Best Practices for Alarm Management: Kaiser Permanente, Children’s...
64
Best Practices for Alarm Management: Kaiser Permanente, Children’s National Medical Center, and The Johns Hopkins Hospital March 5, 2014 3/5/2014 1
Transcript of Best Practices for Alarm Management: Kaiser Permanente, Children’s...

Best Practices for Alarm Management:
Kaiser Permanente, Children’s National Medical Center,
and The Johns Hopkins HospitalMarch 5, 2014
3/5/2014 1

Co-Conveners
3/5/2014 2

Thank You to Our SponsorsThis webinar series is offered at no charge thanks to commercial grants from the companies shown here. HTSI and its co-convening organizations appreciate their generosity. AAMI and HTSI are managing all costs for the series. None of the co-convening organizations participated in seeking, discussing, or otherwise facilitating the commercial grants. The companies had no role in content development, and the webinars do not contain commercial content. Webinar presenters were selected based on topic expertise without regard to industry affiliation by a multi-disciplinary HTSI volunteer planning committee.
3/5/2014 3

LinkedIn - Questions
Please post questions about alarms on HTSI’s LinkedIn page:
http://www.linkedin.com/groups/Healthcare-Technology-Safety-Institute-HTSI-4284508
3/5/2014 4

Speaker Introductions
• D. Hunter Burgoon, RN, PHN, Director of Biomedical Technology Integration, Kaiser Permanente
• Jeff Hooper, MS, Director, Biomedical Engineering, Children’s National Medical Center
• Heather Walsh, RN, MSN, PCNS-BC, Simulation Outreach Coordinator, Children’s National Medical Center
• Maria Cvach, DNP, RN, CCRN, Assistant Director of Nursing, Clinical Standards, The Johns Hopkins Hospital
• Marjorie Funk, PhD, RN, FAHA, FAAN, Professor, Yale University School of Nursing (Moderator)
3/5/2014 5

Kaiser Permanente Alarm Fatigue Project
D. Hunter Burgoon, RN, PHNDirector of Biomedical Technology
3/5/2014 6

Kaiser Permanente at a GlanceKaiser Foundation Health Plan, Inc.
The Permanente Medical Groups
Kaiser Foundation Hospitals
|
Recognized as one of America’s leading health care providers and not-for-profit health plans
9.1 million members
38 hospitals> 600 medical offices
8 states and the District of Columbia
16,942 physicians174,259 employees
> $50 billion annual operating revenue
3/5/2014 7

Kaiser Permanente Alarm Fatigue Project Discussion Points
3/5/2014 8
Awareness and Motivation
Building Consensus
Approval Process
Pilot Project Implementation
Resources and Tools
Results
Next Steps

Alarm Fatigue: A Call for Action
3/5/2014 9
2010 Boston Globe article in April cited alarm fatigue in patient deaths
2011 AAMI Alarms Summit in October
2011 ECRI moves alarm hazards to #1 risk in November
2012 Kaiser Permanente Alarm Fatigue work group created in June
2012 Kaiser Permanente Alarms Summit held in November
2013 Kaiser Permanente launches first pilot sites on first track in March
2013 TJC SEA 50 released on Alarm Fatigue in April
2013 Kaiser Permanente first pilot site completes implementation in October
2014 TJC NPSG 2014 and 2016 on Alarm Fatigue in effect in January
2014 Kaiser Permanente launches four beta sites

Awareness and Motivation
3/5/2014 10

3/5/2014 11
Building Consensus

Pilot Project Implementation
New Adult Telemetry Standard• Actionability
Alarm Customization• Clinical Validity• Actionability
Alarm Hygiene• Validity
Pager Repeats• Validity• Actionability
3/5/2014 12

Pilot Project Implementation
Pager Repeat Reduction
Alarm Hygiene
Alarm Customization
New Telemetry Standard
3/5/2014 13

Approval Process
Alarm Fatigue Work Group
Alarm Management Work Group
Regional Critical Care Peer Groups
Regional Physician
ChairsCardiology
Critical CarePulmonology
HospitalistED
Chief Nursing Officers
Executive Sponsor
3/5/2014 14
Approvers

3/5/2014 15
Results Dispatches Reduced by 50%

ResultsAlerts Reduced by 25%
3/5/2014 16

Resources and ToolsPilot Site Experience Sharing
3/5/2014 17

Resources and ToolsHandbook for Implementation
3/5/2014 18

Resources and ToolsQuick Reference Pocket Guide
3/5/2014 19
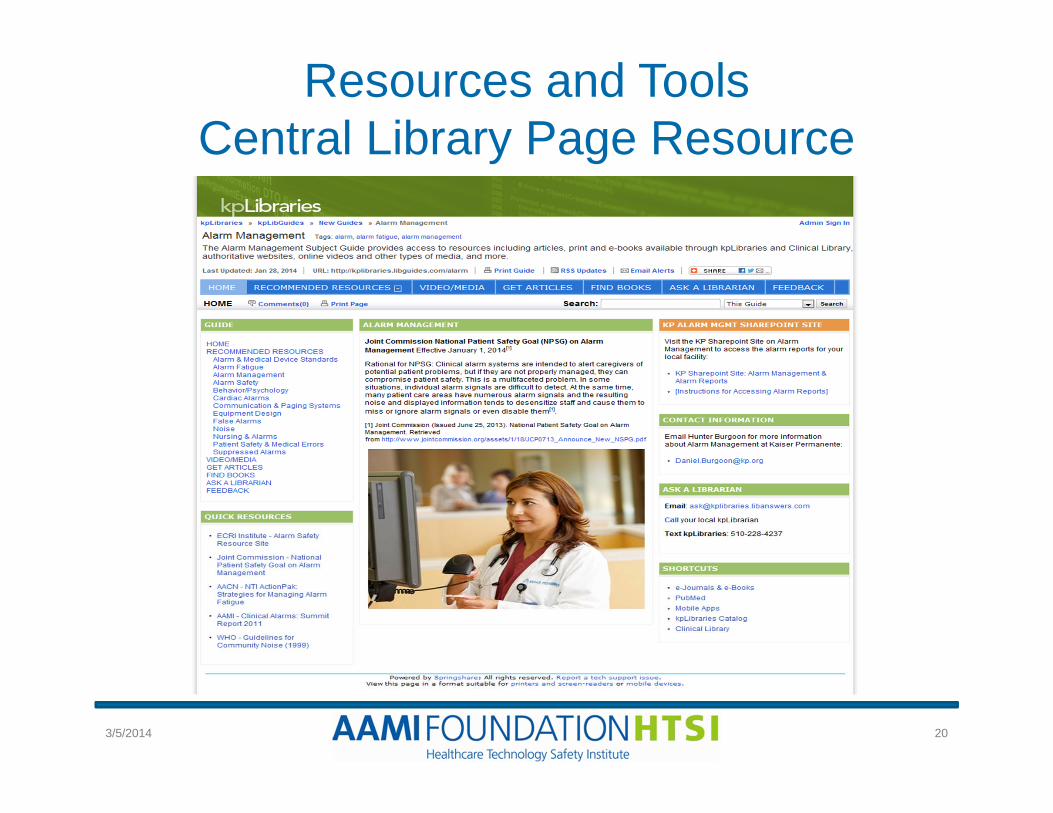
Resources and ToolsCentral Library Page Resource
3/5/2014 20

Next Steps
December• Alarm Fatigue
Handbook Draft Completed
• 2014 Beta Sites Identified and Preparation Started
• First beta launched other to follow in January
• Alarm Fatigue Library Page Work Started
January• Look for an appropriate
date for a second Alarm Summit
• Launch remaining 3 beta sites
• Refine Alarm Fatigue Handbook based on beta input
• Examine Roseville results – see if more changes could be implemented
• Library Page Launched
February• Assess beta site results
and learnings• Request approval for
New Telemetry Standard
• Socialized Beta results and develop a spread plan
March• Begin the Spread
3/5/2014 21

Recap
3/5/2014 22
Awareness and Motivation
Building Consensus
Approval Process
Pilot Project Implementation
Resources and Tools
Results
Next Steps

Children’s National Medical Center: Changing Culture to
Improve Clinical Alarms Management
Jeff Hooper, MSDirector, Biomedical Engineering
Heather Walsh, RN, MSN, PCNS-BCSimulation Outreach Coordinator
3/5/2014 23

Children’s National Health System
• 303-bed freestanding children’s hospital in Washington, DC
• Physiologic monitors at all inpatient bedsides• Monitor attendants notify RNs of alarms in acute
care units
3/5/2014 24

Objectives
Following this webinar, participants will be able to:• Identify methods for data collection• Discuss pediatric acute care considerations• Describe strategies to address monitor alarms• Disseminate efforts within institution to change
culture
3/5/2014 25

Monitor Oversight Committee
• Conducted staff survey about perceptions & concerns
• Lowered volume at central stations 3 levels• Lowered alarm volumes of the monitors in
patient rooms 3 levels • Created 6 profiles based on age with new HR
and RR ranges• Reduced desat alarm from 90 to 88• Added alarm fatigue training to RN orientation
3/5/2014 26

Clinical Alarms Committee
• Monitor Oversight Committee commissioned in June 2012 Clinical Alarms
• Included respiratory therapists, pharmacist and nurse (smart infusion pumps), nursing director, accreditation manager, & patient safety
• Reviewed & recommended alarm notification for new technology
• Executive Leadership – Executive Medical Director to oversee committee (Cardiologist)
3/5/2014 27

Low-Hanging Fruit
• Staff assist: standardized through acute care units & significantly decreased false alarms
• Reviewing code blue alarms to physician phones
• Standardized code blue testing
3/5/2014 28

Automated Notifications
• Current Practice• Nurse call, physiologic monitors
and ventilator alarms alert to Wi-Fi phone
• New Practice• Updating Wi-Fi device to iPhone and including other
EMR-related alerting• Benefit:
• Opportunity to validate which alerts are important for secondary notification
• Used Alarm Committee as the filter for this review process
3/5/2014 29

What Next?
• Alarm Committee not clear on next issue to tackle?
3/5/2014 30

Assumptions: Monitor Practices
• “Every patient is on a monitor.”• “Desat alarms create the majority of alarms.”• Patients are not taken off monitor when don’t
need any longer• “Are patients really alarming all the time?”
3/5/2014 31
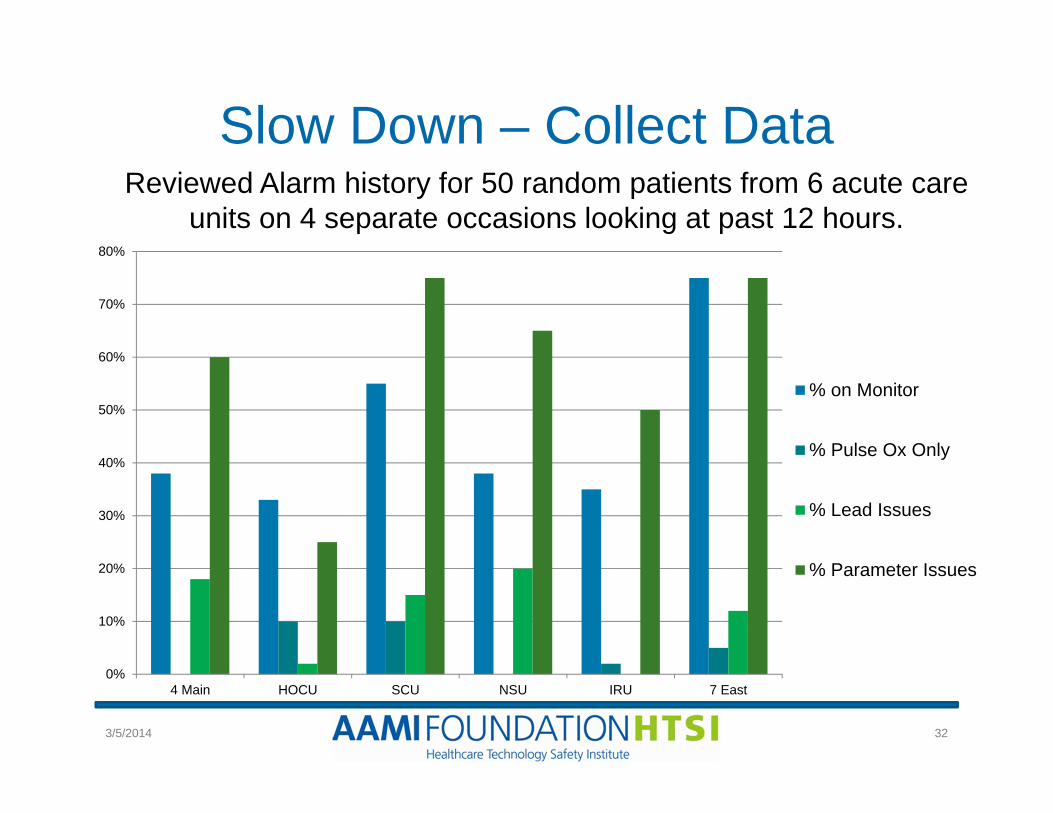
Slow Down – Collect Data
0%
10%
20%
30%
40%
50%
60%
70%
80%
4 Main HOCU SCU NSU IRU 7 East
% on Monitor
% Pulse Ox Only
% Lead Issues
% Parameter Issues
Reviewed Alarm history for 50 random patients from 6 acute care units on 4 separate occasions looking at past 12 hours.
3/5/2014 32

Primary Observations
• Primarily Issues in Acute Care areas• Most alarms are NOT pulse ox• “Tight Alarm Limits” • Electrode placement is an issue• Most patients monitored for all parameters• Less than 50% of acute care patients on
monitors
3/5/2014 33

Narrow limits (HR & RR) were biggest offender
• Patient in acute care (surgical unit)
• 50 alarms in 2 hours!• Changing RR limit to 10
would have eliminated majority of alarms
3/5/2014 34

Significant Alarms
• Apnea between low RR alarms
• Clinically significant?• Clear guidelines for
notification/patient assessment
3/5/2014 35

Limits changed vs. addressing reason for alarm?
• Significant parameter adjustment
• Patient continues to alarm
• Reason for tachycardia? Fever?
3/5/2014 36

Electrode Issues
3/5/2014 37
• Very poor electrode connection
• Baseline drift – one electrode is not attached well
• Interference or bad connection?
• Incorrect lead assignment Lead III?

Patient Experience
• “The nurses did not always respond quick enough to the monitors beeping as my child would’ve liked—the noise was very irritating to him, but I learned how to silence them.”
• “Monitors need to not beep inside the room right by my child’s head—he needs to rest. Need to add feature to turn this off, and have nurses alerted outside the room.”
3/5/2014 38

Patient Experience
• “The monitor was beeping (danger) a lot, especially during the night. I finally asked for help—it was needing to be adjusted for smaller respirations & lower settings (my son had surgery). The tech who came in was fantastic—he reset the settings. It would have been easier for me if this was done without my having to say, ‘Why is this happening?’ I was worried.”
3/5/2014 39

Next Steps
• Recommendations for trends (3 alarms for same parameter) notify RN
• Change limits as appropriate• Discuss on rounds• Daily electrode changes with skin prep• Staff education (RN, MD, PCT)• Implement new technology
3/5/2014 40
3/5/2014 41

The Johns Hopkins Hospital: An Alarming Situation:
Managing Clinical Alarms Using a Systems Approach
Maria Cvach, DNP, RN, CCRNAssistant Director of Nursing, Clinical Standards
The Johns Hopkins Hospital
3/5/2014 42

Problem: Missed Alarm2005-2006 Alarm Related Death by Device
FDA MAUDE DATABASE
Kathy Weil, MS, BSN, RNNurse Consultant
CDRH/FDA
3/5/2014 43
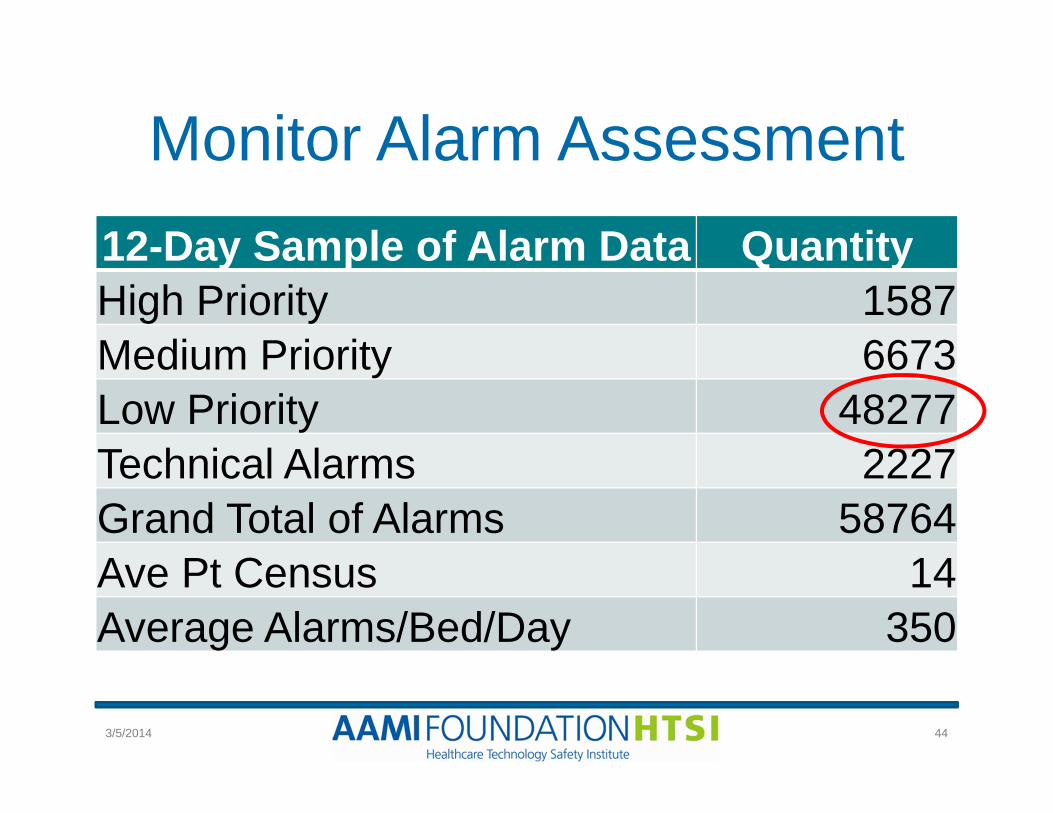
Monitor Alarm Assessment12-Day Sample of Alarm Data QuantityHigh Priority 1587Medium Priority 6673Low Priority 48277Technical Alarms 2227Grand Total of Alarms 58764Ave Pt Census 14Average Alarms/Bed/Day 350
3/5/2014 44

Ventilator Alarm Assessment
3/5/2014 45
7-Day Sample
NICU (14 beds)
PICU (25 beds)
Total ventilator alarms
3390 4156
Alarms/unit/day 242 166

An Alarming Situation
Alarms not set to actionable
limitsToo many alarming devices:
duplicate alarms
Low specificity results in
frequent false alarms
Alarm desensitization
Unclear alarm
responsibility
Large units with inability to hear
alarms
No back-up/ escalation plans
Competing priorities
© adapted from ECRI Institute 2013
3/5/2014 46

What Should All Hospitals Do?
Improving Alarm Management Requires a Systems Approach
© ECRI Institute 2013
3/5/2014 47
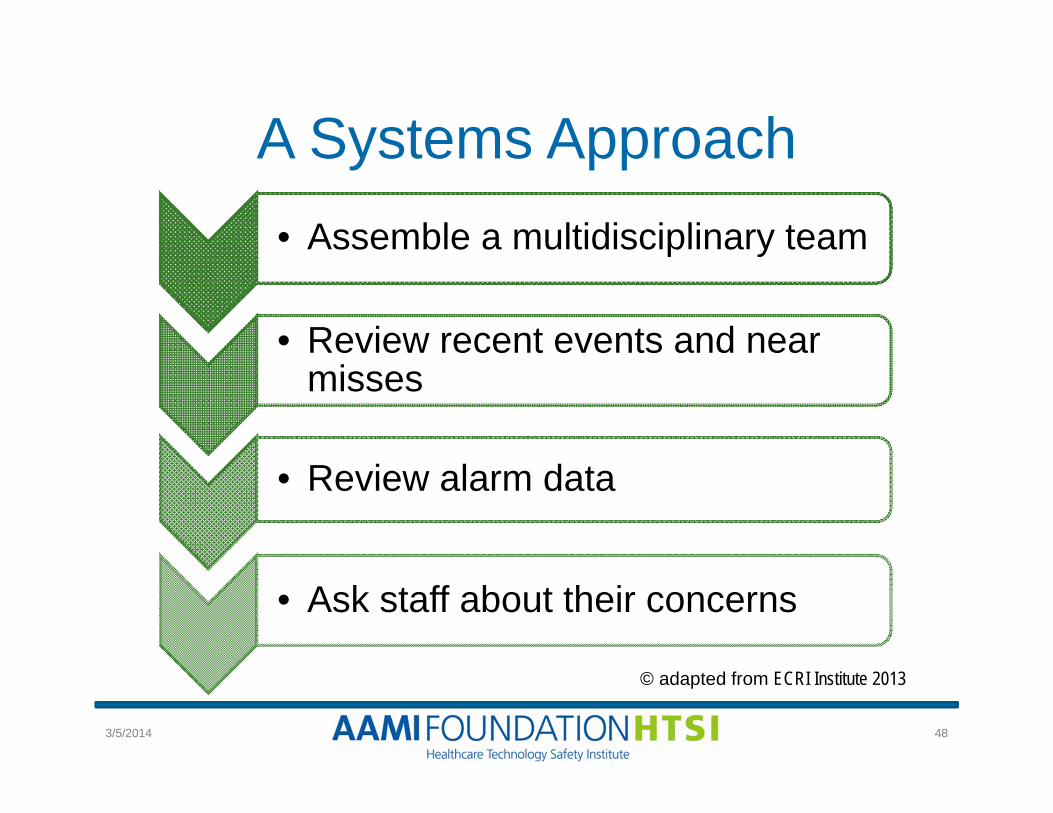
A Systems Approach• Assemble a multidisciplinary team
• Review recent events and near misses
• Review alarm data
• Ask staff about their concerns
© adapted from ECRI Institute 2013
3/5/2014 48

Text 2 Tex3
Who should be on the team?Interdisciplinary Alarm Committee
Support from Hospital Administration
Nursing Biomedical and IT
HospitalVendors
Human Factors
RT
Risk Management
Physicians Patient Rep
3/5/2014 49

A Systems Approach (cont’d)
• Review unit alarm coverage
• Identify patient safety vulnerabilities and potential failures
• Determine underlying causes of potential failures
© adapted from ECRI Institute 2013
3/5/2014 50
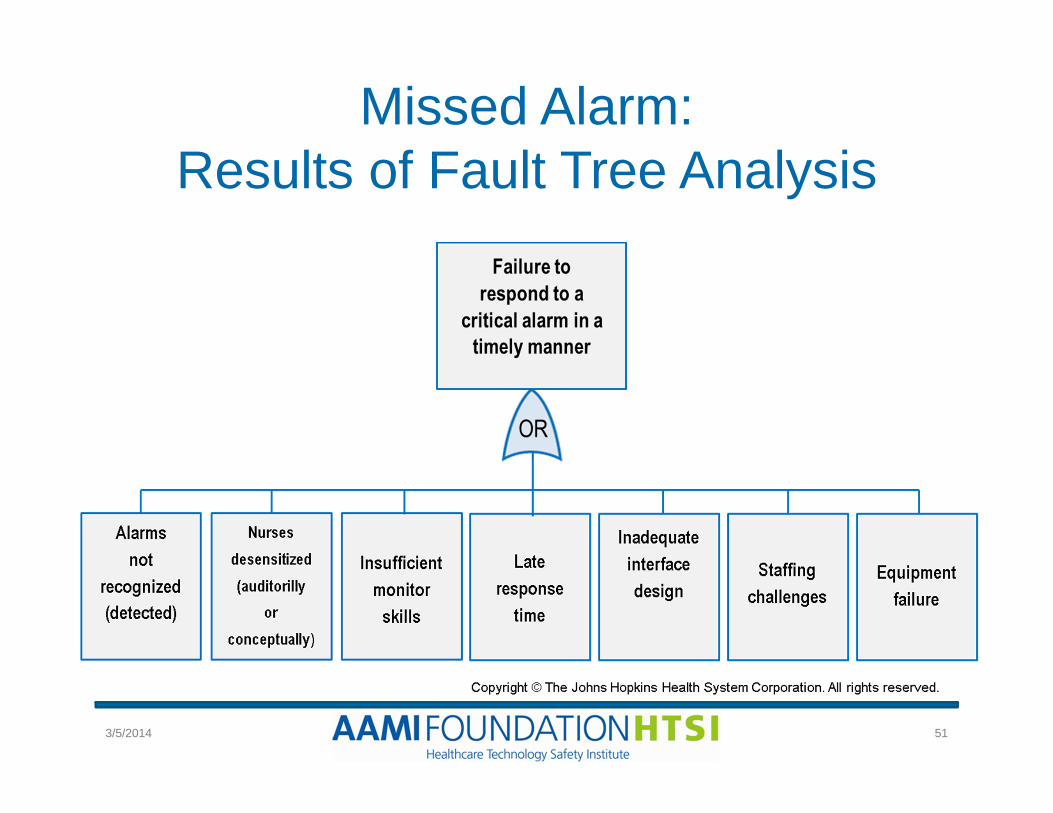
Missed Alarm: Results of Fault Tree Analysis
3/5/2014 51

Central Monitor Station
• Unit floor plan• Unit workflow• Unit staffing• Redundancy
3/5/2014 52

JHH Measures to Reduce Quantities of Alarms
• Minimize recurring alarms; standardize alarms across similar units/settings (e.g., pediatrics, telemetry, ICU)
• Enable actionable alarms• Reprioritize auditory and visual alarms
• Auditory: Higher priority• Visual: Low priority
• Adjust parameter limits appropriately for patient population
• Ensure alarm audibility and accountability3/5/2014 53
Maria Cvach DNP, RN, CCRN

Types of Cardiac Monitor Alarms
PatientExamples:
Arrhythmias, HR, BP, pulse ox
TechnicalExamples:
Lead fail, Low battery
3/5/2014 54

Detailed Alarm Data By Unit
6067
3257
1754
971 917716
521 485 439247 195 93 79 75 56 11 8 7 7
0
1000
2000
3000
4000
5000
6000
7000
3/5/2014 55

Sample JHH Monitor Alarm Inventory Default Parameter Grid
Parameters
Departments
PULSE OX %
HEART RATE BPM
BP SYSTOLIC
mmHg
BP DIASTOLIC
mmHg
BP MEANmmHg
Low High Low High Low High Low High Low HighMedical ICU 89 105 50 140 90 180 40 110 60 120Surgical ICU 89 105 50 120 90 180 40 110 55 120
Coronary Care 89 105 50 120 90 180 40 110 55 120
Cardiac Surgical ICU 89 105 50 120 80 150 40 110 55 120
Neurologic ICU 90 105 50 120 90 180 40 110 55 120
Weinberg ICU 89 105 50 120 90 180 40 110 55 120
Oncology Department
88 105 50 130 90 180 40 110 55 120
Surgical Progressive Step-down Care unit
89 105 50 140 90 180 40 110 60 120
3/5/2014 56

Sample JHH Alarm InventoryClinical Equipment Alarm
InventoryRisk to Patient and Response
Level of OversightTypically Available
Secondary AlarmNotification
High priority cardiac monitor alarms
A Varies by unit Varies by unit; includes beside split screens, auto-view on alarm, hallway waveform screens, acknowledgement pagers/phones, unit-based monitor watch
Medium/technical cardiac monitor alarms
B Varies by unit
Low priority cardiac monitor alarms
C Varies by unit
Ventilator A Varies by unit Nurse call auxiliary outlet
ECMO A High Direct supervision
Bed/chair exit alarm A/B Low Nurse call auxiliary outlet
Sequential compression device
C Low None identified
3/5/2014 57

3/5/2014 58

JHH Alarm Management QI Strategies That Resulted in
Significant Reduction in Alarms Alarm Reduction
Strategy Potential BenefitSustainability
Challenges
Parameter limits and alarm level changes
25%- 74% reduction in frequency of alarms (varied by unit)
Agreement of group on what is an actionable alarm
Daily electrode change46% reduction in frequency of alarms in MPCU and CCU
Behavior may diminish over time; patient discomfort; cost
Alarm escalation notification (each nurse carries acknowledgment pager)
53% reduction in frequency of alarms on a surgical IMC; 23% reduction in time to respond to alarm
Cost of acknowledgement pagers; Using two different devices to communicate alarms
3/5/2014 59

Maria Cvach DNP, RN, CCRN
Impact of Alarm Management Strategies
UNIT Pre-interventionsAverage Alarms/
Monitored Bed/Day
Post-interventionsAverage Alarms/
Monitored Bed/Day
% Reduction in Cardiac
Monitor AlarmsMICU 215 68 68%
CCU 515 194 62%
WICU 771 203 74%
IMC 240 50 79%
Telemetry 90 57 37%
3/5/2014 60

What Should Hospitals Do to Improve Alarm Management?
1. Engage support from leadership and a multidisclipinaryAlarm Management Committee
2. Analyze and measure the problem
3. Use data to drive change
4. Prepare an alarm inventory-risk analysis
5. Use a rapid-cycle, QI change approach
6. Identify the best methods to notify staff of alarm signals
7. Develop an alarm policy
8. Provide initial and ongoing education
3/5/2014 61

Closing Reminders
Thank you for your time and attention!
Mark Your Calendars!Current Challenges With Ventilator Alarms
Tuesday, March 25, 20141:00-2:00 pm Eastern
www.aami.org/htsi/events.html
623/5/2014

Continuing Nursing Education1.0 contact hour
For those desiring CNE, please visit the link below for the test, evaluation form, and certificate:
http://www.aacn.org/DM/CETests/Overview.aspx?TestID=1082&mid=2864&ItemID=1074&menu=CETests
The American Association of Critical-Care Nurses (AACN) is accredited as a provider of continuing nursing education by the American Nurses Credentialing
Center’s Commission on Accreditation.
3/5/2014 63

Evaluation Form and Certificate of Attendance (Non-CNE)
Please let us know how we did!http://aami.confedge.com/ap/survey/s.cfm?s=ALBP
After you fill out the evaluation form and enter your email address, you will receive an electronic
certificate by email
3/5/2014 64