Billing Guide
24
PLEASE SEE ACCOMPANYING FULL PRESCRIBING INFORMATION. Erwinaze ™ (asparaginase Erwinia chrysanthemi) For Injection Billing Guide for Hospital Outpatient Departments Indicated as a component of a multiagent chemotherapeutic regimen for the treatment of patients with acute lymphoblastic leukemia (ALL) who have developed hypersensitivity to Escherichia coli–derived asparaginase.
-
Upload
sweeks9046 -
Category
Documents
-
view
81 -
download
5
description
Overview of Types of Payers, Hospital Billing rules and forms used for billing.
Transcript of Billing Guide

PleAse see ACCOMPANYING Full PresCrIbING INFOrMAtION.
Erwinaze™ (asparaginase Erwinia chrysanthemi)For Injection
Billing Guide for Hospital Outpatient Departments
Indicated as a component of a multiagent chemotherapeutic regimen for the treatment of patients with acute lymphoblastic leukemia (All) who have developed hypersensitivity to Escherichia coli–derived asparaginase.

Erwinaze™ (asparaginase Erwinia chrysanthemi)

Contents Introduction .................................................................................................................................................... 2
Overview of Coverage ..................................................................................................................................... 2
Private Payers............................................................................................................................................ 3
Medicaid ..................................................................................................................................................... 4
Medicare .................................................................................................................................................... 5
Reimbursement for Erwinaze and Intramuscular Chemotherapy Administration ..................................... 6
Private Payers............................................................................................................................................ 6
Medicaid ..................................................................................................................................................... 7
Original Medicare Part B .......................................................................................................................... 8
Hospital Outpatient Department Coding ....................................................................................................... 9
HCPCS Codes ............................................................................................................................................ 9
National Drug Code ................................................................................................................................. 10
Coding for Administration of Chemotherapy ......................................................................................... 11
International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnosis Codes .................................................................................................................. 11
ICD-9-CM Procedure Codes ................................................................................................................... 12
Revenue Codes ........................................................................................................................................ 12
Sample CMS-1450 (UB-04): ErwinazeTM (asparaginase Erwinia chrysanthemi) For Injection .................... 13
Sample Letter of Medical Necessity for ErwinazeTM (asparaginase Erwinia chrysanthemi) For Injection .... 14
Sample Claim Denial Appeal Letter for ErwinazeTM (asparaginase Erwinia chrysanthemi) For Injection .... 17
Strategies to Appeal Denied Claims for ErwinazeTM (asparaginase Erwinia chrysanthemi) For Injection .... 19
Hospital Outpatient Coding for Erwinaze .................................................................................................... 20
Additional Hospital Outpatient Coding for Erwinaze................................................................................... 21
EUSA Pharma (USA), Inc.
BILLING GUIDE

Erwinaze™ (asparaginase Erwinia chrysanthemi)
2
IntroductionEUSA Pharma (USA), Inc., has developed this billing guide as a reference for general coding, coverage, payment, and reimbursement information related to Erwinaze™ (asparaginase Erwinia chrysanthemi). Many factors influence how payers cover and pay for Erwinaze, including the site of service, the type of health insurance a patient may have, and the type of benefits various payers may offer.
This guide is intended to support hospital pharmacy and billing staff when Erwinaze is administered in the hospital outpatient department. To assist you in preparing claims for Erwinaze, this guide contains the following:l General coverage overview for Medicare, Medicaid, and private payersl Coding options and payment information for Erwinaze, including coding for the drug, the diagnosis, and the
administration procedurel Sample claim form for Erwinaze l Sample letter of medical necessity (LOMN)l Strategies to appeal denied claims and sample claims appeal letterl Information about hotline services for reimbursement and patient assistance
These materials are provided as information only. Payer polices vary; therefore, you should contact payers directly to understand local payment policies. For more information about coverage and reimbursement for Erwinaze, contact the Hotline by calling 888-837-4397 or go to www.erwinaze.com. Hotline case managers are available Monday through Friday, from 8:00 am to 5:00 pm CST.
Overview of CoverageCoverage, coding, and payment guidelines for Erwinaze vary by payer. Contacting each patient’s insurance company to understand coverage, coding, and payment guidelines for Erwinaze is recommended.

BILLING GUIDE
3EUSA Pharma (USA), Inc.
Private PayersPrivate insurance coverage policies for Erwinaze vary from plan to plan. Each private insurer determines its own coverage policies for drugs and procedures. In addition, most insurers offer multiple insurance plans; coverage for procedures and/or drugs may vary depending on the plan in which a patient is enrolled. For example, certain plans may require prior authorization for Erwinaze before coverage is allowed, whereas other plans may not. If you determine Erwinaze is medically necessary, you should contact the insurer to verify coverage requirements and request prior authorization, if necessary.
Although most private payers cover chemotherapy cancer treatment and biologics that are new to market, some may impose requirements such as:l Prior authorizationl Step therapyl Quantity limits
Some payers do not require prior authorization, but may require additional documentation to support a claim for a new drug. It may be helpful to provide additional documentation to help the payer verify the medical necessity for treatment with Erwinaze, such as:l Letter of medical necessity (see template in the back section of this guide)l FDA approval letterl Package insertl Chart notesl Additional medical documentation (eg, lab and test results, previously tried therapies, list of all current medications,
diagnostic history, previous or planned surgeries)l Invoicel Average Wholesale Price (AWP) or Wholesale Acquisition Cost (WAC) as published in a pricing compendium
(eg, Red Book™ or First DataBank®)
For information about Erwinaze coverage for your patients with private insurance, please call the Hotline at 888-837-4397.

Erwinaze™ (asparaginase Erwinia chrysanthemi)
4
MedicaidTraditional Medicaid: In general, state Medicaid programs cover drugs for their FDA-approved indications and may provide coverage for other indications, particularly when those indications are supported by pharmaceutical compendia listings. It is important to understand your state Medicaid program’s specific coverage criteria for Erwinaze. Each state’s Medicaid agency determines its own coverage and payment policies.
Managed Medicaid: Many states enroll Medicaid beneficiaries in managed Medicaid plans or offer one or more managed Medicaid plans as options to replace traditional Medicaid.1 These plans share many of the characteristics of private managed care plans, including utilization management strategies such as prior authorization. Erwinaze coverage for patients in managed Medicaid plans varies by plan.
Although most Medicaid plans cover chemotherapy cancer treatment, some may impose requirements such as:l Prior authorizationl Step therapyl Quantity limitsl Mandatory acquisition through a specialty pharmacy
Medicaid plans have varying requirements for supplemental documentation for a new drug, but, in general, they may request:l Drug namel Dose/strengthl Route of administrationl Diagnosisl 11-digit National Drug Code (NDC)l Prior authorization approval number (if applicable)
Some programs or plans that do not require prior authorization may require additional documentation to support a claim for a new drug. If you are filing a claim to a payer that accepts paper claims, it may be helpful to attach additional documentation to help the Medicaid plan verify the medical necessity for treatment with Erwinaze. Appropriate documentation may include:l Referral numberl Letter of medical necessity (see template in the back section of this guide)l FDA approval letterl Package insertl Chart notesl Additional medical documentation (eg, lab and test results, previously tried therapies, list of all current medications,
diagnostic history, previous or planned surgeries)l Invoicel AWP or WAC as published in a pricing compendium (eg, Red Book or First DataBank)
1The Kaiser Family Foundation, Managed Medicaid Enrollment, statehealthfacts.org. http://www.statehealthfacts.org/comparemaptable.jsp?ind=216&cat=4. Accessed August 6, 2011.

BILLING GUIDE
5EUSA Pharma (USA), Inc.
MedicareOriginal Medicare provides eligible beneficiaries with medical benefits through these programs: l Medicare Part A: Covered services include, but are not limited to, inpatient services, hospice care, skilled nursing
facility stays, and some home health servicesl Medicare Part B: Covered benefits include, but are not limited to, physicians’ professional services, hospital outpatient
services, injected or infused drugs that cannot be self-administered, certain other specific drug types, durable medical equipment (DME), clinical laboratory services, other diagnostic services, and some home health services
In general, original Medicare Part B covers an injected or infused drug that is administered in a hospital outpatient setting, such as Erwinaze, when the drug is2:l FDA approvedl Provided incident to a physician’s servicel Not usually self-administeredl Considered reasonable and necessary for its prescribed use
However, the likelihood of Erwinaze patients being covered by Medicare is very low. For information about current Medicare coverage for beneficiaries you treat, please call the Hotline at 888-837-4397.
Medicare Advantage (MA) is the Medicare managed care program. MA plans must at a minimum provide all of the benefits that Original Medicare Part A and Part B provide, but may provide additional benefits as well.
2Medicare Benefit Policy Manual, Chapter 15, Covered Medical and Other Health Services, §50.

Erwinaze™ (asparaginase Erwinia chrysanthemi)
6
reimbursement for erwinaze and Intramuscular Chemotherapy Administration
Private Payers Managed care organizations and other private payers may reimburse hospitals for injected or infused drugs in the outpatient setting using various methodologies, including:l Percentage of AWP l Percentage of Average Sales Price (ASP), after ASP is establishedl Percentage of WAC l Invoice Cost or Cost-Plus l Other or hybrid methodology
Private payers also use various methods to determine hospital outpatient reimbursement for other services associated with Erwinaze therapy, such as intramuscular administration and hospital clinic visits (facility fees). These methodologies may include:l Fee-schedule reimbursement based on a variation of the Medicare Ambulatory Payment Classification (APC) or
another bundled payment methodology with possible negotiated carve-outsl Per diem rates with possible negotiated carve-outsl Global rates for certain specified diagnoses
Some private payers may also pay a global rate that includes payment for infused and injected drugs provided by the hospital during the patient encounter.
The patient cost-share for Erwinaze and associated administration services varies from plan to plan. For example, some patients may have to meet a yearly deductible and then pay either a flat co-payment or a percentage coinsurance. An important step in performing patient-specific benefit verifications prior to initiating therapy includes confirming the patient’s out-of-pocket costs for therapy with Erwinaze so he or she can plan ahead for treatment-related expenses.

BILLING GUIDE
7EUSA Pharma (USA), Inc.
MedicaidErwinaze may be reimbursed separately by state Medicaid programs when administered in the hospital outpatient setting, although some states may opt to pay a bundled rate that includes Erwinaze and other outpatient services provided on the same day. Coverage polices and reimbursement methodologies for Erwinaze and associated facility services vary by state and by plan. Medicaid beneficiaries may have some cost-sharing responsibility for Erwinaze, but these amounts are typically nominal.
When a Medicaid plan pays a hospital separately for outpatient drugs, the plan may reimburse for injected drugs based on a variety of methodologies, including:l Percentage of AWP l Percentage of ASP (after ASP is established) l Percentage of WACl Invoice
Medicaid programs and plans use many of the same methods that private payers use to reimburse hospitals for outpatient services, such as drug administration, clinic visits, and other services related to Erwinaze.
It is particularly important to conduct patient-specific verifications for Medicaid beneficiaries before each scheduled appointment since, in many states, enrollees have the opportunity to switch their plans every month. Therefore, eligibility can change frequently for these patients. The Hotline can assist providers with reimbursement research, including patient-specific benefit verifications for Medicaid patients. Please contact the Hotline to request patient-specific benefit verification at 888-837-4397.

Erwinaze™ (asparaginase Erwinia chrysanthemi)
8
Original Medicare Part b Original Medicare Part B reimbursement for services provided in a hospital outpatient setting is made under a payment system with specific drug carve-outs, known as the Hospital Outpatient Prospective Payment System (OPPS). Original Medicare Part B pays for Erwinaze when it is administered in a hospital outpatient department, in addition to payment for other covered items and services provided to a patient during the same encounter. Until Erwinaze receives a unique Healthcare Common Procedure Coding System (HCPCS) code (see coding section, page 9) or obtains transitional pass-through status, Medicare reimbursement to hospital outpatient departments for Erwinaze will be based on 95% of AWP. If awarded transitional pass-through status by Medicare, reimbursement for Erwinaze will be 106% of ASP or 106% of WAC during 2011, updated quarterly.3 As a new product, Erwinaze will most likely establish an ASP after at least 2 calendar quarters following initial market availability.
Medicare will also pay the hospital a bundled payment for intramuscular chemotherapy administration of Erwinaze. The bundled payment includes reimbursement for all facility fees associated with the procedure, including room charges, injection supplies (excluding the drug injected), personnel costs, and indirect overhead expenses.
Medicare reimburses hospitals 80% of the established allowable for the drug and the intramuscular injection. The remaining 20% is the responsibility of the patient or secondary insurance coverage. Many Medicare beneficiaries have some form of supplemental insurance that will assist with paying the coinsurance and deductible required under Part B.4 It is important for hospitals to routinely collect and update secondary insurance information from all Medicare patients.
Reimbursement for services provided by an MA plan is negotiated between the MA plan and participating providers and may therefore differ significantly from reimbursement for the same service covered by Original Medicare.
3Medicare Claims Processing Manual, Chapter 17, Drugs and Biologicals, § 20.1.2 – Average Sales Price (ASP) Payment Methodology.4MedPAC, Section 6, A Data Book: Healthcare Spending and the Medicare Program, June 2009.

BILLING GUIDE
9EUSA Pharma (USA), Inc.
Hospital Outpatient Department Coding
HCPCs CodesMost payers recognize HCPCS codes for reporting specific services such as drugs, biologics, supplies, and medical equipment.5 As a new drug, Erwinaze has not yet been assigned a permanent, unique HCPCS code. Until Erwinaze receives a permanent HCPCS code, hospital outpatient departments may bill using an unclassified (miscellaneous) HCPCS code, such as:
Payer Type HCPCS Code Description
Non-Medicare Patients
J9999* Not otherwise classified, antineoplastic drugs
J3590* Unclassified biologics
J3490* Unclassified drugs
Medicare Patients Only C9399 Unclassified drugs or biologicals
* HCPCS code J9999 should generally be used to report Erwinaze. HCPCS codes J3590 and J3490 should be used ONLY if mandated by a payer. Many payers have a policy of paying for the intramuscular administration of a chemotherapy code ONLY when a drug in the J9xxx series is used to report the provision of the drug. The use of J3590 or J3490 instead of J9999 will cause the intramuscular injection code to be denied by many payers.
Because miscellaneous HCPCS codes such as those shown in the table above do not provide payers with the product-specific information they need to determine coverage and reimbursement for a drug, billers must provide additional information on each claim form. As illustrated in the UB-04 claim example on page 13, when a miscellaneous drug code must be used in Field Locater (FL) 44, additional information must typically be included in FL80 (Remarks). The additional information required varies by payer, but typically includes:l Drug name (brand/generic)l Route of administrationl The amount of drug used to treat the patient (including any documented wastage from a single-dose vial, but
excluding overfill)l 11-digit NDC
Payers may require additional information, such as a copy of the invoice or notes from the patient’s medical record.
Unclassified codes are generally reported as “1 unit” in FL46 (Service Units) of the UB-04 claim form or its electronic equivalent, regardless of the amount of drug administered. Some payers may require reporting 1 unit per vial used. Check payer guidelines for appropriate reporting of units for an unclassified code.
5Healthcare Common Procedure Coding System Level II, 2011 Expert, Ingenix, 2010.

Erwinaze™ (asparaginase Erwinia chrysanthemi)
10
National Drug CodeMedications listed under Section 510 of the US Federal Food, Drug, and Cosmetic Act are assigned a unique, 3-segment number, known as the National Drug Code (NDC).6 The first segment, known as the labeler code, is assigned by the Food and Drug Administration (FDA) for the specific manufacturer. The second segment, known as the product code, identifies a specific drug, strength, and dosage form of that drug. The third segment, known as the package code, identifies the package size.
When reporting a miscellaneous HCPSC code, payers may require that providers report the NDC. The FDA has assigned the following NDCs to Erwinaze:
NDC Total International Units
57902-249-05Contains 5 vials. Each single vial contains 10,000 International Units of asparaginase Erwinia chrysanthemi, for a total of 50,000 International Units
57902-249-01 Single vial containing 10,000 International Units of asparaginase Erwinia chrysanthemi
NDCs (including the NDC for Erwinaze) are often shown in the package insert and certain other locations using the FDA-approved 10-digit format. Whenever a health plan requires the use of an NDC on the UB-04 claim form, the 10-digit NDC must be converted to an 11-digit format. To do so, the 3 numbered segments described above are converted to a 5-digit/4-digit/2-digit format that requires a strategically placed zero. For example, the 10-digit NDC for Erwinaze is converted as follows:
10-Digit Format
Erwinaze 10-Digit Example
11-Digit FormatErwinaze 11-Digit Example
Reporting on CMS Claim Form
5-3-2 57902-249-05 5-4-2 57902-0249-05 57902024905
5-3-2 57902-249-01 5-4-2 57902-0249-01 57902024901
Hyphens are not used when entering the NDC on the claim form.
HCPCS billing units and the NDC quantity are usually not the same number. Check payer-specific NDC-reporting requirements for reporting HCPCS units and NDC quantities, and any requirements for NDC code placement on the claim.
Most Medicaid plans require providers to list a drug’s NDC on the UB-04 claim form in addition to the HCPCS code. Medicare claims that will cross over to Medicaid as the secondary payer must contain both the HCPCS code and the NDC code.
6United States Food and Drug Administration, National Code Directory.

BILLING GUIDE
11EUSA Pharma (USA), Inc.
Coding for Administration of Chemotherapy Recommended dose7:— To substitute for a dose of pegaspargase: The recommended dose is 25,000 International Units/m2 administered
intramuscularly 3 times a week (Monday/Wednesday/Friday) for 6 doses for each planned dose of pegaspargase
— To substitute for a dose native E coli asparaginase: The recommended dose is 25,000 International Units/m2 administered intramuscularly for each scheduled dose of native E coli asparaginase within a treatment
Current Procedural Terminology (CPT) codes are used by hospitals to report the intramuscular administration of Erwinaze in the outpatient setting to Medicare and to certain other payers. When billing for the facility services associated with the administration of Erwinaze in the hospital outpatient setting, the following CPT code reserved for chemotherapy and other highly complex drugs and biologic agents may be appropriate8:
CPT Code Description
96401Chemotherapy administration, subcutaneous or intramuscular; nonhormonal antineoplastic
International Classification of Diseases, Ninth revision, Clinical Modification (ICD-9-CM) Diagnosis Codes ICD-9-CM diagnosis codes are used to report diseases and conditions.9 ICD-9-CM diagnosis codes help describe why Erwinaze was medically necessary for the treatment of the patient. Coding to the highest level of specificity is required by most payers. The following ICD-9-CM diagnosis codes may be appropriate to describe patients with acute lymphoblastic leukemia (ALL).
Code DescriptionAcute Lymphoid Leukemia ICD-9-CM Diagnosis Codes Require a Fifth Digit
204.00 Lymphoid leukemia, acute Without mention of having achieved remission, failed remission
204.01 In remission
204.02 In relapse
7Erwinaze™ (asparaginase Erwinia chrysanthemi) prescribing information. Langhorne, PA: EUSA Pharma (USA), Inc.; November 2011. 8Current Procedural Terminology CPT 2011, Professional Edition, American Medical Association, 2010.9International Classification of Diseases, Ninth Revision, Clinical Modification, 6th Edition, 2011 Expert, Ingenix, 2010.

Erwinaze™ (asparaginase Erwinia chrysanthemi)
12
ICD-9-CM Procedure CodesHospitals and other facilities typically use ICD-9-CM procedure codes to report services provided to inpatients. However, some hospital outpatient departments may choose to itemize ICD-9-CM procedure codes on claim forms for their own internal tracking purposes. The following ICD-9-CM procedure code may be appropriate for reporting Erwinaze in the hospital outpatient setting.
Code Description
99.25 Injection or infusion of cancer chemotherapeutic substance
revenue CodesRevenue codes assign services and supplies to specific hospital cost centers. The following revenue codes may be used to report services and supplies that are utilized during the course of therapy with Erwinaze.
Revenue Code Description
0636 Drugs requiring detailed coding
0250 Pharmacy, general
0331 Chemotherapy injected
Medicare Part B recommends (but does not require) that hospitals use Revenue Code 0636 on claim lines where separately payable drugs such as Erwinaze are reported.
For information about current coding requirements for Erwinaze, please call the Hotline at 888-837-4397.

BILLING GUIDE
13EUSA Pharma (USA), Inc.
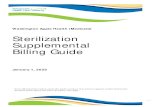
This document is provided for your guidance only.
Fields 42-43: Enter the appropriate revenue code and description corresponding to the HCPCS code in Field 44; eg,- 0636 for Erwinaze- 0331 Chemotherapy
injected
Field 44: Enter appropriate HCPCS and/or CPT codes
Drug: C9399 for Erwinaze
Drug Administration: 96401 Chemotherapy administration, subcutaneous or intramuscular; nonhormonal antineoplastic
Field 46: Enter appropriate number of service units; eg, enter 1 unit for HCPCS code C9399
Field 80 (Remarks)When a "not otherwise classified" code such as C9399, J9999, J3490, or J3590 is used in Field 44, most payers require detailed information about the drug in Field 80. Typically, payers require the drug name, the NDC, the amount of drug used to treat the patient (including any documented, unavoidable wastage in single-dose vials, but excluding any overfill), and route of administration
0636 Drugs requiring detailed coding C9399 MMDDYY 1 XXX XX 0331 Chemotherapy injected 96401 MMDDYY 1 XXX XX
XXX.XX
Most providers today use the electronic equivalent of the CMS-1450 (UB-04) instead of the paper version. Although the paper and electronic (ASC837I) formats are different, the revenue codes, HCPCS/CPT codes, and ICD-9-CM diagnosis codes are the same regardless of the reporting format. Both paper and electronic claims require the detail shown in Field 80 to identify Erwinaze.
Fields 67 and 67A-67Q: Enter appropriate ICD-9-CM diagnosis code for ALL such as 204.00, 204.01, or 204.02, and other documented diagnosis or supplementary codes, as appropriateNote: Other diagnosis codes may be applicable
sample CMs-1450 (ub-04): erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection

Erwinaze™ (asparaginase Erwinia chrysanthemi)
14
sample letter of Medical Necessity for erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection
Many payers require prior authorization in order to cover treatment with Erwinaze. Some payers may require supporting documentation in order to process a claim for payment following Erwinaze therapy. Prior authorization allows the payer to review the reason for the requested therapy to determine medical appropriateness. A patient-specific letter of medical necessity will help explain the physician’s rationale and clinical decision making in choosing Erwinaze therapy. Please note that some payers may have specific forms that must be completed in order to request prior authorization or to document medical necessity. The following is a template letter of medical necessity for Erwinaze therapy that can be customized based on your patient’s medical history and demographic information.

BILLING GUIDE
15EUSA Pharma (USA), Inc.
[Date][Contact Name of medical director or other payer representative][Contact Title][Name of Health Insurance Company][Address][City, State, Zip Code]Insured: [Name]Policy Number: [Number]Group Number: [Number]
Dear [Insert appropriate contact name or department]:
I am writing on behalf of my patient, [name of patient], to [request prior authorization/document medical necessity] for treatment with Erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection. The patient will be/was treated with Erwinaze for [patient’s diagnosis]. Erwinaze is an asparagine-specific enzyme indicated as a component of a multiagent chemotherapeutic regimen for the treatment of patients with acute lymphoblastic leukemia (ALL) who have developed hypersensitivity to Escherichia coli–derived asparaginase.1 Its use is based on the following:• Asparaginase is the cornerstone of pediatric ALL therapy2 and has shown improved outcomes3-6
• Maintaining depletion of asparagine is the key to improving outcomes with asparaginase2
• Completing the planned dosing regimen of asparaginase is a crucial part of ALL treatment to improve event-free survival7,8
• Hypersensitivity is a common side effect of asparaginase treatment and is often the reason for discontinuation of asparaginase9
• Erwinaze is an alternative to E coli–derived asparaginases in patients with hypersensitivity • There is no cross-reactivity between Erwinaze and E coli–derived asparaginases, but there is cross-
reactivity between native E coli asparaginase and pegylated asparaginase10,11
• Switching to Erwinaze following hypersensitivity to E coli–derived asparaginase maintains treatment outcomes12
Patient History and Diagnosis[Name of patient] is a [age]-year-old [male/female] diagnosed with [diagnosis] as of [date]. [Name of patient] has been in my care for [patient’s diagnosis] since [date]. As a result of [patient’s diagnosis], [he/she] [describe resulting condition, including results from any relevant patient assessments]. Additionally, [patient] has previously tried and failed the following treatments [include other drugs or therapies tried, including details of any noncompliance, poor response, or adverse events].
[Provide a brief discussion of patient’s symptoms and therapy to date]. Based on the above facts, the use of Erwinaze is medically necessary and consistent with the FDA approval for Erwinaze. If you have any further questions, please feel free to call me at [physician telephone number, including area code] to discuss. Thank you in advance for your immediate attention to this request.
Sincerely,[Physician’s name][Physician’s practice or hospital name] Attachments [references, additional supporting documents]

Erwinaze™ (asparaginase Erwinia chrysanthemi)
16
references for sample letter of Medical Necessity for erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection
References
1. Erwinaze™ (asparaginase Erwinia chrysanthemi) prescribing information. Langhorne, PA: EUSA Pharma (USA), Inc.; November 2011.
2. Pieters R, Hunger SP, Boos J, et al. L-asparaginase treatment in acute lymphoblastic leukemia. Cancer. 2011;117:238-249.
3. Ortega JA, Nesbit ME, Donaldson MH, et al. L-asparaginase, vincristine, and prednisolone for induction of first remission in acute lymphocytic leukemia. Cancer Res. 1977;37:535-540.
4. Sallan SE, Hitchcock-Bryan S, Gelber R, et al. Influence of intensive asparaginase in the treatment of childhood non-T-cell acute lymphoblastic leukemia. Cancer Res. 1983;43:5601-5607.
5. Pession A, Valsecchi MG, Masera G, et al. Long-term results of a randomized trial on extended use of high dose L-asparaginase for standard risk childhood acute lymphoblastic leukemia. J Clin Oncol. 2005;23:7161-7167.
6. Amylon MD, Shuster J, Pullen J, et al. Intensive high-dose asparaginase consolidation improves survival for pediatric patients with T cell acute lymphoblastic leukemia and advanced stage lymphoblastic lymphoma: a Pediatric Oncology Group study. Leukemia. 1999;13:335-342.
7. Ogawa C, Ohara A, Manabe A, et al. Tokyo Children’s Cancer Study Group (TCCSG) Study L99–15 [abstract]. Blood. 2005;106. Abstract 878.
8. Silverman L, Gelber RD, Kimball Dalton V, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97:1211-1218.
9. Raetz EA, Salzer WL. Tolerability and efficacy of L-asparaginase therapy in pediatric patients with acute lymphoblastic leukemia. J Pediatr Oncol. 2010;32:554-563.
10. Wang B, Relling MV, Storm MC, et al. Evaluation of immunologic crossreaction of antiasparaginase antibodies in acute lymphoblastic leukemia (ALL) and lymphoma patients. Leukemia. 2003;17:1583-1588.
11. Zalewska-Szewczyk B, Gach A, Wyka K, et al. The cross-reactivity of anti-asparaginase antibodies against different L-asparaginase preparations. Clin Exp Med. 2009;9:113-116.
12. Vrooman LM, Supko JG, Neuberg DS, et al. Erwinia asparaginase after allergy to E. coli asparaginase in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2010;54:199-205.

BILLING GUIDE
17EUSA Pharma (USA), Inc.
sample Claim Denial Appeal letter for erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection
[Date][Contact][Title][Name of Health Insurance Company][Address][City, State, Zip Code]Insured: [Patient name]Policy Number: [Policy number]Group Number: [Group number]Diagnosis: [Diagnosis and ICD-9-CM code]
Dear [Name of contact]:
This letter serves as a request for reconsideration of a claim representing charges for Erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection administered to [patient name] on [date(s) of service]. [Patient name] has been under my treatment for [his/her] diagnosis of [diagnosis]. You have indicated that Erwinaze is not covered by [insurance name] because [reason for denial].
Erwinaze is an asparagine-specific enzyme indicated as a component of a multiagent chemotherapeutic regimen for the treatment of patients with acute lymphoblastic leukemia (ALL) who have developed hypersensitivity to Escherichia coli–derived asparaginase.1 Its use is based on the following:• Asparaginase is the cornerstone of pediatric ALL therapy2 and has shown improved outcomes3-6
• Maintaining depletion of asparagine is the key to improving outcomes with asparaginase2
• Completing the planned dosing regimen of asparaginase is a crucial part of ALL treatment to improve event-free survival7,8
• Hypersensitivity is a common side effect of asparaginase treatment and is often the reason for discontinuation of asparaginase9
• Erwinaze is an alternative to E coli–derived asparaginases in patients with hypersensitivity• There is no cross-reactivity between Erwinaze and E coli–derived asparaginases, but there is cross-reactivity
between native E coli asparaginase and pegylated asparaginase10,11
• Switching to Erwinaze following hypersensitivity to E coli–derived asparaginase optimizes treatment outcomes12
Because of [insert relevant patient information—history, diagnosis, etc], I have administered Erwinaze as a medically necessary part of this patient’s treatment and would appreciate your reconsideration of the [date of service] claim for [patient name]. Please contact me at [physician telephone number, including area code] if you require additional information.
Thank you in advance for your immediate attention to this request.
Sincerely,
[Physician’s name][Physician’s practice or hospital name]
Attachments [references, original claim form, denial/explanation of benefits [EOB], additional supporting documents]

Erwinaze™ (asparaginase Erwinia chrysanthemi)
18
references for sample Claim Denial Appeal letter for erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection
References
1. Erwinaze™ (asparaginase Erwinia chrysanthemi) prescribing information. Langhorne, PA: EUSA Pharma (USA), Inc.; November 2011.
2. Pieters R, Hunger SP, Boos J, et al. L-asparaginase treatment in acute lymphoblastic leukemia. Cancer. 2011;117:238-249.
3. Ortega JA, Nesbit ME, Donaldson MH, et al. L-asparaginase, vincristine, and prednisolone for induction of first remission in acute lymphocytic leukemia. Cancer Res. 1977;37:535-540.
4. Sallan SE, Hitchcock-Bryan S, Gelber R, et al. Influence of intensive asparaginase in the treatment of childhood non-T-cell acute lymphoblastic leukemia. Cancer Res. 1983;43:5601-5607.
5. Pession A, Valsecchi MG, Masera G, et al. Long-term results of a randomized trial on extended use of high dose L-asparaginase for standard risk childhood acute lymphoblastic leukemia. J Clin Oncol. 2005;23:7161-7167.
6. Amylon MD, Shuster J, Pullen J, et al. Intensive high-dose asparaginase consolidation improves survival for pediatric patients with T cell acute lymphoblastic leukemia and advanced stage lymphoblastic lymphoma: a Pediatric Oncology Group study. Leukemia. 1999;13:335-342.
7. Ogawa C, Ohara A, Manabe A, et al. Tokyo Children’s Cancer Study Group (TCCSG) Study L99–15 [abstract]. Blood. 2005;106. Abstract 878.
8. Silverman L, Gelber RD, Kimball Dalton V, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97:1211-1218.
9. Raetz EA, Salzer WL. Tolerability and efficacy of L-asparaginase therapy in pediatric patients with acute lymphoblastic leukemia. J Pediatr Oncol. 2010;32:554-563.
10. Wang B, Relling MV, Storm MC, et al. Evaluation of immunologic crossreaction of antiasparaginase antibodies in acute lymphoblastic leukemia (ALL) and lymphoma patients. Leukemia. 2003;17:1583-1588.
11. Zalewska-Szewczyk B, Gach A, Wyka K, et al. The cross-reactivity of anti-asparaginase antibodies against different L-asparaginase preparations. Clin Exp Med. 2009;9:113-116.
12. Vrooman LM, Supko JG, Neuberg DS, et al. Erwinia asparaginase after allergy to E. coli asparaginase in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2010;54:199-205.

BILLING GUIDE
19EUSA Pharma (USA), Inc.
strategies to Appeal Denied Claims for erwinaze™ (asparaginase Erwinia chrysanthemi) For Injection
If a claim for Erwinaze is improperly reimbursed or denied, you may consider submitting an appeal. The following provides some tips for appealing denied claims:
l Call the payer on behalf of the patientl Review the Explanation of Benefits (EOB) to determine the reason for the deniall If additional information is requested, submit the necessary documentation immediatelyl Submit a corrected claim if the denial was due to a technical billing error (eg, missing additional information associated
with miscellaneous codes, incorrect patient identification number, missing diagnosis)l Verify appeal process with payer — Is there a particular form that must be completed? — Can the appeal be conducted over the phone or must it be in writing? — To whom should the appeal be directed? — What information must be included with the appeal (eg, copy of original claim, EOB, supporting documentation)? — How long does the appeal process usually take? — How will the payer communicate the appeal decision?l Review appeal request for accuracy, including patient identification numbers, coding, and requested informationl Request that an oncologist, hematologist, or other specialist who is familiar with Erwinaze review the claim for medical
necessity. It is preferable to have the claim reviewed by a specialist who is currently treating patients with Erwinazel File claims appeal as soon as possible and within timely filing limitsl Reconcile claims appeal responses promptly and thoroughly to ensure appeals have been processed appropriatelyl Record appeal result (eg, payment amount or if further action is required)l Include a copy of the original claim and denial notification, the patient’s complete medical history, the physician’s plan
for continuing treatment, and relevant journal articles supporting the use of Erwinazel If the first-level appeal is denied, consider filing a second-level appeal. Appeals at the second level are typically
conducted by an examiner who is independent of the payer. Medicare Part B also has additional levels of appeals, such as those conducted by an administrative law judge. Contact the Hotline at 888-837-4397 for more information and assistance with payer appeal options

Erwinaze™ (asparaginase Erwinia chrysanthemi)
20
Hospital Outpatient Coding for erwinazeTo ensure appropriate reimbursement, product should be prepared and dispensed in the hospital outpatient pharmacy. Coding for Erwinaze and its administration may vary according to the specific payer’s requirements. It is important to check with the payer to determine any coding or documentation requirements that it has prior to submitting a claim for Erwinaze. The Hotline can assist providers with reimbursement research, including coding information. Please contact the Hotline at 888-837-4397 for more information.
Until the approval of a product-specific HCPCS code, Erwinaze may be billed with one of the following codes:
Payer Type HCPCS Code Description
Non-Medicare Patients
J9999* Not otherwise classified, antineoplastic drugs
J3590* Unclassified biologics
J3490* Unclassified drugs
Medicare Patients Only C9399 Unclassified drugs or biologicals
* HCPCS code J9999 should generally be used to report Erwinaze. HCPCS codes J3590 and J3490 should be used ONLY if mandated by a payer. Many payers have a policy of paying for the intramuscular administration of a chemotherapy code ONLY when a drug in the J9xxx series is used to report the provision of the drug. The use of J3590 or J3490 instead of J9999 will cause the intramuscular injection code to be denied by many payers.
When reporting a miscellaneous HCPSC code, payers may require that providers report the NDC. The FDA has assigned the following NDCs to Erwinaze:
NDC Total International Units
57902-249-05Contains 5 vials. Each single vial contains 10,000 International Units of asparaginase Erwinia chrysanthemi, for a total of 50,000 International Units
57902-249-01 Single vial containing 10,000 International Units of asparaginase Erwinia chrysanthemi
NDCs (including the NDC for Erwinaze) are often shown in the package insert and certain other locations using the FDA-approved 10-digit format. Whenever a health plan requires the use of an NDC on the UB-04 claim form, the 10-digit NDC must be converted to an 11-digit format. To do so, the 3 numbered segments described above are converted to a 5-digit/4-digit/2-digit format that requires a strategically placed zero. For example, the 10-digit NDC for Erwinaze is converted as follows:
10-Digit Format
Erwinaze 10-Digit Example
11-Digit FormatErwinaze 11-Digit Example
Reporting on CMS Claim Form
5-3-2 57902-249-05 5-4-2 57902-0249-05 57902024905
5-3-2 57902-249-01 5-4-2 57902-0249-01 57902024901
Hyphens are not used when entering the NDC on the claim form.

BILLING GUIDE
21EUSA Pharma (USA), Inc.
In addition to the drug itself, providers may report the administration of Erwinaze. Because Erwinaze is a chemotherapeutic agent, it may be reported by the following CPT:
CPT Code Description
96401 Chemotherapy administration, subcutaneous or intramuscular; nonhormonal antineoplastic
Additional Hospital Outpatient Department Coding for erwinaze
Erwinaze is an asparagine-specific enzyme indicated as a component of a multiagent chemotherapeutic regimen for the treatment of patients with acute lymphoblastic leukemia (ALL) who have developed hypersensitivity to E coli–derived asparaginase.
Code DescriptionAcute Lymphoid Leukemia ICD-9-CM Diagnosis Codes Require a Fifth Digit
204.00 Lymphoid leukemia, acute Without mention of having achieved remission, failed remission
204.01 In remission
204.02 In relapse
Hospitals may need to report ICD-9-CM procedure codes. The following ICD-9-CM procedure code may be appropriate for reporting Erwinaze in the hospital outpatient setting:
Code Description
99.25 Injection or infusion of cancer chemotherapeutic substance
Hospitals typically use revenue codes in addition to other types of codes to report other types of codes report services and supplies that are utilized during the course of therapy with Erwinaze.
Revenue Code Description
0636 Drugs requiring detailed coding
0250 Pharmacy, general
0331 Chemotherapy injected
It is important to check with the payer to determine any coding or documentation requirements that it has prior to submitting a claim for Erwinaze. The Hotline can assist providers with reimbursement research, including coding information. Please contact the Hotline at 888-837-4397 for more information.

For Additional Information
Please visit www.erwinaze.com to learn more about Erwinaze, including coding and reimbursement information, and to find downloadable tools.
© 2011 EUSA Pharma (USA), Inc. All rights reserved. 11/11
E-0027-11
Selected Important Risk Information About Erwinaze7
Contraindicationsl History of serious hypersensitivity reactions to Erwinaze, including anaphylaxis
l History of serious pancreatitis with prior l-asparaginase therapy
l History of serious thrombosis with prior l-asparaginase therapy
l History of serious hemorrhagic events with prior l-asparaginase therapy
Warnings and Precautions l If the following occur, discontinue Erwinaze:
— Serious hypersensitivity reactions, including anaphylaxis
— Severe or hemorrhagic pancreatitis
l Glucose intolerance can occur and, in some cases, may be irreversible. Perform appropriate monitoring and treat hyperglycemia with insulin, as necessary
l Thrombosis, hemorrhage: discontinue Erwinaze until resolved
Adverse Reactions l Most common (>1%) adverse reactions are serious hypersensitivity reactions, including
anaphylaxis, pancreatitis, abnormal transaminases, coagulation abnormalities including thrombosis and hemorrhage, nausea and vomiting, and hyperglycemia
Please see full Prescribing Information.
7Erwinaze™ (asparaginase Erwinia chrysanthemi) prescribing information. Langhorne, PA: EUSA Pharma (USA), Inc.; November 2011.