Behavioural Supports Ontario (BSO)/media/sites/sw... · Kaizen events produce an array of tools and...
42
Behavioural Supports Ontario (BSO) Presented to: Southwest LHIN – Quality Symposium Presented by: Bernie Blais, BSO Project Sponsor & CEO North Simcoe Muskoka LHIN Dr. Lisa VanBussel, St. Joseph’s Health Care, London Thursday, May 31, 2012
Transcript of Behavioural Supports Ontario (BSO)/media/sites/sw... · Kaizen events produce an array of tools and...

Behavioural Supports Ontario (BSO)
Presented to: Southwest LHIN – Quality Symposium
Presented by: Bernie Blais, BSO Project Sponsor & CEO North Simcoe Muskoka LHIN Dr. Lisa VanBussel, St. Joseph’s Health Care, London
Thursday, May 31, 2012

2
a changing reality (video presentation)

3
reflectionis this what we’ve come to accept... to expect
what if this was your mother… your father… someone close to you… someone you love… someone who loved and cared for you in return…
or someone you don’t even know
what if we don’t change reality?

nice to meet you
4

objective
Provide provincial and local overviews of strategies deployed - by the Ministry ofHealth and Long Term Care (MOHLTC), Alzheimer Society of Ontario (ASO), HealthQuality Ontario (HQO) and LHINs - to improve the lives of older adults withresponsive behaviours - verbal, physical, or sexual aggression, wandering, agitationet.al. - associated with dementia, mental health and addictions issues and otherneurological disorders, their families and caregivers.
5

agenda changing reality
the local perspective
the provincial picture
better health, better care, better value
continuing our discussion
6

the local perspectivequality improvement in the south west LHIN
7

the local perspective
8
background Demographic change
• By 2021 18% of Canadians will be > 65yrs of age; 45% of this group may be > 85 yrs
Significant impact of mental illness on seniors and their families• Mental health problems in late life usually occurs in context of medical illness, disability
and > range of psychosocial issues.

the local perspective
9
aging at home
In the Fall of 2009, 31 partners from across the LHIN, were challenged to submit a business case to describe what a “coordinated system of care for seniors with behavioural challenges” would look like.
They needed to meet 3 objectives…
Improve the health of the defined population Enhance the care experience (including quality, access and reliability) Reduce or at least control the per capita cost of care.
they succeeded… and so… the journey began!

the local perspective
10
emerging themes | aging at home
Greater system integration Local accountability and engagement across care partners Meaningful for the person, families and caregivers Practice to action LHIN wide collaboration Capacity Building and Education was needed (health promotion).

the local perspective
11
the problem… finding solutions
It is time for a new paradigm, one that views older adults as active participants in an ageintegrated society and as active contributors as well as beneficiaries of development.
- Kalache, 2006
"The Situation is distorted when the Population is defined as the Problem… Rather theProblem is best defined as those factors which have created the gulf between the needsof the population and the approaches to address these needs.”
- Cohen

the local perspective
12
behavioural support system of care | leveraging new and existing resources… 2010/11
BSS – 2010/11 ~ $3 M AAH funding allocated to create a LHIN wide system of care SJHC (LHIN wide coordination – project lead, evaluation) Schedule 1 Hospitals (GBHS, HPHA, LHSC (STEGH), WGH) to create or expand
existing mobile Seniors Mental Health and Addictions Response teams for older adults experiencing responsive behaviours in LTCHs and/or community
Enhanced Psychogeriatric Resource Consultants OTN in LTCHs.

the local perspective
13
top down… bottom up
Establishment of LHIN-wide Steering Committee Memorandum of Agreement - SJHC and Schedule 1s Geriatric Cooperatives - mandate is to build local capacity to address responsive
behavior's where people reside to enable them to be connected to the current community support system. To coordinate, leverage and improve accountability of the existing geriatric mental health and addiction services, crisis services, day programs, hospitals and community partners within each community.

14

the local perspective
15
learning from within and… learning from outside
Evidence informed practice Person centered team based service learning Not an expert model but is a shared learning model Common language and consistency when appropriate Inter-professional and inter-organizational.

16

the local perspective
17
behavioural support system of care | leveraging new and existing resources… 2011/122011/12 ~$3 M Provincial BSO funding combined with AAH $3M LHIN-wide Project Lead Dedicated LHIN-wide Evaluation and QI resources for monthly reporting from HSPs
to Steering Committee/LHIN/CRO 5 Mobile Teams – BSO LTCH resources attached to the teams through a purchase
of service agreement with “host” LTCH 4 EPRCs for skill building (North, Central, South, LHIN-wide LHIN-wide dedicated Specialists – Geriatric Psychiatrist, Psychologist Enhanced Social Work Services OTN – 38/78 LTCHs, clinical and protocol training beginning 78 Long Term Care Homes Overnight Respite in Adult Day Programs.

the local perspective
18
quality improvement & relationship building
Value Stream Mapping ( 2 day event, Nov 2011)• Client value statement “I am a unique individual who wants to live fully with
meaning and dignity through my life journey” Kaizen event (Change for the better ) -May 24, 25, 2012 QI Facilitator (to be hired June, 2012) Collaborative working groups (QI ) - Mobile teams, Intake and access, Standardized
assessment tools and Education Consortium

the local perspective
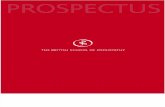
0 5 10 15 20 25 30 35
Woodingford Lodge - Woodstock (09/14/2011)
Woodingford Lodge - Tillsonburg (09/14/2011)
Woodingford Lodge - Ingersoll (09/14/2011)
The Maples Home for Seniors (11/17/2011)
Rockwood Terrace (11/30/2011)
Ritz Lutheran Villa (11/23/2011)
PeopleCare - Tavistock (11/11/2011)
PeopleCare - Oakcrossing (10/18/2011)
Mitchell Nursing Home (11/23/2011)
Meaford Long Term Care Centre (08/31/2011)
McCormick Home (02/15/2012)
Lee Manor Home for the Aged (08/29/2011)
Dearness Home (02/24/2012)
Caressent Care -Mary Bucke (12/16/2011)
Caressant Care - Woodstock (12/19/2011)
Caressant Care - Bonnie Place (11/11/2011)
Long
Term
Car
e Ho
mes
(wit
h liv
e si
te d
ate)
Long Term Care Homes - UtilizationSeptember 1 2011 - Feb 29 2012
Clinical Direct Clinical Indirect Education Administrative
learning to work differently - OTN

the local perspective
20
where are we going?
Change management strategy Improve access to care and transitions of care Solution focused across teams and finding the right balance Engaging and supporting primary care Communication strategy Person-centred team-based service- learning.

BEHAVIOURAL SUPPORTS ONTARIO PROJECT

successful aging
“A state wherein an individual is able to invoke adaptive psychological and social mechanisms to compensate for physiological limitations to achieve a sense of well being, high self-assessed quality of life , and a sense of personal fulfillment even in the context of illness and disability.”
- Bowling and Dieppe , 2005
the local perspective
22

the provincial picture cultural change and BSO
23

the provincial picture
24

current state… a changing reality Local seniors across the province are starting to see changes in how care is provided in long-term care
homes, hospitals and the community. Through the Behavioural Supports Ontario (BSO) Project new services, programs and training are now being introduced to provide appropriate care and support for an increasing number of seniors across Ontario and their families and caregivers, who live and cope with dementia, mental illness and/or other neurological conditions.
First announced by the province last August, BSO represents a comprehensive system redesign that has successfully broken down barriers, encouraged collaborative work, shared knowledge and fostered partnerships among local, regional and provincial agencies. The result is a cultural transformation; a new way of thinking, acting and behaving.
To date, more than 300 new front-line staff have been hired across the province, over 310 long-term care homes have increased their in-house behavioural supports, and upwards of 4,000 new and existing front-line staff have received specialized training in techniques/approaches applicable to behavioural supports.
the provincial picture cont’d…
25

principles for cultural and/or systemic change
Move toward a new vision, fundamentally different and better than the status quo Identify / communicate key themes that a) will have big impact and b) people can relate to Multiples of things (‘lots of lots’) Frame issues in ways that engage and mobilize the imagination, energy and will of a large
number of diverse stakeholders; create a shift in the balance of power and distribute leadership
Reinforce change across multiple processes/subsystems Continual refresh of “the story”; attract new, active supporters Emergent planning and design, based on monitoring progress and adapting as you go Many people contribute to the leadership of change, beyond organizational boundaries Transform mindset and lead to inherently sustainable change Maintain and refresh the leaders’ energy over the long haul.
the provincial picture cont’d…
26

At the core of the project is creating a system that ensures people are treated with dignity and respect in an environment that supports safety for all and is based on QUALITY, evidence-based, patient-centredcare and practice.
the provincial picture cont’d…
QualityAccessible
Effective
Safe
Patient-Centered
EquitableEfficient
Appropriately Resourced
Integrated
Focused on Population
Health
quality at the core
27

a partnership for cultural / systemic change Health care has been traditionally dominated by sector and silo approaches Sustainability requires an integrated system approach to transform system performance,
resource utilization and quality outcomes Improved system effectiveness and quality of care are the goals of an integrated
approach Partnerships, collaboration and coordination at multiple levels are fundamental building
blocks (both provincially and locally) BSO builds on existing program investments (for seniors, care transitions, Emergency
Room/Alternate Level of Care, etc.) to maximize the benefits for older adults and their caregivers
BSO is not a “new service” it has become the catalyst for system-wide transformation.
the provincial picture cont’d…
28

the BSO formulaA unique, LHIN rollout approach is proving to be one of the project’s great strengths:
Thorough research and consultation produced a “Framework for Care” to guide system redesign and cultural change - panel of experts acted as reference on specific questions
4 Early Adopter LHINs first to implement, then share experiences with remaining 10 LHINs through “buddy system” approach
Up-front investments in quality improvement training set the stage for change Persons with lived experience were engaged throughout the planning, implementation
and evaluation processes Commitment to knowledge transfer events, organization and e-tool Team building: mobilize and engage across the system Formal evaluation of outcomes.
the provincial picture cont’d…
29

provincial partnership structure
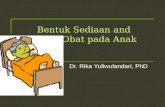
the provincial picture cont’d…
30

collective wisdom and collaboration
the provincial picture cont’d…
Early Adopter LHIN 9LHIN Project Lead
LHIN Steering CommitteeProject Working Group
4 LHIN Early Adopter Steering Committee (SC)
Early Adopter LHIN 4LHIN Project Lead
LHIN Steering CommitteeProject Working Group
Early Adopter LHIN 12LHIN Project Lead
LHIN Steering CommitteeProject Working Group
Early Adopter LHIN 10LHIN Project Lead
LHIN Steering CommitteeProject Working Group
Coordination and Reporting Office (CRO)Project Management
Health Quality Ontario (HQO)
* Quality Improvement Guidance* Coordination between BSS and other related local QI initiatives* System alignment * QI Evaluation/ measurement
Provincial Resource Team (PRT)
* Resource and Advisory
Quality Improvement Teams
LHIN 6
LHIN 7
LHIN 1
LHIN 2
LHIN 3
LHIN 5
LHIN 8
LHIN 11
LHIN 13
LHIN 14
Alzheimer Knowledge Exchange (AKE)
Communication and Knowledge Dissemination
31

the provincial picture cont’d…
32
Primary Care (in Community and in Long Term Care) Collaborative Working Group
Centralized Intake Collaborative Working Group
Mobile Support Teams (Community and Long Term Care) Collaborative Working Group
Behavioural Su pport Units (transitional)

the provincial picture cont’d…
collaborative working groups Collaborative Working Groups initiated early in 2012 (align with key change ideas)
While the intent of the Collaborative Working Groups is to learn collectively, local context is reflected and there is no requirement to produce a single “provincial solution”
Kaizen events produce an array of tools and processes for each change idea (Each element constitutes a “ramp” of Plan-Do-Study-Act (PDSA) cycles i.e., at any given time, up to 79 concurrent pieces of improvement work can be moving BSO toward achieving its aim.)• Primary Care Toolkit - 8 elements• Centralized Intake - 7 elements• Mobile Support Team - 16 elements• Behavioural Support Units - 21 elements• Common Assessment Toolkit - 27 elements
Collaborative Working Group Lead LHIN Participating LHINs ESC SW WW HNHB CW MH TC C CE SE CH NSM NE NW
Primary Care HNHB Centralized Intake NSM
Mobile Teams SE Behavioural Support Units MH
33

primary care collaborative Primary Care toolkit (created by HNHB)
The Primary Care Toolkit was established to provide guidance to clinicians so that they can provide comprehensive care to patients with Mild, Moderate or Severe Responsive Behaviours. It was tested by HNHB in January 2012, with recommendations for specific circumstances for optimal use.
• Safety Checklist Assessment• Behavioural Assessment Tool• Caregiver Burden Assessment • Potentiating Factors Checklist• Cognitive Assessment Tools• Functional Assessment Tools• Laboratory Investigations• Treatment/Management
34
the provincial picture cont’d…


36
the provincial picture cont’d…
centralized intake and mobile teams collaborative Referral, Intake and Triage Mobile Support Team Care (community) Mobile Support Team Care (LTCH) Transition from Mobile Support Team Primary Care toolkit (created by HNHB)
behavioural supports unit collaborative Determine eligibility to SBSU Admission to SBSU Care in SBSU (transitional) Discharge Planning Admission to LTC (following SBSU discharge) Summary of development and testing by LHIN

the provincial picture cont’d…
37
Phase 1:Consultative - develop the Framework for Care
Phase 2:Implement the Framework in 14 LHINs
Pillar 1:System Coordination
Pillar 2:Interdisciplinary Service Delivery
Pillar 3:Knowledgeable Care Team and Capacity Building
the Behavioural Support System

Knowledge Exchange & Training
HQO led Kaizen and VSA improvement events pan-LHIN
7 oversight committees / working groups providing subject matter expertise
4 pan-LHIN collaborative working groups
14 Improvement Facilitators trained
Over 3800 new and existing front-line staff trained
38
better health, better care, better valueFunding & Resources
$40M invested to hire and train new resources/staff
$3.6M invested on service redesign
Over $2.6M in LHIN funding from non-BSO sources
Over 13000 volunteer hours from more than 600 HSPs
12 standardized core competencies and job descriptions
Quality
Over 30 intersectoral system redesign and improvement initiatives
14 Action Plans approve and now in the process of being implemented
Over 310 LTCHs with enhanced in-house behavioural supports
14 LHINs with BSO Outreach teams
5 LHINs indicating BSU implementation

Knowledge Exchange & Training
Mutually reinforcing change across multiple processes/subsystems
39
better health, better care, better valueFunding & Resources
Capacity Building Roadmap distributed to LTCHs
Over 350 new health care staff hired to date
Quality
Reported reduced length of stay of LTC clients in hospital
Timely access to the right services
Consistent client and family education (e.g. prevent premature placements)
Integrate best practices and learning's for better quality care

40
the patient perspective… Mary’s story
better health, better care, better value

41
smiling is infectious and so is BSO
better health, better care, better value

“You matter because you are you; and you matter to the last moment of your life. Wewill do all we can to help you, not only to die peacefully but to live until you die.”
- - Saunders, 1976
- let’s continue our conversation…questions?
thank you