
Presentation by Neil Kirkbride, Chairman of NOF Energy MD, Bel Valves

Benefits of a pathway: The experience
of utilizing a NOF pathway
Megan Yeomans – Clinical Nurse Consultant
Pain Team, Austin Health

Our health service
# NOF Presentations
2010-2011: 262
2011-2012: 246

Management of a # NOF Patient
2009- surgery-focused approach
Patient fits in with:
– a rigid system
–not a patient focused approach
– resulting in a poorer outcome for patient

Management of a # NOF Patient
2009- surgery-focused approach
Patient arrives in ED:
• XRs show #NOF…Patient fasted, given
some morphine
• Page Ortho Reg 11am….No Answer…
• Page Ortho Reg 1:30pm…Nurse from
theatre answers
• That registrar isnt on call, not sure who is
• Ring switch…right reg now paged …reg
rings ED…

Management of a # NOF Patient
2009- surgery-focused approach
ED
• ‘Got a NOF for you’
• Ortho Reg
• ‘What’s the UR?’….looks up XR on
computer…
• OK, Keep her fasted

Management of a # NOF Patient
2009- surgery-focused approach
– 8pm…
–….10pm…
–…Midnight…
–…..2am…

Management of a # NOF Patient
2009- surgery-focused approach
Theatre Nurse
• ‘Are you going to get to that NOF tonight?’
• Ortho Reg (scrubbed)
• ‘Hmmm, probably not, it’s getting a bit late’
• ‘Let’s put her on for tomorrow night’
• Theatre Nurse
• ‘Make sure you ring the ward to let them
know’
• Ortho Reg (scrubbed)
• ‘OK’

Management of a # NOF Patient
2009- surgery-focused approach
1 hour later…..Ward Nurse rings Ortho
Reg……
» Are you doing that NOF tonight??....
Ortho Reg
»Oh sorry….. No, feed her and fast her
from early breakfast!

Management of a # NOF Patient
2009- surgery-focused approach
Overnight…
• Ward nurse feeds patient & calls the resident
• Overnight Resident Looks at ED notes to
write admission
• 2.5mg morphine SC 4 hourly written up

Management of a # NOF Patient
2009- surgery-focused approach
Next Day…
• Patient
• Delirious…so morphine ceased
• Fasted all day
• Operation ‘bumped’ again next
night

Management of a # NOF Patient
2009- surgery-focused approach
3rd Day…
• Patient
• Delirium worsens
• Operation goes ahead that night

Management of a # NOF Patient
2009- surgery-focused approach
4th Day…
• Patient
• Severe Delirium with aggression
• Patient shackled

Management of a # NOF Patient
2009- surgery-focused approach
5th Day…
• Patient
• Patient remains delirious
• Patient noted to be hypoxic
• Bloods checked- patient anaemic
• CXR- Pneumonia

Management of a # NOF Patient
2009- surgery-focused approach
2 weeks later…
• Patient
• Delirium seems to have settled
• Family still say she is ‘not quite right’
• Now medically stable enough for
transfer to rehab

Objectives of this presentation
• To tell our story of why this project was initiated
• The diagnostic process
• What we learned
• The value of an organizational collaborative effort
• Designing and implementing a pain management plan
• Results and Ongoing Improvements

Information we were given
• Health Round Table Information
• DRG 108- Neck of Femur Fracture
• Austin Health had an average LOS >14 days
• The four exemplar hospitals average LOS around 8 days
• Aim – Reduce Length of Stay to that of exemplar hospitals

Background
Visit to another facility and a literature search revealed we needed:
1. Full time Head Of Orthopaedic Unit – implemented Sept 2009
2. More theatre sessions and better access for trauma –
implemented over 2009
3. Institute ortho-geriatric service – commenced February 2010

Orthogeriatric Service
– New full-time Orthogeriatric registrar
– Over seen by a senior geriatrician
• Involved in every patient >65yo with low-impact trauma #
• Cross-campus consultant-led 2x/week ward rounds
• Ortho in Rehab hospital
• Geriatric in Acute hospital

Move toward a patient centred approach
The patients needs have redesigned the
management of this injury and led to the
implementation of a clinical pathway by:
• Considering the patient experience
• Improving communication
• Improving system issues
• Tailoring pain management to the patients
individual needs

Top down commitment
• Attendance List List
• Executive- CEO, CMO, Executive Directors
• CSU/ Medical Directors
• Senior Clinical Staff- ED, Anaesthetists , Orthopedics
Geriatricians
• Austin By Design
• Physiotherapy
• Access, Care & Patient Flow coordinators
• Ward NUM
• Liaison nurses
• Theatre staff…and more

Review process- How are we managing these patients?
• File audit- 30 patient files
• Interview with patients and their families
• Walk Through
– Follow the patient journey from the front door to discharge.
– Chance for two way communication and to understand work
flows
» What works
» What doesn’t

Where we focused
– Time to theatre
– Fasting
– Pain management
– Delirium

Pain with # NOF Before and After Surgery
Pre operative: 44% pre op
Post operative: 42% severe pain (cog intact)
Morrison et al 2000 J Pain Sympt Mgt

How much pain?- identified in the patient files
“The pain scores were overall poorly documented”.
“Often comments were made by the physios and nurses in
the clinical notes about the patient experiencing ‘severe
pain, anxiety, confusion and being tearful’; this was often
not evident when compared with the pain scores ‘if they
were documented’.”

We focused on three main areas
• Three main areas
– ED
– Pre operatively
– Post operatively

The Three Main Areas- ED
Before
• No Standard Pain-relief
• Mostly narcotic-based
• Minimal use of blocks (<10%)
• No review of analgesia efficacy
• Multiple trips to Radiology (Hip & Chest)
• Gap from ED until drug chart written up (on ward)

The Three Main Areas- Pre op on the ward
• Admitted to the ward at various times of the
day.
• Orthopaedic staff in theatre so charts not
done
• Variable pain relief/not standard
• Fasted for varying lengths of time
• Analgesia usually ceased if patient became
confused
• Usually inadequate doses
• Intermittent/ infrequent doses

Patients arrived at various times
Often an adhoc approach to pain management
The Three Main Areas- Theatre

Pre
implementation
Pre
implementation
The next day

Three main areas: Post operative
Before
• No Standard Pain-relief
• PRN-Basis
• Usually no maintenance medications
• No formal review of analgesia efficacy
• Opioids ceased if patient became confused
• Patients not able to participate in physio due to pain.

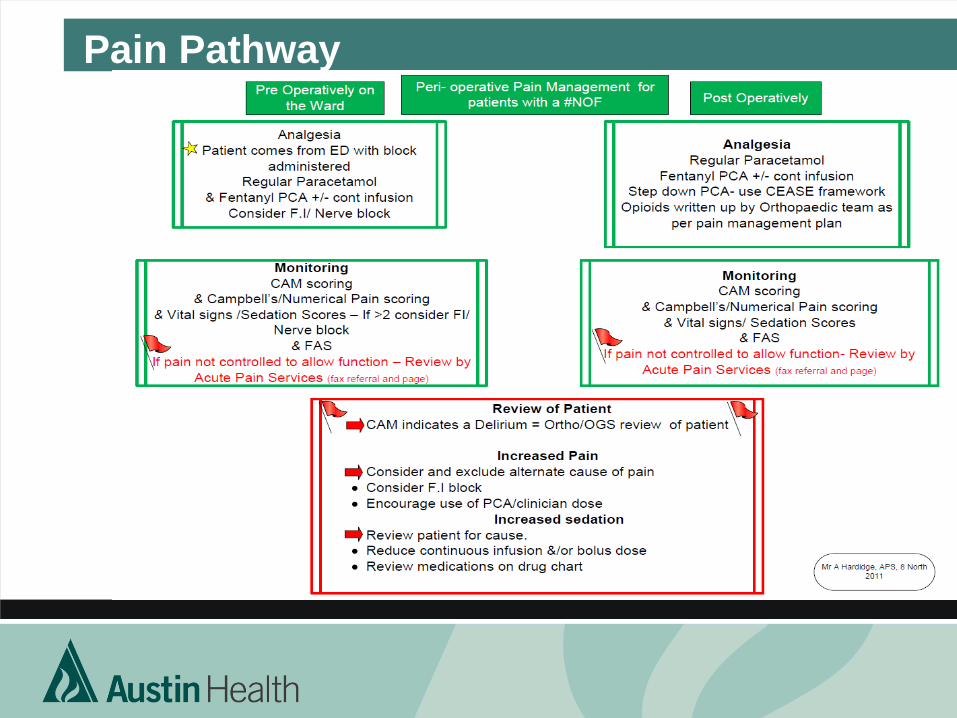
Implementation of clinical pathway

Developed an integrated Clinical Pathway

ED Now
• Regular Paracetamol 1g TDS in elderly (Oral)
• Incremental boluses of Fentanyl to effect (or
Morphine)
• Regular pain scores on function
• Fascia Iliaca Blocks – done in >80% of patients
• Single xrays Chest and Hip – ordered as a package.

Post
implementation
Post
implementation

The Ward Now
• Care Pathway
• Pain Plan
• Hunger clocks
– High protein Supplements
• Delirium screening – Cognitive Assessment Method
• Orthogeriatricians now educated and adopting similar
analgesic prescribing for other patient groups

0-6 hours
Appropriate length of
fasting time
6-9 hours Confirm
theatre time with
theatre staff and ortho
reg
12 hours Definitive
plan required, call
ortho reg feed patient
if surgery is not
imminent

CONFUSION ASSESSMENT METHOD (CAM) adapted from Inouye SK, et al. Ann Intern med. 1990;113:941-8
A -
B -
C -
D -
Delirium = A+B (2points) A+B+C (3points) A+B+D (3points) A+B+C+D (4 points) Salliece Byford. CNS. Austin Health.
A ACUTE ONSET AND FLUCTUATING COURSE
Is there an acute change in mental status from the patient’s baseline? Does the persons behaviour fluctuate during the day (come and go) or increase and decrease in severity?
B
C D
Delirium
INATTENTION Does the patient have difficulty focusing their attention, for example, being easily distracted or having difficulty keeping track of what is being said?
DISORGANISED THINKING Is the patient’s thinking disorganised or incoherent, such as rambling or irrelevant conversation, unclear or illogical flow of ideas, or unpredictable switching from one subject to another?
ALTERED LEVEL OF CONSCIOUSNESS Overall, how would you rate the patient’s level of consciousness?
-- Vigilant (hyperalert) -- Lethargic (drowsy, easily aroused) -- Stupor (difficult to arouse) -- Coma (unarousable)

Delirium
Delirium
Pain Pathway

Post Operative Now
• Patient controlled analgesia:
– If patient cognitively intact, PCA mode +/- continuous infusion
– If patient cognitively impaired, a continuous infusion @5mcg/hr
– Both have clinician boluses to be given prior to movement.
• Nurses are already familiar with PCA
– Monitor regularly
– Pain at Rest
– Pain on Activity
– Sedation Score
– CAM (Delirium) Score

Pain Care Plan
• Guidance is given to PCA orders
• Step down analgesia
• Monitoring guidance
• Reassessment prompts

May 2009-March 2012
0
2
4
6
8
10
12
14
Ma
y-0
9
Jun-0
9
Jul-0
9
Aug-0
9
Sep-0
9
Oct-
09
No
v-0
9
De
c-0
9
Jan-1
0
Feb
-10
Ma
r-1
0
Apr-
10
Ma
y-1
0
Jun-1
0
Jul-1
0
Aug-1
0
Sep-1
0
Oct-
10
No
v-1
0
De
c-1
0
Jan-1
1
Feb
-11
Ma
r-1
1
Apr-
11
Ma
y-1
1
Jun-1
1
Jul-1
1
Aug-1
1
Sep-1
1
Oct-
11
No
v-1
1
De
c-1
1
Jan-1
2
Feb
-12
Ma
r-1
2
Days
Average Length of Stay (HRT Data)
Exemplars
A H
Project starts
Pain Plan
Starts

Top down commitment
• Attendance List List
• Executive- CEO, CMO, Executive Directors
• CSU/ Medical Directors
• Senior Clinical Staff- ED, Anaesthetists , Orthopedics
Geriatricians
• Austin By Design
• Physiotherapy
• Access, Care & Patient Flow coordinators
• Ward NUM
• Liaison nurses
• Theatre staff…and more
• Pain services asked to optimise analgesia… 18months later

Pain DOES matter!
Post-operative pain is associated with:
increased hospital length of stay; delayed ambulation and
long-term functional impairment
(Morrison 2003)

Acknowledgements to:
• Fiona Nielsen: Quality Coordinator Surgical Clinical
Services Unit
• Andrew Hardidge: Director of Orthopaedic Surgery
• Jane Trinca: Director of Acute Pain Service
• Ward 8N: Pain Champions


















![NOF Clinicians Guide[1]](https://static.fdocuments.us/doc/165x107/577d2a461a28ab4e1ea8d8a8/nof-clinicians-guide1.jpg)
