Biliary Disorders
59
BILIARY DISORDER S Erick Sioco Inserto, RN NCM 103
-
Upload
erick-sioco-inserto -
Category
Documents
-
view
232 -
download
0
Transcript of Biliary Disorders
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 1/59
BILIARYDISORDER
SErick Sioco Inserto, RNNCM 103
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 2/59
Gall bladder
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 3/59
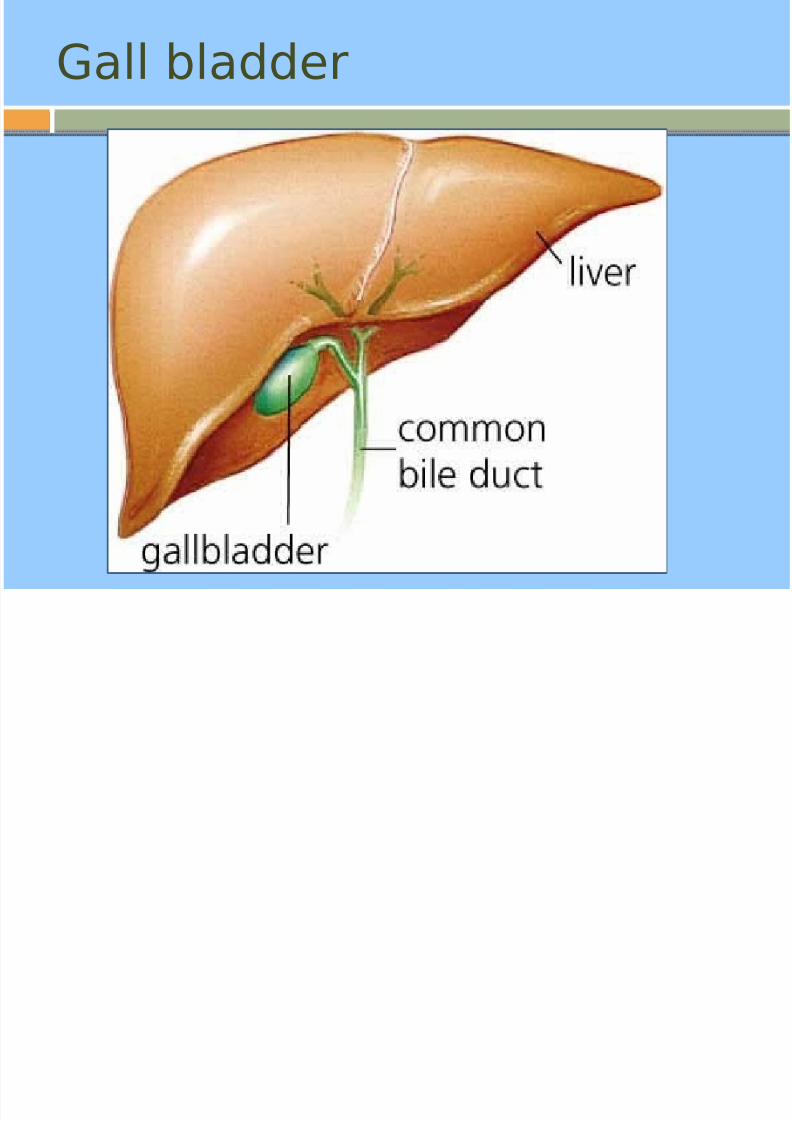
The gallbladder is a small pear-shapedorgan that stores and concentrates bile.
The gallbladder is connected to the liver
by the hepatic duct. It approximately 3 to 4 inches (7.6 to 10.2
cm) long and about 1 inch (2.5 cm)wide.
function of the gallbladder is to store bileand concentrate
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 4/59
Pancreas
Has two functions
Exocrine– secretion of pancreatic enzymes into theGIT through the pancreaticduct.
Endocrine – secretion of insulin, glucagon, andsomatostatin into the bloodstream
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 5/59
Exocrine Pancreas
Secretions are high in protein content andelectrolyte rich fluid
Alkaline
Secretions includeAmylase – aids in the digestion of
carbohydrates
Trypsin – digestion of proteins
Lipase – digestion of fats
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 6/59
Endocrine Pancreas
Islet of langerhansCollection of cells embedded in the
pancreatic tissue
Composed of alpha, beta, delta cells Alpha cells
Secrete glucagon – raises glucose
Beta cellsSecrete insulin – lowers blood glucose
Delta cellsSecrete Somatostatin- exerts a
hypoglycemic effect
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 7/59
Disorders of the GallBladder
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 8/59
Terminology
Cholecystitis – inflammation of thegallbladder
Cholelithiasis – the presence of calculi in
the gallbladder Cholecytectomy- removal of the
gallbladder
Cholecytostomy – opening and drainageof the gall bladder
Choledochotomy – opening of thecommon duct
Choledocholithiasis – stones in the
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 9/59
defined as inflammation of thegallbladder that occurs mostcommonly because of an obstructionof the cystic duct from cholelithiasis
Cholecystitis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 10/59
Manifestations
Pain, Rigidity, tenderness of the upperright abdomen
Fever
Nausea Vomiting Tachycardia (+) Murphy’s Sign
described as tenderness and aninspiratory pause elicited duringpalpation of the RUQ.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 11/59
Causes
Calculous cholecystitis Female sex Obesity or rapid weight loss Drugs (especially hormonal therapy in women)
Pregnancy Increasing age
Acalculous cholecystitis Critical illnessMajor surgery or severe trauma/burns
Sepsis Long-term TPN Prolonged fasting
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 12/59
Other causesCardiac events, including myocardial
infarction
Sickle cell diseaseSalmonella infections
Diabetes mellitus
Patients with AIDS with cytomegalovirus,
cryptosporidiosis, or microsporidiosis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 13/59
Diagnostics
Increased Alanine aminotransferase (ALT)and aspartate aminotransferase (AST)levels
Amylase mildly elevated Ultrasonography
Radiography
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 14/59
Medical Treatment
initial treatment includes bowel rest,intravenous hydration, analgesia, andintravenous antibiotics
Emesis can be treated with antiemeticsand nasogastric suction.
Restoration of hemodynamic stability
Daily stimulation of gallbladdercontraction
Laparoscopic cholecystectomy is the standard of care for the surgical
treatment of cholecystitis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 15/59
Cholecystectomy or Cholecystotomyusually reserved for complicated cases in
which the patient has gangrene or
perforation.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 16/59
Nursing Management
Encourage fluid input and output Monitor vital signs Assess pain and administer analgesics as
ordered Provide diet a liquid or low-fat diet if
surgery is not an option Administer antibiotics as ordered Assist with ambulation Encourage adequate nutrition Assess for complications
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 17/59
is the presence of one or more calculi
(gallstones) in the gallbladder.
Cholelithiasis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 18/59
Risk Factors
Obesity Women Multiple preganancies
Frequent changes in weight Rapid weight loss Treatment of High dose estrogen
Ileal resection or disease Cystic fibrosis Diabetes
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 19/59
Four F’sFemale
Fat
FortyFertile
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 20/59
Pathophysiology
Biliary sludge is often a precursor of gallstones. It consists of Ca bilirubinate(a polymer of bilirubin), cholesterol
microcrystals, and mucin Sludge develops during gallbladder stasis
as occurs during pregnancy or whilereceiving TPN.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 21/59
Types:
Cholesterol stonesBile must be supersaturated with
cholesterol The excess cholesterol must precipitate
from solution as solid microcrystalsmicrocrystals must aggregate and grow.
Black pigment stones are small, hard gallstones composed of Ca
bilirubinate and inorganic Ca salts (eg,Ca carbonate, Ca phosphate)
alcoholic liver disease, chronic hemolysis,and older age
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 22/59
Brown pigment stonesare soft and greasy, consisting of
bilirubinate and fatty acids (Ca palmitateor stearate). They form during infection,inflammation, and parasitic infestation
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 23/59
Manifestations
Asymptomatic Epigastric distress
Fullness
Abdominal distentionVague pain in the RUQMay follow ingestion of fried and fatty
foods
Fever Biliary Colic
steady or intermittent ache in the upperabdomen, usually under the right side of
the rib cage.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 24/59
Biliary colic Nausea
Vomiting
Colicky pain
JaundiceOccurs in few patients
Changes in urine and stool colorUrine is very darkStool is clay colored, grayinsh
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 25/59
Diagnostics
Abdominal xrays
Ultrasound – procedure of choice
Cholescintigraphya radioactive dye is administered IV. The
Biliary tree is then scanned
Cholecystography
An iodide containing contrast agent isadministered to the patient . And a xrayis taken
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 26/59
Surgical treatment
Endoscopic RetrogradeCholangiopancreatography
(ERCP)
is a test that combines the use of aflexible, lighted scope (endoscope) withX-ray pictures to examine the tubes thatdrain the liver, gallbladder,and pancreas
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 27/59
Purpose:
Check persistent abdominal painor jaundice.
Find gallstones or diseases of the liver,
bile ducts, or pancreas. Remove gallstones from the common bile
duct if they are causing a problem suchas blockage (obstruction), inflammationor infection of the common bile duct(cholangitis), or pancreatitis.
Open a narrowed bile duct or insert a
drain.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 28/59
Percutaneous transhepaticCholangiographya radiologic technique used to visualize
the anatomy of the biliary tract. Acontrast medium is injected into a bileduct in the liver, after which X-rays aretaken
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 29/59
Medical Management
Reduce gallbladder pain AnalgesicsSurgery
Administration of IV fluids Nasogastric suction Adequate rest Antibiotic therapy Ursodeoxycholic acid (UDCA) Chenodeoxycholic acid
Has been used to dissolve gallstone primarilycomposed of cholesterol
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 30/59
Non- surgical Treatments
Mono-octanoin or methyl tertiary butylether (MTBE) infusion
Extracorporeal Shockwave Lithotripsy
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 31/59
Nursing Management
Monitor pain administer analgesics asordered
Assess vital signs
Encourage hydration Administer a low fat diet
Instruct to avoid gaseous foods
Prepare the client for surgery
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 32/59
Inflammation of the pancreas that can
occur in two very different forms
Pancreatitis

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 33/59
is a sudden inflammation of
the pancreas
Acute Pancreatitis

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 34/59
Manifestation
Edema on the pancreas
Inflammation
Severe epigastric pain radiating to the
back Nausea, vomiting, diarrhea and loss of
appetite
Fever/chills Hemodynamic instability, including shock

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 35/59
Grey-Turner's sign (hemorrhagic discoloration of the flanks)
Cullen's sign (hemorrhagic discoloration of theumbilicus)
Grünwald sign (appearanceof ecchymosis around the umbilicus due tolocal toxic lesion of the vessels.)
Körte's sign (pain or resistance in the zonewhere the head of pancreas is located
(in epigastrium, 6-7 cm above the umbilicus). Kamenchik's sign (pain with pressure underthe xiphoid process)
Mayo-Robson's sign (pain while pressing at thetop of the angle lateral to the Erector spinae
muscles and below the left 12th rib (leftcostovertebral angle (CVA))

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 36/59
Grey Turners sign

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 37/59
Cullen’s Sign
C it i f Ad i i t th
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 38/59
Criteria for Admission to thehospital
Age > 55 years
WBC >16,00 mm3
Serum Glucose >200 mg/dL
Serum LDH > .350 IU/L AST .250/mL
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 39/59
Causes
I - idiopathic. Thought to be hypertensivesphincter or microlithiasis.
G - gallstone.Gallstones that travel down the common bile
duct and which subsequently get stuck inthe Ampulla of Vater can cause obstructionin the outflow of pancreatic juices from thepancreas into the duodenum. The backflowof these digestive juices
causes lysis(dissolving) of pancreatic cellsand subsequent pancreatitis.
E - ethanol (alcohol) T - trauma
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 40/59
S - steroids M - mumps (paramyxovirus) and other viruses
(Epstein-Barr virus, Cytomegalovirus) A - autoimmune diseas ( Systemic lupus
erythematosus) S - scorpion sting (e.g. Tityus trinitatis), and
also snake bites
H - hypercalcemia, hyperlipidemia/hypertriglyceridemia and hypothermia
E - ERCP (Endoscopic Retrograde Cholangio-Pancreatography - a procedure that
combines endoscopy and fluoroscopy) D - drugs (SAND) - steroids & sulfonamides, azathioprine, NS
AIDS, diureticssuch as furosemide and thiazides,& didanosine) and duodenal ulcers.
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 41/59
Diagnostics
Increased blood amylase level Increased serum blood lipase level
Increase urine amylase level

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 42/59
Medical Treatment
Pain medicines Fluids given through a vein (IV) (NPO)Stopping food or fluid by mouth to
limit the activity of the pancreas NGT to drain insertion Drain fluid that has collected in or around
the pancreas (biliary drainage) Remove gallstones (ERCP, ESWL) Relieve blockages of the pancreatic duct
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 43/59
Nursing Management
Monitor vital sign’s Administer pain medications
Implement NPO status
Complete bed rest Assess fluid and electrolyte balance
(monitor input and output)
Monitor NGT drainage Provide health teachings
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 44/59
is long-standing inflammation of the
pancreas that results in irreversibledeterioration of pancreatic structureand function
Chronic Pancreatitis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 45/59
Causes
Alcoholism Idiopathic
Cystic Fibrosis
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 46/59
Manifestations
Back pain Abdominal pain Weight loss
swollen and tender abdomen nausea vomiting fever rapid pulse Fatty stools (steatorrhea)
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 47/59
Diagnostics
A secretin stimulation test Is considered the gold standard functional
test for diagnosis of chronic pancreatitisbut not often used clinically
ESR, IgG4, rheumatoid factorMay be elevated
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 48/59
Medical Treatment
Chemical dependency treatment is the most importantstep in treating alcohol-related pancreatitis.
Pain relief drugs Endoscopic therapy by introducing stents to drain
blocked pancreatic ducts
Shock wave lithotripsy to pulverize pancreatic stones Surgery (laparoscopic and traditional) Islet cell transplantation may be offered if most or all of
the pancreas is removed. Enzyme therapy for malabsorption helps restore normal
digestion and reduces the amount of fat in the feces,leading to weight gain and improved well-being.Dietary changes such as eating smaller meals andlimiting fats help reduce the need for digestiveenzymes.
Treatment of diabetes, if that develops
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 49/59
Nursing Management
Assess painAdminister analgesics as ordered
Monitor Input and output
Monitor vital signs Assess hydration status (I & 0)
Administer oxygen as ordered
Insruct the patient to avoid alcohol andfatty foods
Assess stools
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 50/59
a malignant neoplasm of the pancreas
Sometimes called a "silent killer" becauseearly pancreatic cancer often does notcause symptoms
Pancreatic cancer
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 51/59
Manifestations
Pain in the upper abdomen that typicallyradiates to the
Loss of appetite and/or nausea and
vomiting Significant weight loss
Painless jaundice (yellow skin/eyes, darkurine)
pale-colored stool and steatorrhea
Trousseau sign
Diabetes mellitus, or elevated blood
sugar levels.
Causes

8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 52/59
Causes
Age (particularly over 60) Male
Smoking
Diets low in vegetables and fruits Diets high in red meat
Diets high in sugar-sweetened drinks (soft
drinks) Obesity
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 53/59
Diabetes mellitus is both risk factor for pancreatic cancer,
and, as noted earlier, new onsetdiabetes can be an early sign of thedisease.
Chronic pancreatitis
Helicobacter pylori infection
Diagnostics
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 54/59
Diagnostics
Computed tomography (CT) scans Magnetic resonance
cholangiopancreatography (MRCP)
Endoscopic ultrasound (EUS) Endoscopic retrograde
cholangiopancreatography (ERCP)
Upper GI series
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 55/59
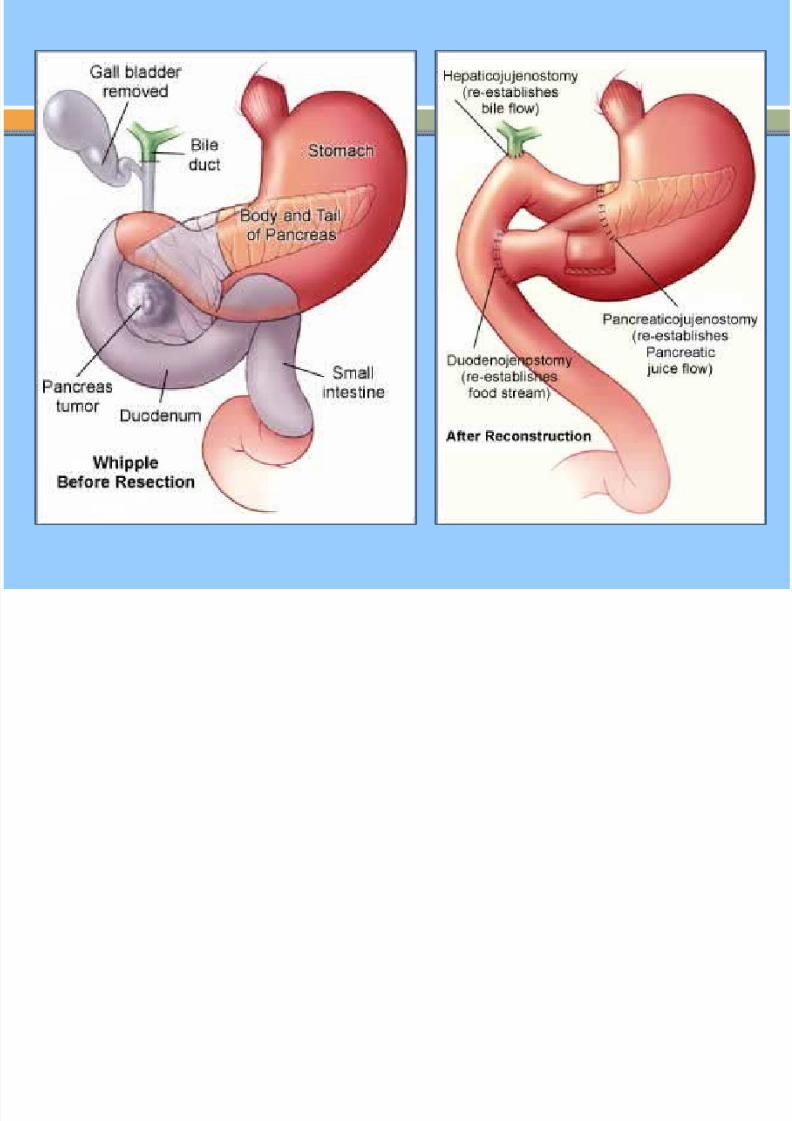
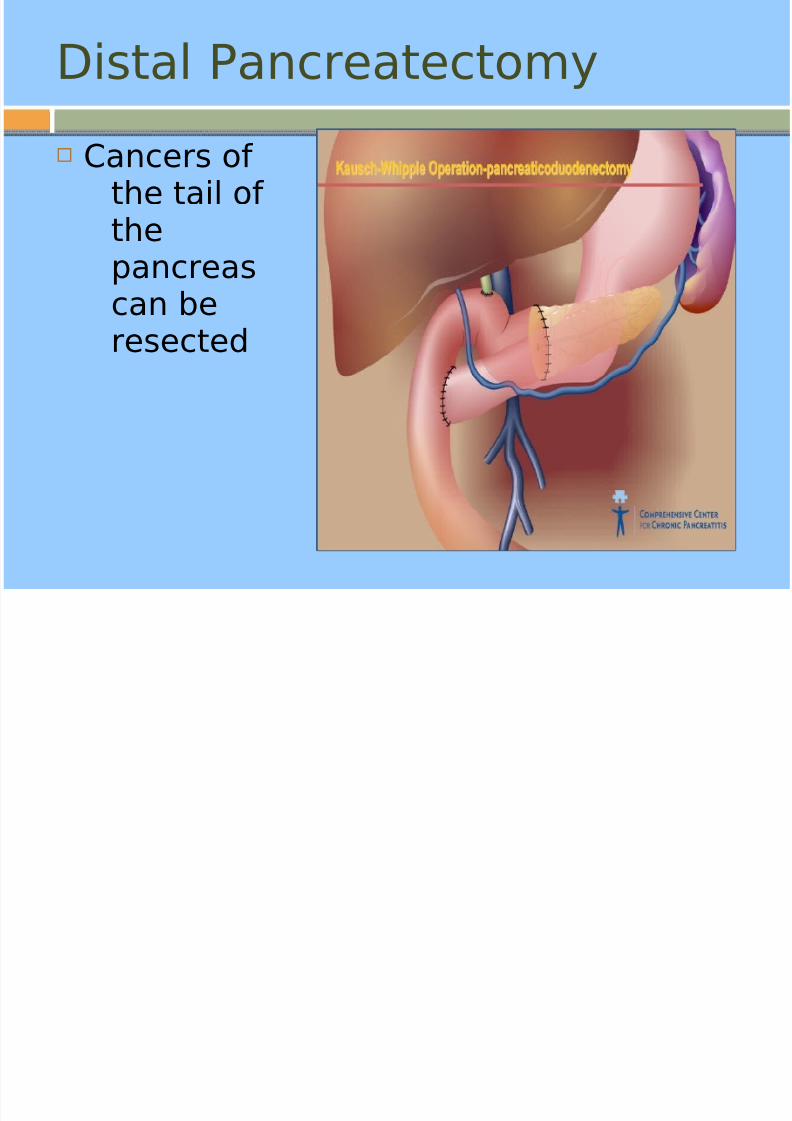
Surgical treatment
Whipple procedure the most common surgical treatment for
cancers involving the head of thepancreas
procedure involves removing thepancreatic head and the curve of theduodenum together (pancreato-duodenectomy)
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 56/59
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 57/59
Distal Pancreatectomy
Cancers of the tail of thepancreascan beresected
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 58/59
Medical Management
Intensity Modulated Radiation Therapyuses hundreds of small radiation beams of
varying intensities to precisely targetcancer cells, while sparing healthy tissue
Chemotherapy
8/6/2019 Biliary Disorders
http://slidepdf.com/reader/full/biliary-disorders 59/59
Nursing Management
Assess painAdminister pain medications as ordered
Encourage adequate nutritionProvide small low fat feedingsMonitor weightAssess and monitor hydration
Provide good skin careProtect bony prominences from pressure
ulcers Relieve discomforts
Relief of itching from jaundice