Benign prostate hyperplasia -...
49
Benign prostate hyperplasia Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara
-
Upload
duongduong -
Category
Documents
-
view
236 -
download
1
Transcript of Benign prostate hyperplasia -...

Benign prostate hyperplasia
Div. of Urology, Dept. Surgery
Medical Faculty,
University of Sumatera Utara
Ref :
• Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3rd
ed, 2001ed, 2001
• Smith’s General Urology (Tanagho & McAninch eds), Lange Medical Books, 15th
ed, 2000

Definition
• Regional nodular growth of varying combinations of glandular and stromal proliferation that occurs in almost all menproliferation that occurs in almost all menwho have testes and who live long enough

TERMINOLOGY
BPH (Benign Prostatic Hyperplasia): histopathologic diagnosis
BPE (Benign Prostatic Enlargement) : anatomic diagnosis
BOO (Bladder Outlet Obstruction): anatomic diagnosis
BPO (Benign Prostatic Obstruction): BOO caused by BPE
LUTS (Lower Urinary Tract Symptoms): clinical manifestation of
lower urinary tract obstruction
Introduction
• Common non-neoplastic lesion.
• Involves peri urethral zone.
• BPH is common as men age.• BPH is common as men age.
• 25% by 50y, but 90% By 80y..!
• About 10% are symptomatic.
Prevalence
The Most Frequent Benign Tumor in Men
• 70 % of men above 60 years.*
• 90 % of men above 80 years.**• 90 % of men above 80 years.**
• 30 – 40 % of men above 70 years
• Indonesia : The Second after Stone Disease in
Urology Clinic ***
* Berry SJ et all J Urol 1984 ;132:474-79
** Carter HB , Coffey DS. Prostate 1990;16 : 39-48
*** Rahardjo D,Birowo P,Pakasi LSMed . J of Ind 1999 ; 8(4) : 260 - 63

Impact of ageing population
• With life expectancy approaching 80 years in many countries � 88% chance developing histological BPH
• � in life expectancy � significantly � the • � in life expectancy � significantly � the number of men affected by BPH
• The number of men presenting with BPH symptoms will � ± 45% in the next 10 years and � further in the following decade
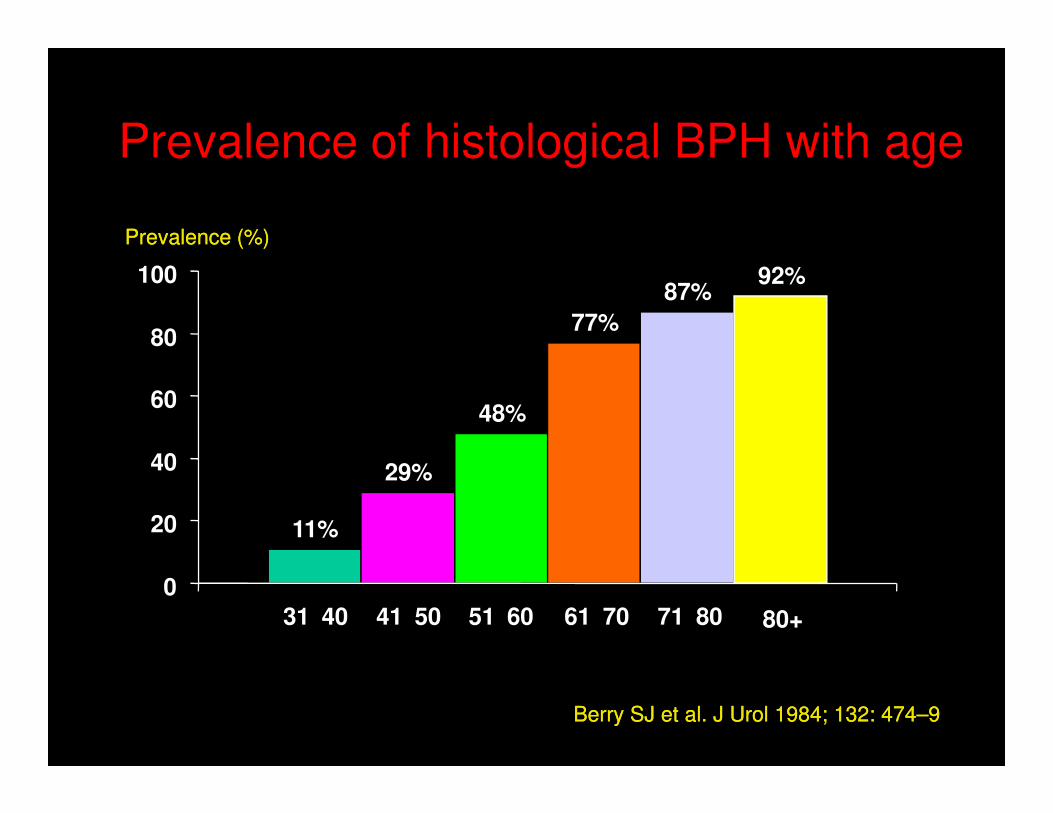
Prevalence of histological BPH with age
48%
77%
87%92%
60
80
100
Prevalence (%)Prevalence (%)
11%
29%
48%
0
20
40
60
31–40 41–50 51–60 61–70 71–80 80+
Berry SJ et al. J Urol 1984; 132: 474–9Berry SJ et al. J Urol 1984; 132: 474–9


Anatomy
• N weight about 20 g
• Classification of Lowsley : 5 lobes : anterior, posterior, median, right lateral, left lateral
• According to Mc Neal : • According to Mc Neal :
- peripheral zone
- central zone
- transitional zone
- an anterior segment
- a preprostatic sphincter zone
Causes
- Many theories
- The actual cause still not clear
- Factors are known to be important:
1. Male sex
2. Aging
3. Testosterone
4. Growth Factors (EGF, FGF, IGF II)
Pathophysiology
• Nodular hyperplasia of glands and stroma.
• Normal 20 to 30 � 50 to 100 gm.
• Press upon the prostatic urethra.
• Obstruction - difficulty on urination
• Dysuria, retention, dribbling, nocturia
• Infections, hydronephrosis, renal failure.
• Not a premalignant condition*
Prostate growth
Increased urethral resistance
Decompensation
Flow ↓
Bladder emptying ↓,
hesitancy, intermittency
Mechanism
• Hormonal imbalance with ageing.
• Estrogen sensitive peri-urethral glands.
• Accumulation of DHT in the prostate and its
growth-promoting androgenic effect
• Some Drugs (Finasteride) inhibit DHT �
diminishes prostatic enlargement.

Morphology
• Microscopically, nodular prostatic hyperplasia
consists of nodules of glands and intervening
stroma. (Mostly glands)stroma. (Mostly glands)
• The glands variably sized, with larger glands
have more prominent papillary infoldings.
• Nodular hyperplasia is NOT a precursor to
carcinoma.

Symptoms LUTS
• Weaker, smaller
stream
• Hesitancy
• Intermittent /
• Nocturia
• Frequency
• Urgency
• dysuria• Intermittent /
interrupted flow
• Feeling of incomplete
emptying or retention
• Terminal dribbling
• dysuria
• Symptoms may
worsen with alcohol
and caffeine, cold
remedies


How to Assess the Patient?
Diagnosis
• Anamnesis
Cardinal symptoms:
Weak StreamWeak Stream
Frequency
Nocturia
Storage symptoms, Voiding Symptoms
Scoring System : M.I, IPSS

1. KENCING TIDAK LAMPIAS
Dalam sebulan ini berapa sering anda merasakan sensasi tidak lampias
saat kencing (terasa belum habis) ?
2. Sering Kencing
Dalam sebulan ini berapa sering anda merasa Ingin Kencing Lagi dalam
2 jam setelah anda Kencing
3.KENCING TERPUTUS PUTUS
Dalam sebulan ini berapa sering kencing anda terhenti sejenak, lalu mulai
5
Gejala Tidak Pernah < 20 % < 50 %
2 3
=50% > 50 % Hampir Selalu
0 1 2 3 4
4 5
0 1 2 3 4 5
0 1
BPH SYMPTOM SCORE / IPSS
Dalam sebulan ini berapa sering kencing anda terhenti sejenak, lalu mulai
lagi ( Terputus putus)
4.TIDAK DAPAT MENUNDA KENCING
Dalam Sebulan ini Berapa sering anda merasa kesulitan untuk menunda
Kencing
5.PANCARAN KENCING YANG LEMAH
Dalam sebulan ini berapa sering anda mengalami Pancaran Kencing Lemah
6. MENGEDAN SAAT KENCING
Dalam sebulan ini berapa sering anda mengedan sebelum memulai kencing
7.KENCING DI MALAM HARI
Dalam Bulan ini berapa sering anda harus bangun tidur di malam hari untuk
Kencing
0 1 2 3 4 5
5
4 5
0 1
0 1 2 3
1 2 3
2 3 4
4 5
Tdk Pernah, =0 1Kali, =1 2kali, =2 3kali, =3 4kali, =4 5kali, =5
0


IPSS (International Prostate
Symptom Score ).
0 – 7 : Mild
8 - 19 : Moderate8 - 19 : Moderate
20 – 35 : Severe
≤ 7 : Watchful & Waiting
≥ 7 : Medical treatment

Diagnosis
Physical
examination :
Prostate :
1. Size
DRE 2. Nodule
3. Consistency
4. Tenderness

DRE

Diagnosis
Uroflowmetry Qmax
Voided volumeVoided volume
Residual urine TAUS
Catheter

Uroflowmetry
Lab test
• Blood Count
• Serum Electrolyte
• Serum Creatinine• Serum Creatinine
• Serum PSA
• Urine :
Proteinuria
Sediment
Culture

IMAGING
• TRUS
• Transabdominal Ultrasound
• With Indication :• With Indication :
IVP
Cystography
CT-Scan
MRI
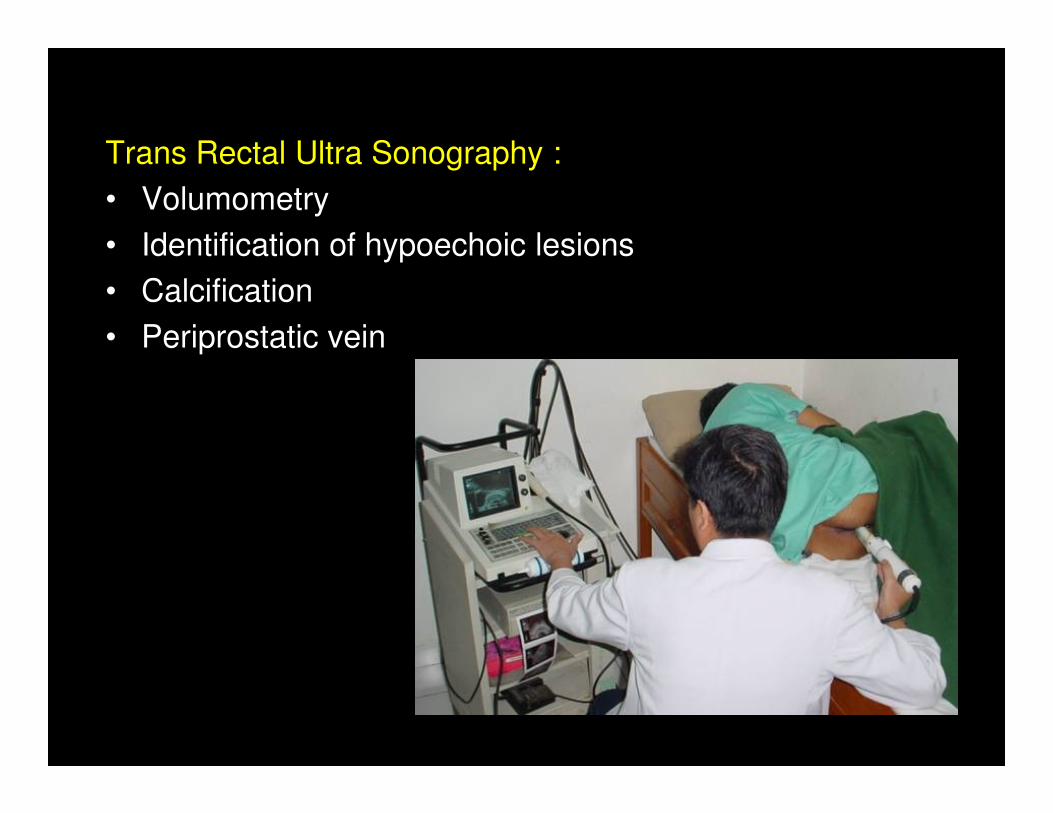
Trans Rectal Ultra Sonography :
• Volumometry
• Identification of hypoechoic lesions
• Calcification
• Periprostatic vein

� Urethral stricture
� Bladder neck contracture
Differential diagnosis
� Bladder neck contracture
� Small bladder stone
� Locally advanced prostate ca
� Poor bladder contractility

Effects of benign prostatic obstruction
• Irreversible bladder changes
• Thickening of the bladder wall
• Recurrent haematuria
• Bladder diverticulum formation
• Repeat urinary tract infections• Repeat urinary tract infections
• Bladder stone formation
• Upper tract dilatation
• Renal impairment
Complications
• Increased risk of UTI due to urinary retention
• Calculi due to alkalinization of residual urine
• Hematuria due to overstretched blood • Hematuria due to overstretched blood
vessels
• Pyelonephritis
• Renal failure
Indication for treatment
• Absolute or near absolute :
- refractory or repeated urinary retention
- azotemia due to BPH
- recurrent gross hematuria- recurrent gross hematuria
- recurrent or residual infection due to BPH
- bladder calculi
- large residual urine
- overflow incontinence
- large bladder diverticula due to BPH

Treatment
• Watchful waiting
• Medical therapies• Medical therapies
• Intervention therapies• Minimally invasive therapies
• Surgical therapies
Watchful waiting
Altering modifiable factor such as:
– Concomitant drug
– Regulation of fluid intake especially in the evening
– Life style change (avoid sedentary life)– Life style change (avoid sedentary life)
– Dietary advice (avoid excessive intake of alcohol, and
highly seasoned or irritative foods)
Evaluation/ monitoring : after 6 months/ 1 year
IPSS, uroflowmetry, post-void
residual urine volume

Medical therapy
• I.P.S.S. > 7
• Flow > 5 ml/s• Flow > 5 ml/s
• Residual urine < 100 ml
• No hard nodule
• PSA < 4 ng/dl
Medical therapy
• Reducing smooth muscle tone (dynamic component) : α-1 adrenergic blocker
• Short acting : prazosin, afluzosin• Long acting : doxasosin, terazosin, tamsulosin
• Reducing prostatic mass (static component):5α redutase inhibitor (finasteride, epristeride)5α redutase inhibitor (finasteride, epristeride)
estrogen aromatase inhibitor
LHRH agonist / antagonist GF inhibitor
antiandrogens
• Unknown
phytotherapy
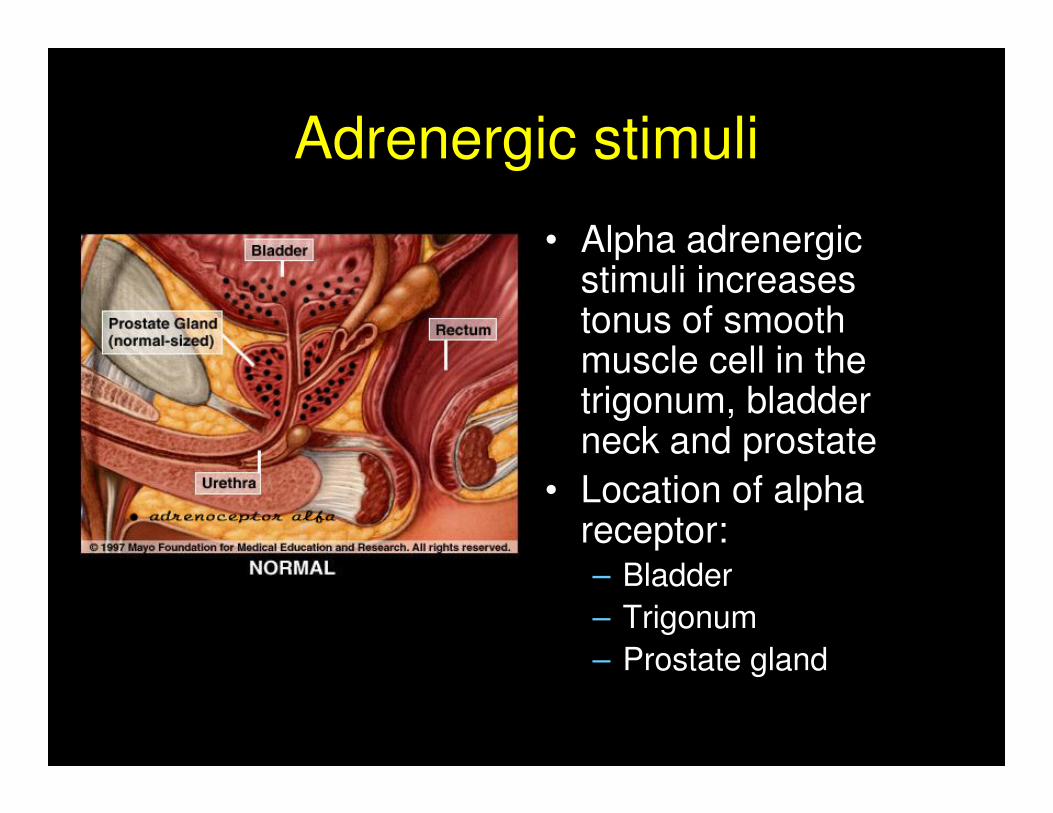
Adrenergic stimuli
• Alpha adrenergic stimuli increases tonus of smooth muscle cell in the trigonum, bladder trigonum, bladder neck and prostate
• Location of alpha receptor:– Bladder
– Trigonum
– Prostate gland

Mode of action alpha blocking agent
• Alpha adrenergic blocking agent blocks adrenergic stimuli � relaxation of the adrenergic stimuli � relaxation of the smooth muscle cell:
– intra urethral pressure ↓
– Improvement of urine flow

Sintesis Protein
Transkripsi DNA
Hipotalamus
LHRHLHRH
ACTHACTH
Rationale of 5Alpha reductase inhibitor
Reseptor Inti
+
Transkripsi DNA
T DHT
5-α reductase
DHT


Invasive Treatment for BPH
Absolute indication:
• Chronic Retention
• With Hematuria
• Concomitant Bladder stone• Concomitant Bladder stone
• Intractable UTI
• Deteriorating kidney function
Relative indication:
• Huge PVR due to obstruction or low Qmax
• Refuse medical treatment
• Failure in medical treatment

Intervention therapy
• Minimally invasive therapy– Thermotherapy
• TUNA (Trans Urethral Needle Ablation)• HIFU (High Intensity Focused Ultrasound)• HIFU (High Intensity Focused Ultrasound)• TUMT (Trans Urethral Microwave Theraphy)• Laser
– Stent
• Surgical therapy• TUIP (Trans Urethral Incision of the Prostate)• TURP (Trans Urethral Resection of Prostate)• Open prostatectomy• TUVP (Transurethral Vaporization of the Prostat)• Laser

Invasive Treatment for BPH
• TURP (gold standard)
• Laser resection (Hol YAG Laser)
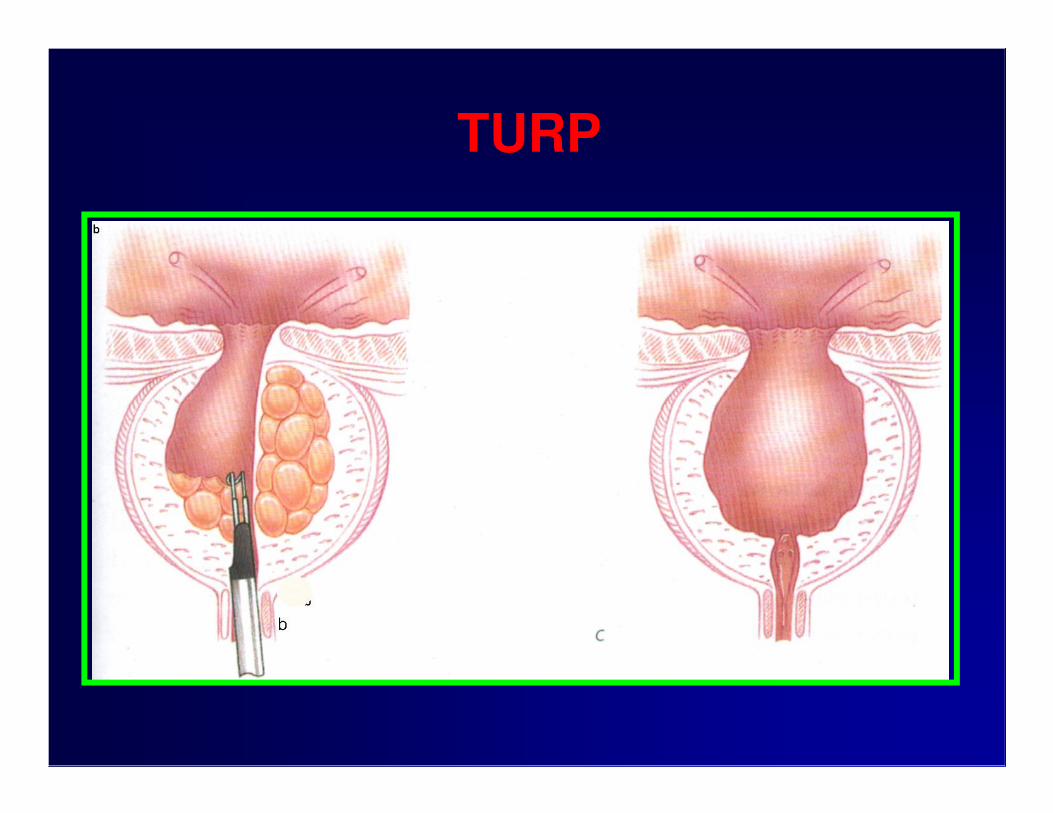
TURP

JARINGAN PROSTAT

TUIP