Benha University Benha Facultyof Medicine Medical ...
19
1 Benha University Benha Facultyof Medicine Medical Biochemistry Department Final Exam of Medical Biochemistry for 2 nd year medical students Date: 2/6/2012 Course code (0704) Important Instructions For All Students:Please Read Carefully ( Illustrate with chemical formula when needed) 1-Give an account on: ( 10 marks) a-Glycogenesis ( definition,importance&steps) (4marks) b-Regulation of lipolysis (4marks) c-Primary hyperoxaluria (2marks) 2-Write short notes on: (10 marks) a-Von Gierk’s disease (2.5marks) b-Reverse cholesterol transport (2.5marks) c-Role of phosphatidylinositol in signal transmission across membrane. (2.5 marks) d- Lipotropic factors (definition&classification) (2.5marks) 3-Enumerate: (13 marks) a-SAM is used in transmethylation reactions (four only) (2marks) b-Hormones which need c AMP as a secondary messenger in their actions. (2marks) c- Importance of HMP shunt (2.5marks) d-Uncouplers of oxidative phosphorylation. (3marks) e-Causes of creatinuria (two physiological and five pathological ) (3.5 marks) Allocated time (Three Hours including MCQ) Total allocated marks (75 marks) Number of papers (4 papers including MCQ) Number of questions (10 questions including MCQ) How to answer ex: comparisons must be in tables, chemical structures must be illustrated by formulae Attention All questions are to be answered
Transcript of Benha University Benha Facultyof Medicine Medical ...
1
Benha University Benha Facultyof Medicine
Medical Biochemistry Department
Final Exam of Medical Biochemistry for 2nd
year medical students
Date: 2/6/2012 Course code (0704)
Important Instructions For All Students:Please Read Carefully
( Illustrate with chemical formula when needed)
1-Give an account on: ( 10 marks)
a-Glycogenesis ( definition,importance&steps) (4marks)
b-Regulation of lipolysis (4marks)
c-Primary hyperoxaluria (2marks)
2-Write short notes on: (10 marks)
a-Von Gierk’s disease (2.5marks)
b-Reverse cholesterol transport (2.5marks)
c-Role of phosphatidylinositol in signal transmission across membrane.
(2.5 marks)
d- Lipotropic factors (definition&classification) (2.5marks)
3-Enumerate: (13 marks)
a-SAM is used in transmethylation reactions (four only) (2marks)
b-Hormones which need c AMP as a secondary messenger in their actions.
(2marks)
c- Importance of HMP shunt (2.5marks)
d-Uncouplers of oxidative phosphorylation. (3marks)
e-Causes of creatinuria (two physiological and five pathological )
(3.5 marks)
Allocated time (Three Hours including MCQ)
Total allocated marks (75 marks)
Number of papers (4 papers including MCQ)
Number of questions (10 questions including MCQ)
How to answer
ex: comparisons must be in tables, chemical structures
must be illustrated by formulae
Attention All questions are to be answered
2
4-On biochemical bases explain: (11 marks)
a-Malonic acid inhibits Kreb’s cycle (1 mark)
b-Drugs as statins group (Mevastatin) is used in treatment of Hypercholesterolemia
(1 mark)
c-Hyperuricemia associated with ,Lesch-Nyhan syndrome (1mark)
d- High serum ammonia is toxic and produces brain damage (1mark)
e-Alcoholism causes fatty liver (2 marks)
f-Cataract is one of the manifestations of galactosemia (2mark)
g-Vitamin C deficiency may leads to anemia (3 marks)
5-In a table differentiate between: (5 marks)
A-Type I and type II diabetes mellitus. (2.5marks)
B-Fate soluble and water soluble vitamins (2.5 marks)
6-Illustrate all of the following reactions with chemical formulae:(6marks)
A-Tyrosine to catecholamines. (2marks)
B-Tryptophan to serotonin. (2marks)
C-Pyruvate to lactate (1mark)
D-Aspartic acid to oxaloacetic acid (1mark)
7-Explain how to detoxify: (3marks)
A-Aspirin (1mark)
B-Benzoic acid (2marks)
8- Define and complete the following : (4marks each 0.5 mark)
1. Nitrogen balance 2. Creatinuria 3. Albinism
4. Proteinuria. 5. Glycosuria.
6. Plasma creatinine level is………
7. Key enzyme in urea cycle is……
8. Normal fasting glucose level in blood is …………
9. Case (3 marks)
An obese 51 years old woman was admitted to hospital in a semiconscious state. Her
blood glucose level was 368 mg/dl. Her urine was positive for both glucose and ketone bodies
A- What is the possible diagnosis? (1.5 marks)
B- On biochemical basis explain the presence of ketone bodies in the patient’s urine
(1.5 marks)
10-MCQ (10marks)

3
Benha University Benha Facultyof Medicine
Medical Biochemistry Department
Final Exam of Medical Biochemistry for 2nd
year medical students
Date: 2/6/2012 Course code (0704)
Model answers) 0 marks each 0.5 mark( 1 Choose the correct answers :
1-Which of the following compounds is a
required substrate for purine biosynthesis? D
(A)5-methyl thymidine.
(B)Allopurinol.
(C) Ribose phosphate.
(D)5-phosphoribosylpyrophosphate(PRPP)
2-Which of the following compounds is an
analogue of hypoxanthine?B
(A)Oxipuranol. (B)Allopurinol.
(C) Ribose phosphate.
(D)5- phosphoribosylpyrophosphate(PRPP).
3-Which of the following contributes nitrogen
atom number “1” to both purine and
pyrimidine rings? A
(A)Aspartate (B)Glutamate.
(C) Carbon dioxide.
(D)Carbamoyl phosphate
4-Ergocalciferol is: C
(A)Provitamin D2. (B)Provitamin D3
(C) Vitamin D2 (D)Vitamin D3
5-Insulin activates: D
(A)Lipolysis. (B)Ketogenesis.
(C) Gluconeogenesis. (D)Glycolysis
6-All are true regard to glucagon,except: D
(A)Increases lipolysis.
(B)Stimulate glycogenolysis.
(C) Stimulate gluconeogenesis.
(D) Stimulate glycogen synthase.
BThe precursor of thyroid hormones is :-7
(A)Histidine. (B)Tyrosine.
(C)Alanine. (D)Glycine.
D Uridine diphoshpate glucose (UDPG) is :--8
(A)-Required for metabolism of galactose.
(B)-Required for synthesis of glucuronic acid.
(C)-A substrate for glycogen synthase.
(D)-All of the above.
cholesterol diet exhibit decreased -Animal fed a high-9
cholesterol synthesis by liver because of the inhibition
B of which one of the following enzymes?
(A)HMG CoA synthetase.
(B) HMG CoA reductase.
(C) HMG CoA lyase.
(D)Mevalonate kinase.
The major process responsible for maintaining -10
B blood glucose 4 hours after the last meal is:
A-Glycolysis.
B-Glycogenolysis.
C-The pentose phosphate pathway.
D-Gluconeogenesis.
11- high –energy phosphate bond among the
following is : B
(A)-Glucose-6-phosphate.
(B)-1,3 –Bisphosphoglycerate.
(C)-Glucose -1-phosphate.
(D)-All of the above.

4
12-After an overnight fast ,the blood levels of
which of the following will be higher in a
person with a carnitine deficiency than in
normal person? B
(A)Glucose. (B)Fatty acids.
(C) Acetoacetate.
(D) 3-Hydroxybutyrate.
13-High intake of which amino acid can
prevent pellagra in people consuming a
niacin-deficient diet? D
(A)Lysine. (B) Methionine.
(C) Threonine. (D) Tryptophan.
14-Which of the following does not take part
in the human urea cycle? D
(A)Arginase. (B) Aspartate.
(C) Argininosuccinate. (D)Urease
15-A person with Insulin –dependent diabetes
mellitus (IDDM) who has neglected to take
insulin injections will have: D
(A)Increased fatty acid synthesis from glucose in
liver.
(B)Decreased conversion of fatty acids to ketone
bodies.
(C)Increased store of triacylglycerol in adipose
tissue.
(D)Increased conversion of acetoacetate to
acetone.
16-Which of the following coenzymes is not
derived from vitamins? D
(A)TPP(thiamine pyrophosphate)
(B)Pyridoxal phosphate.
(C) Co A-SH.
(D)Lipoamide.
17-The synthesis of 1,25 dihydroxycholecalciferol
takes place: C
(A)In the skin under the action of ultraviolet light from
7-dehydrocholesterol.
(B)In the liver from cholecalciferol glucocorticoids.
(C)In the kidney from 25-hydroxycholecalciferol.
(D)In the intestine from cholicalciferol.
18-Biotin is a co-enzyme for all the following carbon
Dioxide fixation reactions except: D
(A)Pyruvate carboxylase.
(B)Acetyl CoA carboxylase.
(C) Propionate carboxylase.
(D)Carbamoyl phosphate synthetase.
19-pyridoxal phosphate is required for all the
following reactions, except : D
(A)Transamination.
(B)Deamination.
(C) Decarboxylation of amino acids.
(D)Carboxylation.
20-Hypercholesterolemia is seen in the following
conditions,except: B
(A)Diabetes mellitus.
(B)Hyperthyrodism.
(C) Nephrotic syndrome.
(D)Obstructive jaundice.
NB:
Oral exam will be held on Sunday 3/6/2012 at
10 AM in medical biochemistry department.
Good Luck
Head of the Department.
Prof . Dr . Amal Abou El Fadle .

5
:Model answers 1-Give an account on: ( 10 marks)
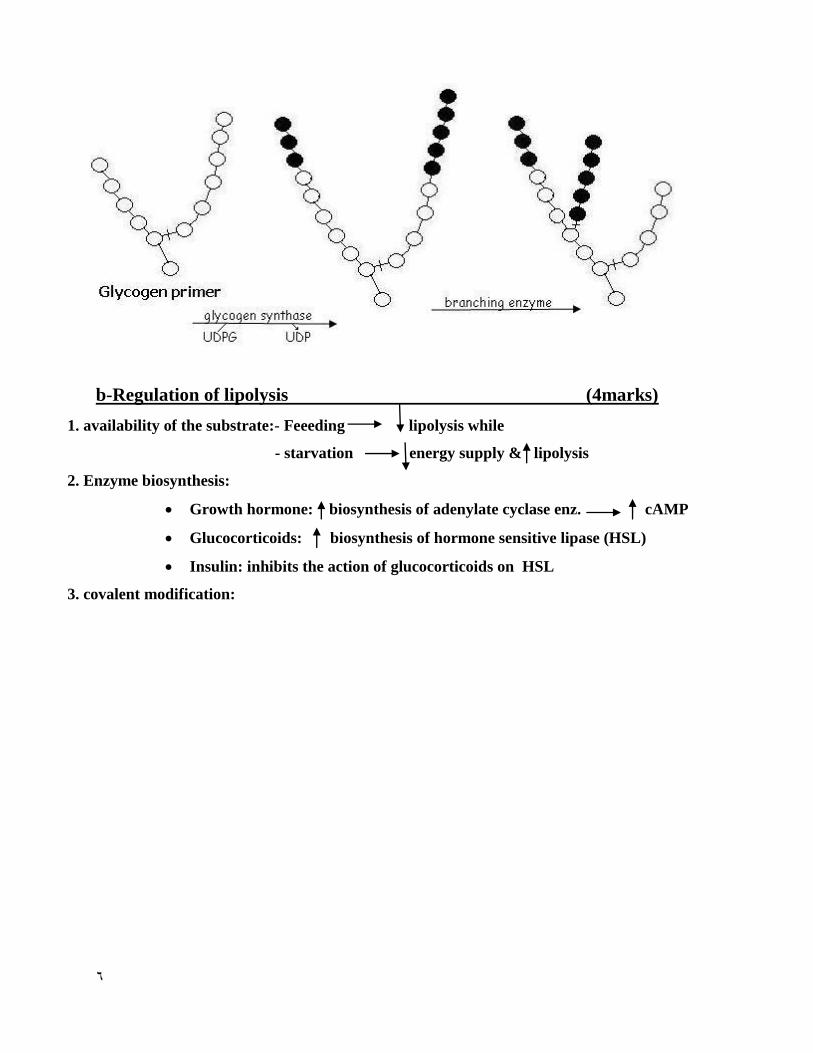
a-Glycogenesis ( definition,importance&steps) (4marks)
Definition : The formation of glycogen from glucose or other hexoses.
Glucose or other hexoses Glycogen (one mark)
Importance : Storage of excess glucose, or other hexoses taken in food.
(one mark)
Steps : (2 marks)
1- Glucose is phosphorylated to G-6-P by glucokinase.
2- G-6-P is then converted to G-1-P by phosphoglucomutase.
3- G-1-P reacts with UTP to form UDPG by UDPG pyrophosphorylase,
UDPG acts as a substrate for glycogen synthesis.
4- Glucose is transferred from UDPG to a glycogen primer forming 1,4-
glucosidic bonds. The reaction is catalyzed by the enzyme glycogen synthase
(the key enzyme) whose function is to elongate short branches in the glycogen
tree up to 12 glucose units.
5- The branching enzyme transfers some of glucose units from the end of a
long branch to one of glucose units in the middle of an adjacent long branch
forming 1,6-glucosidic bond. A new branch appears on which glycogen
synthase can act again.
6
b-Regulation of lipolysis (4marks)
1. availability of the substrate:- Feeeding lipolysis while
- starvation energy supply & lipolysis
2. Enzyme biosynthesis:
Growth hormone: biosynthesis of adenylate cyclase enz. cAMP
Glucocorticoids: biosynthesis of hormone sensitive lipase (HSL)
Insulin: inhibits the action of glucocorticoids on HSL
3. covalent modification:

7
c-Primary hyperoxaluria (2marks)
1- Primary hyperoxaluria :
- Congenital disease caused by decreased metabolism of glyoxalic acid either by:
a- Oxidative decarboxylation to formic acid, or
b- Transamaination to glycine.
- Glyoxalic acid is accumulated and is oxidized to oxalic acid (fig.27).
- There is excretion of large amount of oxalate in urine.
- Oxalate reacts with calcium forming insoluble Ca, oxalate stone in urinary tract.
- Large stones if bilateral may cause renal failure.
2-Write short notes on: (10 marks)
a-Von Gierk’s disease (2.5marks)
Type I glycogenosis ;(Von Gierke’s disease):( each 0.5 mark)
due to deficiency of glucose-6-phosphatase in liver & kidneys leading to accumulation of large amounts of glycogen & enlargement of liver & kidneys together leading to accumulation of large amounts of normal glycogen in liver and kidney leading to 1-Enlargement of liver and kidney. 2-Fasting hypoglycemia : because liver G-6-P cannot leave the liver to supply glucose to blood during fasting .
8
3-Hyperlipemia & hypercholesterolemia : because there is shift to lipid as metabolic fuel ,there is increased lipolysis (increased FFA in plasma ) Increased ketone bodies formation (increased ketogenesis) leading to metabolic acidosis. 4-Hyperuricemia (gout): because G-6-P is elevated in the liver cells leading to increased HMP shunt increased R-5-P stimulation of de novo synthesis of purines increased uric acid formation (hyperuricemia ) 5-lactic Acidemia : because liver cannot form glucose from lactate (no Cori’s cycle )which leads to acidosis.
b- Reverse cholesterol transport (2.5marks)
it is the efflux of cholesterol from peripheral cells to HDL, esterification of cholesterol by
LCAT, binding of the cholesterol –rich HDL (HDL2) to liver & steroidogenic cells by HDL
receptors scavenger receptor class B (SR-B)
c- Role of phosphatidylinositol in signal transmission across membrane
(2.5 marks).
It acts as a second messenger for many hormones:
1. hormone binds to its receptor
2. the occupied receptor interacts with globular protein (Gs) which releases GDP and binds GTP
3. α- subunit of Gs protein dissosciates & activates phospholipase C
4. active phospholipase C cleaves phosphatidyl inositol 4,5-bisphosphate to inositol triphosphate
(IP3) and diacyl glycerol (DAG)
5. IP3 binds to a specific receptor on the endoplasmic reticulum causing release of sequestered
Ca2+
6. Ca2+
and DAG activate protein kinase C (PKC)
7. PKC phosphorylates cellular proteins that mediate cellular response to the hormone.
d- Lipotropic factors (definition&classification) (2.5marks)
9
definition: the essential substances for mobilization of triacyl glycerol from liver
classification:
1. substances needed for priotein biosynthesis:
Proteins of high biological value to supply the body with essential a.a
Methionine : the labile methyl donor necessary for choline & carnitine biosynthesis
2. Substances nededed for phospholipid synthesis:
Essential fatty acids, inositol, choline, folic acid & vitamine B12, methionine & glycine
betaine
3. substances inhibiting lipid peroxidation:
Vitamin A & selenium
3-Enumerate: (13 marks)
a-SAM is used in transmethylation reactions (four only)
(2marks) 4 only each 0.5 mark
SAM is used in many transmethylation reactions as follows:
a- Guanidoacetate to creatine.
b- Ethanolamine to choline.
c- Nor-epinephrine to epinephrine.
d- N-acetyl serotonin to melatonin.
e- Carnosine to anserine.
f- Nicotinamide to N-methyl nicotinamide.
g- Methylation of DNA and RNA.
b-Hormones which need c AMP as a secondary messenger in their actions.
(2marks)
Many hormones as catecholamines; ACTH; TSH; FSH; LH; glucagon; parathromone and
calcitonin ( each 0.25 mark)
c- Importance of HMP shunt (2.5marks)
IMPORTANCE :
11
I. SOURCE OF RIBOSE-5-P : (one mark)
Ribose –5--P is important for nucleotide & nucleic acid synthesis
II. Source of NADPH+H+ (reduced NADP
+): (1.5 marks)
which is important coenzyme for many enzymes e g:
1) Synthesis of a) Fatty Acids.
b) Steroids (required by the enzyme HMGCO-A reductase).
2) Hydroxylation of steroids & other compounds e.g. phenylalanine &
tryptophan etc.
O2 H2O
A – H A –OH
NADPH+H+ NADP
+
3) Keeps glutathione Keeps iron of Hb in reduced state
in reduced state reduces fragility of RBCs.
4) Some reduction reactions a) Folic acid FH4.
b) Retinal Retinol.
5) Source of energy (50%) in cornea, retina & eye lens.
N.B. NADPH+H+ is required by the enzyme glutathione reductase which keeps
glutathione in the reduced state.
d-Uncouplers of oxidative phosphorylation. (3marks)
each 0.5 mark
Oxidation phosphorylation uncouplers are group of compound that include:
1- 2.4 dinitrophenol was used as weight loss but was discontinued because of its toxicity.
2- Dicumarol, which is an anticoagulant.
3- Bilirubin, in abnormal high dose as in jaundice
4- Thyroid hormones,in abnormal high level
5- calcium in larg dose
6- Toxin of some pathogenic microganisms also act as uncoupler.
e-Causes of creatinuria (two physiological and five pathological )
(3.5 marks)
11
Causes of physiological creatinuria:
1- In young children (decreased muscle mass).
2- In females during pregnancy and early postpartum period.
Causes of pathological creatinuria:
In all condition of muscle wasting which include:
1- Starvation.
2- Diabetes mellitus.
3- Fevers.
4- Hyperthyroidism.
5- Hypogonadism.
6- Vit E deficiency.
7- Degenerative muscle diseases (myopathies).
4-On biochemical bases explain: (11 marks)
a-Malonic acid inhibits Kreb’s cycle (1 mark)
malonic acid competitively inhbits succinate dehydrogenase enzyme and causes accumulation of
succinic acid due to inhibition of the reaction
succcinic acid fumaric acid
b-Drugs as statins group (Mevastatin) is used in treatment of
Hypercholesterolemia (1 mark)
This group of drugs competitively inhibits HMG- CoA reductase enzyme which is the key
enzyme for cholesterol biosynthesis
c-Hyperuricemia associated with ,Lesch-Nyhan syndrome (1mark)
this syndrome occurs due to congenital deficiency of HGPRTase enzyme leading to increase
PRPP so de novo synthesis of purines increases than tissue needs leading to hyperuricemia
12
d- High serum ammonia is toxic and produces brain damage (1mark)
ammonia reacts with α- ketoglutarate to form glutamate. The resulting depleted levels of α-
ketoglutarate then impairs the function of TCA cycle in the neurones
e-Alcoholism causes fatty liver: (2 marks)
1.oxidation of ethanol increases NADH+H / NAD ratio which interfers with FA oxidation
CH3.CH2OH + NAD alcohol dehydrogenase CH3.CHO + NADH+H2. oxidation of
acetaldehyde increases active acetate & subsequent lipogenesis
f-Cataract is one of the manifestations of galactosemia (2mark)
Cataract is due to : ( each one mark)
1- Accumulation of galactose in the eye lens which is reduced to its alcohol galactitol increase osmotic pressure overhydration of lens denaturation of the natural translucent lens proteins cataract.
2-Accumulation of Gal.–1-P inhibition of glycolysis & inhibition of
G-6--P dehydrogenase inhibition of HMP shunt ATP cataract.
g-Vitamin C deficiency may leads to anemia (3 marks)
1. microcytic hypochromic anemia due to:
Loss of blood due to hemorrhage
Decreased iron absorption
2. macrocytic hyperchromic anemia due to:
Decreased activation of folic acid to tetrahydrofolate
3. accumulation of met hemoglobin leading to functional anemia
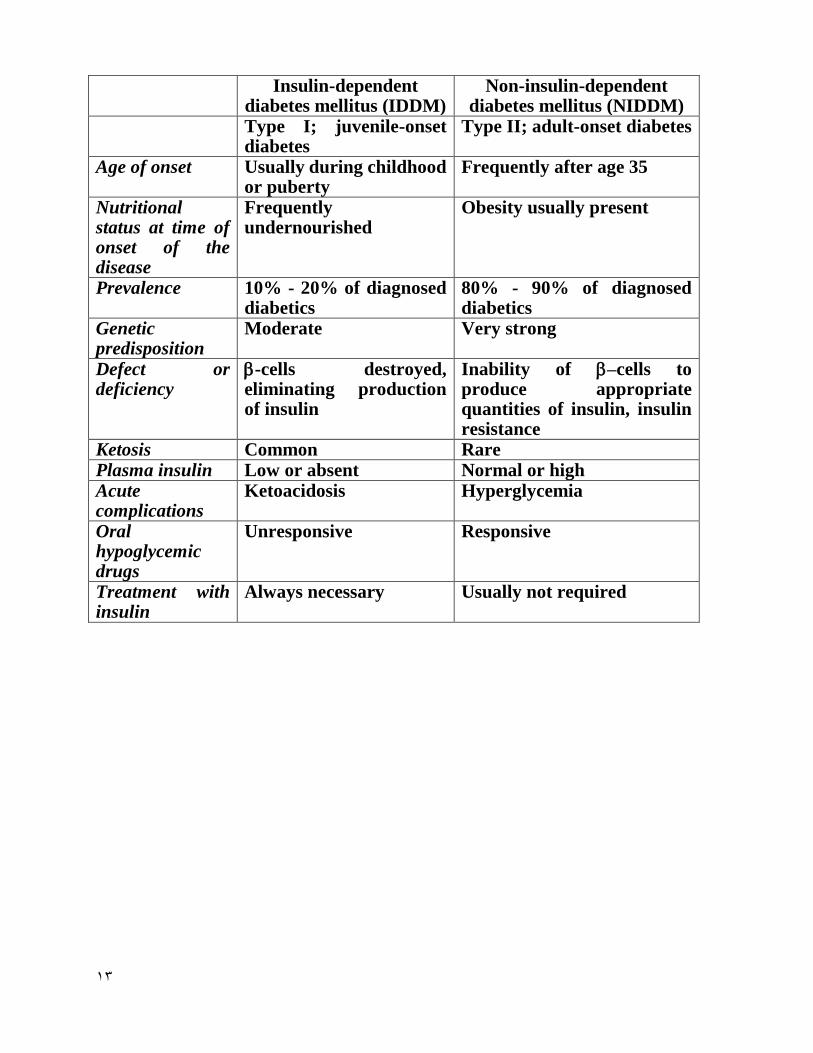
5-In a table differentiate between: (5 marks)
A-Type I and type II diabetes mellitus. (2.5marks)
Five difference each 0.5 mark
13
Insulin-dependent diabetes mellitus (IDDM)
Non-insulin-dependent diabetes mellitus (NIDDM)
Type I; juvenile-onset diabetes
Type II; adult-onset diabetes
Age of onset Usually during childhood or puberty
Frequently after age 35
Nutritional status at time of onset of the disease
Frequently undernourished
Obesity usually present
Prevalence 10% - 20% of diagnosed diabetics
80% - 90% of diagnosed diabetics
Genetic predisposition
Moderate Very strong
Defect or deficiency
-cells destroyed, eliminating production of insulin
Inability of –cells to produce appropriate quantities of insulin, insulin resistance
Ketosis Common Rare Plasma insulin Low or absent Normal or high Acute complications
Ketoacidosis Hyperglycemia
Oral hypoglycemic drugs
Unresponsive Responsive
Treatment with insulin
Always necessary Usually not required

14
B-Fat soluble and water soluble vitamins (2.5 marks)
Five only each 0.5 mark
Fat soluble vitamins Water soluble vitamins
Solubility in fat Soluble Insoluble
Water solubility Insoluble Soluble
Absorption With lipids & requires bile salts Simple absorption
Carrier protein Present No carrier proteins
Storage Stored in liver No storage
Urinary excretion Not excreted Excreted
Deficiency Manifests only when stores are
depleted
Manifests rapidly as there is
no storage
Toxicity Hypervitaminosis may result Unlikely due to excretion
Treatment of
deficiency
Single large dose may prevent
deficiency
Regular dietary supply is
needed
Major vitamins A,D,E and K B complex and C
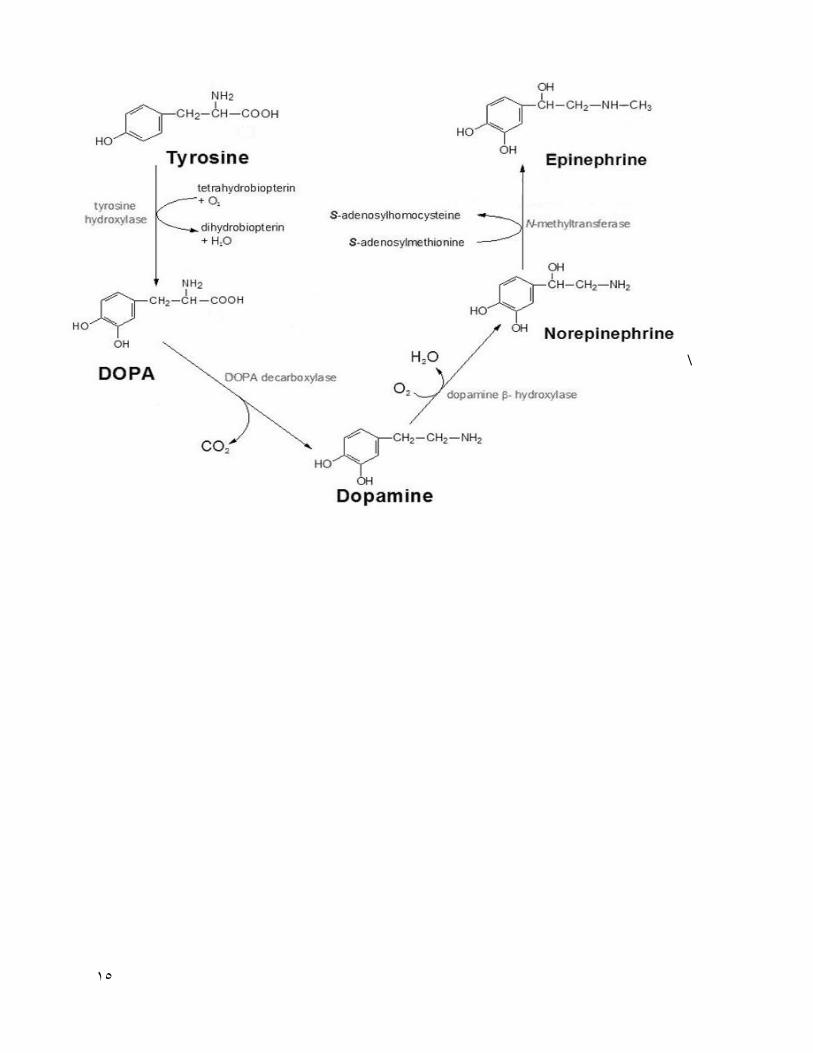
6-Illustrate all of the following reactions with chemical formulae:(6marks)
A-Tyrosine to catecholamines. (2marks)
15
\
16
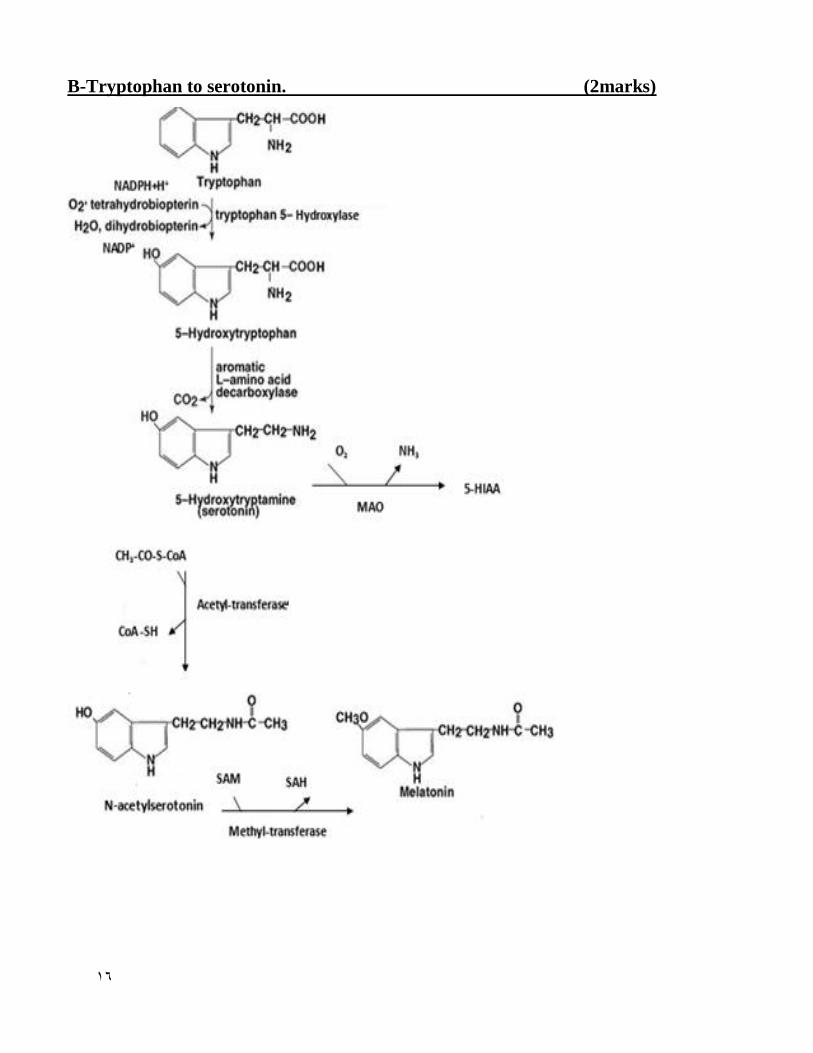
B-Tryptophan to serotonin. (2marks)

17
C-Pyruvate to lactate (1mark)
CH3 CH3
C=O lactate dehydrogenase H-C-OH
COOH NADH+H NAD COOH
D-Aspartic acid to oxaloacetic acid (1mark)
7-Explain how to detoxify: (3marks)
A-Aspirin (1mark)
Hydrolysis occurs to some drugs, e.g. Aspirin (acetylsalicylic acid)
Aspirin + water (H2O) by hydrolysis give salicylic acid + acetic acid
Detoxication by Hydrolysis
B-Benzoic acid (2marks)
Each onr mark
1-benzoic acid + UDP-Glucuronic UDP+Benzoyl-glucuronate
2-
18
8- Define and complete the following : (4marks each 0.5 mark)
1. Nitrogen balance 0.5mark
It is the quantitative difference between the amount of nitrogen intake and the amount of nitrogen
output (excreted).
2. Creatinuria 0.5 mark It is increase excretion of creatine in urine under normal physiological or pathological
states.
3. Albinism 0.5 mark
Albinism:
A genetic disease caused by deficiency of tyrosinase enzyme in melanocytes. No
melanin pigment formation, the skin &hair are whitish, the eye iris are colorless causing
photophobia.
4. Proteinuria. 0.5mark
Presence of detectable amount of protein in urine more than 300 mg/day
5. Glycosuria. 0.5 mark
Presence of detectable amounts of sugar in urine e.g.pentoses ,lactose or glucose in
urine
6. Plasma creatinine level is 0.5 mark
Creatinine: 0.5- 1.2 mg/dl.
7. Key enzyme in urea cycle is…0.5mark…
Carbamoyl phosphate synthetase I enzyme
8. Normal fasting glucose level in blood is … The normal fasting blood glucose level is 70
-110 mg/dl.
9. Case (3 marks)
An obese 51 years old woman was admitted to hospital in a semiconscious state. Her
blood glucose level was 368 mg/dl. Her urine was positive for both glucose and ketone bodies
A- What is the possible diagnosis? (1.5 marks)

19
Diabetic ketoacidosis
B- On biochemical basis explain the presence of ketone bodies in the patient’s urine
(1.5 marks)
Decreased insulin/ anti- insulin ratio leads to the deficient poor glucose utilization by
cells & poor ATP synthesis , activation of hormone sensitive lipase---- increasing free fatty acids
delivered to the liver----- increasing ketogenesis
10-MCQ (10marks)