Bariatric and Metabolic Institute Sensitivity Training: How to Communicate to your Bariatric Patient...
46
Bariatric and Metabolic Institute Sensitivity Training: How to Communicate to your Bariatric Patient Leslie J. Heinberg, PhD February 26, 2011
-
Upload
william-andrews -
Category
Documents
-
view
214 -
download
1
Transcript of Bariatric and Metabolic Institute Sensitivity Training: How to Communicate to your Bariatric Patient...

Bariatric and Metabolic Institute
Sensitivity Training: How to Communicate to your Bariatric Patient
Leslie J. Heinberg, PhD
February 26, 2011


Big Waistlines Mean Bigger Carbon Footprints: Obesity and Climate Change Linked
• A smaller waistline isn't just better for our health - it's also good for the planet, according to a recent study from the International Journal of Epidemiology. Researchers found that a lean population will consume almost 20 percent less food and produce fewer greenhouse gases than a population in which 40 percent of people are obese, similar to the U.S.
• "As if being obese didn't already carry enough social stigma. Now, it seems, you're not just killing yourself by being overweight, but you're killing the planet, too."

What our patients say
• “No other disease prompts cruel, cutting remarks from complete strangers and medical people alike that we hope are allies in our quest for health”
• “I've yet to see any of the messages (regarding public health crisis of obesity) that show compassion and understanding that it is anything but gluttony and laziness”
• “At this point, I can only hope that I'll still be alive to see the attitudes of blaming the victims change.”

Weight Stigma—Acts of Omission
• Ignored
• Not fitting in
• Dating
• Employment

Weight Stigma—Acts of Commission
• Staring
• Laughing
• Teasing
• Jokes
• “Helpful” commentary
• Back-handed compliments

Psychosocial Cost of Obesity
• Stigma
Obese people are often perceived as:– Lazy or unmotivated
– Gluttonous and lacking willpower or self control
– Unattractive
– Slow, stupid, incompetent, immoral/bad
Thin people are often perceived as:– Energetic or motivated
– In Control
– Beautiful, smart, moral/good, valuable

Social Stigma
• By age 6, and probably earlier, children are aware of the societal bias against fat people and generally express it themselves– Bias increases with age
• 6th grade children rank overweight children as the least desirable playmate– More so than blind child, child in wheelchair, or one with facial
disfigurement
Latner et al., 2007

Social Stigma
• Prejudice against obese has been shown in diverse samples of adults including:– Nurses (Brown, 2006)
– Employers (Roehling & Roehling, 2007)
– Teachers (Puhl & Latner, 2007)
– Dietitians (Berryman et al., 2006)
• A survey of college students found that they would prefer to marry an embezzler, drug user, shoplifter, or blind person than someone who is obese.

Social Stigma
Puhl & Brownell, 2006
Source of Stigma Ever Experienced
Multiple Times
Family Members 72% 62%
Doctors 69% 52%
Classmates 64% 56%
Co-workers/Colleagues 54% 38%
Spouse 47% 32%
Employers/Supervisors 43% 26%
Dietitians/Nutritionists 37% 26%
Teachers/Professors 32% 21%
Mental Health Professionals 21% 13%

Social Stigma
Puhl & Brownell, 2006
Coping Responses to Stigma Women Men
Positive Self-Talk 92% 92%
Eating 80% 79%
Heading off negative remarks 89% 93%
Social support from non-overweight people
90% 85%
Seeing the situation as the other person’s problem
86% 89%
Crying, isolating self 76% 75%
Negative self-talk 75% 69%
Avoiding or leaving situation 53% 46%

Social Stigma
• Sources of Worst Stigma Experience– Peers 15.8%
– Parent 12.7%
– Stranger 9.8%
– Spouse 9.5%
– Health Professional 8.2%
• Perceptions of most common stereotypes– Lazy 62.5%
– Overeats/binges 27.0%
– Unintelligent 18.8%
– Lack of willpower 18.2%
– Poor hygiene 12.9%
– Unattractive/ugly 6.4%
Puhl et al., 2007
Psychosocial Costs of Obesity
• Discrimination
– Hiring, placement, and discharge prejudice in employment
– Inequities in wages and promotions
– Prejudice in health care and education
– Public accommodations (e.g., airlines, restaurants, theaters, buses, etc)
– Jury selection, rental housing, & in adoption
Puhl & Heuer (2009). The stigma of obesity: A review and update. Obesity, 17 (5).
Stigmatization Experiences of Bariatric Patients
• Stigmatization experience in the last month– 100% reported
– Frequency negatively associated with
–Self-esteem
– Frequency positively associated with
–Depression
–Anxiety
–Body image disturbance
–Emotional eating
–Diagnoses of BED
Friedman et al., 2008
Stigmatization Experiences of Bariatric Patients
• Stigmatization was reported to be relatively infrequent– Consistent with “several times in your life”
• Stigmatization experiences– Unrelated to BMI
– Occurrence associated with
–Poorer weight-related QOL
–Depressive Symptoms
Sarwer et al., 2008

Two Types of Anti-fat Attitudes
• Explicit – Negative attitudes held in one’s conscious awareness
– Subject to social desirability
• Implicit– Negative attitudes that occur outside one’s conscious
awareness
– Occur automatically
https://implicit.harvard.edu/implicit/demo/index.jsp
Power Differential
Health-care providers
Patients

Physicians’ views of obese patients
• Non-compliant
• Lazy
• Lacking in self-control
• Awkward
• Weak-willed
• Sloppy
• Unsuccessful
• Unintelligent
• Dishonest
• Less desire to help the patient
• A “waste of (physician’s) time”
Campbell et al., 2000; Fogelman et al., 2002; Foster, 2003; Hebl & Zu, 2001; Kristeller & Hoerr, 1997, Price et al., 1987; Puhl & Heuer, 2009

Physician Bias
• Higher BMI is significantly and negatively associated with physician perceptions than their patients will be non-adherent to medication (PrR=0.76 per 10 kg/m2 increase in BMI)– Independent of actual medical adherence
• Higher BMI is significantly and negatively associated with physicians’ reported “respect” for their patients (PrR=0.83 per 10 kg/m2 increase in BMI)– Independent of age and gender of patient
Huizinga, Bleich, et al., 2009; Huizinga, Cooper, et al., 2009

We’re not immune
• Health care professionals specializing in obesity (clinical or research) have strong negative associations and attitudes toward obese persons– Implicit attitude test given to audience at NAASO
– Implicit anti-fat bias
–Associated with stereotypes of
–Lazy
–Stupid
–Worthless
Schwartz et al., 2003
We’re not immune
– Factors associated with less implicit bias:
–Men
–Older
–+ Emotional outlook
–> BMI
–Having friends who are obese
Schwartz et al., 2003

We’re not immune
• Mental health professionals are more likely to assign negative psychological symptoms to obese patient vignette– More psychopathology
– More severe symptoms
– Worse prognosis
• Moderating factors– Men are less harsh than women
– Older MHP < younger
– Larger BMI < Smaller BMI
Davie-Coelho et al., 2000; Hassel et al., 2001
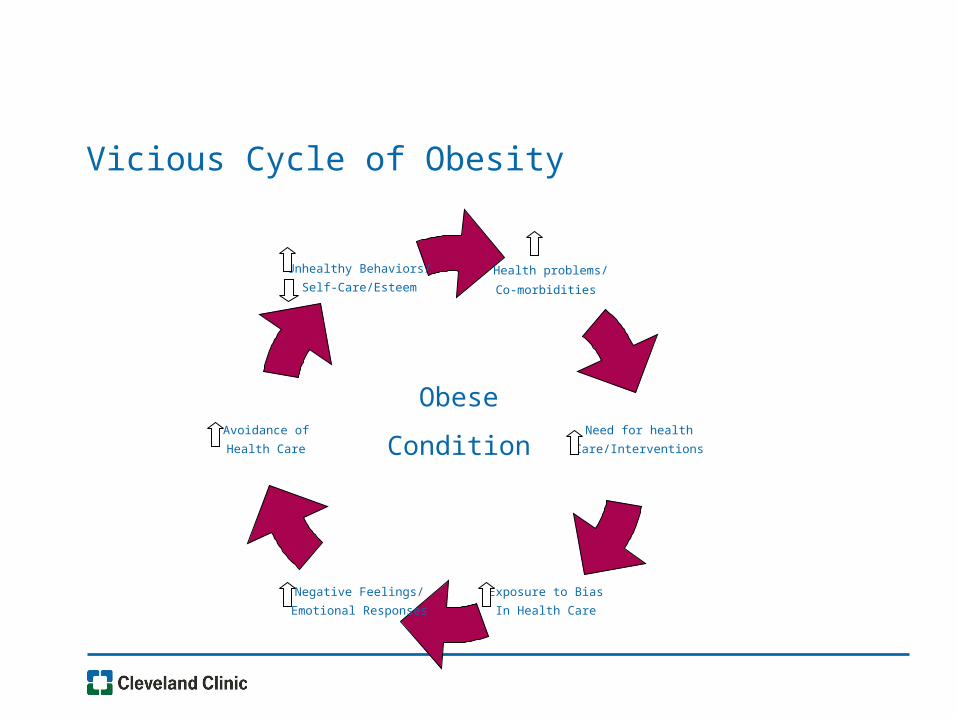
Vicious Cycle of Obesity
Need for health
Care/Interventions
Health problems/
Co-morbidities
Unhealthy Behaviors/
Self-Care/Esteem
Exposure to Bias
In Health Care
Negative Feelings/
Emotional Responses
Avoidance of
Health Care
Obese
Condition

Language We Use
• If providers want to help their patients adopt healthier lifestyles, they need to provide support to their patients, rather than instill shame and stigma.
• The language we use can make or break the relationship.

Language We Use
Should Providers Use The "F" Word When Discussing Obesity With Their Patients?
Aug 2, 2010
Last week, the British Public Health Minister (Ann Milton) urged healthcare professionals in the U.K. to tell their patients they are “fat” rather than “obese”, since (according to Milton) the word “fat” has more of an emotional impact and will better encourage them to get healthy. She added that it is important for people to take personal responsibility for their lifestyles, and that people will be less worried about their weight if they are told they are obese than if they are told they are fat.

What’s in a Name? Patients’ Preferred Terms for Describing Obesity (Wadden & Didie, 2003)
• “Imagine that you are visiting your doctor for a check-up. The nurse has measured your weight and found that you are at least 50 lb over your recommended weight. The doctor will be in shortly to speak with you”– Rate a list of terms to describe weight on how desirable or
undesirable
• “Good morning. I want to talk with you about your:”Weight Heaviness Weight problems
BMI Excess weight Fatness
Excess fat Large size Unhealthy body weight
Obesity Unhealthy BMI

Ratings of 11 terms to describe excess weight(N=167 Obese women presenting for RCT on Obesity)
Weight
Weight Problem
BMI
Excess WeightUnhealthy
Body Weight
Unhealthy BMI
HeavinessObesity
Large SizeExcess Fat
Fatness
-2 -1 0 1 2
Very Undesirable Very Desirable
Wadden & Didie, 2003

Ratings of 11 terms to describe excess weight(N=52 Obese men presenting for RCT on Obesity)
Weight
Weight Problem
BMI
Excess WeightUnhealthy
Body Weight
Unhealthy BMI
HeavinessObesity
Large SizeExcess Fat
Fatness
-2 -1 0 1 2
Very Undesirable Very Desirable
Wadden & Didie, 2003

Ratings of 11 terms to describe excess weight(N=105 Morbidly obese women presenting for Bariatric Surgery)
Weight
Weight Problem
BMI
Excess WeightUnhealthy
Body Weight
Unhealthy BMI
HeavinessObesity
Large SizeExcess Fat
Fatness
-2 -1 0 1 2
Very Undesirable Very Desirable
Wadden & Didie, 2003
Is the “Obesity” word the new “F” word?
• Fat is a relative term
• Obese is a scientific term– Implies a disease state
– Seen as more politically correct
“Obese” versus “Fat”
• Examined impact of group label on weight bias
• Participants answered a number of question regarding their attitudes about “obese” people or “fat” people
• Overall, the term “obese” evokes stronger negative evaluations than “fat”
Vartanian, 2010

“Obese” versus “Fat”
0
1
2
3
4
5
6
7
Favorable Control Disgust Pity Similar Become
Women Obese
Men Obese
Women Fat
Men Fat
Vartanian, 2010
* ** §
*
§
*; Obese > Fat p < .05
§; Women > Men, p <.05
Non-verbal Message
• Grunts/Groans in transporting
• Eye-rolling
• Facial Expressions
• Body Language


Non-Verbal Communication
Special Populations—Very High BMI/Bariatric SNF
• Arrive by ambulance
• Often stretcher bound
• Can’t wait in waiting room
• Can’t fit in psychology or nutrition offices
• Inappropriate for workshop
• Attract attention (even disdain) from other patients
• Transporting to exam rooms difficult
• Weighing often impossibility
Special Populations—Very High BMI/Bariatric SNF
• Privacy and dignity are paramount
• Eye-contact
• Touch
• Recognize discomfort and offer to help
• Offer option to get out of stretcher
Critical points from our diversity training module
• In working with patients of ALL shapes and sizes, it is important to:– Express warmth and empathy by making direct eye contact
– Think before you speak
– Address the patient by name
– Shake hands when appropriate
– Sit near the patient at eye level when carrying on a conversation
– Be discreet (do not ask for extra-large gown, etc. where other patients or visitors can hear)
– Focus on the patient, not the patient’s obesity
– Acknowledge the challenges that the patient deals with on a daily basis

Weighing Procedures
• An area of privacy—patients should be weighed in a private setting, away from other patients and personnel.
• Without negative comment—weight should be recorded silently without commentary or negative body language (e.g., expression of shock or disgust).
• An appropriate scale—wide-based scales that measure >350 lbs are recommended.
Toolkit for Healthcare Professionals
• Yale Rudd Center for Food Policy and Obesity– Kelly Brownell, PhD & Rebecca Puhl, PhD
– Excellent resource for physicians
–Setting up physical environment
• http://www.yaleruddcenter.org/resources/bias_toolkit/index.html

Promote a culture of sensitivity
• Obesity is a chronic disease that results from a complex interplay between biological, genetic, psychosocial and environmental factors
• Bariatric patients come in ALL shapes and sizes as well as personality profiles and physical and psychological strengths and weaknesses
• There is benefit and merit in all human diversity including the diversity of size, shape and weight
• Bariatric patients have the right to be treated as a unique individual