BASHH Guideline on the Management of Vulvovaginal ... · 1 1 BASHH Guideline on the Management of...
42
1 BASHH Guideline on the Management of Vulvovaginal 1 Candidiasis (2018) 2 3 Clinical Effectiveness Group (CEG) 4 British Association for Sexual Health and HIV (BASHH) 5 6 Guideline Development Group 7 Cara Saxon (Lead Author), Anne Edwards, Riina Rautemaa-Richardson, Caroline Owen, Bavithra 8 Nathan, Bret Palmer, Clare Wood, Humera Ahmed, Sameena Ahmad, Patient Representatives (2), 9 Mark FitzGerald (CEG Editor) 10 11 New in the 2018 guidelines: 12 Terminology: 13 the new guidelines refer to ‘acute’, ‘recurrent’ and ‘chronic’ vulvovaginal candidiasis (VVC) and 14 no longer use the terms ‘uncomplicated’ and ‘complicated’ VVC; the new definitions are felt to 15 be more reflective of how women with VVC typically present to clinical services and are 16 subsequently managed 17 the elements of complicated VVC are still covered within the guideline 18 Diagnosis: 19 culture is no longer required in the setting of acute VVC 20 culture is still recommended for recurrent or chronic VVC with appropriate speciation and 21 sensitivity testing depending on clinical indication 22 greater emphasis has been placed on ensuring that other vulval pathologies are not missed in 23 the setting of possible recurrent or chronic VVC 24 interpretation of antifungal susceptibility testing is dependent on the pH at which the test is 25 performed 26 27
-
Upload
nguyennguyet -
Category
Documents
-
view
247 -
download
0
Transcript of BASHH Guideline on the Management of Vulvovaginal ... · 1 1 BASHH Guideline on the Management of...

1
BASHH Guideline on the Management of Vulvovaginal 1
Candidiasis (2018) 2
3
Clinical Effectiveness Group (CEG) 4
British Association for Sexual Health and HIV (BASHH) 5
6
Guideline Development Group 7
Cara Saxon (Lead Author), Anne Edwards, Riina Rautemaa-Richardson, Caroline Owen, Bavithra 8
Nathan, Bret Palmer, Clare Wood, Humera Ahmed, Sameena Ahmad, Patient Representatives (2), 9
Mark FitzGerald (CEG Editor) 10
11
New in the 2018 guidelines: 12
Terminology: 13
the new guidelines refer to ‘acute’, ‘recurrent’ and ‘chronic’ vulvovaginal candidiasis (VVC) and 14
no longer use the terms ‘uncomplicated’ and ‘complicated’ VVC; the new definitions are felt to 15
be more reflective of how women with VVC typically present to clinical services and are 16
subsequently managed 17
the elements of complicated VVC are still covered within the guideline 18
Diagnosis: 19
culture is no longer required in the setting of acute VVC 20
culture is still recommended for recurrent or chronic VVC with appropriate speciation and 21
sensitivity testing depending on clinical indication 22
greater emphasis has been placed on ensuring that other vulval pathologies are not missed in 23
the setting of possible recurrent or chronic VVC 24
interpretation of antifungal susceptibility testing is dependent on the pH at which the test is 25
performed 26
27

2
Treatment: 1
Oral azoles – continue to avoid in pregnancy, risk of pregnancy and breast feeding 2
Ketaconazole is no longer recommended for the treatment of VVC 3
Non-azole therapies to be reserved for azole resistance and certain non-albicans Candida species 4
Licensed nystatin pessaries are no longer available; various unlicensed brands of nystatin 5
pessaries are available but some are imported so the patient information leaflet may not be in 6
English and there have been intermittent supply issues 7
8
9
INTRODUCTION AND METHODOLOGY 10
Objectives 11
This guideline offers recommendations on the diagnostic tests, treatment regimens and health 12
promotion principles for the effective management of vulvovaginal candidiasis (VVC). It covers the 13
management of acute, recurrent and chronic VVC. 14
It is aimed at individuals aged 16 years and older (see specific guideline for under 16 year olds) 15
presenting to healthcare professionals working in departments offering level 3 care in sexually 16
transmitted infections (STIs) management within the UK. 17
However, the principles of the recommendations can be applied in other settings using local care 18
pathways where appropriate. Guidelines for the management of vaginal discharge in non-19
genitourinary medicine settings can be found at www.fsrh.org/guidelines. 20
21
Search strategy 22
This document was produced in accordance with the guidance set out in the CEG’s document 23
‘Framework for guideline development and assessment’ at http://www.bashh.org/guidelines. The 24
GRADE system was used to assess the evidence and make recommendations as detailed in the 25
guidance. 26
The following reference sources were used to provide a comprehensive basis for the guideline: 27
1. Medline, Embase, Cochrane and CINAHL Search 28
a. January 2007-August 2016+ 29

3
b. The search strategy comprised the following terms in the title or abstract: [Vagina* 1
OR vulva* OR vulvovaginal OR vulvo-vaginal OR vaginosis OR vaginitis OR vulvitis OR 2
thrush (NOT oral)] AND [Candida OR candidiasis OR candidosis OR yeast]. The search 3
was limited to English language and human subjects. 1412 citations were identified. 4
2. 2007 UK National Guidelines on the Management of Vulvovaginal Candidiasis. 5
+ The search period was extended to March 2018 during the peer review of first draft of the 6
guideline to identify any new relevant evidence. 7
8
Methods 9
The broad search terms used above were necessary given the various international terminology 10
used for VVC but resulted in a large number of citations (1412). 11
The article titles and abstracts of all 1412 citations were reviewed for relevance. Citations clearly 12
from animal studies, non-patient based studies, single case reports, studies in children, and 13
those on subjects not relevant to the diagnosis or management of VVC were excluded on first 14
review. 15
The titles and abstracts of the remaining citations (800) were reviewed by at least two members 16
of the writing group. Priority was given to randomised controlled trials, systematic review 17
evidence, and studies related to pertinent clinical questions to be addressed by the guideline. 18
The full texts of approximately 210 citations were obtained and reviewed using the GRADE 19
system by at least two members of the writing group. Recommendations were made and graded 20
on the basis of best available evidence. 21
22
Equality impact assessment 23
To be included in final publication 24
25
Piloting & feedback 26
The first draft was produced by the writing group and then circulated to BASHH CEG for using the 27
AGREE appraisal tool. The second draft of the guideline is posted on BASHH website for wider 28
consultation and simultaneously reviewed by the BASHH Public Panel. The final draft will be 29
presented to the CEG for review and piloting in their clinics. 30

4
Once the guideline is published to the BASHH website the CEG will keep it under review should 1
critical new evidence become available that affects the current recommendations. The guideline will 2
be formally reviewed and updated every 5 years. 3
4
5
DEFINITIONS 6
Acute VVC 7
first or single isolated presentation of vulvovaginal candidiasis (VVC) 8
patients typically present with signs and symptoms of acute vulvovaginitis and are usually 9
microscopy and culture positive for a Candida sp. 10
11
Recurrent VVC 12
at least 4 episodes per 12 months with 2 episodes confirmed on microscopy or culture when 13
symptomatic (at least one must be culture) 14
patients typically report good or complete responses to therapy and are asymptomatic between 15
episodes. 16
17
Chronic VVC 18
Patients present with chronic, continuous symptoms, which may improve during menses and 19
typically remit with antifungal therapy, often recurring when this is ceased, particularly after 20
short course therapy (usually but not always confirmed on microscopy or culture at 21
presentation), OR 22
recurrent episodes or chronic symptoms suggestive of VVC confirmed on microscopy or culture 23
whilst patients are symptomatic and reporting poor or partial response to therapy. 24
25
26
27

5
AETIOLOGY 1
Candidiasis is a fungal infection caused by yeasts that belong to the genus Candida. Yeasts are 2
eukaryotic, unicellular microorganisms which have the ability to develop multicellular characteristics 3
by forming pseudohyphae and biofilms. Candida yeasts are present in low numbers on healthy skin 4
in moist areas and are part of the normal flora of the mucous membranes of the respiratory, 5
gastrointestinal and female genital tracts; overgrowth of these organisms can cause infection to 6
develop. There are over 20 species that can cause infections in humans, of which Candida albicans is 7
the most common. Candida can also cause serious systemic infections, but these do not originate 8
from the genital tract infections. 9
Vulvovaginal candidiasis (VVC) is caused by: 10
Candida albicans in 80-89% 1, 2, 3 11
other Candida species or yeasts such as C. glabrata, C. tropicalis, C. krusei, C. parapsilosis, 12
and Saccharomyces cerevisiae in the remainder 13
Despite the widespread availability of antifungal agents in the UK and other countries there has not 14
been a significant increase in azole resistance in C. albicans species or increased prevalence of non-15
albicans Candida species. 3-5 There remains conflicting evidence on the virulence of non-albicans 16
Candida species compared with C. albicans. 6, 7 17
An estimated 75% of women will have at least one lifetime episode of VVC, and 40%–45% will have 18
two or more episodes. 8 Previous studies have reported that approximately 5% of women of 19
reproductive age with a primary episode of VVC will develop recurrent disease. 9, 10 A large internet-20
based survey across five European countries (including the UK) and the US found that over 20% of 21
women reporting at least one episode of vaginal yeast infection also reported a 12-month period 22
with four or more infections. The probability of developing recurrent VVC after an initial infection 23
was 10% by the age of 25 years and 25% by the age of 50 years. 11 24
25
Risk factors and pathogenesis 26
Recurrent and chronic VVC are thought to be related to host factors rather than a more virulent 27
strain or the reintroduction of the organism to the genital tract. The majority are usually due to C. 28
albicans. 12 For many women an identifiable host factor is not found but can include: 29
persistence of Candida sp (as detected by PCR although culture-negative between attacks) 13 30
poorly controlled diabetes mellitus 31

6
immunosuppression 1
hyperoestrogenaemia (including HRT and the combined oral contraceptive pill) 14-18 2
recent (up to three months before the episodes) antibiotic use causing a disturbance in the 3
vaginal flora 14, 19, 20 4
Studies have also identified a link to allergy (allergic rhinitis, asthma and hay fever)17, 21 and pro-5
inflammatory genetic markers. However women suffering from allergic diseases are more likely to 6
have used corticosteroids, so it is unclear as to whether the steroid use, or concomitant atopic 7
disease makes them more susceptible. 17 Perceived increased stress and a lower mean cortisol 8
(which may correspond to chronic stress) have been weakly associated with recurrent VVC however 9
the evidence is limited and further research is required. 22 10
It is unclear if iron deficiency anaemia is associated with recurrent VVC. A previous study found no 11
evidence of low iron levels in women with VVC23 however a more recent study suggests a possible 12
link between iron deficiency anaemia and recurrent VVC. 24 The earlier study reported statistically 13
significant lower serum level of zinc, magnesium and calcium in patients with recurrent VVC, 14
although all levels were still within the normal range; other studies have not supported the link with 15
serum zinc levels. 23, 25 16
Mannose binding lectin (MBL) deficiency is genetic condition that affects the immune system. 17
Several studies have shown that MBL codon 54 gene polymorphism is associated with recurrent and 18
acute VVC. In particular, possessing the MBL variant allele B heterozygous genotype increases the 19
susceptibility of women to recurrent or acute VVC compared to healthy controls, while the risk of 20
recurrent VVC is also increased for women carrying the allele B homozygote genotype. 26-28 21
22
23
CLINICAL FEATURES 24
Vulvovaginal candidiasis (VVC) typically presents with: 29-33 25
vulval itch and 26
a non-offensive vaginal discharge 27
28
Other symptoms can include: 29, 32-34 29
soreness or burning 30
7
superficial dyspareunia 1
cyclical symptoms 2
3
Clinical signs may include: 29-34 4
erythema 5
fissuring 6
swelling/oedema 7
vaginal discharge typically non-offensive and curdy but may be thin or absent 8
there may also satellite lesions and excoriation marks 9
10
None of these features are pathognomonic for VVC and there can be a significant discrepancy 11
between symptoms and signs particularly in chronic disease. 34, 35 Although Candida albicans is the 12
most pathogenic of the Candida species clinical symptoms or signs cannot be used to guide which 13
Candida sp is the cause for the infection. 35, 36 Health-related quality of life both physical and 14
psychological is significantly affected in recurrent VVC. 32 15
16
Differential diagnoses and colonisation 17
Many women (more than half of self-diagnosed women in one study 37) presenting with these 18
symptoms may have other conditions such as: 19
o dermatitis/eczema 20
o lichen sclerosus 21
o other infections 22
o vulvodynia 23
the preponderance of certain symptoms and signs, whilst not pathognomonic can be more 24
suggestive of other conditions (table 1 and 2) 25
it should also be noted that some women may have dual pathology with VVC and one of these 26
other conditions 27
up to 20% of women during reproductive years may be colonized with Candida spp. but have no 28
clinical signs or symptoms; 38,39 these women do not require treatment 29

8
it is also possible that women with vulval symptoms due to other conditions (such as eczema, 1
lichen sclerosus) may have colonization with Candida which is not necessarily contributing to the 2
symptoms. 3
4
DIAGNOSIS 5
Vulvovaginal candidiasis (VVC) is a clinical diagnosis based on typical features supported by 6
laboratory confirmation of Candida sp. from a vaginal sample 7
In women presenting with clinical features of acute VVC to a service providing level 3 STI care 8
supporting the diagnosis with routine microscopy is good clinical practice 35, 40-45 (Grade 1B) 9
(figure 1) 10
Recurrent or chronic VVC is defined as four or more symptomatic episodes over a 12-month 11
period; at least two of these episodes should be confirmed by microscopy or culture, one of 12
these should be a positive culture with moderate or heavy growth of Candida sp. 46-49 (Grade 1C) 13
14
Clinical examination and syndromic management 15
Clinical examination of the external genitalia is recommended in women presenting with 16
symptoms suggestive of acute VVC in order to exclude alternative or co-existing vulvovaginal 17
pathologies 18
Women presenting with features suggesting recurrent or chronic VVC should always have a 19
clinical examination 50 (Grade 1C) 20
Empirical treatment for acute VVC based on the reported symptoms may be given in non-21
specialist settings 51; if the symptoms do not resolve, or if they recur, examination and 22
microbiological testing (as below) should be performed 50 23
24
Microscopy 25
A vaginal swab taken from the anterior fornix 52 (Grade 1C) for Gram stain and/or dark field wet 26
film microscopy 27
Presence of spores, pseudohyphae and neutrophils is indicative of infection caused by Candida 28
species 29
Presence of spores only and neutrophils may reflect infection caused by C. glabrata 30

9
Neutrophils in vaginal secretions suggest an inflammatory response and therefore presence of 1
infection which may or may not be due to Candida seen on microscopy. Absence of neutrophils 2
in the presence of Candida is likely to represent colonisation. 3
4
Culture 5
Acute VVC: 6
fungal culture is no longer considered a cost-effective addition to microscopy nor a reliable test 7
on its own for the diagnosis of VVC due to its inability to differentiate colonisation from infection 8
9
Recurrent or chronic VVC: 10
a vaginal swab should be taken from the anterior fornix 52 (Grade 1C) for direct plating onto solid 11
fungal growth medium (Sabouraud plate) 12
any fungal growth should ideally be identified to species level, or at least as C. albicans/non-13
albicans Candida 46-49 (Grade 1B) and sensitivity to fluconazole tested 14
mixed infection with C. albicans and a non-albicans Candida species are not rare and should be 15
sought for in the laboratory 16
in cases of recurrent or chronic VVC with poor or partial response to therapy, full speciation and 17
sensitivity testing to fluconazole, clotrimazole, flucytosine, amphotericin B and nystatin is 18
preferred 19
of note clotrimazole is broader spectrum and used at higher concentrations than fluconazole so 20
fluconazole susceptibility cannot be used as a marker for clotrimazole resistance 21
where clinical examination is not possible or required self-collected vaginal swab for microscopy 22
and or culture is a reasonable alternative to clinician taken samples 53 (Grade 1C) 23
self-collected swabs done at home can be considered in recurrent or chronic VVC where initial 24
samples collected in clinic have come back negative 54, 55 (Grade 2C) 25
for patients reporting poor or partial response to sensitivity guided antifungal therapy a negative 26
post-treatment fungal culture (implying mycological cure) indicates the need to consider 27
alternative or additional diagnoses with similar clinical features. 28
29

10
Interpretation of anti-fungal sensitivity testing 1
It is useful to know that standard in vitro susceptibility testing for Candida spp. is performed at 2
pH 7.0 because the activity of most azole antifungals is significantly decreased in acidic 3
environment 4
in cases of VVC, the vaginal pH is usually in the range of 4 to 4.5, therefore, isolates with 5
elevated MICs are unlikely to respond to standard doses of azole treatment despite still 6
designated as susceptible: 7
o e.g. C. glabrata has variable intrinsic resistance to azole antifungals and their marginal 8
efficacy is lost at pH 4.5 9
if standard neutral pH is used for susceptibility testing caution is needed when interpreting the 10
results as standard breakpoints may not apply. 56 (Grade 1B) 11
12
Molecular and point of care testing for VVC 13
A number of studies have looked at molecular and rapid antigen detection point of care tests for 14
Candida. 57-59 There are significant differences between the tests and their sensitivity and specificity 15
when compared with the agreed standard of care (microscopy and culture). Some tests are highly 16
sensitive and unable to differentiate between colonization and infection. Further research and 17
evaluation of cost-effectiveness is required before any recommendations can be made regarding 18
their use in level 3 STI services. 19
20
STI screening 21
VVC is not a sexually transmitted infection (STI) or a marker for STIs. The offer of STI screening 22
should be based on a risk assessment and consideration that some of the clinical features of VVC are 23
similar to those of STIs. For comprehensive guidance on screening for STIs please refer to the 2015 24
BASHH CEG group guidance on tests for STIs [https://www.bashhguidelines.org/media/1084/sti-25
testing-tables-2015-dec-update-4.pdf]. 26
27
28
29
30

11
MANAGEMENT 1
General advice for all women with VVC symptoms 2
Patients should also be provided with information about the importance of good skin care: 3
avoiding the use of local irritants such as perfumed soaps or wipes 4
the use an emollient cream for personal hygiene as a soap substitute, as a moisturiser and a 5
barrier cream (patient needs to be informed that this does not constitute “internal use”). 6
7
General advice for recurrent and chronic VVC 8
In patients with recurrent or chronic VVC careful review of their daily hygiene routine may identify 9
potential local irritants not perceived as such by the patient for example washing hair in bath water 10
or excessive cleaning. (grade 2D) No genital hygiene practices have been definitively linked with 11
recurrent or chronic VVC however a number have shown weak associations which may be worth 12
considering in certain patients: 13
wearing of tight fitting synthetic clothing 14, 60, 61 (grade 2C) 14
using intermenstrual or daily panty liners 61-64 (grade 2C) 15
vaginal douching 20, 61, 65, 66 (grade 2C) 16
Vulval emollients may give symptomatic relief as vulval dermatitis (eczema) both primary and 17
secondary is commonly present. 18
An association between sexual intercourse and Candida colonisation levels or vaginal symptoms has 19
not been identified although there is a paucity of research in this area. 67 Patients reporting a link 20
between symptoms and sexual activity may wish to consider the use of a gentle water-based 21
lubricant. (grade 2D) 22
23
Further Investigation 24
No additional investigations are routinely recommended in patients presenting with acute VVC 25
unless clinically indicated. 26
In recurrent or chronic VVC screening for the following conditions may be considered particularly if 27
there are additional indicators: 28
diabetes with urinalysis or random blood glucose (grade 2C) 29

12
iron-deficiency anaemia with a full blood count or serum ferritin (grade 2C) 1
mannose binding lectin deficiency* (grade 2B) 2
3
*Some women with recurrent VVC can spend considerable time searching for answers as to why 4
they are affected by the condition often trialing extreme lifestyle measures to reduce symptoms. 5
Identifying MBL deficiency or the MBL 54 gene polymorphism may help a patient better understand 6
their condition, offer additional reassurance and reduce the need for significant lifestyle changes 7
that can impact on quality of life and are unlikely to improve symptoms. Additionally, patients with 8
the B allele polymorphism have been found to have an improved response to a reducing 9
maintenance regimen with fluconazole therapy. 27 (grade 2C) 10
11
12
TREATMENTS 13
Acute VVC 14
Treatment choice: 15
Studies and data published over the past 10 years on the treatment of acute vulvovaginal candidiasis 16
(VVC) support the treatment regimen recommended in the 2007 guidelines: 17
all intravaginal imidazoles and oral azoles give a clinical and mycological cure rate of over 80% in 18
acute VVC 68, 69 (Grade 1B) 19
intravaginal imidazoles and oral azoles are equally effective and tolerable in the management of 20
acute VVC with no difference in treatment outcomes 69-72 (Grade 1B) 21
recommended and alternative regimens have been made for this guideline update based on 22
differences in cost and convenience of dosing: 23
o Fluconazole 150mg stat PO is the recommended treatment for acute VVC due to 24
comparative cost and convenience of the stat dose (7-30 times cheaper than all other 25
listed regimens; current UK prices June 2018) 26
o Clotrimazole 500mg pessary PV stat is the recommended topical treatment when an oral 27
imidazole is contraindicated, due to comparative cost (with other topical agents) and 28
convenience of the stat dose (current UK list prices June 2018) 29

13
one RCT suggested that a single dose of oral fluconazole may be more effective than prolonged 1
intravaginal clotrimazole 200mg (for 6 days) at clinical cure at 7 days. 70 (Grade 1C) 2
3
Treatment considerations: 4
oral therapies must be avoided in pregnancy, risk of pregnancy and breast feeding 39, 60, 69 (Grade 5
1B) 6
oral azoles also prolong the QT time and caution should be taken if prescribed in combination 7
with other drugs with a similar effect 8
as there is minimal absorption of topically applied imidazoles from the vulvo-vaginal mucosae 9
there is limited risk of systemic side effects 10
topical therapies can cause vulvovaginal irritation and this should be considered if symptoms 11
worsen or persist 12
intravaginal and topical treatments can also damage latex condoms and diaphragms with case 13
reports of unplanned pregnancies 70; women must be appropriately counselled about this risk 14
a medication history should be taken to advise women that oral fluconazole and other azoles as 15
can interact with medications; fluconazole is a potent inhibitor of cytochrome P450 (CYP) 16
isoenzyme 2C9 and a moderate inhibitor of CYP3A4O 17
18
Nystatin preparations give a 70-90% cure rate in the setting of acute VVC. 39 There is insufficient 19
evidence to show a significant difference between intravaginal imidazoles and nystatin pessaries in 20
the treatment outcomes. There is data showing that intravaginal nystatin is well tolerated with cure 21
rates comparable to fluconazole. 73 One study showed that boric acid was cheap and tolerable to use 22
in the treatment of acute VVC. 74 However: 23
both nystatin and boric acid are unlicensed drugs and should be reserved for the management 24
of infections caused by azole resistant Candida strains. 25
26
Recommended regimen: 27
Fluconazole* capsule 150mg stat PO (1B) 28
29

14
Recommended topical regimen (if oral therapy contraindicated): 1
Clotrimazole pessary 500mg stat PV** (1B) 2
3
Alternative regimens: 4
Clotrimazole vaginal cream (10%) 5g stat** (1B) 5
Clotrimazole pessary 200mg nocte for 3 days or 100mg nocte for 6 days** (1C) 6
Econazole pessary 150mg stat or 150mg nocte for 3 days** (1B) 7
Fenticonazole pessary 600mg stat or 200mg nocte for 3 nights** (1B) 8
Itraconazole 200mg bd for 1 day PO* (1B) 9
Miconazole pessary 100mg nocte for 14 nights** (1B) 10
11
* Oral therapies must be avoided in pregnancy, risk of pregnancy and breast feeding 39, 60, 69 (Grade 12
1B) 13
**Creams and pessaries may damage diaphragms and latex condoms. 14
15
Recurrent VVC 16
The principle of therapy involves an induction regimen to ensure clinical remission, followed 17
immediately by a maintenance regimen: 18
Fluconazole 150mg every 72 hours for 3 doses followed by 150mg weekly for a six-month period 19
has been shown to have good efficacy and tolerability in two randomized control trials achieving 20
clinical remission in 82-90% 75 (Grade 1A) 21
Fluconazole reduced the frequency of recurrent VVC in 88% immediately after the cessation of 22
therapy, 64% at 3 months after and 61% at 6 months after the end of treatment 75 23
when oral therapy needs to be avoided 500 mg of intravaginal clotrimazole administered weekly 24
may used as an alternative (Grade 1B) 25
there is no evidence for the superiority of itraconazole over fluconazole and microbiological 26
cross-resistance is common whereby it is not likely to be helpful in clinically fluconazole-resistant 27
cases 28

15
if a patient relapses between doses consider twice-weekly 150mg fluconazole or 50mg 1
fluconazole daily; (Grade 2C)alternatively consider the addition of cetirizine 10mg od 76 2
there is a low risk of idiosyncratic drug-induced hepatitis with oral azoles, although fluconazole is 3
less frequently associated with hepatotoxicity than itraconazole (see later ‘Reactions to 4
treatment’); the production of Ketaconazole has stopped globally due to toxicity. 5
6
There are no trials addressing the optimal duration of suppressive therapy with the majority of trials 7
using 6 months maintenance as standard: 8
if recurrences after maintenance regimen are infrequent, each episode should be treated 9
independently 10
if recurrent disease is re-established the induction and maintenance regimens should be 11
repeated (Grade 2C) 12
13
One study achieved clinical remission in 90% of women at 6 months and 77% of women at 12 14
months using an individualized reducing regimen of fluconazole. 77 However it is not clear how this 15
strategy compares to the standard 6 month regimens. A study comparing these strategies is 16
required before recommendations on reducing regimens can be made. 17
18
Recommended Regimen: 19
Induction: fluconazole 150mg every 72 hours x 3 doses* (1A) 20
Maintenance: fluconazole 150mg once a week for 6 months* (1A) 21
22
Alternative Regimens: 23
Induction: topical imidazole therapy can be increased to 10-14 days according to 24
symptomatic response(Grade 2C) 25
Maintenance for 6 months: 26
o Clotrimazole pessary 500mg once a week (1B) 27
o Itraconazole 50-100mg daily*(2C) 28
29

16
* Oral therapies must be avoided in pregnancy, risk of pregnancy and breast feeding 39, 60, 69 (Grade 1
1B) 2
3
Chronic VVC 4
Patients reporting chronic, continuous symptoms, which may improve during menses and remit with 5
antifungal therapy have only recently been recognized as having a distinct condition to recurrent 6
VVC 33: 7
symptoms often recur when therapy is stopped, particularly after short course therapy 8
management is often challenging and further research into appropriate treatment strategies and 9
duration is needed 10
general advice should be given as above 11
suppressive treatment regimens such as those recommended for recurrent VVC should be 12
trialed 13
rescue doses of antifungal therapy during antibiotic courses may be considered, especially if this 14
was a known previous precipitant of flares 33 (Grade 2C) 15
refer patients in this category to specialized vulval services. 16
17
One retrospective study of 208 patients found long-term maintenance regimens of fluconazole or 18
itraconazole were well tolerated in women with chronic VVC (mean duration of follow up 26.2 19
months; range 5 months to 8.5 years). 78 A study comparing maintenance regimens and durations is 20
required before specific recommendations can be made. 21
It’s important to note that patients reporting recurrent episodes or chronic symptoms of VVC with 22
poor or partial response to therapy may have a non-albicans Candida species and/or azole 23
resistance. A sustained resolution of symptoms may be achievable for these patients with the 24
correct treatment following species identification with antifungal sensitivity testing. 25
26
27
28
29

17
Non-albicans Candida species and azole resistance 1
Candida albicans is normally susceptible to all yeast-active antifungals although resistance may 2
rarely develop on prolonged or repeated azole treatment courses; resistance to other yeast-3
active antifungals is very rare 4
the most common non-albicans Candida species causing vulvovaginitis are Candida glabrata and 5
Candida krusei: 6
o these can be the sole cause of infection or in combination with C. albicans 7
o most vaginal C. glabrata strains are reported as susceptible to azoles 79 but with 8
elevated MICs and often with poor clinical response to standard dose treatment 9
o Candida krusei is intrinsically resistant to fluconazole 80 10
some non-albicans Candida species such as C. guilliermondii and C. parapsilosis are normally 11
susceptible to azoles and patients clinically respond to treatment with these 12
for an infection caused by an azole resistant Candida species longer courses are advised 13
although there is no data on optimum duration; two weeks is suggested 14
for isolates with an elevated MIC but still designated susceptible, higher and more frequent 15
dosing of fluconazole may be effective (200-300 mg od over 48 hrs for 1 week) 16
17
Treatment options and availability: 18
Nystatin pessaries are the only licensed alternative to azole therapy and are therefore the usual first 19
line treatment for non-albicans Candida infection. (Grade 1B) Unfortunately the licensed nystatin 20
product is no longer available (March 2018). Various unlicensed brands of Nystatin pessaries are 21
available but some are imported so the patient information leaflet may not be in English and there 22
have been intermittent supply issues. An alternative would be local pharmacy production of 23
Amphotericin B vaginal suppositories 50mg once a day for 14 days which is has a 70% success rate 24
but there can also be sourcing difficulties. 80(Grade 2C) 25
Boric acid vaginal suppositories 600mg daily for 14 days are a safe and effective alternative. 79, 82 26
(Grade 1B) If mucosal irritation occurs the dose can be reduced to 300mg daily (additional cost likely 27
as it needs to be compounded specially). 83 There may be a teratogenic risk so boric acid should be 28
avoided in pregnancy or risk of pregnancy. 84 29
Intravaginal flucytosine (5g cream or 1g pessary) either alone 79, 85 or with amphotericin 5, 85 to reduce 30
the chances of resistance (for which there is a low genetic barrier) can also be used for two weeks. 31
(Grade 2C) 32

18
In patients with recurrent or chronic VVC due to fluconazole resistant Candida species, 14 days of 1
nystatin pessaries a month for 6 months has been shown to be effective and is more likely to 2
achieve mycological cure than fluconazole regimens. 86 (Grade 2C) There is no evidence for the 3
treatment protocols for the alternative treatment options but it would seem reasonable to consider 4
extrapolating this suggested regimen of 14 days a month for 6 months to the alternative options. 5
(Grade 2D) 6
There are no studies where the efficacy and tolerability of these drugs has been compared. Where 7
there is reduced sensitivity increasing the dose or combining topical and oral agents may be 8
beneficial. 9
10
Recommended Regimen: 11
Nystatin pessaries 100,000units nocte for 14 days (1B) 12
13
Alternative Regimens: 14
Boric acid suppositories 600mg daily for 14 days* (1B) 15
Amphotericin B vaginal suppositories 50mg once a day for 14 days (2C) 16
Flucytosine 5g cream or 1g pessary +/- amphotericin daily for 14 days (2C) 17
18
Recurrent or chronic VVC due to azole resistant Candida: 19
Nystatin pessaries 100,000units nocte for 14 days/month for 6 months (2C) 20
Consider 14 days per month for 6 month of the alternative regimens (2D) 21
22
*Avoid in pregnancy or risk of pregnancy 23
24
Severe Vulvovaginal Candidiasis 25
In patients with severe VVC (i.e., extensive vulvar erythema, oedema, excoriation, and fissure 26
formation) 87 regardless of a history of recurrence, fluconazole 150mg should be repeated after 27
three days as this improves symptomatic response but does not influence the risk or rate of 28
recurrence. 88 (Grade 1B) There is no benefit of a seven day topical treatment course over a single 29
19
oral dose of fluconazole. 89 If oral treatment is contra-indicated it is more logical to repeat a single 1
dose pessary after three days. Two doses of clotrimazole 500mg vaginal tablet or miconazole nitrate 2
vaginal suppository 1,200 mg were as effective as two doses of an oral fluconazole 150 mg regimen 3
in the treatment of patients with severe VVC. 90, 91 (Grade 1B). Due to significant differences in cost 4
fluconazole is the recommended regimen. 5
6
Recommended regimen: 7
Fluconazole 150mg on day 1 and 4 (1B) 8
9
Alternative regimens: 10
Clotrimazole 500mg tablet or pessary on day 1 and 4 (1B) 11
Miconazole nitrate vaginal suppository 1200mg on day 1 and 4 (1B) 12
13
Low-potency corticosteroids are also thought by some experts to improve symptomatic relief in 14
conjunction with adequate antifungal therapy. 92 (Grade 2D) 15
16
Pregnancy & Breastfeeding 17
Asymptomatic colonization with Candida species is more common (30-40%) 15 and symptomatic 18
candidiasis is more prevalent throughout pregnancy 19
oral therapies must be avoided in pregnancy, risk of pregnancy and breast feeding 39, 60, 69 (Grade 20
1B) 21
topical imidazoles should be used for symptomatic VVC in pregnancy and breast feeding (Grade 22
1B) 23
there is no evidence that any one topical imidazole is more effective than another 24
longer courses are recommended in pregnancy; a four day course will cure just over 50% 25
whereas a seven day course cures over 90%. 93 (Grade 1B) 26
27
28

20
Fluconazole in pregnancy 1
Given the conflicting evidence we continue to advise against the use of fluconazole and other oral 2
azoles in pregnancy (Grade 1B): 3
there is accumulating evidence that that treatment with fluconazole in the first trimester does 4
not appear to increase the overall risk of congenital malformations although one study reported 5
a possible link with tetralogy of Fallot 94 6
the United States National Birth Defects Prevention Study (NBDPS) found associations between 7
fluconazole use in the first trimester of pregnancy with cleft lip with cleft palate and d-8
transposition of the great arteries although overall fluconazole use in the NBDPS was low 95 9
a nationwide register-based cohort study in Denmark (1997-2013) with a cohort of 1405500 10
pregnancies found a statistically significant increased risk of spontaneous abortion in women 11
exposed to fluconazole between 7-22 weeks gestation compared with risk among unexposed 12
women and women with topical imidazole exposure in pregnancy. 96 13
14
VVC and pregnancy outcome 15
Previous studies did not find evidence of an association between Candida colonization and 16
premature delivery or low birth weight (BASHH 2007 26, 27) 17
Currently there is very limited evidence around the significance of detecting asymptomatic VVC 18
in pregnancy and the theoretical risk of pre-term birth or low birth weight; in the absence of well 19
designed studies we are not in a position to make specific recommendations. 97-99 20
21
Recommended regimens (Acute VVC): 22
Clotrimazole pessary 500mg PV nocte for 7 days (1B) 23
24
Alternative regimens (Acute VVC): 25
Clotrimazole vaginal cream (10%) 5g nocte for 7 days** (1C) 26
Clotrimazole pessary 200mg or 100mg nocte for 7 days** (1C) 27
Econazole pessary 150mg nocte for 7 days** (1C) 28
Fenticonazole pessary 600mg stat or 200mg nocte for 7 days** (1C) 29

21
Miconazole pessary 100mg nocte for 14 nights** (1C) 1
2
Recommended regimen (Recurrent/Chronic VVC): 3
Induction: topical imidazole therapy can be increased to 10-14 days according to symptomatic 4
response(Grade 2C) 5
Maintenance: Clotrimazole pessary 500mg weekly (1C) 6
7
Breastfeeding: 8
Treatment regimens using topical imidazoles only should be as per the recommendations listed 9
above for non-pregnant women with acute, recurrent and chronic VVC. 10
11
Alternative or Supplementary Treatments 12
Proven benefit: 13
Antihistamines: 14
o Zafirlukast 20mg bd for 6 months may induce remission. 100 15
o Zafirlukast may be considered as maintenance prophylaxis for recurrent VVC, 16
particularly in women with a history of atopy76 17
o Cetirizine 10mg daily for 6 months may cause remission in women who fail to get 18
complete resolution of symptoms with suppressive fluconazole. 76(Grade 1C) 19
20
Insufficient or no evidence of benefit: 21
Probiotics: there continues to be insufficient evidence to support the use of oral or vaginal 22
probiotics (mainly Lactobacilli) for the treatment or prevention of VVC: 23
o An increasing number of studies suggest that their adjunctive use may improve clinical 24
outcomes or reduced the likelihood of recurrence 70, 101, 102 25
o However, the quality of evidence is variable and inconsistent in terms of the probiotic or 26
regimen used 103, 104 27

22
o the mode of action might be via modulation of inflammatory processes rather than 1
competition with Candida. 105 2
Tea tree and other essential oils: are antifungal in vitro but they may cause hypersensitivity 3
reactions. 70, 106 There is insufficient evidence to recommend use in recurrent VVC. 70 4
Dermasilk® briefs: are made of a pure fibroin fabric impregnated with a permanent 5
antimicrobial protection. Small studies have shown a reduction in itching, burning, erythema and 6
recurrences than cotton briefs in women with recurrent VVC on a standard fluconazole 7
suppressive regimen. 107 8
Yoghurt and honey mixes: there is insufficient evidence to support the use of vaginal 9
applications of yoghurt and honey mixes although there have been some reports of benefit with 10
symptom improvement. 109, 110 11
Diet:there is no evidence to support any dietary modifications, including reducing carbohydrate 12
or yeast intake. 92, 108 13
Oral garlic: there is no evidence of benefit from oral garlic on Candida colonization. 111 14
Observational studies have shown that garlic taken orally may cause heartburn, nausea, 15
diarrhoea, flatulence, bloating, and an offensive body odour. 70 16
17
Diabetes Mellitus 18
Symptomatic VVC is more prevalent in diabetic women and most problematic in those with poor 19
glycaemic control. Non-albicans Candida species are more prevalent than in non-diabetic women, in 20
particular C. glabrata. 112-114 21
In diabetic women with symptomatic VVC where C. albicans is isolated single-dose fluconazole 22
(150mg) gives a similar response to non-diabetics. 113(Grade 1C) In diabetic women with 23
symptomatic VVC due to C. glabrata treatment with boric acid 600mg intravaginal suppository once 24
a day for 14 days achieved a higher mycological cure rate at 15 days compared to fluconazole 25
150mgs stat. 115 (Grade 1B) 26
27
Recommendations: 28
Known diabetic women with poor glycaemic control should be encouraged to improve this 29
23
Fluconazole 150mg stat dose for confirmed C. albicans in diabetic women with acute VVC 1
(1C) 2
Boric acid 600mg intravaginal suppository once a day 14 for confirmed C. glabrata in 3
diabetic women with acute VVC (1B) 4
5
HIV Infection 6
VVC occurs more frequently and with greater persistence in HIV-infected women. 116, 117 Increased 7
HIV shedding in the vagina, plasma HIV load above 1000 copies/mL, CD4 lymphocyte count below 8
200 cells/mm3 and the absence of antiretroviral therapy (ART) have been associated with an 9
increased risk of symptomatic VVC. 29, 117 There is no evidence to suggest that HIV-infected women 10
respond less well to conventional methods than HIV-negative women. Treatment for HIV-infected 11
women should be as for HIV-negative women following the recommendations above including the 12
use of suppression therapy as necessary. 118 (Grade 1C) 13
It is important to state that VVC is not a risk factor in the acquisition of HIV. 119 14
15
Recommendation: 16
Treatment regimens for HIV-positive women should be the same as for HIV-negative women 17
(1C) 18
Please refer to www.hiv-druginteractions.org.uk to check for drug interaction between 19
antifungals and antiretrovirals. 20
21
Hormones and Contraception 22
In immunocompetent women there is a strong link between Candida and hormonal status. This is 23
evidenced by Candida species only being found in pubertal/post pubertal and not pre-pubertal 24
females. 120 Also postmenopausal women taking HRT are significantly more prone to develop VVC 25
than women who are not and those with VVC are likely to have been susceptible to it before 26
menopause. 18 27
There is some evidence that combined oral contraceptive (COC) users may have an increased risk of 28
VVC however there are inconsistencies with some studies not finding an association and the quality 29
of the evidence is mixed.119, 121 Women with recurrent or chronic VVC using the COC may wish to 30

24
trial alternative contraception but should be cautioned that the evidence supporting the association 1
between the COC and VVC is weak. (Grade 2C) 2
There is limited evidence for the progestogen-only injection with one systematic review identifying 3
four studies with conflicting results (two found no difference in VVC compared with controls, one 4
found a significant decreased risk and one found a significant increased risk of VVC). 119 There is no 5
available evidence regarding the progestogen-only pill or implant or vaginal rings in relation to VVC. 6
While there is some evidence of higher rates of Candida infection in copper intrauterine device (Cu-7
IUD) and levonorgestrel intrauterine system (LNG-IUS) users, other studies show an increase in 8
Candida present but no difference in symptomatic cases. 122-125 9
10
Recommendations: 11
HRT is associated with an increased risk of VVC 12
Women with recurrent or chronic VVC using the COC may wish to trial alternative 13
contraception but should be cautioned that the evidence supporting the association 14
between the COC and VVC is weak (2C) 15
Cu-IUD/LNG-IUS users with recurrent or chronic VVC may wish to consider an alternative 16
method of contraception* (2C) 17
18
*The Cu-IUD and LNG-IUS are highly effective methods of contraception particularly the Cu-IUD in 19
patients unable to tolerate hormonal methods. Removal of either device should only be considered 20
if a suitably effective alternative can be used. A careful risk-benefit assessment should be made 21
taking into consideration that keeping the Cu-IUD or LNG-IUS and controlling the recurrent VVC 22
symptoms may be a more appropriate option for some patients. 23
24
Reactions to Treatment 25
The most common treatment-related adverse events reported in the patients who received 150 26
mg single dose fluconazole for VVC were headache, nausea, and abdominal pain. 27
anaphylaxis has been reported rarely with fluconazole and itraconazole 28
there is a low risk of idiosyncratic drug-induced hepatitis with oral azoles; fluconazole is less 29
frequently associated with hepatotoxicity than itraconazole 30

25
oral azoles also prolong the QT time and caution should be taken if prescribed in combination 1
with other similar drugs 2
topical azole therapies and other topical agents can cause vulvovaginal irritation and this should 3
be considered if symptoms worsen or persist. 4
5
6
FOLLOW-UP 7
Follow-up and test of cure for patients with acute VVC is unnecessary if symptoms resolve. 8
Patients with recurrent or chronic VVC should be advised to return if they experience poor or 9
partial response to therapy; repeat microscopy and culture is indicated to assess for 10
microbiological cure or new resistance 11
Patients that demonstrate microbiological response but not clinical response to therapy should 12
be reassessed for alternative causes of their symptoms 13
On completion of suppressive therapy patients should be advised about the management of 14
future acute episodes (as per acute VVC) and when to return for review (e.g. if frequency of 15
recurrence >4 episodes per year or acute symptoms don’t settle with treatment). 16
17
18
CONTACT TRACING & TREATMENT 19
There is no evidence to support the treatment of asymptomatic male sexual partners in any of 20
acute, recurrent or chronic VVC. 126-129 (Grade 1A) 21
22
23
CONSIDERATION OF RESOURCE IMPLICATIONS 24
It is acknowledged that some tests, e.g. for the precise speciation of Candida, may not be able in 25
all settings 26
Some treatment preparations, e.g. flucytosine cream, may not be available on local formularies. 27
It is advised that such preparations are discussed with the unit pharmacist prior to prescribing. 28

26
QUALIFYING STATEMENT 1
The recommendations in this guideline may not be appropriate for use in all clinical situations. 2
Decisions to follow these recommendations must be based on the professional judgement of the 3
clinician and consideration of individual patient circumstances and available resources. 4
All possible care has been taken to ensure the publication of the correct dosage of medication and 5
route of administration. However, it remains the responsibility of the prescribing physician to ensure 6
the accuracy and appropriateness of the medication they prescribe. 7
8
9
AUDITABLE OUTCOMES 10
Fluconazole used first line for acute VVC in non-pregnant women and women with no evidence 11
of pregnancy risk. Target 97%. 12
All women with recurrent or chronic VVC to be offered a genital examination performed by an 13
appropriately trained clinician. Target 97% 14
All women with suspected recurrent or chronic VVC should have microscopy and/or culture with 15
full speciation and sensitivity testing for at least 2 (of the ≥4 per year) episodes (including at 16
least one culture). Target 97%. 17
Documentation of a discussion around the offer of suppressive or alternative long term therapy 18
for all women with proven recurrent and chronic VVC. Target 97% 19
Documentation of a discussion about what constitutes good vulval skin care for all women with 20
recurrent or chronic VVC. Target 97% 21
22
23
RECOMMENDATIONS FOR FUTURE RESEARCH 24
Further assessment of sensitivity and specificity of molecular and rapid antigen detection point 25
of care diagnostic tests and the value of their use in a service providing level 3 STI care 26
Appropriate regimen and duration of therapy for women that have a recurrence of symptoms 27
after completing 6 months of treatment for recurrent or chronic VVC 28

27
Further assessment of the benefit of treating asymptomatic colonization with Candida in 1
pregnancy on pregnancy outcome 2
3
4
ACKNOWLEDGEMENTS 5
Stephen Woods (Deputy Library Manager, Academy Library, Wythenshawe Hospital, Manchester 6
University Hospitals NHS Foundation Trust, Manchester, UK) for performing the literature searches 7
and obtaining full text articles for review. 8
Two patient representatives from clinics of the writing group reviewed the first draft of the 9
guideline. They provided feedback from their perspective as a patient, in particular looking at: 10
treatment preferences 11
ensuring the guideline covers all issues important to patients 12
the language of the guideline is appropriately respectful to patients (acknowledging the 13
intended audience is healthcare professionals). 14
15
16
REFERENCES 17
1. Holland J, Young ML, Lee O, et al. Vulvovaginal carriage of yeasts other than Candida albicans. 18
Sex Transm Infect 2003;79(3):249-250. 19
2. Wang FJ, Zhang D, Liu ZH et al. Species Distribution and In Vitro Antifungal Susceptibility of 20
Vulvovaginal Candida Isolates in China. Chin Med J (Engl) 2016;129(10):1161-5. 21
3. Guerrero-Lozano I, Aznar-Marin P, Garcia-Agudo, L, et al. 4. Vulvovaginal candidosis by non-22
albicans Candida species. Mycoses 2012;55(Suppl4):95–338. 23
4. Bulik CC, Sobel JD, Nailor MD. Susceptibility profile of vaginal isolates of Candida albicans prior 24
to and following fluconazole introduction - impact of two decades. Mycoses 2011;54(1):34-8. 25
5. Hetticarachchi N, Ashbee HR, Wilson JD. Prevalence and management of non-albicans vaginal 26
candidiasis. Sex Transm Infect 2010;86(20):99-100. 27
6. Dennerstein GJ, Ellis DH, Reed CS et al. Pathogenicity of non-albicans yeasts in the vagina. J Low 28
Genit Tract Dis 2011;15(1):33-6. 29

28
7. Zeng J, Zong LL, Mao T, et al. Distribution of Candida albican genotype and Candida species is 1
associated with the severity of vulvovagianl candidiasis. Nan Fang Yi Ke Da Xue Xue Bao 2
2011;31(10):1649-53. 3
8. Hurley R, De Louvois J. Candida vaginitis. Postgrad Med J 1979;55:645–47 4
9. Nyirjesy P. Chronic vulvovaginal candidiasis. Am Fam Physician 2001;63(4):697-702. 5
10. Hurley R. Recurrent Candida infection. Clin Obstet Gynaecol 1981;8(1):209-14. 6
11. Foxman B, Muraglia R, Dietz JP, et al. Prevalence of recurrent vulvovaginal candidiasis in 5 7
European countries and the United States: Results from an internet panel survey. J Low Genit 8
Tract Dis 2013;17(3):340-5. 9
12. Fidel PL, Jr., Sobel JD. Immunopathogenesis of recurrent vulvovaginal candidiasis. Clin Microbiol 10
Rev 1996;9(3):335-48 11
13. El-Din SS, Reynolds MT, Ashbee HR, Barton RC, Evans EG. An investigation into the pathogenesis 12
of vulvo- vaginal candidosis. Sex Transm Infect 2001;77(3):179-183. 13
14. Patel D, Gillespie B, Sobel J, et al. Risk factors for recurrent vulvovaginal candidiasis in women 14
receiving maintenance antifungal therapy: results of a prospective cohort study. Am J Obstet 15
Gynecol 2004;190(3):644-653. 16
15. Bauters T, Dhont M, Temmerman M, I, Nelis H. Prevalence of vulvovaginal candidiasis and 17
susceptibility to fluconazole in women. Am J Obstet Gynecol 2002;187(3):569-574. 18
16. Ahmad A, Khan AU. Prevalence of Candida species and potential risk factors for vulvovaginal 19
candidiasis in Aligarh, India. Eur J Obstet Gynecol Reprod Biol 2009;144(1):68-71. 20
17. Donders GG, Mertens I, Bellen G, et al. Self-elimination of risk factors for recurrent vaginal 21
candidosis. Mycoses 2011;54(1):39-45. 22
18. Fischer G, Bradford J. Vulvovaginal candidiasis in postmenopausal women: the role of hormone 23
replacement therapy. J Low Genit Tract Dis 2011;15(4):263-7. 24
19. Pirotta MV, Garland SM. Genital Candida species detected in samples from women in 25
Melbourne, Australia, before and after treatment with antibiotics. J Clin Microbiol 26
2006;44(9):3213-7. 27
20. Oliveira CS, Gandra R, Loth EA, et al. Clinical, Epidemiological and laboratory findings amoung 28
women with recurrent vulvovaginal candidiasis (RVVC) in an university hospital, Brazil. Mycoses 29
2015;58(Suppl3):68(P038). 30
21. Moraes PS. Recurrent vaginal candidiasis and allergic rhinitis: a common association. Ann Allergy 31
22. Ehrstrom S, Kornfeld D, Rylander E. Perceived stress in women with recurrent vulvovaginal 32
candidiasis. J Psychosom Obstet Gynaecol 2007;28(3):169-76. 33

29
23. Spacek J, Jilek P, Buchta V, at al. The serum levels of calcium, magnesium, iron and zinc in 1
patients with recurrent vulvovaginal candidosis during attack, remission and in healthy controls. 2
Mycoses 2005;48(6):391-395. 3
24. Naderi N, Etaati Z, Rezvani Joibari M, et al. Immune deviation in recurrent vulvovaginal 4
candidiasis: Correlation with Iron Deficiency Anemia. Iran J Immunol 2013;10(2):118-26 5
25. Bohler K, Meisinger V, Klade H, et al. Zinc levels of serum and cervicovaginal secretion in 6
recurrent vulvovaginal candidiasis. Genitourin-Med 1994;70(5):308-310. 7
26. Henić E, Thiel S, Mårdh PA. Mannan-binding lectin in women with a history of recurrent 8
vulvovaginal candidiasis. Eur J Obstet Gynecol Reprod Biol 2010;148(2):163-5. 9
27. Donders GG, Babula O, Bellen G, et al. Mannose-binding lectin gene polymorphism and 10
resistance to therapy in women with recurrent vulvovaginal candidiasis. BJOG 11
2008;115(10):1225-31. 12
28. Nedovic B, Posteraro B, Leoncini E, et al. Mannose-binding lectin codon 54 gene polymorphism 13
and vulvovaginal candidiasis: a systematic review and meta-analysis. Biomed Res Int 14
2014:738298-99. 15
29. Apalata T, Longo-Mbenza B, Sturm A, et al. Factors Associated with Symptomatic Vulvovaginal 16
Candidiasis: A Study among Women Attending a Primary Healthcare Clinic in Kwazulu-Natal, 17
South Africa. Ann Med Health Sci Res 2014;4(3):410-6. 18
30. Narayankhedkar A, Hodiwala A, Mane A.Clinicoetiological Characterization of Infectious Vaginitis 19
amongst Women of Reproductive Age Group from Navi Mumbai, India. J Sex Transm Dis 20
2015:817092. 21
31. Beikert FC, Le MT, Koeninger A, et al. Recurrent vulvovaginal candidosis: focus on the vulva. 22
Mycoses 2011;54(6):e807-10. 23
32. Zhu YX, Li T, Fan SR, et al. Health-related quality of life as measured with the Short-Form 36 (SF-24
36) questionnaire in patients with recurrent vulvovaginal candidiasis. Health Qual Life Outcomes 25
2016;14:65. 26
33. Hong E, Dixit S, Fidel PL, et al. Vulvovaginal candidiasis as a chronic disease: diagnostic criteria 27
and definition. J Low Genit Tract Dis 2014;18(1):31-8. 28
34. Spacek J, Buchta V, Jílek P, et al. Clinical aspects and luteal phase assessment in patients with 29
recurrent vulvovaginal candidiasis. Eur J Obstet Gynecol Reprod Biol 2007;131(2):198-202. 30
35. Schaaf VM, Perez-Stable EJ, Borchardt K. The limited value of symptoms and signs in the 31
diagnosis of vaginal infections. Arch Intern Med 1990;150(9):1929-1933. 32
36. Geiger AM, Foxman B, Sobel JD. Chronic vulvovaginal candidiasis: characteristics of women with 33
Candida albicans, C glabrata and no candida. Genitourin-Med 1995;71(5):304-307. 34

30
37. Ferris DG, Dekle C, Litaker MS. Women's use of over-the-counter antifungal medications for 1
gynecologic symptoms. J Fam Pract 1996;42(6):595-600. 2
38. Lindner JG, Plantema FH, Hoogkamp K. Quantitative studies of the vaginal flora of healthy 3
women and of obstetric and gynaecological patients. J Med Microbiol 1978; 11(3):233-24. 4
39. Odds FC. Candida and Candidosis; A review and bibliography. Second ed. London: Bailliere 5
Tindall; 1988. 6
40. Abbott J. Clinical and microscopic diagnosis of vaginal yeast infection: a prospective analysis. Ann 7
Emerg Med 1995; 25(5):587-591. 8
41. Bergman JJ, Berg AO, Schneeweiss R, et al. Clinical comparison of microscopic and culture 9
techniques in the diagnosis of Candida vaginitis. J Fam Pract 1984; 18(4):549-552. 10
42. Eckert LO, Hawes SE, Stevens CE, et al. Vulvovaginal candidiasis: clinical manifestations, risk 11
factors, management algorithm. Obstet Gynecol 1998; 92(5):757-765. 12
43. Sonnex C, Lefort W. Microscopic features of vaginal candidiasis and their relation to 13
symptomatology. Sex Transm Infect 1999; 75(6):417-419. 14
44. Zdolsek B, Hellberg D, Froman G, et al. Culture and wet smear microscopy in the diagnosis of 15
low-symptomatic vulvovaginal candidosis. Eur J Obstet Gynecol Reprod Biol 1995;58(1):47-51. 16
45. Liu XP, Fan SR. Methylrosaniline chloride stained vaginal smears for the diagnosis of vulvovaginal 17
candidiasis. Int J Gynaecol Obstet 2007;99(2):83-6. 18
46. Hopwood V, Crowley T, Horrocks CT, et al. Vaginal candidosis: relation between yeast counts 19
and symptoms and clinical signs in non-pregnant women. Genitourin-Med 1988;64(5):331-334. 20
47. Odds FC, Webster CE, Riley VC, et al. Epidemiology of vaginal Candida infection: significance of 21
numbers of vaginal yeasts and their biotypes. Eur J Obstet Gynecol Reprod Biol 1987;25(1):53-66. 22
48. Odds FC, Webster CE, Mayuranathan P, et al. Candida concentrations in the vagina and their 23
association with signs and symptoms of vaginal candidosis. J Med Vet Mycol 1988; 26(5):277-24
283. 25
49. Priestley CJ, Jones BM, Dhar J, Goodwin L. What is normal vaginal flora? Genitourin-Med 26
1997;73(1):23-28. 27
50. Singh RH, Erbelding EJ, Zenilman JM, et al. The role of the speculum and bimanual examinations 28
when evaluating attendees at a sexually transmitted diseases clinic. Sex Transm Infect 2007 29
83:206-1. 30
51. Faculty of Sexual and Reproductive Health (FSRH) / British Association for Sexual Health and HIV 31
(BASHH). Management of Vaginal Discharge in Non-Genito Urinary Medicine Settings. Available 32
at: www.bashh.org/documents/4264.pdf. (accessed: 01/03/2018) 33

31
52. Emmerson J, Gunputrao A, Hawkswell J, Dexter A, Sykes R, Searle S et al. Sampling for vaginal 1
candidosis: how good is it? Int J STD AIDS 1994;5(5):356-358. 2
53. Barnes P, Vieira R, Chauhan M O020 Pilot study comparing self-collected vaginal swab with 3
clinician taken vaginal swab for the detection of candida and bacterial vaginosis. Sex Transm 4
Infect 2016;92:A8. 5
54. Engberts MK, Boon ME, van Haaften M, et al. Symptomatic candidiasis: Using self sampled 6
vaginal smears to establish the presence of Candida, lactobacilli, and Gardnerella vaginalis. 7
Diagn Cytopathol 2007;35(10):635-9. 8
55. Vergers-Spooren HC1, van der Meijden WI, Luijendijk A, et al. Self-sampling in the diagnosis of 9
recurrent vulvovaginal candidosis. J Low Genit Tract Dis 2013;17(2):187-92. 10
56. Danby CS, Boikov D, Rautemaa-Richardson R, et al. Effect of pH on in vitro susceptibility of 11
Candida glabrata and Candida albicans to 11 antifungal agents and implications for clinical use. 12
Antimicrob Agents Chemother 2012;56(3):1403-6. 13
57. Cartwright CP, Lembke BD, Ramachandran K, et al. Comparison of nucleic acid amplification 14
assays with BD affirm VPIII for diagnosis of vaginitis in symptomatic women. J Clin Microbiol 15
2013;51(11):3694-9. 16
58. Chatwani AJ, Mehta R, Hassan S, et al. Rapid testing for vaginal yeast detection: a prospective 17
study. Am J Obstet Gynecol 2007;196(4):309. 18
59. Dan M, Leshem Y, Yeshaya A, et al. Performance of a rapid yeast test in detecting Candida spp. in 19
the vagina. Diagn Microbiol Infect Dis 2010;67(1):52-5. 20
60. Elegbe IA, Elegbe I. Quantitative relationships of Candida albicans infections and dressing 21
patterns in Nigerian women. Am J Public Health 1983;73(4):450-452. 22
61. Ekpenyong CE, Inyang-etoh EC, Ettebong EO, et al. Recurrent vulvovaginal candidosis among 23
young women in south eastern Nigeria: The role of lifestyle and health-care practices. Int J STD 24
AIDS 2012;23(10):704-9. 25
62. Pontes AC, Amaral RL, Giraldo PC, et al. A systematic review of the effect of daily panty liner use 26
on the vulvovaginal environment. Int J Gynaecol Obstet 2014;127(1):1-5. 27
63. Giraldo PC, Amaral RL, Juliato C, et al. The effect of "breathable" panty liners on the female 28
lower genital tract. Int J Gynaecol Obstet 2011;115(1):61-4 29
64. Janković S, Bojović D, Vukadinović D, et al. Risk factors for recurrent vulvovaginal candidiasis. 30
Vojnosanit Pregl 2010;67(10):819-24. 31
65. Shaaban OM, Abbas AM, Moharram AM, et al. Does vaginal douching affect the type of candidal 32
vulvovaginal infection? Med Mycol 2015;53(8):817-27. 33

32
66. Heng LS, Yatsuya H, Morita S, et al. Vaginal douching in Cambodian women: its prevalence and 1
association with vaginal candidiasis. J Epidemiol 2010;20(1):70-6. 2
67. Watson C, Fairley C, Garland S, et al. The effect of sexual intercourse on vaginal colonisation with 3
candida. Sex Transm Infect 2015;91:A119-A120 (P06.14). 4
68. Watson MC, Grimshaw JM, Bond CM, et al. Oral versus intra-vaginal imidazole and triazole anti-5
fungal treatment of uncomplicated vulvovaginal candidiasis (thrush): a systematic review. Int J 6
Gynaecol Obstet 2002; 109(1):85-95. 7
69. Nurbhai M, Grimshaw J, Watson M, et al. Oral versus intra-vaginal imidazole and triazole anti-8
fungal treatment of uncomplicated vulvovaginal candidiasis (thrush). Cochrane Database Syst 9
Rev 2007;4: CD002845. 10
70. Lopez M, Ester J. Candidiasis (vulvovaginal). BMJ Clin Evid 2015:0815. 11
71. Pitsouni E, Iavazzo C, Falagas ME. Itraconazole vs fluconazole for the treatment of 12
uncomplicated acute vaginal and vulvovaginal candidiasis in nonpregnant women: a 13
metaanalysis of randomized controlled trials. Am J Obstet Gynecol 2008;198(2):153-60. 14
72. Sekhavat L, Tabatabaii A, Tezerjani FZ. Oral fluconazole 150 mg single dose versus intra-vaginal 15
clotrimazole treatment of acute vulvovaginal candidiasis. J Infect Public Health 2011;4(4):195-9. 16
73. Dressen G, Kusche W, Neumeister C, et al. Diagnosis of vulvovaginal Candidiasis and 17
effectiveness of combined topical treatment with nystatin: Results of a non-interventional study 18
in 973 patients. Open Womens Health J 2012;6:19-23. 19
74. Khameneie KM, Arianpour N, Roozegar R, et al. Fluconazole and Boric Acid for Treatment of 20
Vaginal Candidiasis--New Words About Old Issue. East Afr Med J 2013;90(4):117-23. 21
75. Rosa MI, Silva BR, Pires PS, et al. Weekly fluconazole therapy for recurrent vulvovaginal 22
candidiasis: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol 23
2013;167(2):132-6. 24
76. Neves NA, Carvalho LP, Lopes AC, et al. Successful treatment of refractory recurrent vaginal 25
candidiasis with cetirizine plus fluconazole. J Low Genit Tract Dis 2005;9(3):167-70. 26
77. Donders G, Bellen G, Byttebier G, et al. Individualized decreasing-dose maintenance fluconazole 27
regimen for recurrent vulvovaginal candidiasis (ReCiDiF trial). Am J Obstet Gynecol 28
2008;199(6):613. 29
78. Nguyen Y, Lee A, Fischer G. Management of chronic vulvovaginal candidiasis: A long term 30
retrospective study. Australas J Dermatol 2017;58(4):e188-e192 31
79. Sobel J, Chaim W, Nagappan V, et al. Treatment of vaginitis caused by Candida glabrata: use of 32
topical boric acid and flucytosine. Am J Obstet Gynecol 2003;189(5):1297-1300. 33
33
80. Singh S, Sobel J, Bhargava P, et al. Vaginitis due to Candida krusei: epidemiology, clinical aspects, 1
and therapy. Clin Infect Dis 2002;35(9):1066-70. 2
81. Phillips A. Treatment of non-albicans Candida vaginitis with amphotericin B vaginal 3
suppositories. Am J Obstet Gynecol 2005;192(6):2009-2012. 4
82. Iavazzo C, Gkegkes ID, Zarkada IM, et al. Boric Acid for Recurrent Vulvovaginal Candidiasis: The 5
Clinical Evidence. J Womens Health (Larchmt) 2011;20(8):1245-55. 6
83. Guaschino S, De Seta F, Sartore A, et al. Efficacy of maintenance therapy with topical boric acid 7
in comparison with oral itraconazole in the treatment of recurrent vulvovaginal candidiasis. Am J 8
Obstet Gynecol 2001;184(4):598-602. 9
84. Acs N, Bunhidy F, Puh E, et al. Teratogenic effects of vaginal boric acid treatment during 10
pregnancy. Int J Gynaecol Obstet 2006;93(1):55-6. 11
85. White DJ, Habib AR, Vanthuyne A, et al. Combined topical flucytosine and amphotericin B for 12
refractory vaginal Candida glabrata infections. Sex Transm Infect 2001;77(3):212-213. 13
86. Fan S, Liu X, Wu C, et al. Vaginal nystatin versus oral fluconazole for the treatment for recurrent 14
vulvovaginal candidiasis. Mycopathologia 2015;179(1-2):95-101. 15
87. Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 16
2015. (http://www.cdc.gov/std/tg2015/default.htm) 17
88. Sobel JD, Kapernick PS, Zervos M, et al. Treatment of complicated Candida vaginitis: comparison 18
of single and sequential doses of fluconazole. Am J Obstet Gynecol 2001;185(2):363-369. 19
89. Sobel JD, Brooker D, Stein GE, et al. Single oral dose fluconazole compared with conventional 20
clotrimazole topical therapy of Candida vaginitis. Fluconazole Vaginitis Study Group. Am J Obstet 21
Gynecol 1995;72(4 Pt 1):1263-1268. 22
90. Fan S, Liu X, Liang Y. Miconazole nitrate vaginal suppository 1,200 mg versus oral fluconazole 23
150 mg in treating severe vulvovaginal candidiasis. Gynecol Obstet Invest 2015;80(2):113-8. 24
91. Zhou X, Li T, Fan S, et al. The efficacy and safety of clotrimazole vaginal tablet vs. oral fluconazole 25
in treating severe vulvovaginal candidiasis. Mycoses 2016;59(7):419-28. 26
92. Sobel JD, Faro S, Force RW, et al. Vulvovaginal candidiasis: epidemiologic, diagnostic, and 27
therapeutic considerations. Am J Obstet Gynecol 1998;178(2):203-211. 28
93. Young GL, Jewell D. Topical treatment for vaginal candidiasis (thrush) in pregnancy. Cochrane 29
Database Syst Rev. 2001;(4):CD000225. 30
94. Alsaad AM, Kaplan YC, Koren G. Exposure to fluconazole and risk of congenital malformations in 31
the offspring: A systematic review and meta-analysis. Reprod Toxicol 2015;52:78-82. 32
95. Howley MM, Carter TC, Browne ML, et al. Fluconazole use and birth defects in the National Birth 33
Defects Prevention Study. Am J Obstet Gynecol 2016;214(5):657. 34

34
96. Mølgaard-Nielsen D, Svanström H, Melbye M, et al. Association Between Use of Oral Fluconazole 1
During Pregnancy and Risk of Spontaneous Abortion and Stillbirth. JAMA 2016;315(1):58-67. 2
97. Farr A, Kiss H, Holzer I, et al. Effect of asymptomatic vaginal colonization with Candida albicans 3
on pregnancy outcome. Acta Obstet Gynecol Scand 2015;94(9):989-96. 4
98. Banhidy F, Dudas I, Czeize AE. Preconceptional screening of sexually transmitted 5
infections/diseases. Cent Eur J Med 2010;6(1):49-57. 6
99. Roberts CL, Algert CS, Rickard KL, et al. Treatment of vaginal candidiasis for the prevention of 7
preterm birth: a systematic review and meta-analysis. Syst Rev 2015;21;4:31. 8
100. White DJ, Vanthuyne A, Wood PM, et al. Zafirlukast for severe recurrent vulvovaginal 9
candidiasis: an open label pilot study. Sex Transm infect 2004;80(3). 10
101. Kovachev SM, Vatcheva-Dobrevska RS. Local Probiotic Therapy for Vaginal Candida albicans 11
Infections. Probiotics Antimicrob Proteins 2015;7(1):38-44. 12
102. Palacios S, Espadaler J, Fernández-Moya JM, et al. Is it possible to prevent recurrent 13
vulvovaginitis? The role of Lactobacillus plantarum I1001 (CECT7504). Eur J Clin Microbiol Infect 14
Dis 2016;35(10):1701–1708. 15
103. Hanson L, VandeVusse L, Jermé M, et al. Probiotics for Treatment and Prevention of 16
Urogenital Infections in Women: A Systematic Review. J Midwifery Womens Health 17
2016;61(3):339-55. 18
104. Abad CL, Safdar N. The role of Lactobacillus probiotics in the treatment or prevention of 19
urogenital infections - A systematic review. J Chemother 2009;21(3):243-52. 20
105. Kalliomaki M, Salminen S, Arvilommi H, et al. Probiotics in primary prevention of atopic 21
disease: a randomised placebo-controlled trial. Lancet 2001;357(9262):1076-1079. 22
106. Hammer KA, Carson CF, Riley TV. In-vitro activity of essential oils, in particular Melaleuca 23
alternifolia (tea tree) oil and tea tree oil products, against Candida spp. J Antimicrob Chemother 24
1998;42(5):591-595. 25
107. D'Antuono A, Baldi E, Bellavista S, et al. Use of Dermasilk briefs in recurrent vulvovaginal 26
candidosis: safety and effectiveness. Mycoses 2012;55(3):e85-9. 27
108. Mardh PA, Rodrigues AG, Genc M, et al. Facts and myths on recurrent vulvovaginal 28
candidosis--a review on epidemiology, clinical manifestations, diagnosis, pathogenesis and 29
therapy. Int J STD AIDS 2002; 3(8):522-539. 30
109. Abdelmonem AM, Rasheed SM, Mohamed AS. Bee-honey and yogurt: a novel mixture for 31
treating patients with vulvovaginal candidiasis during pregnancy. Arch Gynecol Obstet 32
2012;286(1):109-14. 33
35
110. Darvishi M, Jahdi F, Hamzegardeshi Z, et al. The Comparison of vaginal cream of mixing 1
yogurt, honey and clotrimazole on symptoms of vaginal candidiasis. Glob J Health Sci 2
2015;7(6):108-16. 3
111. Watson CJ, Grando D, Fairley CK, et al. The effects of oral garlic on vaginal candida colony 4
counts: a randomised placebo controlled double-blind trial. BJOG 2014;121(4):498-506. 5
112. Bohannon NJ. Treatment of vulvovaginal candidiasis in patients with diabetes. Diabetes care 6
1998;21(3):451-456. 7
113. Goswami D, Goswami R, Banerjee U, et al. Pattern of Candida species isolated from patients 8
with diabetes mellitus and vulvovaginal candidiasis and their response to single dose oral 9
fluconazole therapy. J infect 2006;52(2):111-7. 10
114. Akimoto-Gunther L, Bonfim-Mendonca PS, Godoy JSR, et al. Hyperglycemia and increased 11
risk of vulvovaginal candidiasis (VVC). Mycoses 2015;58(Suppl4):168 (P316). 12
115. Ray D, Goswami R, Banerjee U, et al. Prevalence of Candida glabrata and Its Response to 13
Boric Acid Vaginal Suppositories in Comparison With Oral Fluconazole in Patients With Diabetes 14
and Vulvovaginal Candidiasis. Diabetes care 2007;30(2). 15
116. Duerr A, Heilig CM, Meikle SF, et al. Incident and persistent vulvovaginal candidiasis among 16
human immunodeficiency virus-infected women: Risk factors and severity. Obstet Gynecol 17
2003;101(3). 18
117. Apalata T, Carr WH, Sturm WA, et al. Determinants of symptomatic vulvovaginal candidiasis 19
among human immunodeficiency virus type 1 infected women in rural KwaZulu-Natal, South 20
Africa. Infect Dis Obstet Gynecol 2014;387070. 21
118. Sobel J. Vulvovaginal candidiasis: a comparison of HIV-positive and -negative women. Int J 22
STD AIDS 2002;13(6):358-362. 23
119. van de Wijgert JH, Verwijs MC, Turner AN, et al. Hormonal contraception decreases bacterial 24
vaginosis but oral contraception may increase candidiasis: implications for HIV transmission. 25
AIDS. 2013;27(13):2141-53. 26
120. Baka S, Tsouma I, Logothetis E, et al. Pathogens implicated in cases of vulvovaginitis in 27
prepubertal and pubertal girls. Clin Microbiol Infect 2012;18:233-234(P1009). 28
121. Spinillo A, Pizzoli G, Colonna L, et al. Epidemiologic characteristics of women with idiopathic 29
recurrent vulvovaginal candidiasis. Obstet Gynecol 1993; 81(5)(Pt 1):721-727. 30
122. Donders GG, Berger J, Heuninckx H, et al. Vaginal flora changes on Pap smears after 31
insertion of intrauterine levonorgestrel releasing device (Mirena). Contraception 2011;83(4):352-32
6 33

36
123. Güdücü N, Gönenç G, Işçi H, et al. Clinical importance of detection of bacterial vaginosis, 1
trichomonas vaginalis, candida albicans and actinomyces in Papanicolaou smears. Clin Exp 2
Obstet Gynecol 2012;39(3):333-6. 3
124. Behboudi-Gandevani S, Imani S, Moghaddam-Banaem L, et al. Can intrauterine 4
contraceptive devices lead to VulvoVaginal Candidiasis (VVC) and Anemia in Iranian new users? 5
Sex Reprod Healthc 2015;6(1):40-3. 6
125. Guzel AB, Ilkit M, Akar T, et al. Evaluation of risk factors in patients with vulvovaginal 7
candidiasis and the value of chromID Candida agar versus CHROMagar Candida for recovery and 8
presumptive identification of vaginal yeast species. Med Mycol 2011; 49: 16–25. 9
126. Bisschop MP, Merkus JM, Scheygrond H, et al. Co-treatment of the male partner in vaginal 10
candidosis: a double-blind randomized control study. BJOG 1986;93(1):79-81. 11
127. Fong IW. The value of treating the sexual partners of women with recurrent vaginal 12
candidiasis with ketoconazole. Genitourin-Med 1992;68(3):174-176. 13
128. Lisboa C, Costa AR, Ricardo E, et al. Genital candidosis in heterosexual couples. J Eur Acad 14
Dermatol Venereol 2011;25(2):145-51. 15
129. Spence, D. Candidiasis (Vulvovaginal). BMJ Clin Evid 2010 5;2010. 16
17
18
EDITORIAL INDEPENDENCE 19
This guideline was commissioned, edited and endorsed by the BASHH CEG. 20
21
22
CONFLICTS OF INTEREST 23
All members of the guideline writing committee completed the BASHH conflict of interest 24
declaration at the time the guideline’s final draft was submitted to the CEG. 25
26
27
WRITING GROUP AFFILIATIONS 28
Cara Saxon (Lead Author): Consultant Physician in Genitourinary Medicine, Withington Clinic, 29
Manchester University Hospitals NHS Foundation Trust, Manchester, UK 30

37
Anne Edwards: Consultant Physician in Genitourinary Medicine, Oxford University Hospitals NHS 1
Foundation Trust, Oxford, UK 2
Riina Rautemaa-Richardson: Consultant in Medical Mycology, Wythenshawe Hospital, Manchester 3
University Hospitals NHS Foundation Trust, Manchester, UK 4
Caroline Owen: Consultant Physician in Dermatology, East Lancashire Hospitals NHS Trust, 5
Blackburn, UK 6
Bavithra Nathan: Consultant Physician in Genitourinary Medicine, Kingston Hospital NHS Foundation 7
Trust, Kingston-upon-Thames, UK 8
Bret Palmer: Specialty Trainee in Genitourinary Medicine, Oxford Deanery, UK 9
Clare Wood: Specialty Trainee in Genitourinary Medicine, North Western Deanery, UK 10
Humera Ahmed: Pharmacist, Manchester, UK 11
Sameena Ahmad: Consultant Physician in Genitourinary Medicine, Withington Clinic, Manchester 12
University Hospitals NHS Foundation Trust, Manchester, UK 13
Patient Representatives (see acknowledgments) 14
Mark FitzGerald: Clinical Effectiveness Group Editor 15
16
17
MEMBERSHIP OF THE CLINICAL EFFECTIVENESS GROUP 18
Dr Keith Radcliffe (Chair) 19
Dr Mark FitzGerald 20
Dr Deepa Grover 21
Dr Steve Higgins 22
Dr Margaret Kingston 23
Dr Michael Rayment 24
Dr Darren Cousins 25
Dr Ann Sullivan 26
Dr Helen Fifer 27
Dr Craig Tipple 28

38
Dr Sarah Flew 1
Dr Cara Saxon 2

39
Table 1. Clinical Features of Vulvovaginal Candidiasis and Common Differential Diagnoses – Symptoms* 1
Vulvovaginal Candidiasis Lichen Sclerosus Vulvo- / vestibulodynia
Contact Dermatitis/Eczema
Chronic Lichen Simplex/Chronic Eczema
Vulval Itch Yes Yes, severe No Yes Yes
Vulval soreness Yes – but not always; ‘prickling’
Yes, severe Burning is predominant symptom
Yes Possible
Discharge Yes - odourless, typically ‘curdy’ but may be thin or absent (absence doesn’t exclude diagnosis)
No+ No+ Possible, but this is exudate from inflamed skin, not a true discharge
No+
Superficial Dyspareunia
Possible Yes (especially if loss of vulval architecture)
Yes – point penetration pain
Possible Possible
Superficial dysuria
Possible Possible Not usually Possible Not usually
Swelling Possible No No Possible Possible (secondary to lichenification – thickening of skin from chronic scratching)
Response to topical steroid
Improvement/no change/worse
Improvement but requires high potency
No Improvement Improvement
* the symptoms and signs listed in this table are not pathognomic of the conditions but an indication of a ‘typical clinical presentation’ and to highlight the potential 2 differences and similarities between each of these conditions, further information about the alternative conditions listed can be found at www.bad.org.uk “ 3 + unless dual pathology 4
5

40
Table 2. Clinical Features of Vulvovaginal Candidiasis and Common Differential Diagnoses – Signs* 1 2
VV Candidiasis Lichen Sclerosus Vulvodynia Contact Dermatitis Chronic Lichen Simplex
Erythema Yes Yes but usually in conjunction with other features
Possible Yes Possible
Fissuring Possible Possible No Possible Possible
Discharge Yes - odourless, typically ‘curdy’ but may be thin or absent (absence doesn’t exclude diagnosis)
No+ No+ Possible, but this is exudate from inflamed skin, not a true discharge
No+
Oedema Possible No No Possible Possible
Other features Satellite lesions Pallor, atrophy, loss of vulval architecture, areas of haemorrhage, introital narrowing
Cotton tip provoked tenderness
Erythema, exudate Lichenification, (thickening of affected skin caused by long term scratching)
Excoriations (scratch marks)
Possible Possible No Often Often
* the symptoms and signs listed in this table are not pathognomic of the conditions but an indication of a ‘typical clinical presentation’ and to highlight the potential 3 differences and similarities between each of these conditions, further information about the alternative conditions listed can be found at www.bad.org.uk “ 4 + unless dual pathology 5
6

41
Table 3. Vulvovaginal candidiasis treatment options 1
Preferred Alternative
Acute VVC
Non-pregnant women
Fluconazole 150mg PO stat (1B) If oral therapy is contraindicated: Clotrimazole 500mg PV stat (1B)
Clotrimazole vaginal cream (10%) 5g stat** (1B)
Clotrimazole pessary 200mg nocte for 3 days or 100mg nocte for 6 days**
(1C)
Econazole pessary 150mg stat or 150mg nocte for 3 days** (1B)
Fenticonazole pessary 600mg stat or 200mg nocte for 3 nights** (1B)
Itraconazole 200mg bd for 1 day PO* (1B)
Miconazole pessary 100mg nocte for 14 nights** (1B)
Pregnancy Clotrimazole pessary 500mg PV nocte for 7
days (1B)
Clotrimazole vaginal cream (10%) 5g nocte for 7 days** (1C)
Clotrimazole pessary 200mg or 100mg nocte for 7 days** (1C)
Econazole pessary 150mg nocte for 7 days** (1C)
Fenticonazole pessary 600mg stat or 200mg nocte for 7 days** (1C)
Miconazole pessary 100mg nocte for 14 nights** (1C)
NAC sp & azole
resistance
Nystatin pessaries 100,000units nocte for
14 days (1B)
Boric acid suppositories 600mg daily for 14 days* (1B)
Amphotericin B vaginal suppositories 50mg once a day for 14 days (2C)
Flucytosine 5g cream or 1g pessary +/- amphotericin daily for 14 days (2C)
Recurrent or Chronic VVC
Non-pregnant women
Induction: fluconazole 150mg every 72 hours x 3 doses* (1A) Maintenance: fluconazole 150mg once a week for 6 months* (1A)
Induction: topical imidazole therapy can be increased to 10-14 days according
to symptomatic response(Grade 2C) Maintenance for 6 months: Clotrimazole pessary 500mg once a week (1B) or Itraconazole 50-100mg daily*(2C)
Pregnancy Induction: topical imidazole therapy can be increased to 10-14 days according to symptomatic response(Grade 2C) Maintenance: Clotrimazole pessary 500mg weekly (1C)
NAC sp & azole
resistance
Nystatin pessaries 100,000units nocte for
14 days/month for 6 months (2C)
Consider 14 days per month for 6 month of the alternative regimens (2D)
Severe VVC
Fluconazole 150mg on day 1 and 4 (1B)
Clotrimazole 500mg tablet or pessary on day 1 and 4 (1B)
Miconazole nitrate vaginal suppository 1200mg on day 1 and 4 (1B)
Breast feeding
Treatment regimens using topical imidazoles only should be as per the recommendations listed above for non-pregnant women with acute,
recurrent and chronic VVC.
NAC – Non-albicans Candida; * Oral therapies must be avoided in pregnancy, risk of pregnancy and breast feeding (1B); **Creams and pessaries may damage diaphragms and latex condoms. 2
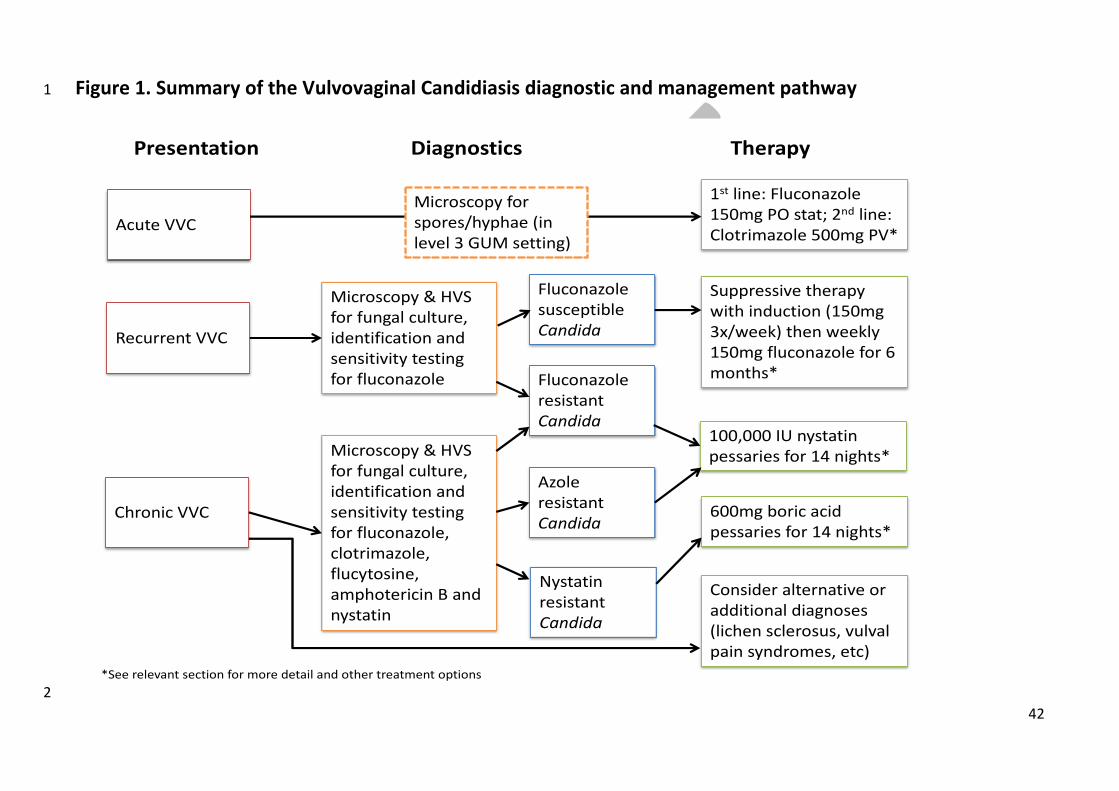
42
Figure 1. Summary of the Vulvovaginal Candidiasis diagnostic and management pathway 1
2
Acute VVC
Chronic VVC
1st line: Fluconazole 150mg PO stat; 2nd line: Clotrimazole 500mg PV*
Microscopy & HVS for fungal culture, identification and sensitivity testing for fluconazole
Presentation Diagnostics Therapy
Recurrent VVC
Microscopy & HVS for fungal culture, identification and sensitivity testing for fluconazole, clotrimazole, flucytosine, amphotericin B and nystatin
100,000 IU nystatin pessaries for 14 nights*
Fluconazole resistant Candida
Fluconazole susceptible Candida
Consider alternative or additional diagnoses (lichen sclerosus, vulval pain syndromes, etc)
Suppressive therapy with induction (150mg 3x/week) then weekly 150mg fluconazole for 6 months*
Azole resistant Candida
Nystatin resistant Candida
600mg boric acid pessaries for 14 nights*
Microscopy for spores/hyphae (in level 3 GUM setting)
*See relevant section for more detail and other treatment options