Benchmarking and IT Meet Pay For Performance Demands Donna Isgett, RN, MSN Vice President of...
40
Benchmarking and IT Meet Pay For Performance Demands Donna Isgett, RN, MSN Vice President of Clinical Effectiveness McLeod Health, Florence, SC Gail E. Latimer, RN, MSN Vice President and Chief Nursing Officer Siemens Medical Solutions, Malvern, PA
-
Upload
philip-webster -
Category
Documents
-
view
213 -
download
0
Transcript of Benchmarking and IT Meet Pay For Performance Demands Donna Isgett, RN, MSN Vice President of...

Benchmarking and IT Meet Pay For Performance Demands
Donna Isgett, RN, MSNVice President of Clinical EffectivenessMcLeod Health, Florence, SC
Gail E. Latimer, RN, MSNVice President and Chief Nursing OfficerSiemens Medical Solutions, Malvern, PA

Page 2
Learning Objectives
Identify strategies to promote Pay for Performance
Describe the process and methodologies McLeod has employed to build it’s culture of quality evidence-based practice and transparency
Understand the role of physician and executive leadership in developing this culture
Identify CMS outcomes achieved to date as a result of the Medicare demonstration project

Page 3
Quality - Quality Everywhere
1997• Dana Farber Cancer Institute Event
2000• To Err is Human, IOM Report
• Healthgrades.com
• Business Roundtable: Leapfrog Group
• Crossing the Quality Chasm, IOM Report
• JCAHO Sentinel Event Alerts
2002• Robert Wood Johnson - Pursuing Perfection Grant
• CMS 7 Scopes of Work
2004• Premier/CMS Demonstration Project

Page 4
Milliken Award for Quality
CMS/Premier Demonstration Project “Top Performer”
Publication Features: Modern HealthcareUS News and World ReportUSA Today
McLeod Quality

Page 5
CMS/Premier Hospital Quality Incentive
AMI, CABG, HF, CAP, Hip and Knee278 participating hospitals
Quality - Pay for Performance
The first national project to measure hospital performance and offer additional Medicare payment for top quality care (October, 2003)
Widely accepted quality measures(34)
27 indicators from the National Quality Forum
Public reporting

Page 6
Quality - Results that Make a Difference
McLeod Regional Medical CenterOctober 2003 - September 2004
Composite Quality Score
Clinical Focus Area National Top Decile MRMC Decile
AMI 95.8% 98.0% 1
CABG 95.6% 95.6% 1
HF 85.2% 85.0% 2
CAP 83.5% 85.8% 1
Hip/Knee 94.8% 95.1% 1
Page 7
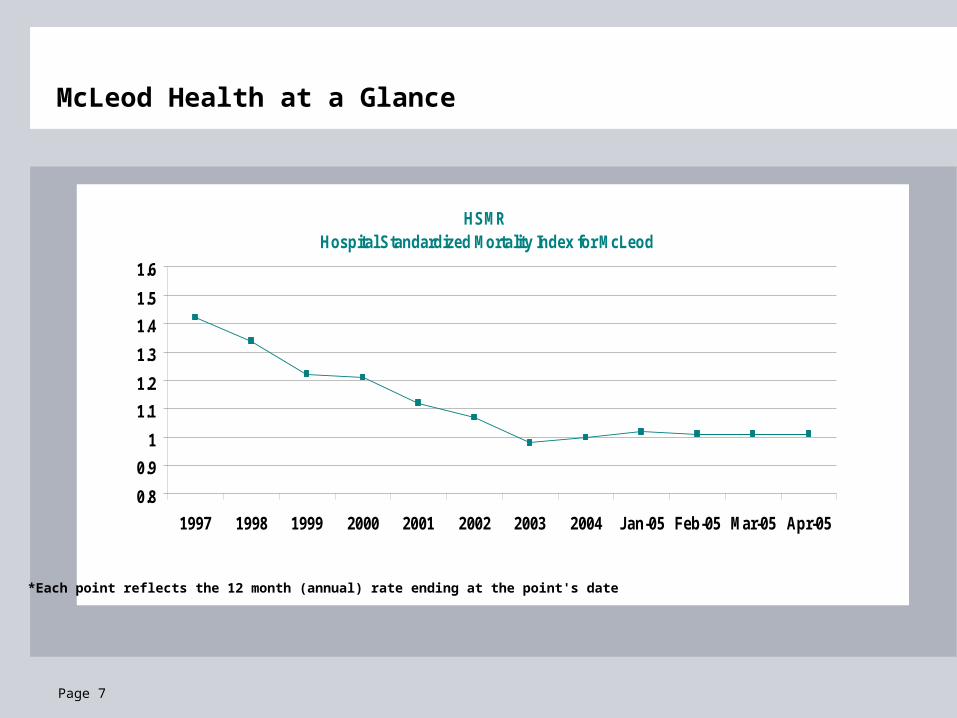
McLeod Health at a Glance
HSMR Hospital Standardized Mortality Index for McLeod
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
1997 1998 1999 2000 2001 2002 2003 2004 Jan-05 Feb-05 Mar-05 Apr-05
*Each point reflects the 12 month (annual) rate ending at the point's date

Page 8
Page 9
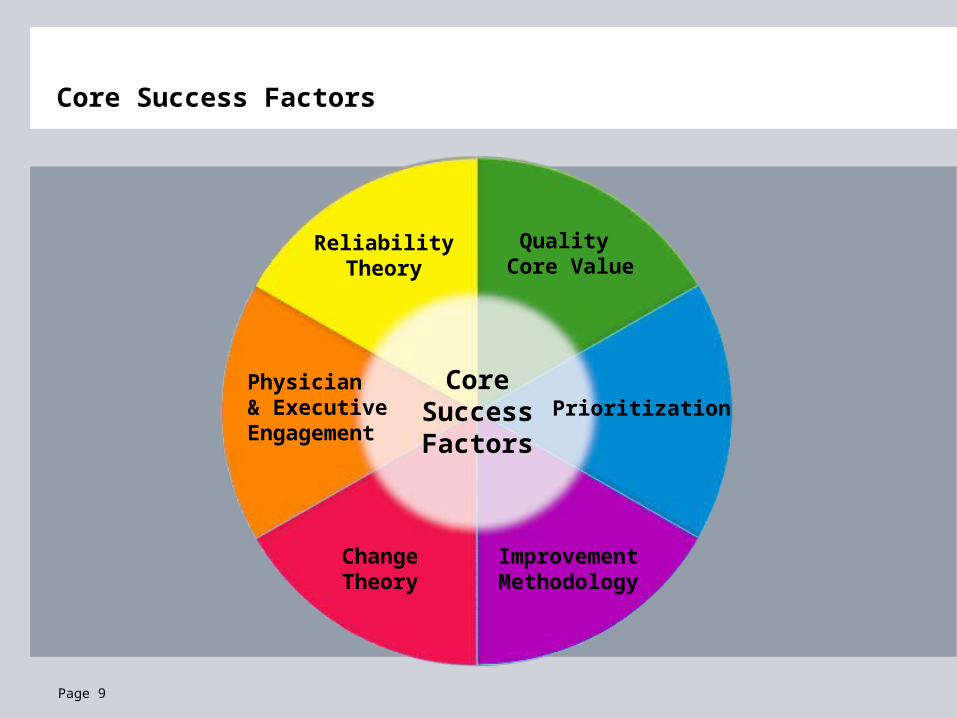
ReliabilityTheory
Quality Core Value
Physician & Executive Engagement
Improvement Methodology
PrioritizationCore
Success Factors
Change Theory
Core Success Factors

Page 10
Quality Core Value
CoreSuccess Factors
Clinical Effectiveness: Promoting Change

Page 11
Core Values
Value of Person
Value of Integrity
Value of Caring
Value of Quality
Page 12
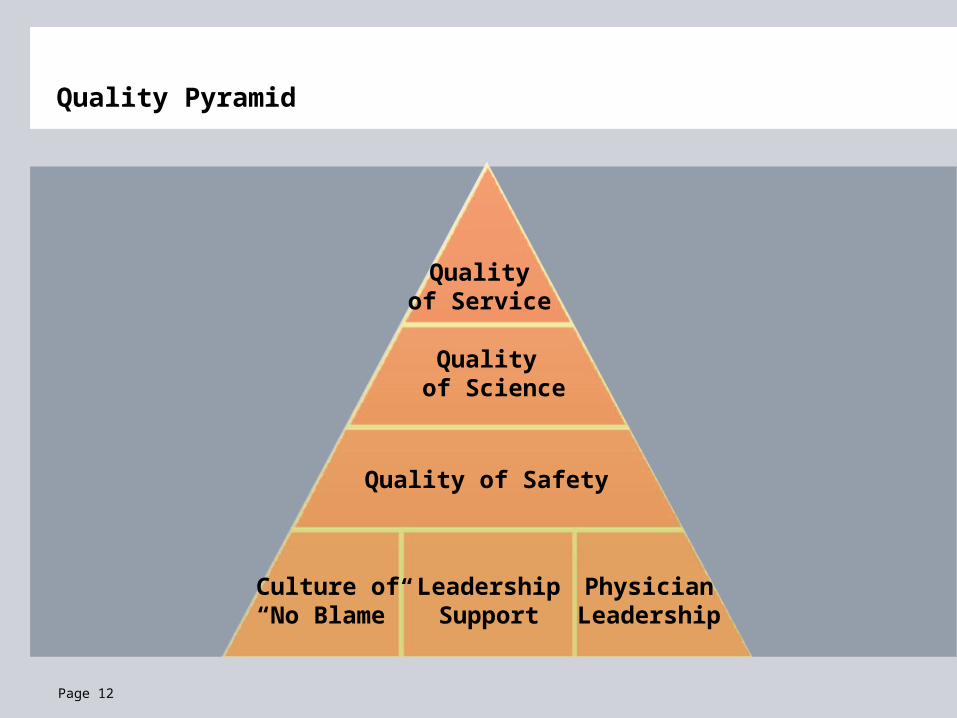
Quality of Service
Culture of“No Blame”
Leadership Support
Physician Leadership
Quality of Safety
Quality of Science
Quality Pyramid

Page 13
Quality Core Value
CoreSuccess Factors
Prioritization
Clinical Effectiveness: Promoting Change

Page 14
Cost
LOS Complications
Readmissions
Prioritization: Benchmarking Assessment
Mortality
Opportunity

Page 15
Prioritization: National Benchmarking
Purchased Databases
Premier Perspective
Vermont Oxford
STS (Society of Thoracic Surgeons)
Public Data
Medicare website
CMS 7 scopes of work
Leapfrog Group
Healthgrades.com

Page 16
Quality Core Value
Improvement Methodology
PrioritizationCore
Success Factors
Clinical Effectiveness: Promoting Change

Page 17
Methodology:
GE’s Total Quality Management (TQM)
Problem Solving Process (PSP)
Results Oriented ProcessImplemented - 1994
1. Identify & Select Problem
5. ImplementSolution
4. Select/PlanSolution
3. GeneratePotential Solutions
2. Analyzefor Cause
ProblemSolvingProcess
6. EvaluateSolution
Performance Improvement

Page 18
Quality Core Value
Improvement Methodology
PrioritizationCore
Success Factors
Change Theory
Clinical Effectiveness: Promoting Change

Page 19
Kotter’s Theory of Change
1. Establishing a Sense of Urgency
2. Forming a Powerful Guiding Coalition
3. Creating a Vision
4. Communicating the Vision
5. Empowering Others to Act on the Vision
6. Planning for and Creating Short-Term Wins
7. Consolidating Improvements and Producing Still More Change
8. Institutionalizing New Approaches
John Kotter, Leading Change

Page 20
Quality Core Value
Improvement Methodology
PrioritizationCore
Success Factors
Change Theory
Physician & Executive Engagement
Clinical Effectiveness: Promoting Change

Page 21
Clinical Effectiveness: Quality of the Science
Design Principles:
Physician Leadership
Evidence Based
Data Driven
Senior Leadership Key:
Priority of Work
Dedicated Staff
Implementation of Ideas

Page 22
ReliabilityTheory
Quality Core Value
Physician & Executive Engagement
Improvement Methodology
PrioritizationCore
Success Factors
Change Theory
Core Success Factors

Page 23
Intent, Vigilance and Hard Work: 101 Performance
Level 1 (Designing basic failure prevention)
Common equipment, standard orders sheets
Personal check lists
Working harder next time
Feedback of information on compliance
Awareness and training
© Institute for Healthcare Improvement

Page 24
Level 1 Changes at McLeod
Pre-printed order sets
Data feedback to physicians and hospital staff
Education to physicians and hospital staff
Pre-printed Rx scripts
Disease specific discharge sheets to include detailed instructions/meds
© Institute for Healthcare Improvement

Page 25
Human Factors and Reliability Science: 102 Performance
Level 2
Decision aids and reminders built into the system
Desired action the default (based on evidence)
Redundancy
Scheduling
Taking advantage of habits and patterns
Standardization of process
© Institute for Healthcare Improvement

Page 26
Level 2 Changes at McLeod
Decision aids and reminders built into the system:
Antibiotics in Pyxis in ER and reminder on Pyxis "Blood cultures needed? Check with physician”
Decision aids and reminders built into the system:
List of all positive troponins for intervention
Desired action the default (based on evidence):
House-wide pneumonia vaccination standing order
Desired action the default (based on evidence):
Automatic printing of smoking cessation information for patients
Redundancy:
Medication check against allergies
© Institute for Healthcare Improvement

Page 27
Level 2 Changes at McLeod
Taking advantage of habits and patterns
All operative antibiotics given as leaving holding area
Radiologist to contact ED physician if chest XRay positive for pneumonia
Standardization of process
All patients screened for smoking at admission and counseled on discharge
© Institute for Healthcare Improvement

Page 28
ReliabilityTheory
Quality Core Value
Physician & Executive Engagement
Improvement Methodology
PrioritizationCore
Success Factors
Change Theory
Core Success Factors

Page 29
Key Ways IT Can Support Pay for Performance
Reliability
Hand-off communication
Patients “in the know”

Page 30
Workflow EngineThe Right Information, to the Right Person, at the Right Time…

Page 32
Workflow EngineListening, Monitoring, and Escalating…

Page 33
Increase Accuracy and Reliability of Clinical ProcessesComputerized Physician Order Entry

Page 34
Increase Accuracy and Reliability of Clinical Processes Evidence-based Content

Page 35
Increase Accuracy and Reliability of Clinical ProcessesHand-off Communication

Page 36

Page 37
Personal Health CardsSMART Card
A secure SMART Card contains your critical healthcare information
Allows medical providers the ability to track patients through a course of treatment that crosses multiple organizations
Authenticates the patient and provides for improved insurance processing
Delivers a scalable, portable health record – and control of patient medical data

Page 38
Healthcare Technology Utilized
PHR- Personal health record/SMART cards Schedule appointments Reminders Medication history Personal spending account Monitoring
HomePhysician’s
Office Hospital InsuranceProvider

Page 39
Healthcare Technology Utilized
HomePhysician’s
Office Hospital InsuranceProvider
Interoperability Electronic patient records Referring physicians Trends/ benchmarking Billing

Page 40
InsuranceProvider
Healthcare Technology Utilized
HomePhysician’s
Office Hospital
Clinical Information System Point of care information Evidence-based practice CPOE Workflow engine PACS/results Trends/benchmarking

Page 41
Healthcare Technology Utilized
InsuranceProviderHome
Physician’sOffice Hospital
Clinical information
Billing codes
Payment
Trends/benchmarking