Best therapy of healthcare-associated pneumonia: narrow vs ...
36
Best therapy of healthcare-associated pneumonia: narrow vs broad spectrum antimicrobials? Michele Bartoletti Infectious Diseases Unit S. Orsola Teaching Hospital ESCMID COURSE - Ferney-Voltaire (France) November 5 -6 2015 “Moving antimicrobial stewardship forward in special patient populations” ESCMID Online Lecture Library © by author
Transcript of Best therapy of healthcare-associated pneumonia: narrow vs ...

Best therapy of healthcare-associated pneumonia: narrow vs broad spectrum antimicrobials?
Michele Bartoletti Infectious Diseases Unit S. Orsola Teaching Hospital
ESCMID COURSE - Ferney-Voltaire (France) November 5 -6 2015
“Moving antimicrobial stewardship forward in special patient populations”
ESCMID Online Lecture Library
© by author

CAP
Pneumonia classification
ESCMID Online Lecture Library
© by author

CAP
HAP
Pneumonia classification
ESCMID Online Lecture Library
© by author

CAP
HAP
VAP
Pneumonia classification
non-VAP
ESCMID Online Lecture Library
© by author

CAP
HAP
VAP
HCAPHCAP
Pneumonia classification
non-VAP
ESCMID Online Lecture Library
© by author

Community onset MDR bloodstream infections
Community onset MRSA bacteremiaMorin and Hadler J Infect Dis 2001
Friedman et al. Ann Intern Med 2002
Tacconelli et al. JAC 2004
Community onset MRSA bacteremia
CAP HAP, VAPATS 1996
HCAP ATS guidelines 2005
Origin of HCAP
ESCMID Online Lecture Library
© by author

Contact with the health system
Prior hospitalization and/or surgery
IV/wound care at home
Residence in a nursing home or LTCF
Chronic hemodialysisChemotherapy
HCAPFriedman et al. Ann Intern Med 2002
ESCMID Online Lecture Library
© by author

Pneumonia treated in the internal medicine department: focus on healthcare-associated pneumonia
Giannella M. Clin Microbiol Infect. 2012;18:786-94
CAP
N=148 (%)HCAP
N=65 (%)HAP
N=21 (%)P
Gram-positive
S. pneumoniae
MRSAMSSA
94 (63.5)
1 (0.7)1 (0.7)
25 (38.5)
8 (12.3)1 (1.5)
3 (14.3)
2 (9.5)2 (9.5)
<0.001
<0.0010.03
Gram-negative
Enterobacteriaceae
P. aeruginosa
L. pneumophila
H. influenzae
A. baumannii
17 (11.5)
5 (3.4)11 (7.4)
5 (3.4)
0
8 (12.3)
11 (16.9)2 (3.1)
3 (4.6)
0
5 (23.8)
6 (28.6)0
0
2 (9.5)
0.27
<0.0010.34
0.86
0.008
1002 pts with pneumonia hospitalized in IMDs
ESCMID Online Lecture Library
© by author

Failure to cover MDR pathogens leads to inadequate initial
antimicrobial coverage and accounts for excess mortality
HCAP patients should be identified and treated with initial
broad-spectrum antibiotic therapy
HCAP presents an etiological pattern
similar to that of HAP
The concept of HCAP
ESCMID Online Lecture Library
© by author

Prevalence 18-67%
Median age 64-81 years
High rate of comorbidities (CHF, COPD, cerebrovascular
disease)
Poor functional status
Risk factors for aspiration pneumonia
Treatment restrictions
Mortality 18-28%
Kollef et al. Chest 2005; Carratala et al. Arch Intern Med 2007;
Shindo et al Chest 2009; Venditti et al. Ann Intern Med 2009;
Chalmers et al Clin Infect Dis 2011; Jung et al. BMC Infect Dis 2011
HCAP
ESCMID Online Lecture Library
© by author

HCAP = HAP ?
Aggressive broad-spectrum therapy
HCAP = SEVERE HOSPITALIZED CAP ?
Beta – lactam +
Macrolide
• Increased costs and comsumption of antibiotics
• Incresed risk of MDR pathogens selection
•Increased risk of inadequate empirical therapy
• Increased risk for mortality
ESCMID Online Lecture Library
© by author

HCAP comprises very heterogeneous conditions, not all
patients need broad spectrum antibiotic therapy
Increased frequency of MDR and increased mortality are
not consistently related
Guideline concordant treatment could not be shown to
be associated with better outcome
Brito V. and Niederman MS. Curr Opin Infect Dis 2009
Ewig S. et al. Lancet Infect Dis 2010
Ewig S. et al. Curr Opin Infect Dis 2012
Criticisms to the HCAP concept
ESCMID Online Lecture Library
© by author

HCAP comprises very heterogeneous conditions, not all
patients need broad spectrum antibiotic therapy
Increased frequency of MDR and increased mortality are
not consistently related
Guideline concordant treatment could not be shown to
be associated with better outcome
Brito V. and Niederman MS. Curr Opin Infect Dis 2009
Ewig S. et al. Lancet Infect Dis 2010
Ewig S. et al. Curr Opin Infect Dis 2012
Criticisms to the HCAP concept
ESCMID Online Lecture Library
© by author

Predicting MDR risk by HCAP model
Webb BJ et al. Respiratory Med 2014
ESCMID Online Lecture Library
© by author
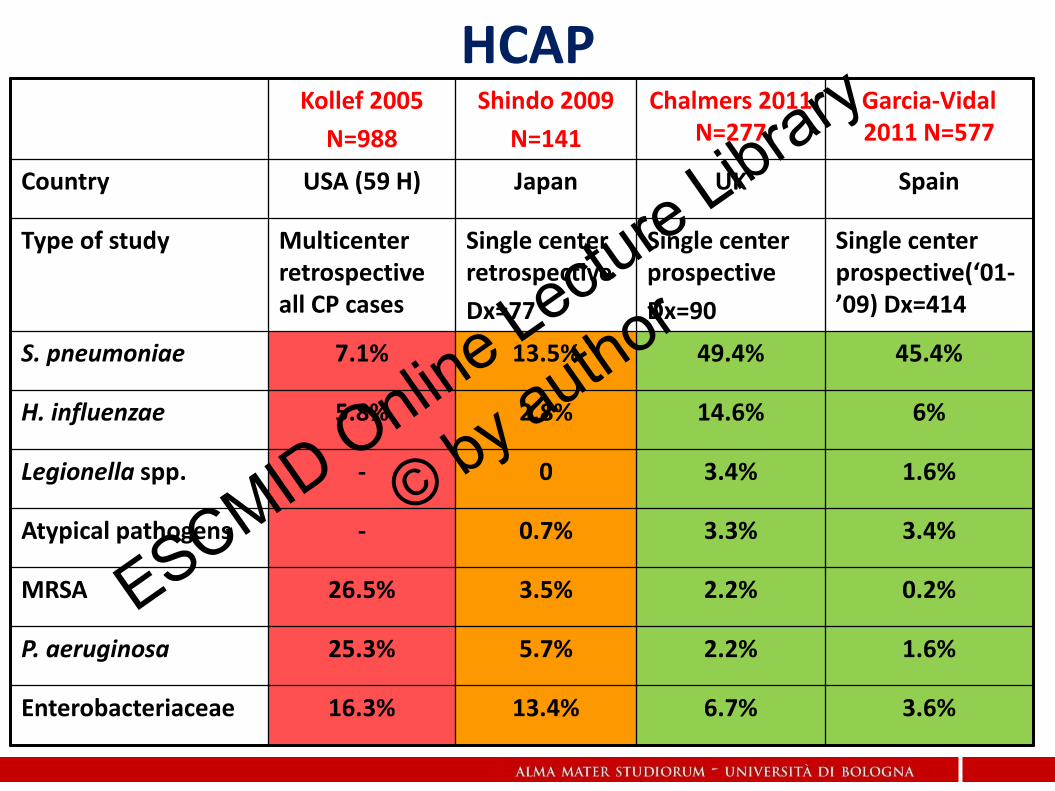
Kollef 2005
N=988
Shindo 2009
N=141
Chalmers 2011 N=277
Garcia-Vidal 2011 N=577
Country USA (59 H) Japan UK Spain
Type of study Multicenter retrospective all CP cases
Single center retrospective
Dx=77
Single center prospective
Dx=90
Single center prospective(‘01-’09) Dx=414
S. pneumoniae 7.1% 13.5% 49.4% 45.4%
H. influenzae 5.8% 2.8% 14.6% 6%
Legionella spp. - 0 3.4% 1.6%
Atypical pathogens - 0.7% 3.3% 3.4%
MRSA 26.5% 3.5% 2.2% 0.2%
P. aeruginosa 25.3% 5.7% 2.2% 1.6%
Enterobacteriaceae 16.3% 13.4% 6.7% 3.6%
HCAP
ESCMID Online Lecture Library
© by author

HCAP comprises very heterogeneous conditions, not all
patients need broad spectrum antibiotic therapy
Increased frequency of MDR and increased mortality are
not consistently related
Guideline concordant treatment are not associated to a
better outcome
Brito V. and Niederman MS. Curr Opin Infect Dis 2009
Ewig S. et al. Lancet Infect Dis 2010
Ewig S. et al. Curr Opin Infect Dis 2012
Criticisms to the HCAP concept
ESCMID Online Lecture Library
© by author

Impact on mortality of
GLs concordant therapy
Grenier et al.
J Antimicrob Chemother 2011
NO
Chalmers et al.
Clin Infect Dis 2011
NO
Attridge et al.
Eur Respir J 2011
NO
Falcone et al.
Intern Emerg Med 2012
YES
Webb BJ et al.
Respiratory Medicine 2012
NO
Rotheberg et al.
J Abtimicrob Chemother 2015
NO
GLs concordant therapy in HCAP
ESCMID Online Lecture Library
© by author

Clinical prediction models for CAP-DRP
Webb BJ et al. Respiratory Med 2014
ESCMID Online Lecture Library
© by author

1. Identify patients at risk for CAP caused by DRP.
ESCMID Online Lecture Library
© by author

Risk Factors for Drug-Resistant Pathogens in Community-acquired and Healthcare-associated Pneumonia
Objectives: to clarify risk factors for drug-resistant pathogens
(DRPs) in patients with CAP and HCAP.
Methods: prospective observational study conducted in
hospitalized patients with pneumonia at 10 institutions in Japan.
Pathogens identified as not susceptible to ceftriaxone, ampicillin-
sulbactam, macrolides, and respiratory fluoroquinolones were
defined as CAP-DRPs.
Y Shindo et al. AM J Resp Crit Care Med 2013
ESCMID Online Lecture Library
© by author

Risk Factors for Drug-Resistant Pathogens in Community-acquired and Healthcare-associated Pneumonia
Y Shindo et al. AM J Resp Crit Care Med 2013
Main Results:1,413 patients (887 CAP and 526 HCAP) were analyzed.
Independent risk factors for CAP-DRPs were almost identical in patients with CAP and HCAP.
These included:
o prior hospitalization (AOR 2.06; 95% CI, 1.23–3.43),
o immunosuppression (AOR, 2.31; 95% CI, 1.05–5.11),
o previous antibiotic use (AOR,2.45;95%CI,1.51–3.98),
o use of gastric acid–suppressive agents (AOR, 2.22; 95%CI, 1.39–3.57),
o tube feeding (AOR, 2.43; 95% CI, 1.18–5.00),
o nonambulatory status (AOR, 2.45; 95% CI, 1.40–4.30)7
ESCMID Online Lecture Library
© by author

Risk Factors for Drug-Resistant Pathogens in Community-acquired and Healthcare-associated Pneumonia
Y Shindo et al. AM J Resp Crit Care Med 2013
When no risk factors or only one risk factor is observed in a
pneumonia patient (86% of patients with CAP and 36% of
patients with HCAP in the current study), CAP-DRPs are low
(<10%) .
ESCMID Online Lecture Library
© by author

1. Identify patients at risk for CAP caused by DRP.
2. Stratify for disease severity.
ESCMID Online Lecture Library
© by author

A New Strategy for Healthcare-Associated Pneumonia: A 2-Year Prospective MulticenterCohort Study Using Risk Factors for Multidrug- Resistant Pathogens to Select InitialEmpiric Therapy. T.Maruyama et al. Clin Infect Dis 2013
124 CAP
321 HCAP
n=110 n=92 n=41 n=78
93.1% of HCAP patients were treated according to the therapy algorithm, with only 53% receiving broad-spectrum empiric therapy, 92.9% received appropriate therapy for the identified pathogen
ESCMID Online Lecture Library
© by author

1. Identify patients at risk for CAP caused by DRP.
2. Stratify for disease severity.
3. Discontinue unecessary
antibioticsESCMID Online Lecture Library
© by author

De-escalation therapy among bacteraemic patients withcommunity-acquired pneumonia
Carugati M Clin Microbiol Infect 2015; 21: 936.e11–936.e18
METHODS:Secondary analysis of the Community-Acquired Pneumonia Organization database
DET was defined as changing an appropriate empirical broad-spectrum regimen toa narrower-spectrum regimen according to culture results within 7 days from hospital admission
Study population: 261 patients with bacteriemic CAP
165 DET gropup 96 N-DET gropup
There was a significantly lower 30-day mortality rate in the DET group than in the N-DET group in univariate analysis ( 15.1% vs. 25.0%, p 0.04)
After adjustment for confounders, DET was not associated with an increased risk of 30-day mortality RR 0.78 (95% CI 0.47–1.27), p 0.32)
ESCMID Online Lecture Library
© by author

Retrospective study, 2007-2009, 102 HCAP
77 NC, 29 PC
De-escalation in 55/77 NC within median 4 days
Schlueter et al. Infection 2010
ESCMID Online Lecture Library
© by author

Is de-escalation feasible in patients with severe sepsis or septic shock?
ESCMID Online Lecture Library
© by author

De-escalation of empirical therapy is associated with lowermortality in patients with severe sepsis and septic shock
A total of 628 patients with severe sepsis or septic shock at ICU admission were treated empirically with broad-spectrum antibiotics.
De-escalation was applied in 219 patients (34.9 %).
Garnacho-Montero J Intensive Care Med 2014; 40 (1):32-40
Patients with adequated empirical therapy
In terms of survival de-escalation therapy was a protective factor (OR0.54; 95 % CI 0.33–0.89). PS adjusted analysis confirmed this finding.
ESCMID Online Lecture Library
© by author

Is de-escalation feasible in a ESBL-endemic setting?
ESCMID Online Lecture Library
© by author

Safety and clinical outcomes of carbapenem de-escalation as part ofan antimicrobial stewardship programme in an ESBL-endemic setting
Lew KY et al JAC. 2015 Apr;70(4):1219-25
Criteria for de-escalation
Empirical therapy Definitive therapy
•Afebrile
•Not on inotropes
•Systolic blood pressure returned to baseline
•Not mechanically ventilated or fraction of inspired oxygen ≤0.4
•Respiratory rate < 25 bpm
Microbiology-driven
Patients receiving meropenem or imipenem underwent a prospective ASP review for eligibility for de-escalation.
Patients in whom carbapenem was de-escalated or not de-escalated, representing the acceptance and rejection of the ASP recommendation, respectively, were compared
ESCMID Online Lecture Library
© by author

Safety and clinical outcomes of carbapenem de-escalation as part ofan antimicrobial stewardship programme in an ESBL-endemic setting
Lew KY et al JAC. 2015 Apr;70(4):1219-25
De escalated patients
N= 204
Non de-escalated patients
N=96
P
Respiratory infections 60(29) 29(30) 0.84
Culture-negative infections 46(22) 27(28) 0.47
ESBL producing strain 35(22) 25(26) 0.20
Outcome
Survival at discharge 173 (84.8) 79 (82.3) 0.54
Duration of carbapenem use (days)
6 (4-8) 8 (7-11) <0.001
Incidence of CDAD 2 (1) 4 (4) 0.08
Incidence of XDR A.baumannii at 30 days
4(2) 7 (7.3) 0.04
ESCMID Online Lecture Library
© by author

Predictive Value of Methicillin-Resistant Staphylococcusaureus (MRSA) Nasal Swab PCR Assay for MRSA Pneumonia
Dangerfield B. et alAntimicrob Agents Chemother. 2014;58(2):859-64
All patients with confirmed pneumonia who had both a nasal swab MRSA PCR test and a bacterial culture within predefined time intervals were included in the study
435 patients enrolled
54% cases were calssified as HCAP
14% of cases had a nasal swab culturepositive for MRSA
5.7% of cases had bloodculture or sputum positive for MRSA
Ability of nasal swab MRSA PCR assay in predicting MRSA pneumonia
SE SP PPV NPV
88.0% 90.1% 35.4% 99.2%
ESCMID Online Lecture Library
© by author

Association Between Hospitalization With Community-Acquired Laboratory-Confirmed Influenza Pneumonia andPrior Receipt of Influenza Vaccination
Grijalva G et al JAMA. 2015;314(14):1488-1497.
METHODSThe Etiology of Pneumonia in the Community (EPIC) study was a prospectiveobservational multicenter study of hospitalizations for community-acquiredpneumonia
In this case-control study, authors used EPIC data from patients 6 months or older withlaboratory-confirmed influenza infection and verified vaccination status during theinfluenza seasons
RESULTSOverall, 2767 patients hospitalized for pneumonia were eligible for the study; 162(5.9%) had laboratory-confirmed influenza. Twenty-eight of 162 cases (17%) withinfluenza-associated pneumonia and 766 of 2605 controls (29%) with influenza-negativepneumonia had been vaccinated.
The adjusted odds ratio of prior influenza vaccination between cases and controlswas 0.43 (95% CI, 0.28-0.68; estimated vaccine effectiveness, 56.7%; 95% CI, 31.9%-72.5%).
ESCMID Online Lecture Library
© by author

Antimicrobial stewardship:Reduction of unecessary antibiotic use for patients with pneumoniae
DE-ESCALATION: microbiological and clinically driven approach
No RF for MDR pathogens
Bloodcultures, culture of respiratory samples, urinary antigens, sample for respiratory viruses and influenza
β-lactam + macrolide
Etiologial diagnosis
De-escalation narrowing the antimicrobial spectrum
RF for MDR pathogens
Bloodcultures, culture of respiratory samples, urinary antigens, sample for respiratory viruses and influenza, nasal swab for MRSA
Pip/tzb + quinolone + anti MRSA*
Culture-negative and no clinical improvement
Repeat diagnostc work-up
SEVERE CAP/HCAP
Cultures-negative but clinical improvement
Switch to Oral intake(if possible)
72 h
ESCMID Online Lecture Library
© by author

Take home messages
Clinical severity, patient risk factors for DRP, and local epidemiology should be considered in the choice of empirical therapy for pneumonia
Attempt to etiological diagnosis is mandatory in hospitalized patients with pneumonia
Antimicrobial stewardship programs focused on de-escalation and reduction of length of therapy for pneumonia treated in IMDs should be implemented
ESCMID Online Lecture Library
© by author