
1313 EMBASE
141 Cochrane Methodology Register
126 MathSciNet
Papers obtained and read in full.
Did they present a trial design for evaluating
markers for treatment selection?
Yes
71 articles
88 Articles
No
65 articles
Reference and citation
checks, plus internet
searches (17 articles)
Figure 1. Flow chart of search results.
Tajik et al.
Clin Cancer Res; 19(17) September 1, 2013 Clinical Cancer ResearchOF2
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

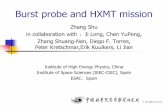
Trial design categoriesTo ease the presentation, we present the flow elements for
two treatment options, labeled as experimental (Exp) andcontrol (Ctrl), in the presence of a single, binary biomarker(Fig. 2). However, the flow diagrams are generalizable toconditions with more than two treatment options and inwhich the biomarker hasmore than two levels, or is numer-ic. For sake of simplicity and consistency, we define bio-marker positivity as the biomarker status that is associatedwith a better outcome on the experimental treatment.Therefore, in cases where overexpression of the biomarkeris associated with a worse response to treatment, we con-sider the normal expression as biomarker-positive andoverexpression as biomarker-negative.Single-arm. In single-arm trials, all patients, irrespective
of their biomarker status, are included in the trial and allundergo the experimental treatment (Fig. 2A; refs. 4–8).This trial has no control group, and no random assignment.Enrichment. With an enrichment design, all potentially
eligible patients are first tested for the biomarker and onlybiomarker-positives are randomly assigned to the experi-mental or control treatment. Other patients are in principleexcluded from further investigation in the study (Fig. 2B).We found12 labels for describing this design,whichwere allinterchangeable and referred to the main feature of thedesign: biomarker status performs as a key trial eligibilitycriterion (Table 1).The pivotal trial for trastuzumab is a well-known example
of an enrichment design (9). Patients with HER2-positivebreast adenocarcinoma were enrolled and randomly allo-cated to chemotherapy with or without trastuzumab. Thisstudy provided strong evidence that trastuzumab combinedwith chemotherapy improves outcomes among womenwith HER2-positive breast cancer.Randomize-all. In designs in the randomize-all catego-
ry, all patients meeting the trial eligibility criteria, irrespec-tive of their biomarker status, are randomly allocated toeither experimental or control treatment. Thereafter, asso-ciations between biomarker status and treatment responseare evaluated (Fig. 2C).Because its eligibility criteria is not restricted by biomark-
er status, it has commonly been labeled as "randomize-all"(2, 10–13), "all-comers" (14–18), or "untargeted" (19–22).The design is also called "traditional" (23–25) or "conven-tional" (1, 26) because it has the samepatient flow elementsas routine randomized controlled trials (RCT) for evaluat-ing treatment options. It is possible that researchers evaluatea biomarker retrospectively, using data and stored biospeci-mens collected in previously completed RCTs. In suchscenarios, trials are commonly labeled as "biomarker anal-ysis within an existing RCT" (18) or "prospective/retrospec-tive" (27). All these label variations mainly refer to thetiming of introducing the biomarker question to the trial.The type of randomization is another source of variability
in labeling of randomize-all trials. In cases where a simple1:1 randomization procedure is applied to all patients, trialsare labeled as "simple randomization" (28). However, incases where the biomarker under evaluation is binary or
categorical with few categories, randomization can be doneseparately for each biomarker category through stratifiedrandomization. Labels such as "biomarker-stratified" (29,30), "stratified randomized" (31), "non-targeted RCT (strat-ified by marker)" (32), "stratified analysis" (25), "stratifi-cation" (33, 34), and "separate randomization" (35) allrefer to this type of randomization. A special case of strat-ified randomization is when randomization is conductedbymeans of a Bayesian response-adaptive procedure, ratherthan a standard equal randomization procedure. The"Bayesian adaptive randomization design" by Zhou andcolleagues is an example (36). It has also been called"outcome-based adaptive randomization" (5, 37).
The next source of variability in labeling the trials in therandomize-all category is the trial’s statistical analysis plan.In many cases, authors have coined a design label forreferring to a randomize-all design when analyzed on thebasis of their novel analysis plan. Examples of such labelsare "biomarker analysis" (38), "sequential testing" (39),"prospective subset" (2), "adaptive threshold" (40), "adap-tive biomarker" (33), "adaptive signature" (41), "cross-validated adaptive signature" (42), and "generalized adap-tive signature" (33). All these designs have a randomize-allpatient flow structure, but they differ in their analysis plan.
The Sequential Tarceva in unresectable non–small celllung cancer (NSCLC) trial (SATURN; ref. 43) has beenlabeled as "prospective-subset design" (2). In the SATURNtrial, all eligible patients were randomly allocated to erlo-tinib or placebo plus standard supportive care. The trial hadtwo primary objectives: evaluating the effectiveness of erlo-tinib separately in all patients and in patients with EGFreceptor (EGFR) immunohistochemistry-positive tumors.To address the multiple comparisons issue, authors usedan a splitting technique; the a level of 5%was split betweenthe two primary objectives: 3% for all patients and 2%for patients with EGFR immunohistochemistry-positivetumors.
There are five "adaptive" designs in this category, whichare labeled after adaptive elements in their analysis plan.Each of these adaptive plans evaluates the efficacy ofexperimental treatment in all patients and, if not signifi-cant, tries to define a biomarker-defined subset that isresponsive to the experimental treatment. In settings wherea single continuous candidate biomarker is available butits positivity threshold is not predefined, adaptive thresh-old plans try to find such a threshold (40). Adaptivebiomarker designs have been proposed to evaluate mul-tiple binary biomarkers defined in advance (33). Adaptivesignature (41) and cross-validated adaptive signature (42)designs develop a predictive combination of biomarkers ina training set of the trial and consequently evaluate it in atest set. The proposed "generalized adaptive signaturedesign" uses a training set of the trial to select amongseveral candidate biomarkers and optimize cutoff points,and thereafter evaluates the selected biomarkers in a testset (33).
Biomarker-strategy. The distinguishing feature of designsin the biomarker-strategy category is the inclusion of a new
Trial Designs for Personalizing Cancer Care
www.aacrjournals.org Clin Cancer Res; 19(17) September 1, 2013 OF3
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

Tab
le1.
Patient
flow
elem
ents
oftheex
trac
teddes
ignlabelsfortria
lsev
alua
tingprogn
ostic
andpredictiv
ebiomarke
rs.L
abelsclus
teredinthe
samebulletdes
cribeiden
tical
triald
esigns
andareintercha
ngea
ble
Des
ignlabels
Patients
Interven
tion
Comparison
Patient
flow
category
*Single-arm
(4–8),un
controlledco
hortpha
rmac
ogen
etic
stud
y(50),
nonran
dom
ized
(34)
Mþ,M
�Exp
—1.
Single-arm
*Enrichm
ent(1,3,11
,15,16
,18,29
,33,37
,39,44
,48,61
–75
),targeted
(2,1
0–13
,15,
18,2
0,48
,64,
67,6
9,76
,77),e
nriche
d(23,
76),marke
ren
richm
ent(78),b
iomarke
r-en
richm
ent(56,
68),biomarke
ren
riche
d(14,
23,7
9,80
),biomarke
rse
lected
(79),e
fficien
ttargeted
(28),
clinicallyen
riche
d(79),selec
tion(2,1
0,81
),RCTof
testpos
itive
s(48),
screen
ingen
richm
ent(82)
Mþ
Exp
Std
2.Enrichm
ent
*Ran
dom
ize-all(2,
10–13
),trad
ition
al(23–
25),stan
dard(33),
conv
entio
nal(1,
26),simple
rand
omization(28),u
ntarge
ted
(19,
19–22
),un
selected
(18,
64),all-co
mers(14–
18),all-co
mers
(stratified
bymarke
rstatus
;ref.67
),includ
ingtest
nega
tives
and
pos
itive
s(73),tes
tasbas
elineinRCT(48),p
rosp
ectiv
e/retros
pec
tive
(27),b
iomarke
rana
lysis(30,38
),biomarke
rana
lysiswith
inan
existin
gRCT(18),con
trolledco
hortphrmac
ogen
eticstud
y(50),retrosp
ectiv
ebiomarke
r(79),ind
irect
predictiv
ebiomarke
r-bas
ed(46),h
ybrid
(77)
*Seq
uentialtes
tingstrategy
(16,
18)
*Prosp
ectiv
esu
bse
t(2)
*Adap
tivethresh
old(29,
64,7
6,78
),biomarke
radap
tivethresh
old(74)
*Adap
tivebiomarke
r(33)
*Adap
tivesign
ature(23,
41,44
,62,
67,69
,70,
83,84
),molec
ular
sign
ature(62),c
ross-validated
adap
tivesign
ature(42),g
eneralized
adap
tivesign
ature(33)
*Marke
rstratifi
ed(28),m
arke
r-stratifi
ed(16),b
iomarke
r-stratifi
ed(29,
30),biomarke
r-stratifi
edwith
fallbac
kan
alysis
(69),s
tratified
rand
omized
(31),s
eparaterand
omization(35),s
tratifica
tion(33,
34),
stratifi
ed(65),s
tratified
analys
is(25),n
ontargeted
RCT(stratified
bymarke
r;ref.32
),marke
rbytrea
tmen
tinteraction(30,
53),
marke
r-by-trea
tmen
tinteraction(8),trea
tmen
tbymarke
rinteraction
(3),trea
tmen
t-by-marke
rinteraction(64),m
arke
r�
trea
tmen
tinteraction(85),interac
tion(10),treatmen
t-marke
rinteraction(11)
*Outco
me-bas
edad
aptiv
erand
omization(5,3
6),a
dap
tive
rand
omization(15,76
,86),B
ayes
ianad
aptiv
e(68),B
ayes
ianad
aptiv
erand
omization(2,2
8,62
),co
mbined
dyn
amic
multia
rm(80)
Mþ,M
�Exp
Std
3.Ran
dom
ize-all
(Con
tinue
don
thefollo
wingpag
e)
Tajik et al.
Clin Cancer Res; 19(17) September 1, 2013 Clinical Cancer ResearchOF4
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

Tab
le1.
Patient
flow
elem
ents
oftheex
trac
teddes
ignlabelsfortria
lsev
alua
tingprogn
ostic
andpredictiv
ebiomarke
rs.L
abelsclus
teredin
the
samebulletdes
cribeiden
tical
triald
esigns
andareintercha
ngea
ble
(Con
t'd)
Des
ignlabels
Patients
Interven
tion
Comparison
Patient
flow
category
*Biomarke
r-strategy
,with
biomarke
ras
sessmen
tin
theco
ntrola
rm(1),marke
rstrategy
(33,
82,8
5),b
iomarke
r-strategy
(15,
38,4
4),
biomarke
r-strategy
(23),s
trateg
y(13),m
arke
r-bas
edstrategy
(3,3
0,45
,53,
61,7
6,87
),marke
r-bas
ed(39),ran
dom
disclos
ure(48),
custom
ized
(12),p
arallelc
ontrolledphrmac
ogen
etic
stud
y(50),
marke
r-bas
edstrategy
des
ignI(45
),strategy
(13),c
lassifier
rand
omizationdes
ign(49),b
iomarke
r-gu
ided
(47),ind
ividua
lprofile
(10),b
iomarke
r-bas
edas
sign
men
tof
spec
ificdrugtherap
y(62)
*Seq
uentialb
efore–
afterpha
rmac
ogen
etic
diagn
ostic
stud
y(50)
Mþ,M
�M-bas
edstrategy
Std
4.Biomarke
r-strategy
a.With
biomarke
ras
sess
men
tin
theco
ntrola
rm
*Biomarke
r-strategy
with
outb
iomarke
rass
essm
entintheco
ntrolarm
(1),biomarke
r-strategy
des
ignwith
stan
dardco
ntrol(2),d
irect
predictiv
ebiomarke
r-bas
ed(46),R
CTof
testing(48),tes
t-trea
tmen
t(51),p
arallelc
ontrolledpha
rmac
ogen
etic
diagn
ostic
stud
y(50),
marke
rstrategy
(28,
33,7
0),m
arke
r-bas
edwith
norand
omizationin
theno
nmarke
r-bas
edarm
(35),c
lass
ical
(48),tria
lsof
asing
letests/co
mparingtw
ostrategies
(22)
Unk
nown
M-bas
edstrategy
Std
b.W
ithou
tbiomarke
ras
sess
men
tin
theco
ntrola
rm
*Mod
ified
marke
r-bas
edstrategy
(31,
33,5
3,68
),biomarke
r-strategy
with
rand
omized
control(2),m
arke
r-bas
eddes
ignwith
rand
omizationin
theno
nmarke
r-bas
edarm
(35),m
arke
r-bas
edstrategy
des
ignII(45),m
arke
r-strategy
(28),a
ugmen
tedstrategy
(13)
Mþ,M
�M-bas
edstrategy
Exp
,Std
c.With
trea
tmen
trand
omization
intheco
ntrola
rm
*Com
binationof
biomarke
rtriald
esigns
(1)
*Hyb
rid(18,
37,7
6,88
)*
Interm
ediate
riskrand
omized
(2),tw
o-way
stratifi
ed(49,
89),mod
ified
marke
rstrategy
(33)
*Disco
rdan
tris
krand
omization(2),discrep
antca
serand
omized
(31),
disco
rdan
ttest
resu
ltsRCT(48)
*Tw
o-stag
esa
mple-enrichm
ent(54),two-stag
een
richm
ent(16)
*Ta
ndem
two-step
pha
seIIpredictormarke
rev
alua
tion(60),tan
dem
two-step
pha
seIIpredictorb
iomarke
reva
luation(7),tand
emtw
ostep
(2,7
),tand
emtw
ostag
e(2),ad
aptiv
e(16,
23,67
,90)
*Adap
tivepatient
enric
hmen
t(55),a
dap
tiveac
crua
l(18
,37,
78),
adap
tiveac
crua
lbas
edon
interim
analys
is(64),a
dap
tivemod
ifying
types
ofpatientsac
crue
d(33)
*Adap
tiveparallelS
imon
two-stag
e(88),b
iomarke
r-ad
aptiv
eparallel
two-stag
e(7),ad
aptiv
eparallel(2),two-stag
eBay
esian(63)
*Bay
esianco
varia
tead
justed
resp
onse
-adap
tive(BCARA)
rand
omization(91)
*Adap
tive(16,
23,62
,67,
69),ad
aptiv
ean
alys
is(39),a
dap
tive
biomarke
rdriv
en(14),m
ultia
rmmultis
tage
(67)
5.Com
binationof
patient
flow
catego
ries
Trial Designs for Personalizing Cancer Care
www.aacrjournals.org Clin Cancer Res; 19(17) September 1, 2013 OF5
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

management strategy. This strategy is not the standard orexperimental treatment, but a prespecified maker-basedtreatment strategy. For example, biomarker-positive patientswould receive experimental therapy, whereas all biomarker-negative patients get standard of care. Eligible patients arerandomized to this biomarker-based treatment strategy or tocontrol treatment. In our review, we could identify threesubtypes of this category.
Biomarker-strategy, with biomarker assessment in the controlarm. Biomarker status is assessed in all patients enrolledin the trial, who are then randomly allocated to either thebiomarker-strategy arm or to standard treatment (ref. 1; Fig.2D). Some other labels for this design type were biomarker-strategy (15, 38, 44), "marker-based strategy I" (45), "cus-
tomized strategy" (12), "direct predictive biomarker-based"(46), and "biomarker-guided" (47). There were also otherlabels in use, such as "random disclosure" (48), "classifierrandomization" (49), or "parallel controlled phrmacoge-netic study" (50).
Biomarker-strategy, without biomarker measurement in thecontrol arm. In settings where it is not feasible or ethicalto evaluate the biomarker in all patients, biomarker statusis only acquired in patients allocated to the biomarker-strategy arm (Fig. 2E). This design is also labeled as"biomarker-strategy with standard control" (2), "directpredictive biomarker-based" (46), "RCT of testing" (48),"test-treatment" (51), or "parallel controlled pharmaco-genetic diagnostic study" (50).
Biomarker-strategy, with treatment randomization in thecontrol arm. Sargent and Allegra (52) have proposed amodification of the biomarker-strategy design, wherein asecond randomization between experimental versus con-trol therapy replaces the control arm (Fig. 2F). They calledit "modified marker-based strategy" design (53). Someother authors referred to the design as "marker-basedstrategy design II" (45), "augmented strategy" (13), orsimply "marker-strategy" (28).
Combination of patient flows. A final, fifth categoryconsists of trial designs in which two or more of theaforementioned basic patient flow structures are combinedto form a new design. Combination of designs is usuallyrequired when the trial aims at evaluating multiple hypoth-eses,multiple biomarkers,multiple treatments, or when thetrial has several stages. Freidlin and colleagues have simi-larly proposed a category called "combination of biomarkertrial designs" in a comparable review of study designs (1).
The simplest combination is when in enrichment trialsbiomarker-negative patients are not excluded from thestudy but assigned to control treatment(s) for which theoutcomes are assessed. Here, an enrichment flow is com-bined in parallel with a single-arm trial of standard therapyin biomarker-negative patients. Most authors have referredto this flow as "hybrid" design. An example of a hybriddesign is the Trial Assigning Individualized Options forTreatment (TAILORx). The study was designed to evaluateOncotype Dx, a 21-gene recurrence score, in tamoxifen-treated patients with breast cancer. In this trial, patientsare divided into three subgroups of low, intermediate, andhigh risk based on their OncotypeDx recurrence score. Low-risk patients receive hormonal therapy, high-risk patientsreceive both hormonal and chemotherapy, whereas pati-ents at intermediate risk are randomized to hormonaltherapy or chemotherapy plus hormonal therapy. This trialis a parallel combination of enrichment trial in intermedi-ate-risk group and two single-arm trials in the low- andhigh-risk groups. Other labels used for this design are"intermediate risk randomized" (2) or "two-way stratified"(49) design.
The Microarray In Node-negative Disease may AvoidChemoTherapy (MINDACT) trial also has an enrichmentelement in its patient flow. Here, patients with discordantrisk estimations by tumor’s clinicopathologic features and a
CCR Reviews
© 2013 American Association for Cancer Research
Exp
Exp
Ctrl
A
BR
Exp
Ctrl
R
Exp
Ctrl
Ctrl
R
M�
M�
M�
M�
C Testbiomarker
M-basedstrategy
Biomarker-based strategy
Control strategy
D Testbiomarker
Exp
Ctrl
Exp
Ctrl
R
R
M�
M�
Control strategy
F Testbiomarker
Exp
Ctrl
Ctrl
R
M�
M�
Control strategy
E
Testbiomarker
Biomarker-based strategy
Testbiomarker
Testbiomarker
Figure 2. The main types of patients' flow in RCTs for evaluation ofprognostic and prediction biomarkers: (A) single-arm; (B) enrichment;(C) randomize-all; (D) biomarker-strategywith biomarkermeasurement inthe control arm; (E) biomarker-strategy without biomarker measurementin the control arm; (F) biomarker-strategywith treatment randomization inthe control arm [Marker (M), biomarker under evaluation].
Tajik et al.
Clin Cancer Res; 19(17) September 1, 2013 Clinical Cancer ResearchOF6
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

70-gene signature (MammaPrint) are eligible for random-ization. Patients with concordant risk estimations receivecontrol treatment. Consenting discordant patients are ran-domized to treatment determined on the basis of theclinocopathologic risk category versus MammaPrint riskcategory. This way, theMINDACT is a trial combining threeflow types: enrichment, single-arm, andbiomarker-strategy.This combination has been described in the literature as"discrepant case randomization" (31), "discordant riskrandomization" (2), and "discordant test results RCT"(48). Simon refers to this trial as a modified marker-basedstrategy (33), as only patients for whom the treatmentassignment is influenced by biomarker results arerandomized.Staged trial designs are also, in essence, a combination of
basic patient flows. For instance, the proposed "two-stagesample-enrichment" design by Liu and colleagues (54)startswith accruing only biomarker-positive patients duringthe initial stage of the trial. At the end of the first stage, aninterimanalysis is conducted comparing the outcomeof theexperimental versus control treatment in biomarker-posi-tives. If the results are not promising for the new treatment,
accrual stops and no treatment benefit is claimed. Other-wise, accrual continues with recruiting unselected popula-tion. This design is a combination of an enrichment and atraditional flow, conditional on the result of the interimanalysis.
Contrariwise, in "adaptive patient enrichment" design(55)—also labeled as "adaptive accrual" (18, 37)—the trialbegins with a biomarker-stratified first stage in which itaccrues both biomarker-positive and -negative patients. Ifthe results of an interim analysis comparing the outcome ofthe experimental versus control treatment in biomarker-negatives are not promising, accrual to biomarker-negativesubgroup is terminated and the second stage continues as anenrichment trial in biomarker-positive patients until theplanned total sample size is reached.
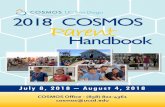
Effects assessed by each category of designsThere are four types of effects we are commonly interested
in when designing a biomarker trial: the treatment effect,the biomarker effect, the biomarker by treatment effect, andthe strategy effect. These are presented with 8 study ques-tions in Table 2. The treatment effect (experimental vs.
Table 2. List of effects that canbeassessedandquestions that canbeansweredby the trials of eachdesigncategory
Biomarker-strategy
Questions trial can answer Single-arm Enrichment Randomize-all
With biomarkermeasurement inthe control arm
Without biomarkermeasurement inthe control arm
With treatmentrandomization inthe control arm
Treatment effectsQ1. How does the experimental treatmentcompare with the control treatment inbiomarker-positives?
— H H H H Indirect H
Q2. How does the experimental treatmentcompare with the control treatment inbiomarker-negatives?
— — H — — H
Q3. How does the experimental treatmentcompare with the control treatment in overallstudy population?
— — H — — H
Biomarker effectsQ4. Is the biomarker status associated withtheoutcome in the standardof care group? (Isthe biomarker prognostic?)
— — H H H Indirect H
Q5. Is the biomarker status associated withthe outcome in the experimental treatmentgroup?
H — H H H H
Biomarker by treatment effectQ6. Is the biomarker status associated with abenefit of experimental treatment? (Is thebiomarker is predictive?)
— — H — — H
Strategy effectsQ7. How does the biomarker-basedtreatment strategy compare with the controltreatment in the overall study population?
— — H Indirect H H H
Q8. How does the biomarker-basedtreatment strategy compare with theexperimental treatment in the overall studypopulation?
— — H Indirect — — H
Trial Designs for Personalizing Cancer Care
www.aacrjournals.org Clin Cancer Res; 19(17) September 1, 2013 OF7
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

control) can be estimated separately for biomarker-positivepatients (Q1), for biomarker-negative patients (Q2), andin the overall population (Q3). Single-arm trials do notanswer any of these questions, as they lack a control arm toallow comparisons. Enrichment trials recruit biomarker-positive patients and allocate them to experimental orcontrol treatment, thus letting us evaluate the effect oftreatment, but only in biomarker-positive patients (Q1;ref. 1). Randomize-all trials recruit patients from the wholespectrum of the biomarker values and allocate them ran-domly to either of the two treatment options. Therefore,they allow estimation of the treatment effect in biomarker-positives, -negatives, and in the overall population (Q1–3).
To evaluate if a biomarker is prognostic (Q4), one needsto compare the outcome of biomarker-positive and -nega-tive patients on control treatment, a comparison which ispossible in randomize-all study designs but not in single-arm or enrichment trials (1, 28). The only effect one canestimate in the single-arm trials is the biomarker effect inthe experimental arm, whether biomarker status is associ-ated with the outcome of experimental treatment (Q5).
To assess the predictive capacity of a biomarker (Q6)—the biomarker by treatment effect—one needs to have theoutcome of biomarker-positive and -negative patientsseparately after experimental and control treatments. Ran-domize-all trials allow such an assessment by providingestimates for all four aforementioned outcomes (1).
In the biomarker-strategy trials, patients are randomizedto treatment strategies, instead of treatments. This featurepermits direct comparison of the outcomes of a biomarker-based strategy versus those in a strategy of control treatmentfor all (Q7). Addition of a randomization to the controlarm of a biomarker-strategy trial allows direct comparisonwith a strategy of experimental treatment for all (Q8;ref. 56). With a randomize-all trial, one cannot estimatethese effects using randomization properties. By combiningmarker-positivity rate, outcome of experimental treatmentin biomarker-positives and outcome of control treatmentin biomarker-negatives, an indirect estimate of strategyeffects, can be obtained (57), though it might be biasedconsidering confounding effects of other prognostic factorsand it may miss the additional effects of testing, apartfrom treatment selection (58). In biomarker-strategy de-signs, there are biomarker-positive and -negative patientswho are treatedwith the control treatment, soone can assessprognostic capacity of the biomarker in all three subtypes.However, the evaluation of biomarker-predictive capacity isonly possible when treatment is randomized in the controlarm allowing estimation of experimental treatment effect inbiomarker-negative patients (1).
DiscussionThis systematic review documented a substantial vari-
ability in the labeling of clinical trial designs for evaluatingbiomarkers for treatment selection in individual patients.We identified more than 300 labels, half of which wereunique. In evaluating the heterogeneity in design labels, we
used a classification scheme based on patient flow compo-nents of the corresponding trial designs. Under each of thefour basic patient flow categories, several labels could becategorized, where some labels are completely interchange-able terms. Other designs, while having the same patientflow elements, carried specific objectives or had diverginganalysis plans, which authors have labeled differently, toemphasize these distinctive aspects.
Using our patient flow scheme, one would be able toclassify biomarker trial designs into a small set of basiccategories. This could be useful for identifying similaritiesbetween novel designs and existing ones, or to evaluateproposed modifications of existing designs. It could also behelpful in reducing the confusion around the design ofbiomarker trials and help with standardizing the reportingofbiomarker clinical trials. Because the classification isbasedon patient flow, it is directly connected to the possiblecomparisons that canbemade in the trial and, consequently,the questions that could be potentially answered by the trial.
By comparing the designs in Table 2, a biomarker-strategydesign with treatment randomization in the control armseems a very attractive option, allowing for direct estimationof all biomarker-related effects, yet this feature might comeat the cost of a large sample size. Nevertheless, in situationswhere the biomarker-strategy is complex—having a largenumber of treatment options or biomarker categories—orwhen the trial is planned primarily for confirmatory assess-ment of a specific biomarker-based strategy, a biomarker-strategy trial can be the design of choice. A limitation ofbiomarker-strategy trials is that assessments are restricted toa prespecified biomarker-treatment combination strategyand they cannot be used for further identification or vali-dation of other biomarkers.
Randomize-all trials alsoallowassessmentof all biomark-er-related effects, but provide indirect estimates of strategyeffects. An attractive aspect of randomize-all trials is thatthey allow identification and evaluation of biomarkers thatwere not specified in the design phase of the trial. Single ormultiple biomarkers can be studied and multimarker mod-els can be developed and tested in trials of randomize-allcategory. If one collects and stores biologic specimens fromparticipants of a randomize-all trial in biobanks, the trialdata can be used later to identify or evaluate single ormultiple biomarkers, possibly not even known at the timeof trial design (59). However, as all analyses that emergeafter designing the trial are considered post hoc and explor-atory, cross-validation and/or independent validationapproaches are required to establish the use of biomarkers.
Enrichment design can be selected when there is a strongprior biologic evidence that the experimental treatment hasno effect in biomarker-negative patients (3, 20). Yet, apositive trial does not prove the use of the biomarkerbecause there may exist a positive treatment effect in theunevaluated biomarker-negative patients (1, 3).
Biomarker trials have predominantly been proposed anddiscussed in the setting of phase III trials in oncology. Allcategories identified in this review apply when designing aphase III biomarker trial, though some designs have been
Tajik et al.
Clin Cancer Res; 19(17) September 1, 2013 Clinical Cancer ResearchOF8
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

suggested primarily for a phase II setting. These includerandomize-all designs with adaptive randomization, suchas the outcome-based trials with Bayesian adaptive ran-domization (5, 36), as well as some of the designs in thecombined category, such as tandem two-step phase IIpredictor marker evaluation (60), which aim at finding apromising treatment/biomarker pair that can be movedforward to a phase III evaluation.To our knowledge, this review is the first systematic
review of trial designs for evaluation of prognostic andpredictive biomarkers. Several other narrative reviews areavailable, most often written by experts (1, 2, 33, 35, 53),who commonly have discussed a selected series of biomark-er trial designs and used their personally preferred designlabels. Yet our review was also not without limitation,which was the shortcoming of our search strategy in theelectronic databases. The retrieval of methodologic articlesis challenging because no specific keywords are availableto distinguish articles that have described or presented amethod from those which have just applied that method.Most of the search terms we could use were nonspecific.Even the terms "prognostic" and "predictive" are common-ly used by authors in other situations. To compensate forthese challenges, we designed our search strategy to bebroad and sensitive. We also looked for relevant articlesby checking the references and citations of the selectedretrieved articles.Biomarkers are changing the way doctors handle many
cancers, but there is still a long way to go before biomarkersreach their full potential in cancer management. With theadvent of rapidly growing technologies for measuring new
biomarkers, there is a parallel need for validating the clinicaluse of using such biomarkers for selection treatment ofindividual patients. Well-designed and properly conductedtrials may support the timely introduction of new biomar-kers in clinical management, to the benefit of cancerpatients.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: P. Tajik, P.M. BossuytDevelopment ofmethodology: P. Tajik, A.H. Zwinderman, B.W.Mol, P.M.BossuytAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): P. Tajik, B.W. Mol, P.M. BossuytAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): P. Tajik, A.H. Zwinderman, B.W. Mol,P.M. BossuytWriting, review, and/or revision of the manuscript: P. Tajik, A.H.Zwinderman, B.W. Mol, P.M. BossuytAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): P. TajikStudy supervision: P.M. Bossuyt
AcknowledgmentsThe authors thank Ms. Faridi van Etten-Jamaludin for her help with
developing the search strategy and searching the databases.
Grant SupportFunding for this research was provided by The Netherlands Organization
for Health Research and Development (ZonMw), the Hague, the Nether-lands (grant number 152002026).
Received December 3, 2012; revised May 24, 2013; accepted June 9, 2013;published OnlineFirst June 20, 2013.
References1. Freidlin B, McShane LM, Korn EL. Randomized clinical trials with
biomarkers: design issues. J Natl Cancer Inst 2010;102:152–60.2. Buyse M, Michiels S, Sargent DJ, Grothey A, Matheson A, de GA.
Integrating biomarkers in clinical trials. Expert Rev Mol Diagn 2011;11:171–82.
3. Mandrekar SJ, Sargent DJ. Clinical trial designs for predictive bio-marker validation: one size does not fit all. J Biopharm Stat 2009;19:530–42.
4. Seymour L, Ivy SP, Sargent D, Spriggs D, Baker L, Rubinstein L, et al.The design of phase II clinical trials testing cancer therapeutics:consensus recommendations from the clinical trial design task forceof the national cancer institute investigational drug steering commit-tee. Clin Cancer Res 2010;16:1764–9.
5. Ang MK, Tan SB, Lim WT. Phase II clinical trials in oncology: are wehitting the target? Expert Rev Anticancer Ther 2010;10:427–38.
6. Farley J, Rose PG. Trial design for evaluation of novel targetedtherapies. Gynecol Oncol 2010;116:173–6.
7. McShane LM, Hunsberger S, Adjei AA. Effective incorporation ofbiomarkers into phase II trials. Clin Cancer Res 2009;15:1898–905.
8. Pusztai L, Hess KR. Clinical trial design for microarray predictivemarker discovery and assessment. Ann Oncol 2004;15:1731–7.
9. RomondEH,PerezEA,Bryant J, SumanVJ,GeyerCEJr, DavidsonNE,et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005;353:1673–84.
10. Ziegler A, Koch A, Krockenberger K, Grosshennig A. Personalized med-icine using DNA biomarkers: a review. Hum Genet 2012;131:1627–38.
11. Di MM, Gallo C, De ME, Morabito A, Piccirillo MC, Gridelli C, et al.Methodological aspects of lung cancer clinical trials in the era oftargeted agents. Lung Cancer 2010;67:127–35.
12. Bria E, Di MM, Carlini P, Cuppone F, Giannarelli D, Cognetti F, et al.Targeting targeted agents: open issues for clinical trial design. J ExpClin Cancer Res 2009;28:66.
13. Hoering A, Leblanc M, Crowley JJ. Randomized phase III clinical trialdesigns for targeted agents. Clin Cancer Res 2008;14:4358–67.
14. FerraldeschiR,AttardG, deBonoJS.Novel strategies to test biologicalhypotheses in early drug development for advanced prostate cancer.Clin Chem 2013;59:75–84.
15. Lai TL, Lavori PW, Shih MC, Sikic BI. Clinical trial designs fortesting biomarker-based personalized therapies. Clin Trials 2012;9:141–54.
16. An MW, Mandrekar SJ, Sargent DJ. A 2-stage phase II design withdirect assignment option in stage II for initial marker validation. ClinCancer Res 2012;18:4225–33.
17. TrusheimMR, Burgess B, HuSX, Long T, Averbuch SD, Flynn AA, et al.Quantifying factors for the successof stratifiedmedicine. NatRevDrugDiscov 2011;10:817–33.
18. Mandrekar SJ, Sargent DJ. Clinical trial designs for predictive bio-marker validation: theoretical considerations and practical challenges.J Clin Oncol 2009;27:4027–34.
19. French B, Joo J, Geller NL, Kimmel SE, Rosenberg Y, Anderson JL,et al. Statistical design of personalized medicine interventions: theClarification of Optimal Anticoagulation throughGenetics (COAG) trial.Trials 2010;11:108.
20. MaitournamA,SimonR.On theefficiencyof targeted clinical trials. StatMed 2005;24:329–39.
21. Suman VJ, Dueck A, Sargent DJ. Clinical trials of novel and targetedtherapies: endpoints, trial design, and analysis. Cancer Invest 2008;26:439–44.
Trial Designs for Personalizing Cancer Care
www.aacrjournals.org Clin Cancer Res; 19(17) September 1, 2013 OF9
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

22. Bossuyt PM, Lijmer JG,Mol BW.Randomised comparisons ofmedicaltests: sometimes invalid, not always efficient. Lancet 2000;356:1844–7.
23. Beckman RA, Clark J, Chen C. Integrating predictive biomarkers andclassifiers into oncology clinical development programmes. Nat RevDrug Discov 2011;10:735–48.
24. Coyle VM, Johnston PG. Genomic markers for decision making: whatis preventing us from using markers? Nat Rev Clin Oncol 2010;7:90–7.
25. Simon R. Development and validation of biomarker classifiers fortreatment selection. J Stat Plan Inference 2008;138:308–20.
26. Paik S. Clinical trial methods to discover and validate predictivemarkers for treatment response in cancer. Biotechnol Annu Rev2003;9:259–67.
27. Wang SJ, O'Neill RT, Hung HJ. Statistical considerations in evaluatingpharmacogenomics-based clinical effect for confirmatory trials. ClinTrials 2010;7:525–36.
28. Lee JJ, Xuemin G, Suyu L. Bayesian adaptive randomization designsfor targeted agent development. Clin Trials 2010;7:584–96.
29. Simon R. Clinical trials for predictive medicine. Stat Med 2012;31:3031–40.
30. Johnson DR, Galanis E. Incorporation of prognostic and predictivefactors into glioma clinical trials. Curr Oncol Rep 2013;15:56–63.
31. Buyse M. Towards validation of statistically reliable biomarkers. Eur JCancer Suppl 2007;5:89–95.
32. Lee CK, Lord SJ, Coates AS, Simes RJ. Molecular biomarkers toindividualise treatment: assessing the evidence.Med J Aust 2009;190:631–6.
33. Simon R. Clinical trial designs for evaluating the medical utility ofprognostic and predictive biomarkers in oncology. Per Med 2010;7:33–47.
34. Le TC, KamalM, TredanO, Delord JP, CamponeM,Goncalves A, et al.Designs and challenges for personalized medicine studies in oncol-ogy: focus on the SHIVA trial. Target Oncol 2012;7:253–65.
35. Mandrekar SJ, Grothey A, Goetz MP, Sargent DJ. Clinical trial designsfor prospective validation of biomarkers. Am J Pharmacogenomics2005;5:317–25.
36. ZhouX, Liu S, KimES, Herbst RS, Lee JJ. Bayesian adaptive design fortargeted therapy development in lung cancer–a step toward person-alized medicine. Clin Trials 2008;5:181–93.
37. Sato Y, Laird NM, Yoshida T. Biostatistic tools in pharmacoge-nomics—advances, challenges, potential. Curr Pharm Des 2010;16:2232–40.
38. Baker SG, Kramer BS, Sargent DJ, Bonetti M. Biomarkers, subgroupevaluation, and clinical trial design. Discov Med 2012;13:187–92.
39. Mandrekar SJ, Sargent DJ. Predictive biomarker validation in practice:lessons from real trials. Clin Trials 2010;7:567–73.
40. Jiang W, Freidlin B, Simon R. Biomarker-adaptive threshold design: aprocedure for evaluating treatment with possible biomarker-definedsubset effect. J Natl Cancer Inst 2007;99:1036–43.
41. Freidlin B, Simon R. Adaptive signature design: an adaptive clinicaltrial design for generating and prospectively testing a gene expres-sion signature for sensitive patients. Clin Cancer Res 2005;11:7872–8.
42. Freidlin B, Jiang W, Simon R. The cross-validated adaptive signaturedesign. Clin Cancer Res 2010;16:691–8.
43. Cappuzzo F, Ciuleanu T, Stelmakh L, Cicenas S, Szczesna A, JuhaszE, et al. Erlotinib asmaintenance treatment in advanced non–small-celllung cancer: a multicentre, randomised, placebo-controlled phase 3study. Lancet Oncol 2010;11:521–9.
44. Freidlin B, Korn EL. Biomarker-adaptive clinical trial designs. Pharma-cogenomics 2010;11:1679–82.
45. Young KY, Laird A, Zhou XH. The efficiency of clinical trial designs forpredictive biomarker validation. Clin Trials 2010;7:557–66.
46. Fraser GA, Meyer RM. Biomarkers and the design of clinical trials incancer. Biomark Med 2007;1:387–97.
47. Wang SJ. Biomarker as a classifier in pharmacogenomics clinicaltrials: a tribute to 30th anniversary of PSI. Pharm Stat 2007;6:283–96.
48. Lijmer JG, Bossuyt PM. Various randomized designs can be used toevaluate medical tests. J Clin Epidemiol 2009;62:364–73.
49. Therasse P, Carbonnelle S, Bogaerts J. Clinical trials design andtreatment tailoring: general principles applied to breast cancerresearch. Crit Rev Oncol Hematol 2006;59:98–105.
50. Stingl Kirchheiner JC, Brockmoller J. Why, when, and how shouldpharmacogenetics be applied in clinical studies?: current and futureapproaches to study designs. Clin Pharmacol Ther 2011;89:198–209.
51. Ferrante di RL, Davenport C, Eisinga A, Hyde C, Deeks JJ. A capture-recapture analysis demonstrated that randomized controlled trialsevaluating the impact of diagnostic tests on patient outcomes arerare. J Clin Epidemiol 2012;65:282–7.
52. Sargent D, Allegra C. Issues in clinical trial design for tumor markerstudies. Semin Oncol 2002;29:222–30.
53. Sargent DJ, Conley BA, Allegra C, Collette L. Clinical trial designs forpredictive marker validation in cancer treatment trials. J Clin Oncol2005;23:2020–7.
54. Liu A, Liu C, Li Q, Yu KF, Yuan VW. A threshold sample-enrichmentapproach in a clinical trial with heterogeneous subpopulations. ClinTrials 2010;7:537–45.
55. Wang SJ, Hung HM, O'Neill RT. Adaptive patient enrichment designsin therapeutic trials. Biom J 2009;51:358–74.
56. Freidlin B,McShane LM,PolleyMY,Korn EL. Randomizedphase II trialdesigns with biomarkers. J Clin Oncol 2012;30:3304–9.
57. Song X, Pepe MS. Evaluating markers for selecting a patient's treat-ment. Biometrics 2004;60:874–83.
58. Bossuyt PM,McCaffery K. Additional patient outcomes and pathwaysin evaluations of testing. 2009 Nov 9. In: Medical tests-white paperseries [Internet]. Rockville (MD): Agency for Healthcare Research andQuality (US); 2009-. Available from: http://www.ncbi.nlm.nih.gov/books/NBK49463/.
59. Tajik P, Bossuyt PM. Genomic markers to tailor treatments: waiting orinitiating? Hum Genet 2011;130:15–8.
60. Pusztai L, Anderson K, Hess KR. Pharmacogenomic predictor dis-covery in phase II clinical trials for breast cancer. Clin Cancer Res2007;13:6080–6.
61. Scheibler F, Zumbe P, Janssen I, Viebahn M, Schroer-Gunther M,Grosselfinger R, et al. Randomized controlled trials on PET: a sys-tematic review of topics, design, and quality. J Nucl Med 2012;53:1016–25.
62. Kelloff GJ, Sigman CC. Cancer biomarkers: selecting the right drug forthe right patient. Nat Rev Drug Discov 2012;11:201–14.
63. Karuri SW, SimonR. A two-stageBayesian design for co-developmentof new drugs and companion diagnostics. Stat Med 2012;31:901–14.
64. Shi Q, Mandrekar SJ, Sargent DJ. Predictive biomarkers in colorectalcancer: usage, validation, and design in clinical trials. Scand J Gastro-enterol 2012;47:356–62.
65. ZhengG,WuCO,YangS,WaclawiwMA,DeMetsDL,GellerNL.NHLBIclinical trials workshop: an executive summary. Stat Med 2012;31:2938–43.
66. Mandrekar SJ, Sargent DJ. All-comers versus enrichment designstrategy in phase II trials. J Thorac Oncol 2011;6:658–60.
67. Mandrekar SJ, Sargent DJ. Design of clinical trials for biomarkerresearch in oncology. Clin Investig 2011;1:1629–36.
68. Galanis E, Wu W, Sarkaria J, Chang SM, Colman H, Sargent D, et al.Incorporation of biomarker assessment in novel clinical trial designs:personalizing brain tumor treatments. Curr Oncol Rep 2011;13:42–9.
69. Simon R. Clinical trials for predictive medicine: new challenges andparadigms. Clin Trials 2010;7:516–24.
70. Simon R. Advances in clinical trial designs for predictive biomarkerdiscoveryandvalidation.CurrentBreastCancerReports2009;1:216–21.
71. Mandrekar SJ, Sargent DJ. Genomic advances and their impact onclinical trial design. Genome Med 2009;1:69.
72. Liu JP, Lin JR, Chow SC. Inference on treatment effects for targetedclinical trials under enrichment design. Pharm Stat 2009;8:356–70.
73. Simon R. Designs and adaptive analysis plans for pivotal clinical trialsof therapeutics and companion diagnostics. Expert Opin Med Diagn2008;2:721–9.
74. Simon R. The use of genomics in clinical trial design. Clin Cancer Res2008;14:5984–93.
75. Ma BB, Britten CD, Siu LL. Clinical trial designs for targeted agents.Hematol Oncol Clin North Am 2002;16:1287–305.
Tajik et al.
Clin Cancer Res; 19(17) September 1, 2013 Clinical Cancer ResearchOF10
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

76. European Medicines Agency. Reflection paper on methodologicalissues associated with pharmacogenomic biomarkers in relation toclinical development and patient selection [Internet]. London; 2011[cited 2012 Jul 3]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2011/07/WC500108672.pdf.
77. George SL. Statistical issues in translational cancer research. ClinCancer Res 2008;14:5954–8.
78. Van Schaeybroeck S, Allen WL, Turkington RC, Johnston PG. Imple-menting prognostic and predictive biomarkers in CRC clinical trials.Nat Rev Clin Oncol 2011;8:222–32.
79. Hodgson DR, Wellings R, Harbron C. Practical perspectives of per-sonalized healthcare in oncology. N Biotechnol 2012;29:656–64.
80. Younes A, Berry DA. From drug discovery to biomarker-driven clinicaltrials in lymphoma. Nat Rev Clin Oncol 2012;9:643–53.
81. BuyseM, Sargent DJ, Grothey A, Matheson A, de GA. Biomarkers andsurrogate end points—the challenge of statistical validation. Nat RevClin Oncol 2010;7:309–17.
82. Simon R, Wang SJ. Use of genomic signatures in therapeutics devel-opment in oncology and other diseases. Pharmacogenomics J 2006;6:166–73.
83. Berry DA, Herbst RS, Rubin EH. Reports from the 2010 Clinicaland Translational Cancer Research Think Tank meeting: design
strategies for personalized therapy trials. Clin Cancer Res 2012;18:638–44.
84. Scher HI, Nasso SF, Rubin EH, Simon R. Adaptive clinical trial designsfor simultaneous testing ofmatcheddiagnostics and therapeutics.ClinCancer Res 2011;17:6634–40.
85. ConleyBA, TaubeSE.Prognostic andpredictivemarkers in cancer.DisMarkers 2004;20:35–43.
86. Wistuba II, Gelovani JG, Jacoby JJ, Davis SE, Herbst RS. Methodo-logical and practical challenges for personalized cancer therapies. NatRev Clin Oncol 2011;8:135–41.
87. Cho D, McDermott D, Atkins M. Designing clinical trials for kidneycancer based on newly developed prognostic and predictive tools.Curr Urol Rep 2006;7:8–15.
88. JonesCL, Holmgren E. An adaptive Simon two-stage design for phase2 studies of targeted therapies. Contemp Clin Trials 2007;28:654–61.
89. Spira A, Edmiston KH. Clinical trial design in the age of molecularprofiling. Methods Mol Biol 2012;823:19–34.
90. White TJ, Clark AG, Broder S. Genome-based biomarkers foradverse drug effects, patient enrichment and prediction of drugresponse, and their incorporation into clinical trial design. Per Med2006;3:177–85.
91. Eickhoff JC, Kim K, Beach J, Kolesar JM, Gee JR. A Bayesian adaptivedesign with biomarkers for targeted therapies. Clin Trials 2010;7:546–56.
Trial Designs for Personalizing Cancer Care
www.aacrjournals.org Clin Cancer Res; 19(17) September 1, 2013 OF11
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722

Published OnlineFirst June 20, 2013.Clin Cancer Res Parvin Tajik, Aleiko H. Zwinderman, Ben W. Mol, et al. Review and ClassificationTrial Designs for Personalizing Cancer Care: A Systematic
Updated version
10.1158/1078-0432.CCR-12-3722doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2013/06/20/1078-0432.CCR-12-3722.DC1Access the most recent supplemental material at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/early/2013/08/05/1078-0432.CCR-12-3722To request permission to re-use all or part of this article, use this link
Research. on April 13, 2019. © 2013 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 20, 2013; DOI: 10.1158/1078-0432.CCR-12-3722