
Barrett’s esophagus - University of Nevada, Reno
26
Barrett’s esophagus Thomas C. Caves, MD Digestive Health Associates August 8, 2016
Transcript of Barrett’s esophagus - University of Nevada, Reno

Barrett’s esophagusThomas C. Caves, MD
Digestive Health Associates
August 8, 2016

Definition
• Metaplastic columnar epithelium
• replaces normal squamous epithelium (above the Z-line)
• presence of goblet cells
• Short versus long segment
• Prague Scoring system
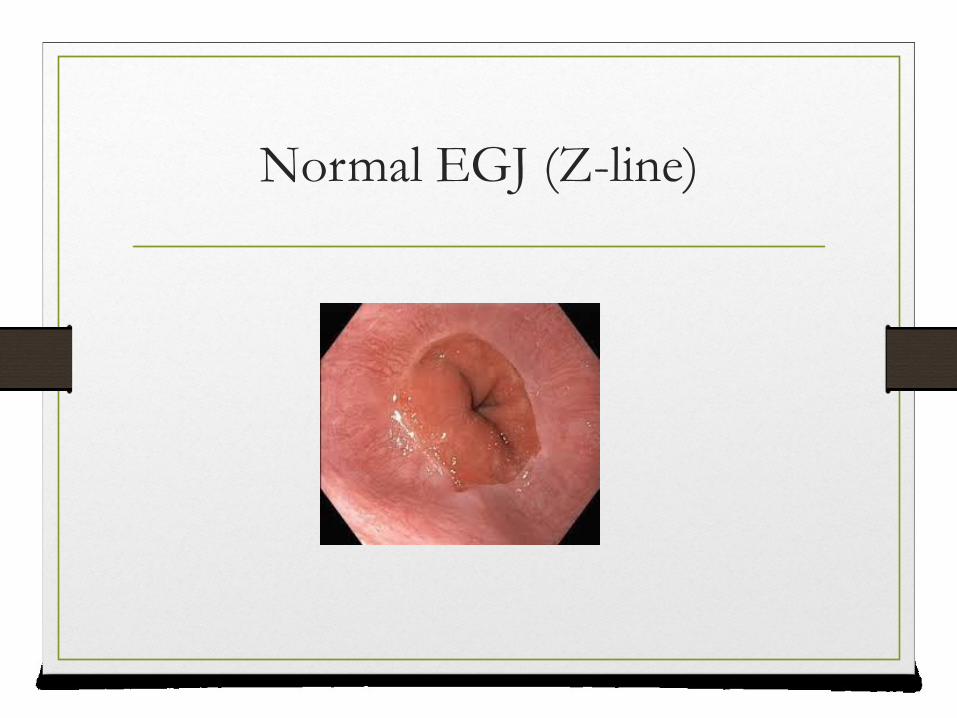
Normal EGJ (Z-line)

Long segment Barrett’s esophagus
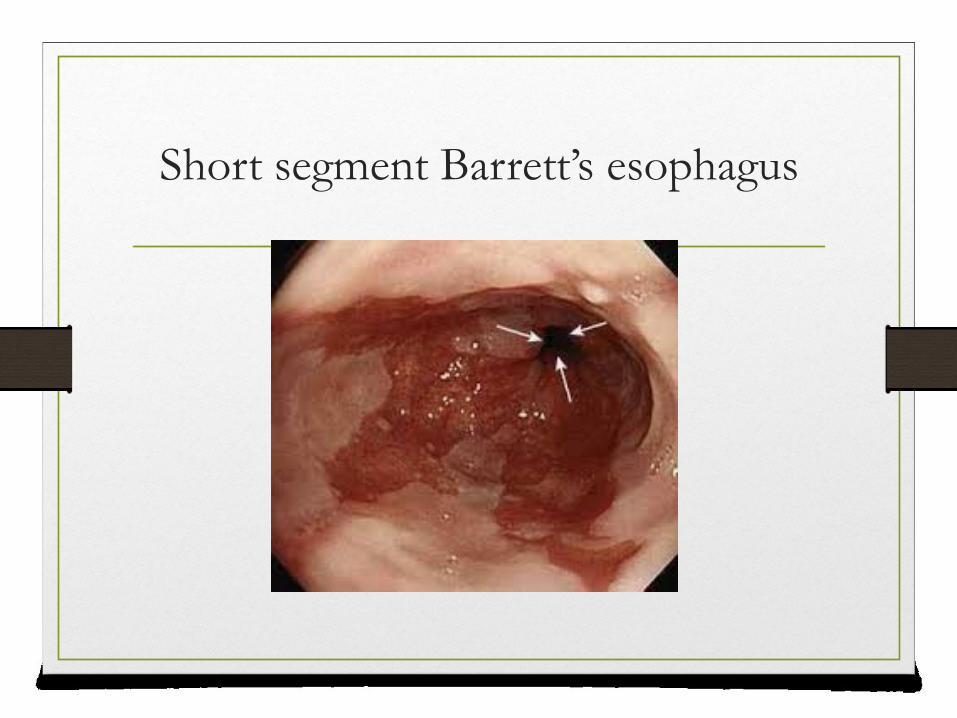
Short segment Barrett’s esophagus

Barrett’s “islands”
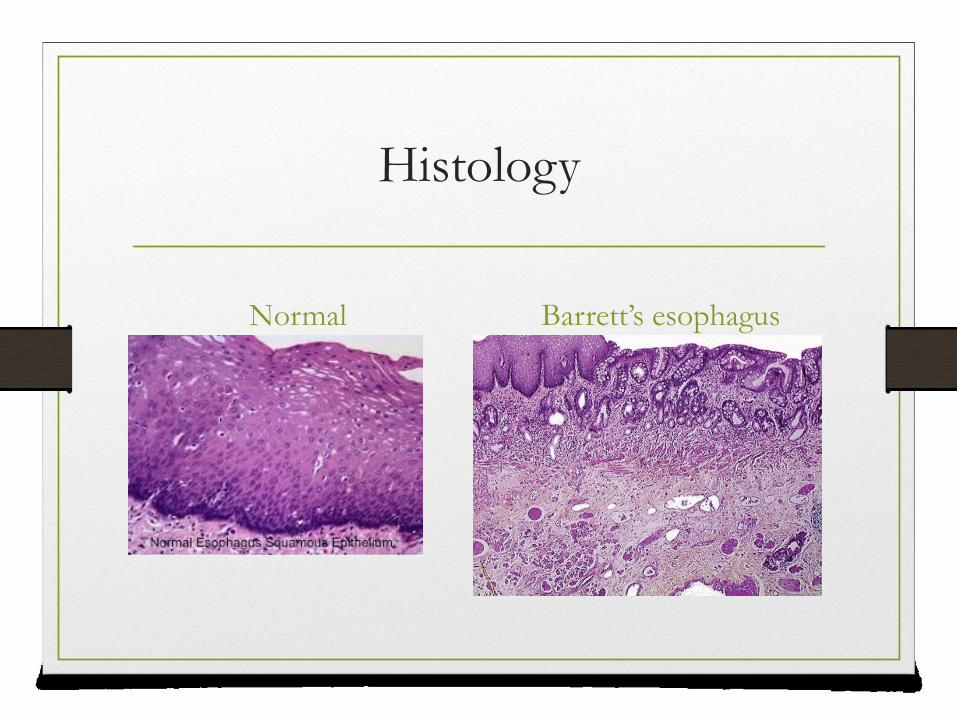
Histology
Normal Barrett’s esophagus

Goblet cells

Epidemiology
• 1% of general population
• 3.5 million patients in the US
• 5% without reflux symptoms
• 5-15% in patients with reflux
• 2:1 male predominance

Risk Factors
• GERD
• erosive esophagitis
• Genetics
• germline MSR1 mutations
• Obesity
• Age
• Gender/Race

Dysplasia
• Low grade or high grade
• Varies depending length of Barrett’s esophagus• Short segment 8%
• Long segment 24%

Degrees of dysplasia
Low grade High grade

Risk of Adenocarcinoma of the EGJ
• Varies with degree of dysplasia
• Non dysplastic 0.1-0.4% per year
• Low grade dysplasia 1.0% per year
• High grade dysplasia 6-10% per year

Adenocarcinoma of the EGJ

Esophageal cancer

Screening Surveillance
• Male
• Older
• Obese (abdominal)
• Caucasian
• GERD
• Hiatal hernia
• Repeat EGD 1 year after diagnosis then every 3-5 years
• Low grade dysplasia- 6 months (or treat)
• High grade dysplasia-treat

Treatment
• Acid suppression
• Weight loss
• Aspirin
• plus as statin?
• Ablation

Radiofrequency ablation
• Radiofrequency energy applied directly to Barrett’s tissue
• 360 degrees via balloon
• 90 degrees via probe attached to scope
Radiofrequency Ablation Indications
• High grade dysplasia
• Low grade dysplasia
• Non dysplastic Barrett’s• Not yet
Halo 360 (balloon) ablation
• https://www.youtube.com/watch?feature=player_de
tailpage&v=iu4kv90cOII

Halo 90 ablation
• https://www.youtube.com/watch?v=q6x8_pVvvAc
&feature=player_detailpage

Eradication Rates
• Complete
• 80-100%
• Dysplasia
• 90-100%

RFA complications
• Stricture
• Chest pain
• Bleeding
• Perforation

Other Treatments
• Photodynamic therapy
• Cryoablation
• Esophagectomy
• Endoscopic mucosal resection (raised lesions)
• Surveillance (low grade dysplasia)
What next (after RFA)?
• Surveillance endoscopy
• 3, 6, 12 months
• Acid suppression
• 20% recurrence rate
• Weight loss
• ?NSAID’s

Future of Barrett’s Esophagus
• Identification of at risk patients
• Sampling techniques
• Markers for progression to dysplasia/carcinoma
• RFA for all patients?
• Chemoprophylaxis














![Barrett’s esophagus and new therapeutic modalitiesThe prevalence of Barrett’s esophagus in the adult population is 0.4–1.6% [1,3,12,13]. Assum-ing a US adult population in 2007](https://static.fdocuments.us/doc/165x107/5f4d5b4d6dfbad3c763bb443/barrettas-esophagus-and-new-therapeutic-modalities-the-prevalence-of-barrettas.jpg)


