Belgian Heart Disease Prevention Project -...
9
The Belgian Heart Disease Prevention Project Modification of the Coronary Risk Profile in an Industrial Population MARCEL KORNITZER, M.D., GuY DE BACKER, M.D., MICHELE DRAMAIX, M.SC., AND CLAUDE THILLY, M.D. SUMMARY The Belgian Heart Disease Prevention Project is a controlled, multifactorial prevention trial involving 19,390 males aged 40-59 years employed by 30 Belgian industries. These industries were paired and randomized into a control or intervention unit. In each intervention factory, the subjects from the two highest deciles of a coronary risk-score distribution curve were given individual advice twice a year. A health education campaign was also organized in each intervention factory. In the control group, 10% of randomly chosen sub- jects had the same baseline examination as the whole of the intervention group. After 2 years, high-risk sub- jects and random samples of the control and intervention group were compared regarding the coronary risk profile by means of a multiple logistic function (MLF). In the intervention high-risk group, the MLF showed a decrease of 20%, and in the control group there was an increment of 12.5% (p < 0.001). Comparing the ran- dom samples an increment of 25% was found in the control group vs a drop of 2.26 in the intervention group (p < 0.001). The coronary risk profile can be altered in a middle-aged male working population through mass media health education supplemented by face-to-face counseling in high-risk subjects. EPIDEMIOLOGIC STUDIES of cardiovascular dis- ease in Europe and the United States have repeatedly shown that the incidence of ischemic heart disease (IHD) is related to several risk factors. The most im- portant of these are blood cholesterol, arterial blood pressure and cigarette smoking. Despite the major development of medical care during this century, IHD remains a highly lethal illness, because of the high proportion of sudden deaths. Primary prevention seems to be the most rational way of tackling this dis- ease, which is responsible for the death of one in every three men and one in every four women in Belgium. Various unifactorial trials suggest that reduction of serum cholesterol has a favorable influence on the in- cidence of IHD.1-3 The Veterans Administration Cooperative Study Group4 revealed the beneficial effect of the treatment of high blood pressure on the incidence of complications of hypertension. A con- trolled study of changes in smoking habits5 is un- derway, but results have not yet been published. There are strong reasons, both theoretical and prac- tical, why multifactorial trials are appropriate: 1) The total effect of a multifactorial approach is likely to be greater. 2) When people are advised to change one thing, they may change other things as well. For example, weight reduction can also have an effect on blood pressure levels. From the Laboratory of Epidemiology and Social Medicine, Free University of Brussels, and the Department of Cardiology, Univer- sity Ghent, Belgium. Dr. De Backer is an Established Investigator, Nationaal Fonds voor Wetenschappelijk Onderzoek, University Ghent. Supported by grant 20.202 of the FRSM. Address for correspondence: Marcel Kornitzer, M.D., Ecole de Sante Publique, Campus Erasme CP.590, 808 Route de Lennick, 1070 Bruxelles, Belgium. Received November 17, 1978; revision accepted July 13, 1979. Circulation 61, No. 1, 1980. 3) In the health education field a unifactorial de- sign may be unachievable. However, a multifactorial design is less appropriate to study the causality of the relation between a single risk factor and IHD. If the trial is effective, it will not be possible to relate the beneficial effects to specific items of the preventive program; if the trial fails, it is difficult to identify in a multifactorial model what parts of the intervention program were inefficient. In the early 1970s several controlled, multifactorial prevention studies were launched that used a wide variety of methods and intervention techniques. The Goteborg study6 involved the random allocation of 10,000 subjects into an intervention group and 20,000 subjects into two control groups; with the cooperation of specialized clinics, the intervention group was given advice during face-to-face interviews and group dynamics. The Oslo study7 investigated the effects of simultaneously modifying the serum cholesterol levels and smoking habits of 4049-year-old men. In the United States, the Multiple Risk Factor Intervention Trial8 involves middle-aged men defined as high-risk subjects on the basis of a multiple logistic function (MLF). In these last two studies, the counseling is mainly face-to-face. All these studies were based on randomization of subjects. A controlled multifactorial study conducted in North Karelia9 involved a mass campaign of health education in that Finnish province, which has the highest incidence of IHD; a neighboring province was used as control. Counseling was mainly provided through mass media. The Stanford Three Communities Study'0 12 con- sisted essentially of a controlled trial in health educa- tion using mass media as well as face-to-face inter- vention in high-risk subjects. One community was subjected to health education both via mass media and individual techniques; in a second community only mass media were used, and a third community served as control. 18 by guest on July 8, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
duongxuyen -
Category
Documents
-
view
215 -
download
0
Transcript of Belgian Heart Disease Prevention Project -...

The Belgian Heart Disease Prevention Project
Modification of the Coronary Risk Profilein an Industrial Population
MARCEL KORNITZER, M.D., GuY DE BACKER, M.D., MICHELE DRAMAIX, M.SC.,
AND CLAUDE THILLY, M.D.
SUMMARY The Belgian Heart Disease Prevention Project is a controlled, multifactorial prevention trialinvolving 19,390 males aged 40-59 years employed by 30 Belgian industries. These industries were paired andrandomized into a control or intervention unit. In each intervention factory, the subjects from the two highestdeciles of a coronary risk-score distribution curve were given individual advice twice a year. A health educationcampaign was also organized in each intervention factory. In the control group, 10% of randomly chosen sub-jects had the same baseline examination as the whole of the intervention group. After 2 years, high-risk sub-jects and random samples of the control and intervention group were compared regarding the coronary riskprofile by means of a multiple logistic function (MLF). In the intervention high-risk group, the MLF showed adecrease of 20%, and in the control group there was an increment of 12.5% (p < 0.001). Comparing the ran-dom samples an increment of 25% was found in the control group vs a drop of 2.26 in the intervention group(p < 0.001). The coronary risk profile can be altered in a middle-aged male working population through mass
media health education supplemented by face-to-face counseling in high-risk subjects.
EPIDEMIOLOGIC STUDIES of cardiovascular dis-ease in Europe and the United States have repeatedlyshown that the incidence of ischemic heart disease(IHD) is related to several risk factors. The most im-portant of these are blood cholesterol, arterial bloodpressure and cigarette smoking. Despite the majordevelopment of medical care during this century, IHDremains a highly lethal illness, because of the highproportion of sudden deaths. Primary preventionseems to be the most rational way of tackling this dis-ease, which is responsible for the death of one in everythree men and one in every four women in Belgium.
Various unifactorial trials suggest that reduction ofserum cholesterol has a favorable influence on the in-cidence of IHD.1-3 The Veterans AdministrationCooperative Study Group4 revealed the beneficialeffect of the treatment of high blood pressure on theincidence of complications of hypertension. A con-trolled study of changes in smoking habits5 is un-derway, but results have not yet been published.
There are strong reasons, both theoretical and prac-tical, why multifactorial trials are appropriate:
1) The total effect of a multifactorial approach islikely to be greater.
2) When people are advised to change one thing,they may change other things as well. For example,weight reduction can also have an effect on bloodpressure levels.
From the Laboratory of Epidemiology and Social Medicine, FreeUniversity of Brussels, and the Department of Cardiology, Univer-sity Ghent, Belgium.
Dr. De Backer is an Established Investigator, Nationaal Fondsvoor Wetenschappelijk Onderzoek, University Ghent.
Supported by grant 20.202 of the FRSM.Address for correspondence: Marcel Kornitzer, M.D., Ecole de
Sante Publique, Campus Erasme CP.590, 808 Route de Lennick,1070 Bruxelles, Belgium.Received November 17, 1978; revision accepted July 13, 1979.Circulation 61, No. 1, 1980.
3) In the health education field a unifactorial de-sign may be unachievable.
However, a multifactorial design is less appropriateto study the causality of the relation between a singlerisk factor and IHD. If the trial is effective, it will notbe possible to relate the beneficial effects to specificitems of the preventive program; if the trial fails, it isdifficult to identify in a multifactorial model whatparts of the intervention program were inefficient.
In the early 1970s several controlled, multifactorialprevention studies were launched that used a widevariety of methods and intervention techniques. TheGoteborg study6 involved the random allocation of10,000 subjects into an intervention group and 20,000subjects into two control groups; with the cooperationof specialized clinics, the intervention group was givenadvice during face-to-face interviews and groupdynamics. The Oslo study7 investigated the effects ofsimultaneously modifying the serum cholesterol levelsand smoking habits of 4049-year-old men. In theUnited States, the Multiple Risk Factor InterventionTrial8 involves middle-aged men defined as high-risksubjects on the basis of a multiple logistic function(MLF). In these last two studies, the counseling ismainly face-to-face. All these studies were based onrandomization of subjects. A controlled multifactorialstudy conducted in North Karelia9 involved a masscampaign of health education in that Finnishprovince, which has the highest incidence of IHD; aneighboring province was used as control. Counselingwas mainly provided through mass media.The Stanford Three Communities Study'0 12 con-
sisted essentially of a controlled trial in health educa-tion using mass media as well as face-to-face inter-vention in high-risk subjects. One community wassubjected to health education both via mass media andindividual techniques; in a second community onlymass media were used, and a third community servedas control.
18
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
BELGIAN HEART PROJECT/Kornitzer et al.
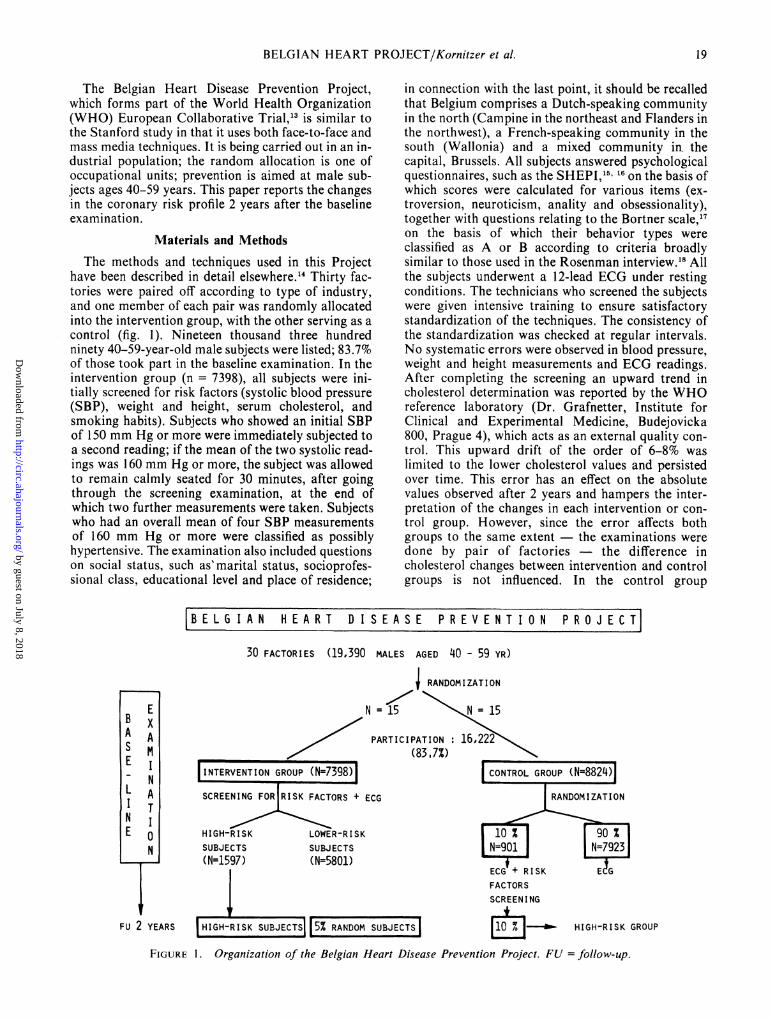
The Belgian Heart Disease Prevention Project,which forms part of the World Health Organization(WHO) European Collaborative Trial,13 is similar tothe Stanford study in that it uses both face-to-face andmass media techniques. It is being carried out in an in-dustrial population; the random allocation is one ofoccupational units; prevention is aimed at male sub-jects ages 40-59 years. This paper reports the changesin the coronary risk profile 2 years after the baselineexamination.
Materials and MethodsThe methods and techniques used in this Project
have been described in detail elsewhere.'4 Thirty fac-tories were paired off according to type of industry,and one member of each pair was randomly allocatedinto the intervention group, with the other serving as acontrol (fig. 1). Nineteen thousand three hundredninety 40-59-year-old male subjects were listed; 83.7%of those took part in the baseline examination. In theintervention group (n = 7398), all subjects were ini-tially screened for risk factors (systolic blood pressure(SBP), weight and height, serum cholesterol, andsmoking habits). Subjects who showed an initial SBPof 150 mm Hg or more were immediately subjected toa second reading; if the mean of the two systolic read-ings was 160 mm Hg or more, the subject was allowedto remain calmly seated for 30 minutes, after goingthrough the screening examination, at the end ofwhich two further measurements were taken. Subjectswho had an overall mean of four SBP measurementsof 160 mm Hg or more were classified as possiblyhypertensive. The examination also included questionson social status, such as'marital status, socioprofes-sional class, educational level and place of residence;
in connection with the last point, it should be recalledthat Belgium comprises a Dutch-speaking communityin the north (Campine in the northeast and Flanders inthe northwest), a French-speaking community in thesouth (Wallonia) and a mixed community in thecapital, Brussels. All subjects answered psychologicalquestionnaires, such as the SHEPI,15' 16 on the basis ofwhich scores were calculated for various items (ex-troversion, neuroticism, anality and obsessionality),together with questions relating to the Bortner scale,17on the basis of which their behavior types wereclassified as A or B according to criteria broadlysimilar to those used in the Rosenman interview.'8 Allthe subjects underwent a 12-lead ECG under restingconditions. The technicians who screened the subjectswere given intensive training to ensure satisfactorystandardization of the techniques. The consistency ofthe standardization was checked at regular intervals.No systematic errors were observed in blood pressure,weight and height measurements and ECG readings.After completing the screening an upward trend incholesterol determination was reported by the WHOreference laboratory (Dr. Grafnetter, Institute forClinical and Experimental Medicine, Budejovicka800, Prague 4), which acts as an external quality con-trol. This upward drift of the order of 6-8% waslimited to the lower cholesterol values and persistedover time. This error has an effect on the absolutevalues observed after 2 years and hampers the inter-pretation of the changes in each intervention or con-trol group. However, since the error affects bothgroups to the same extent - the examinations weredone by pair of factories - the difference incholesterol changes between intervention and controlgroups is not influenced. In the control group
BELG IAN HEART D I SEASE PREVENT I ON PROJECTT
30 FACTORIES (19,390 MALES AGED 40 - 59 YR)
} RANDOMIZATION
N = \ =15
PARTICIPATION:(83.7%)
INTERVENTION GROUP (N=7398)~a
SCREENING FOR RISK FACTORS + ECG
HIGH-RISK LOWER-RISKSUBJECTS SUBJECTS(N=1597) (N=5801)
FACTORSSCREENING
1 .--HIGH-RISK SUBJECTS 5% RANDOM SUBJECTS] HIGH-RISK GROUP
FIGURE 1. Organization of the Belgian Heart Disease Prevention Project. FU =follow-up.
EA .A
E NL A
ITN IE 0
N
*u 2 YEARS
19
F
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 61, No 1, JANUARY 1980
TABLE 1. Calculation of Coronary Risk Score
Points to be added to scoreFactor 0 1 112 2 212 3
Age (years) <50 50+Job activity Heavy Light Sedentary
Cigarettes/day <5 5- 20+Systolic blood pressure(mm Hg) <120 120- 140- 160+
Serum cholesterol(mg/dl) <210 210- 220- 230- 240- 250- 260+
(n = 8824), 10% of the subjects in each occupationalunit were randomly selected to undergo the samethorough initial examination as all the subjects in theintervention group; the other 90% were subjected onlyto an ECG at rest. For all the subjects in the interven-tion group, and for the 10% of the control group thatunderwent the same thorough initial examinations,risk profiles were established on the basis of the initialresults, according to a "risk score" (table 1). The sub-jects who belonged to the top 21% of the risk score dis-tribution were arbitrarily placed in the high-risk group(n = 1601), and the others in the lower-risk group.Among the high-risk subjects in the interventiongroup, 85% smoked five or more cigarettes a day,96.5% had a serum cholesterol value of 220 mg/100ml or more, 29% had an initial systolic blood pressureof . 160 mm Hg, 17.5% had a mean of four bloodpressure values > 160 mm Hg, and 21% of the sub-jects had a relative weight . 1153%. The subjects in theintervention group were also classified according to aMLF, using the coefficients of the European cohorts inthe Seven Countries Study.'9 Sixty percent of the high-risk subjects according to the risk score distributionwere also located in the two highest deciles of theMLF.
Intervention Program
The high-risk subjects in the intervention groupwere given individual counseling twice a year by twophysicians in the Project. At the start of the Project,these subjects were given written information concern-ing their particular risk factors and they all benefitedfrom the mass counseling program (posters regularlydisplayed on factory premises, antismoking talks anddietary advice to the factory canteen stafl).The lower-risk group received literature on par-
ticular risk factors and benefited from the mass cam-paign; individual counseling was only given once in arandomly selected sample of 5% of the total interven-tion group.The subject's family doctors and the occupational
physicians received regular information about the riskfactors of each individual, and they took an importantpart in the intervention program.The program was directed against the following risk
factors: serum cholesterol; cigarette smoking;hypertension; obesity; and sedentary habit.
Serum CholesterolAll the subjects were considered at risk. Individual
advice or literature was given concerning the reductionof total fat intake and of dietary cholesterol and thepartial replacement of saturated by polyunsaturatedfats.
Cigarette SmokingSubjects who smoked five or more cigarettes a day
were encouraged to quit.
Hypertension
Subjects with a mean SBP (mean of four readingson the same day) of 160 mm Hg or more were givenpreventive advice - to lose weight if they were obese,not to add salt to prepared foods and to consult theirfamily doctors, who should consider drug prescrip-tion. These doctors had already received informationand instructions on the treatment of hypertension,with emphasis on the importance of regular follow-upand continuous treatment.
ObesityAll subjects with an excess in weight of 15% or more
by local standards were regarded as being at risk andwere given advice on weight reduction - to reducecaloric intake and increase physical exercise.
Sedentary HabitEfforts were directed toward encouraging regular
physical exercise among subjects whose occupationalphysical activity was regarded as light and who did notengage in any exercise during leisure.
Follow-up
High-risk subjects in the intervention group wererecalled twice a year and examined by one of the doc-tors participating in the Belgian Heart DiseasePrevention Project. In addition, 5% of the subjects inthe intervention group were randomly selected for an-nual examinations. Finally, the group of subjects fromthe control group who underwent the completebaseline examination was reexamined after 2 years.
In this paper, we compare the results after 2 years in
20 CIRCULATION
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
BELGIAN HEART PROJECT/Kornitzer et al.
mmHg153
150-
150
io.
139.1,
130
SYSTOLIC BLOOD PRESSURE
HIGH-RISK GROUP
P<.001
RANDOM SAMPLE\> ~~~~~~~~~~- 0.3~~~~~~~~~~P'.00147%
- INTERVENTION0- -0 CONTROL
0
mgr%
11479
132.5
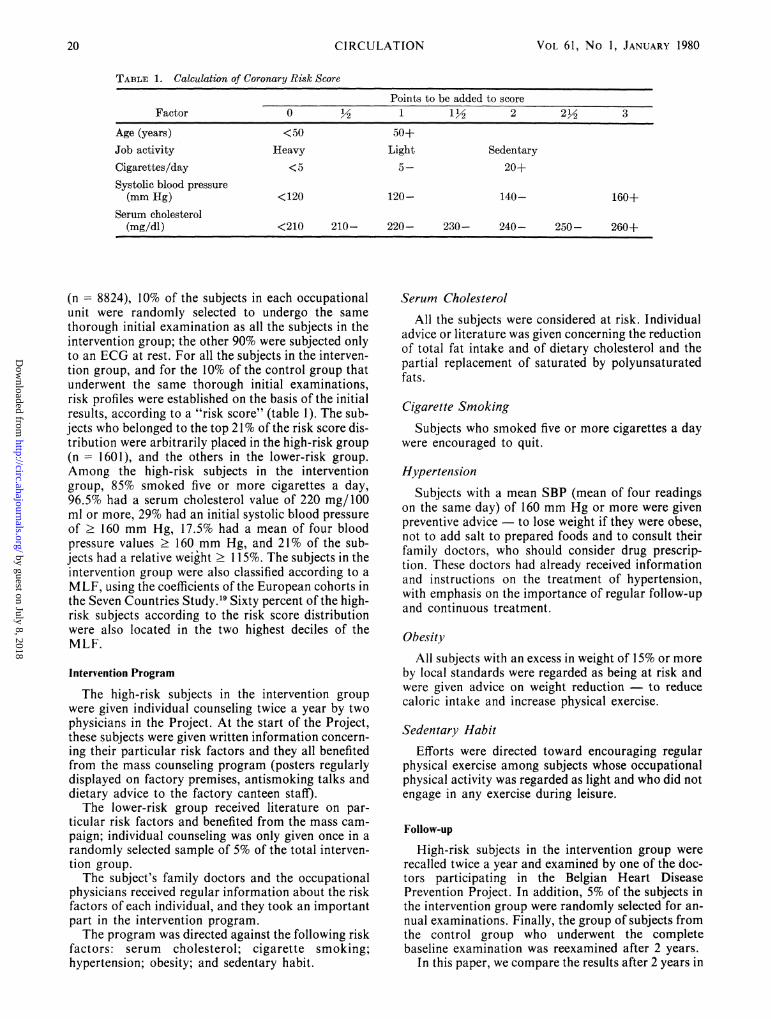
YearS 2FIGURE 2. Modification of systolic blood pressure; on theleft ordinate the mean baseline values, on the right ordinatethe mean values after 2 years. Statistics show the differencebetween control and intervention groups at 2 years.
subjects from the random sample of the interventiongroup with values in the random sample of the controlgroup (hereafter referred as the "random samples");we also compare the results of the high-risk subjects ofthe intervention group with the results of the high-risksubjects of the control group (hereafter referred as the"HR subjects").
SERUM CHOLESTEROL
0 Years 2FIGURE 3. Modification of serum cholesterol; on the leftordinate the mean baseline values, on the right ordinate themean values after 2 years. Statistics show the differencebetween the control and intervention groups at 2 years.
ResultsFigure 2 shows the changes in SBP. For the HR
subjects the mean SBP drop was 3.4% in the controlgroup and 7.8% in the intervention group; thedifference between the groups was statistically signifi-cant. The 3.4% drop among the HR subjects in thecontrol group probably reflects a regression towardthe mean and the effects of treatment in some controlsubjects whose high blood pressure was being treatedin any case; if this 3.4% drop is subtracted from the7.8% observed in the intervention group, there is still anet difference of 4.4%. This difference is in part relatedto treatment and in part influenced by repeated bloodpressure measurements in the high-risk interventiongroup, the so-called pressor effect.20 For the randomsamples we observed no change in the control groupand a drop of 4.7% in the intervention group.
Figure 3 shows the changes in serum cholesterolafter 2 years. For the HR subjects, there was an in-crease of 0.4% in the control group and a drop of 3.9%in the intervention group, the difference between thegroups being statistically significant. For the randomsamples, there was a 4.3% increase in the controlgroup and a 1% increase in the intervention group, thenet difference being statistically significant. The factthat there was no regression towards the mean amongHR subjects in the control group is explained in theMethods section.
The 4.3% increase in the random sample of the con-trol group is explained partly by the laboratory driftand partly by a normal increase with age. At allevents, since the laboratory error affected both thecontrol group and the intervention group, and sincethe blood samples were obtained from each controlfactory and each intervention factory in the samemonth, the observed difference in cholesterol changebetween the two groups can be ascribed to the in-tervention program.
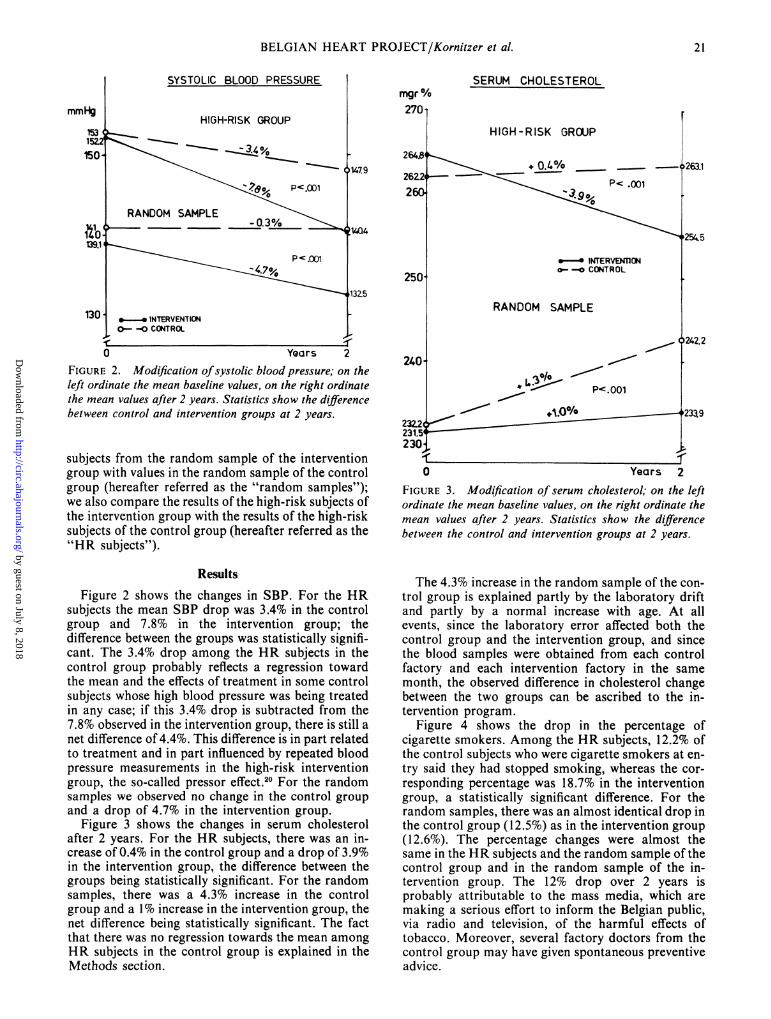
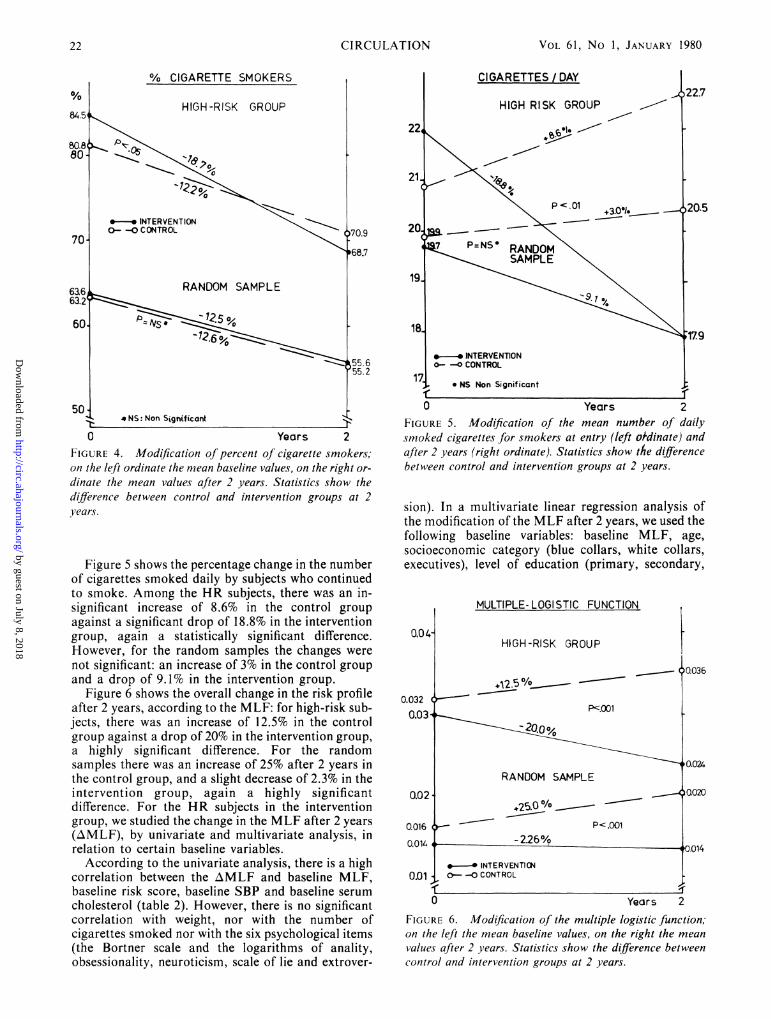
Figure 4 shows the drop in the percentage ofcigarette smokers. Among the HR subjects, 12.2% ofthe control subjects who were cigarette smokers at en-try said they had stopped smoking, whereas the cor-responding percentage was 18.7% in the interventiongroup, a statistically significant difference. For therandom samples, there was an almost identical drop inthe control group (12.5%) as in the intervention group(12.6%). The percentage changes were almost thesame in the HR subjects and the random sample of thecontrol group and in the random sample of the in-tervention group. The 12% drop over 2 years isprobably attributable to the mass media, which aremaking a serious effort to inform the Belgian public,via radio and television, of the harmful effects oftobacco. Moreover, several factory doctors from thecontrol group may have given spontaneous preventiveadvice.
-i
21
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 61, No 1, JANUARY 1980
% CIGARETTE SMOKERS
0 Years 2FIGURE 4. Modification of percent of cigarette smokers;on the left ordinate the mean baseline values, on the right or-dinate the mean values after 2 years. Statistics show thedifference between control and intervention groups at 2years.
Figure 5 shows the percentage change in the numberof cigarettes smoked daily by subjects who continuedto smoke. Among the HR subjects, there was an in-significant increase of 8.6% in the control groupagainst a significant drop of 18.8% in the interventiongroup, again a statistically significant difference.However, for the random samples the changes werenot significant: an increase of 3% in the control groupand a drop of 9.1% in the intervention group.
Figure 6 shows the overall change in the risk profileafter 2 years, according to the MLF: for high-risk sub-jects, there was an increase of 12.5% in the controlgroup against a drop of 20% in the intervention group,a highly significant difference. For the randomsamples there was an increase of 25% after 2 years inthe control group, and a slight decrease of 2.3% in theintervention group, again a highly significantdifference. For the HR subjects in the interventiongroup, we studied the change in the MLF after 2 years(AMLF), by univariate and multivariate analysis, inrelation to certain baseline variables.
According to the univariate analysis, there is a highcorrelation between the AMLF and baseline MLF,baseline risk score, baseline SBP and baseline serumcholesterol (table 2). However, there is no significantcorrelation with weight, nor with the number ofcigarettes smoked nor with the six psychological items(the Bortner scale and the logarithms of anality,obsessionality, neuroticism, scale of lie and extrover-
0 Years 2FIGURE 5. Modification of the mean number of dailysmoked cigarettes for smokers at entry (left ordinate) andafter 2 years (right ordinate). Statistics show the differencebetween control and intervention groups at 2 years.
sion). In a multivariate linear regression analysis ofthe modification of the MLF after 2 years, we used thefollowing baseline variables: baseline MLF, age,socioeconomic category (blue collars, white collars,executives), level of education (primary, secondary,
0.04-
0.0320.03
0.02.
0016
0.014
0.01
MULTIPLE- LOGISTIC FUNCTION
HIGH-RISK GROUP
pZ.001
RANDOM SAMPLE
'25.CO/0P<.001
- 2.26%
[ .-. INTERVENTICN0- -0 CONTROL
0
FIGURE 6. Modification of the multiple logistic function,on the left the mean baseline values, on the right the mean
values after 2 years. Statistics show the difference betweencontrol and intervention groups at 2 years.
0036
0.024
0020
0.014
, ,Years 2
22 CIRCULATION
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

BELGIAN HEART PROJECT/Kornitzer et al.
TABLE 2. Correlation Coefficients of Baseline Variables with Multiple Logistic Function Modification (AMLF)at 2 Years
High-risk subjects - Intervention group
MLF Risk score Serum cholesterol SBP Weight Cigarettes/day-0.64* -0.19* -0.31* -0.40* -0.03 0.05
Bortner scale S.H.-E.P.I. lnA lnB lnN E lnL-0.06 -0.03 0.02 -0.03 -0.01 -0.06
*p <.0.001.Abbreviations: ln = natural logarithm; SBP = systolic blood pressure.
university), marital status (married vs others), place ofresidence (Wallonia vs other parts of Belgium),changes in eating habits (reduction in fat intake vs theothers), Bortner scale (behavior type A or B), Ln ofscore A (anality), Ln B (obsessionality), Ln N(neuroticism), E (extroversion) (table 3). There is asignificant correlation with baseline MLF, age andplace of residence: Subjects with the highest baselineMLF show the greatest drop, the youngest subjectsshow a greater drop than the older subjects, and thesubjects residing in the French-speaking part ofBelgium show a more significant drop than thoseresiding in the north or Dutch-speaking part of thecountry.
DiscussionThe Belgian Heart Disease Prevention Project has
produced a prevention strategy which, if successful,could be applied by any occupational medical service,subject to minor modification. We considered that asuccessful multifactorial prevention trial that achieveda significant drop in the incidence of IHD would havebeen frustrating if it had been too costly andsophisticated, i.e., not applicable to a larger group ofmale, middle-aged workers. Face-to-face counselingwas given by two doctors engaged in the Project to21% of subjects who had the highest coronary risk ineach intervention factory as defined by a coronary riskscore. Each subject was recalled twice a year. Thetotal time devoted to each high-risk subject in the in-tervention group (including screening) was 1 hour inthe first year and 30 minutes per year thereafter. Themass media approach included use of posters, printedinformation, a conference on smoking and changes inthe canteen menus. Only the last item required a part-time dietician. Since we wanted to find out the trend ofthe coronary risk profile in the population, a randomsample of the total group was reexamined, includingalso high-risk subjects who had received individualcounseling. Comparison of the HR group with the
random sample (in the intervention group) shows thatfor blood pressure, the results were satisfactory andidentical when compared with the respective controlgroups; for serum cholesterol the results were betterfor the HR group than for the random sample; forcigarette smoking, only the HR group showed afavorable trend, and finally, for the total risk profile, afavorable trend appeared in both the random sampleand the HR group, although the difference in relationto the control group was distinctly greater for thelatter.The Stanford Three Communities Study10-12 was
started in 1972. This study involved health educationvia mass media and face-to-face counseling in twocommunities with a third serving as control. Resultswere reported on subjects of both sexes, ages 35-59years. The Stanford Study differed from ours in thatboth sexes were involved and that complete, urbanpopulations were studied, whereas we studied only40-59-year-old male industrial workers. On the otherhand, the Stanford Study, like the Belgian Project,was based on multifactorial prevention and also in-cluded individual counseling in a high-risk group ofsubjects defined by the two highest deciles of risk usinga MLF.
Table 4 compares the results of the Stanford studywith those of the Belgian Heart Disease PreventionProject after 2 years. We have used only the figures forWatsonville, where the high-risk subjects were sub-jected mainly to face-to-face counseling, whereas therandom sample was subjected to mass media; the con-trol community was the town of Tracy. For serumcholesterol there was a drop of 5 mg/100 ml in thecase of the high-risk subjects in the Stanford study,whereas the drop was 11.2 mg/100 ml in the Belgiansample. For the Stanford random sample, the dropwas 5.6 mg/100 ml, but was 7.6 mg/lOOml in theBelgian study. Thus, in the case of serum cholesterol,our study seems to obtain better results over 2 years.As for SBP, the drop over 2 years was substantiallythe same in both studies, both for the high-risk sub-
TABLE 3. Multivariate Analysis of Multiple Logistic Function (MLF) Modification at 2 Years
High-risk subjects - Intervention groupVariables Coefficients r r2 F p
Baseline MLF -0.52 0.52 0.27 238.40 0.001Age (years) 5.02 0.58 0.34 70.48 0.001
Geographic region 11.81 0.61 0.37 31.05 0.001
23
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 61, No 1, JANUARY 1980
TABLE 4. The Stanford Three Communities Study vs the Belgian Heart Disease Prevention Project Results at2 Years
Watsonville vs Tracy Belgian Heart ProjectHigh-risk Random sample High-risk Random sampleI vs C I vs C I vs C I vs C
Serum cholesterol (mg/dl) -5. -5.6 -11.2 -7.6
Systolic blood pressure (mm Hg) -6. -5.6 -7.5 -6.
Cigarette smokers (%) -37. -21. -6.5 +0.1
Cigarettes/day f%) -27. -12.1
Multiple logistic function (%l ) -28. -20.6 -32.5 -27.3
Abbreviations: I = intervention; C = control.
jects and for the random samples. Regarding theproportion of cigarette smokers, difference in per-centage of those who quit was distinctly greater in theStanford study (37% for high-risk subjects and 21%for the random sample); in the Belgian study, the cor-responding figures were 6.5% and 0.1%. As for thedrop in the number of cigarettes smoked daily, theresults were also better in the Californian compared tothe Belgian study.
Finally, in regard to the overall change in the cor-onary risk profile, expressed in terms of the MLF, theresults were very similar for the HR subjects in thetwo studies, whereas for the random samples, resultsafter 2 years were somewhat better in the Belgianstudy. In summary, the change in the overall riskprofile seems to be substantially the same in theBelgian and Stanford studies; smoking seems to play apredominant role in the results of the Stanford study,whereas the drop in serum cholesterol plays an impor-tant role in the Belgian results.The authors of the Stanford Three Communities
Study did not perform a multivariate analysis of thechange in risk profile in relation to baseline psycho-socio-biochemical data, so we cannot make a com-parison there. The three items that influencesignificantly and independently the change in the MLFof the HR subjects in the Belgian Project are, in orderof importance: baseline MLF, age and place ofresidence. In the case of the baseline MLF, part of thedrop is probably accounted for by the regressiontoward the mean. Another explanation is that the sub-jects with the highest risk profile made the biggest im-pression on the doctors involved in health education,and that they in their turn produced more compellingarguments and invested greater conviction in theirefforts to modify the risk factors. The fact that theyoungest subjects responded more favorably to healtheducation is extremely encouraging, since it isprobably they who will benefit most from the drop inrisk for IHD. Finally, the fact that the Walloonsresponded better to health education than theFlemings or Brussels citizens is probably accountedfor by sociocultural or psychological items not con-sidered at the baseline examination and therefore notanalyzable.
We believe it is important that health education hasthe same effect in all the socio-economic categories:The face-to-face technique seems to convince white-and blue-collar workers as well as it does executives.
References1. Christakis G, Rinzler SH, Archer M, Kraus A: Effect of the
anti-coronary club program on coronary heart disease risk fac-tors status. JAMA 198: 129, 1966
2. Miettienen M, Turpeinen 0, Karvonen MJ, Elosuo R,Paavilainen E: Effect of cholesterol-lowering diet on mortalityfrom coronary heart disease and other causes. Lancet 2: 835,1972
3. Dayton S, Pearce ML, Hashimoto S, Dixon WJ, Tomiyasu U:A controlled clinical trial of a diet high in unsaturated fat inpreventing complications of atherosclerosis. Circulation 40(suppl II): II-11, 1969
4. Veterans Administration Cooperative Study Group on Anti-hypertensive Agents: Effects of treatment on morbidity inhypertension. II. Results in patients with diastolic bloodpressure averaging 90 through 114 mm Hg. JAMA 213: 1143,1970
5. Rose G: Smoking cessation in high-risk subjects. Health 12: 19,1975
6. Wilhelmsen L, Tibblin G, Werko L: A primary preventivestudy in Gothenburg, Sweden. Prev Med 1: 153, 1972
7. Leren P, Askevold EM, Foss OP, Froili A, Grymyr D,Helgeland A, Hjermann I, Holme I, Lund-Larsen PG, NorumKR: The Oslo Study - Cardiovascular disease in middle-agedand young Oslo men. Acta Med Scand 588 (suppl 588): 588,1975
8. The Multiple Risk Factor Intervention Trial (MRFIT): Anational study of primary prevention of coronary heart disease.JAMA 235: 825, 1976
9. Puska P. Koskela K, Pakarinen H, Puumalainen P, SoininenV, Tuomilehto J: The North Karelia Project: a programme forcommunity control of cardiovascular diseases. Scand J SocMed 4: 57, 1976
10. Farquhar JW, Wood PD, Breitrose H, Haskell WL, Meyer AJ,Maccoby N, Alexander JK, Brown BJ, McAlister AL, NashJD, Stern MP: Community education for cardiovascularhealth. Lancet 1: 1192, 1977
11. Haskell WL, Stern MP, Wood PD, Brown WB, Farquhar JW,Maccoby N: Multifactor education campaign to reduce car-diovascular risk in three communities: physiological results.Circulation 50 (suppl III): 111-101, 1974
12. Meyer AJ, McAlister A, Nash J, Maccoby N, Farquhar JW:Maintenance of cardiovascular risk reduction: results in highrisk subjects. Circulation 54 (suppl II): 887, 1976
13. World Health Organization European Collaborative Group:An international controlled trial in the multifactorial preven-tion of coronary heart disease. Int J Epidemiol 3: 219, 1974
CIRCULATION24
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

BELGIAN HEART PROJECT/Kornitzer et al.
14. De Backer G, Kornitzer M, Thilly C, Depoorter AM: TheBelgian multifactor preventive trial in CVD -design andmethodology. Hart Bulletin 8: 143, 19i7
15. Eysenck HJ: Manual for the Eysenck personality inventory.Eduqational and indiistrial testing service, San Diego, Califor-nia 9: 2107, 1968
16. Sandler Y, Hazari A: The obsessional: on the psychologicalclassification of obsessional character traits and symptoms. BrJ Med Psychol 33: 113, 1960
17. Bortner RJ: A short rating scale as a potential measure ofpattern A behavior. J Chronic Dis 22: 87, 1969
18. Rosenman RH, Friedman M, Straus R, Wurm M, KositchekR, Hahn W, Werthessen NT: A predictive study of coronaryheart disease. The Western Collaborative Group Study. JAMA15: 189, 1964-
19. Keys A, Aravanis C, Blackburn HW, Van Buchem FS, FusinaR, Djordjevic BS, Fidanza F, Karvonen MJ, Menotti A, PudduV, Taylor HL: Probability of middle-aged men developing cor-onary heart disease in five years. Circulation 15: 77, 1972
20. Sutherland I: Estimates of pressor effect and regression towardsthe mean in the intervention study. Hart Bulletin 2: 68, 1977
AppendixStaff members of the Belgian Heart Disease Prevention Project:
PromotorsM. Graffar, M.D. (Director of the Laboratory of Epidemiology
and Social Medicine, University of Brussels); K. Vuylsteek, M.D.(Director of the Laboratory of Hygiene and Social Medicine, StateUniversity of Ghent); R. Pannier, M.D. (Director of the Depart-ment of Internal Medicine, Sect. Cardiology, State University ofGhent); J. Lequime, M.D. (Director of the Laboratory of Car-diological Research, University of Brussels).
Directors
G. De Backer, M.D. (bevoegdverklaard navorser, NationaalFonds voor Wetenschappelijk Onderzoek); M. Kornitzer, M.D.(Laboratory of Epidemiology and Social Medicine, University ofBrussels); C. Thilly, M.D. (Laboratory of Epidemiology and SocialMedicine, University of Brussels).
Occupational Units Recruitment
G. De Backer, M.D. and M. Kornitzer, M.D.
Screening
F. Callenaere, M. de Maesschalck, J. Debaille, J. S. Van derAuwera, R. Vandewalle, W. Van Hove, M. Vleminckx.
Data Analysis and Central AdministrationC. Thilly, M.D. (in charge); Secretary and codification: 0. De
Dycker, H. Gheyssens, A. Van Hemeldonck. Programmation: L.Ravet-Ramioul, M. Dramaix-Wilmet.
Prevention
G. De Backer, M.D. (in charge); M. De Smet, M.D., M. Kor-nitzer, M.D., G. Versele, M.D. Secretary: F. Gobert, P. Claus, C.Ghijsbrecht.
Follow-up
M. Kornitzer, M.D. (in charge); L. Berghmans, M.D., C. Remy,M.D. Secretary: N. Ariel. Independent referee: M. Englert (HeadDepartment of Cardiology, St. Pierre hospital, Brussels)
Psychosocial AspectsC. Degre, F. Kittel, R-M. Rustin, C. Dumon.
Laboratory
A-M. Depoorter, M.D. (in charge); H. Devos.
Occupational Physicians Collaborating at the TrialL. Baeyens, M.D., P. Bioul, M.D., Z. Bourda, M.D., A.
Danthine, M.D., M. Demeyere, M.D., J. De Schrijver, M.D., D.Dewever, M.D., J. Deyaert, M.D., H. Dewulf, M.D., P. Dothee,M.D., J-B. Elskens, J.D., L. Hermans, M.D., P. Laloux, M.D.,M-J. Lefebvre M.D., G. Lescouhier, M.D., W. Meiresonne, M.D.,C. Nicaise, M.D., M. Oversteyns, M.D., J-P Pepersack, M.D., M.Rogowski, M.D., J. Stevens, M.D., P. Stiernet, M.D., 0.Vanhauwaert, M.D., P. Van Hecker, M.D., E. Van Oostende,M.D., T. Van Peteghem, M.D., M. Vermeulen, M.D., A. Vincke,M.D., A. Vos, M.D.
AcknowledgmentThis trial was made possible by generous support of the Caisse
Generale d'Epargne et de Retraite, S.A. Continental Pharma,Societ6 Gen&ale de Belgique, S.A. Vandermoortele, UnionProfessionnelle des Entreprises d'Assurances.
25
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

M Kornitzer, G De Backer, M Dramaix and C Thillyan industrial population.
The Belgian heart disease prevention project. Modification of the coronary risk profile in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.61.1.18
1980;61:18-25Circulation.
http://circ.ahajournals.org/content/61/1/18the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from