Bio212 vop22 GI - cloud.ensemblevideo.com · Gastroesophageal Reflux Disease (GERDs): disorder...
24
11/24/2015 1 Gastrointestinal Disorders • Disorders of the esophagus and stomach • Disorders of the small and large intestine • Appendicitis Objectives: Part 1: Disorders of the esophagus and stomach
Transcript of Bio212 vop22 GI - cloud.ensemblevideo.com · Gastroesophageal Reflux Disease (GERDs): disorder...

11/24/2015
1
Gastrointestinal Disorders
• Disorders of the esophagus and stomach
• Disorders of the small and large intestine
• Appendicitis
Objectives:
Part 1: Disorders of the esophagus and
stomach

11/24/2015
2
Dysphagic Disorders of the Esophagus:ex. Achalasia
• Etiologies: decreased ganglion cells in the myenteric plexus, alteration of vagal tone, atrophy of smooth muscle.
• Manifestations: dysphagia, spasm of esophagus after swallowing, regurgitation of undigested food (heart burn/chest pain), weight loss, lung infections (nocturnal aspiration).
Dysphagic Disorders of the Esophagus:ex. Achalasia
• Preventative measures: avoidance of alcohol, temperature extremes with food/liquids, sleep with a high pillow to avoid aspiration
• Treatment: esophageal dilators, botulinumtoxin, serotonin, surgery.

11/24/2015
3
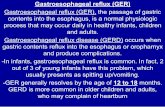
Disorders of the Esophagus:Gastroesophageal Reflux Disease (GERDs): disorder involving
the reflux of stomach contents
• May be due to weak or incompetent lower esophageal sphincter which allows reflux to occur and reduced ability to clear refluxed acid from the esophagus once it has occurred.
• Can over time lead to esophageal mucosal injury.
Disorders of the Esophagus:Gastroesophagael Reflux Disease (GERDs)
Manifestations:
• Heartburn (sometimes severe, occurs 30-60 minutes after eating, made worse by bending at the waist or lying down) and chest pain
• Belching
• Respiratory-like symptoms (aspiration)

11/24/2015
4
Disorders of the Esophagus:Gastroesophagael Reflux Disease (GERDs)
Treatment:• Preventative: Avoiding large meals, alcohol, and foods
that reduce the tonicity of the lower esophageal sphincter. Avoid body positions several hours after eating that make the problem worse. Sleep with head elevated. Maintain a good body weight.
• Antacids, alginic acid for mild cases• For more problematic cases: histamine-2 receptor
blocking antagonist drugs, proton pump inhibitors and/or surgery may be indicated.
Disorders of the Esophagus:Hiatal Hernia: a tear or weakness in the wall of the diaphragm in
which a protrusion of the upper part of the stomach/esophagus
pushes through the opening in the diaphragm into the thorax
region.
• Etiologies: congenital defects, stress/trauma to diaphragm
• Diagnosis: upper GI, radiography, endoscopy

11/24/2015
5
Disorders of the Esophagus:Hiatal Hernia
Manifestations:• Largely asymptomatic• If present: anything that increased abdominal
pressure such pregnancy, heaving bending/lifting, straining with constipation, severe vomiting, hard sneezing/coughing, obesity.
• Regurgitation of food, heart burn/chest pain, dysphagia.
Disorders of the Esophagus:Hiatal Hernia
Types:
• Sliding Hiatal Hernia: occurs when the lower esophageal sphincter slides up through the esophageal hiatus. This sliding can occur all the time or only during moments of increased abdominal pressure.
• Rolling Hiatal Hernia: a portion of the stomach is squeezed up through the esophageal hiatus against the esophagus and the lower esophageal sphincter.

11/24/2015
6
Disorders of the Esophagus:Hiatal Hernia
Complications:
• GERDs
• Strangulation of stomach could potentially lead to ischemic and necrotic tissue (rolling hiatal hernia)
• A large herniation can restrict the inflation of lung tissue causing breathing difficulties (rare).
Disorders of the Esophagus:Esophagitis: inflammation of the mucosal lining of the esophagus
• Etiologies: infections, irritation, GERDs, surgery, hernias, ingesting toxic substances, tumors, diverticula, autoimmune disorders
• Manifestations: heartburn, nausea/vomiting, painful swallowing, mouth/esophageal ulceration
• Complications: dysphagia, bleeding ulcers (anemia), GERDs, pulmonary aspiration, esophageal cancer.

11/24/2015
7
Disorders of the Stomach:Gastric Dumping Syndrome: rapid emptying of the stomach 10-
20 (or longer) minutes after eating.• Etiologies: pyloric stenosis or ulceration around pyloric
sphincter, gastric bypass surgery, rapid distention of the small intestine.
• When food is dumped rapidly into the small intestine, huge amounts of hypertonic solutes cause water to be drawn from small capillaries into the intestine. This leads to irritation of both small and large intestines, malabsorption of food, and rapid movement of materials through the GI tract.
Disorders of the Stomach:Gastric Dumping Syndrome
Manifestations:• Diarrhea, gas• Cramping• Malnourishment (dizziness, weakness), hypoglycemia• SweatingTreatment:• Preventative/Mild: Avoidance of problem foods/diet, eating smaller meals,
limiting sugar• More severe issues: drugs (alpha-glycoside hydrolase inhibitor that interferes
with carbohydrate absorption), somatostatin (slows down the release of insulin, decreases gastric dumping) and surgery.
Disorders of the Stomach:Gastritis: inflammation of the stomach lining
• Acute Gastritis: caused by irritating agents (alcohol, allergies, cortisone, chemicals, hot liquids), irritating foods, trauma/burns, CNS damage, chemotherapy/radiation
• Chronic Gastritis: caused by destruction of parietal cells leading to decreased production of HCl (chronic alcoholism, autoimmunity, aging, genetics)
• Manifestations: epigastric pain, anorexia, belching, inability to produce intrinsic factor (Vit. B12 deficiency)
• Complications: dehydration/electrolyte imbalances, acidosis, massive perforation/hemorrhage.

11/24/2015
8
Disorders of the Stomach:Ulcers: open sores that develop in the walls of the stomach after
the mucosal layer has been eroded way.
Peptic Ulcers:
Gastric: solitary and small
Duodenal: elongated, oval shape, most common site of ulcers because there isn’t the thick mucus layer protection like the stomach.
Disorders of the Stomach:Ulcers
Etiologies: • Helicobacter pylori attack of mucosal lining,• Autoimmune disorders• Acid imbalance/overproduction• Factors that alter mucosal barrier• Certain medications (rheumatoid arthritis)• Stomach cancer• NSAIDs

11/24/2015
9
Disorders of the Stomach:Ulcers
Manifestations: • Epigastric pain• Anorexia, nausea/vomiting• Weight loss• Bloody or blackish stools• B12 deficiencyTreatment:• Antibiotics• Proton pump inhibitors, antihistamines, sucralfate• Surgery (small vessels tied up and the ulcer is oversewn),
transfusion

11/24/2015
10
Disorders of the Stomach:UlcersStress Ulcers: Post-stress ischemia of the stomach mucosa and sympathetic vasoconstriction leading to diffuse, superficial ulcer formation. (burns, shock, trauma), other health complications could exacerbate stress ulcer formation.
• Can potentially lead to massive tissue necrosis, perforation and possible life-threatening bleeding.
• Treatment: Preventative: antacids, antihistamines, proton pump inhibitors, sucralfate (binds to mucosa to create a protective barrier). If severe, endoscopic treatment, transfusion, vasopressin.
Peptic Ulcer Stress Ulcer

11/24/2015
11
Disorders of the Stomach:Stomach Cancer
• Risk factors: genetics,carcinogens in the diet (smoked, preserved foods), autoimmune gastritis, gastric adenomas or polyps, chronic ulcers
• Manifestations: weight loss/anorexia, indigestion, epigastric pain, vomiting, abdominal mass.
Part 2: Disorders of the small and large
intestine
Irritable Bowel Syndrome (IBS): Chronic and recurrent intestinal symptoms not explained by
structural and biochemical abnormalities so diagnosis is
based on signs and symptoms lasting a duration or
intermittently occurring at least 12 weeks or longer.
• Manifestations: abdominal pain, bloating, constipation or diarrhea, relief with defecation, abnormal defecation frequency, lumpy/hard or loose/watery stools, mucus in stools.
• Celiac Disease and lactose intolerance may be precipitating factors with some individuals.

11/24/2015
12
Irritable Bowel Syndrome (IBS):
Treatment:
• Stress management, fruits/vegetables and fluids, avoidance of trigger foods (fats, gas-producing foods, caffeine, alcohol), anti-spasmodic and anticholinergic drugs
Irritable Bowel Disease: Inflammatory disease of the intestines characterized by remissions and relapses. Suspected etiologies: combination of genetics and abnormal microbial gut flora leading to an exaggerated immune response.
• Ulcerative Colitis
• Crohn Disease
Irritable Bowel Disease: Crohn Disease (regional enteritis, ileocolitis): chronic relapsing granulomatous inflammatory disease.Manifestations:• Skip Lesions: originate from the submucosa (which has
thickened and become hyperplasic). The lesions are sporadic (some areas of disease and other areas unaffected). Over time, these lesions can push into the lumen as well as out toward the serosa. Seen as a “string sign,” a thin stream of barium as seen in an upper GI.
• Usually affects distal ileum, initially. Lesions can move into the large intestine other areas along the GI tract.

11/24/2015
13
Irritable Bowel Disease: Crohn Disease Manifestations:• Mild, intermittent diarrhea (liquid stools with blood,
pus and mucus, steatorrhea), colicky pain in the upper and middle abdomen)
• General malaise and low grade fever• Weight loss, anemia, malabsorption• Complications: stenosis/obstruction,
ulcerations/perforation/peritonitis, formation of fistulas and abscesses, arthritis and uveitis
Irritable Bowel Disease: Crohn Disease
Treatment:
• There is no cure. Supportive and palliative treatment with hope of possible remission.
• Drugs such as corticosteroids, anti-cholinergics, anti-diarrheal drugs, immunomodulating drugs are used.
• Diet (avoidance of trigger foods) and nutritional supplementation.
• Resection surgery of disease areas.

11/24/2015
14
Irritable Bowel Disease: Ulcerative Colitis: inflammatory disease of the colon and rectum.
• Blood congestion and edema of the colon wall causes gut mucosa (often times at base of crypts) to become fragile (friable), non-protective and it starts to fall apart leading to ulcerations. The lesions are continuous.
Irritable Bowel Disease: Ulcerative ColitisManifestations:• Abdominal pain• Diarrhea, bloody stools, flatulenceComplications:• Irritation can lead to reduced wall motility• Enlarged colon (toxic megacolon)• Necrosis, perforation, hemorrhage of wall, peritonitis• Increased risk for colon cancer

11/24/2015
15
Irritable Bowel Disease: Ulcerative Colitis
Treatment:
• Resection surgery, colostomy
• Corticosteroids,anti-cholinergics, anti-diarrheal drugs
• Diet (avoidance of trigger foods)
• Immunomodulating drugs

11/24/2015
16
Irritable Bowel Disease: Crohn Disease and Ulcerative Colitis
Diagnosis:
• Sigmoidoscopy and colonscopy
• Stool cultures
• Radiographic studies (CT scans)
• Medical history and physical exam
Malabsorption Syndromes: problems with
intestinal mucosa and the reduced ability for absorption of a
single nutrient or a number of different nutrients.
Etiologies:• Infections• Food intolerances • Lymphatic obstruction• Autoimmunity• Endocrine Issues• Problems with the pancreas, liver or gall bladder• Atherosclerosis, congestive heart failure• Diseases of the small intestine
Malabsorption Syndromes:Celiac Disease:
• Extreme intolerance to gluten, patients may lack a specific enzyme that would normally detoxify gluten. There is inflammation and antibody production.
• Lesions of mucosa develop causing blunting, loss of villi and elongation of the intestinal crypts
Lactose Deficiency or Intolerance:
• Caused by enzyme deficiency of lactase.

11/24/2015
17
Malabsorption Syndromes:
General Manifestations:
• Abdominal pain, cramping, bloating• Diarrhea, flatulence• Bruising/bleeding (deficiency of vitamins)
• Bone pain and fracture (deficiency of minerals and vitamins)• Neuropathy
• Edema• Increased susceptibility for certain types of cancers, autoimmune
disorders and osteoporosis.
Intestinal Obstruction: interference with the
normal flow of intestinal contents through the GI tract.
• Could involve in any part of the GI tract, but tends to be more common in the small intestine.
• Obstruction can be acute or chronic, partial or complete.
Etiologies:• Mechanical: hernias, volvulus, intussusception, tumors,
adhesions, congenital anomalies.• Non-mechanical: paralytic ileus (inhibition of
peristalsis) can be caused by abdominal surgery, peritonitis, rib fracture, concussion, spinal cord injury.

11/24/2015
18
Intestinal Obstruction: Manifestations:
• Abdominal distention
• Cramping and mid-abdominal pain (the more severe the pain is the higher up in the intestine is the obstruction)
• Vomiting
• Absolute constipation (occurs right away with large intestine obstruction, occurs after diarrhea and flatulence with the small intestine).

11/24/2015
19
Intestinal Obstruction: Pathogenesis:• Intra-luminal accumulation of gas and fluid close to
obstruction• Loss of water, electrolytes, decrease in ECF that could
potentially lead to hypovolemia and hypovolemic shock.
• Distention and ischemia of intestinal tube/wall, rapid proliferation of bacteria, perforation and release of bacteria/toxins into peritoneal cavity causing peritonitis and potentially sepsis.
Intestinal Obstruction: Treatment: timing of treatment very important
• Fluid/electrolyte correction
• Intubation and removal of the obstruction
• Control peritonitis and shock if present
Diverticulosis (diverticular disease): weakening and
out-pocketing of the wall of the GI tract.
• Can occur anywhere along the GI tract, but more typically occurs in the colon.
• The mucosal layer of the colon herniates through the muscularis layer. The diverticula develop between the longitudinal muscle bands of the haustra.

11/24/2015
20
Diverticulosis
Etiologies:
• Aging process
• Low residue diet and sedentary lifestyle
Manifestations during diverticulitis (inflammatory episode of the diverticula which accumulate bacteria):
• Diarrhea and/or constipation, flatulence
• Pain (lower abdomen) and bloating
• Most people remain asymptomatic
Diverticulosis
Complications:
• Bleeding and rupture of pockets
• Perforation, hemorrhage, peritonitis
• Fistula and abscess development

11/24/2015
21
Diverticulosis
Treatment:
• High residue diet (low residue during flare-ups)
• Temporary or permanent colostomy
• Anti-spasmotic drugs
• Antibiotics
• Surgery
Colorectal Cancer: Adenocarcinoma
Risk Factors:• Age• Genetics• Diet, fluid intake, exercise
Manifestations:• Fecal blood• Change in bowel habits• Diarrhea and/or constipation• Pain
Colon Cancer
Diagnosis: colonoscopy, blood tests (CEA)
Screening: Digital rectal exam, stool testing, colonoscopy
Treatment:
• Surgery, radiation, chemotherapy

11/24/2015
22

11/24/2015
23
Part 3: Appendicitis
Acute Appendicitis: infection and inflammation of the appendix
• Possible etiologies: viral infection, obstruction of the appendicular artery, fecalith (hardened stool that forms around vegetable fiber)
• Begins as an obstruction of outflow which causes a fluid build-up.
• There is inflammation and a bacterial over-growth.
• If untreated: necrosis and perforation, rupture of the appendix leading to peritonitis and potentially sepsis.

11/24/2015
24
Acute Appendicitis: Manifestations:
• Localized periumbilical pain that develops over a few days and suddenly shifts to the lower right quadrant. After rupture, the pain subsides for a short time and then fever and abdominal tenderness (board-like abdomen).
• Blood: increased inflammatory markers, increased WBCs
• Nausea, vomiting, anorexiaTreatment:
• Antibiotics, corticosteroids• Surgical removal