
Basal Ganglia examinatinandishesr.com/wp-content/uploads/BG-examination.pdf•Akatisia •Shuffling...
14
Basal Ganglia examinatin Malakouti SK School of Behavioral Sciences, Iran University of Medical Sciences Malakouti SK, Tehran Instutute of Psychiatry, IUMS
Transcript of Basal Ganglia examinatinandishesr.com/wp-content/uploads/BG-examination.pdf•Akatisia •Shuffling...

Basal Ganglia examinatinMalakouti SK
School of Behavioral Sciences,
Iran University of Medical Sciences
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

B.G component
• Striatum (GABA)
• Pallidum (GABA)
• Sustantia nigra (DA)
• Subthalamic N.(Glutaminergic)
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

B.G components
• Striatum (GABA)
• Pallidum (GABA)
• Sustantia nigra (DA)
• Subthalamic N. (Glutaminergic)
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Frontal areas connected with BG(striato-thalamo circuit), 5 neural loop (Alexander, Crutcher-1990
• Skeletomotor: • Premotor c. (PMC)
• Supplementary motor area. (SMA)
• Motor C. (MC)• Oculomotor: frontal eye field(FEF)
• Supplementary eye field (SEF)
• Prefrontal c.• Dorsolateral f.(DLFC)(9-10)
• Orbitifrontal c (LOFC)
• Limbic circuit• Anterior cingulate area(ACA)
• medial orbitofrontal cortex(MOFC)
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Caud.
SNcThal.
GPi
+
-
--
-
++
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

LCSPT dysfunction and correlated symptoms
• Forebrain DA hypoactivity
• Limbic-striatum disinhibition
• Pallidum over-inhibition
• Decreased inhibition of thalamus
• Disinhibition of
prefrontal, amygdala
• explain characteristic:• emotional
• cognitive
• motor activity
• guilty ruminations
• motor slowing
• would not explain underactivity of • decreased attention
• Executive dysfunction
Malakouti SK, Tehran Instutute of Psychiatry, IUMS
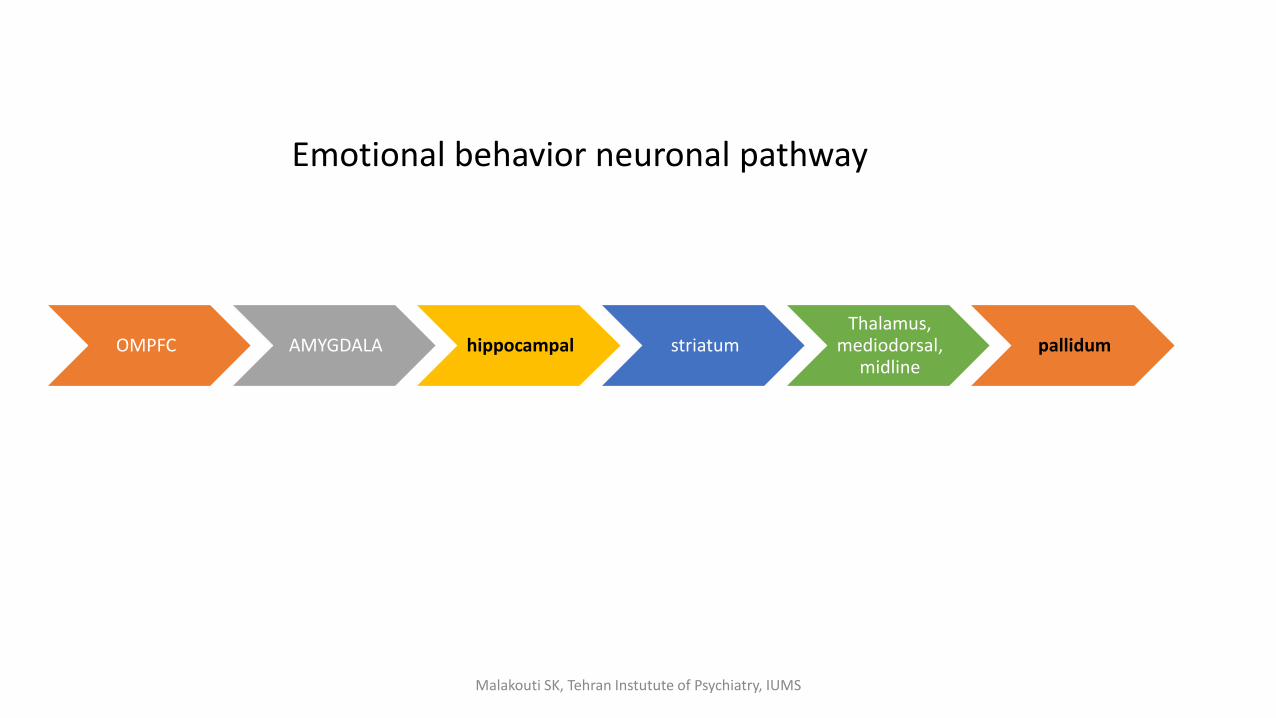
OMPFC AMYGDALA hippocampal striatumThalamus,
mediodorsal, midline
pallidum
Emotional behavior neuronal pathway
Malakouti SK, Tehran Instutute of Psychiatry, IUMS
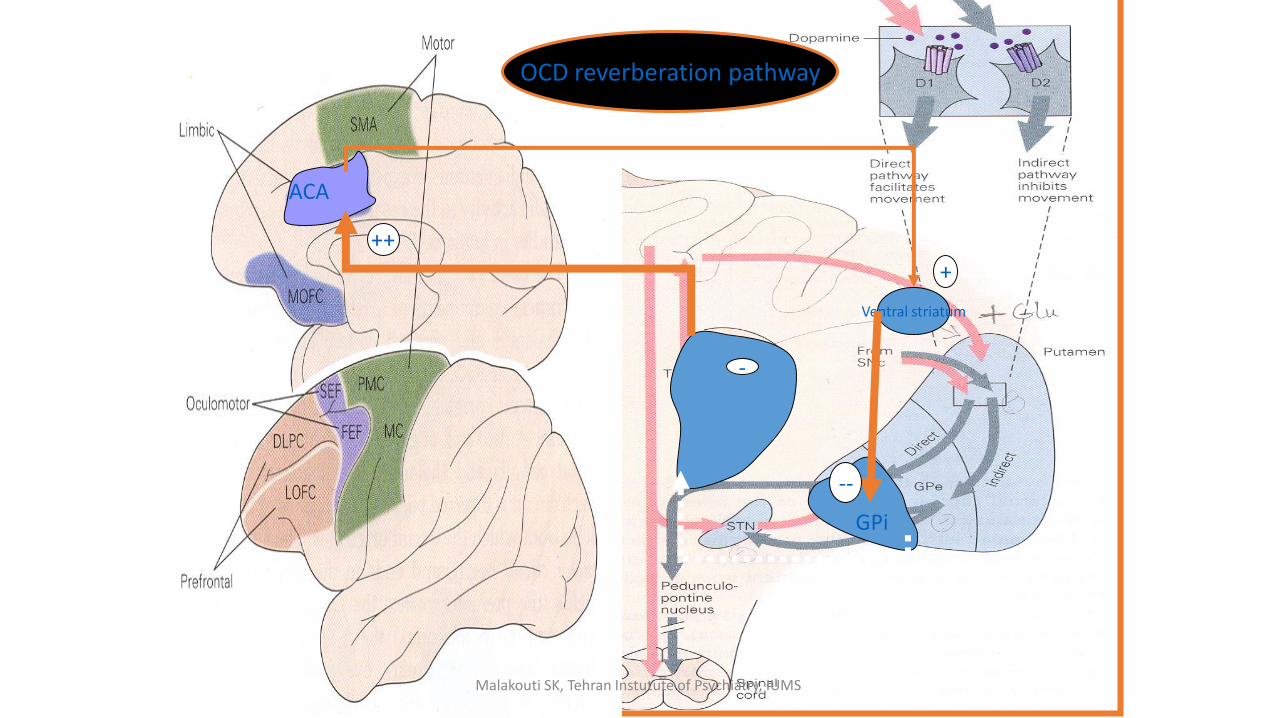
ACA
Ventral striatum
GPi
--
-
OCD reverberation pathway
+
++
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

BG and Cerebral cortex contributes to:
1. Voluntary movement
2. Skeletomotor
3. Oculomotor
4. Cognition
5. Emotion
6. Motivation
7. Social appropriate response
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Movement manifestation of BG dysfunction
• Tremor
• Agitation
• Akatisia
• Shuffling gait
• Striatal hand: ulnar deviation, flexion of fingers at the metacarpal
phalangeal joints
• Pill rolling tremor
• Loss of agility
• Involuntary movements
• chorea
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Striatal hand
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Cognitive manifestation of BG dysfunction
• Cognitive problem: • mental torpor, • cognitive dilapidation, • apathy,
• Learning, speech and language, praxis, calculation are intact.
• Retrieved material impaired. Required number of prompt indicate the degree of impairment.
• Impersistence and slowed completion of task
• Huntington’s disease
• Parkinson’s disease
• Lacunaire syndrome
• Tumors
• Progressive supranuclearpalsy
• Multisystem atrophy
• Wilson’s disease
• Corticobasal degeneration
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

feature Cortical subcortical
Language Aphasia Preserved
Speech Normal until late stage Dysarthria early
Recall Impaired Impaired
Recognition cue Ineffective Effective
Encoding ineffective Effective
Priming absent Present
Procedural intact Impaired
Visuoperception Severely impaired Mild impaired
Calculation Acalculia Relatively preserved
Executive function Relative to overall impairment More than overall impairement
Cognitive speed Normal Slowed
Malakouti SK, Tehran Instutute of Psychiatry, IUMS

Features Cortical subcortical
Personality and mood No insight, unconcerned, infrequent
depression
Insight, apathetic, frequent
depression
Motor speed Normal until late stage Slowed
Posture Normal until late stage Stooped, rigid
Gait Normal until late stage Abnormal
coordination Normal until late stage abnormal
Involuntary movement Normal until late stage Tremor, chorea, tic, dystonia
Malakouti SK, Tehran Instutute of Psychiatry, IUMS


















