
Behaviour change: Taylor et al sociocultural review tables ...
71
APPENDICES Appendix 1 The social determinants and economics of public health 116 Appendix 2 Critical Appraisal Tool 127 Appendix 3 Search strategy 129 Appendix 4 Report bibliography 131 Appendix 5 Flowchart of papers identified, received and screened 134 Appendix 6 Data extraction fields 135 Appendix 7 Evidence tables 136 Appendix 8 References of reviewed paper 180 115
Transcript of Behaviour change: Taylor et al sociocultural review tables ...
APPENDICES
Appendix 1 The social determinants and economics of public health 116
Appendix 2 Critical Appraisal Tool 127
Appendix 3 Search strategy 129
Appendix 4 Report bibliography 131
Appendix 5 Flowchart of papers identified, received and screened 134
Appendix 6 Data extraction fields 135
Appendix 7 Evidence tables 136
Appendix 8 References of reviewed paper 180
115
APPENDIX 1: The social determinants and economics of pubic health
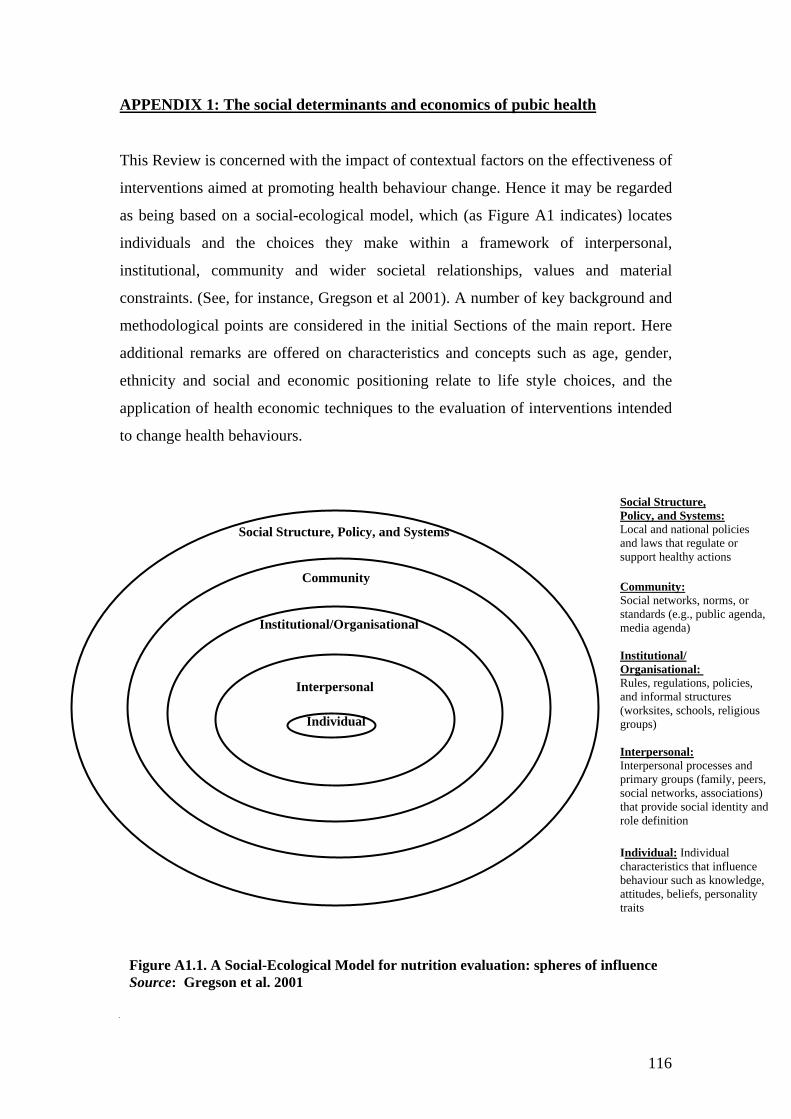
This Review is concerned with the impact of contextual factors on the effectiveness of
interventions aimed at promoting health behaviour change. Hence it may be regarded
as being based on a social-ecological model, which (as Figure A1 indicates) locates
individuals and the choices they make within a framework of interpersonal,
institutional, community and wider societal relationships, values and material
constraints. (See, for instance, Gregson et al 2001). A number of key background and
methodological points are considered in the initial Sections of the main report. Here
additional remarks are offered on characteristics and concepts such as age, gender,
ethnicity and social and economic positioning relate to life style choices, and the
application of health economic techniques to the evaluation of interventions intended
to change health behaviours.
Social Structure, Policy, and Systems
Community
Institutional/Organisational
Interpersonal
Individual
1.2.1 Smoking, health and class
A1. Smoking, health and class
Social Structure, Policy, and Systems:Local and national policies and laws that regulate or support healthy actions
Community: Social networks, norms, or standards (e.g., public agenda, media agenda) Institutional/ Organisational: Rules, regulations, policies, and informal structures (worksites, schools, religious groups) Interpersonal: Interpersonal processes and primary groups (family, peers, social networks, associations) that provide social identity and role definition Individual: Individual characteristics that influence behaviour such as knowledge, attitudes, beliefs, personality traits
Figure A1.1. A Social-Ecological Model for nutrition evaluation: spheres of influence Source: Gregson et al. 2001
116
A.1 Smoking, health and class
Tobacco smoking in the United Kingdom has been estimated to be responsible for in
excess of 50 per cent of the differences in premature mortality between more and less
advantaged social groups (Jarvis and Wardle 2005). Although some commentators
may believe this to exaggerate the actual contribution of smoking to health
inequalities (Marmot 2006) the habit is unquestionably hazardous and is currently at
least two or three times as prevalent in less affluent and educated groups in England
as it is amongst the better off. This is illustrated by the fact that 30 per cent of
pregnant women in the economically least advantaged quartile of the population
continue to smoke, compared to only 15 per cent of their peers in the most advantaged
quartile. This is likely to have immediate and longer-term health consequences for the
women concerned and their babies.
Reducing the prevalence of smoking therefore remains a key public health priority
amongst all socio-economic groups. However, it is important not to take a simplistic
view regarding how this should be achieved, or the extent to which individuals ought
to be judged as irresponsible if they do not behave in ways that others consider best
for their health.
For example, social disadvantage and smoking have not always be directly linked. At
a population level tobacco use classically begins amongst rich, relatively advantaged,
males and ends amongst poorer, relatively disadvantaged, females. While the smoking
pandemic is relatively advanced in the UK, such initial patterns can still be seen
elsewhere in the developing world and even in some EU member states. It is of note,
for instance, that lung cancer rates in parts of Spain (lung cancer is a key tracer
condition for tobacco related harm) are higher in better off, as opposed to less
affluent, men and women (Mackenbach et al 2004).
Further relative reductions in smoking rates in the more advantaged sections of the
UK population could well increase relative health inequalities, and hence might be
seen as undesirable by some commentators. But such a trend, were it to occur, would
not in absolute terms further disadvantage any group in society, and might in the long
117

term prove to be part of an overall trend that could ultimately result in the cessation of
the smoking habit at a total population level.
The multiple social, economic and psychological determinants of public health act at
a variety of levels over long periods, and on many occasions synergistically. Seen
from this standpoint, they need to be understood comprehensively as dynamic as
opposed to static phenomena, and not simply from the perspective of any one
disciplinary perspective. Temporary increases in inequalities may on occasions be
indicators of desirable progress. Similarly, it might also be argued that for individuals
living in stressful or risky situations immediate behavioural ‘rewards’ are often more
important than they are for those living in better – more secure and congenial –
circumstances. The latter can (not least in economic terms) rationally afford to
prioritise securing long-term rewards. The poor, by contrast, are more likely
(rationally) to apply high discount rates.
Public health improvement programmes should of course attempt to protect
individuals at the highest risk of smoking related or other causes of premature death
and disability. But such observations serve as a reminder that individuals should not
be unfairly blamed for living out the logic of their personal and group situations.
Failures to recognise such points with due sensitivity, or to respect adequately the
autonomy of individuals of all ages, could help to explain why on past occasions
‘public health’ messages and programmes have often been regarded with suspicion by
many of the people they were designed to help (Mechanic 1999). They may also
explain why approaches that focus on promoting informed behavioural choice without
also seeking to modify the structural determinants of choice – the restraints and
opportunities conferred via the social and economic contexts in which people live –
may not prove to be as effective as their instigators intend.
A.2 Social class and health
Concepts such as social class should not be used in a simplistic, potentially counter-
productive, manner. One obvious danger to avoid is that of over-generalising, and
making false assumptions to the effect that all the members of large, and in some
respects crudely defined, groups such as those which comprise the current NS
118

(National Statistics) Standard Occupational Classification are alike. In reality, health
behaviour related characteristics may frequently be more usefully seen as being
distributed on varying gradients across the whole population, rather than being
clustered in one (in some respects purely constructed) ‘class’ as opposed to another
(Graham and Kelly 2004). This is not least because the intervention needed to reduce
social gradients may well differ markedly from those designed to ‘lift’ individuals
from one class to another.
Understanding why harmful habits such as smoking, harmful alcohol consumption
and/or excessive ‘junk food’ eating can be found in some members of all social
classes can on occasions be as valuable as understanding why they may be more
prevalent in the less protected/advantaged groups within a community (Blaxter 1990).
At the same time, it is also important to recognise that alternative measures of social
positioning or prestige (such as Cambridge scale, which provides a measure of
general social advantage and is based on patterns of friendship between occupational
groups’ members – Blackburn and Prandy 1997) may sometimes have more potential
to inform understanding of health behaviour variations than conventional materially
based measures.
In contexts such as diet and smoking high Cambridge scale scores are strongly linked
to healthier behaviour (Bartley et al 2000). But this relationship is not so robust in the
case of sports participation. One interpretation of these data is that – at the current
point in British history – visibly ‘unhealthy’ behaviours tend to serve (like trends in
clothing fashion, musical taste, accent and manners) as identifiers of status and rank,
at least as far as most members of the most successful – rational, and economically
and politically dominant – section of the community is concerned.
It may be postulated that only the unusually confident amongst that latter are likely to
feel able, should they wish it, to ignore such signalling systems. By contrast in other
groups (including young people at the borderline between dependence and
independence) visible habits such as smoking may still serve as markers of
membership, and shared values and identities. Such possibilities suggest that as
societies become more affluent, and their members awareness of need rises from basic
119

to more sophisticated levels, their value and stratification systems may change
radically. This will create new contextual influences on health behaviours.
A.3 Gender and health
Since the 1840s, throughout the period of British history in which accurate records
have been available, female life expectancy has consistently been greater than that of
males, by an order of five or more years. This has in all probability been in part due to
inherent biological variations (including, perhaps, factors relating to taking physical
risks) and in part to social influences. For the purposes of this Review it is of note that
gender related differences in areas such as alcohol and tobacco use and sexual risk
taking appear presently to be reducing in the UK. At the same time trends such as
increased suicide rates in young males seen during the 1990s might also have been
linked to altered gender related role expectations and opportunities. Understanding the
contextual drivers of such changes may have implications relevant to the current and
future effectiveness of health behaviour change interventions.
A.4 Ethnicity and health
Nazroo (1998) has argued that ‘un-theorised ethnicity’ can lead to false assumptions
that particular ethnic – or more crudely, racial – groups within a society are more or
less disposed to given diseases or health conditions than others. Even when disease
incidence and prevalence rates differ markedly between ethnic groups, appropriate
analyses might show that (when the relevant figures standardised for factors such as
income or access to adequate housing or sports facilities) no inherent vulnerability in
fact exists. An inadequate appreciation of this may perpetuate destructive forms of
social division and exclusion, and fragment understanding of population health as a
derivate of integrated society-wide values and functions.
This is not to deny that particular groups within the modern British community, such
as people of South Asian, African, Afro-Caribbean or Irish origin may not have
particular genetic and/or cultural characteristics and social situations (leading to, for
example, experiences of social exclusion) that influence their vulnerability to given
forms of mental or physical illness. For instance, literature examined in preparation
120

for this tertiary review is indicative of such phenomena in fields ranging from
schizophrenia (in young Afro-Caribbeans) and depressive illness (in Irish adults, and
young South Asian women) to stroke (in Afro-Caribbean adults) and diabetes and
coronary heart disease (in older South Asian adults).
Validated epidemiological observations should inform public health strategies. Yet a
significant proportion of the available US literature on ethnicity and health (which is
often focused only on African-American experience) may be taken to illustrate the
risks that ‘un-theorised’ analyses of ethnicity and health may create. On occasions
health variations that might properly be seen as either generic functions of material
and social inequality, or forms of discrimination and prejudice that are imbedded in
the wider fabric of society, still appear to interpreted as the characteristics of a
particular ‘race’ that exist independently of the behaviours of the rest of the
population (Williams et al 2003). Although the US has played a leading role in the
latter field and is in overall terms much wealthier than Britain and the rest of Western
Europe, it is relevant to note that in overall terms the health status of its population is
relatively poor – see Banks et al 2006.
A.5 Social capital and health
Social capital theory can be linked to the concept of human capital. The definition and
measurement of ‘social capital’ is a complex field (Swann and Morgan 2002, Morgan
and Swann 2004). Different writers have used the term in health related and other
contexts to refer to contrasting ideas. These range from the material and substantive
resources (such as human contacts) available to members of communities or groups to
features such as the extent to which trust and shared values exist between the actors in
social networks, or a more formal system of care and support (Hawe and Shiell 2000).
It would be inappropriate to attempt here to discuss such issues in depth. Many
authors have contributed to this area of debate, and the examination of the ways in
which social and material factors influence pathological processes. For example, it
has been argued by some American observers that loneliness (defined essentially in
terms of living in unsupportive environments) may contribute to the genesis of cardiac
121

disorders. There is also an extensive literature on the interface between depression
and schizophrenia and coronary heart disease and type 2 diabetes.
In Europe Lynch et al (1997) analysed Finnish experience, and found in the research
context of a relatively small and stable town population that poverty and psycho-
social deprivation in childhood were strongly associated with health endangering
behaviours later in life. By contrast, researchers such as Wilkinson (1996, 2006) and
Marmot (2004) have highlighted issues linked to relative as opposed to absolute
income inequalities, and the apparent impact of social status and working life control
variations on the incidence of CVD. This is observable even after known physical risk
factors have been accounted for. (See, for example, Cmnd 4386, Saving Lives: Our
Healthier Nation).
A.6 The economics of public health
The development of health economics in Britain in the 1960s and 1970s was strongly
supported by the pharmaceutical industry, in large part in relation to efforts to
encourage NHS and other health care providers to accept the costs of new medicines
for the treatment of conditions such as arthritis and peptic ulcer disease. Governments
seeking to contain health service costs, and focus health resource usage on those areas
that generate the best returns, have also supported the ongoing development of health
economics. Generic utility measures such as Quality Adjusted Life Years and
techniques such as incremental cost utility analysis have gained a particular
application in evaluating pharmaceuticals, together with surgical interventions like hip
replacements and coronary artery bypasses in the NHS and elsewhere, through the
pioneering work of agencies such as NICE (Williams 2004).
It is logical that public health intervention commissioners and practitioners should
similarly wish to be able to use (health economic) techniques to evaluate the benefits
and costs of health promotion programmes and allied interventions, both to help
ensure adequate levels of investment in preventive activities and also to make sure
that the resources available for public health improvement are used to optimal effect.
However, there are a number of barriers to be overcome in achieving this goal
(Akehurst 2006, Drummond 2006, Maynard 2006). It would be outside the scope of
122

this analysis to seek to discuss these in detail. But illustrations of the practical,
theoretical and ethical issues to be considered in this context include the following:
• inadequate data on the epidemiological impacts of health behaviour
change and allied interventions and the difficulty of conducting randomised
controlled trials of public health interventions. Without robust figures on the
effects of interventions health economic analyses cannot be undertaken. Modelling
based on incomplete information may allow economists to project a range of
possible outcomes and values that give policy makers an idea of the scale of the
possible opportunities available in areas such as exercise and dietary
improvement. But such speculative calculations are inevitably only of limited
value, particularly in politically contentious areas;
• the existence of complex synergies between public health interventions and
secular trends. These make causality difficult to attribute in relation to population
level behaviour change, and can critically affect evaluations of interventional
benefits. For example, if smoking cessation interventions are (perhaps
simplistically) seen as being responsible, when they succeed in facilitating
quitting, for the lifetime protection of former smokers from additional tobacco
related harm then they are normally regarded as highly cost effective. But were
they (perhaps more realistically) to be seen as accelerating social trends already in
motion, and hence regarded as responsible for only a few years additional
protection, then their apparent cost effectiveness would be significantly reduced;
• inter-sectorial implications. The costs and benefits of HBC and other public
health interventions are incurred and enjoyed not just within the NHS, but in
social care and many other parts of the economy. This has led some commentators
to question the extent to which approaches based on, for example, affordability
thresholds that may (or may not) appropriately be applied in relatively narrowly
used areas of health specific technology development can coherently be used in
fields which potentially effect the entire population. However, in this context it
may be noted that the presently accepted application of incremental cost utility
analysis to areas drug use also normally fails to take into account wider
123

externalities and inter-sectorial impacts, such as family welfare gains and the
employment consequences of pharmaceutical industry financial successes;
• the use of QALY’s as a measure of population level health and welfare
gains. Following on from the above, the instruments used to measure QALY
values may from a practical perspective be difficult to apply in fields which extend
beyond immediate health risk factor reduction for individuals, into positive
community health promotion and the evaluation of interventions aimed at
changing, rather than supporting the expression of, individual and group
preferences. One ethical consideration linked to this last is that people in different
social situations may rationally wish to apply different ‘personal discount rates’ to
the costs and benefits of changing life styles, and extending their chances of living
longer. Some people may have good reason to delay reward taking, while others
may have good reasons to take more immediate gains. Aggregating such
preferences in the field of public health has potential implications that are not
necessarily relevant to pharmaceutical care option appraisals. It might, for
instance, risk imposing ‘white middle class values’ on other minority groups. At a
macro economic level the issue of discounting public health improvement gains
also raises complex considerations as to the long term direction that society should
seek to take, and the extent to which the present population should be prepared to
invest in future generations’ health; and
• equity versus efficiency in the public health arena. Tensions potentially exist
between the policy objective of equalising the health of all members of a
population and that of maximising its rate of health improvement, and its
members’ average life expectancy figures. Differences in the ways health
economic calculations are undertaken in, for example, the US as opposed to the
UK, may on occasions reflect such factors, and the contrasting values of different
social groups. Such problems raise questions about, for example, the evaluation of
public health evaluations that advantage well educated and/or intellectually able
individuals more than others.
124

It therefore seems unlikely that public health evaluation techniques precisely
comparable to those currently used to decide whether, and to what extent, health care
funders should be prepared to buy new medicines will emerge in the foreseeable
future. Yet suggesting this does not imply that a further application of economic
theory and method public health policy making and relative impact measurement will
not bring additional benefits, particularly if this is combined with better biomedical,
epidemiological, psychological and sociological appreciations of the motors and
mechanisms of health behaviour change.
References
Akehurst, R. 2006, Personal communication Banks, J., Marmot, M., Oldfield, Z. & Smith, J.P. 2006, “Disease and disadvantage in the United States and in England”, Journal of the American Medical Association, vol. 295, no.17, pp. 237-245. Bartley, M., Sacker, A., Firth, D.& Fitzpatrick, R. 2000, Dimensions of inequality and the health of women In Graham H. (Ed) Understanding health inequalities, Buckingham: Oxford University Press. Blackburn, R.M. & Prandy, K. 1997, “The reproduction of social inequality” Sociology, vol.31, pp.491-509. Blaxter M. 1990, Health and Lifestyles, London: Routledge. Cmnd 4386. 1998, Saving lives: our healthier nation London: Stationary Office. Drummond, M. 2006, Personal communication Graham, H. & Kelly, M. 2004, Health inequalities: concepts, frameworks and policy. London: Health development agency. Gregson, J., Foerster, S.B., Orr, R., Jones, L., Benedict, J., Clarke, B., Hersey, J., Lewis, J. & Zotz, K. 2001, “System, environmental, and policy changes: using the social-ecological model as a framework for evaluating nutrition education and social marketing programs with low income audiences”, Journal of nutrition education, vol. 33, supplement 1, pp. s4-s15. Hawe, P. & Shiell, A. 2000, “Social capital and health promotion: a review”, Social science and medicine, vol.51, pp.871-875. Jarvis M. J. & Wardle, J. 2005, Social patterning of health behaviours: the case of cigarette smoking. In: Marmot M. & Wilkinson R. (eds) Social Determinants of Health. Oxford: Oxford University Press, 2nd edition.
125

Lynch, J., Kaplin, G.A. & Salonen, J.T. 1997, “Why do poor people behave poorly? Variation in adult health behaviours and psychological characteristics by stages of the socio-economic life course”, Social science and medicine, vol. 44, no.6, pp.809-819. Mackenbach, J.P., Huisman, M., Andersen, O., Bopp, M., Borgan, J.K. et al. 2004, “Inequalities in lung cancer mortality by the educational level in ten European populations” European Journal of Cancer, vol. 40, pp.126-135. Marmot M. 2004, The Status Syndrome: How Social Standing Affects Our Health and Longevity. London: Bloomsbury Publishing.
Marmot M. 2006, “Smoking and inequalities” Lancet, vol.368, pp. 341-342. Maynard A. (2006) Personal communication Mechanic, D. 1999, “Issues in promoting health”, Social Science and Medicine, vol. 48, pp.711-718. Morgan, A. & Swann, C. (Eds) 2004, Social capital for health: Issues of definition, measurement and links to health, London: Health Development Agency. Nazroo, J.Y. 1998, “Genetic cultural or socio-economic vulnerability? Explaining ethnic inequalities in health”, Sociology of health and illness, vol. 20, no. 5, pp. 710-730. Swann, C. & Morgan, A. (Eds) 2002, Social capital for health: Insights from qualitative research, London: Health Development Agency. Wilkinson, R. 1996, Unhealthy Societies: The Afflictions of Inequality. London: Routledge. Wilkinson, R. 2006, Personal communication
Williams, A. 2004, What could be nicer than NICE? London: Office of Health Economics.
Williams, D.R., Neighbors, H.W. & Jackson, J.S.2003, “Racial/ethnic discrimination and health: findings from community studies”, The American public health association, vol. 93, no.2, pp.200-208.
126

APPENDIX 2: Critical Appraisal Tool
Ref: Authors _____________________________________________________ Year of publication _____________________________________________________ Title _____________________________________________________ Source _____________________________________________________ Form completed by _________________________________ Date ______________ Relevance to topic Does this paper address your topic area? Yes No Unsure
Selection Criteria Did the paper have a clearly focussed aim or research question? Consider whether the following are discussed:
• The population studied • The interventions given • The outcomes considered • Inclusion and exclusion criteria • Types of studies
Did the paper consider inequalities?
Yes Yes Yes Yes Yes Yes Yes
No No No No No No No
Unsure Unsure Unsure Unsure Unsure Unsure Unsure
Systematicity Do the reviewers include all:
a) Relevant databases searched b) Years searched c) Were references from bibliographies followed up? d) Were experts consulted? e) Was grey literature searched? f) Were search terms specified? g) Is the search strategy adequate? h) Did the review include English language studies only?
Yes Yes Yes Yes Yes Yes Yes Yes
No No No No No No No No
Unsure Unsure Unsure Unsure Unsure Unsure Unsure Unsure
Is it worth continuing? Yes No Why/why not?
127

Quality Did the authors assess the quality (rigour) of the included studies? Consider whether the following are used:
A rating system More than one assessor
Yes Yes Yes
No No No
Unsure Unsure Unsure
If study results have been combined, was it reasonable to do so? Consider whether the following are true:
• Are the results of included studies clearly displayed? • Are the studies sufficiently similar in design? • How were the variations between studies investigated?
Are there sufficient data to support conclusions?
Yes Yes Yes Yes Yes
No No No No No
Unsure Unsure Unsure Unsure Unsure
Relevance to UK Can the results be applied/are generalisable to a UK population/ population group?
Are there differences in health care provision with the UK?
Is the paper focused on a particular target group (age, sex, population sub-group etc)?
Yes Yes Yes
No No No
Unsure Unsure Unsure
Accept for inclusion?
Yes
No
Refer to third party
Additional comments:
128
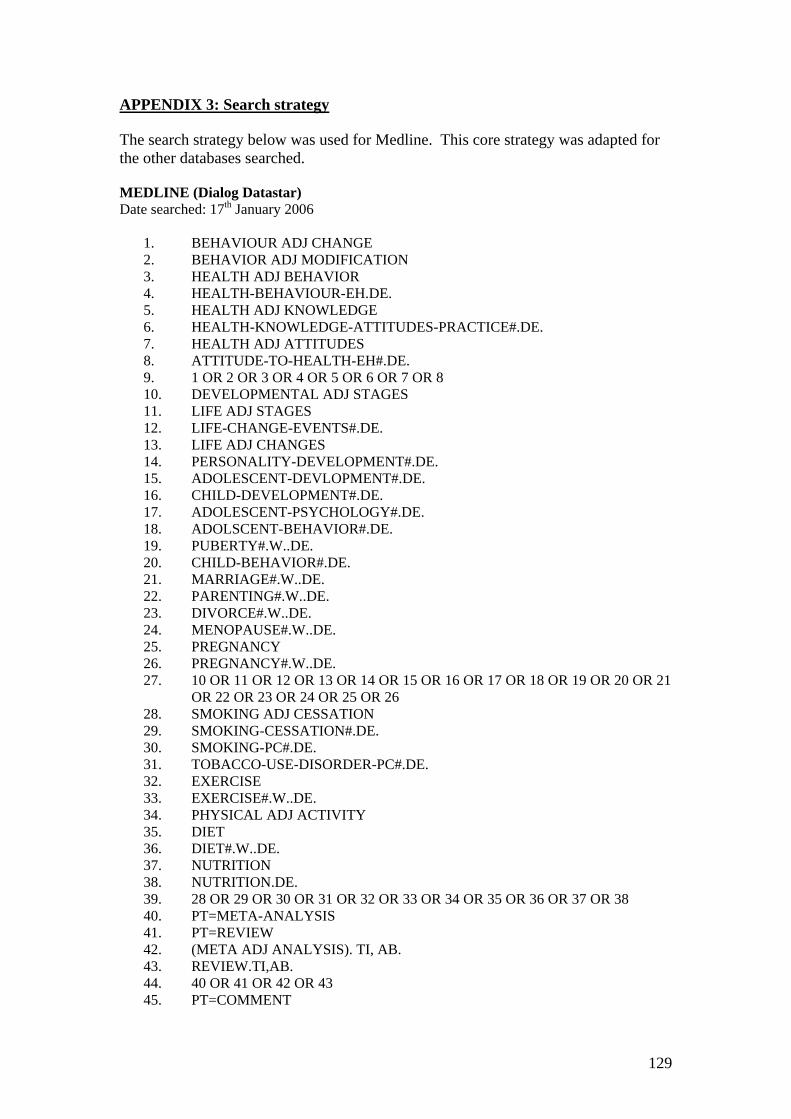
APPENDIX 3: Search strategy The search strategy below was used for Medline. This core strategy was adapted for the other databases searched. MEDLINE (Dialog Datastar) Date searched: 17th January 2006
1. BEHAVIOUR ADJ CHANGE 2. BEHAVIOR ADJ MODIFICATION 3. HEALTH ADJ BEHAVIOR 4. HEALTH-BEHAVIOUR-EH.DE. 5. HEALTH ADJ KNOWLEDGE 6. HEALTH-KNOWLEDGE-ATTITUDES-PRACTICE#.DE. 7. HEALTH ADJ ATTITUDES 8. ATTITUDE-TO-HEALTH-EH#.DE. 9. 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 10. DEVELOPMENTAL ADJ STAGES 11. LIFE ADJ STAGES 12. LIFE-CHANGE-EVENTS#.DE. 13. LIFE ADJ CHANGES 14. PERSONALITY-DEVELOPMENT#.DE. 15. ADOLESCENT-DEVLOPMENT#.DE. 16. CHILD-DEVELOPMENT#.DE. 17. ADOLESCENT-PSYCHOLOGY#.DE. 18. ADOLSCENT-BEHAVIOR#.DE. 19. PUBERTY#.W..DE. 20. CHILD-BEHAVIOR#.DE. 21. MARRIAGE#.W..DE. 22. PARENTING#.W..DE. 23. DIVORCE#.W..DE. 24. MENOPAUSE#.W..DE. 25. PREGNANCY 26. PREGNANCY#.W..DE. 27. 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21
OR 22 OR 23 OR 24 OR 25 OR 26 28. SMOKING ADJ CESSATION 29. SMOKING-CESSATION#.DE. 30. SMOKING-PC#.DE. 31. TOBACCO-USE-DISORDER-PC#.DE. 32. EXERCISE 33. EXERCISE#.W..DE. 34. PHYSICAL ADJ ACTIVITY 35. DIET 36. DIET#.W..DE. 37. NUTRITION 38. NUTRITION.DE. 39. 28 OR 29 OR 30 OR 31 OR 32 OR 33 OR 34 OR 35 OR 36 OR 37 OR 38 40. PT=META-ANALYSIS 41. PT=REVIEW 42. (META ADJ ANALYSIS). TI, AB. 43. REVIEW.TI,AB. 44. 40 OR 41 OR 42 OR 43 45. PT=COMMENT
129

46. PT=LETTER 47. 45 OR 46 48. 44 NOT 47 49. 9 AND 27 AND 39 AND 48
130

APPENDIX 4: Report bibliography Acheson, D. 1998, Independent Inquiry into Inequalities in Health Report, London: The Stationary Office. Adshead, F. 2006, Social marketing principles, 26th July 2006. http://www.number-10.gov.uk/output/Page9913.asp [Last accessed August,14th 2006]. Alberti, K.G.M.M. 2006, Personal communication. Banks, J., Marmot, M., Oldfield, Z. & Smith, J.P. 2006, “Disease and disadvantage in the United States and in England”, Journal of the American Medical Association, vol. 295, no.17, pp. 237-245. Batty, G.D., Der, G., Macintyre, S., Deary, I.J. 2006, “Does IQ explain socio-economic inequalities in health? Evidence from population based cohort study in the West of Scotland”, British Medical Journal, vol. 332, pp. 580-583. Belza, B. & Warms, C. 2004, “Physical activity and exercise in women’s health”, Nursing clinics of north America, vol. 39, pp. 181-193. Blair A. 2006, Speech on Healthy Living, 26th July 2006. http://www.number-10.gov.uk/output/Page9921.asp [Last accessed July 29th, 2006]. Blaxter M. 1990, Health and Lifestyles, London: Routledge. Calnan, M. 1994, Lifestyle and it’s social meaning In Albrecht, G. (Ed) Advances in medical sociology, Greenwich: JAI Press. Cater, S. & Coleman, L. 2006, 'Planned' teenage pregnancy: Views and experiences of young people from poor and disadvantaged backgrounds, Bristol: The Policy Press. Cmnd 6374. 2004, Choosing health: making healthy choices easier, London: The Stationery Office. Cochrane injuries group driver education reviewers. 2001, “Evidence based road safety: the driving standards agencies schools program”, Lancet, vol. 358, pp.230-232. Drever F. and Whitehead M. (Eds) 1997, Health Inequalities, London: The Stationery Office. Gatrell, A., Thomas, C., Bennett, S., Bostock, L., Popay, J., Williams, G. & Shahtahmasebi, S. 2000, Understanding health inequalities: Locating people with geographical and social spaces In Graham H. (Ed) Understanding health inequalities, Buckingham: Oxford University Press. Graham, H. (Ed) 2000, Understanding health inequalities, Buckingham: Oxford University Press.
131

Hillsdon, M. & Thorogood, M. 1996, “A systematic review of physical activity promotion activities”, British Journal of Sports Medicine, vol. 30, pp. 84-89. Kessel, A. 2006, Air, the environment and public health, Cambridge: Cambridge University Press. Khaw, K.T., Bingham, S., Welch, A., Luben, R., Wareham, N., Oakes, S. & Day, N. 2001, “Relation between plasma ascorbic acid and mortality in men and women in EPIC-Norfolk prospective study: prospective population study” Lancet, vol. 357, pp.657-663. Khaw, K.T., Jakes, R., Bingham, S., Welch, A., Luben, R., Day, N. and Wareham, N. 2006, “Work and leisure time physical activity assessed using a simple, pragmatic, validated questionnaire and incident cardiovascular disease and all course mortality in men and women: the European prospective investigation into cancer in Norfolk prospective population study”, International Journal of Epidemiology, May 18th 2006 (online copy read ahead of publication). Kramer, M.S. 2002, Aerobic exercise for women during pregnancy. The Cochrane database of systematic review, issue 2. Lange-Collett, J. 2002, “Promoting health among perimenopausal women through diet and exercise”, Journal of the American academy of nurse practitioners, vol. 14, no.4, pp.172-177. Mackenbach, J.P., Huisman, M., Andersen, O., Bopp, M., Borgan, J.K. et al. 2004, “Inequalities in lung cancer mortality by the educational level in ten European populations” European Journal of Cancer, vol. 40, pp.126-135. Marmot M. 2005, Personal communication. Marmot M. 2006, “Smoking and inequalities” Lancet, vol.368, pp. 341-342. Matrix. 2005, Rapid review of the economic evidence of physical activity interventions London: National Institute for health and clinical excellence. Mayo, E. 2006, Social marketing/changing behaviour 26th July 2006. http://www.number-10.gov.uk/output/Page.9910 asp [Last accessed August,14th 2006]. Mechanic, D. 1995, “Sociological dimensions of illness behaviour”, Social Science and Medicine, vol. 41, no.9, pp. 1207-1216. National Institute for Health and Clinical Excellence. 2006, NICE Public health guidance methods manual London: National Institute for Health and Clinical Excellence.
132

Nicklas, T.A., Baranowski, T., Baranowski, J.C., Cullen, K., Rittenberry, M.S. & Olvera, N. 2001, “Family and child care provider influences on pre-school children’s fruit, juice, and vegetable consumption”, Nutrition reviews, vol. 59, no.7, pp.224-235. Oliver A., Healey A. and Le Grande J. 2002, “Addressing Health Inequalities”, Lancet, vol. 360, pp 565-567. Rowntree, B. S., 1901, Poverty: A Study of Town Life, London:Macmillan. Scottish Intercollegiate Guidelines network. 2002, SIGN 50. A guideline developers handbook, Edinburgh: Scottish Intercollegiate Guidelines network. Suhrcke, M., McKee, M., Sauto Arce ,R .,Tsolova, S. & Mortensen, J. 2005, The Contribution of Health to the economy in the European Union. Luxembourg: Office for Official Publications of the European Communities. Taylor, D. & Bury, M. 2006, “A theory of care transition: from medical dominance to managed consumerism in ageing societies” (in preparation) Taylor, D., Bury, M., Campling, N., Carter, S., Garfield, S., Newbould, J. & Rennie, T. (2006) A review of the use of the health belief model, the theory of reasoned action, the theory of planned behaviour and the transtheoretical model to study and predict health related behaviour change. London: National Institute for health and clinical excellence (under review). Wanless, D. 2004, Securing good health for the whole population, London: HM Treasury. Wilcox, S. 2002, “Physical activity in older women or color” Topics in geriatric rehabilitation, vol. 18, no. 1, pp. 21-33.
133
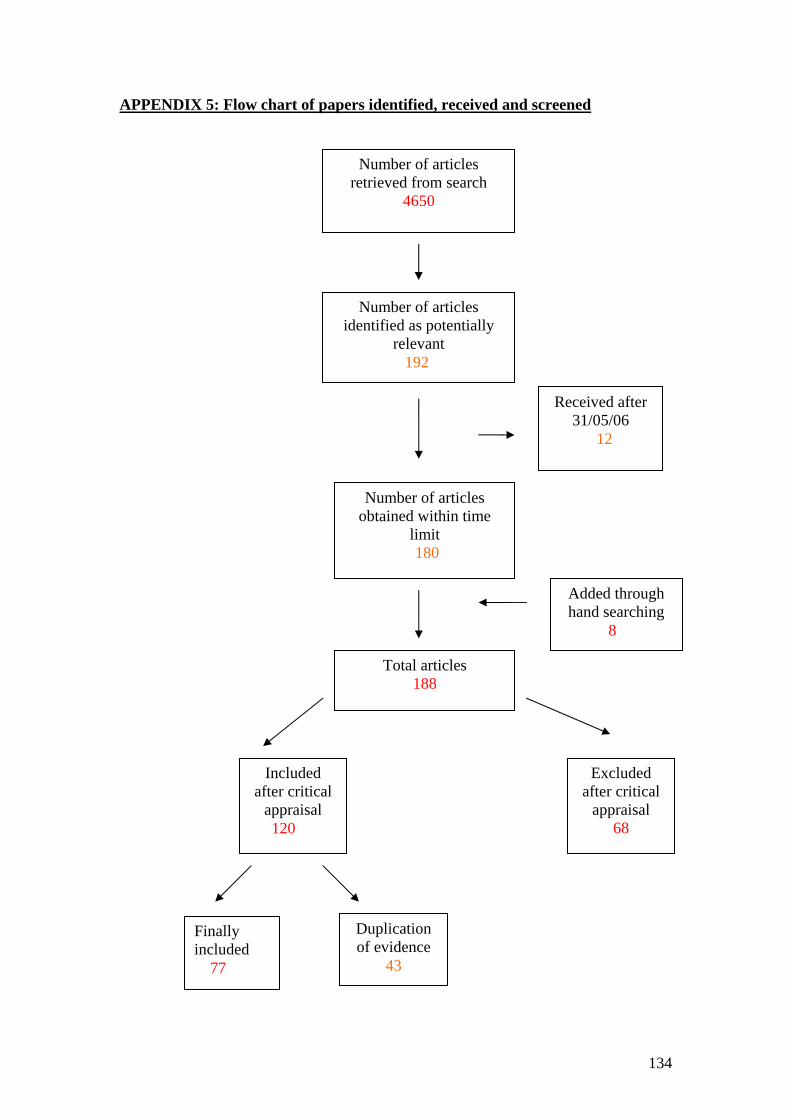
APPENDIX 5: Flow chart of papers identified, received and screened
Number of articles identified as potentially
relevant 192
Number of articles retrieved from search
4650
Number of articles obtained within time
limit 180
Excluded after critical
appraisal 68
Included after critical
appraisal 120
Added through hand searching
8
Total articles 188
Received after 31/05/06
12
Finally included 77
Duplication of evidence
43
134
135
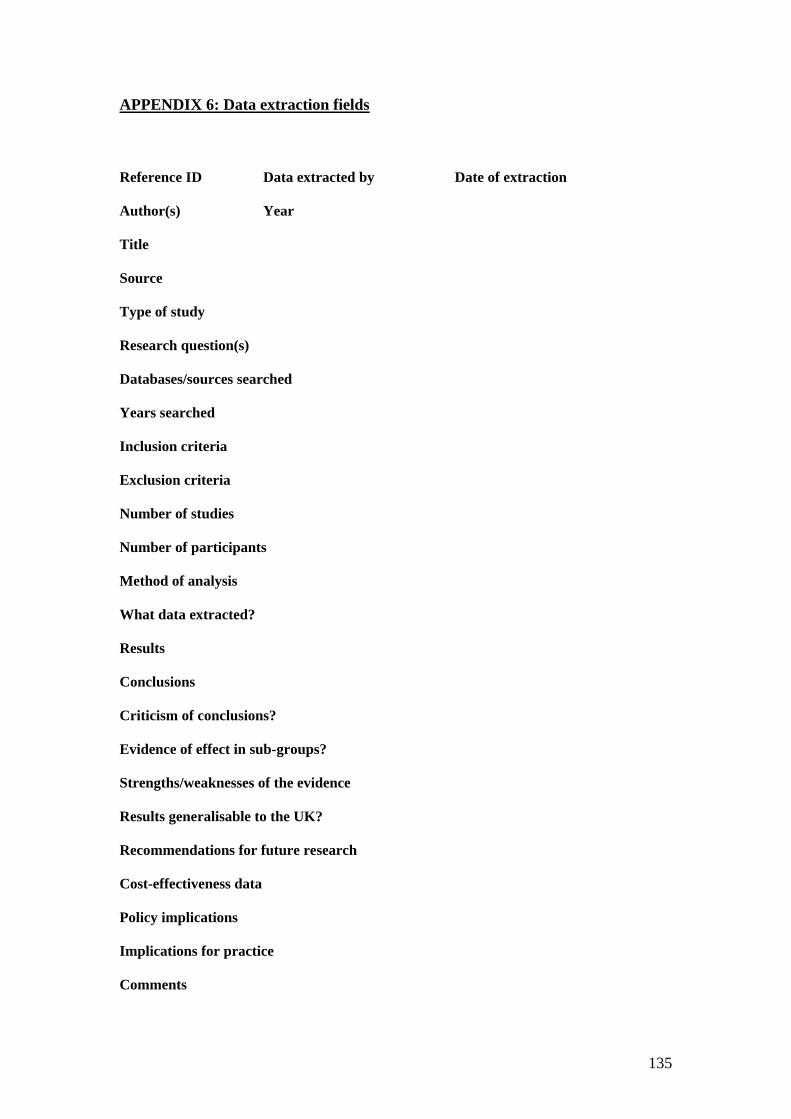
APPENDIX 6: Data extraction fields
Reference ID Data extracted by Date of extraction Author(s) Year Title Source Type of study Research question(s) Databases/sources searched Years searched Inclusion criteria Exclusion criteria Number of studies Number of participants Method of analysis What data extracted? Results Conclusions Criticism of conclusions? Evidence of effect in sub-groups? Strengths/weaknesses of the evidence Results generalisable to the UK? Recommendations for future research Cost-effectiveness data Policy implications Implications for practice Comments
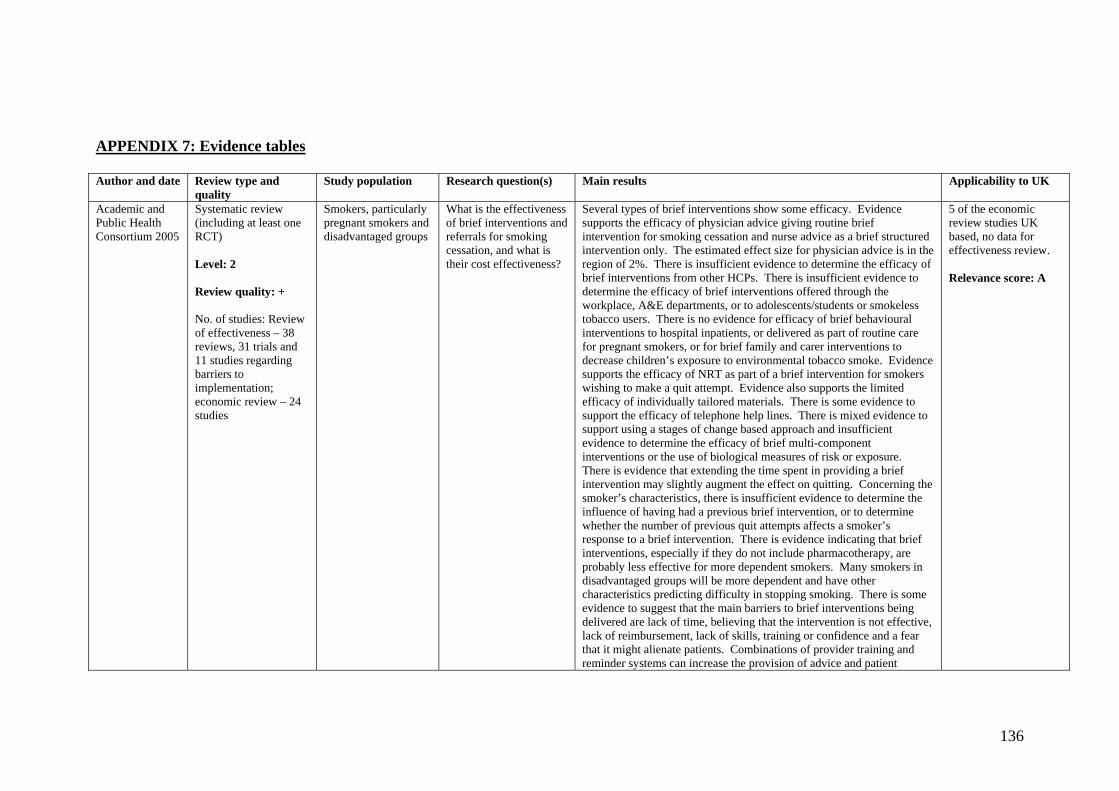
APPENDIX 7: Evidence tables Author and date Review type and
quality Study population Research question(s) Main results Applicability to UK
Academic and Public Health Consortium 2005
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: Review of effectiveness – 38 reviews, 31 trials and 11 studies regarding barriers to implementation; economic review – 24 studies
Smokers, particularly pregnant smokers and disadvantaged groups
What is the effectiveness of brief interventions and referrals for smoking cessation, and what is their cost effectiveness?
Several types of brief interventions show some efficacy. Evidence supports the efficacy of physician advice giving routine brief intervention for smoking cessation and nurse advice as a brief structured intervention only. The estimated effect size for physician advice is in the region of 2%. There is insufficient evidence to determine the efficacy of brief interventions from other HCPs. There is insufficient evidence to determine the efficacy of brief interventions offered through the workplace, A&E departments, or to adolescents/students or smokeless tobacco users. There is no evidence for efficacy of brief behavioural interventions to hospital inpatients, or delivered as part of routine care for pregnant smokers, or for brief family and carer interventions to decrease children’s exposure to environmental tobacco smoke. Evidence supports the efficacy of NRT as part of a brief intervention for smokers wishing to make a quit attempt. Evidence also supports the limited efficacy of individually tailored materials. There is some evidence to support the efficacy of telephone help lines. There is mixed evidence to support using a stages of change based approach and insufficient evidence to determine the efficacy of brief multi-component interventions or the use of biological measures of risk or exposure. There is evidence that extending the time spent in providing a brief intervention may slightly augment the effect on quitting. Concerning the smoker’s characteristics, there is insufficient evidence to determine the influence of having had a previous brief intervention, or to determine whether the number of previous quit attempts affects a smoker’s response to a brief intervention. There is evidence indicating that brief interventions, especially if they do not include pharmacotherapy, are probably less effective for more dependent smokers. Many smokers in disadvantaged groups will be more dependent and have other characteristics predicting difficulty in stopping smoking. There is some evidence to suggest that the main barriers to brief interventions being delivered are lack of time, believing that the intervention is not effective, lack of reimbursement, lack of skills, training or confidence and a fear that it might alienate patients. Combinations of provider training and reminder systems can increase the provision of advice and patient
5 of the economic review studies UK based, no data for effectiveness review. Relevance score: A
136
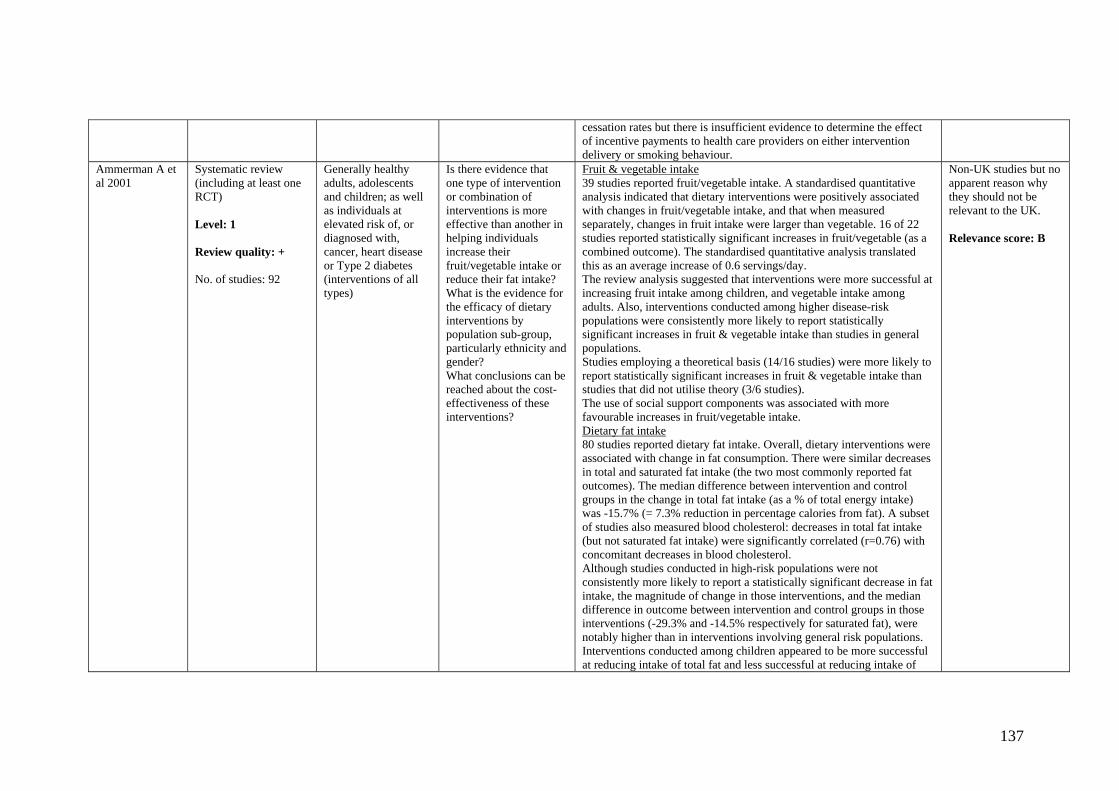
cessation rates but there is insufficient evidence to determine the effect of incentive payments to health care providers on either intervention delivery or smoking behaviour.
Ammerman A et al 2001
Systematic review (including at least one RCT) Level: 1 Review quality: + No. of studies: 92
Generally healthy adults, adolescents and children; as well as individuals at elevated risk of, or diagnosed with, cancer, heart disease or Type 2 diabetes (interventions of all types)
Is there evidence that one type of intervention or combination of interventions is more effective than another in helping individuals increase their fruit/vegetable intake or reduce their fat intake? What is the evidence for the efficacy of dietary interventions by population sub-group, particularly ethnicity and gender? What conclusions can be reached about the cost-effectiveness of these interventions?
Fruit & vegetable intake 39 studies reported fruit/vegetable intake. A standardised quantitative analysis indicated that dietary interventions were positively associated with changes in fruit/vegetable intake, and that when measured separately, changes in fruit intake were larger than vegetable. 16 of 22 studies reported statistically significant increases in fruit/vegetable (as a combined outcome). The standardised quantitative analysis translated this as an average increase of 0.6 servings/day. The review analysis suggested that interventions were more successful at increasing fruit intake among children, and vegetable intake among adults. Also, interventions conducted among higher disease-risk populations were consistently more likely to report statistically significant increases in fruit & vegetable intake than studies in general populations. Studies employing a theoretical basis (14/16 studies) were more likely to report statistically significant increases in fruit & vegetable intake than studies that did not utilise theory (3/6 studies). The use of social support components was associated with more favourable increases in fruit/vegetable intake. Dietary fat intake 80 studies reported dietary fat intake. Overall, dietary interventions were associated with change in fat consumption. There were similar decreases in total and saturated fat intake (the two most commonly reported fat outcomes). The median difference between intervention and control groups in the change in total fat intake (as a % of total energy intake) was -15.7% (= 7.3% reduction in percentage calories from fat). A subset of studies also measured blood cholesterol: decreases in total fat intake (but not saturated fat intake) were significantly correlated (r=0.76) with concomitant decreases in blood cholesterol. Although studies conducted in high-risk populations were not consistently more likely to report a statistically significant decrease in fat intake, the magnitude of change in those interventions, and the median difference in outcome between intervention and control groups in those interventions (-29.3% and -14.5% respectively for saturated fat), were notably higher than in interventions involving general risk populations. Interventions conducted among children appeared to be more successful at reducing intake of total fat and less successful at reducing intake of
Non-UK studies but no apparent reason why they should not be relevant to the UK. Relevance score: B
137

saturated fat than interventions among adults (although this was a very small number of studies). Interventions employing a theoretical framework were not consistently more likely to report significant effects. The use of social support, small groups and goal setting appeared particularly effective at reducing fat intake. Studies involving families and using interactive food-related activities were more likely to report significant decreases in fat intake, although magnitude of decrease was not higher. All 5 of the studies which were designed to be culturally or ethnically specific reported significant decreases in total and saturated fat intake.
Ammerman A et al 2002
Three tier analytic approach (inc. meta-analysis) – RCTs and non-RCTs Level: 2 Review quality: + No. of studies: 92
Healthy adult or at risk populations
What is the overall effectiveness of behavioural dietary interventions in promoting dietary change related to chronic disease risk reduction? What is the relative effectiveness of specific intervention features among different population sub-groups?
Meta-analysis; studies typically showed small to moderate changes in the intervention group that were significantly larger than in the comparison group. However, the magnitude of effects varied by setting and population and by the length and intensity of the intervention. Interventions appeared more successful at changing dietary behaviour among populations at risk (or diagnosed with) disease more than among general healthy populations. Differences in deltas analysis; dietary interventions were similarly successful in reducing intake of total and saturated fat, and increasing fruit and vegetable intake. There was an average decrease of 7.3% of daily calories from fat. Amongst fruit and vegetable studies included in differences in delta analysis intervention groups increased their intake of fruit and vegetables about 17% more than control groups. This represents an average increase of 0.6 servings of fruits and vegetables per day. Summary of significant findings approach; the majority of studies (n=49) reported significant intervention effect for changes in dietary intake. 86% of the studies found significant effect in terms of reduction in total far, 87% of studies found significant effect in reducing saturated fat intake and 77% of studies found a significant effect in increasing fruit and vegetable intake. General results; interventions with younger people (less than 18 years) were more likely to report significant decreases in total fat intake than those with adults, although the opposite was true for the intake of saturated fat. Two intervention components appeared successful at modifying dietary behaviour – goal setting and small groups.
Unable to ascertain if review included studies from the UK. Relevance score: B
Ashenden R, Silagy C &
Systematic review (including at least one
Adults attending general practice
In relation to four behaviours (smoking,
Smoking cessation: Provision of brief or intensive advice increases the odds of quitting (OR: 1.32, CI: 1.18 – 1.48). Number of smokers needed
Studies from the UK were represented in the
138

Weller D 1997
RCT) Level: 1 Review quality: + No. of studies: Smoking - 23 trials, diet – 10 trials, exercise – 6 trials
alcohol consumption, diet, and exercise): Is the provision of advice more effective in eliciting lifestyle-related behaviour change than providing no advice? Is providing intense advice more effective than brief advice?
to treat to produce one quitter: 50 with brief advice, 25 with intensive advice. However, a direct comparison between intensive and brief advice (n=6275) found no statistical difference (OR: 1.07, CI: 0.88 – 1.29). Diet: Evidence variable, no conclusions drawn. Exercise: Evidence variable, no conclusions drawn. However, evidence in three of the six trials demonstrating short- and long-term effects.
review (7 smoking, 3 diet, 2 exercise). Relevance score: A
Ashworth NL et al 2005
Systematic review (RCTs and quasi-RCTs) Level: 1 Review quality: ++ No. of studies: 6
Older adults (50 years or over), with either a recognised cardiovascular risk factor, or existing cardiovascular disease, or chronic obstructive airways disease or osteoarthritis
What is the effectiveness of home based versus center based physical activity programs on the health of older adults?
224 participants received a home based exercise programme and 148 received a center based exercise programme. Cardiovascular: the largest trial (accounting for approximately 60% of the participants) looked at sedentary older adults. 3 trials looked at patients with peripheral vascular disease (intermittent claudication). In patients with peripheral vascular disease center based programmes were superior to home at improving distance walked and time to claudication pain at up to 6 months. However the risk of a training effect may be high. There were no longer term studies in this population. Notably home based programmes appeared to have a significantly higher adherence rate than center based programmes. However this was based primarily on the 1 study (with the highest quality rating of the studies found) of sedentary older adults. This showed an adherence rate of 68% in the home based programme at 2 year follow-up compared with 36% adherence in the center based group. There was essentially no difference in terms of treadmill performance or cardiovascular risk factors between groups. COPD: 2 trials looked at older adults with COPD. In patients with COPD the evidence is conflicting. 1 study showed similar changes in various physiological measures at 3 months that persisted in the home based group up to 18 months but not in the center based group. The other study showed significantly better improvements in physiological measures in the center based group after 8 weeks but again the possibility of training effects is high. Osteoarthritis: no studies were found.
4 of the 6 studies performed in the US, 1 in Spain, and the country of origin for the final trial not stated. Relevance score: B
Bessell T L 2002 Systematic review (including at least one RCT)
Internet users, non-Internet users and other communications media users and non-
What is the effect of consumer use of online health information on decision-making,
Only 6 of the 10 studies were deemed good quality. 1 showed the Internet to be an effective medium to deliver a smoking cessation programme (52% of smokers had quit 12 months after enrolling on online programme). 3 other studies all showed positive outcomes of
Non-UK studies. Majority of studies in the review were US based.
139
Level: 1 Review quality: - No. of studies: 10
users attitudes, knowledge, satisfaction and health outcomes and utilisation?
Internet interventions, one of which showed significant reductions in fast food calories and fat and more fruit/vegetable intake in internet + classroom intervention compared to classroom intervention in a poor US school (though ‘change’ was reported in points, so cannot determine real extent of change). Another study compared a 6-month internet-based weight loss programme + additional resources such as email lessons, support and bulletin board with an internet-based programme only, in overweight US employees. The former intervention showed better weight loss. [The sixth study looked at attitudes towards surgery]. The 4 poorer quality studies, did not address dietary, smoking or exercise behaviour.
Relevance score: B
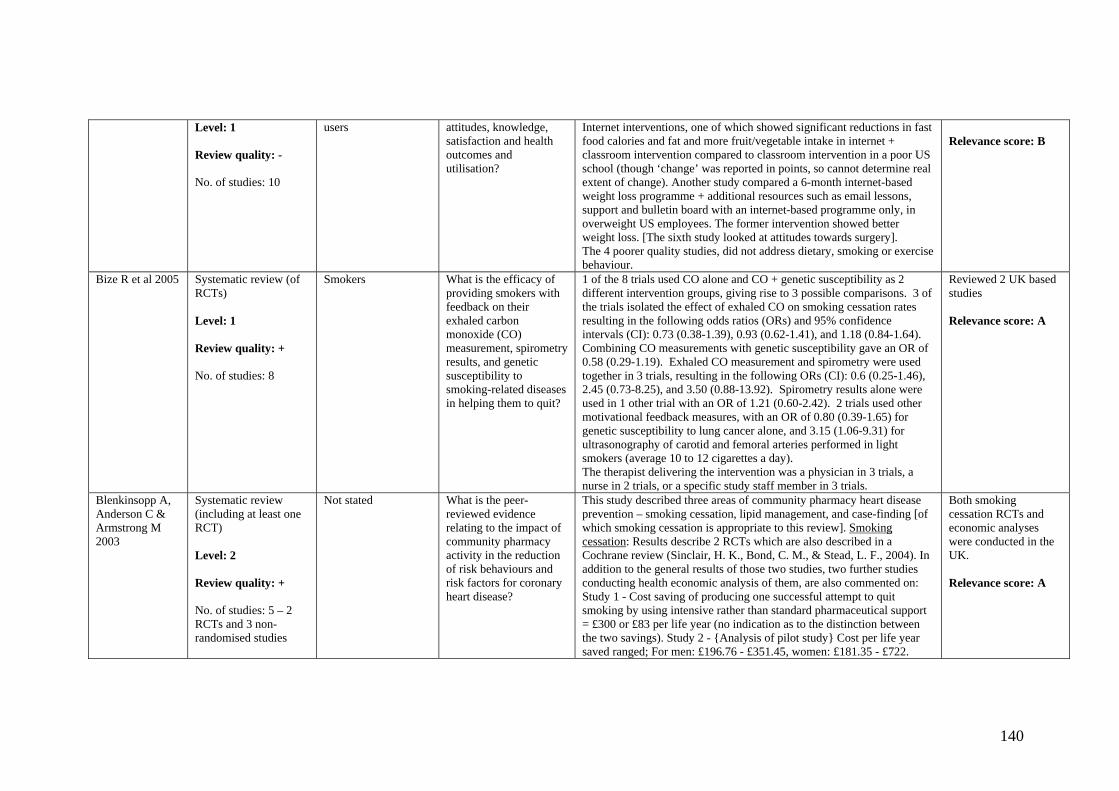
Bize R et al 2005 Systematic review (of RCTs) Level: 1 Review quality: + No. of studies: 8
Smokers What is the efficacy of providing smokers with feedback on their exhaled carbon monoxide (CO) measurement, spirometry results, and genetic susceptibility to smoking-related diseases in helping them to quit?
1 of the 8 trials used CO alone and CO + genetic susceptibility as 2 different intervention groups, giving rise to 3 possible comparisons. 3 of the trials isolated the effect of exhaled CO on smoking cessation rates resulting in the following odds ratios (ORs) and 95% confidence intervals (CI): 0.73 (0.38-1.39), 0.93 (0.62-1.41), and 1.18 (0.84-1.64). Combining CO measurements with genetic susceptibility gave an OR of 0.58 (0.29-1.19). Exhaled CO measurement and spirometry were used together in 3 trials, resulting in the following ORs (CI): 0.6 (0.25-1.46), 2.45 (0.73-8.25), and 3.50 (0.88-13.92). Spirometry results alone were used in 1 other trial with an OR of 1.21 (0.60-2.42). 2 trials used other motivational feedback measures, with an OR of 0.80 (0.39-1.65) for genetic susceptibility to lung cancer alone, and 3.15 (1.06-9.31) for ultrasonography of carotid and femoral arteries performed in light smokers (average 10 to 12 cigarettes a day). The therapist delivering the intervention was a physician in 3 trials, a nurse in 2 trials, or a specific study staff member in 3 trials.
Reviewed 2 UK based studies Relevance score: A
Blenkinsopp A, Anderson C & Armstrong M 2003
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 5 – 2 RCTs and 3 non-randomised studies
Not stated What is the peer-reviewed evidence relating to the impact of community pharmacy activity in the reduction of risk behaviours and risk factors for coronary heart disease?
This study described three areas of community pharmacy heart disease prevention – smoking cessation, lipid management, and case-finding [of which smoking cessation is appropriate to this review]. Smoking cessation: Results describe 2 RCTs which are also described in a Cochrane review (Sinclair, H. K., Bond, C. M., & Stead, L. F., 2004). In addition to the general results of those two studies, two further studies conducting health economic analysis of them, are also commented on: Study 1 - Cost saving of producing one successful attempt to quit smoking by using intensive rather than standard pharmaceutical support = £300 or £83 per life year (no indication as to the distinction between the two savings). Study 2 - {Analysis of pilot study} Cost per life year saved ranged; For men: £196.76 - £351.45, women: £181.35 - £722.
Both smoking cessation RCTs and economic analyses were conducted in the UK. Relevance score: A
140
These findings demonstrate significant economic savings of community pharmacy interventions in smoking cessation, where conclusive evidence of effectiveness is limited.
Blue CL & Conrad KM 1995
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 10
Adults (undergoing worksite exercise programmes and specific strategies to improve exercise adherence)
What effect do worksite exercise interventions that seek to increase adherence to exercise have?
9 of the 10 included studies showed that exercise adherence strategies worked to increase or improve exercise behaviour. The most impressive results came from programmes with multiple interventions. Long term outcomes were only assessed in a minority of studies. However, one study examined data adherence over 12 years and found a ‘dropping off’ of adherence to exercise over time. Another study measuring short term outcomes only indicated that relapse training may reduce ‘dropping off.’
Review does not state which countries studies were carried out in. Relevance score: B
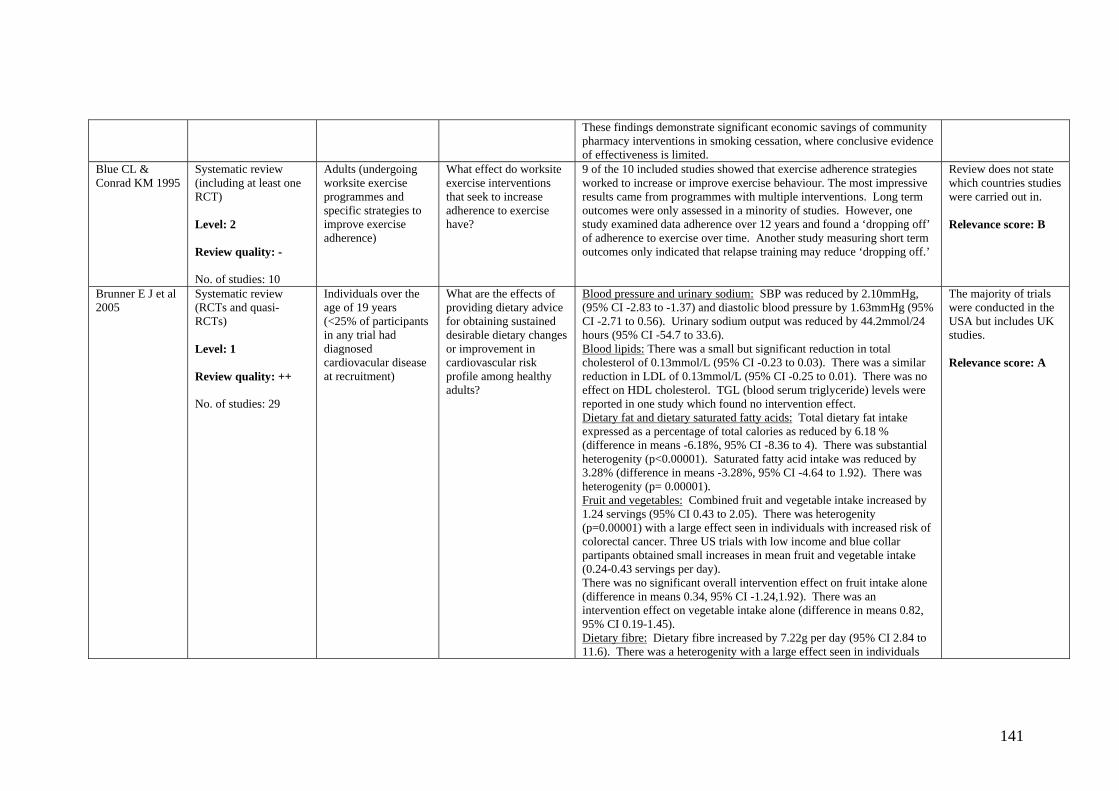
Brunner E J et al 2005
Systematic review (RCTs and quasi-RCTs) Level: 1 Review quality: ++ No. of studies: 29
Individuals over the age of 19 years (<25% of participants in any trial had diagnosed cardiovacular disease at recruitment)
What are the effects of providing dietary advice for obtaining sustained desirable dietary changes or improvement in cardiovascular risk profile among healthy adults?
Blood pressure and urinary sodium: SBP was reduced by 2.10mmHg, (95% CI -2.83 to -1.37) and diastolic blood pressure by 1.63mmHg (95% CI -2.71 to 0.56). Urinary sodium output was reduced by 44.2mmol/24 hours (95% CI -54.7 to 33.6). Blood lipids: There was a small but significant reduction in total cholesterol of 0.13mmol/L (95% CI -0.23 to 0.03). There was a similar reduction in LDL of 0.13mmol/L (95% CI -0.25 to 0.01). There was no effect on HDL cholesterol. TGL (blood serum triglyceride) levels were reported in one study which found no intervention effect. Dietary fat and dietary saturated fatty acids: Total dietary fat intake expressed as a percentage of total calories as reduced by 6.18 % (difference in means -6.18%, 95% CI -8.36 to 4). There was substantial heterogenity (p<0.00001). Saturated fatty acid intake was reduced by 3.28% (difference in means -3.28%, 95% CI -4.64 to 1.92). There was heterogenity (p= 0.00001). Fruit and vegetables: Combined fruit and vegetable intake increased by 1.24 servings (95% CI 0.43 to 2.05). There was heterogenity (p=0.00001) with a large effect seen in individuals with increased risk of colorectal cancer. Three US trials with low income and blue collar partipants obtained small increases in mean fruit and vegetable intake (0.24-0.43 servings per day). There was no significant overall intervention effect on fruit intake alone (difference in means 0.34, 95% CI -1.24,1.92). There was an intervention effect on vegetable intake alone (difference in means 0.82, 95% CI 0.19-1.45). Dietary fibre: Dietary fibre increased by 7.22g per day (95% CI 2.84 to 11.6). There was a heterogenity with a large effect seen in individuals
The majority of trials were conducted in the USA but includes UK studies. Relevance score: A
141
with increased risk of colorectal cancer. Gender: Women were more likely than men to report reduced dietary fat intake and increased fruit and vegetable intakes but no gender differences in total blood cholestrol. There were large intervention effects on fat intake in the 2 women’s health trial pilot studies. Disease risk groups: Participants at higher risk of cardiovacsular disease did not report greater reductions in dietary fat intake or cholesterol level but those at high cancer risk had a substantially greater reported intake of fruit and vegetables. Intervention setting: Trials conducted in healthcare settings tended to show greater reporting of reduced dietary fat an increased fruit and vegetable consumption than workplace/ community settings. However no differences in blood cholesterol reductions were found. Intervention intensity: Overall high intensity interventions involving more than 3 scheduled contacts tended to be associated with larger effect sizes than low intensity interventions. The difference in effect size was significant for dietary fat and for fruit and vegetables, however there was heterogeneity in the effects within these high intensity subgroups. No differences in blood cholestrol reductions were found. There is therefore inconsistent evidence that higher intensity interventions are associated with larger dietary changes.
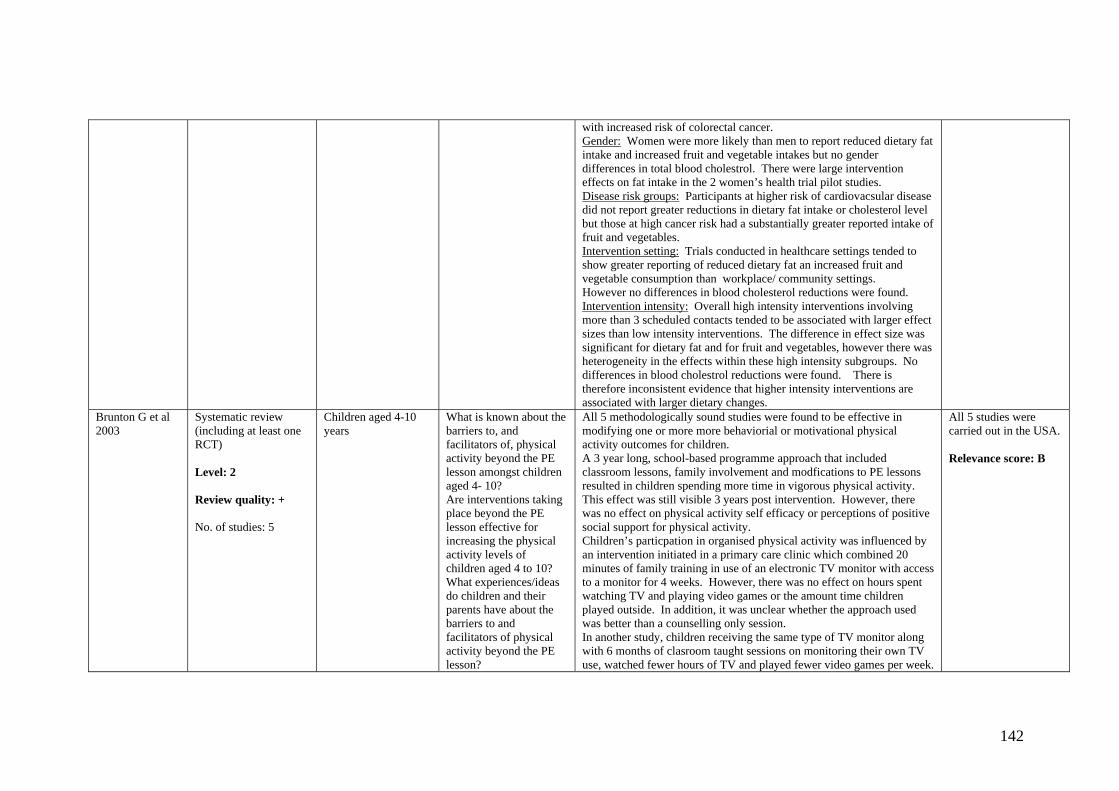
Brunton G et al 2003
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 5
Children aged 4-10 years
What is known about the barriers to, and facilitators of, physical activity beyond the PE lesson amongst children aged 4- 10? Are interventions taking place beyond the PE lesson effective for increasing the physical activity levels of children aged 4 to 10? What experiences/ideas do children and their parents have about the barriers to and facilitators of physical activity beyond the PE lesson?
All 5 methodologically sound studies were found to be effective in modifying one or more more behaviorial or motivational physical activity outcomes for children. A 3 year long, school-based programme approach that included classroom lessons, family involvement and modfications to PE lessons resulted in children spending more time in vigorous physical activity. This effect was still visible 3 years post intervention. However, there was no effect on physical activity self efficacy or perceptions of positive social support for physical activity. Children’s particpation in organised physical activity was influenced by an intervention initiated in a primary care clinic which combined 20 minutes of family training in use of an electronic TV monitor with access to a monitor for 4 weeks. However, there was no effect on hours spent watching TV and playing video games or the amount time children played outside. In addition, it was unclear whether the approach used was better than a counselling only session. In another study, children receiving the same type of TV monitor along with 6 months of clasroom taught sessions on monitoring their own TV use, watched fewer hours of TV and played fewer video games per week.
All 5 studies were carried out in the USA. Relevance score: B
142
To what extent do interventions build on these views? What do the above suggest for developing effective and appropriate interventions to be tested in the future?
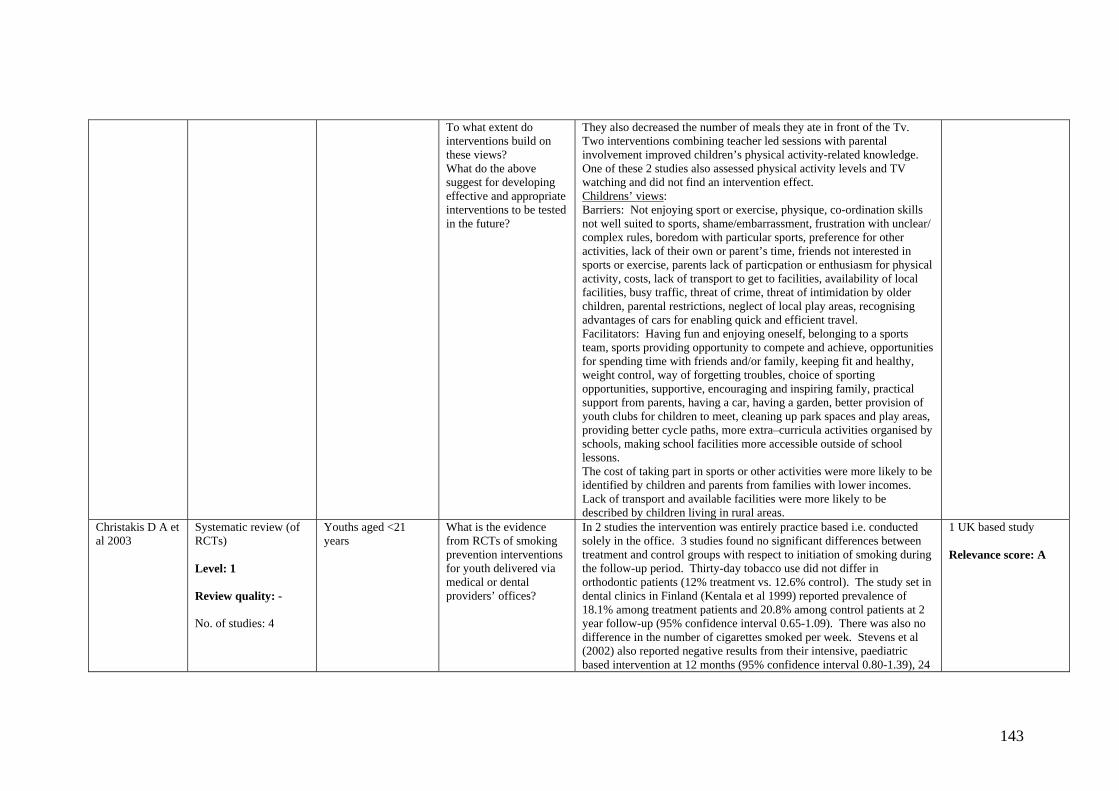
They also decreased the number of meals they ate in front of the Tv. Two interventions combining teacher led sessions with parental involvement improved children’s physical activity-related knowledge. One of these 2 studies also assessed physical activity levels and TV watching and did not find an intervention effect. Childrens’ views: Barriers: Not enjoying sport or exercise, physique, co-ordination skills not well suited to sports, shame/embarrassment, frustration with unclear/ complex rules, boredom with particular sports, preference for other activities, lack of their own or parent’s time, friends not interested in sports or exercise, parents lack of particpation or enthusiasm for physical activity, costs, lack of transport to get to facilities, availability of local facilities, busy traffic, threat of crime, threat of intimidation by older children, parental restrictions, neglect of local play areas, recognising advantages of cars for enabling quick and efficient travel. Facilitators: Having fun and enjoying oneself, belonging to a sports team, sports providing opportunity to compete and achieve, opportunities for spending time with friends and/or family, keeping fit and healthy, weight control, way of forgetting troubles, choice of sporting opportunities, supportive, encouraging and inspiring family, practical support from parents, having a car, having a garden, better provision of youth clubs for children to meet, cleaning up park spaces and play areas, providing better cycle paths, more extra–curricula activities organised by schools, making school facilities more accessible outside of school lessons. The cost of taking part in sports or other activities were more likely to be identified by children and parents from families with lower incomes. Lack of transport and available facilities were more likely to be described by children living in rural areas.
Christakis D A et al 2003
Systematic review (of RCTs) Level: 1 Review quality: - No. of studies: 4
Youths aged <21 years
What is the evidence from RCTs of smoking prevention interventions for youth delivered via medical or dental providers’ offices?
In 2 studies the intervention was entirely practice based i.e. conducted solely in the office. 3 studies found no significant differences between treatment and control groups with respect to initiation of smoking during the follow-up period. Thirty-day tobacco use did not differ in orthodontic patients (12% treatment vs. 12.6% control). The study set in dental clinics in Finland (Kentala et al 1999) reported prevalence of 18.1% among treatment patients and 20.8% among control patients at 2 year follow-up (95% confidence interval 0.65-1.09). There was also no difference in the number of cigarettes smoked per week. Stevens et al (2002) also reported negative results from their intensive, paediatric based intervention at 12 months (95% confidence interval 0.80-1.39), 24
1 UK based study Relevance score: A
143

months (95% confidence interval 0.82-1.31), and 36 months (95% confidence interval 0.79-1.20) after the intervention. In the Fidler et al (2001) study 5.1% of the intervention group and 7.8% of the control group reported smoking at 12 month follow-up (95% confidence interval 0.44-0.91), a small but significant reduction in reported smoking among intervention youth.
Ciliska D et al 2000
Systematic review Level: 2 Review quality: ++ No. of studies: 15
Children aged 4 years of age and older
What is the effectiveness of community based interventions to increase fruit and vegetable consumption in people 4 years of age and older?
After validity rating, the reports rated strong or moderate were selected - 1 was rated strong, and 17 moderate. 4 studies were targeted to parents of young children, 6 to school aged children, and 5 to adults. Interventions with parents of young children: Del Traduce et al (1988) found an increase in fruit and vegetable consumption from 2.6-3.7 servings/day. Cox et al (1996) – statistically significant increased consumption of fruits and vegetables vs. usual control group. Intervention group increased intake of fruit (1.5-2.6) vs. no change in control, vegetables (0.9-1.6) vs. (0.6-0.8) in the control group. Kolinsky et al (1992) – 5 intervention centres – 2 in Maryland had significant increase in fruit consumption compared to control, from 1.9 to 2.72 servings/day also increased intake of vitamin C rich foods. But, the 3 centres in New York had no change in overall vegetable intake or in any fruit and vegetable intake. Hayes et al (1998) – increase in fruit and vegetable consumption of 0.56 servings/day in intervention group and 0.13 in control group. Interventions with school children: Graves et al (1982) – significant effect of intervention on attitude scales of eating nutritious foods and eating vegetables but not for eating new foods. Shannon et al (1982) – significant increase in consumption of carrots/broccoli and spinach salad and green beans. Shannon & Chen (1988) – improvement in attitudes in both groups (control and intervention) over time, however if entry knowledge and attitude scores were low, then intervention children improved more than control. No overall significant differences between groups. Perry et al (1998a) – lunch intake 1.53 servings of fruit and vegetables/day for intervention group vs. 1.06 for control group and increased consumption of fruits. Perry et al (1998b) – analysis of variance showed no difference by sites, gender or ethnicity. Only Texas site showed difference in fruit intake (increased intake in intervention group). Cullen et al (1997) – 1 week post test, increased 24 hour recall fruit and vegetable consumption in intervention group, but not maintained at 3 months post test. Nicolas et al (1998) – significant increase in knowledge in intervention group, and significant increase in fruit and vegetable intake in intervention group.
All studies were conducted in the US with 6 targeting school children. Relevance score: B
144

Interventions with adults (non-worksite): Campbell et al (1994) – daily intake of fruit and vegetables decreased in each group (control and intervention) by 0.25 servings/day. Gorbach et al (1990) and Henderson et al (1990) – 12 month and 24 month follow-up, fruit and vegetable intake significantly increased in intervention group more than in control from baseline of 15.9% of total kcal/day to 22% at 12 months and 23.1% at 24 months. Brownson et al (1996) – no change in proportion of people who consumed 5+ fruits and vegetables/day. Interventions with adults (worksite): Sorensen et al (1996) and Glanz (1998) – intake of fruit and vegetables increased by 0.2 servings per day in intervention group vs. 0.02 in control groups. Collected 3 years after pre-test. Hunt et al (1993) – mean increase in total fruit servings/month was 2.9 in control and 6.8 in intervention and in vegetables a decrease in the control and increase in intervention group (6.8 servings/month).
Contento I et al 1995
Review including RCTs but not systematic Level: 3 Review quality: - No. of studies: preschool children – 23, school age children – 43, adults – 59, pregnant women – 34, older adults (over 65 years of age) - 14
Preschool children, school age children, adults, pregnant women and older adults
Does nutrition education work? If so, what are the successful elements across interventions? What are the implications for nutrition education program design implementation, policy and research?
Preschool children: 1. Involvement of parents/family, either as major recipients of program or in conjunction with program offered to pre-school child is extremely important. 2. Behaviourally focussed approach, specifically targeting children's behaviours, shown to increase preference and consumption without didactic teaching. 3. Use of developmentally appropriate learning experiences and materials is critical to success. 4. Food-based activities have been successful in increasing children's food preferences. 5. Activity-based teaching strategies that encourage interaction with real-world objects are essential. School age children: 1. Nutrition education more likely to be effective when behaviourally focussed. 2. More likely to be effective when educational strategies are employed that are directly relevant to a behaviourally focus and derived from appropriate theory and research. 3. Interventions need to devote adequate time and intensity to nutrition education to be effective. 4. Family involvement enhances the effectiveness of programs for younger children. 5. Incorporation of a self-evaluation or self-assessment and feed-back component is effective in interventions for older children. 6. Effective nutrition education includes intervening in the school environment. 7. Interventions in the larger community can enhance school nutrition education. Adults: Communications: 1. Communications using the media are effective if personally relevant to issues people confront and choices. 2. Use of systematic, audience-based planning framework, can greatly facilitate the process of designing and delivering community-based nutrition education relevant to intended customers. 3. Mass media health campaigns, based on social marketing processes, can increase awareness
Authors do not differentiate between countries of studies included. However, review has much reference to US interventions and focuses on the US predominantly Relevance score: B
145

of anticipated consequences of diet and knowledge about behaviours to reduce risk. Interpersonal motivational and behavioural change strategies: 1. Individualised interpersonal counselling and education is likely to be effective in facilitating behavioural change. 2. Educational strategies for individuals and groups are more likely to be motivational if information emphasises personal consequences of behaviours and other motivators and reinforcements relevant to needs and interests of target group. 3. Behavioural change strategies based on social learning theory and behavioural self-management are likely to be effective. Sites: 1. Point of choice interventions in grocery stores and eating establishments can be highly effective in changing purchase intentions and behaviour (but probably only while intervention lasts). 2. Worksite intervention strategies have increasingly moved from using the clinical approach, where high-risk individuals identified and treated, to using public health approach directed at all individuals. 3. Comprehensive community nutrition education/health promotion activities involving mass media, small groups, point-of-purchase information, and others in concert may be moderately effective in reducing diet-related disease risk. Community activation and organisation: Extensive involvement of existing leadership from the beginning of a community intervention and ongoing involvement of organisations and volunteers at each step of the process, so that programs become infused into life of community, are likely to have long-term effectiveness. Pregnant women: Methods and timing of interventions: 1. Nutrition counselling and classes that focus on a pregnant woman’s specific behaviours, as determined via individualised assessment, have the highest chances of success. 2. Prenatal classes can also be effective, if they are coupled with individual follow-up sessions to reinforce and maintain behaviour, if affective-based educational strategies are used, or if they address the specific needs of the target group. 3. Other media channels do not appear to be as effective as individualised personal nutrition education in improving maternal diets during pregnancy. 4. The decision to breast feed is made early. 5. Prenatal exposure to information about the benefits of breast feeding with respect to the health of the infant, convenience for the mother, and problems and myths concerning breastfeeding positively influences the intention and initiation of breast feeding. 6. An educational programme that includes women’s partners and provides incentives for participation can have a dramatic effect in motivating women to breastfeed. 7. Intensive in-hospital bedside counselling and follow-up support strategies increase
146

breast feeding duration. 8. The use of peer breastfeeding counsellors and provision of home support can improve breast feeding duration. Older adults: 1. The use of personalised approaches, such as self-assessment of nutritional status or behaviours and comparison with recommendations, is effective as a starting point for nutrition education. Such an approach is useful in group settings. 2. The use of a behavioural approach is key. Such an approach includes individual self-assessment techniques, such as goal setting, problem solving, enhancement of self-efficacy and social support. 3. Active participation is essential, particularly when combined with a behavioural approach. 4. Attention to motivators and reinforcements is of primary importance, but is often neglected. Older adults, like other adults, already possess a great deal of nutrition information that they do not put into practice. 5. An empowerment philosophy that includes enhancing personal choice, control and social support should be used. 6. Subgroups of older adults need to be identified and targeted. The age, gender and cultural background of older adults need to be considered when developing nutrition education programmes. Those with special needs, such as the very frail, where inadequate nutrition is a problem, diabetics, and others also need to be recognised. 7. Sensitivity to age-related physical changes is necessary.
Contributors to the Cochrane Collaboration and the Campbell Collaboration 2000
Review of reviews Level: 2 Review quality: + No. of studies: N/A
Not stated What is the evidence on heart disease, stroke and cancer that can be used in the public health arena?
Heart disease and stroke: 1) Higher cigarette prices reduce cigarette consumption. However, the effects of increasing cigarette prices differ across demographic groups, more marked reduction is shown with increasing price amongst women and young people. In the poorest groups an increase in price produces significant hardship for those who do not curtail their consumption. 2) Adverse dietary patterns are reinforced by poverty as pricing policy encourages purchase and consumption of cholesterol raising diets. By extending VAT to the main sources of dietary saturated fat, cardoivascular disease could be avoided and tax revenue generated. However, it is unclear whether this will improve poor people's diets or worsen health by increasing poverty. 3) School interventions: interactive programmes are more effective at changing behaviour than non interactive ones Cancer: 1) No systematic reviews have been identified that examine targeting health information on at risk groups on cancer rates. 2) Community intervention programmes in school children, adolescents and adults found the most sucessful interventions for increasing fruit and vegetable consumption were those that were part of a multi component programme. Successful interventions also included education directed at
Includes UK studies Relevance score: A
147
behaviourial change, were over a longer period of time period with multiple contacts made with participants and used a message specifically targeted to fruit and vegetables rather than nutrition in general. 3) Public health campaigns on diet, exercise and smoking are likely to be more effective if they take into account variations accross cultural groups. 4) Evidence suggests that school health promotion inititatives can have a positive impact on children's health and behaviour but do not do so consistently. Most are able to increase knowledge but changing children's attitudes and behaviour is harder to achieve. 5) Free telephone quit lines, as part of an antismoking campaign, can improve quit rates.
Cyarto E V, Moorhead G E & Brown W J 2004
Systematic review (RCTs and non-RCTs) Level: 2 Review quality: - No. of studies: Physical activity (PA) review – 8, progressive resistance training (PRT) review - 21 RCTs
Individuals aged 60 years or more
What is the evidence relating to physical activity intervention studies in older people?
PA Review: Most studies demonstrated success in increasing PA in older people with only 2 studies reporting negative findings. All general practice interventions reported positive effect on PA levels with the most effective study maintaining contact with participants for the longest duration and tailoring the intervention. PRT Review: With exceptions, significant increases in strength was reported for healthy participants, those with chronic disease, and the frail or physically limited. Positive effects on disease outcomes were also demonstrated including diabetic glycaemic control, osteoarthritis and chronic heart failure (mixed results for bone mineral density). Most studies demonstrated positive impact of PRT on functional measures although results were sometimes statistically limited.
PA review included 2 studies from the UK whereas PRT review did not include any UK studies. Relevance score: A
DeHaven M et al 2004
Narrative synthesis Level: 2 Review quality: - No. of studies: 53
32.1% did not target a specific population, but if it did it tended to be African Americans and adults.
Are health programmes in faith-based organisations effective?
Most programmes focussed on primary prevention (50.9%), usually patient education, in the area of general health maintenance, CV health or cancer. Only just over half of the articles reported outcomes (52.8%). Programmes focussing on heart disease, weight/nutrition, breast cancer, prostate cancer, and smoking cessation achieved statistically significant effects in terms of (respectively) reducing cholesterol and blood pressure levels, increasing fruit/vegetable consumption and reducing weight, increased use of mammography and breast self-examination, increasing knowledge about prostate cancer, and increasing readiness to change regarding smoking cessation. 91% of these programmes were targeted at African Americans. 2 of 4 ‘faith-based’ programmes (“developed as part of a congregation’s health ministry”) showed significant effects (decreased mental illness symptoms). 5 out of 6 ‘collaborative’ programmes showed intervention effects with
Non UK studies. Most results were based on African Americans. Relevance score: B
148
improvements in overall health status, increases in fruit/vegetable consumption and decreases in weight and blood pressure.
Dishman R K & Buckworth J 1996
Quantitative synthesis (meta-analysis) Level: 2 Review quality: - No. of studies: 127
Healthy adults and CHD patients, and those at risk of CHD and other chronic diseases
What is the efficacy of physical activity interventions and what are the factors that moderate their success?
Interventions for physical activity have a moderately large effect, equivalent to improving success from 50% without intervention to 70-88%. Effect sizes of the interventions did not differ by gender, age or race. Effects were larger among healthy subjects than patients, although small effects were observed in studies of CHD patients, those at high risk for CHD or other chronic diseases. Interventions incorporating behaviour modification approaches had larger effect sizes than other approaches. Effects were larger among studies using mediated approaches than those using face-to-face delivery. Interventions in community settings and those delivered to groups had larger effects than those in schools and other settings, or delivered to individuals, family and to individual + group combination. Effects were larger when physical activity was not supervised, compared with supervised programme. Effects were unrelated to the duration of the intervention and the follow up. Effects were larger for interventions encouraging active leisure time than those prescribing strength or aerobic exercise. Effect sizes did not differ according to frequency or duration, however, low intensity activity interventions had larger effects than higher intensity interventions.
Non-UK studies. Relevance score: B
Dobbins M et al 2001
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 19
Children and adolescents; school based
What is the effectiveness of school-based interventions in promoting physical activity and school attending children and adolescents aged 6 to 18 years?
There is conflicting evidence regarding whether or not school based interventions to promote physical activity in primary children have a positive effect on lifestyle behaviours including physical activity rates (2 positive, 1 no effect), duration of physical activity (3 positive, 3 no effect) and television viewing (2 positive, 1 approaching significance). It is unclear which interventions are likely to be most effective, although there is some indication that programmes of longer duration may be more likely to affect physical activity duration. There is very limited evidence (tested by only one study) to suggest that children exposed to school based interventions lead more active lives as adults. There is conflicting evidence regarding whether or not school based interventions increase physical activity rates in adolescents (1 positive, 1 no effect). There is very limited evidence that school based interventions increase physical duration in adolescent girls (one positive) and no evidence for boys. There is no evidence of the impact on school based interventions on television viewing in adolescents. Generally school based interventions are not effective in altering most physical health status
1 UK study Relevance score: A
149

indicators. However, few projects measured these secondary outcomes. Edwards N, Aubin P& Morrison M 2000
Systematic review (RCTs and non-RCTs) Level: 2 Review quality: ++ No. of studies: 19
Women and their families
What is the effectiveness of strategies to reduce smoking relapse during the postpartum period? Do smoking relapse interventions that target the partner or family members yield any improved benefits over smoking relapse interventions targeting the woman alone? What is the effectiveness of smoking relapse interventions during pregnancy vs. interventions during pregnancy and postpartum or during the postpartum period only?
Postpartum interventions: 1/1 study showed a significantly lower relapse rate at 6 months postpartum but this was not maintained at 12 months. The intervention was multicomponent, involved multiple levels of the healthcare system and was delivered over 3 months. Prenatal interventions: 2/3 studies showed no intervention effect on quit rates. Borderline studies: Mixed effect were seen. One study compared extended and care group compared to minimal care at 6 months postpartum. Extended care resulted in significantly lower relapse rates. Studies specificlly examined spontaneous quitters as a sub group. All the women in the effective postpartum study were spontaneous quitters. One borderline study showed that strategies had greater effects on spontaneous quitters than those who quit with the help of an intervention. The role of partners: limited or absent parter involvement in interventions was seen.
Unable to tell where all studies performed Relevance score: B
Engbers LH et al 2005
Systematic review (RCTs) Level: 2 Review quality: ++ No. of studies: 13
Adults (undergoing worksite health promotion programs)
What is the effectiveness of worksite health promotion programs (WHPPs) with environmental modifications on physical activity, dietary intake, and related outcomes?
Physical activity (PA): Three studies of relatively low quality – inconclusive evidence on effectiveness on PA of WHPPs including environmental modifications. Diet: 6 of the 13 studies measured effect of WHPP on fruit and vegetable intake and all demonstrated significant positive changes compared to controls. For 6 studies that measured the effect of WHPP on fat intake all but one found significant decrease in fat intake. No differences were observed for the study that measured the impact of WHPP on fibre intake. Health risk indicators: None of the 4 studies evaluating the effect of WHPPs on cholesterol levels demonstrated significant effects. Of the 3 studies evaluating the effect of WHPPs on Body Mass Index (BMI), only 1 study demonstrated a small significant increase. No significant changes were found in the only study that evaluated the effects of WHPP on blood pressure.
Not specified where studies were conducted. Relevance score: B
Eysenbach G et al 2004
Systematic review (including at least one
Adults (using virtual community
What is the evidence on the effects on health and
The review includes 12 studies on depression, 12 on social support and 3 on health care use, these are not reported here.
Review does not state which countries studies
150
RCT) Level: 2 Review quality: - No. of studies: 38
interventions focusing on emotional and social support, health education, or health-related behaviour change)
social outcomes of computer based peer to peer communities and electronic self-support groups, used by people to discuss health related issues remotely?
Weight loss or healthy body-weight interventions (9 studies): the findings were mixed but were mainly non significant. Diabetes intervention (5 studies): there was a significant improvement in glycosylated haemoglobin in one before-and-after study. Smoking cessation (6 studies): the levels of abstinence following the intervention were variable. 1 RCT found no significant improvement in the intervention group over the comparison group. 1 RCT found some small differences, although significance levels were not reported.
from. Relevance score: B
Fletcher A & Rake C 1998
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 23
Free living (i.e. not institutionalised) individuals over 65
What is the evidence from studies of interventions to promote health eating in elderly people living in the community?
Nutrition interventions in elderly people in the community meal setting: A small RCT and a small uncontrolled study showed post-intervention benefits. The RCT found changes in self reported behaviour and the controlled study found changes in serum lipids. The control study showed no effects but was very weak and the control group was possibly contaminated. The reviewers' state that large benefits seen in the RCT (62% eating adequately intervention vs 9% control) were likely to be due to the focus of high-risk individuals with nutritionally inadequate diets, the use of a motivational group-led model and emphasis on improving vitamin, protein and mineral intake. Nutrition interventions in elderly people in communal settings: 9 studies provide very weak evidence of effect but all pointing in the direction of improved behaviour following intervention. Participants were mostly women. A range of income groups were represented. Nutrition interventions in the elderly population living in the community: No RCTs. 2 controlled and 4 uncontrolled studies (3 of the latter post-intervention data only). 1 controlled study showed no evidence of effectiveness but small differences were observed which the study was underpowered to detect. The other controlled study showed very large (>50%) increase in wholegrain bread sales in participants randomised to community organisation strategy (including the media, community events, bread pricing and social marketing) compared to a patient education system (leaflets handed out by local physicians) or control. Nutrition interventions as part of health promotion interventions: 4 RCTs, only 1 showed effectiveness. The intervention was based on personal computerised feedback to lifestyle questionnaires.
No studies in UK, 21 US. The best conducted studies were in the context of adding health promotion to insurance policies in the US. Relevance score: B
Foster C & Hillsdon M 2004
Systematic review (including 1 RCT) Level: 2
Adults What is the effect of environmental interventions to increase health-enhancing physical activity
Changing the environment: Three studies addressed the impact of physical changes to the working environment on HEPA or physical fitness and showed small increases in fitness. 1/3 studies was an RCT. The intervention approached but did not reach statistical significance (p=0.08). 2/3 studies were carried out in military settings and the 3rd was
Almost half the studies conducted in the UK Relevance score: A
151
Review quality: - No. of studies: 19
(HEPA)? carried out in a factory. Stair interventions: 16 before and after studies studies have reported the results of written media (e.g. posters, riser banners) to prompt stair use rather than esculators or lifts. Most only demonstrated a short term effect of up to 3 months, with only 1 seeing an effect 6 months after baseline. 2 studies found that younger people were more likely to respond to prompts and that an in one intervention the effect was greater in a shopping center than a railway station. 2 studies demonstrated differences between the sexes, with one finding that fewer women chose to use the stairs and the other finding that women were more likely to use the stairs. 1 study found that poster size was related to effectiveness and also that stair risers had a greater effect than posters alone.
Gepkens A & Gunning-Schepers L J 1996
Systematic review (narrative synthesis) Level: 2 Review quality: - No. of studies: 129
Not stated How effective are interventions to reduce socioeconomic health differences? What are the possible conditions for success?
Structural measures (mostly financial acessability, USA): 11 effective, 4 dubious, 1 ineffective. Interventions within existing healthcare services: 5 effective, 4 dubious, 3 ineffective. Health education: Providing information: 6 effective, 6 dubious, 4 ineffective. Providing information and personal support: 32 effective, 12 dubious, 5 ineffective. Health promotion and structural measures: 2 effective, 1 dubious. Remainder 2 effective, 1 dubious. Evaluating the health education interventions shows that programmes providing only information seem to be especially effective in the higher SES groups whereas programmes providing infomration in combination with personal support (for example by a health visitor) seem to be the most effective type on intervention for all SES groups. Most interventions have been aimed at increasing knowledge or behaviour rather than health outcomes.
A relatively large proportion of studies (20% published, 26% unpublished) were carried out in the UK. However, most structural interventions were aimed at the finanancial accessability of health services in the USA. Relevance score: A
Gorin SS & Heck JE, 2004
Meta-analysis (of RCTs and quasi-experimental studies) Level: 2 Review quality: - No. of studies: 37
Health professionals Are somee health professions more effective in providing smoking cessation? Which intervention and study characteristics explain most variation in intervention effects?
Physician and health professional team interventions are effective in smoking cessation rates. Effectiveness of nurse and dentist interventions are not statistically significant. Physician and dentist interventions are more effective than nurse interventions (however, small dentist study number may caution comparability with this group). Funnel plot analysis suggested that publication bias may have occurred.
Only included studies from US. Does not include pharmacist interventions which may be more significant in the UK compared to US (where review was conducted) Relevance score: B
Hajek P et al, 2005
Systematic review (of RCTs or quasi-randomised CTs)
Smokers Do specific interventions for relapse prevention reduce the proportion of
They detected no benefit of brief and skills-based relapse prevention interventions for women who had quit smoking due to pregnancy, or for smokers undergoing a period of brief abstinence. They also failed to
Includes 2 UK studies Relevance score: A
152

Level: 1 Review quality: - No. of studies: 40
recent quitters who return to smoking?
detect significant effects in trials in other smokers who had quit on their own or with a formal programme. Amongst trials recruiting smokers and evaluating the effect of additional relapse prevention components they also found no evidence of benefit in any subgroup. They did not find that providing training in skills thought to be needed for relapse avoidance reduced relapse, but most studies did not use experimental design best suited to the task, and had limited power to detect expected small differences between interventions.
Harden A, Weston R & Oakley A, 1999
Systematic review (narrative synthesis) (including at least one RCT) Level: 3 Review quality: + No. of studies: 27
Young people aged 11-24 years old
What is the effectiveness of peer-delivered health promotion in promoting young people's health? What characteristics differentiate peer-delivered interventions from teacher-delivered interventions?
Of the outcome studies, seven were effective for behavioural outcomes, three were effective for 'proxy outcomes', 1 was ineffective and 1 was unclear. Specifically for smoking, 3 were effective for behavioural outcomes, 1 was ineffective and 1 was unclear. There was no clear relationship between the characteristics of the interventions and effectiveness. Of the process evaluations the main results were as follows: in terms of acceptability, most young people expressed positive views on peer-delivered health promotion and negative views were rarely documented. In terms of implementation issues, conflict between the philosophy of peer education and the school environment was identified as a barrier and such organisational contexts made working with young people challenging. There was some evidence that peer-delivered interventions were more likely to be effective in young women.
No outcome studies were UK-based. Relevance score: A
Hey K & Perera R, 2005
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 15
Smokers Do competitions, contests and incentives reduce the prevalence of smoking and relapse? Does the amount and type of incentive affect cessation and relapse prevention? Do incentives improve recruitment to smoking cessation programmes, both within the community and within the workplace? Does the amount and type of incentive affect recruitment?
Competitions and incentives offer smokers who quit for a minimum period the change to win money or prizes. They do not appear to help smokers to quit in the medium to long-term. Smokers may quit while they take part in the competition or receive rewards for quitting, but do no better than unassisted quitters once the rewards stop. The type of reward and whether or not the smokers put up their own money to take part make little difference to the success of the quit attempt. Competitions and rewards may attract more people to make a quit attempt than might otherwise do so, but cessation rates remain the same as for non-contestants.
Mostly US studies. Two-thirds based in worksites. The structure of the US healthcare system obliges employers to cover health insurance for workers, so have more incentive for workers to quit smoking. Relevance score: A
153
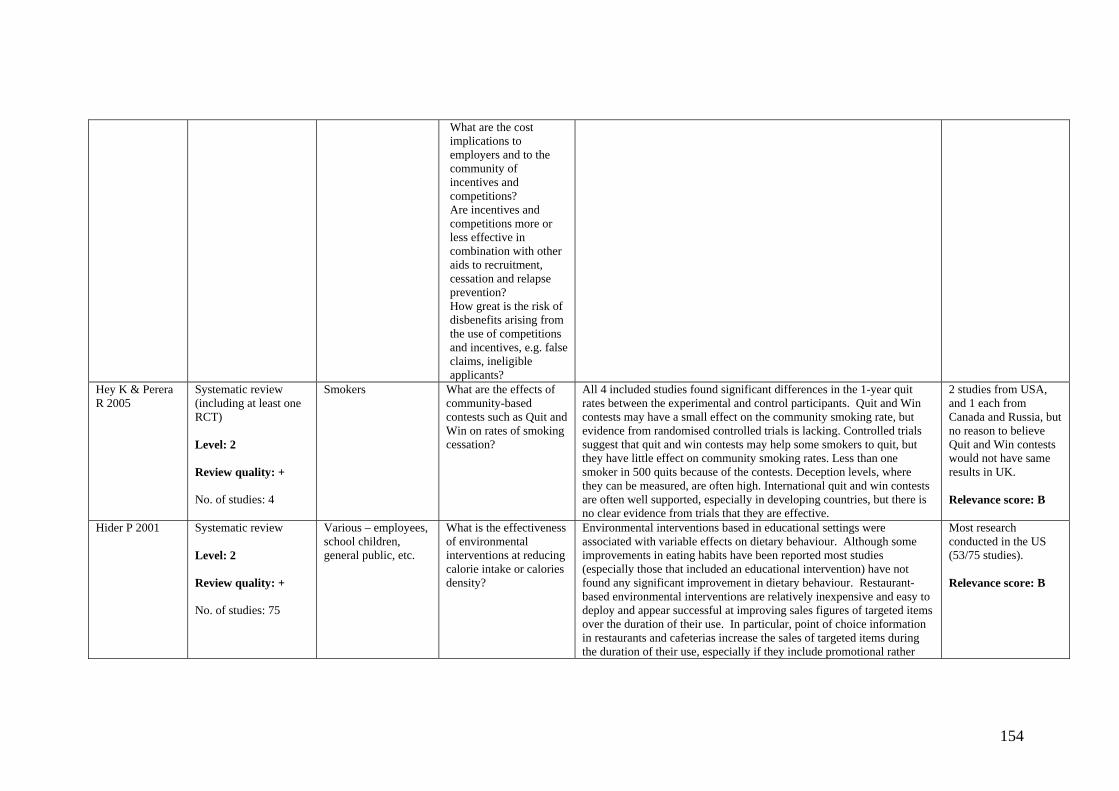
What are the cost implications to employers and to the community of incentives and competitions? Are incentives and competitions more or less effective in combination with other aids to recruitment, cessation and relapse prevention? How great is the risk of disbenefits arising from the use of competitions and incentives, e.g. false claims, ineligible applicants?
Hey K & Perera R 2005
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 4
Smokers What are the effects of community-based contests such as Quit and Win on rates of smoking cessation?
All 4 included studies found significant differences in the 1-year quit rates between the experimental and control participants. Quit and Win contests may have a small effect on the community smoking rate, but evidence from randomised controlled trials is lacking. Controlled trials suggest that quit and win contests may help some smokers to quit, but they have little effect on community smoking rates. Less than one smoker in 500 quits because of the contests. Deception levels, where they can be measured, are often high. International quit and win contests are often well supported, especially in developing countries, but there is no clear evidence from trials that they are effective.
2 studies from USA, and 1 each from Canada and Russia, but no reason to believe Quit and Win contests would not have same results in UK. Relevance score: B
Hider P 2001 Systematic review Level: 2 Review quality: + No. of studies: 75
Various – employees, school children, general public, etc.
What is the effectiveness of environmental interventions at reducing calorie intake or calories density?
Environmental interventions based in educational settings were associated with variable effects on dietary behaviour. Although some improvements in eating habits have been reported most studies (especially those that included an educational intervention) have not found any significant improvement in dietary behaviour. Restaurant-based environmental interventions are relatively inexpensive and easy to deploy and appear successful at improving sales figures of targeted items over the duration of their use. In particular, point of choice information in restaurants and cafeterias increase the sales of targeted items during the duration of their use, especially if they include promotional rather
Most research conducted in the US (53/75 studies). Relevance score: B
154

than just educational messages. Mixed educational and environmental interventions located at workplaces can effectively improve dietary habits although not all programmes have been successful. Providing shoppers with electronic feedback about their purchases appears a promising supermarket-based intervention to reduce calorie intake. Other environmental interventions in supermarkets have generally provided positive results and most have at least been associated with significant increases in the sales of selected items. In recent trials community based environmental interventions, despite their potential to improve the health status of the whole population, have been associated with only modest results.
Hillsdon M et al 1995
Systematic review of RCTs Level: 1 Review quality: + No. of studies: 10
Health, free living adults
What is the evidence of effective promotion of physical activity?
Location of exercise: One study compared home and facility based exercise and found that adherence was significantly higher in the home based groups. Another home based study showed a positive relationship between the convenience of exercise and its adoption and maintenance which may explain why home based exercise seems preferable. Frequency of exercise: At the end of the trials those subjects still exercising were usually exercising around twice per week. 1 study tested prescribed regimes of 5/week vs 3/week and found that after 2 years adherence was higher in the 3/week group. Self monitoring: 2 studies found greater levels of exercise in subjects randomised to self monitoring, whereas one did not. However, in the latter study only 55% of partiicpants completed their records. Relapse Prevention Training: 1 study showed no difference between relapse prevention training compared to reinforcement strategies. Another study showed that relapse prevention training increased exercise levels in subjects exercising alone but not in those exercising in a group. Professional contact: 1 study found that subjects randomised to follow up telephone prompting carried out more physical activity than those who did not. Significantly higher levels of exercise were achieved in groups with higher prompt frequency.
All studies carried out in the USA. Relevance score: B
Jepson R 2000 Review of reviews Level: 2 Review quality: + No. of studies: N/A
How effective are interventions to change health related behaviours? [NB. Six behaviours were included in the review but data has been
Smoking Reasonable effect: physician advice, smoking cessation programmes implemented in pregnancy, advice given by niurses, group programmes and individual smoking cessation. Modest effect (evidence not strong): mass media campaigns, school-based programmes, simple physician advice, self help materials. Likely to be ineffective: local ordinances alone as tobacco obtained from other sources. Not enough evidence of effect: Prevention of smoking in public places. Exercise Reasonable effect: GP advice, behaviour modification produces larger
The majority of research on smoking and exercise was USA based; countries where diet-based research was conducted unknown.
155
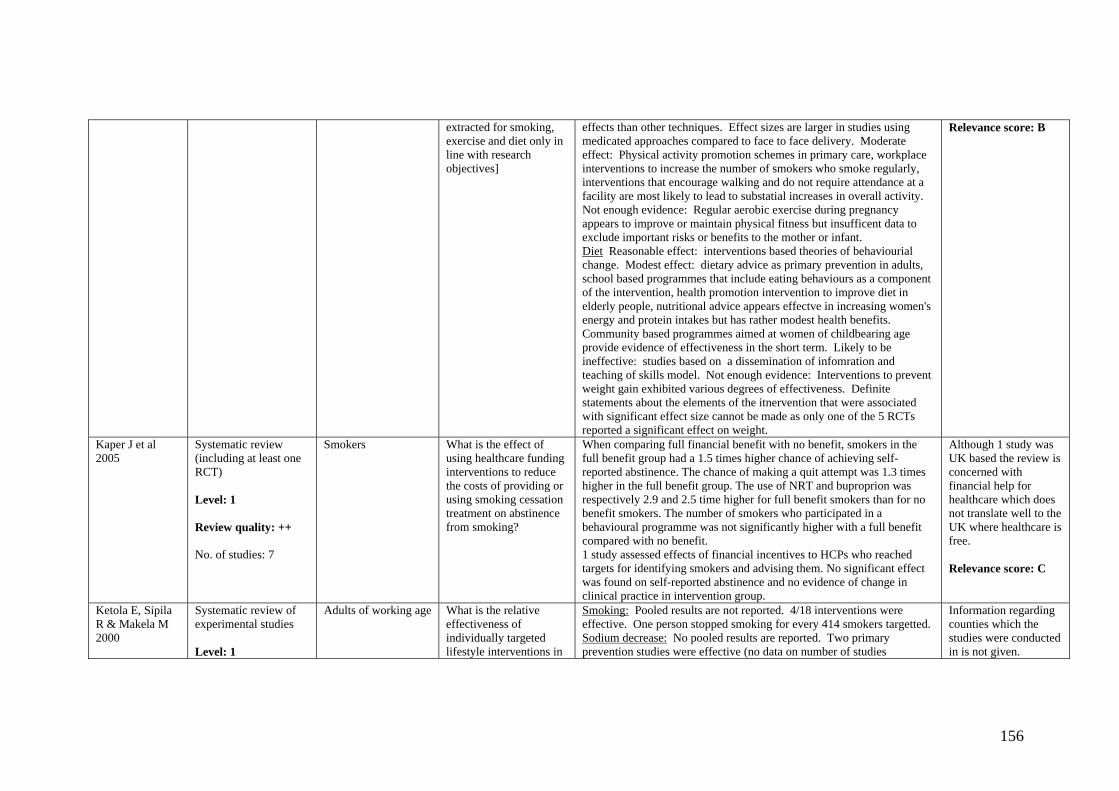
extracted for smoking, exercise and diet only in line with research objectives]
effects than other techniques. Effect sizes are larger in studies using medicated approaches compared to face to face delivery. Moderate effect: Physical activity promotion schemes in primary care, workplace interventions to increase the number of smokers who smoke regularly, interventions that encourage walking and do not require attendance at a facility are most likely to lead to substatial increases in overall activity. Not enough evidence: Regular aerobic exercise during pregnancy appears to improve or maintain physical fitness but insufficent data to exclude important risks or benefits to the mother or infant. Diet Reasonable effect: interventions based theories of behaviourial change. Modest effect: dietary advice as primary prevention in adults, school based programmes that include eating behaviours as a component of the intervention, health promotion intervention to improve diet in elderly people, nutritional advice appears effectve in increasing women's energy and protein intakes but has rather modest health benefits. Community based programmes aimed at women of childbearing age provide evidence of effectiveness in the short term. Likely to be ineffective: studies based on a dissemination of infomration and teaching of skills model. Not enough evidence: Interventions to prevent weight gain exhibited various degrees of effectiveness. Definite statements about the elements of the itnervention that were associated with significant effect size cannot be made as only one of the 5 RCTs reported a significant effect on weight.
Relevance score: B
Kaper J et al 2005
Systematic review (including at least one RCT) Level: 1 Review quality: ++ No. of studies: 7
Smokers What is the effect of using healthcare funding interventions to reduce the costs of providing or using smoking cessation treatment on abstinence from smoking?
When comparing full financial benefit with no benefit, smokers in the full benefit group had a 1.5 times higher chance of achieving self-reported abstinence. The chance of making a quit attempt was 1.3 times higher in the full benefit group. The use of NRT and buproprion was respectively 2.9 and 2.5 time higher for full benefit smokers than for no benefit smokers. The number of smokers who participated in a behavioural programme was not significantly higher with a full benefit compared with no benefit. 1 study assessed effects of financial incentives to HCPs who reached targets for identifying smokers and advising them. No significant effect was found on self-reported abstinence and no evidence of change in clinical practice in intervention group.
Although 1 study was UK based the review is concerned with financial help for healthcare which does not translate well to the UK where healthcare is free. Relevance score: C
Ketola E, Sipila R & Makela M 2000
Systematic review of experimental studies Level: 1
Adults of working age What is the relative effectiveness of individually targeted lifestyle interventions in
Smoking: Pooled results are not reported. 4/18 interventions were effective. One person stopped smoking for every 414 smokers targetted. Sodium decrease: No pooled results are reported. Two primary prevention studies were effective (no data on number of studies
Information regarding counties which the studies were conducted in is not given.
156

Review quality: - No. of studies: 42
primary and secondary prevention of CVD?
measuring this outcome). 1/2 single factorial secondary prevention studies were effective, the other having insufficient data for evaluation). 2/4 multifactorial secondary prevention studies were effective. Exercise: Results were not combined due to heterogeneous outcome measures. 10/16 interventions were effective.
Relevance score: B
Kramer M S & Kakuma R 2003
Systematic review Level: 1 Review quality: - No. of studies: 23
Pregnant women What are the effects of advice to increase or reduce energy or protein intake, or of actual energy or protein supplementation or restriction, during pregnancy on energy and protein intakes, gestational weight gain and the outcome of pregnancy?
In 5 trials involving 1134 women, nutritional advice to increase energy and protein intakes was successful in achieving those goals, but no consistent benefit was observed on pregnancy outcomes. In 13 trials involving 4665 women, balanced enery/protein supplementation was associated with modest increases in maternal weight gain and in mean birth weight, and a substantial reduction in risk of small for gestational age (SGA) birth. These effects did not appear greater in undernourished women. No significiant effects were detected on preterm birth, but significantly reduced risks were observed for stillbirth and neonatal death. In 2 trials involving 1076 women, high protein supplementation was associated with a small, nonsignificant increase in maternal weight gain but a nonsignificant reduction in mean birthweight, a significantly increased risk of SGA birth, and a nonsignificantly increased risk of neonatal death. In 33 trials involving 966 women, isocaloric protein supplementation was also associated with an increased risk of SGA birth. In 3 trials involving 384 women, energy/protein restriction of pregnant women who were overweight or exhibited high weight gain significantly reduced weekly maternal weight gain and mean birth weight but had no effect on pregnancy induced hypertension or pre-eclampsia.
6 studies performed in the UK Relevance score: A
Krummel DA et al 2001
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 51 (16 smoking, 19 physical activity, 8 diet, 8 multiple risk factors).
Adult women What interventions are effective in promoting cardiovascular health in women?
Smoking: Pregnancy and the postpartum period are opportune times to treat tobacco dependence in women. More intense interventions with individualised approaches yield the best outcomes. Most pregnant women who reduce/quit during pregnancy resume postpartum. Women are more likely to participate in community based programmes than men but are less likely to quit as a result. Physical activity: Behavioural strategies, such as daily self monitoring, feedback, contracts and incentives have been effective in study participants. Whether these changes in physical activity behaviour are sustained as a lifestyle change is unknown. Women respond better to lifestyle physical activity recommendations versus structured exercise regimens. Diet: Very few interventions have been tailored towards women. Multifactorial: no interventions were specifically tailored towards women.
Unable to tell where studies performed. Relevance score: B
Lancaster T & Stead L F 2004
Systematic review (including at least one
Smokers What is the effectiveness of advice from
Main result: Brief advice versus no advice (or usual care) increased the odds of quitting (evidence from 17 trials: OR=1.74, 95%CI: 1.48-2.05).
At least 12 studies were conducted in the
157

RCT) Level: 2 Review quality: ++ No. of studies: 39
physicians in promoting smoking cessation? Are minimal interventions by physicians more or less effective than more intensive interventions? What is the effectiveness of various aids to advice in promoting smoking cessation? What is the effect of anti-smoking advice on disease specific and all-cause mortality?
No conclusive evidence that effectiveness of physician advice varied depending on intensity of intervention, amount of follow-up, aids used in consultation (indirect comparisons). However, 1) Small advantage of intensive advice over minimal advice (direct comparison) but indications of some heterogeneity, 2) Small benefit of follow-up visits (direct comparison). Effectiveness of advice may be greater in populations with established disease versus smokers from unselected population (indirect comparison) but this is derived from a small number of trials. Only one study determined the effect of smoking on mortality (inconclusive evidence).
UK, with the majority conducted in Western countries (US, Canada, Australia). Relevance score: A
Lancaster T & Stead LF 2005
Systematic review of experimental studies Level: 1 Review quality: - No. of studies: 21
Smokers Is individual counselling more effective than no treatment or brief advice in promoting smoking cessation? Is individual counselling more effective than self help materials in promoting smoking cessation? Is a more intensive counselling intervention more effective than a less intensive intervention?
Individual counselling was more effective than control. In a subgroup of 3 trials where all participants received nicotine therapy the point estimate of effect was smaller and failed to reach significance. There was no evidence of a greater effect of intensive counselling compared to brief counselling (3 studies only).
2 UK studies, the rest USA. Relevance score: A
Lancaster T & Stead LF 2005
Systematic review of experimental studies Level: 1 Review quality: - No. of studies: 60
Smokers Are self help interventions better than no treatment in promoting smoking cessation? Do different forms of self help (written materials, audi and video tape) have equivalent
In 11 studies comparing posted self help materials to no intervention there was a pooled effect that just reached significance (OR 1.24, 95% CI 1.07-1.45, NNT 100). This analysis excluded 2 trials with strongly positive outcomes that introduced significant heterogeneity. 4 further trials in which controls received alternative written materials did not show benefit of the smoking cessation self help materials. In 5 trials where the materials were delivered in person rather than by post there was no evidence of a significant effect (OR 1.2, 95% CI, 0.96-1.49). In 11 trials in which self-help materials were tested as an adjunct to face to
Studies carried out in a large variety of countries including UK. Relevance score: A
158
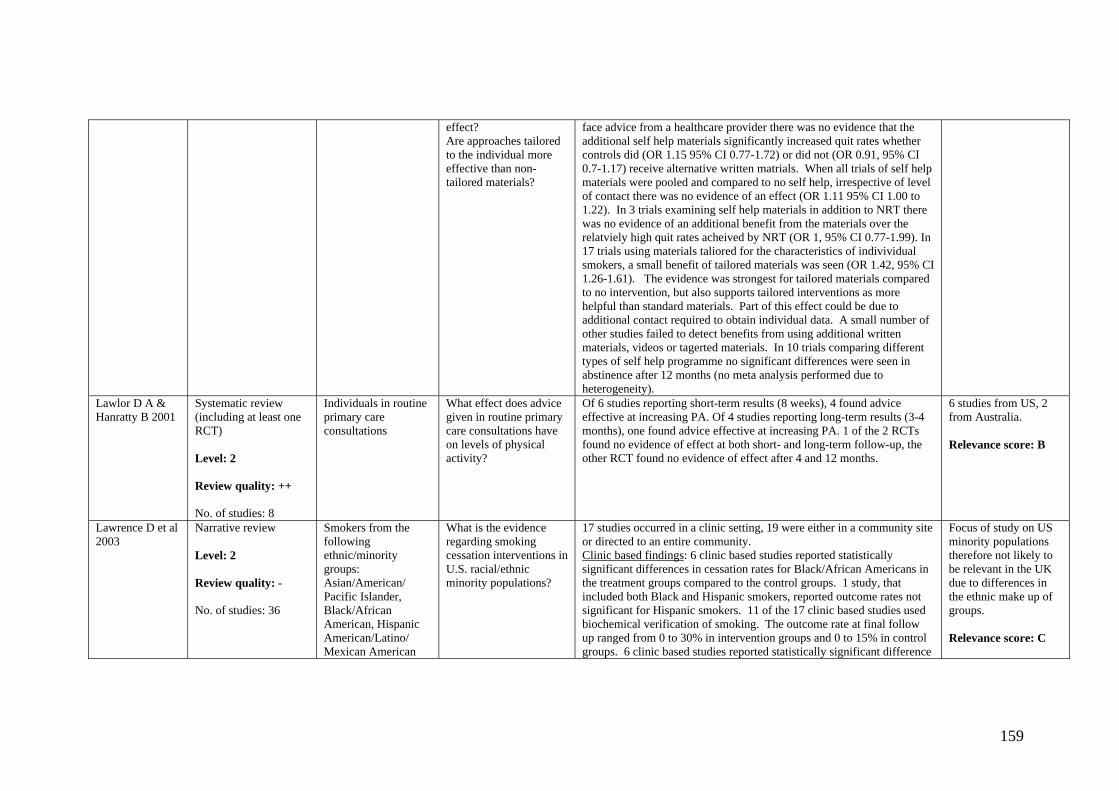
effect? Are approaches tailored to the individual more effective than non-tailored materials?
face advice from a healthcare provider there was no evidence that the additional self help materials significantly increased quit rates whether controls did (OR 1.15 95% CI 0.77-1.72) or did not (OR 0.91, 95% CI 0.7-1.17) receive alternative written matrials. When all trials of self help materials were pooled and compared to no self help, irrespective of level of contact there was no evidence of an effect (OR 1.11 95% CI 1.00 to 1.22). In 3 trials examining self help materials in addition to NRT there was no evidence of an additional benefit from the materials over the relatviely high quit rates acheived by NRT (OR 1, 95% CI 0.77-1.99). In 17 trials using materials taliored for the characteristics of indivividual smokers, a small benefit of tailored materials was seen (OR 1.42, 95% CI 1.26-1.61). The evidence was strongest for tailored materials compared to no intervention, but also supports tailored interventions as more helpful than standard materials. Part of this effect could be due to additional contact required to obtain individual data. A small number of other studies failed to detect benefits from using additional written materials, videos or tagerted materials. In 10 trials comparing different types of self help programme no significant differences were seen in abstinence after 12 months (no meta analysis performed due to heterogeneity).
Lawlor D A & Hanratty B 2001
Systematic review (including at least one RCT) Level: 2 Review quality: ++ No. of studies: 8
Individuals in routine primary care consultations
What effect does advice given in routine primary care consultations have on levels of physical activity?
Of 6 studies reporting short-term results (8 weeks), 4 found advice effective at increasing PA. Of 4 studies reporting long-term results (3-4 months), one found advice effective at increasing PA. 1 of the 2 RCTs found no evidence of effect at both short- and long-term follow-up, the other RCT found no evidence of effect after 4 and 12 months.
6 studies from US, 2 from Australia. Relevance score: B
Lawrence D et al 2003
Narrative review Level: 2 Review quality: - No. of studies: 36
Smokers from the following ethnic/minority groups: Asian/American/ Pacific Islander, Black/African American, Hispanic American/Latino/ Mexican American
What is the evidence regarding smoking cessation interventions in U.S. racial/ethnic minority populations?
17 studies occurred in a clinic setting, 19 were either in a community site or directed to an entire community. Clinic based findings: 6 clinic based studies reported statistically significant differences in cessation rates for Black/African Americans in the treatment groups compared to the control groups. 1 study, that included both Black and Hispanic smokers, reported outcome rates not significant for Hispanic smokers. 11 of the 17 clinic based studies used biochemical verification of smoking. The outcome rate at final follow up ranged from 0 to 30% in intervention groups and 0 to 15% in control groups. 6 clinic based studies reported statistically significant difference
Focus of study on US minority populations therefore not likely to be relevant in the UK due to differences in the ethnic make up of groups. Relevance score: C
159
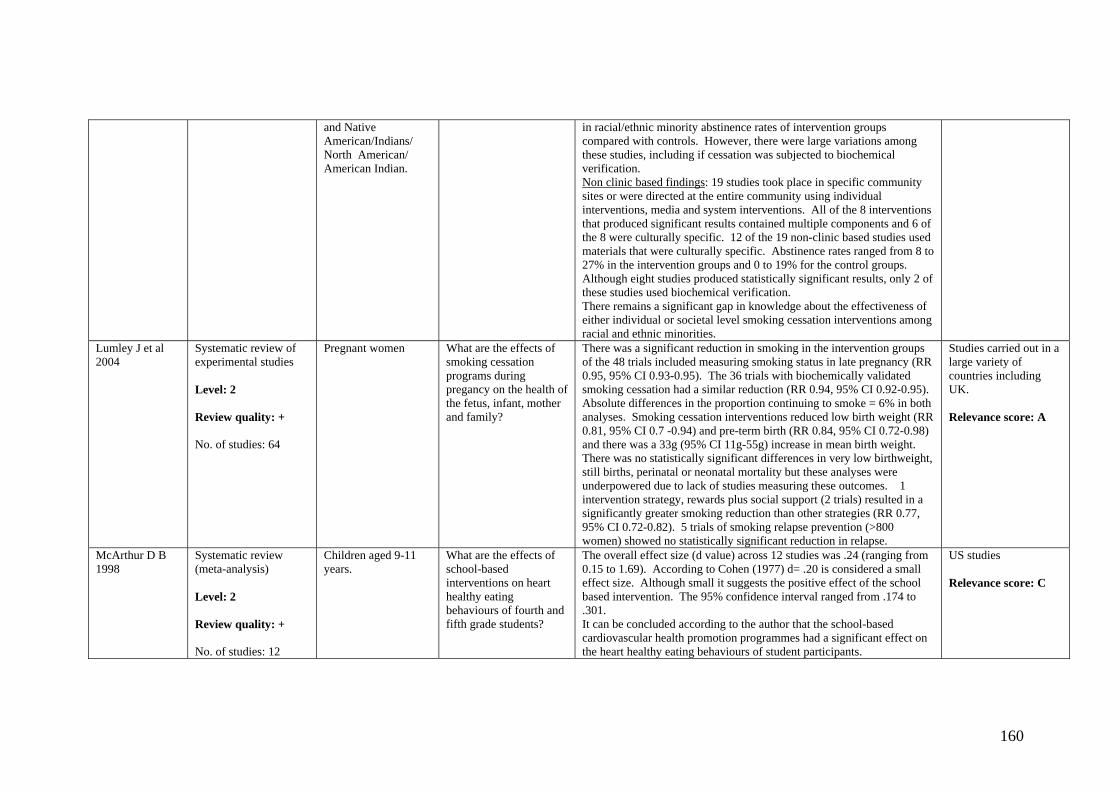
and Native American/Indians/ North American/ American Indian.
in racial/ethnic minority abstinence rates of intervention groups compared with controls. However, there were large variations among these studies, including if cessation was subjected to biochemical verification. Non clinic based findings: 19 studies took place in specific community sites or were directed at the entire community using individual interventions, media and system interventions. All of the 8 interventions that produced significant results contained multiple components and 6 of the 8 were culturally specific. 12 of the 19 non-clinic based studies used materials that were culturally specific. Abstinence rates ranged from 8 to 27% in the intervention groups and 0 to 19% for the control groups. Although eight studies produced statistically significant results, only 2 of these studies used biochemical verification. There remains a significant gap in knowledge about the effectiveness of either individual or societal level smoking cessation interventions among racial and ethnic minorities.
Lumley J et al 2004
Systematic review of experimental studies Level: 2 Review quality: + No. of studies: 64
Pregnant women What are the effects of smoking cessation programs during pregancy on the health of the fetus, infant, mother and family?
There was a significant reduction in smoking in the intervention groups of the 48 trials included measuring smoking status in late pregnancy (RR 0.95, 95% CI 0.93-0.95). The 36 trials with biochemically validated smoking cessation had a similar reduction (RR 0.94, 95% CI 0.92-0.95). Absolute differences in the proportion continuing to smoke = 6% in both analyses. Smoking cessation interventions reduced low birth weight (RR 0.81, 95% CI 0.7 -0.94) and pre-term birth (RR 0.84, 95% CI 0.72-0.98) and there was a 33g (95% CI 11g-55g) increase in mean birth weight. There was no statistically significant differences in very low birthweight, still births, perinatal or neonatal mortality but these analyses were underpowered due to lack of studies measuring these outcomes. 1 intervention strategy, rewards plus social support (2 trials) resulted in a significantly greater smoking reduction than other strategies (RR 0.77, 95% CI 0.72-0.82). 5 trials of smoking relapse prevention (>800 women) showed no statistically significant reduction in relapse.
Studies carried out in a large variety of countries including UK. Relevance score: A
McArthur D B 1998
Systematic review (meta-analysis) Level: 2 Review quality: + No. of studies: 12
Children aged 9-11 years.
What are the effects of school-based interventions on heart healthy eating behaviours of fourth and fifth grade students?
The overall effect size (d value) across 12 studies was .24 (ranging from 0.15 to 1.69). According to Cohen (1977) d= .20 is considered a small effect size. Although small it suggests the positive effect of the school based intervention. The 95% confidence interval ranged from .174 to .301. It can be concluded according to the author that the school-based cardiovascular health promotion programmes had a significant effect on the heart healthy eating behaviours of student participants.
US studies Relevance score: C
160
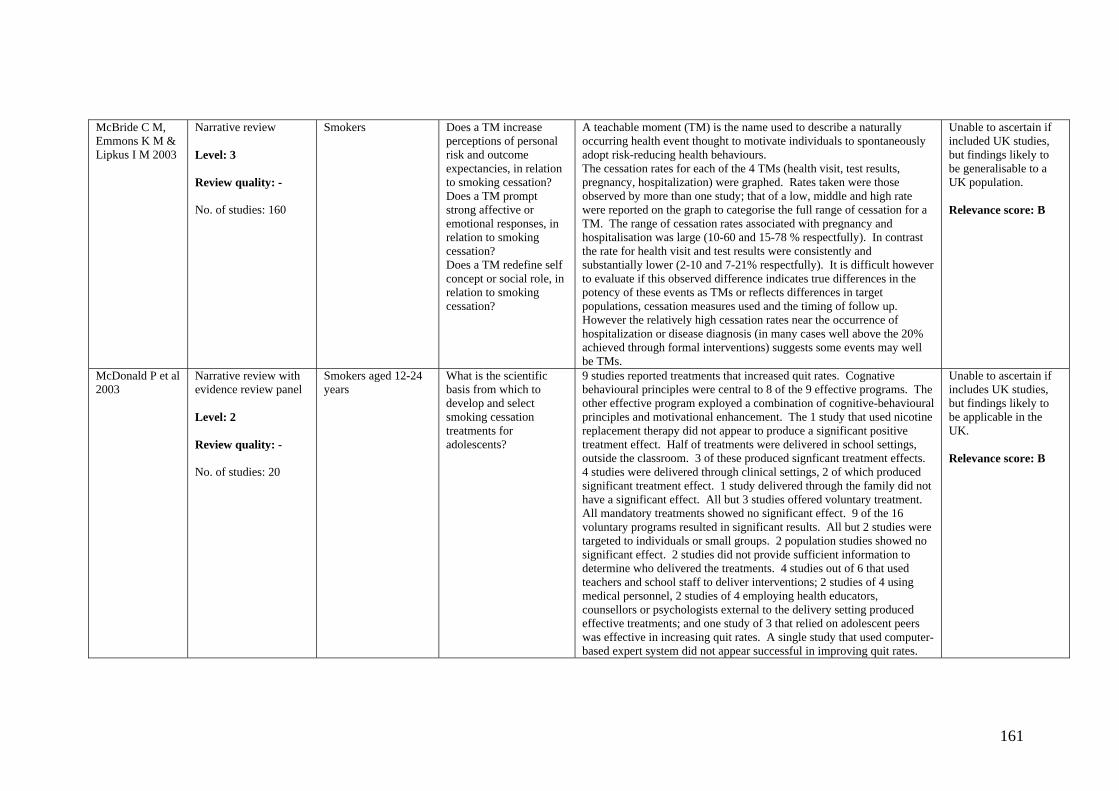
McBride C M, Emmons K M & Lipkus I M 2003
Narrative review Level: 3 Review quality: - No. of studies: 160
Smokers Does a TM increase perceptions of personal risk and outcome expectancies, in relation to smoking cessation? Does a TM prompt strong affective or emotional responses, in relation to smoking cessation? Does a TM redefine self concept or social role, in relation to smoking cessation?
A teachable moment (TM) is the name used to describe a naturally occurring health event thought to motivate individuals to spontaneously adopt risk-reducing health behaviours. The cessation rates for each of the 4 TMs (health visit, test results, pregnancy, hospitalization) were graphed. Rates taken were those observed by more than one study; that of a low, middle and high rate were reported on the graph to categorise the full range of cessation for a TM. The range of cessation rates associated with pregnancy and hospitalisation was large (10-60 and 15-78 % respectfully). In contrast the rate for health visit and test results were consistently and substantially lower (2-10 and 7-21% respectfully). It is difficult however to evaluate if this observed difference indicates true differences in the potency of these events as TMs or reflects differences in target populations, cessation measures used and the timing of follow up. However the relatively high cessation rates near the occurrence of hospitalization or disease diagnosis (in many cases well above the 20% achieved through formal interventions) suggests some events may well be TMs.
Unable to ascertain if included UK studies, but findings likely to be generalisable to a UK population. Relevance score: B
McDonald P et al 2003
Narrative review with evidence review panel Level: 2 Review quality: - No. of studies: 20
Smokers aged 12-24 years
What is the scientific basis from which to develop and select smoking cessation treatments for adolescents?
9 studies reported treatments that increased quit rates. Cognative behavioural principles were central to 8 of the 9 effective programs. The other effective program exployed a combination of cognitive-behavioural principles and motivational enhancement. The 1 study that used nicotine replacement therapy did not appear to produce a significant positive treatment effect. Half of treatments were delivered in school settings, outside the classroom. 3 of these produced signficant treatment effects. 4 studies were delivered through clinical settings, 2 of which produced significant treatment effect. 1 study delivered through the family did not have a significant effect. All but 3 studies offered voluntary treatment. All mandatory treatments showed no significant effect. 9 of the 16 voluntary programs resulted in significant results. All but 2 studies were targeted to individuals or small groups. 2 population studies showed no significant effect. 2 studies did not provide sufficient information to determine who delivered the treatments. 4 studies out of 6 that used teachers and school staff to deliver interventions; 2 studies of 4 using medical personnel, 2 studies of 4 employing health educators, counsellors or psychologists external to the delivery setting produced effective treatments; and one study of 3 that relied on adolescent peers was effective in increasing quit rates. A single study that used computer-based expert system did not appear successful in improving quit rates.
Unable to ascertain if includes UK studies, but findings likely to be applicable in the UK. Relevance score: B
161
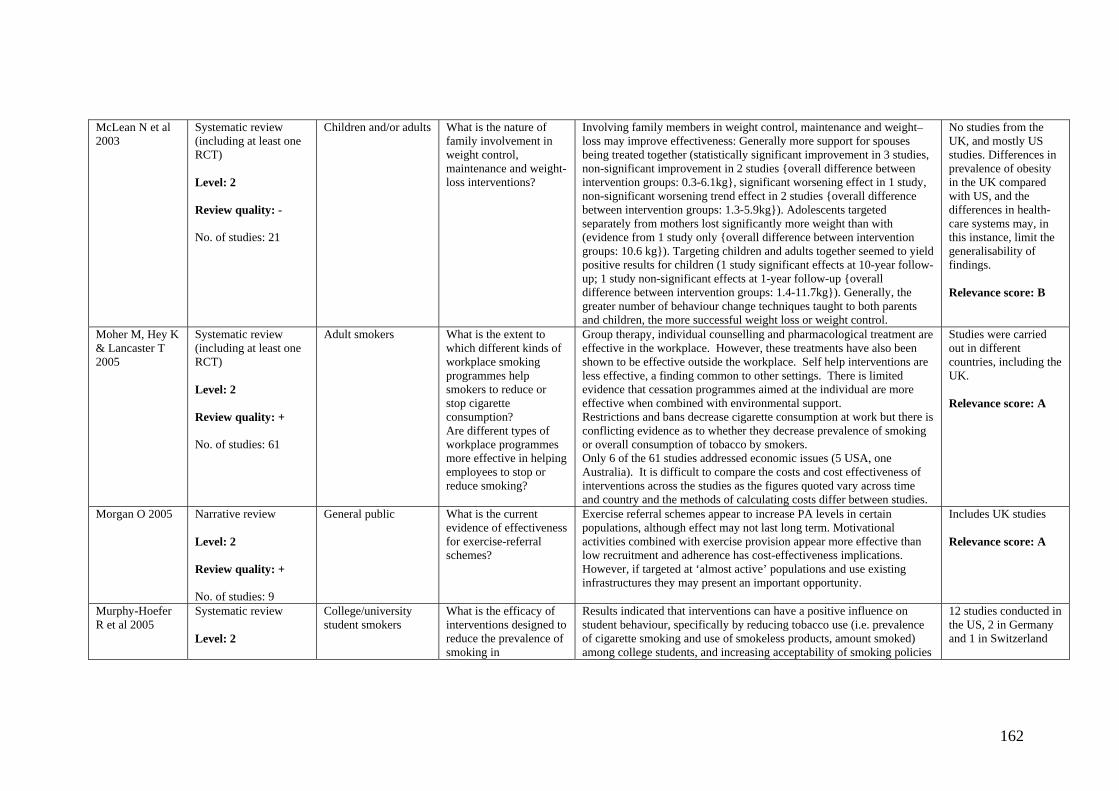
McLean N et al 2003
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 21
Children and/or adults What is the nature of family involvement in weight control, maintenance and weight-loss interventions?
Involving family members in weight control, maintenance and weight–loss may improve effectiveness: Generally more support for spouses being treated together (statistically significant improvement in 3 studies, non-significant improvement in 2 studies {overall difference between intervention groups: 0.3-6.1kg}, significant worsening effect in 1 study, non-significant worsening trend effect in 2 studies {overall difference between intervention groups: 1.3-5.9kg}). Adolescents targeted separately from mothers lost significantly more weight than with (evidence from 1 study only {overall difference between intervention groups: 10.6 kg}). Targeting children and adults together seemed to yield positive results for children (1 study significant effects at 10-year follow-up; 1 study non-significant effects at 1-year follow-up {overall difference between intervention groups: 1.4-11.7kg}). Generally, the greater number of behaviour change techniques taught to both parents and children, the more successful weight loss or weight control.
No studies from the UK, and mostly US studies. Differences in prevalence of obesity in the UK compared with US, and the differences in health-care systems may, in this instance, limit the generalisability of findings. Relevance score: B
Moher M, Hey K & Lancaster T 2005
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 61
Adult smokers What is the extent to which different kinds of workplace smoking programmes help smokers to reduce or stop cigarette consumption? Are different types of workplace programmes more effective in helping employees to stop or reduce smoking?
Group therapy, individual counselling and pharmacological treatment are effective in the workplace. However, these treatments have also been shown to be effective outside the workplace. Self help interventions are less effective, a finding common to other settings. There is limited evidence that cessation programmes aimed at the individual are more effective when combined with environmental support. Restrictions and bans decrease cigarette consumption at work but there is conflicting evidence as to whether they decrease prevalence of smoking or overall consumption of tobacco by smokers. Only 6 of the 61 studies addressed economic issues (5 USA, one Australia). It is difficult to compare the costs and cost effectiveness of interventions across the studies as the figures quoted vary across time and country and the methods of calculating costs differ between studies.
Studies were carried out in different countries, including the UK. Relevance score: A
Morgan O 2005 Narrative review Level: 2 Review quality: + No. of studies: 9
General public What is the current evidence of effectiveness for exercise-referral schemes?
Exercise referral schemes appear to increase PA levels in certain populations, although effect may not last long term. Motivational activities combined with exercise provision appear more effective than low recruitment and adherence has cost-effectiveness implications. However, if targeted at ‘almost active’ populations and use existing infrastructures they may present an important opportunity.
Includes UK studies Relevance score: A
Murphy-Hoefer R et al 2005
Systematic review Level: 2
College/university student smokers
What is the efficacy of interventions designed to reduce the prevalence of smoking in
Results indicated that interventions can have a positive influence on student behaviour, specifically by reducing tobacco use (i.e. prevalence of cigarette smoking and use of smokeless products, amount smoked) among college students, and increasing acceptability of smoking policies
12 studies conducted in the US, 2 in Germany and 1 in Switzerland
162

Review quality: + No. of studies: 14
college/university students?
and campus restrictions among tobacco users and nonusers. With individual level interventions quit rates were 23% (intervention group) 15% (control group) within 3 months, 36% and 16% respectively within 1 year and 13% and 9% respectively for quit by 3 months and abstinent at 1 year. With institutional level interventions Chaloupka (1997) found that the price of cigarettes and amount of tax on them had a significant negative impact on smoking by college students. 10% increase in price would reduce smoking participation by over 5% and consumption among smokers by 4.2% to 7.9%. Apel (1997) found that a smoke free policy led to led to 28% of men and 30% of women smoking less after introduction of the policy.
Relevance score: B
Nishi N, Jenicek M & Tatara K 1998
Systematic review (meta-analysis) Level: 1 Review quality: + No. of studies: 5
Smokers in group exercise programs.
What is the effect of group exercise programs on smoking cessation?
The summary odds ratio for the 3 studies whose main aim was smoking cessation was 2.35 (95% CI 0.75-7.31). When the 2 other studies, in which smoking cessation was not the main aim, were added the summary odds ratio dropped to 1.85 (95% CI 0.65-5.24). This indicates that exercise may be effective for aiding smoking cessation. Most studies were successful in increasing physical fitness of the intervention group. However, no detail is given of the successful interventions – why they might be successful in increasing chances of smoking cessation. Also, it is not explained exactly what the odds ratio’s mean – do they mean that if you exercise you are twice as likely to give up smoking? Or twice as many people give up smoking if they exercise concurrently? Finally, no detail is given of the differences between the studies whose main aim was/was not smoking cessation – what is important in smoking cessation then, as regards exercise?
Non-UK studies Relevance score: B
Ogilvie D et al 2004
Systematic review Level: 2 Review quality: - No. of studies: 22
Urban dwelling adults What interventions are effective in promoting a population shift from using cars towards walking and cycling and what are the health effects of such interventions?
Some evidence was found that targeted behaviour change programmes can change the behaviour of motivated subgroups, resulting (in the largest study) in a shift of around 5% of all trips at a population level. Single studies of commuter subsidies and a new railway station also showed positive effects. The balance of best available evidence about publicity campaigns, engineering measures (extending and improving cycle route networks), and other interventions (such as financial incentives) suggests that they have not been effective. Participants in trials of active commuting experienced short term improvements in certain measures of health and fitness, but they found no good evidence on effects on health of any effective intervention at population level.
8 of the studies carried out in the UK Relevance score: A
Park E W et al 2004
Systematic review of randomised controlled
Smokers Does an intervention to enhance partner support
An increase in quit rates was not detected. The odds ratio for self-reported abstinence at 6-9 months was 1.08 (CI 95% 0.81-1.44) and at 12
The review does not state which countries
163
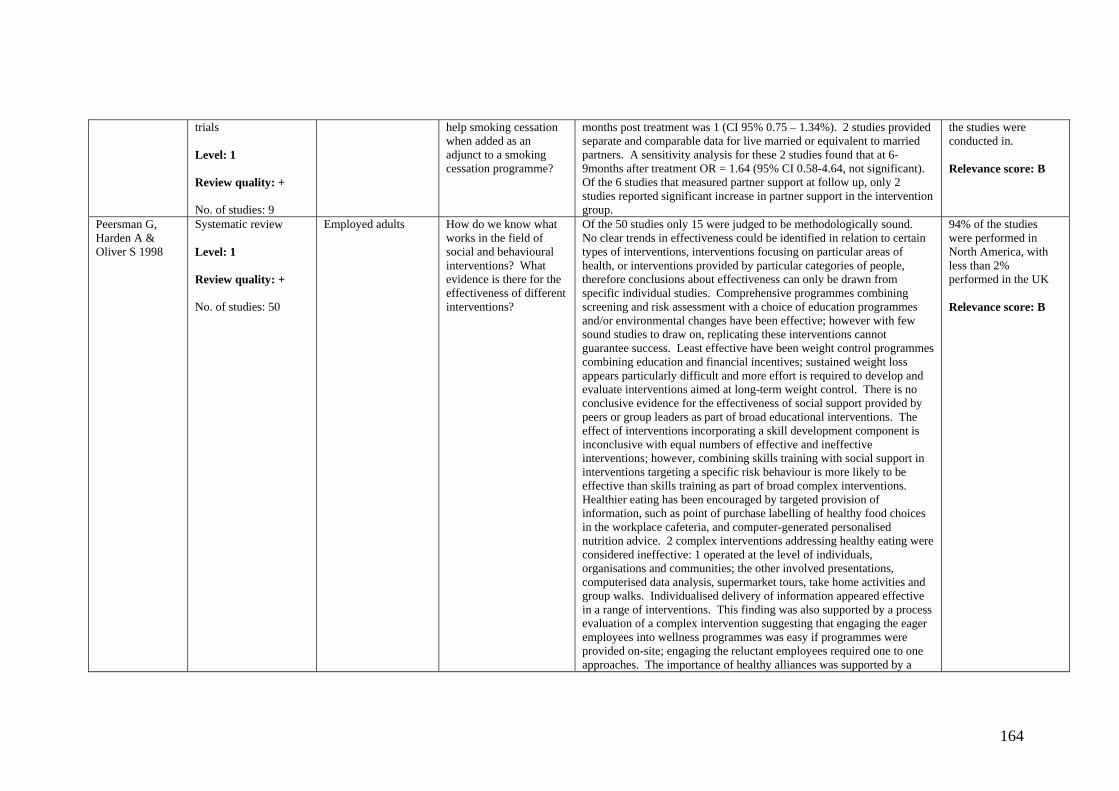
trials Level: 1 Review quality: + No. of studies: 9
help smoking cessation when added as an adjunct to a smoking cessation programme?
months post treatment was 1 (CI 95% 0.75 – 1.34%). 2 studies provided separate and comparable data for live married or equivalent to married partners. A sensitivity analysis for these 2 studies found that at 6-9months after treatment OR = 1.64 (95% CI 0.58-4.64, not significant). Of the 6 studies that measured partner support at follow up, only 2 studies reported significant increase in partner support in the intervention group.
the studies were conducted in. Relevance score: B
Peersman G, Harden A & Oliver S 1998
Systematic review Level: 1 Review quality: + No. of studies: 50
Employed adults How do we know what works in the field of social and behavioural interventions? What evidence is there for the effectiveness of different interventions?
Of the 50 studies only 15 were judged to be methodologically sound. No clear trends in effectiveness could be identified in relation to certain types of interventions, interventions focusing on particular areas of health, or interventions provided by particular categories of people, therefore conclusions about effectiveness can only be drawn from specific individual studies. Comprehensive programmes combining screening and risk assessment with a choice of education programmes and/or environmental changes have been effective; however with few sound studies to draw on, replicating these interventions cannot guarantee success. Least effective have been weight control programmes combining education and financial incentives; sustained weight loss appears particularly difficult and more effort is required to develop and evaluate interventions aimed at long-term weight control. There is no conclusive evidence for the effectiveness of social support provided by peers or group leaders as part of broad educational interventions. The effect of interventions incorporating a skill development component is inconclusive with equal numbers of effective and ineffective interventions; however, combining skills training with social support in interventions targeting a specific risk behaviour is more likely to be effective than skills training as part of broad complex interventions. Healthier eating has been encouraged by targeted provision of information, such as point of purchase labelling of healthy food choices in the workplace cafeteria, and computer-generated personalised nutrition advice. 2 complex interventions addressing healthy eating were considered ineffective: 1 operated at the level of individuals, organisations and communities; the other involved presentations, computerised data analysis, supermarket tours, take home activities and group walks. Individualised delivery of information appeared effective in a range of interventions. This finding was also supported by a process evaluation of a complex intervention suggesting that engaging the eager employees into wellness programmes was easy if programmes were provided on-site; engaging the reluctant employees required one to one approaches. The importance of healthy alliances was supported by a
94% of the studies were performed in North America, with less than 2% performed in the UK Relevance score: B
164

number of studies showing success in controlling blood pressure, smoking and alcohol consumption, as well as improving knowledge and changing behaviour related to cancer prevention; however, other studies involving healthy alliances had disappointing results.
Petrella R & Lattanzio C 2002
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 13
Healthy adults What is the effect of counselling patients to become more physically active?
6 RCTs, 5 quasi-experimental studies 5 studies had 4-8 weeks follow-up, 8 were >6 months follow-up. A US project, INSURE, enrolled >2000 patients where GPs (with limited training and support) provided specific health services. After 12 months, 33.8% intervention group had begun exercising, compared to 24.1% control group (p<.05). Another US study gave 24 patients saw a physician for brief advice, had 15 mins of exercise training, and educational materials including a card with study protocol and supportive rationale. At 1-month follow-up intervention patients were exercising more frequently, intensively and for longer than control group. However, this is short follow-up period so cannot comment on the longer term effectiveness of this advice. An Australian study tested the effectiveness of adding self-help educational materials to lifestyle counselling using videos. A significant increase in total energy expenditure (kJ/kg/h) over 12 months was seen in both counselling and counselling + video material groups but no difference between the groups. A US study evaluated the effect of physician visits encouraging healthy behaviour in elderly people. No difference was found between intervention and control groups. A US study trained GPs to provide 3-5 mins of PA counselling to patients. Patients also received ‘booster’ phone calls 2 weeks in to reinforce the counselling. At 6-week follow-up 52% of intervention patients reported regular activity compared to 12% of control patients. They also significantly increased duration of walking compared with controls (+37 mins/week vs. +7 mins/week) and showed greater readiness to become active. Physicians were supportive of the program. Longer term efficacy needs evaluation. A US study tested efficacy of brief physician-delivered PA counselling. PA increased but no difference between intervention and control groups. Limitations include small sample size (n=63) and short term follow-up. An Australian study assessed effectiveness of brief physician intervention at routine consultations to increase PA in >400 sedentary patients. At 12-month follow-up no significant differences were found between intervention and control. A New Zealand study compared written and oral advice about PA in 37
UK-based studies included Relevance score: A
165
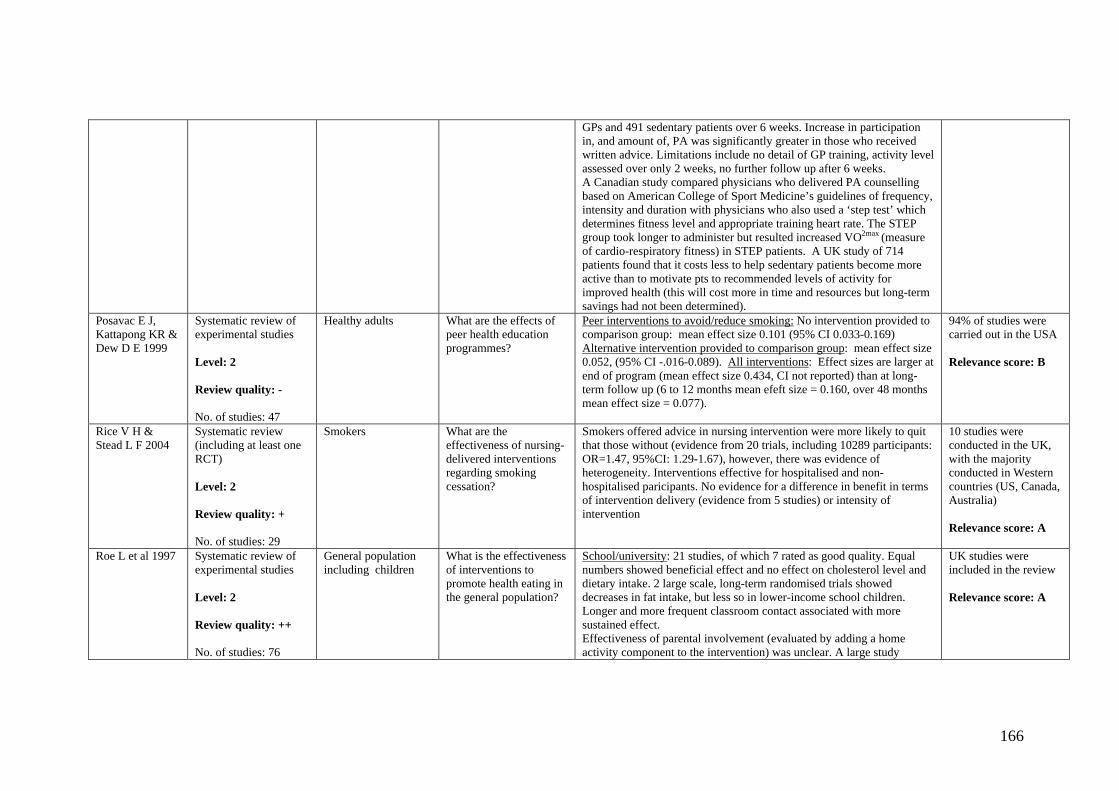
GPs and 491 sedentary patients over 6 weeks. Increase in participation in, and amount of, PA was significantly greater in those who received written advice. Limitations include no detail of GP training, activity level assessed over only 2 weeks, no further follow up after 6 weeks. A Canadian study compared physicians who delivered PA counselling based on American College of Sport Medicine’s guidelines of frequency, intensity and duration with physicians who also used a ‘step test’ which determines fitness level and appropriate training heart rate. The STEP group took longer to administer but resulted increased VO2max (measure of cardio-respiratory fitness) in STEP patients. A UK study of 714 patients found that it costs less to help sedentary patients become more active than to motivate pts to recommended levels of activity for improved health (this will cost more in time and resources but long-term savings had not been determined).
Posavac E J, Kattapong KR & Dew D E 1999
Systematic review of experimental studies Level: 2 Review quality: - No. of studies: 47
Healthy adults What are the effects of peer health education programmes?
Peer interventions to avoid/reduce smoking: No intervention provided to comparison group: mean effect size 0.101 (95% CI 0.033-0.169) Alternative intervention provided to comparison group: mean effect size 0.052, (95% CI -.016-0.089). All interventions: Effect sizes are larger at end of program (mean effect size 0.434, CI not reported) than at long- term follow up (6 to 12 months mean efeft size = 0.160, over 48 months mean effect size = 0.077).
94% of studies were carried out in the USA Relevance score: B
Rice V H & Stead L F 2004
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 29
Smokers What are the effectiveness of nursing-delivered interventions regarding smoking cessation?
Smokers offered advice in nursing intervention were more likely to quit that those without (evidence from 20 trials, including 10289 participants: OR=1.47, 95%CI: 1.29-1.67), however, there was evidence of heterogeneity. Interventions effective for hospitalised and non-hospitalised paricipants. No evidence for a difference in benefit in terms of intervention delivery (evidence from 5 studies) or intensity of intervention
10 studies were conducted in the UK, with the majority conducted in Western countries (US, Canada, Australia) Relevance score: A
Roe L et al 1997
Systematic review of experimental studies Level: 2 Review quality: ++ No. of studies: 76
General population including children
What is the effectiveness of interventions to promote health eating in the general population?
School/university: 21 studies, of which 7 rated as good quality. Equal numbers showed beneficial effect and no effect on cholesterol level and dietary intake. 2 large scale, long-term randomised trials showed decreases in fat intake, but less so in lower-income school children. Longer and more frequent classroom contact associated with more sustained effect. Effectiveness of parental involvement (evaluated by adding a home activity component to the intervention) was unclear. A large study
UK studies were included in the review Relevance score: A
166

showed no effect, 1 moderate quality study found some effect but which was not sustained at one year, and another found an effect only in girls. Workplace: 9 RCTs were directed at entire workplace populations (mainly male) of which 4 were good quality. The majority showed beneficial effects on dietary change (although outcomes often poorly measured). Secular trends and contamination between study & control groups limit the effects of some studies. The most effective interventions focussed solely on changing diet or blood cholesterol (rather than a range of lifestyle factors), and usually included individual screening or counselling. A conclusion from the most effective large-scale studies was that they need not be intensive, but require substantial workplace organisation and resource. For example, a reduction of fat intake of 1% energy was seen in an US intervention which consisted of workplace events, cholesterol screening, classes and cafeteria meal modification. Individual health screening among manual workers in Glasgow showed reduced blood cholesterol of 2.5%. Primary care: 7 RCTs of which 4 were good quality. All interventions involved individual counselling or printed educational material, based on theoretical models. Individual tailoring of the intervention enhanced effectiveness. More intensive intervention to those at higher risk was associated with sustained reductions in blood cholesterol. 3 of the good quality studies were nurse-administered health checks in GP practices in UK. They showed that a single health check with a nurse, supplemented by take-home materials, brief follow-up and referral resulted in dietary changes and reduced blood cholesterol level or 2-3% in large populations (sustained for 3 years in one study). The fourth good quality study provided individually tailored computerised information, and resulted in reduced fat intake of 4% energy, but no change in fruit/vegetable intake. A moderate quality study found non-tailored educational materials found no effect on diet. Few interventions were conducted on younger adults, ethnic minorities and lower-income groups. Community: 10 large-scale cohort studies and 6 RCTs; 7 were good quality. The long-term studies were consistent in showing no intervention effect on blood cholesterol (compared to the secular trend in control groups). 3 of the 4 good quality cohort studies showed 1-2% reduction in cholesterol; the fourth study showed 3% reduction in cholesterol in men only. 2 good quality RCTs involved highly selected and motivated participants who attended educational sessions and completed food records; large reductions in fat intake (10% energy) or cholesterol (7%) were seen in the short-term. There was a lack of
167
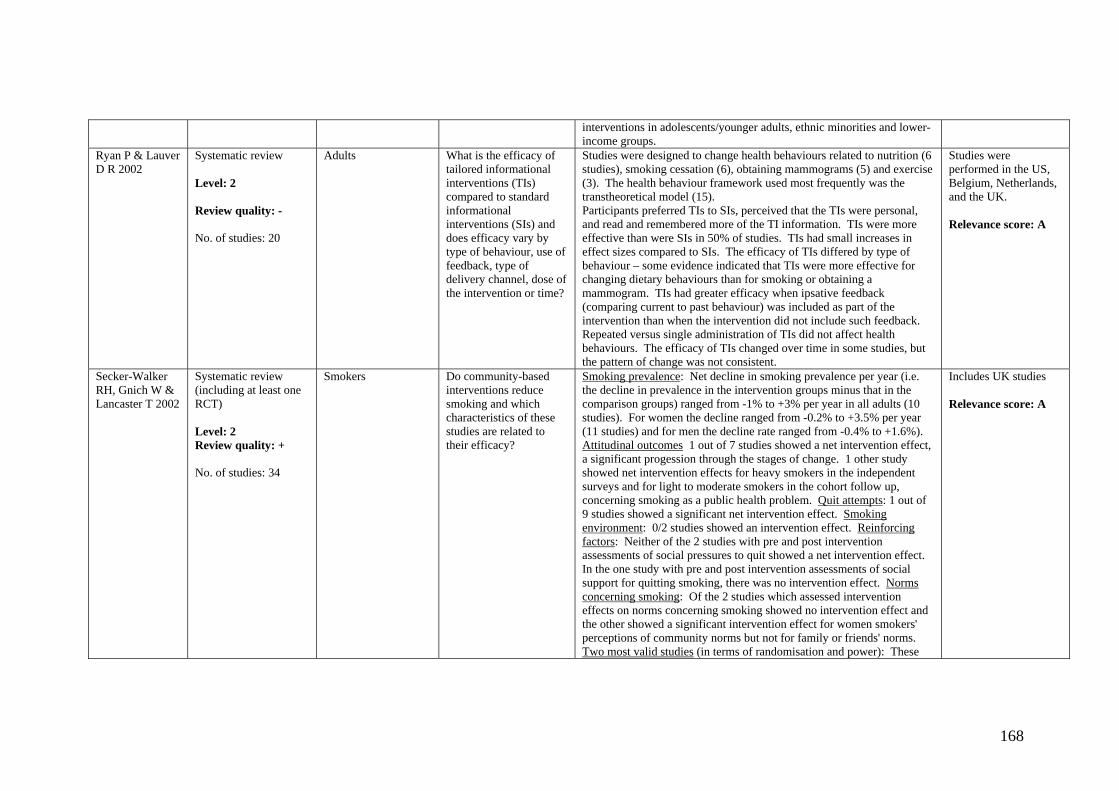
interventions in adolescents/younger adults, ethnic minorities and lower-income groups.
Ryan P & Lauver D R 2002
Systematic review Level: 2 Review quality: - No. of studies: 20
Adults What is the efficacy of tailored informational interventions (TIs) compared to standard informational interventions (SIs) and does efficacy vary by type of behaviour, use of feedback, type of delivery channel, dose of the intervention or time?
Studies were designed to change health behaviours related to nutrition (6 studies), smoking cessation (6), obtaining mammograms (5) and exercise (3). The health behaviour framework used most frequently was the transtheoretical model (15). Participants preferred TIs to SIs, perceived that the TIs were personal, and read and remembered more of the TI information. TIs were more effective than were SIs in 50% of studies. TIs had small increases in effect sizes compared to SIs. The efficacy of TIs differed by type of behaviour – some evidence indicated that TIs were more effective for changing dietary behaviours than for smoking or obtaining a mammogram. TIs had greater efficacy when ipsative feedback (comparing current to past behaviour) was included as part of the intervention than when the intervention did not include such feedback. Repeated versus single administration of TIs did not affect health behaviours. The efficacy of TIs changed over time in some studies, but the pattern of change was not consistent.
Studies were performed in the US, Belgium, Netherlands, and the UK. Relevance score: A
Secker-Walker RH, Gnich W & Lancaster T 2002
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 34
Smokers Do community-based interventions reduce smoking and which characteristics of these studies are related to their efficacy?
Smoking prevalence: Net decline in smoking prevalence per year (i.e. the decline in prevalence in the intervention groups minus that in the comparison groups) ranged from -1% to +3% per year in all adults (10 studies). For women the decline ranged from -0.2% to +3.5% per year (11 studies) and for men the decline rate ranged from -0.4% to +1.6%). Attitudinal outcomes 1 out of 7 studies showed a net intervention effect, a significant progession through the stages of change. 1 other study showed net intervention effects for heavy smokers in the independent surveys and for light to moderate smokers in the cohort follow up, concerning smoking as a public health problem. Quit attempts: 1 out of 9 studies showed a significant net intervention effect. Smoking environment: 0/2 studies showed an intervention effect. Reinforcing factors: Neither of the 2 studies with pre and post intervention assessments of social pressures to quit showed a net intervention effect. In the one study with pre and post intervention assessments of social support for quitting smoking, there was no intervention effect. Norms concerning smoking: Of the 2 studies which assessed intervention effects on norms concerning smoking showed no intervention effect and the other showed a significant intervention effect for women smokers' perceptions of community norms but not for family or friends' norms. Two most valid studies (in terms of randomisation and power): These
Includes UK studies Relevance score: A
168

found no intervention effect for changes in smoking prevalence but a significant increase in quit rate was seen in one study and a significant increase in quit rate among men but not women was seen in the other study. This indicates success on an individual but not a community level. Interventions most likely to be successful: Intervention success was not related to the number of risk behaviours adressed, the setting of the intervention (e.g. urban vs rural), the theoretical basis of the intervention, the channel of delivery or the involvement of community members. The 4 projects lasting less than 2 years had no demonstrable effect but among those lasting 2 to 5 years or more than 5 years there was litlle difference in the proportion of studies reporting at least one favourable outcome. Significantly higher levels of exposure and higher participation rates tended to be associated with more favourable outcomes.
Serra C et al 2000
Review of uncontrolled studies Level: 2 Review quality: + No. of studies: 11
Smokers What is the effectiveness of interventions to reduce tobacco consumption in public places?
Strategies aimed at populations: 6 studies in hospital or workplace. 2 hospital studies found significant effects of an institutional ban: a) A children’s hospital saw reductions in people seen smoking (53% at baseline to 0% at 6-month follow up), numbers of cigarette butts in ashtrays and concentration of nicotine vapour in elevators (although no differences in restrooms and outpatient clinics). A similar intervention in an adult hospital found comparable results. An information campaign (signs, leaflets, displays) led to significant reductions in smoking in public areas of hospitals. A policy of restricting smoking to designated areas and times in a workplace setting significantly reduced the number of workers being bothered by people’s smoke. One study evaluated warning signs; emphasising the harm of smoking had a larger impact than emphasising the benefit of quitting in cardiac inpatients, but no effect on visitors. Another study found no difference between negatively (threatening punitive action) and positively (non-threatening and courteous) worded signs, but both together appeared reduce the proportion of smokers compared to baseline. Strategies aimed at individuals: In offices, continuous requests to stop smokers smoking had more effect than occasional requests. In a barbershop, a large reduction in smoking customers was seen when requests combined with signs. In supermarkets, requests showed higher effect than signs alone. In a university cafeteria, signs and verbal prompting together were more effective than several signs on tables/walls. Another study showed that assertive requests to stop smoking was dependent on the area; 39% stopped smoking after a
All included studies were conducted in the US. Relevance score: B
169

request in a recreational area, 75% in a non-recreational area, and 66% if the smoker was in the company of others. Most effective interventions are where institutions developed, resourced and supported programmes to ban smoking. High success rates from a strategy which included education, dissemination of information, training for managers and quitting support for smokers. Commitment from management and communication with those affected by the ban appeared to be an important part of successful interventions. Posted signs had little effect on their own; strategies aimed at individuals had short-term effect, and are unacceptable as public health strategies.
Shepherd J et al 2001
Systematic review (including at least one RCT) Level: 3 Review quality: + No. of studies: 6 outcome evaluations, 8 qualitative studies
Young people aged 11- 16 years
What is the evidence from outcome and/or process evaluations of interventions to improve young people’s nutrition? What are the views of young people on the barriers to and facilitators of healthy eating?
Whole school approach found to be effective for healthy eating behaviour, particularly in young women but difficult to identify key features of success. Increasing availability of healthy foods in schools, complemented by classroom activities and media campaigns has been effective for healthy eating behaviour. School based interventions educating young people about nutrition and alerting them to environmental influences upon their ability to eat healthy foods can be effective for healthy eating behaviour, particularly in young women. Multiple component interventions involving classroom activities, parental involvement and risk factor screening can be effective for certain clinical risk factors. Teaching cooking skills and motivating young people to promote healthy eating has been effective for increasing consumption of healthy foods and reducing blood pressure. Gender differences in effectiveness of interventions.
1/7 interventions conducted in the UK. Qualitative evidence taken from UK only. Some interventions carried out outside the UK have tested issues raised in these UK based qualitative studies. Relevance score: A
Sinclair H K, Bond C M & Stead L F 2004
Systematic review (including at least one RCT) Level: 1 Review quality: + No. of studies: 2
Smokers What is the effectiveness of interventions by community pharmacy personnel to assist clients to stop smoking?
1 of the 2 trials demonstrated significant improvement in abstinence rates in the intervention group compared to control up to and including 12 months after the start of intervention. The other trial did not demonstrate statistically significant improvement but a trend towards improved abstinence with pharmacy intervention. Pharmacists valued their training received in both trials, and the training intervention had long-term benefits for the knowledge and attitudes of pharmacists and staff over the 3-year period.
Both recent (1998 and 2001) UK trials Relevance score: A
170
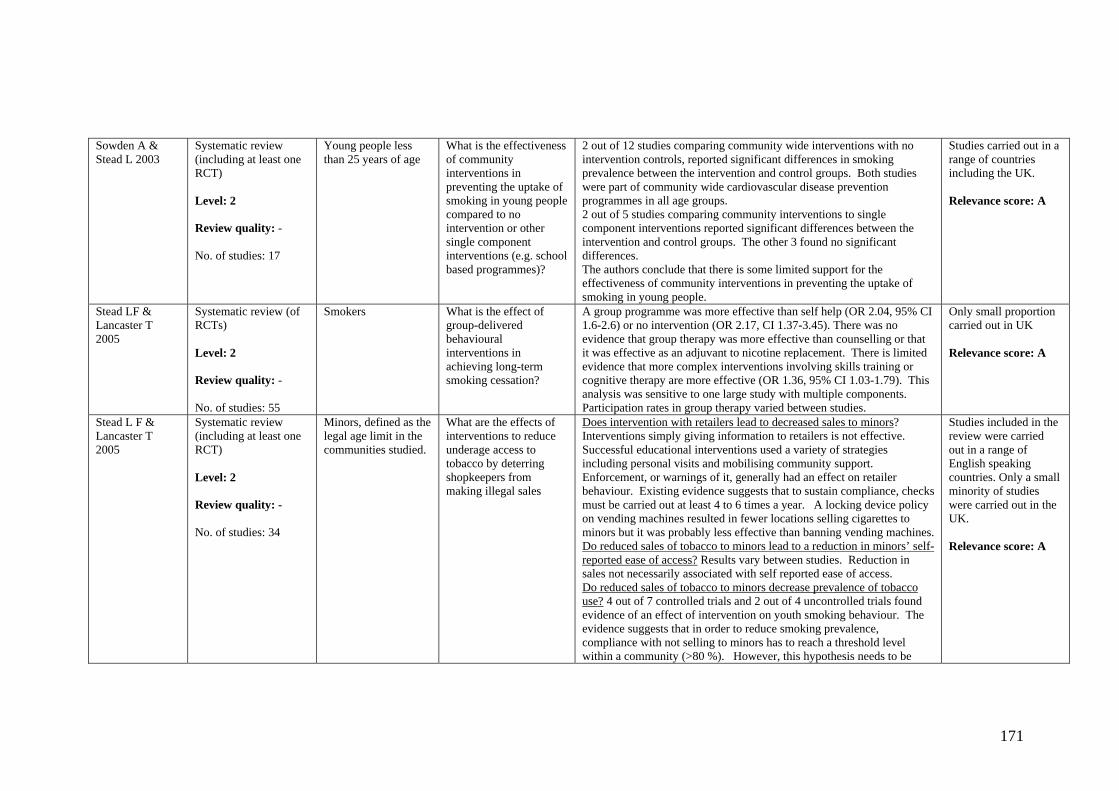
Sowden A & Stead L 2003
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 17
Young people less than 25 years of age
What is the effectiveness of community interventions in preventing the uptake of smoking in young people compared to no intervention or other single component interventions (e.g. school based programmes)?
2 out of 12 studies comparing community wide interventions with no intervention controls, reported significant differences in smoking prevalence between the intervention and control groups. Both studies were part of community wide cardiovascular disease prevention programmes in all age groups. 2 out of 5 studies comparing community interventions to single component interventions reported significant differences between the intervention and control groups. The other 3 found no significant differences. The authors conclude that there is some limited support for the effectiveness of community interventions in preventing the uptake of smoking in young people.
Studies carried out in a range of countries including the UK. Relevance score: A
Stead LF & Lancaster T 2005
Systematic review (of RCTs) Level: 2 Review quality: - No. of studies: 55
Smokers What is the effect of group-delivered behavioural interventions in achieving long-term smoking cessation?
A group programme was more effective than self help (OR 2.04, 95% CI 1.6-2.6) or no intervention (OR 2.17, CI 1.37-3.45). There was no evidence that group therapy was more effective than counselling or that it was effective as an adjuvant to nicotine replacement. There is limited evidence that more complex interventions involving skills training or cognitive therapy are more effective (OR 1.36, 95% CI 1.03-1.79). This analysis was sensitive to one large study with multiple components. Participation rates in group therapy varied between studies.
Only small proportion carried out in UK Relevance score: A
Stead L F & Lancaster T 2005
Systematic review (including at least one RCT) Level: 2 Review quality: - No. of studies: 34
Minors, defined as the legal age limit in the communities studied.
What are the effects of interventions to reduce underage access to tobacco by deterring shopkeepers from making illegal sales
Does intervention with retailers lead to decreased sales to minors? Interventions simply giving information to retailers is not effective. Successful educational interventions used a variety of strategies including personal visits and mobilising community support. Enforcement, or warnings of it, generally had an effect on retailer behaviour. Existing evidence suggests that to sustain compliance, checks must be carried out at least 4 to 6 times a year. A locking device policy on vending machines resulted in fewer locations selling cigarettes to minors but it was probably less effective than banning vending machines. Do reduced sales of tobacco to minors lead to a reduction in minors’ self-reported ease of access? Results vary between studies. Reduction in sales not necessarily associated with self reported ease of access. Do reduced sales of tobacco to minors decrease prevalence of tobacco use? 4 out of 7 controlled trials and 2 out of 4 uncontrolled trials found evidence of an effect of intervention on youth smoking behaviour. The evidence suggests that in order to reduce smoking prevalence, compliance with not selling to minors has to reach a threshold level within a community (>80 %). However, this hypothesis needs to be
Studies included in the review were carried out in a range of English speaking countries. Only a small minority of studies were carried out in the UK. Relevance score: A
171

tested prospectively. Stead L F, Lancaster T & Perera R 2003
Systematic review (including at least one RCT) Level: 1 Review quality: - No. of studies: 27
Smokers What is the effect of telephone support to help smokers quit?
Proactive + minimal intervention vs. minimal intervention 13 trials, 10 of which the minimal intervention was self-help materials. In a meta-analysis there was evidence of a significant benefit from the addition of the telephone counselling component (OR 1.56). The results of this are supported by individual studies. Proactive + face-to-face vs. face-to-face 4 studies, none of which showed a significant increase in quitting from the addition of telephone follow-up. Pooled estimate reflects this (OR 1.08). Proactive + NRT vs. NRT 4 studies, none of which showed a statistically significant effect of adding telephone support (OR 1.08). Proactive vs. Group programme 1 study showed no difference in 6-month sustained quit rates at 24-month follow up. Reactive: Help lines + self-help materials vs. self-help materials 1 study showed some effect, 1 showed negative effect and one showed no effect. Reactive: Tailored responses to helpline calls 2 studies failed to find a significantly increase benefit from tailored counselling or materials. Telephone counselling as the sole intervention or added to self help materials increases the odds of quitting (OR 1.56). Despite some guidelines recommending using telephone counselling to follow up face-to-face counselling, this review showed evidence that benefits from phone counselling were stronger when it was the main intervention rather than when it was used to support face-to-face. The better results achieved by dedicated phone support services could reflect a difference in provider skills. Or, that phone contact could encourage use of self-help materials. Timing may affect the impact of the intervention – may need calls during first few weeks of quit attempt when risk of relapse is higher. Other studies and reviews have shown that phone counselling as a follow-up to in-hospital counselling was effective. Rigorous review of reactive services is difficult due to reluctance to refuse help to some callers. 1 suggested benefit of hotlines is that they can attract calls from specific minority groups by using targeted advertising. But well educated white women are overrepresented as users of telephone services for health care in general. Counselling via telephone hotlines can be provided as part of a programme or separately and give access to more people than face to face. The review of trials found telephone counselling is effective compared to a programme with no personal contact.
23/27 studies were from US. No UK studies included. Relevance score: B
172
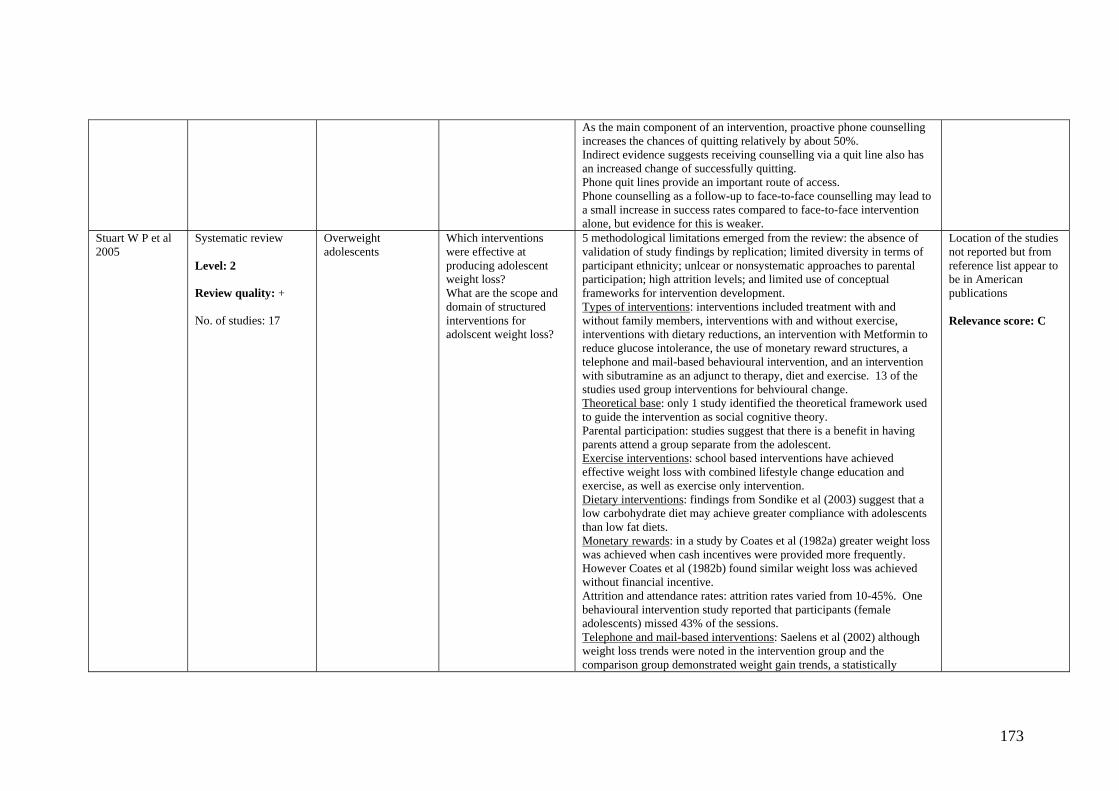
As the main component of an intervention, proactive phone counselling increases the chances of quitting relatively by about 50%. Indirect evidence suggests receiving counselling via a quit line also has an increased change of successfully quitting. Phone quit lines provide an important route of access. Phone counselling as a follow-up to face-to-face counselling may lead to a small increase in success rates compared to face-to-face intervention alone, but evidence for this is weaker.
Stuart W P et al 2005
Systematic review Level: 2 Review quality: + No. of studies: 17
Overweight adolescents
Which interventions were effective at producing adolescent weight loss? What are the scope and domain of structured interventions for adolscent weight loss?
5 methodological limitations emerged from the review: the absence of validation of study findings by replication; limited diversity in terms of participant ethnicity; unlcear or nonsystematic approaches to parental participation; high attrition levels; and limited use of conceptual frameworks for intervention development. Types of interventions: interventions included treatment with and without family members, interventions with and without exercise, interventions with dietary reductions, an intervention with Metformin to reduce glucose intolerance, the use of monetary reward structures, a telephone and mail-based behavioural intervention, and an intervention with sibutramine as an adjunct to therapy, diet and exercise. 13 of the studies used group interventions for behvioural change. Theoretical base: only 1 study identified the theoretical framework used to guide the intervention as social cognitive theory. Parental participation: studies suggest that there is a benefit in having parents attend a group separate from the adolescent. Exercise interventions: school based interventions have achieved effective weight loss with combined lifestyle change education and exercise, as well as exercise only intervention. Dietary interventions: findings from Sondike et al (2003) suggest that a low carbohydrate diet may achieve greater compliance with adolescents than low fat diets. Monetary rewards: in a study by Coates et al (1982a) greater weight loss was achieved when cash incentives were provided more frequently. However Coates et al (1982b) found similar weight loss was achieved without financial incentive. Attrition and attendance rates: attrition rates varied from 10-45%. One behavioural intervention study reported that participants (female adolescents) missed 43% of the sessions. Telephone and mail-based interventions: Saelens et al (2002) although weight loss trends were noted in the intervention group and the comparison group demonstrated weight gain trends, a statistically
Location of the studies not reported but from reference list appear to be in American publications Relevance score: C
173

significant difference between the groups was not identified at follow-up. Medication interventions: Freemark & Bursey (2001) BMI was reduced by 1.3% in the group taking metformin, whereas the control group BMI increased 2.3%. Berkpwitz et al (2003) reported that adolescents who took sibutramine combined with a behavioural, diet and exercise intervention, had a 4.5% greater BMI loss than those in the control group.
Summerbell CD et al 2005
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 22
Young people less than 18 years
To assess the effectiveness of interventions designed to prevent obesity in childhood through diet, physical activity and/or lifestyle and social support
22 studies were included, 10 long term (at least 12 months) and 12 short term (12 weeks to 12 months). 19 were school/preschool based, one was a community based intervention targeting low income families and 2 were family based interventions targeting non obese children of obese or overweight children. Nearly all studies resulted in some improvement in diet or physical activity. 6/10 long term studies combined dietary and physical activity interventions; 5 resulted in no difference in overweight status between groups and one resulted in improvements for girls receiving the intervention and not boys. 2 studies focussed on physical activity alone. Of these 1 appeared to be effective in preventing obesity and the other did not report sufficient data to determine whether there was a significant difference between the 2 groups, although from the data provided it is unlikely that the changes would be clinically significant. 2 studies focussed on nutrition alone but neither were effective in preventing obesity. 4/12 short term studies focused on interventions to increase physical activity levels and 2 of these resulted in minor reductions in overweight status in favour of the intervention. The other 8 studies combined advice on diet and physical activity but none had a significant impact on obesity. 4/12 short term studies focused on interventions to increase physical activity levels and 2 of these resulted in minor reductions in overweight status in favour of the intervention. The other 8 studies combined advice on diet and physical activity but none had a significant impact on obesity. There was an absence of cost effectiveness data in the primary studies reviewed. Some studies conducted in well educated population groups and families, limiting the generalisability of the findings and potentially widening the inequalities experienced.
A small proportion of studies carried out in the UK. Relevance score: A
Taylor WC, Baranowski T & Young D R 1998
Systematic review (including at least one RCT) Level: 2
Low income, ethnic minorities and populations with disability.
How effective are interventions that have targeted populations at risk of inactivity, including low income,
Ethnic groups: 2 interventions reported no significant changes in physical activity 2 reported mixed results i.e. changes in some outcomes but not all), two reported changes in subgroups and 2 reported consistent positive changes. The studies reporting positive, consistent change were both weight loss programmes for women. The final 2 studies did not
All studies identified were US based. There may be cultural differences to the UK.
174
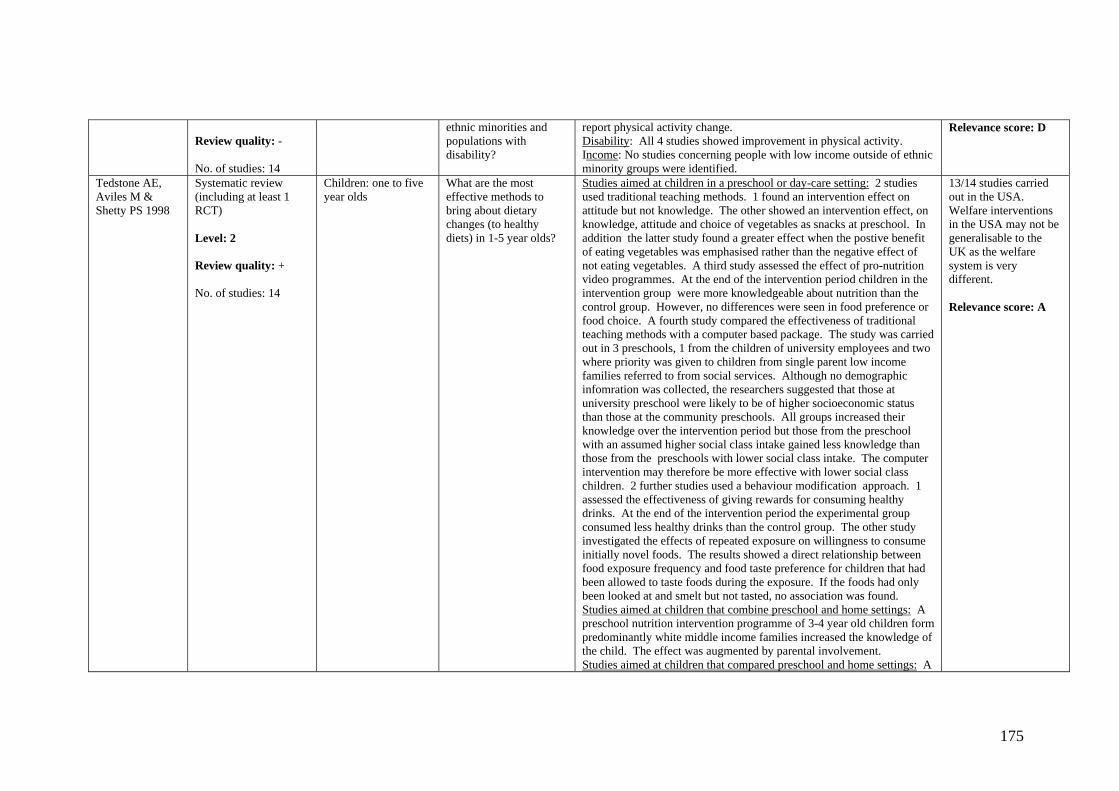
Review quality: - No. of studies: 14
ethnic minorities and populations with disability?
report physical activity change. Disability: All 4 studies showed improvement in physical activity. Income: No studies concerning people with low income outside of ethnic minority groups were identified.
Relevance score: D
Tedstone AE, Aviles M & Shetty PS 1998
Systematic review (including at least 1 RCT) Level: 2 Review quality: + No. of studies: 14
Children: one to five year olds
What are the most effective methods to bring about dietary changes (to healthy diets) in 1-5 year olds?
Studies aimed at children in a preschool or day-care setting: 2 studies used traditional teaching methods. 1 found an intervention effect on attitude but not knowledge. The other showed an intervention effect, on knowledge, attitude and choice of vegetables as snacks at preschool. In addition the latter study found a greater effect when the postive benefit of eating vegetables was emphasised rather than the negative effect of not eating vegetables. A third study assessed the effect of pro-nutrition video programmes. At the end of the intervention period children in the intervention group were more knowledgeable about nutrition than the control group. However, no differences were seen in food preference or food choice. A fourth study compared the effectiveness of traditional teaching methods with a computer based package. The study was carried out in 3 preschools, 1 from the children of university employees and two where priority was given to children from single parent low income families referred to from social services. Although no demographic infomration was collected, the researchers suggested that those at university preschool were likely to be of higher socioeconomic status than those at the community preschools. All groups increased their knowledge over the intervention period but those from the preschool with an assumed higher social class intake gained less knowledge than those from the preschools with lower social class intake. The computer intervention may therefore be more effective with lower social class children. 2 further studies used a behaviour modification approach. 1 assessed the effectiveness of giving rewards for consuming healthy drinks. At the end of the intervention period the experimental group consumed less healthy drinks than the control group. The other study investigated the effects of repeated exposure on willingness to consume initially novel foods. The results showed a direct relationship between food exposure frequency and food taste preference for children that had been allowed to taste foods during the exposure. If the foods had only been looked at and smelt but not tasted, no association was found. Studies aimed at children that combine preschool and home settings: A preschool nutrition intervention programme of 3-4 year old children form predominantly white middle income families increased the knowledge of the child. The effect was augmented by parental involvement. Studies aimed at children that compared preschool and home settings: A
13/14 studies carried out in the USA. Welfare interventions in the USA may not be generalisable to the UK as the welfare system is very different. Relevance score: A
175
nutrition education programme significantly improved knowledge in both preschool and home settings. Knowledge gain was signficantly higher in the preschool to home setting. Studies aimed at children in a home setting: A nurtition education programme tested in children from middle to upper socioeconomic background increases understanding of health and nutrition as related concepts. Studies aimed at carers in combined primary-care and home settings: A study in the UK targeted mothers of children from a deprived low-income background in inner city Bristol. Mothers were provided with advice on the food components of a healthy diet and related organisational skills including meal planning, reuglar meals and eating together. At the end of the intervention period a 7 day food diary showed an overall improvent in the children’s diet, organisation of meals, mothers’ report of own and child’s diets and a small improvement in self esteem. Welfare scheme studies aimed at carers in the USA: 2/2 studies were found to be effective. Healthy eating promotions aimed at day care staff: A single workshop for day care meal providers had no impact on menu plans provided by day care centres (controlled trial).
Thomas R 2002 Systematic review (including at least one RCT) Level: 1 Review quality: + No. of studies: 76
Children aged 5- 18 years at school
Are school programmes, characterised by intervention type more effective than minimal or no intervention in preventing smoking? Are different types of intervention characterised by theoretical orientation (e.g. social influences vs. information giving)? What effect does the method of delivery e.g. length of programme, peer vs. researcher/teacher led have?
No high quality studies measured information alone vs. control. Studies comparing information alone to other interventions found information alone to be less effective. The majority of school based interventions have been based on social influences. The results have been conflicting with 8 high quality studies showing positive effect on smoking prevalence and seven not showing effect. 1 not showing effect has been considered the most rigorous undertaken in terms of quality, duration and rigorous evaluation. However it has been criticised for not including key components which have been incorporated into successful programmes and for focussing on White run schools only. 1 good quality study found that social competence (e.g. improved behaviour) without an anti smoking intervention lead to lower rates of smoking amongst boys but not girls. There is a lack of good quality evidence assessing combinations of social competence and social influences. There is limited conflicting evidence to assess whether school interventions in combination with wider interventions are effective. Few studies compared different formats of intervention; no good quality
A small proportion of studies carried out in UK. Relevance score: A
176
studies compared peer with teacher delivery or age, gender or culture specific interventions with standardised interventions.
Thompson R et al 2003
Systematic review (including at least one RCT) Level: 1 Review quality: ++ No. of studies: 12 (including 13 comparisons)
Healthy adults In adults, what is the relative efficacy of dietary advice given by a dietician compared with another health professional, or using self-help resources in reducing blood cholesterol?
For short-term effects (<9weeks): Dietary advice from a dietician was more effective than advice from a doctor in reducing blood cholesterol (effect size small but significant: -0.25mmol/L; CI -0.37, -0.12mmol/L). No evidence for difference between dietician and self-help resources. No differences observed for secondary outcomes (e.g. LDL/HDL cholesterol, body weight etc). When doctor, nurse, counsellor and self-help resources were combined and compared with dietician, dietician advice was found to be more effective in reducing blood cholesterol.
Included 2 UK studies (most US; all developed/Western countries). Relevance score: A
van Berkel TFM et al 1999
Systematic review Level: 2 Review quality: - No. of studies: 29, 10 of which related to smoking cessation interventions
Patients with coronary heart disease.
What is the impact of smoking cessation on prognosis and on smoking intervention trials in patients with coronary heart disease?
In 6/10 studies a significantly higher number of quitters was found in the intervention group, in 2 more quitters were found in the intervention group but this was not significant and in 2 studies no difference was found. Sequential meta analysis of the 10 studies resulted in 61% quitters in the intervention group and 42% in the control group, thus 19% more quitters were observed if an intervention was offered (OR=0.5, 95% CI = 0.41 – 0.61). None of the less effective studies had MI as an inclusion criteria
1/10 UK based Relevance score: A
van Teijlingen et al 1998
Systematic review Level: 2 Review quality: + No. of studies: 10 reports, 9 studies
Pregnant women Do women of childbearing age and women who are pregnant change their dietary knowledge, attitudes and/or behaviour in response to specific interventions? What is the extent of such changes (if any)? What are the characteristis of interventions (if any) which appear to be effective?
5 studies were in women of childbearing age and 4 in women who were pregnant. Of these 7 were RCTs, 1 was a non-randomised, controlled before and after study and in the other it was unclear whether the control group was allocated randomly or not. Many of the studies were subject to bias, particularly lack of observer blinding, and using assessment tools of unknown validity. All 5 interventions assessed in women of childbearing age were community based; 2 appeared to be predominantly educational (1 involving a video supplemented by printed material, the other involving a series of nutrition lessons), 2 involved an exercise programme (1 strength training alone, the other as part of a wider intervention also involving education and peer support) and 1 was described as offering empowerment and support to new mothers. The duration of these interventions varied from a single session to regular meetings for at least a year. Taken together the studies suggest that participants can improve their
Includes 2 UK studies Relevance score: A
177

knowledge and dietary intake, particularly fat intake, and that the changes are statistically significantly greater in groups receiving an intervention compared with the controls. Insufficient data were obtained to comment on whether the changes are sustained. This, along with the diversity of the interventions and methodological flaws in some of the evaluations make it difficult to identify interventions which are likely to be successful if more widely applied. Of the 4 interventions in pregnant women, 2 were community based and 2 were clinic based. All had an educational component and in 3 this was enhanced by counselling and/or psychosocial support of varying degrees. 1of the interventions involved distributing printed material at the clinic booking appointment and mailing a second pack at 26 weeks gestation; the others consisted of a number of contacts throughout the second half of pregnancy. Only 1 study in pregnant women provided specific outcome data in relation to a healthy diet as defined in this review; it had adequate statistical power and demonstrated small improvements in both control and intervention groups, with a greater, but statistical non-significant, improvement in the intervention group. This study also evaluated changes in knowledge and attitudes and demonstrated small changes in the desired direction in control and intervention groups; the difference in knowledge scores between the groups reached statistical significance but the magnitude of the difference is unlikely to represent an improvement which is worthwhile in practice. The other 3 studies suggested that pregnant women appear to improve their intake of energy and possibly protein in response to interventions designed to improve pregnancy outcomes, but they did not provide data on other components of a healthy diet or on knowledge or attitudes. Taken together it is not possible to conclude whether or not healthy eating interventions in pregnancy are effective.
Wantland D J et al 2004
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 22
Healthy adults What are the patient/client knowledge and behavioural change outcomes after Web-based interventions as compared to outcomes seen after implementation of non Web-based interventions?
Of the 17 studies assessing knowledge/behavioural change outcomes, 16 revealed improved knowledge and/or behavioural outcomes for P’s using web-based interventions, of which 6 were statistically significant (the one study favouring non-Web based intervention was not statistically significant). Effect sizes ranged from small (.01 to .19: 6 studies), moderate (.20 to .47: 5 studies) to moderately large (.54 to .75: 5 studies). There was no relation between the length of an intervention and its outcome effect size. 5 studies comparing assessment instruments/methods when administered to web-based and non web-based groups revealed 2 studies showing
Not clear, no discussion in paper. Relevance score: B
178

moderate negative effect sizes favouring the paper-based/traditional format (-.24 and -.22), neither of which were statistically significant. The remaining 3 studies showed small to moderate positive effect sizes (range of .17 to .44), only one of which was statistically significant. Most studies did not discuss ethnicity, income level or homelessness. In studies which reviewed their Web site statistics, there was large variability in the average intervention time and the number of logons to the sites. The average session time was 19.3 minutes. Interventions which directed the patient to relevant, individually tailored materials reported longer website session times per visit and more visits. Those which incorporated chat rooms showed increased social support scores.
White M, Carlin L & Rankin J 1998
Systematic review (including at least one RCT) Level: 2 Review quality: + No. of studies: 40 papers (reporting 29 studies)
Minority ethnic groups
What is the effectiveness of nutritional health promotion in minority ethnic groups?
One-to-one or small group counselling or education in home or clinic setting 3 studies were found to be effective, 2 ineffective and 3 inconclusive (no UK studies). 2 ‘one-to-one’ interventions failed to distinguish efficacy between different ethnic groups, and a third found that the intervention was effective in both black and white Ps. Classroom education in community or public centre (adult) 3 studies were effective, 5 partially effective and 4 inconclusive (all USA studies) Community-wide intervention 1 study partially effective, 4 inconclusive (no UK studies) Supplementation/fortification in clinic setting 2 studies effective (both UK) School-based interventions (children) 1 study effective, 7 partially effective, 3 ineffective and 2 inconclusive (no UK studies)
Only 2 of the studies were conducted in the UK and 23 out of 29 were conducted in the US. Relevance score: A
179
APPENDIX 8: References of reviewed papers Academic and Public Health Consortium 2005, “An assessment of brief interventions and referral for smoking cessation in primary care and other settings with particular reference to pregnant smokers and disadvantaged groups with consideration of the tailoring and targeting of interventions.”, London: National Institute for Health and Clinical Excellence.
Ammerman, A., Lindquist, C., Hersey, J., Jackman, A.M., Gavin, N.I, Garces, C., Lohr, K.N., Cary, T.S. & Whitener, B.L. 2001, The efficacy of interventions to modify dietary behavior related to cancer risk, Rockville: Agency for healthcare research and quality.
Ammerman, A.S., Lindquist, C.H., Lohr, K.N. & Hersey, J. 2002, "The efficacy of behavioral interventions to modify dietary fat and fruit and vegetable intake: A review of the evidence", Preventive medicine, vol. 35, no. 1, pp. 25-41.
Ashenden, R., Silagy, C. & Weller, D. 1997, "A systematic review of the effectiveness of promoting lifestyle change in general practice", Family Practice, vol. 14, No.2, pp. 160-175.
Ashworth, N.L., Chad, K.E., Harrison, E.L., Reeder, B.A., & Marshall, S.C. 2005,Home versus center based physical activity programs in older adults”, The Cochrane database of systematic reviews, issue 1. Bessell, T.L., McDonald, S., Silagy, C.A., Anderson, J.N., Hiller, J.E. & Sansom, L.M. 2002, "Do Internet interventions for consumers cause more harm than good? : a systematic review", Health Expectations, vol. 5, no. 1, pp. 28-37. Bize, R., Burnand, B., Mueller, Y. & Cornuz, J. 2005, Biomedical risk assessment as an aid for smoking cessation”, The Cochrane Database of Systematic Reviews Issue 4.
Blenkinsopp, A., Anderson, C. & Armstrong, M. 2003, "Systematic review of the effectiveness of community pharmacy-based interventions to reduce risk behaviours and risk factors for coronary heart disease", Journal of Public Health Medicine, vol. 25, no. 2, pp. 144-153.
Blue, C.L. & Conrad, K.M. 1995, "Adherence to worksite exercise programs: an integrative review of recent research", American Association of Occupational Health Nurses Journal, vol. 43, no. 2, pp. 76-86.
Brunner, E.J., Thorogood, M., Rees, K. & Hewitt, G. 2005, Dietary advice for reducing cardiovascular risk, The Cochrane Database of Systematic Reviews, Issue 4.
Brunton, G., Harden, A., Rees, R., Kavanagh, J., Oliver, S. & Oakley, A. 2003, Children and physical activity: a systematic review of barriers and facilitators, London: The Institute of Education, University of London.
180
Christakis, D.A., Garrison, M.M., Ebel, B.E., Wiehe, S.E. & Rivara, F.P. 2003, "Pediatric smoking prevention interventions delivered by care providers: a systematic review", American journal of preventive medicine, vol. 25, no. 4, pp. 358-362.
Ciliska, D., Miles, E. O’Brien, M.A., Turl, C., Tomasik, H.H., Donovan, U. & Beyers, J. 2000, “The effectiveness of community interventions to increase fruit and vegetable consumption in people four years of age and older”, Journal of Nutrition Education, vol. 32, no. 6, pp. 341-352.
Contento, I., Balch, G.I, Bronner, Y.L., Lytle, L.A., Maloney, S.K., Olson, C.M., & Swadener, S. S. 1995, "The effectiveness of nutrition education and implications for nutrition education policy, programs, and research: a review of research", Journal of Nutrition Education, vol. 27, no. 6, pp. 277-422.
Contributors to the Cochrane Collaboration and the Campbell Collaboration 2000, Evidence from systematic reviews of research relevant to implementing the 'wider public health' agenda., York: NHS Centre for Reviews and Dissemination.
Cyarto, E.V, Moorhead, G.E. & Brown, W. J. 2004, "Updating the evidence relating to physical activity intervention studies in older people", Journal of science and medicine in sport, vol. 7, no. 1 (Suppl), pp. 30-38.
DeHaven, M.J., Hunter, I.B., Wilder, L., Walton, J.W. & Berry, J. 2004, "Health Programs in Faith-Based Organizations: Are They Effective?", American Journal of Public Health, vol. 94, no. 6, pp.1030-1036.
Dishman, R.K. & Buckworth, J. 1996, "Increasing physical activity: A quantitative synthesis", Medicine and science in sports and exercise, vol. 28, no. 6, pp. 706-719.
Dobbins, M., Lockett, D., Michel, I., Beyers, J., Feldman, L., Vohra, J. & Micucci, S. 2001, “The effectiveness of school-based interventions in promoting physical activity and fitness among children and youth: a systematic review”, Ontario: Public health research, education and development program.
Edwards, N., Aubin, P. & Morrison, M. 2000, The effectiveness of postpartum smoking relapse prevention strategies Ontario: Public Health Research, Education and Development Program.
Engbers, L.H., van-Poppel, M.N.M., Paw, M.& van Mechelen, W. 2005, "Worksite Health Promotion Programs with Environmental Changes: A Systematic Review", American journal of preventive medicine , vol. 29, no. 1, pp. 61-70.
Eysenbach, G., Powell, J., Englesakis, M., Rizo, C. & Stern, A. 2004, "Health related virtual communities and electronic support groups: systematic review of the effects of online peer to peer interactions", British Medical Journal, vol. 328, no. 7449, pp. 1166-1170.
Fletcher, A. & Rake, C. 1998, Effectiveness of interventions to promote healthy eating in elderly people living in the community: a review, London: Health Education Authority.
181

Foster, C. & Hillsdon, M. 2004, "Changing the environment to promote health-enhancing physical activity", Journal of Sports Sciences, vol. 22, no. 8, pp.755-769.
Gepkens, A. & Gunning-Schepers, L.J. 1996, “Interventions to reduce socioeconomic health differences. A review of the international literature”, European Journal of Public Health, vol. 6, pp. 218-226. Gorin, S.S. & Heck, J.E. 2004, "Meta-analysis of the efficacy of tobacco counseling by health care providers", Cancer Epidemiology Biomarkers & Prevention, vol. 13, no. 12, pp. 2012-2022.
Hajek, P., Stead, L.F., West, R., Jarvis, M. & Lancaster, T. 2005, Relapse prevention interventions for smoking cessation”, The Cochrane Database of Systematic Reviews Issue 1.
Harden, A., Weston, R. & Oakley, A. 1999, A review of the effectiveness and appropriateness of peer-delivered health promotion interventions for young people, London: Evidence for Policy and Practice Information and Co-coordinating Centre.
Hey, K. & Perera, R. 2005, Competitions and incentives for smoking cessation, The Cochrane Database of Systematic Reviews, issue 2.
Hey, K. & Perera, R. 2005, Quit and Win contests for smoking cessation, The Cochrane Database of Systematic Reviews, issue 2.
Hider, P. 2001, Environmental interventions to reduce energy intake or density: a critical appraisal of the literature, Christchurch: New Zealand health technology assessment the clearing house for health outcomes and health technology assessment.
Hillsdon, M., Thorogood, M., Anstiss, T. & Morris, J. 1995, "Randomised controlled trials of physical activity promotion in free living populations: A review", Journal of Epidemiology and Community Health, vol. 49, no. 5, pp. 448-453.
Jepson, R. 2000, The effectiveness of interventions to change health-related behaviours: a review of reviews Glasgow: MRC Social & Public Health Sciences Unit.
Kaper, J., Wagena, E. J., Severens, J.L. & van-Schayck, C.P. 2005, Healthcare financing systems for increasing the use of tobacco dependence treatment, The Cochrane Database of Systematic Reviews Issue 1.
Ketola, E., Sipilä, R. & Mäkelä, M. 2000, "Effectiveness of individual lifestyle interventions in reducing cardiovascular disease and risk factors", Annals of medicine, vol. 32, pp.239-251.
Kramer, M. S. & Kakuma, R. 2003, Energy and protein intake in pregnancy, The Cochrane Database of Systematic Reviews Issue 4.
Krummel, D.A., Koffman, D.M., Bronner, Y., Davis, J., Greenlund, K., Tessaro, I., Upson, D. & Wilbur, J. 2001, "Cardiovascular health interventions in women: What works?", Journal of Women's Health and Gender Based Medicine, vol. 10, no. 2, pp. 117-134.
182
Lancaster, T. & Stead, L. F. 2005a, Individual behavioural counselling for smoking cessation, The Cochrane Database of Systematic Reviews, Issue 2.
Lancaster, T. & Stead, L. F. 2005b, "Self-help interventions for smoking cessation", The Cochrane Database of Systematic Reviews, Issue 3.
Lancaster, T. & Stead, L.F. 2004, Physician advice for smoking cessation The Cochrane Database of Systematic Reviews, Issue 4. Lawlor, D.A. & Hanratty, B. 2001, "The effect of physical activity advice given in routine primary care consultations: a systematic review", Journal of Public Health Medicine, vol. 23, no. 3, pp. 219-226.
Lawrence, D., Graber, J.E., Mills, S.L., Meissner, H.I & Warnecke, R. 2003, "Smoking cessation interventions in US racial/ethnic minority populations: an assessment of the literature", Preventive medicine, vol. 36, no. 2, pp. 204-216.
Lumley, J., Oliver, S.S., Chamberlain, C. & Oakley, L. 2004, "Interventions for promoting smoking cessation during pregnancy", The Cochrane Database of Systematic Reviews, Issue 4.
McArthur, D.B. 1998, "Heart healthy eating behaviors of children following a school-based intervention: a meta-analysis", Issues in Comprehensive Pediatric Nursing, vol. 21, no. 1, pp.35-48.
McBride, C.M., Emmons, K.M. & Lipkus, I.M. 2003, "Understanding the potential of teachable moments: The case of smoking cessation", Health education research, vol. 18, no. 2, pp.156-170.
McDonald, P., Colwell, B., Backinger, C.L., Husten, C. & Maule, C.O. 2003, "Better practices for youth tobacco cessation: Evidence of review panel", American journal of health behavior, vol. 27, supplement 2, pp. S144-S158.
McLean, N., Griffin, S., Toney, K. & Hardeman, W. 2003, "Family involvement in weight control, weight maintenance and weight- loss interventions: A systematic review of randomised trials", International Journal of Obesity, vol. 27, no. 9, pp. 987-1005.
Moher, M., Hey, K. & Lancaster, T. 2005, Workplace interventions for smoking cessation, The Cochrane Database of Systematic Reviews, Issue 2.
Morgan, O. 2005, "Approaches to increase physical activity: reviewing the evidence for exercise-referral schemes", Public health, vol. 119, no. 5, pp. 361-70.
Murphy-Hoefer, R., Griffith, R., Pederson, L.L., Crossett, L., Iyer, S.R. & Hiller, M.D. 2005, "A review of interventions to reduce tobacco use in colleges and universities", American journal of preventive medicine, vol. 28, no. 2, pp. 188-200.
Nishi, N., Jenicek, M., & Tatara, K. 1998, "A meta-analytic review of the effect of exercise on smoking cessation", Journal of Epidemiology, vol. 8, no. 2, pp. 79-84.
183

Ogilvie, D., Egan, M., Hamilton, V. & Petticrew, M. 2004, "Promoting walking and cycling as an alternative to using cars: Systematic review", British Medical Journal, vol. 329, no. 7469, pp. 763-766.
Park, E.W., Tudiver, F., Schultz, J.K. & Campbell, T. 2004, "Does Enhancing Partner Support and Interaction Improve Smoking Cessation? A Meta-Analysis", Annals of Family Medicine, vol. 2, no. 2, pp. 170-174.
Peersman, G., Harden, A. & Oliver, S. 1998, Effectiveness of health promotion interventions in the workplace: a review, London: Health Education Authority.
Petrella, R.J. & Lattanzio, C.N. 2002, "Does counseling help patients get active? Systematic review of the literature", Canadian Family Physician, vol. 48, pp. 72-80.
Posavac, E.J., Kattapong, K.R. & Dew, D.E.1999, "Peer-based interventions to influence health-related behaviors and attitudes: a meta-analysis", Psychological Reports, vol. 85, no. 3 Pt. 2, pp. 1179-94.
Rice, V.H. & Stead, L.F. 2004, Nursing interventions for smoking cessation, The Cochrane Database of Systematic Reviews Issue 1.
Roe, L., Hunt, P., Bradshaw, H. & Rayner, M. 1997, Health promotion interventions to promote healthy eating in the general population: a review, London: Health Education Authority.
Ryan, P. & Lauver, D. R. 2002, "The efficacy of tailored interventions", Journal of Nursing Scholarship, vol. 34, no. 4, pp. 331-337.
Secker-Walker, R.H., Gnich, W., Platt, S. & Lancaster, T. 2002, Community interventions for reducing smoking among adults”, The Cochrane Database of Systematic Reviews Issue 3.
Serra, C., Cabezas, C., Bonfill, X. & Pladevall-Vila, M. 2000, Interventions for preventing tobacco smoking in public places”, The Cochrane Database of Systematic Reviews Issue 3.
Shepherd, J., Harden, A., Rees, R., Brunton, G., Garcia, J., Oliver, S. & Oakley, A. 2001, Young people and healthy eating: a systematic review of research on barriers and facilitators" London: Evidence for Policy and Practice Information and Co-coordinating Centre.
Sinclair, H. K., Bond, C. M. & Stead, L. F. 2004, Community pharmacy personnel interventions for smoking cessation”, The Cochrane Database of Systematic Reviews Issue 1.
Sowden, A. & Stead, L. 2003, Community interventions for preventing smoking in young people, The Cochrane Database of Systematic Reviews, Issue 1.
Stead, L. F. & Lancaster, T. 2005a, “Group behaviour therapy programmes for smoking cessation” The Cochrane Database of Systematic Reviews, Issue 2.
184

Stead, L. F. & Lancaster, T. 2005b, Interventions for preventing tobacco sales to minors, The Cochrane Database of Systematic Reviews Issue 1. Stead, L.F., Lancaster, T. & Perera, R. 2003, Telephone counselling for smoking cessation, The Cochrane Database of Systematic Reviews Issue 1.
Stuart, W.P., Broome, M.E., Smith, B.A. & Weaver, M. 2005, "An integrative review of interventions for adolescent weight loss", Journal of School Nursing, vol. 21, no. 2, pp. 77-85.
Summerbell, C.D., Waters E., Edmunds, L.D., Kelly S., Brown, T. & Campbell K. J. 2005, "Interventions for preventing obesity in children (review)", The Cochrane Database of Systematic Reviews, Issue 3.
Taylor, W.C., Baranowski, T. & Young, D.R. 1998, "Physical activity interventions in low-income, ethnic minority, and populations with disability", American journal of preventive medicine, vol. 15, no. 4, pp. 334-343.
Tedstone, A.E., Aviles, M., Shetty, P.S. & Daniels, L. A. 1998, Effectiveness of interventions to promote healthy eating in preschool children aged 1 to 5 years, London: Health Education Authority.
Thomas, R. 2002, School-based programmes for preventing smoking, The Cochrane Database of Systematic Reviews, Issue 2.
Thompson, R.L., Summerbell, C.D., Hooper, L., Higgins, J.P.T., Little, P.S., Talbot, D. & Ebrahim, S. 2003, Dietary advice given by a dietitian versus other health professional or self-help resources to reduce blood cholesterol”, The Cochrane Database of Systematic Reviews Issue 3.
van Berkel, T.F., Boersma, H., Roos-Hesselink, J.W., Erdman, R.A. & Simoons, M.L. 1999, "Impact of smoking cessation and smoking interventions in patients with coronary heart disease", European Heart Journal, vol. 20, no.24, pp. 1773-1782.
van Teijlingen, E., Wilson, B., Barry, N., Ralph, A., McNeill, G., Graham, W. & Campbell, D. 1998, Effectiveness of interventions to promote healthy eating in pregnant women and women of childbearing age: a review, London: Health Education Authority.
Wantland, D.J., Portillo, C.J., Holzemer, W.L., Slaughter, R. & McGhee, E.M. 2004, "The effectiveness of web-based vs. non-web-based interventions: A meta-analysis of behavioral change outcomes", Journal of Medical Internet Research, vol. 6, no. 4, pp. e40.
White, M., Carlin, L., Rankin, J. & Adamson, A. 1998, Effectiveness of interventions to promote healthy eating in people from ethnic minority groups: a review” London: Health Education Authority.
185


















