
BIMA Grafting: Why Do It ? (Evidence...
40
David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts of Interest:None BIMA Grafting: Why Do It ? (Evidence Basis) Advanced Techniques for State of the Art CABG Session AATS 2015
Transcript of BIMA Grafting: Why Do It ? (Evidence...

David P Taggart MD PhD FRCS FESC
Professor of Cardiovascular Surgery, University of Oxford
Conflicts of Interest:None
BIMA Grafting: Why Do It ? (Evidence Basis)
Advanced Techniques for State of the Art CABG Session
AATS 2015

SURVIVAL BENEFIT WITH A SINGLE IMA GRAFT
JACC 1995; 25; 188-82
o10 years after CABG, an IMA to the LAD risk of:
•death (x1.6), MI (x1.4), angina (x1.25), redo surgery (x2)
•Patency rate of > 95% at 10 years (veins = 25% - 50%)
If it was not for the IMA there would be no CABG today !!!

[JACC 1996]

IMA vs SVG vs RA
oMORPHOLOGY: IMA has thin smooth muscle media +tight internal elastic laminaoPHYSIOLOGY: IMA produces >NO in basal and stimulated states >RA >SVG
IMA RA SVG

% progression of native CAD
IMA SVG
Kitamura (1987) 18 46
Loop (1996) 39 67
Manninen (1998) 26 45
Hamada (2001) 12 38
Borges (2010) 17 44
AVERAGE 22 48
CIRC 2007
✗ impairs re-endothelialization, ✗ creates pro-thrombotic environment ✗ impairs distal endothelial function
Increased EDRFs (especiallyNO) produced by IMA results(i) in superior graft patency(ii) protects native coronary
artery circulation

o 43 patients (mortality 5%)o 6 BIMA (mortality 0%)o Graft Flow Measurements (45ml/min (range 30-60ml/min)o Repeat Angiography at 2-3 weeks 97% patency
If 1 IMA Better than 0 are 2 IMA better than 1 ?

% PATENCY RATES FOR BOTH IMA TO LEFT SIDED CORONARIES
STUDY NOS (%) TIME LIMA RIMA
Wendler (CIRC 2000) 172 (35%) 7days 98 97
Endo (CIRC 2002)1 1100 (98%) 7 days 98 98
Calafiore (JTCVS 2000) 295 (16%) 13 days 97 96
Calafiore (JTCVS 2002) 33 (22%) 3 years 100 100
Glineur (CIRC 2008) 299 (99%) 6 months 97 97
Dion (EJCTS 2000)2 161 (32%) 7 years 97 96
Tatoulis (Curr Op Cardiol 2011) 2176 10 years 91-97
Tatoulis (Curr Op Cardiol 2011) 440 10 years 89-95
1= vein graft patency 92%; 2= vein graft patency 72%
✔ Both IMA have similar patency when used to left sided coronaries
✔ Both IMA have similar patency when used as in situ or composite grafts
✗ INFERIOR PATENCY IF ANASTOMOSED TO AORTA
✗ INFERIOR PATENCY IF IMA ANASTOMOSED TO RCA
ANGIOGRAPHIC PATENCY OF BILATERAL IMA

Patency of RIMA to 20 years [Tatoulis et al Curr Op Cardiol 2011]

o4693 BIMA vs 11269 SIMA (from 7 databases) oMatched for age, gender, LV function, DMoHR for death with BIMA: 0.80 [ 95% CI=0.70 to 0.94] oNNT of 13-16 (to prevent one death)
Does Superior Angiographic Patency of BIMA Improve Survival ?
David P Taggart, Roberto D’Amico, Douglas G Altman [Lancet 2001]

[CIRC 2014]
15,583 patients followed for a mean of >9 years

ACS 2013

o3102 patients randomized to single or bilateral IMA grafts• primary outcome = 10 year survival (1 year = safety end point)•67 surgeons, 28 centres, seven countries•30 day mortality 1.2%, 1 yr mortality 2.4%•1 year incidence of stroke, MI, repeat revascularization all < 2%•Interim 5 year outcomes will be reported 2015

ART Surgery SIMA(n=1552)
BIMA (n=1542)
Δ
Off-Pump 40% 41.8%
Grafts
1 0.7% 0.5%
2 17.7% 17.8%
3 48.5% 50.4%
4+ 33.2% 31.3%
Surgery length: mins mean (SD) 199 (58) 222 (61) 23 mins
Ventilation length: mins mean (SD) 863 (3293) 968 (3029) 105 mins
Duration ITU stay: hours mean (SD) 38 (106) 41 (94) 3 hours
Duration of post-op stay: days mean (SD) 7.5 (7.6) 8.0 (7.4) 0.5 days
Re-exploration for any cause 3.5% 4.3%
Blood transfusion 12% 12%
Intra Aortic Balloon Pump 3.7% 4.4%
Renal support 4.4% 5.9%
82%
Wound Reconstruction 0.6% 1.9% Δ 1.3%
Increased incidence of wound reconstruction with BIMA: N N Harm 78ART was all comer so incidence might be lower by avoiding obese diabetics
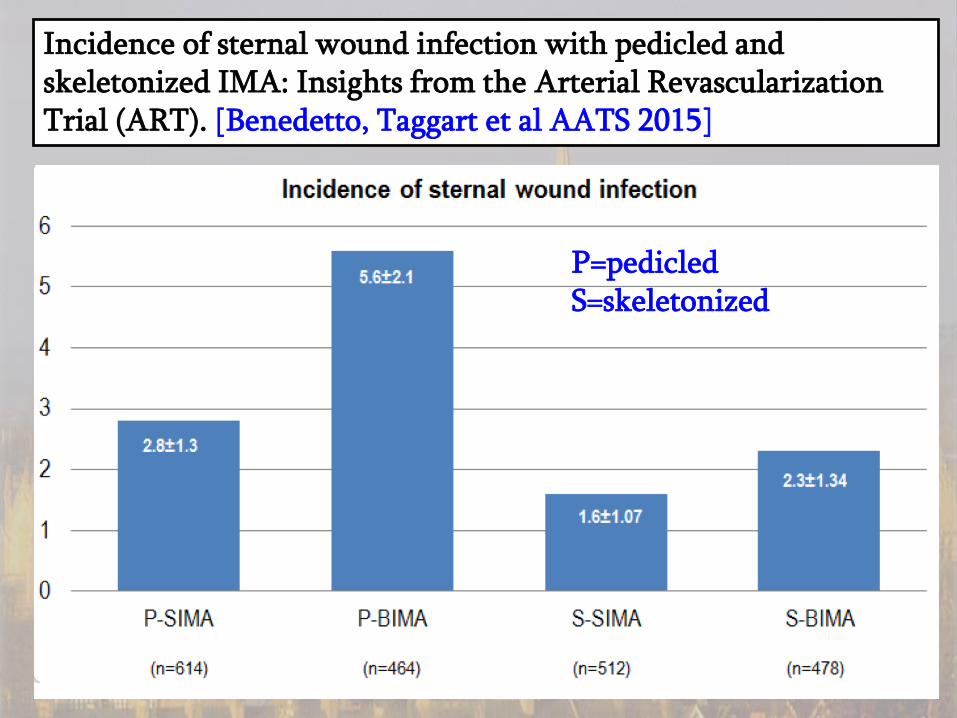
Incidence of sternal wound infection with pedicled and skeletonized IMA: Insights from the Arterial Revascularization Trial (ART). [Benedetto, Taggart et al AATS 2015]
P=pedicledS=skeletonized

SKELETONIZED
PEDICLED
2.8% 2.4%
1.7% 3.3%

STERNAL PERFUSION Skeletonized vs Non-Skeletonized [CIRC 2006]
greater reductions in sternal perfusion in diabetic patients
sk

Standard CABG with CPB vs OPCABG and Risk of Stroke
CONVENTIONAL CABG with CPB
Manoeuvre Requires Risk
1. CPB Connection
Aortic cannula STROKE
2. CPB CPB circulation SIRS/MOD
Cognitive dysfn
3. Stop heart Aortic clamp STROKE
4. Vein to aorta Aortic clamp STROKE
OPCABG
IMA +veins
-
-
-
OPCABG
Composite
Arteries
-
-
-
-
Composite arterial grafts based on in situ BIMA OPCABG eliminates any aortic manipulation (thereby minimizing the risk of stroke)

RR:0.46: 95% CI 0.29-0.72; p=0.0008
JTCVS 2011

BI MA SKELETONI Z ATI ON
• ARTERY
Longer and wider
See Full Lengt h
Easier composit es
Easier sequent ials
• CHEST WALL
Not denuded
Bet t er Healing
Less wound inf ect ion
Less Bleeding
Preparat ion: Harvest , divide dist ally and clip Wrap in papaverine swab + increase BP t o 150 f or 5 mins No need t o heparinize !!!! No need t o inj ect
When not t o use✗ Diabet es especially if insulin dependent and obese✗ Bad lungs (prolonged vent ilat ion)✗ Pat ient s on st eroids and immunosuppressives? Elderly

Summary and Conclusions
Strong evidence that with BIMA:
✔ Superior angiographic patency to vein grafts
✔ Superior long-term survival
✔ Skeletonization reduces wound infection/reconstruction
✔ Reduce risk of stroke as part of a No Touch Aortic Technique
✗ Increase sternal wound reconstruction (obese, diabetes, COPD)


BI MA: I n Sit u vs Composit e
RI MA
RI MA
RI MA
LI MA
LlI MA
LI MA
LAD
LAD
LAD
I nt d
Diag
OM
OM
OM
OM I nt d

ART OutcomesSIMA
(n=1552)BIMA
(n=1542)Δ
30 days
All Mortality 1.2% 1.2%
CVA 1.2% 1.0%
MI 1.5% 1.4%
Revasc 0.4% 0.7%
Wound reconstruction 0.6% 1.9% 1.3%
1 year
All Mortality 2.3% 2.5%
CVA 1.8% 1.5%
MI 2.0% 2.0%
Revasc 1.3% 1.8%
Increased incidence of wound reconstruction with BIMA: NNH 78ART was all comer so incidence might be lower by avoiding obese diabetics

o5 RCTs including 936 patientso71% repeat angiography at mean of 22 months (range 10-52 months)oFailure rate 14.1% RA and 14.6% SVG
o35 studies with angiographic patency rates: OR for RA patency vs SVGoEarly patency (<1 yr; 6795 grafts): OR 1.04 (95% CI=0.68-1.61)oMedium-term patency (1-5 yrs; 3232 grafts): OR 2.06 (95% CI=1.29-3.29)oLong-term patency (<5 yrs; 1157 grafts): OR 2.28 (95% CI=1.32-3.94)
JTCVS 2010
EJCTS 2011

[CIRC 2008]
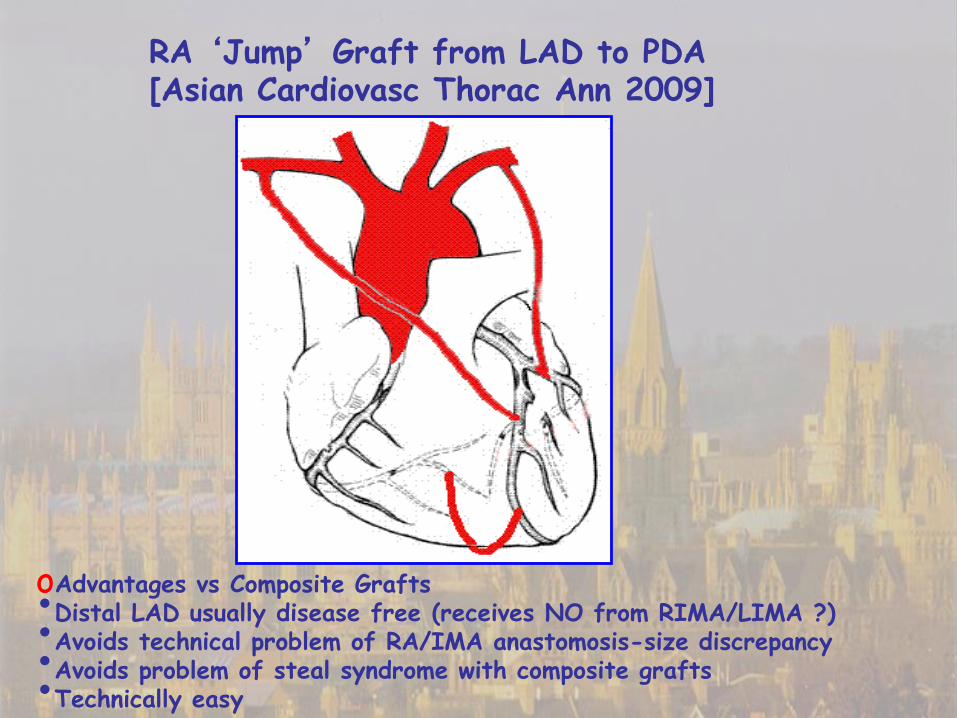
oAdvantages vs Composite Grafts•Distal LAD usually disease free (receives NO from RIMA/LIMA ?)•Avoids technical problem of RA/IMA anastomosis-size discrepancy•Avoids problem of steal syndrome with composite grafts•Technically easy
RA ‘Jump’ Graft from LAD to PDA [Asian Cardiovasc Thorac Ann 2009]

JACC 2012
o 510 patients RCTo RA/SVG to RCA or Circumflexo 269 patients late angiography at mean of 7.7 yearso Graft occlusion 8.9% RA vs 18.6% SVG (p=0.002)o Functional occlusion 12% RA vs 19.7% SVG (p=0.03)

[EJCTS 2015]

7 YEARS number % patent p
LIMA 514 96%
RA 629 83% 0.001
RIMA 58 88% 0.32
Free IMA 55 80% 0.6
SVG 171 82 0.77
[EJCTS 2012]

[ATS2014]

No…but probably 80%-90%✔ Younger patients survival advantage✔ Older patients ‘No Touch Aortic Technique’
Best angiographic evidence favours RIMA > RA
Total Arterial Revascularization For All ?
✗ General ContraindicationsPoor LV (EF <30%)Large RCA with moderate stenosis needs SVG or stent
✗ BIMA contraindicationsObese diabeticsBad lungsSteroids/immunosuppresants

[JTCVS 2010]
< 70 years > 70 years
BUT: All RIMA anastomosed to aorta = inferior patency
RCT: RA vs RIMA

[CIRC 2011]

2 different hospitalsIMA harvested as pediclesIMA: aortic anastomosis
RA BIMA p
Death 0.6% 1.7% 0.08
CVA 0.8 2.1 0.07
SWI 1.1 2.7 0.07
[EJCTS 2015]

[ATS 2014]

Summary and Conclusions
o STRONG ANGIOGRAPHIC EVIDENCE OF SUPERIOR PATENCY OF
• both IMA vs SVG
• RA vs SVG
• IMA vs RA (in studies out to 20 years)
o CLINICAL EVIDENCE
• Strong evidence of improved survival with BIMA vs SVG
• Strong evidence of improved survival with RA vs SVG
• One small RCT of RA vs RIMA (but RIMA anastomosed to aorta)
• One small PPM reported superior survival and MACCE with RIMA vs RA
• One PPM reported superior survival and MACCE with RA vs RIMA (but with RIMA anastomosed to aorta as a free graft)
o Best evidence still supports RIMA as 2nd best arterial grafto For BIMA avoid obese diabetes and skeletonizeo But RA a good alternative when contraindications to RIMA

oNo large randomized trials
o Angiographic evidence of • patency of BIMA• patency of RA (vs SVG)
o Clinical evidence for survival benefit of • BIMA• RA
o Comparison of clinical outcomes of RIMA vs RA
oWhen may RA possibly be preferable to RIMA ?
RIMA or RA as the Second Arterial Graft ?

66%
79%

JAHA 2013

2780 patients1620 angiogramsMean 7.7 years FURIMA (145)RA (871)RGEA (92)SVG (845): HR x3 Failure
ALL
> 4 years


















