Biochemical tests in clinical medicine lect1
40
Biochemical tests in clinical medicine Dr. Hala Kamel MBChB, MSc, MD Assist. prof. Biochemistry Dep., Faculty of Medicine ASU & UQ
-
Upload
mudassar-anwer -
Category
Education
-
view
593 -
download
1
Transcript of Biochemical tests in clinical medicine lect1
Biochemical tests in clinical
medicine
Dr. Hala Kamel
MBChB, MSc, MD
Assist. prof. Biochemistry Dep.,
Faculty of Medicine
ASU & UQ
Clinical Biochemistry
History
Clinical Examination
Diagnostic services
Laboratory services
Clinical Biochemistry
Clinical Biochemistry Laboratory
Clinical biochemistry Laboratory play an
important, often unrecognised role, in disease
diagnosis and the monitoring of treatment.
•They are responsible for most laboratory testing
performed on samples sent to the diagnostic
laboratory by medical practitioners.
•Laboratory results produced by MLS‟s are used
by medical staff in the diagnosis of disorders in
approx. 70% of all patient cases.
Clinical Biochemistry
• Analysis of the chemical constituents of the blood, urine, faeces and tissues.
• Most of the laboratory testing uses sophisticated instrumentation interfaced to a laboratory information system.
• Diseases such as diabetes, renal failure, heart attack, drug analysis and hepatitis are some of the conditions investigated by clinical biochemists.
Introduction
• Clinical Biochemistry
• Dissolved elements in body fluids
• Concentration and type e.g. glucose,
electrolytes, hormones and significance of
levels and interpretation.
• Accurate and precise laboratory
measurements can aid in diagnosis and
management of disease
Uses of Biochemical tests
• 1- Diagnosis
• 2- Screening
• 3-Prognosis
• 4- Treatment
Use of Biochemical Tests
• 1-Diagnosis
• History and Physical Examination of patient --form
Differential Diagnosis i.e. Hypothesis
• Lab tests and Radiology to support or reject hypothesis.
Limitations of tests must be appreciated
• Interpretation must be carefully done in context of clinical
details
2-Screening
• Detection of sub-clinical
• Neonatal screening PKU, CHT
• Criteria for same.
• Natural history known
• Acceptable tests no false negatives, few
false positives
• Ease of treatment
• Positive outcome
Screening
• Natural history of disease
• Acceptable and reliable screening Tests,
FP issues
• Therapy available
• Prevalence
• Entire population
• or “at risk groups”
3-Prognosis
• Serial tests to identify progressive
disease creatinine in renal failure
• Tests to identify risks of disease in future
in certain groups cholesterol in “at risk
families”
• Calculation of risk depends on
epidemiological data
• Likely outcome of disease
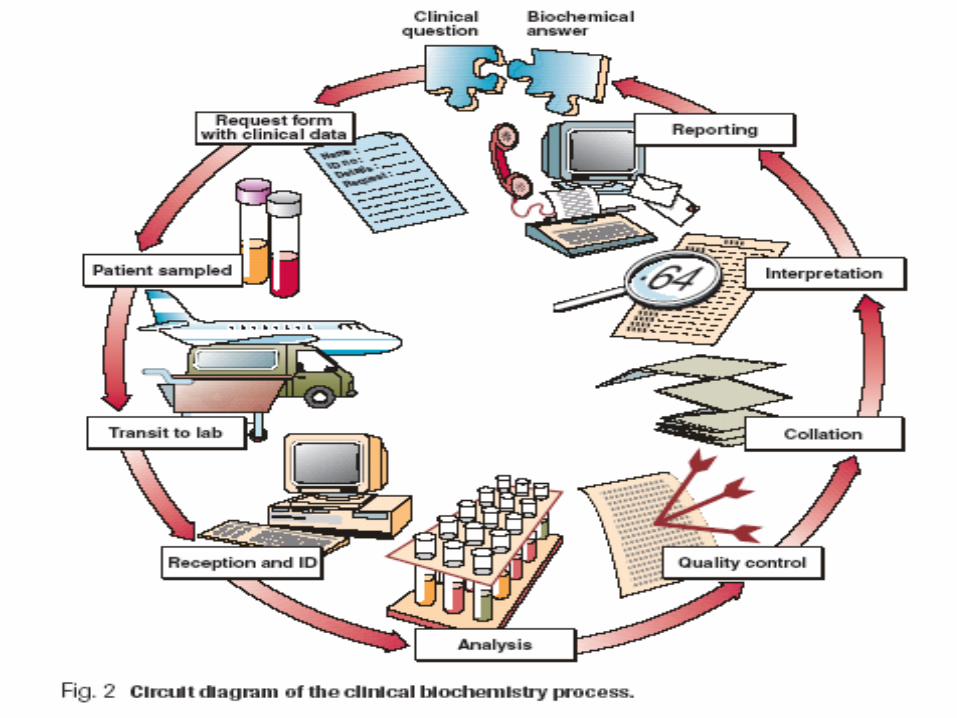
Sampling
• Test Request
• Clinician requests that analysis be conducted.
• Requirements
• Name, DOB, Gender, Hos. No. MRN
• Ward, Address
• Requesting Clinician
• Hypothesis / Problem
• Tests sought,time of sampling,date
• Clinical details, Drugs or Therapy.
Sampling Issues.
• Patient Centred Factors
• Age
• Gender
• Posture
• Physiological State
• Pregnancy
• Exercise
• Fasting / Fed
• Time
Sampling contd.• Plasma,serum
• Bottle and preservative, anti coagulant used
• Age of sample
• Time of sampling
• Guidance from lab on sample requirements
• Correct label
• Transport
• High risk specimen.
VariationPatient Variables :
• Age, gender, fasting, time of day, exercise, posture, need to document these.
• Biological Variation
• Pre-Analytical Variation
• Sample site, type of bottle
• Transportation to lab.
• Stability of analyte age
• Analytical Variation
• Post Analytical Interpretation
Analysis
• Accuracy & Precision
• Detection limits
• Specificity& sensitivity
• quality assurance
• reference ranges
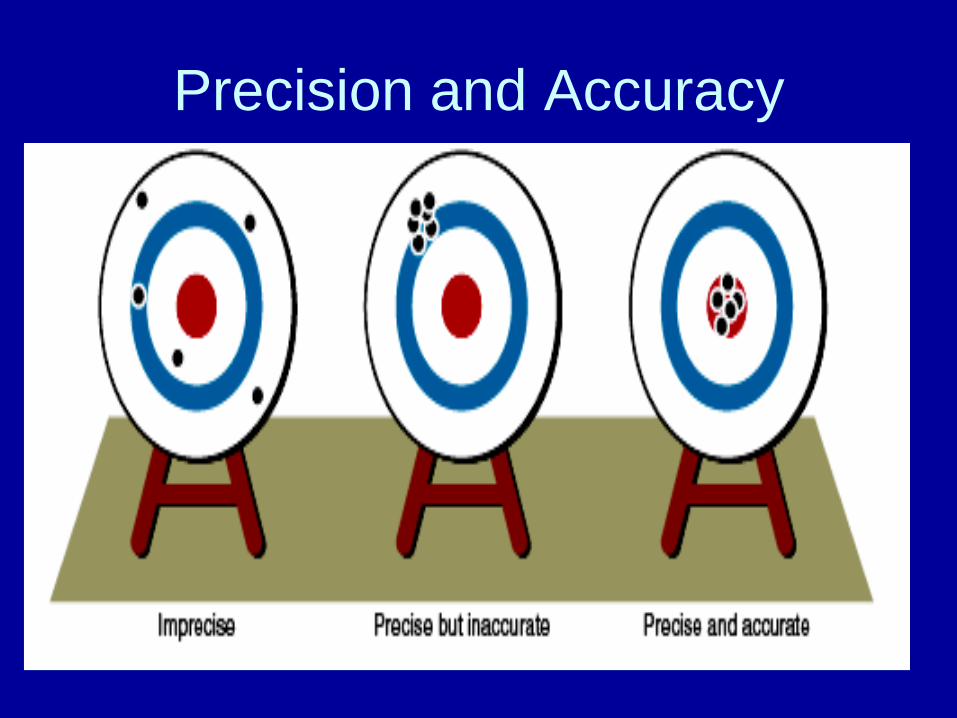
Precision and accuracy
• Precision is the reproducibility of an
analytical method.
• If there is 2 methods performed for the
same analyte repeated measurement of
the same analyte will show more closed
results to each others ( less scattering )
• Repeated measurement of an analyte will
be close to each other if precise
Precision and accuracy
• Accuracy defines how close the measured
value is to the actual value.
• Accuracy is therefore poor, as if the „sights‟ are off. so
repeated measurement of an analyte is accurate if it is
very close to actual value known before
• It is the objective in every biochemical method to
provide good precision and accuracy.
• Automation of analyses has improved precision
in most cases.
Precision and Accuracy
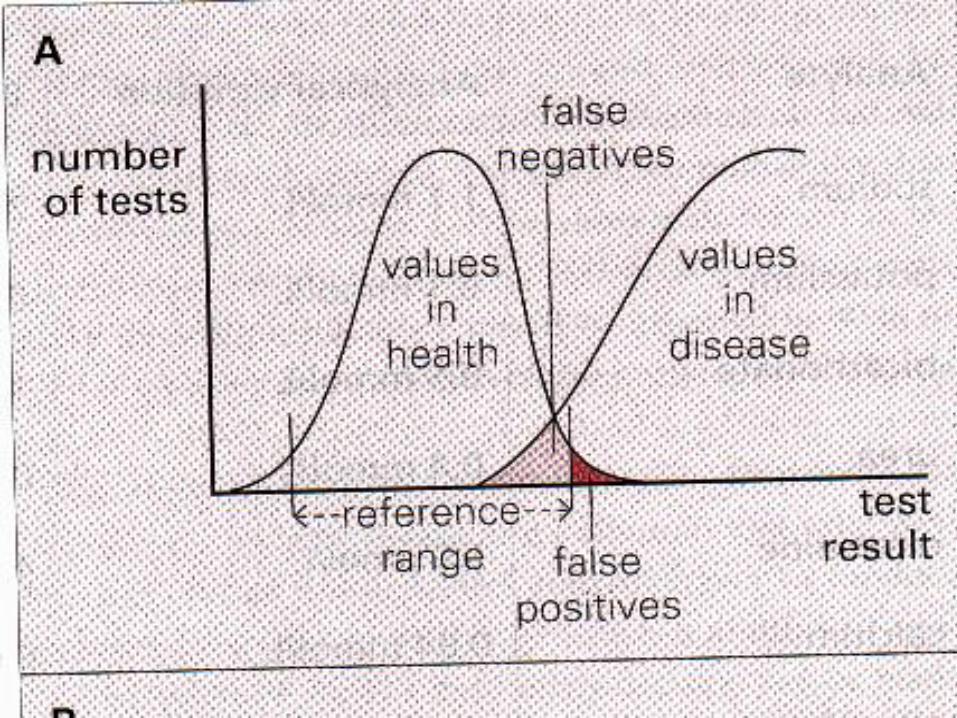
Diagnostic SensitivityPositive test result in presence of disease.
Diagnostic Specificity
Negative test result with no disease.
Diagnostic Sensitivity = TPTP + FN
Diagnostic Specificity = TN
FP+ TN
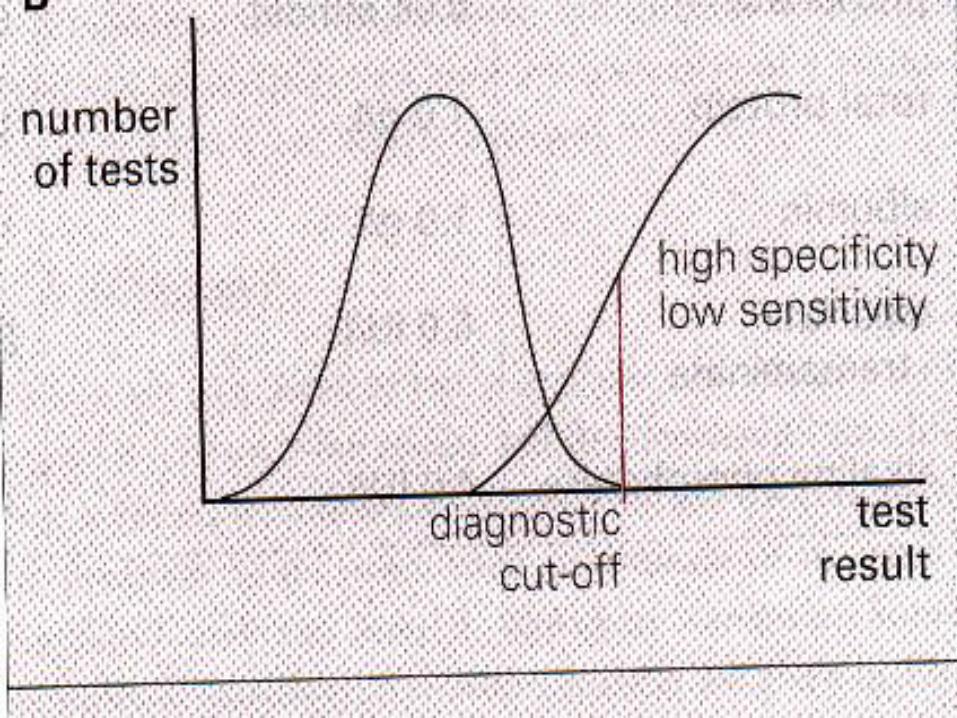
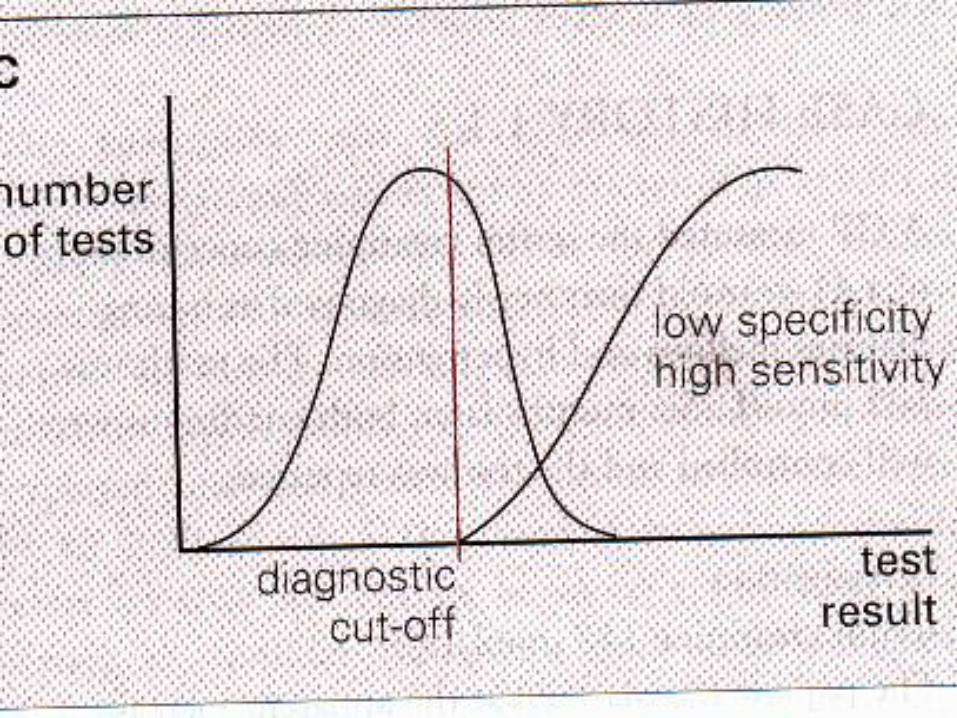
Analytical sensitivity and
specificity
• The analytical sensitivity of an assay is a
measure of how little of the analyte the method
can detect to improve the detection limit to help
in discrimination normal results and those with
suspected disease( Positivity in disease)
• Analytical specificity of an assay relates to how
good the assay is at discriminating between the
requested analyte and potentially interfering
substances. So it measures the negativity in
normal results
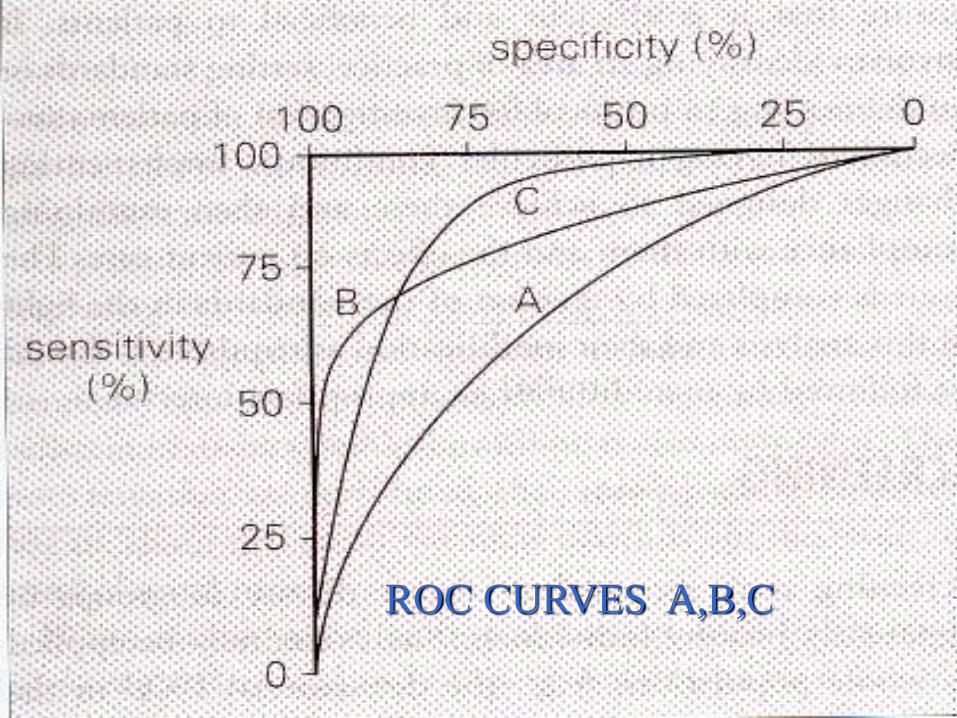
ROC CURVES A,B,C
Test Efficiency and Predictive
Values
TE = TP +TN X 100
Total No. of Tests
PV Pos = TP X 100
TP + FP
PV Neg = TN X 100
TN + FN
Features of PD pos. and PD neg.
• Prevalence of disease in population.
• Low prevalence with less than 100%
specificity high FP will result in low PV
• Screening with follow up testing should have
a high PV neg.
Likelihood Ratios
• LR pos = Sens. /1 – Spec.
• LR neg = Spec. / 1- Sens.
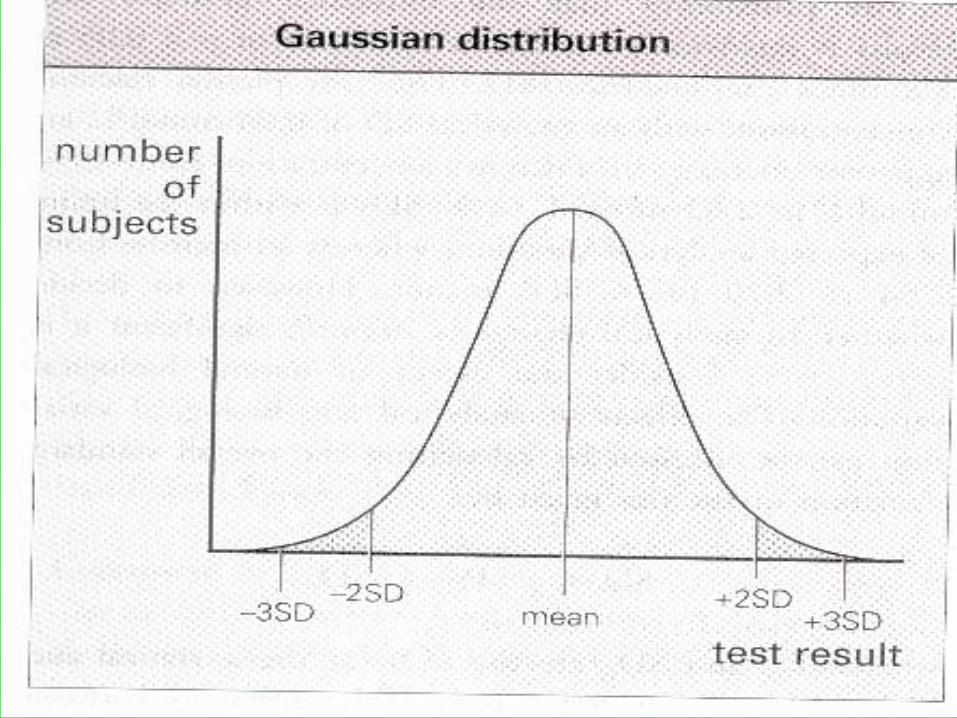
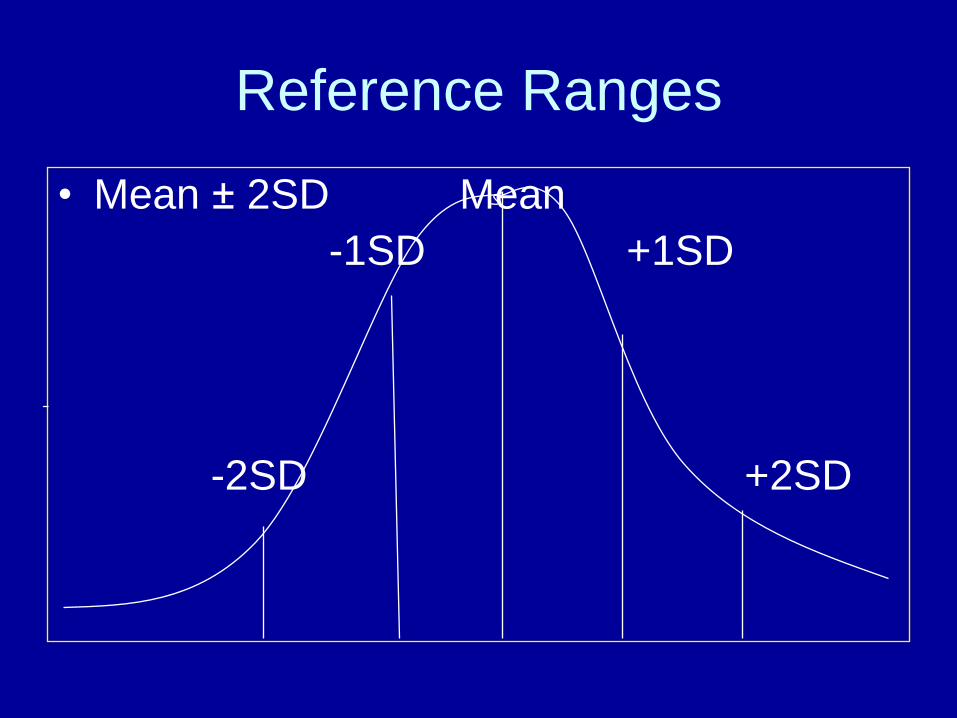
Reference Ranges
• Mean ± 2SD Mean
-1SD +1SD
-2SD +2SD
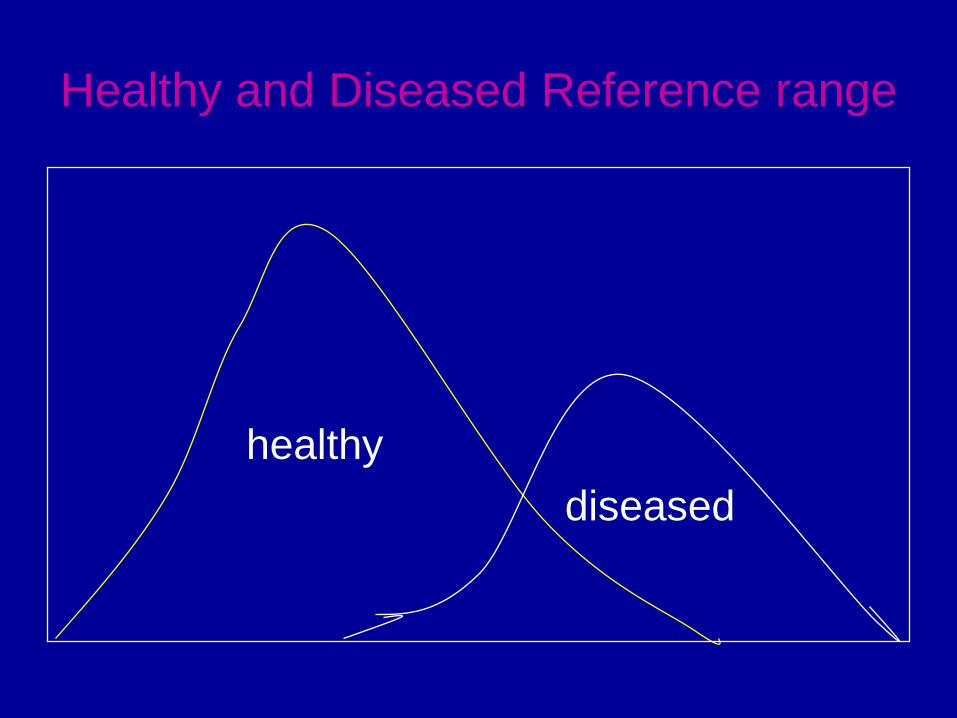
Healthy and Diseased Reference range
healthy
diseased
Biological Factors affecting
interpretation • Sex
• Age
• Diet
• Time of sampling
• Stress and anxiety
• Posture
• Exercise
• Medical History
• Pregnancy
• Menstrual cycle
• Drug History
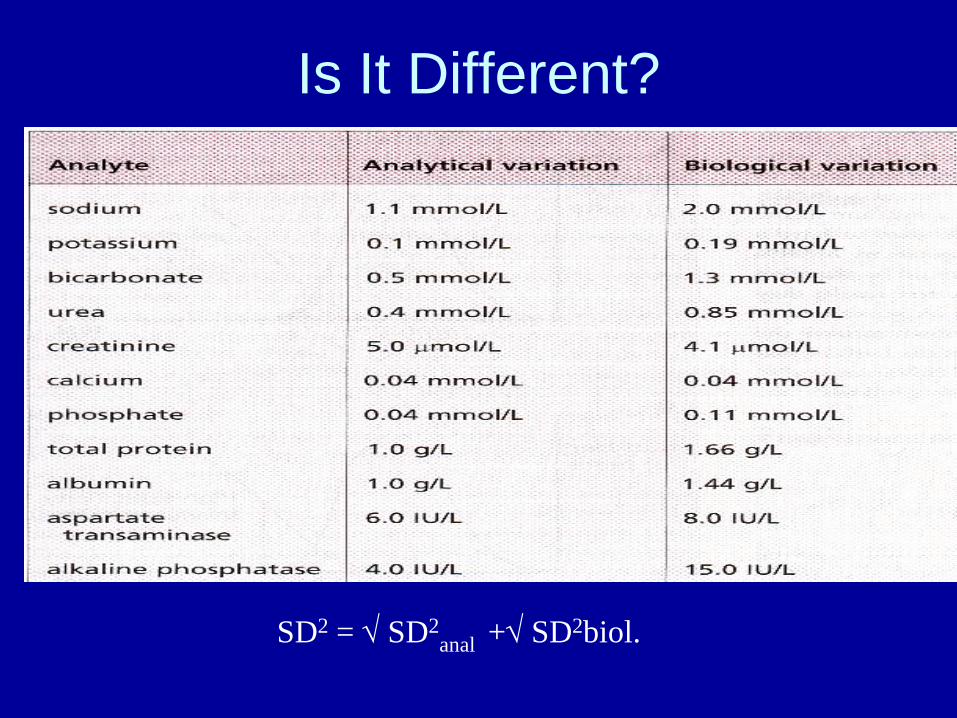
Is It Different?
SD2 = SD2anal + SD2biol.
Receiving the report
• Does the results fit in with the excepted?
• If not, how to explain the discrepancy?
• How can the results change the
diagnosis?
• How to manage that patient?
• What should be done?
Interpretation
• Is Result Normal?
• Has it changed?
• Does it support the clinical hypothesis?
Does it Support the Hypothesis?• Consistent support diagnosis
• Inconsistent needs explanation
• Error in sampling, patient labelling
analysis,or reporting.
• Repeat test
• ? Diagnosis
• Statistical random event abnormal test no
disease.
• Diagnostic Utility : Sensitivity, Specificity
Errors
• Pre-analytical
• Analytical
• Post-analytical,
• Interpretation,
• Delays
• Wrong records
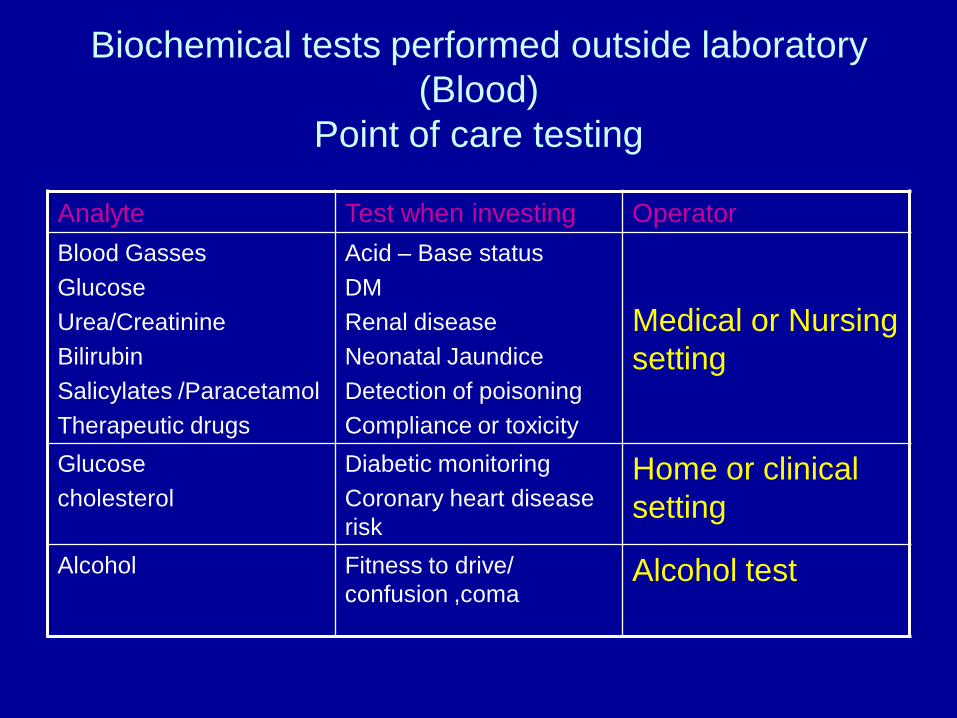
Biochemical tests performed outside laboratory
(Blood)
Point of care testing
Analyte Test when investing Operator
Blood Gasses
Glucose
Urea/Creatinine
Bilirubin
Salicylates /Paracetamol
Therapeutic drugs
Acid – Base status
DM
Renal disease
Neonatal Jaundice
Detection of poisoning
Compliance or toxicity
Medical or Nursing
setting
Glucose
cholesterol
Diabetic monitoring
Coronary heart disease
risk
Home or clinical
setting
Alcohol Fitness to drive/
confusion ,comaAlcohol test
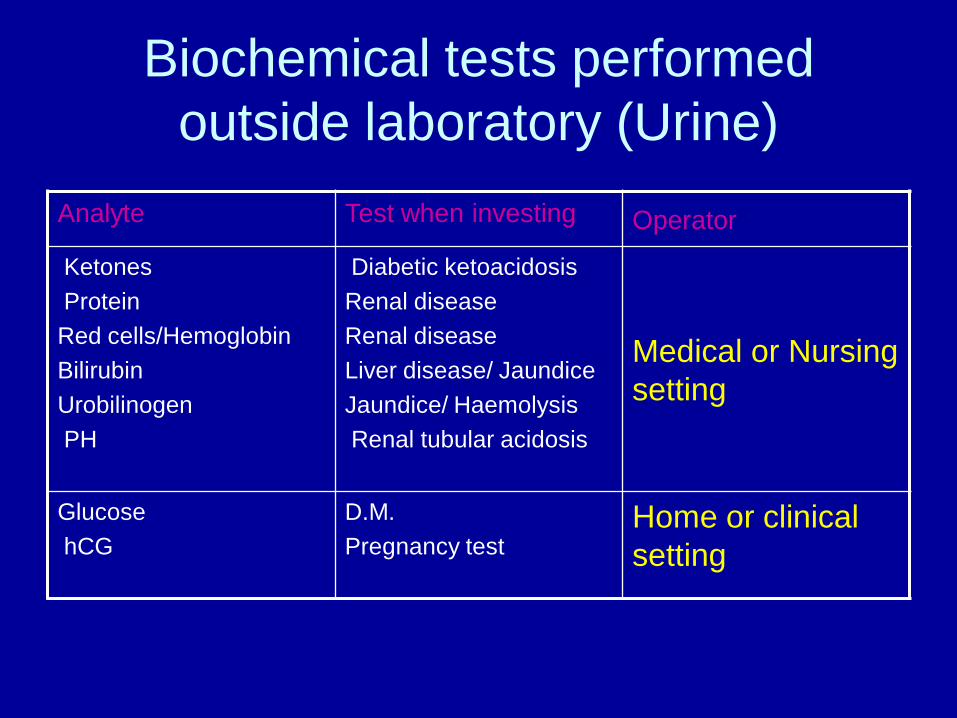
Biochemical tests performed
outside laboratory (Urine)
Analyte Test when investing Operator
Ketones
Protein
Red cells/Hemoglobin
Bilirubin
Urobilinogen
PH
Diabetic ketoacidosis
Renal disease
Renal disease
Liver disease/ Jaundice
Jaundice/ Haemolysis
Renal tubular acidosis
Medical or Nursing
setting
Glucose
hCG
D.M.
Pregnancy testHome or clinical
setting
POCT: Advantages
• Faster stabilization of life-threatening crises (eg drug overdose, electrolyte disturbance)
• Immediate risk stratification (eg chest pain)
• Closer therapeutic management (eg diabetes)
• Better patient compliance with therapy (diabetes, anticoagulation, hyperlipidaemia)
• Reduce:
– repeat clinic/practice visits
– length of stay in hospital
– complications (intra- & postoperative)
– use of blood products (surgery)