Benefits of postoperative shed blood reinfusion in patients undergoing unilateral total knee...
5
ORIGINAL ARTICLE Manuel Mun˜oz Daniel Ariza Marı´a J. Garcera´n Aurelio Go´mez Arturo Campos Benefits of postoperative shed blood reinfusion in patients undergoing unilateral total knee replacement Received: 20 July 2004 / Published online: 9 April 2005 Ó Springer-Verlag 2005 Abstract Introduction In patients undergoing total knee replacement (TKR), most of the measured blood loss occurs during the postoperative period, and 30–50% of these patients receive allogeneic blood transfusion (ABT). For this reason, the salvage and return of un- washed filtered shed blood (USB) from postoperative drainage may represent an alternative to ABT in these patients. We have, therefore, evaluated the clinical util- ity of USB return in TKR patients, with a special focus on patients with mild anaemia. Materials and methods Data from 200 TKR patients (group 2) receiving USB within the first 6 postoperative hours (ConstaVac CBC II, Sryker) were prospectively collected. A retrospective series of 100 TRK patients served as the control group (group 1). Results USB return was possible in 162 pa- tients who received a mean of 0.98±0.4 U/pte, without any clinically relevant incident. Return of USB de- creased both the percentage of patients with ABT (48% vs 11%, for groups 1 and 2, respectively; p<0.01) and the ABT units/patient index (1.31±1.27 vs 0.29±0.87 units/patient, respectively; p<0.01). A transfusion pro- tocol was not established, but there was no difference between groups with respect to either perioperative Hb levels or overall transfusion index, indicating that the transfusion criteria were uniform. However, for the subgroups of patients who needed ABT, the pre- operative Hb level was 1 g/dL lower in those receiving USB (13.4±1.4 vs 12.4±1.2 g/dL; p<0.05). There was no difference in the postoperative complication rate, and patients in group 2 recovered the ability to walk 1 day earlier, and their hospital stay was 3 days shorter than in group 1 (p<0.01). Conclusions Return of USB after TKR seems to shorten the hospital stay and effectively reduce postoperative requirements for ABT, especially in patients with preoperative Hb >13 g/dL. For pa- tients with preoperative Hb <13 g/dL, although the return of USB also decreased the requirements for ABT, a further reduction will probably be obtained with the addition of another blood-saving method. Keywords Total knee replacement Allogeneic transfusion Anaemia Postoperative blood salvage Length of hospital stay Introduction Unilateral total knee replacement (TKR) can result in a substantial blood loss, and 30–50% of these patients receive allogeneic blood transfusion (ABT) [15, 18]. Since allogeneic blood is a scarce and increasingly expensive resource, and ABT is not a risk-free therapy, different methods to avoid ABT in these patients have been developed [1, 22]. Among them, preoperative autologous blood donation, perioperative blood salvage, and administration of drugs to either reduce blood loss (aprotinin, tranexamic acid) or stimulate erythrocyte production (iron, human recombinant erythropoietin) have been tried with different degrees of effectiveness [1, 22]. Preoperative autologous blood donation (PAD) is regarded in many countries as the standard care for major blood-losing operations, with the aim of mini- mising the exposure to ABT [20], and a very recent M. Mun˜oz (&) GIEMSA, School of Medicine, University of Ma´laga, Campus de Teatinos, s/n, 29071 Ma´laga, Spain E-mail: [email protected] Fax: +34-952-131534 D. Ariza A. Go´mez Department of Anaesthesiology, University Hospital ‘Virgen de la Victoria’, Ma´laga, Spain M. J. Garcera´n Department of Orthopaedic Surgery, University Hospital ‘Virgen de la Victoria’, Ma´laga, Spain A. Campos Department of Haematology, University Hospital ‘Virgen de la Victoria’, Ma´laga, Spain Arch Orthop Trauma Surg (2005) 125: 385–389 DOI 10.1007/s00402-005-0817-3
-
Upload
manuel-munoz -
Category
Documents
-
view
215 -
download
0
Transcript of Benefits of postoperative shed blood reinfusion in patients undergoing unilateral total knee...
ORIGINAL ARTICLE
Manuel Munoz Æ Daniel Ariza Æ Marıa J. Garceran
Aurelio Gomez Æ Arturo Campos
Benefits of postoperative shed blood reinfusion in patients undergoingunilateral total knee replacement
Received: 20 July 2004 / Published online: 9 April 2005� Springer-Verlag 2005
Abstract Introduction In patients undergoing total kneereplacement (TKR), most of the measured blood lossoccurs during the postoperative period, and 30–50% ofthese patients receive allogeneic blood transfusion(ABT). For this reason, the salvage and return of un-washed filtered shed blood (USB) from postoperativedrainage may represent an alternative to ABT in thesepatients. We have, therefore, evaluated the clinical util-ity of USB return in TKR patients, with a special focuson patients with mild anaemia. Materials and methodsData from 200 TKR patients (group 2) receiving USBwithin the first 6 postoperative hours (ConstaVac CBCII, Sryker) were prospectively collected. A retrospectiveseries of 100 TRK patients served as the control group(group 1). Results USB return was possible in 162 pa-tients who received a mean of 0.98±0.4 U/pte, withoutany clinically relevant incident. Return of USB de-creased both the percentage of patients with ABT (48%vs 11%, for groups 1 and 2, respectively; p<0.01) andthe ABT units/patient index (1.31±1.27 vs 0.29±0.87units/patient, respectively; p<0.01). A transfusion pro-tocol was not established, but there was no differencebetween groups with respect to either perioperative Hblevels or overall transfusion index, indicating that the
transfusion criteria were uniform. However, for thesubgroups of patients who needed ABT, the pre-operative Hb level was 1 g/dL lower in those receivingUSB (13.4±1.4 vs 12.4±1.2 g/dL; p<0.05). There wasno difference in the postoperative complication rate, andpatients in group 2 recovered the ability to walk 1 dayearlier, and their hospital stay was 3 days shorter than ingroup 1 (p<0.01). Conclusions Return of USB afterTKR seems to shorten the hospital stay and effectivelyreduce postoperative requirements for ABT, especiallyin patients with preoperative Hb >13 g/dL. For pa-tients with preoperative Hb <13 g/dL, although thereturn of USB also decreased the requirements for ABT,a further reduction will probably be obtained with theaddition of another blood-saving method.
Keywords Total knee replacement Æ Allogeneictransfusion Æ Anaemia Æ Postoperative blood salvage ÆLength of hospital stay
Introduction
Unilateral total knee replacement (TKR) can result in asubstantial blood loss, and 30–50% of these patientsreceive allogeneic blood transfusion (ABT) [15, 18].Since allogeneic blood is a scarce and increasinglyexpensive resource, and ABT is not a risk-free therapy,different methods to avoid ABT in these patients havebeen developed [1, 22]. Among them, preoperativeautologous blood donation, perioperative blood salvage,and administration of drugs to either reduce blood loss(aprotinin, tranexamic acid) or stimulate erythrocyteproduction (iron, human recombinant erythropoietin)have been tried with different degrees of effectiveness [1,22].
Preoperative autologous blood donation (PAD) isregarded in many countries as the standard care formajor blood-losing operations, with the aim of mini-mising the exposure to ABT [20], and a very recent
M. Munoz (&)GIEMSA, School of Medicine, University of Malaga,Campus de Teatinos, s/n, 29071 Malaga, SpainE-mail: [email protected]: +34-952-131534
D. Ariza Æ A. GomezDepartment of Anaesthesiology,University Hospital ‘Virgen de la Victoria’,Malaga, Spain
M. J. GarceranDepartment of Orthopaedic Surgery,University Hospital ‘Virgen de la Victoria’,Malaga, Spain
A. CamposDepartment of Haematology,University Hospital ‘Virgen de la Victoria’,Malaga, Spain
Arch Orthop Trauma Surg (2005) 125: 385–389DOI 10.1007/s00402-005-0817-3

meta-analysis of randomised controlled trials has foundthat for orthopaedic surgery, PAD reduced the proba-bility of receiving an ABT by 84% (RR 0.16, 95%CI0.07–0.36), although it increased the risk of exposure toany kind of transfusion, whereas perioperative cell sal-vage (CS) reduced this probability by 65% (RR 0.35,95%CI 0.24–0.52) [2].
In a previous meta-analysis, it was concluded thatCS decreased the frequency of exposure to allogeneicblood, without differences between devices producingeither washed (RR 0.39, 95%CI 0.30–0.51) or un-washed cells (RR 0.35, 95%CI 0.26–0.46), when com-pared with a control [8]. However, though there may besubstantial hidden blood loss due to bleeding into thetissues and residual blood in the joint following TKA,50% of the true total loss occurs during the postop-erative period [19], and consequently, salvage and re-turn of unwashed filtered shed blood (USB) frompostoperative drainage may represent an alternative toABT in these patients.
In our hospital this blood-saving technique has beenused since May 2002, and we have, therefore, evaluatedthe utility of USB return to reduce exposure to ABT inTRK patients, with a special focus on patients with mildanaemia. As secondary end-points, we analysed theimpact of USB return on both the rate of postoperativecomplications and the length of hospital stay.
Patients and methods
Data from 200 primary TRK patients operated onbetween May 2002 and December 2003 and receivingUSB were prospectively collected (group 2). A retro-spective series of 100 TRK patients operated on by thesame surgical team between January 2000 and Febru-ary 2001 and not receiving USB served as the controlgroup (group 1). All surgical procedures involved theapplication of a tourniquet that was deflated beforeknee closure, using a total condylar knee (Duracon,Stryker, USA), with the tibial component being ce-mented.
The anaesthesiologist, who was unaware of the study,estimated blood losses in both the operation theatre andthe anaesthesia recovery unit, and performed the rein-fusion of USB. In the ward, measurement of postoper-ative blood loss and decisions on postoperativetransfusions were made by the attending surgeon. Forcalculation of requirements for ABT, one unit of packedred cells was considered as one blood unit.
Postoperative blood salvage and reinfusion
At the end of surgery, the collection blood canister(ConstaVac CBC II, Stryker, USA) was connected totwo drainage catheters through a Y-connector, and USBwas collected without anticoagulant at a negative
pressure of 25 mmHg and reinfused within the first 6postoperative hours. The canister is connected to thereinfusion bag to which USB is transferred, scrappingthe last 60–80 mL to minimize fat particles and otherdebris being transfused to the patient, and allowing forseveral returns if needed. A 40-lm screen filter(SQ40SJKL, Pall, UK) was intercalated in the patient’sline to eliminate microaggregates. The volume ofrecovered USB was converted into blood units accord-ing to the expression: U=USB volume (ml)xUSB hae-matocrit (%)/400 (ml) [16]. Patients in group 1 receiveda standard drainage, without reinfusion of USB.
Clinical data
A set of demographic and clinical data was collected forall patients, including age, gender, height, weight,co-morbidities, preoperative treatments, type of anaes-thesia, tourniquet and operation time, intra- and post-operative blood loss, volume of USB returned, numberof ABT, perioperative Hb levels, deep venous throm-bosis, pulmonary embolism, infection and length ofhospital stay (LOS).
Statistical analysis
Statistical analysis of the results was performed usingStudent’s t-test, the chi-square test, and Fischer’s exacttest. Linear regression analysis was also performed(SPSS 12.0 package, licensed to the University ofMalaga).
Results
There were no differences in age, height, weight, co-morbidities or preoperative treatments between groups,although there were more women in group 2 (67% vs80%, for group 1 and 2, respectively; p<0.01) (Tables 1and 2). Similarly, perioperative Hb levels and blood losswere not different in either group (Table 1). In group 2,USB return was possible in 162 patients who received amean of 0.98±0.4 units per patient, without any clini-cally relevant incident. With respect to the controlgroup, the percentage of patients with ABT (RR 0.23;p<0.01) and packed red cell/patient index were lower inthe USB group (1.31±1.27 vs 0.29±0.87 units/patient,respectively; p<0.01) (Table 1). The differences intransfusion requirements persisted even after the pa-tient’s stratification according to a preoperative Hb>13 g/dL (RR 0.08) or <13 g/dL (RR 0.39) (Table 2).
Preoperative Hb levels were compared after eachgroup of patients was further subdivided into two sub-groups, according to the need for ABT. There was nodifference in preoperative Hb level between the sub-groups of patients that needed no supplementary ABT
386
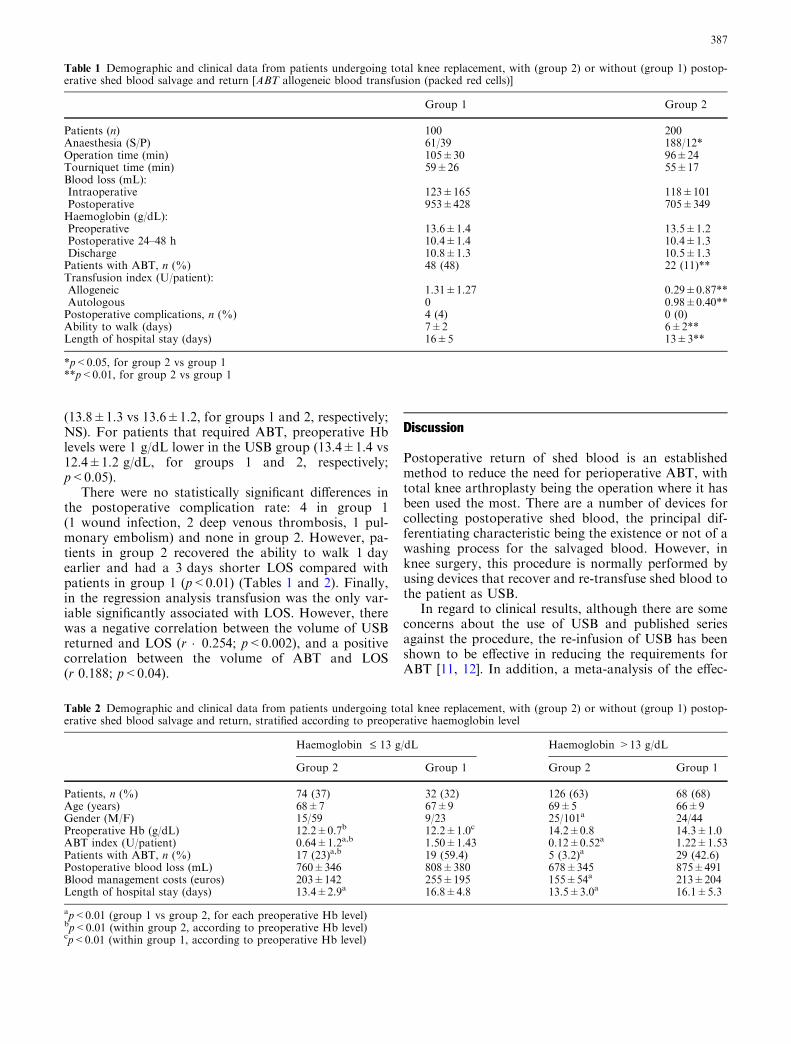
(13.8±1.3 vs 13.6±1.2, for groups 1 and 2, respectively;NS). For patients that required ABT, preoperative Hblevels were 1 g/dL lower in the USB group (13.4±1.4 vs12.4±1.2 g/dL, for groups 1 and 2, respectively;p<0.05).
There were no statistically significant differences inthe postoperative complication rate: 4 in group 1(1 wound infection, 2 deep venous thrombosis, 1 pul-monary embolism) and none in group 2. However, pa-tients in group 2 recovered the ability to walk 1 dayearlier and had a 3 days shorter LOS compared withpatients in group 1 (p<0.01) (Tables 1 and 2). Finally,in the regression analysis transfusion was the only var-iable significantly associated with LOS. However, therewas a negative correlation between the volume of USBreturned and LOS (r �0.254; p<0.002), and a positivecorrelation between the volume of ABT and LOS(r 0.188; p<0.04).
Discussion
Postoperative return of shed blood is an establishedmethod to reduce the need for perioperative ABT, withtotal knee arthroplasty being the operation where it hasbeen used the most. There are a number of devices forcollecting postoperative shed blood, the principal dif-ferentiating characteristic being the existence or not of awashing process for the salvaged blood. However, inknee surgery, this procedure is normally performed byusing devices that recover and re-transfuse shed blood tothe patient as USB.
In regard to clinical results, although there are someconcerns about the use of USB and published seriesagainst the procedure, the re-infusion of USB has beenshown to be effective in reducing the requirements forABT [11, 12]. In addition, a meta-analysis of the effec-
Table 2 Demographic and clinical data from patients undergoing total knee replacement, with (group 2) or without (group 1) postop-erative shed blood salvage and return, stratified according to preoperative haemoglobin level
Haemoglobin £ 13 g/dL Haemoglobin >13 g/dL
Group 2 Group 1 Group 2 Group 1
Patients, n (%) 74 (37) 32 (32) 126 (63) 68 (68)Age (years) 68±7 67±9 69±5 66±9Gender (M/F) 15/59 9/23 25/101a 24/44Preoperative Hb (g/dL) 12.2±0.7b 12.2±1.0c 14.2±0.8 14.3±1.0ABT index (U/patient) 0.64±1.2a,b 1.50±1.43 0.12±0.52a 1.22±1.53Patients with ABT, n (%) 17 (23)a,b 19 (59.4) 5 (3.2)a 29 (42.6)Postoperative blood loss (mL) 760±346 808±380 678±345 875±491Blood management costs (euros) 203±142 255±195 155±54a 213±204Length of hospital stay (days) 13.4±2.9a 16.8±4.8 13.5±3.0a 16.1±5.3
ap<0.01 (group 1 vs group 2, for each preoperative Hb level)bp<0.01 (within group 2, according to preoperative Hb level)cp<0.01 (within group 1, according to preoperative Hb level)
Table 1 Demographic and clinical data from patients undergoing total knee replacement, with (group 2) or without (group 1) postop-erative shed blood salvage and return [ABT allogeneic blood transfusion (packed red cells)]
Group 1 Group 2
Patients (n) 100 200Anaesthesia (S/P) 61/39 188/12*Operation time (min) 105±30 96±24Tourniquet time (min) 59±26 55±17Blood loss (mL):Intraoperative 123±165 118±101Postoperative 953±428 705±349Haemoglobin (g/dL):Preoperative 13.6±1.4 13.5±1.2Postoperative 24–48 h 10.4±1.4 10.4±1.3Discharge 10.8±1.3 10.5±1.3Patients with ABT, n (%) 48 (48) 22 (11)**Transfusion index (U/patient):Allogeneic 1.31±1.27 0.29±0.87**Autologous 0 0.98±0.40**Postoperative complications, n (%) 4 (4) 0 (0)Ability to walk (days) 7±2 6±2**Length of hospital stay (days) 16±5 13±3**
*p<0.05, for group 2 vs group 1**p<0.01, for group 2 vs group 1
387

tiveness of cell salvage in minimising perioperativeallogeneic transfusion concluded that, in orthopaedicsurgery, devices producing either washed or unwashedcells decreased the frequency of exposure to allogeneicblood to a similar degree compared with a control (RR0.30 and 0.35, respectively) [8]. However, the results ofthis meta-analysis have been criticized because of thesmall number of patients included in the studies.
In our study, we found that USB return decreased by77% the relative risk of receiving ABT (48% vs 11%,p<0.01; absolute risk reduction 37%) and reduced theABT index by 1 unit in patients undergoing TKR (Ta-ble 1). A transfusion protocol was not established, butthere was no difference between the groups in respect ofeither perioperative Hb levels or overall transfusion in-dex, indicating that the transfusion criteria were uniform(Table 1). Moreover, our data are in concordance withthose of 7 studies published over the last 5 years andincluding almost 2000 patients, showing a 68% decreasein the relative risk of receiving ABT (60% vs 19%,p<0.01; absolute risk reduction 41%) (Table 3) [4, 4, 6,7, 14, 16, 21, 23], and with those of the above-mentionedmeta-analysis [8]. These results seem to confirm theeffectiveness of USB return to reduce the need for ABTin TKR patients.
Very recently, in a series of 365 patients who under-went surgery for TKR, Steinberg et al. [23] reported thatpostoperative salvage and reinfusion of USB decreasedby 65% the requirements for ABT, and also reduced thepacked red cell/patient index, with respect to a controlgroup. In addition, they reported that a cut-off point ofthe preoperative Hb level for receiving blood transfusionwas found to be 13.25 g/dL for both of them. In ourseries, for the subgroups of patients who needed ABT,the preoperative Hb was 1 g/dL lower in the USB groupwith respect to the control group (12.4±1.2 vs13.4±1.4 g/dL; p<0.05), whereas there were no differ-ences between preoperative Hb levels for patients whorequired ABT. Keeping in mind that the transfusion ofone blood unit should increase the patient’s Hb level by1 g/dL, the amount of USB returned (0.98 unit per pa-tient) would account for this difference. Once again,these results supported the clinical utility of USB return.
According to Steinberg et al. [23], the preoperativeHb level is a major predictor for the risk of transfusion
in TKR, and patients with preoperative Hb level>13.25 g/dL may need no blood transfusion. However,in our control series, at least one ABT was needed for42% of the patients with preoperative Hb >13 g/dL,whereas this was true for only 3% of the patientsreceiving USB. For this reason, as the postoperativeblood loss is unpredictable, we believe that the collectorsystem should be of use in both anaemic and non-anaemic TKR patients to provide a wider safety margin.
Return of USB presents very few adverse effects,mostly chills, febricula, tachycardia, and hypotension,which can be prevented by limiting the volume to return(max. 1000–1500 mL), using a slow infusion rate anddiscarding the last 50–100 mL of USB, as the ConstaVacCBC II does [11]. We did not observe any adverse effectof USB return during the study, but there was a trend toa lower rate of postoperative complications in patientsreceiving USB, as previously reported [13], and to afaster recovery, as suggested by the earlier ability towalk and the shorter LOS (Table 1) [15]. These effectsare possibly related to the decreased exposure to ABTand to the recently described immunostimulatory effectof USB [6]. In fact, blood transfusion was the onlyvariable significantly associated with LOS, but there wasa negative correlation between the volume of USB re-turned and LOS, and a positive correlation between thevolume of ABT and LOS. However, it must be pointedout that though postoperative USB reinfusion seems tobe beneficial, the number of patients was too small todetermine a significant benefit over ABT with enoughstatistical power. Thus, these results need to be con-firmed by a large randomised trial.
In our community, the cost of one collection-reinfu-sion unit is about 135 euros, and the price of packed redcells plus the drainage catheters is about 180 euros.Based on these prices, for patients with preoperative Hb>13 g/dL, mean transfusion costs were 213 and 155euros/patient for group 1 and 2, respectively (p<0.01),whereas for patients with preoperative Hb <13 g/dL,mean transfusion costs were 255 and 203 euros/patient,respectively (NS). In addition, although the return ofUSB effectively reduces the requirements for ABT inanaemic patients from group 2 (Table 2), it becameevident that some additional blood-saving methodshould be employed, since 23% of them still needed
Table 3 Results of some studies on the effectiveness of unwashed shed blood return (+USB) to decrease the requirements for allogeneicblood transfusion (+ABT) in total knee replacement
Study Year +USB +ABT/total(%)
Control +ABT/total(%)
Relative risk
Henderson et al. [7] 1999 35/159 22 134/180 74 0.30Dıaz and Moral [4] 1999 13/91 14 25/57 44 0.33Peter et al. [14] 2001 30/160 19 67/93 72 0.26Sinha et al. [21] 2001 8/50 22 44/50 88 0.25Fernandez et al. [5] 2002 26/81 32 56/82 68 0.47Sanz et al. [16] 2004 43/250 17 112/250 45 0.38Steinberg et al. [23] 2004 36/194 19 89/171 52 0.36All studies 191/985 19 527/883 60 0.32
388

ABT. In this regard, the administration of erythropoie-tin (40,000 IU) plus intravenous iron (400 mg) has beenshown to decrease the requirements for ABT in TKRand to be more cost-effective than other recently re-ported blood-saving protocols [3, 9, 10]. Therefore, webelieve that a reasonable increase in blood managementcosts (+300 euros/patient) produced by supplementingUSB with EPO plus intravenous iron in anaemic pa-tients would probably be offset by the reduction in boththe requirements for ABT and the length of hospitalstay. However, a cost-benefit analysis of these inter-ventions is difficult to make because of the complex costsinvolved in blood transfusion. Thus, a formal cost-benefit study is also required to address this issue.
Acknowledgements This study was financially supported by grantFIS PI 02/1826 from Instituto de Salud Carlos III (Spain) and theEuropean Union, it was approved by the Ethics Committee of theUniversity Hospital ‘Virgen de la Victoria’ (Malaga, Spain), and itcomplied with current Spanish laws.
References
1. Amin M, Fergusson D, Aziz A, Wilson K, Coyle D, Hebert P(2003) The cost of allogeneic red blood cells—a systematic re-view. Transf Med 13:275–285
2. Carless P, Moxey A, O’Connell D, Henry D (2004) Autologoustransfusion techniques: a systematic review of their efficacy.Transf Med 14:123–144
3. Cuenca J, Martınez F, Garcıa-Erce JA, Benedi JA, Larrode M,Perez-Serrano L (2004) Transfusion in total knee replacement.Presurgical administration of EPO and parenteral iron (ab-stract). TATM 6 (Suppl 1):89
4. Diaz-Espallardo C, Moral-Garcıa V (1999) Analisis de la rel-acion coste-efectividad de un programa de autotransfusion encirugıa protesica primaria de rodilla y cadera. Rev Esp Ane-stesiol Reanim 46:396–403
5. Fernandez CM, Rubio F, Crespo J, Acedo A (2002) Auto-transfusion postoperatoria en cirugıa de rodilla. In: Munoz M(ed) Anemia y transfusion en cirugıa. SPICUM, Malaga,pp 432–436
6. Gharehbahian A, Haque G, Truman C, Evans R, Morse H,Newman J et al (2004) Effect of autologous salvaged blood onpost-operative natural killer cell precursor frequency. Lancet363:1025–1030
7. Henderson MS, Newman JH, Hand GCR (1999) Blood lossfollowing knee replacement surgery, use it don’t lose it. Knee6:125–129
8. Huet C, Salmi LR, Fergusson D, Koopman-van Gements AW,Rubens F, Laupacis A (1999) A meta-analysis of the effec-tiveness of cell salvage to minimize perioperative allogeneicblood transfusion in cardiac and orthopaedic surgery. Inter-national Study of Perioperative Transfusion (ISPOT) Investi-gators. Anesth Analg 89:861–869
9. Kourtzis N, Pafilas D, Kasimatis G (2004) Blood saving pro-tocol in elective total knee arthroplasty. Am J Surg 187:261–267
10. Minoda Y, Sakawa A, Fukuoka S, Tada K, Takaoka K (2004)Blood management for patients with hemoglobin level lowerthan 130 g/l in total knee arthroplasty. Arch Orthop TraumaSurg 124:317–319
11. Munoz M, Garcıa-Vallejo JJ, Lopez-Andrade A, Gomez A,Ruiz MD, Maldonado J (2001) Autotransfusion postoperatoriaen cirugıa ortopedica. Un analisis de la calidad, seguridad yeficacia de la sangre recuperada de los drenajes postoperatori-os. Rev Esp Anestesiol Reanim 48:131–140
12. Munoz M, Garcıa-Vallejo JJ, Ruiz MD, Romero R, Olalla E,Sebastian C (2004) Transfusion of post-operative shed blood:Laboratory characteristics and clinical utility. Eur Spine J 13(Suppl 1):S107–S113
13. Newman JH, Bowers M, Murphy J (1997) The clinicaladvantage of autologous transfusion. A randomised, controlledstudy after knee replacement. J Bone Joint Surg Br 79:630–632
14. Peter VK, Radford M, Matthews MG (2001) Re-transfusion ofautologous blood from wound drains: the means for reducingtransfusion requirements in total knee arthroplasty. Knee8:321–323
15. Rosencher N, Kerkkamp HE, Macheras G, Munuera LM,Menichella G, Barton DM et al (2003) Orthopedic SurgeryTransfusion Hemoglobin European Overview (OSTHEO)study: blood management in elective knee and hip arthroplastyin Europe. Transfusion 43:459–469
16. Sanz Penuelas RA, Torcal Abian F, Rodriguez A, Castro M,Perez-Cerda F (2004) Postoperative autologous blood trans-fusion after unilateral total knee arthroplasty (abstract). 13th
World Congress of Anaesthesiologists, www.wca2004.com:S004
17. Sebastian C, Romero R, Olalla E, Ferrer C, Garcıa-Vallejo JJ,Munoz M (2000) Postoperative blood salvage and reinfusion inspinal surgery. Blood quality, effectiveness and impact on pa-tient blood parameters. Eur Spine J 9:458–465
18. Sehat KR, Evans R, Newman JH (2000) How much blood isreally lost in total knee arthroplasty? Correct blood loss man-agement should take hidden loss into account. Knee 7:151–155
19. Sehat KR, Evans RL, Newman JH (2004) Hidden blood lossfollowing hip and knee arthroplasty. Correct management ofblood loss should take hidden loss into account. J Bone JointSurg Br 86:561–565
20. Scottish Intercollegiate Guidelines Network (2004) Periopera-tive blood transfusion for elective surgery. A national clinicalguideline. www.sign.ac.uk
21. Sinha A, Sinha M, Burgert S (2001) Reinfusion of drainedblood as an alternative to homologous blood transfusion aftertotal knee replacement. Inter Orthop 25:257–259
22. Spahn DR, Casutt M (2000) Eliminating blood transfusions.Anesthesiology 93:242–255
23. Steinberg EL, Ben-Galim P, Yaniv Y, Dekel S, Menahem A(2004) Comparative analysis of the benefits of autotransfusionof blood by a shed blood collector after total knee replacement.Arch Orthop Trauma Surg 124:114–118
389