
Bendtsen - TTH pathophysiologydrustvoneurologasrbije.org/arhiva/predavanja/glavobolje_2012... · 3...
17
1 Danish Headache Center Tension-type headache Pathophysiology Lars Bendtsen Associate professor, MD, PhD, Dr Med Sci Danish Headache Center, Department of Neurology Glostrup Hospital, University of Copenhagen, Denmark European Headache School, Belgrade, May, 2012 Pathophysiology of Tension-Type Headache • Peripheral mechanisms M l f t − Muscular factors • Central mechanisms − Altered central nociception Bendtsen and Fernández-de-las-Peñas, Cur. Pain Head. Rep. 2011
-
Upload
trinhkhanh -
Category
Documents
-
view
213 -
download
0
Transcript of Bendtsen - TTH pathophysiologydrustvoneurologasrbije.org/arhiva/predavanja/glavobolje_2012... · 3...
1
Danish Headache Center
Tension-type headachePathophysiology
Lars BendtsenAssociate professor, MD, PhD, Dr Med Sci
Danish Headache Center, Department of NeurologyGlostrup Hospital, University of Copenhagen, Denmark
European Headache School, Belgrade, May, 2012
Pathophysiology of Tension-Type Headache
• Peripheral mechanisms
M l f t− Muscular factors
• Central mechanisms
− Altered central nociception
Bendtsen and Fernández-de-las-Peñas, Cur. Pain Head. Rep. 2011
2
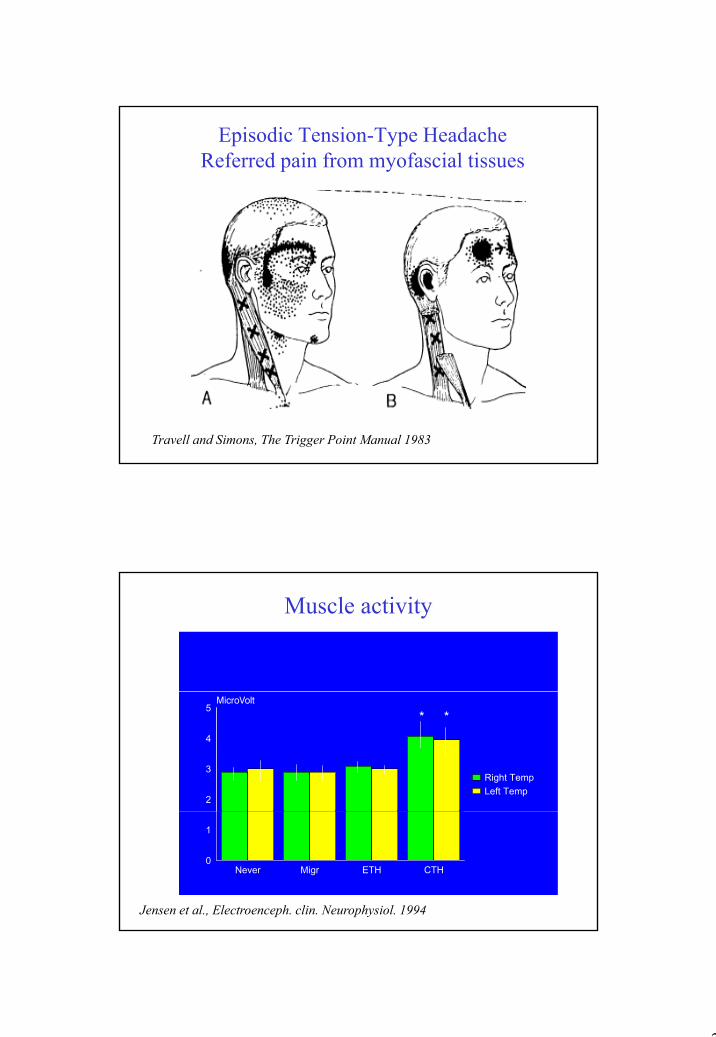
Episodic Tension-Type HeadacheReferred pain from myofascial tissues
Travell and Simons, The Trigger Point Manual 1983
Muscle activity
2
3
4
5
Right Temp Left Temp
* *
Jensen et al., Electroenceph. clin. Neurophysiol. 1994
Never Migr ETH CTH0
1
3
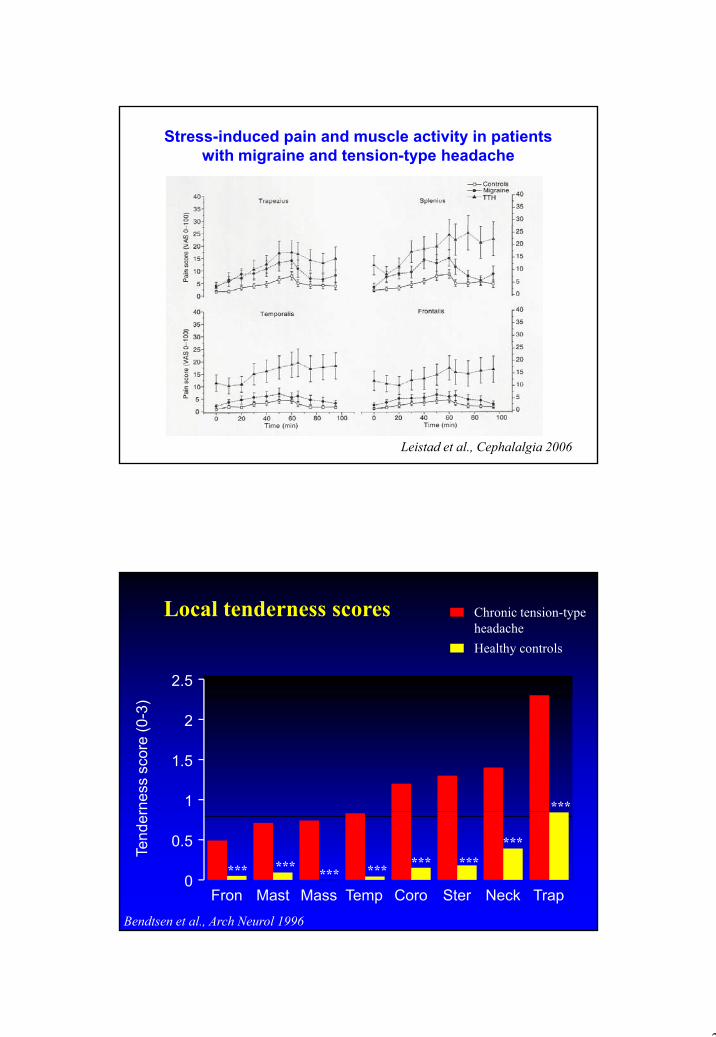
Stress-induced pain and muscle activity in patients with migraine and tension-type headache
Leistad et al., Cephalalgia 2006
2.5
Chronic tension-type headacheHealthy controls
Local tenderness scores
1
1.5
2
rnes
s sc
ore
(0-3
)
***
Fron Mast Mass Temp Coro Ster Neck Trap0
0.5
Tend
er
*** ***
***************
Bendtsen et al., Arch Neurol 1996
4
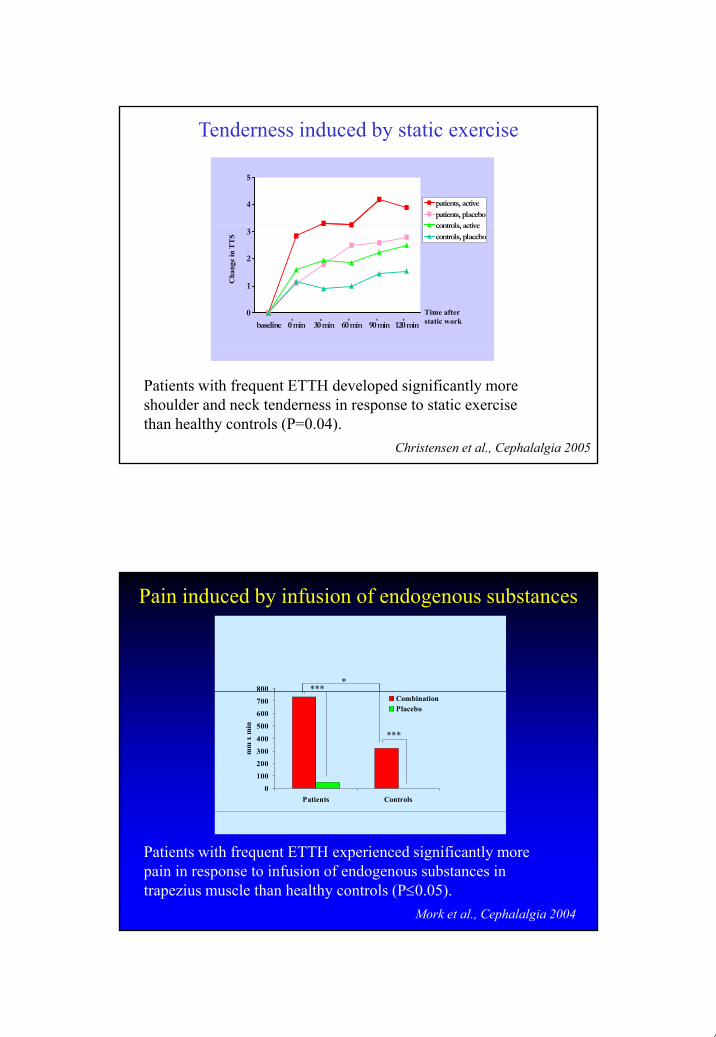
Tenderness induced by static exercise
4
5
patients, activepatients, placebocontrols active
0
1
2
3
baseline 0 min 30 min 60 min 90 min 120 min
controls, activecontrols, placebo
Cha
nge
in T
TS
Time afterstatic work
Christensen et al., Cephalalgia 2005
Patients with frequent ETTH developed significantly more shoulder and neck tenderness in response to static exercise than healthy controls (P=0.04).
Pain induced by infusion of endogenous substances
800 ****
0
100
200300
400
500
600700
Patients Controls
mm
x m
in
CombinationPlacebo
***
Mork et al., Cephalalgia 2004
Patients with frequent ETTH experienced significantly more pain in response to infusion of endogenous substances in trapezius muscle than healthy controls (P≤0.05).
5
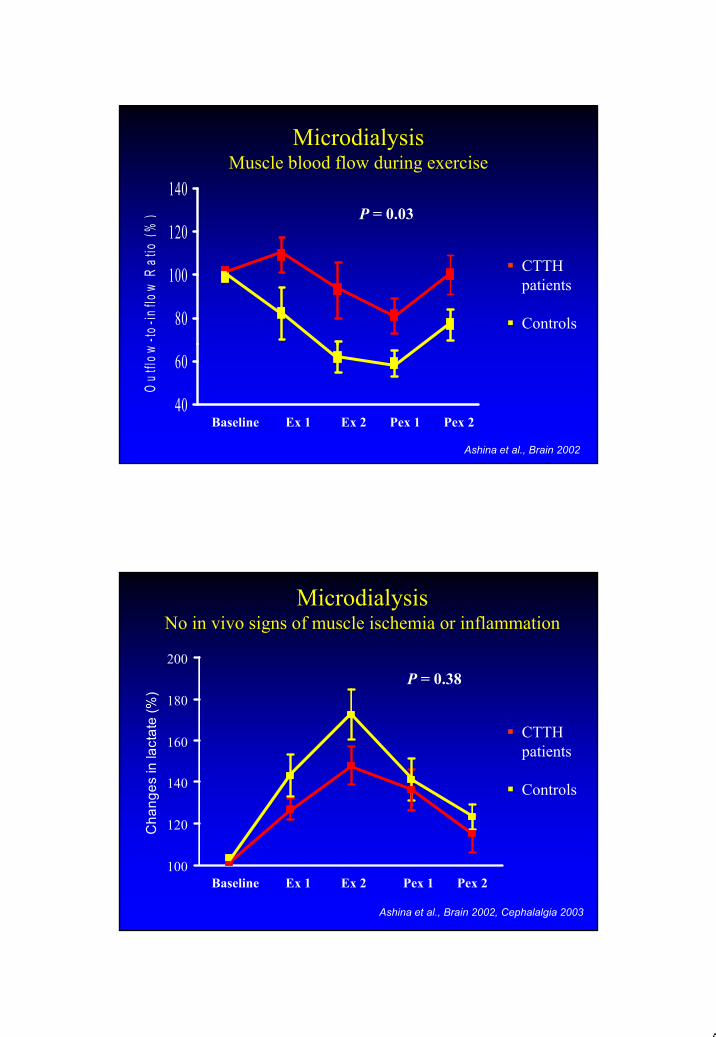
120
140
%) P = 0.03
MicrodialysisMuscle blood flow during exercise
80
100
120
-to-in
flow
Rat
io (%
CTTH patients
Controls
40
60
Out
flow
Baseline Ex 1 Ex 2 Pex 1 Pex 2
Ashina et al., Brain 2002
200P = 0.38
MicrodialysisNo in vivo signs of muscle ischemia or inflammation
140
160
180
ange
s in
lact
ate
(%)
CTTH patients
Controls
100
120Cha
Baseline Ex 1 Ex 2 Pex 1 Pex 2
Ashina et al., Brain 2002, Cephalalgia 2003
6
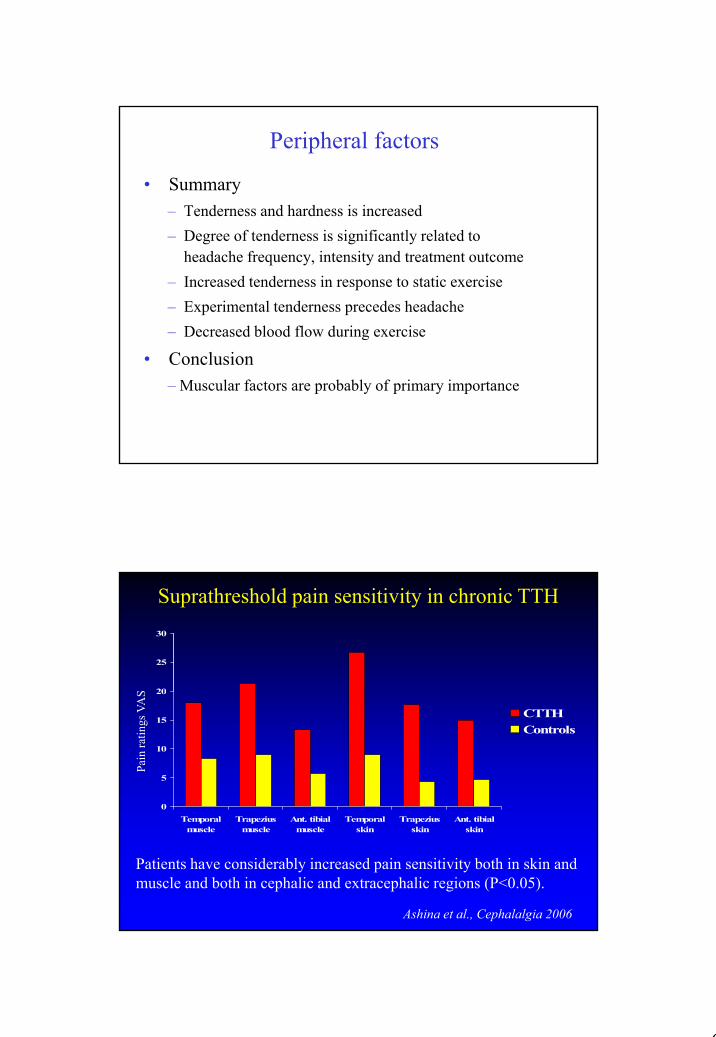
Peripheral factors
• Summary – Tenderness and hardness is increased– Degree of tenderness is significantly related to
headache frequency, intensity and treatment outcome– Increased tenderness in response to static exercise– Experimental tenderness precedes headache– Decreased blood flow during exercise
• Conclusion– Muscular factors are probably of primary importance
Suprathreshold pain sensitivity in chronic TTH
20
25
30
S
0
5
10
15
20
CTTHControls
Pain
ratin
gs V
AS
Ashina et al., Cephalalgia 2006
Patients have considerably increased pain sensitivity both in skin and muscle and both in cephalic and extracephalic regions (P<0.05).
Temporalmuscle
Trapeziusmuscle
Ant. tibialmuscle
Temporalskin
Trapeziusskin
Ant. tibialskin
7
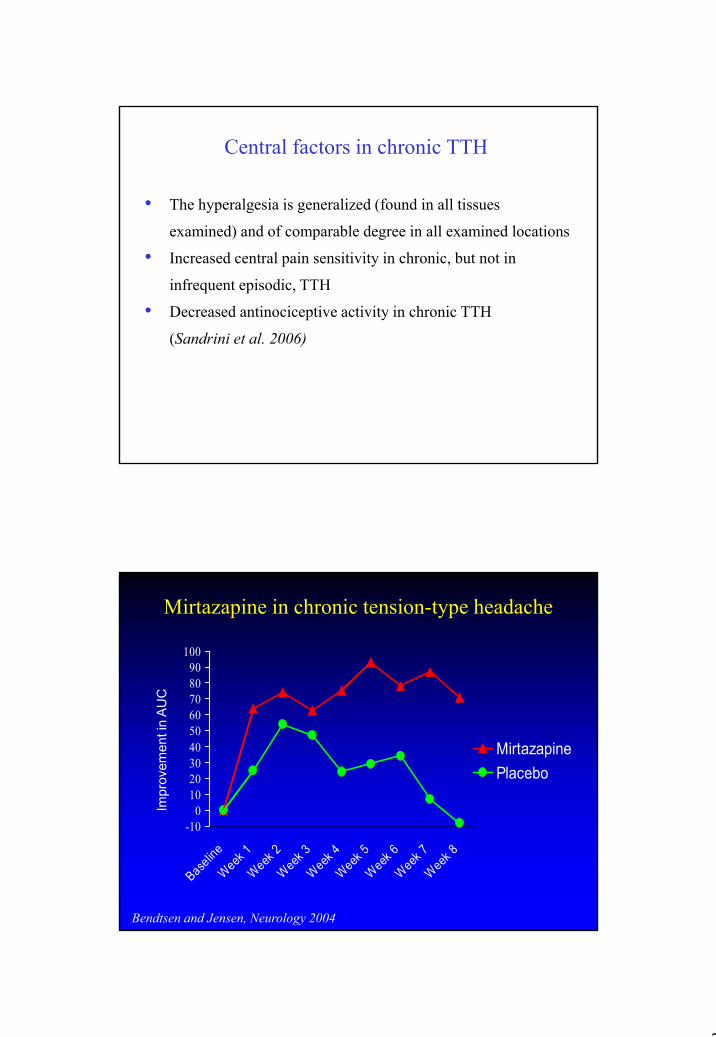
Central factors in chronic TTH
• The hyperalgesia is generalized (found in all tissues
examined) and of comparable degree in all examined locations
• Increased central pain sensitivity in chronic, but not in
infrequent episodic, TTH
• Decreased antinociceptive activity in chronic TTH
(Sandrini et al. 2006)( )
Mirtazapine in chronic tension-type headache
8090
100
C
010203040506070
MirtazapinePlacebo
Impr
ovem
ent i
n A
UC
Bendtsen and Jensen, Neurology 2004
-100
Baseline
Week 1
Week 2
Week 3
Week 4
Week 5
Week 6
Week 7
Week 8
8
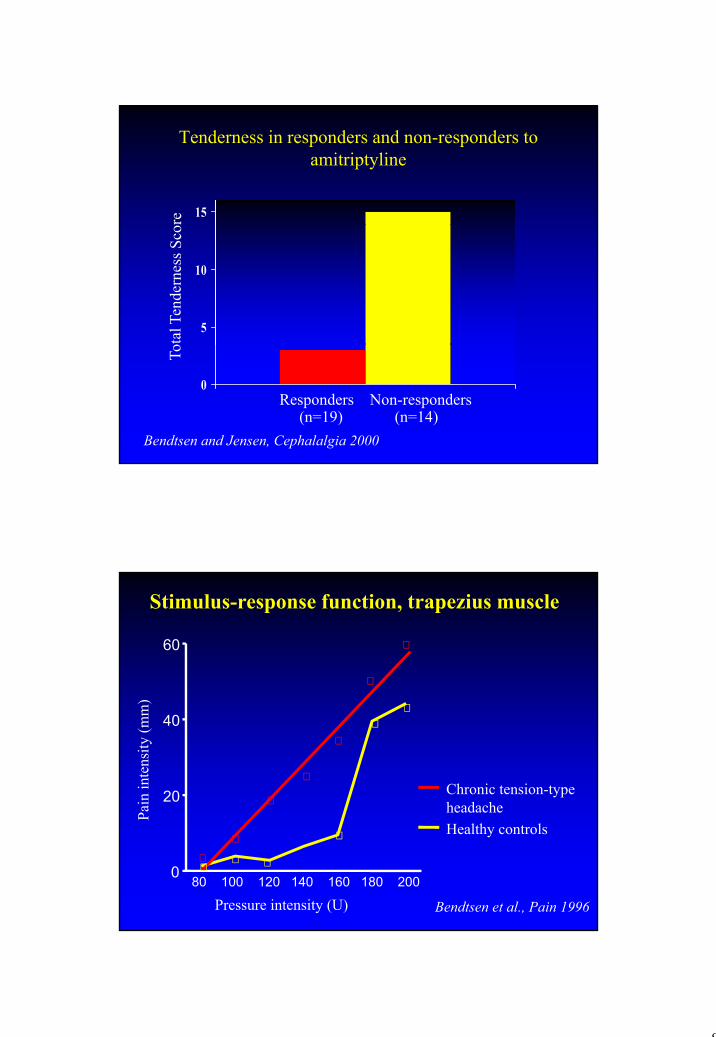
Tenderness in responders and non-responders to amitriptyline
15
5
10
0Responders Non-responders
(n=19) (n=14)Bendtsen and Jensen, Cephalalgia 2000
Stimulus-response function, trapezius muscle
60
20
40
ain
inte
nsity
(mm
)
Chronic tension-type headache
0
Pa
80 100 120 140 160 180 200
Pressure intensity (U)
headacheHealthy controls
Bendtsen et al., Pain 1996
9
Chronic tension-type headache
Continuous painful input from pericranial myofascial tissues
induce and maintain
central sensitization such that normally innocuous stimuli become painfulstimuli become painful
Conversion from episodic to chronic tension-type headache
Bendtsen, Cephalalgia 2000
Central sensitization in chronic TTH
• How to test this hypothesis?
10
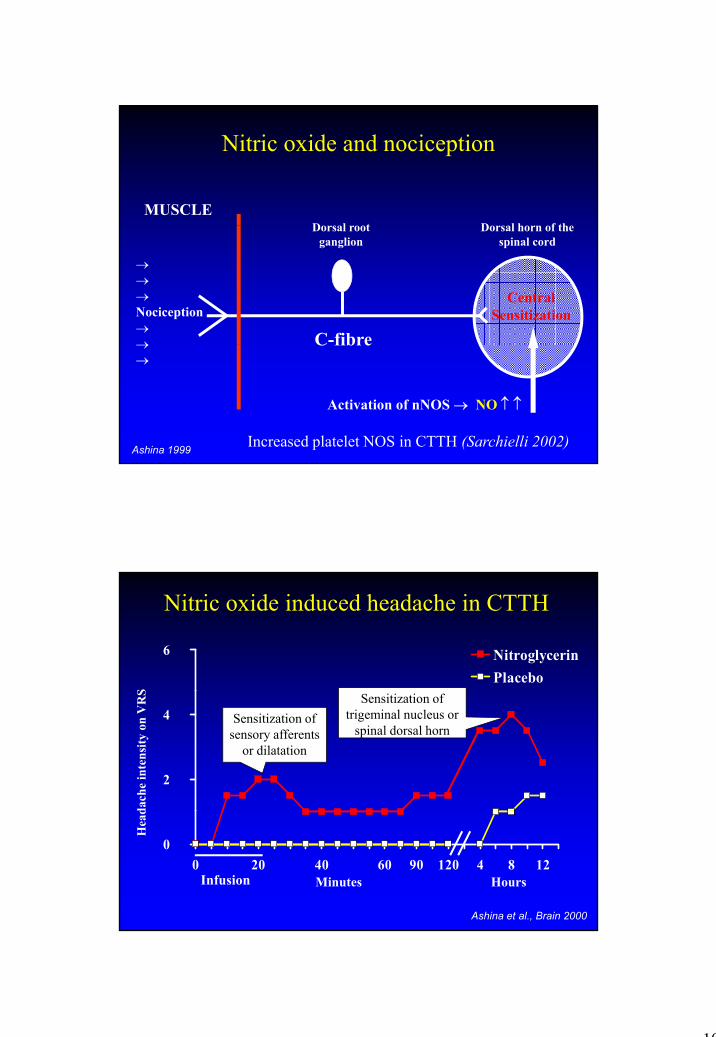
D l tMUSCLE
Nitric oxide and nociception
D l h f th
C-fibre
Dorsal root ganglion
→→→Nociception→→
Central Sensitization
Dorsal horn of the spinal cord
C fibre→→
Activation of nNOS → NO ↑ ↑
Ashina 1999 Increased platelet NOS in CTTH (Sarchielli 2002)
Nitric oxide induced headache in CTTH
6 NitroglycerinPlacebo
S
2
4
dach
e in
tens
ity o
n V
RS
Sensitization of sensory afferents
or dilatation
Sensitization of trigeminal nucleus or
spinal dorsal horn
00 20 40 60 90 120 4 8 12
Infusion Minutes Hours
Hea
d
Ashina et al., Brain 2000
11
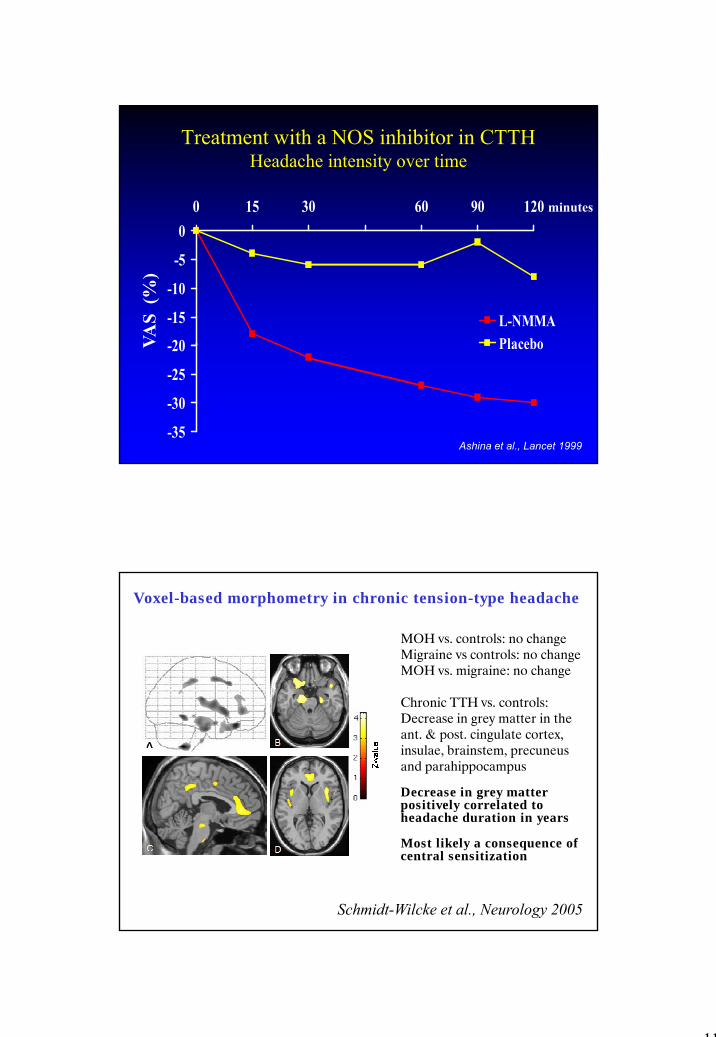
Treatment with a NOS inhibitor in CTTH Headache intensity over time
00 15 30 60 90 120 minutes
20
-15
-10
-5
0
L-NMMAPlaceboVA
S (%
)
-35
-30
-25
-20 Placebo
Ashina et al., Lancet 1999
V
Voxel-based morphometry in chronic tension-type headache
MOH vs. controls: no changeMigraine vs controls: no changeMOH vs. migraine: no change
Chronic TTH vs. controls:Decrease in grey matter in theant. & post. cingulate cortex,insulae, brainstem, precuneus and parahippocampus
Decrease in grey matter positively correlated to
Schmidt-Wilcke et al., Neurology 2005
p yheadache duration in years
Most likely a consequence of central sensitization
12
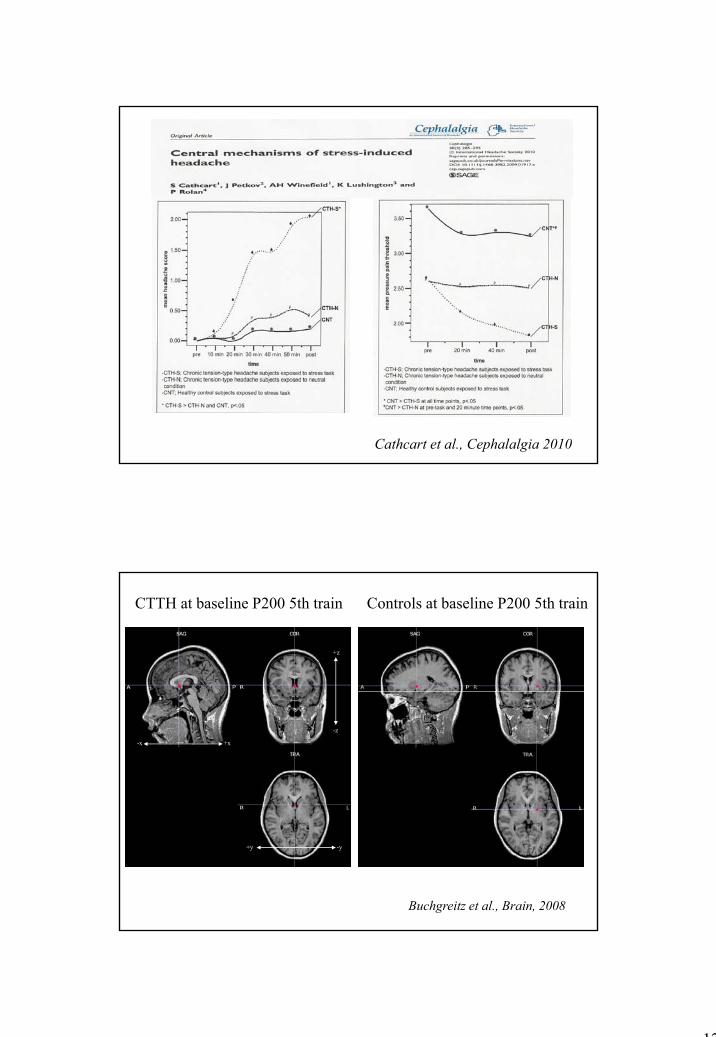
Cathcart et al., Cephalalgia 2010
CTTH at baseline P200 5th train Controls at baseline P200 5th train
+z
-z
-x +x
+y -y
Buchgreitz et al., Brain, 2008
13
+z
-z
-x +x
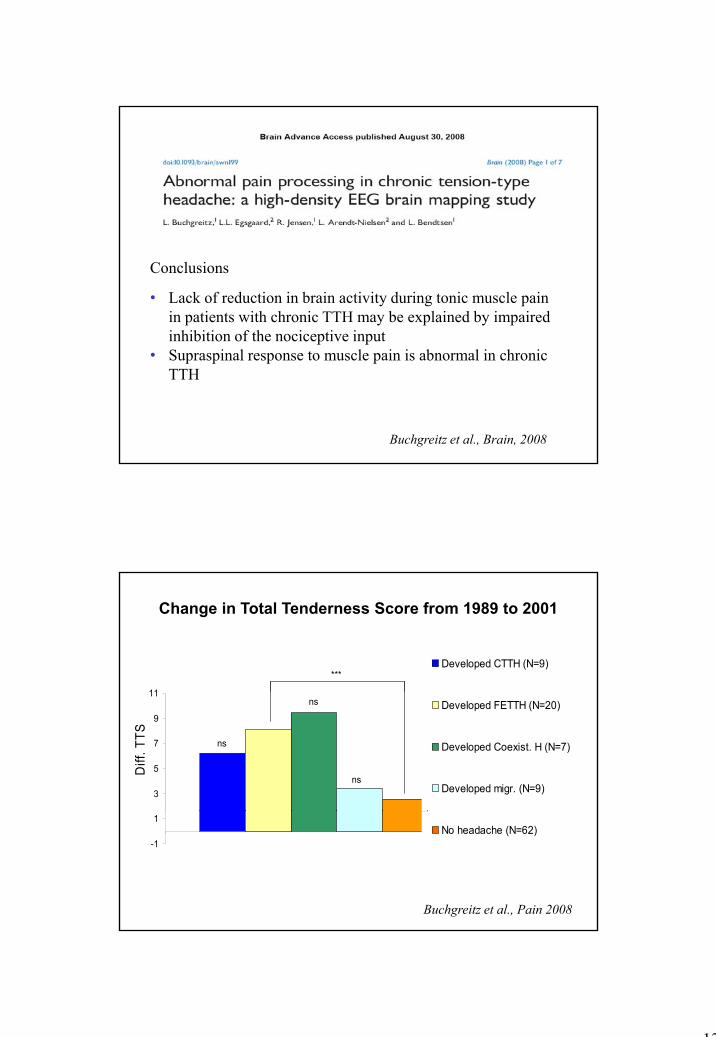
• Lack of reduction in brain activity during tonic muscle pain in patients with chronic TTH may be explained by impaired inhibition of the nociceptive input
Conclusions
+y -y
Buchgreitz et al., Brain, 2008
• Supraspinal response to muscle pain is abnormal in chronic TTH
11
Developed CTTH (N=9)***
Change in Total Tenderness Score from 1989 to 2001
3
5
7
9
11Developed FETTH (N=20)
Developed Coexist. H (N=7)
Developed migr. (N=9)
ns
ns
ns
Diff
. TTS
-1
1
1No headache (N=62)
Buchgreitz et al., Pain 2008
14
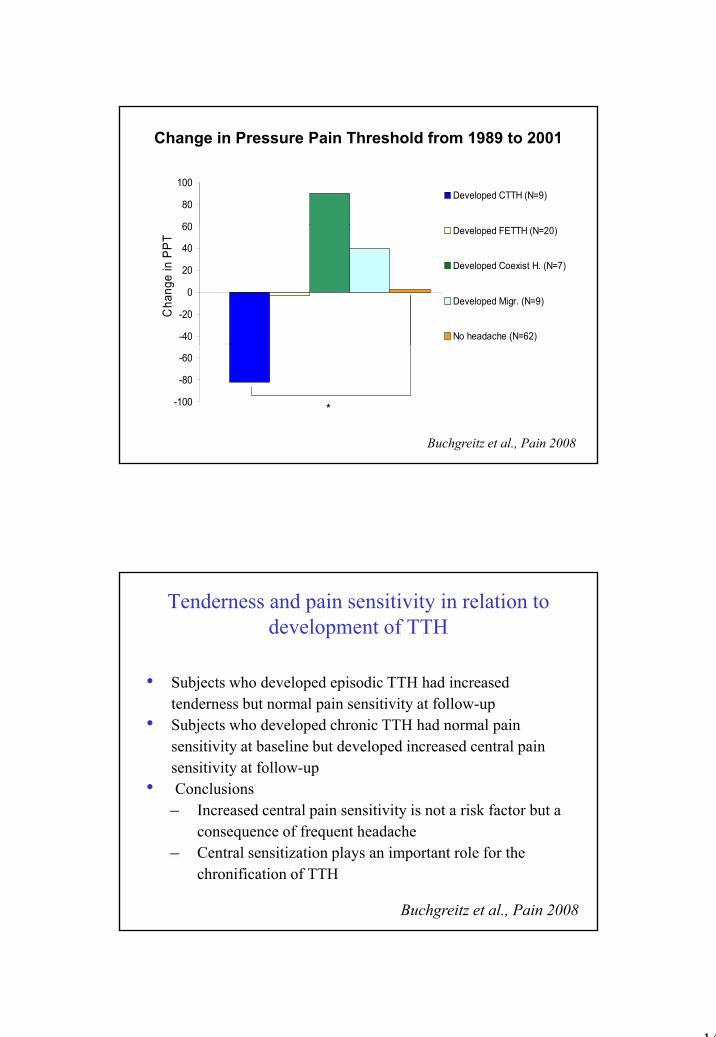
60
80
100Developed CTTH (N=9)
Change in Pressure Pain Threshold from 1989 to 2001
-40
-20
0
20
40
60 Developed FETTH (N=20)
Developed Coexist H. (N=7)
Developed Migr. (N=9)
No headache (N=62)
Cha
nge
in P
PT
-100
-80
-60
*
Buchgreitz et al., Pain 2008
Tenderness and pain sensitivity in relation to development of TTH
• Subjects who developed episodic TTH had increased tenderness but normal pain sensitivity at follow-up
• Subjects who developed chronic TTH had normal pain sensitivity at baseline but developed increased central pain sensitivity at follow-up
• Conclusions─ Increased central pain sensitivity is not a risk factor but a─ Increased central pain sensitivity is not a risk factor but a
consequence of frequent headache─ Central sensitization plays an important role for the
chronification of TTH
Buchgreitz et al., Pain 2008
15
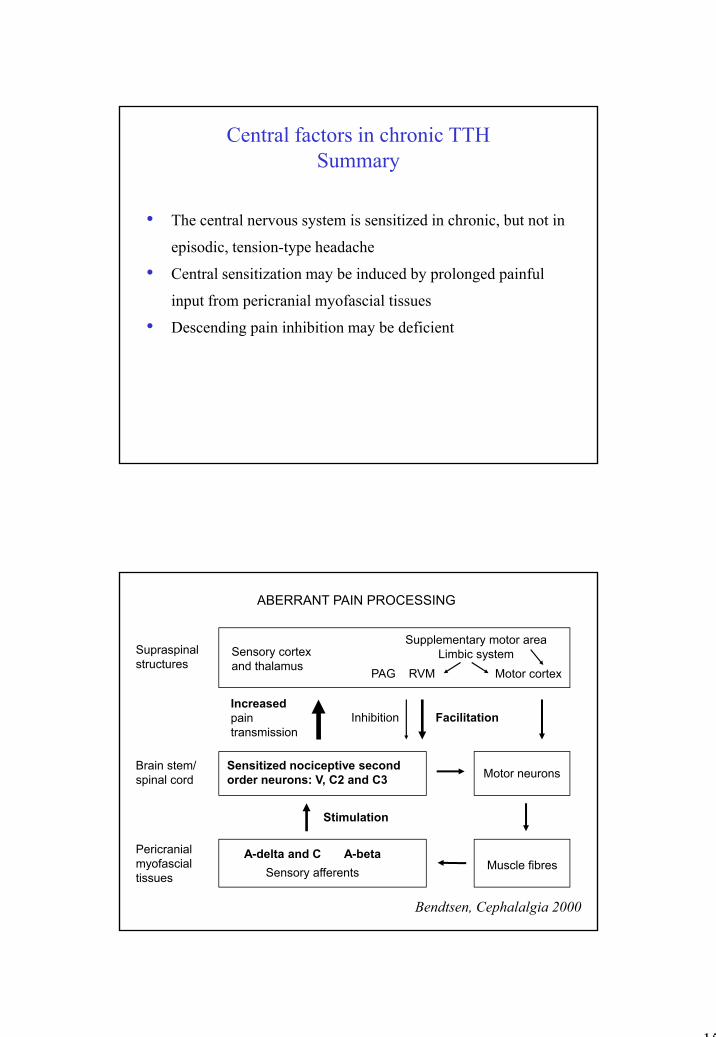
Central factors in chronic TTHSummary
• The central nervous system is sensitized in chronic, but not inThe central nervous system is sensitized in chronic, but not in
episodic, tension-type headache
• Central sensitization may be induced by prolonged painful
input from pericranial myofascial tissues
• Descending pain inhibition may be deficient
Sensory cortex and thalamus
Supraspinal structures
ABERRANT PAIN PROCESSING
Supplementary motor area Limbic system
PAG RVM Motor cortex
Brain stem/ spinal cord
Sensitized nociceptive second order neurons: V, C2 and C3 Motor neurons
Increasedpain transmission
Inhibition Facilitation
Pericranialmyofascial tissues
A-delta and C A-beta Sensory afferents Muscle fibres
Stimulation
Bendtsen, Cephalalgia 2000
16
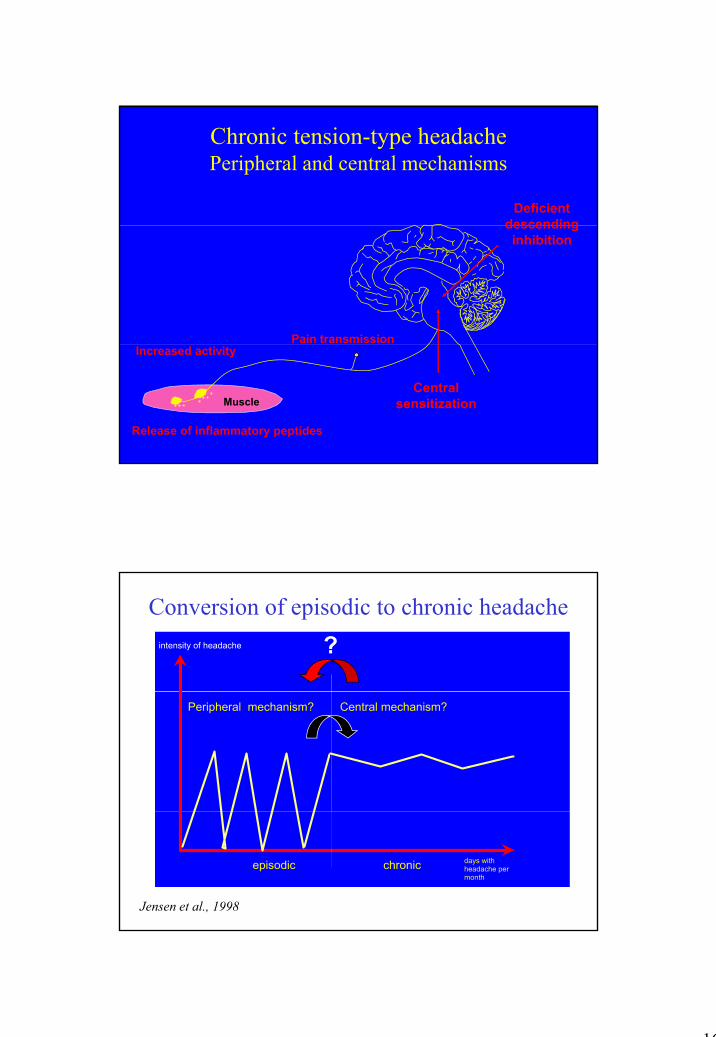
Chronic tension-type headachePeripheral and central mechanisms
Deficient descending
Pain transmission
descending inhibition
Muscle
Increased activity
Release of inflammatory peptides
Central sensitization
Conversion of episodic to chronic headacheintensity of headache ?
Peripheral mechanism? Central mechanism?
Jensen et al., 1998
episodic chronic days with headache permonth
17
• Identify source of peripheral nociception to prevent development of central sensitization and thereby conversion of episodic to chronic TTH
Future perspectives
of episodic to chronic TTH• Reduce established central sensitization• Animal model (Ellrich et al. 2005, 2006)• Muscular factors
– Abnormal activation or release of chemical mediators• Central factors
– Neuroimaging– Reduction of central sensitization, e.g., by nitric
oxide inhibitors or NMDA-antagonists


















