Bangladesh WS report - Home - WBTI Report on National Assessment of the status of Global Strategy...
31
1 Report on National Assessment of the status of Global Strategy for IYCF practices : Finding gaps Reaching consensus BANGLADESH Prepared by Dr. M Quamrul Hassan Member of BOT, BBF Assistant Professor, Paediatrics Institute of Child and Mother Health, Dhaka And Labin Rahman Assistant Coordinator Bangladesh Breastfeeding Foundation Bangladesh Breastfeeding Foundation (BBF) 8/12 Sir Syed Road, Mohammadpur, Dhaka, Bangladesh Ph: 9126501 Email: [email protected] Web site: bbfbd.org
Transcript of Bangladesh WS report - Home - WBTI Report on National Assessment of the status of Global Strategy...

1
Report on
National Assessment of the status of Global Strategy for IYCF practices :
Finding gaps Reaching consensus
BANGLADESH Prepared by Dr. M Quamrul Hassan Member of BOT, BBF Assistant Professor, Paediatrics Institute of Child and Mother Health, Dhaka
And Labin Rahman Assistant Coordinator Bangladesh Breastfeeding Foundation
Bangladesh Breastfeeding Foundation (BBF)
8/12 Sir Syed Road, Mohammadpur, Dhaka, Bangladesh Ph: 9126501 Email: [email protected] Web site: bbfbd.org

2
Key words APPAR Asia Pacific Participatory Action Research BBF Bangladesh Breastfeeding Foundation BDHS Bangladesh Demographic Health Survey IBFAN International Baby Food Action Network IYCF Infant and Young Child Feeding MDG Millennium Development Goal MICS Multiple Indicator Cluster Survey WHA World Health Assembly

3
National Assessment of the Status of Global Strategy for
Infant and Young Child Feeding and Finding Gaps
Introduction: Optimal Infant and Young Child Feeding (IYCF) yields the best survival, growth,
intelligence and development outcomes, reduces chronic disease rates, and, where fully
implemented, can reduce under-five mortality by at least one-half. And it is vital to
protect optimal breastfeeding in unstable situations like emergencies and in presence of
HIV/AIDS endemicity, where additional guidance is needed.
With these facts in the background, the “Global Strategy for Infant and Young Child
Feeding,” approved by WHA in May 2002, was endorsed by the UNICEF Executive
Board as the foundation for UNICEF's action in support of optimal infant and young child
feeding for survival, growth and development of children worldwide. The Strategy is
reflective of rights-based programming, includes a lifecycle approach and recognition of
gender needs, and it is supportive of mother and family, impacting directly on early
childhood survival, growth and development.
The clear goal of the global IYCF strategy is to improve the survival, growth and
development of all children during the first three years of life through protection,
promotion, and support of early and exclusive breastfeeding for the first six months,
followed by continued breastfeeding up to 2 years or longer with age-appropriate,
active, frequent complementary feeding. Breastfeeding frequency and amount should
not diminish when complementary foods are added after 6 months.1
There are nine specific operational targets in the Global Strategy. First, the four targets
of the Innocenti Declaration (WHO/UNICEF meeting on 1 August 1990) are reaffirmed with
urgency.
In brief, they call on governments for measures to establish:
1. Coordinator/Committee – Support the development of a national breastfeeding coordinator of appropriate authority and a multisectoral national breastfeeding committee.
1 WHO/UNICEF Integrated Management of Childhood Illness (IMCI) documents

4
2. BFHI – All maternity services should be enabled to fully practise the Ten Steps to Successful Breastfeeding [the Baby-friendly Hospital Initiative].
3. International Code - Support implementation of the International Code of
Marketing of Breastmilk Substitutes and subsequent relevant WHA Resolutions ("the Code").
4. Maternity Protection - Be creative in supporting legislation to protect the
breastfeeding rights of working women (ratification and/or implementation of the ILO Maternity Protection Convention 2000 No. 183 and Maternity Protection Recommendation 2000 No. 191).
The Global Strategy specifies five additional targets. These call on governments to: 5. Develop Policy and Programmes – Support, develop, implement, monitor and
evaluate a comprehensive policy on infant and young child feeding, in the context of overall national development strategy and frameworks, and national policies and programmes for nutrition, child and maternal reproductive health, and poverty reduction.
6. Ensure multisectoral, and multiple level support for optimal breastfeeding –
Build on development and other multisectoral strategies to provide consistent/complementary messages from all sectors to provide health, social, workplace, and political support for optimal breastfeeding.
7. Support proper complementary foods and feeding –The preparation and
content of age-appropriate complementary foods, as well as the active, frequent and responsive feeding needs should both be included in programming, while active support for breastfeeding is continued.
8. Address exceptionally difficult circumstances –
− include infant and young child feeding in emergencies in national policies
− include special policies, guidance and support for infant feeding in areas with HIV/AIDS
− provide guidance on feeding infants and young children in exceptionally difficult circumstances, and on the related support required by mothers, families and other caregivers.
9. Enhance legislation to support the previous eight operational targets.
Tools used for assessment IYCF country status:
WHO adopted a detailed tool for assessing IYCF status in any country2. This tool is
designed to help users assess the strengths and weaknesses of policies and
programmes for protecting, promoting and supporting optimal feeding practices, and to
determine where improvements may be needed to meet the aims and objectives of the
Global Strategy for IYCF. WHO and LINKAGES were jointly responsible for developing
the tool. A large number of experts provided a variety of technical inputs, or served as
reviewers; these included staff of or individuals affiliated with WHO,
2 Infant and Young Child Feeding: A tool for assessing national practices, policies and programmes. World Health Organization, Geneva. ISBN 92 4 156254 4. ©World Health Organization, 2003

5
LINKAGES/Academy for Educational Development (AED), Wellstart International (WSI),
the United States Agency for International Development (USAID), the United Nations
Children’s Fund (UNICEF), the World Alliance for Breastfeeding Action (WABA), and a
number of nongovernmental organizations and individuals from various countries.
The Tool can be used as a companion piece to the Global Strategy for Infant and Young
Child Feeding as an assessment tool to help determine where improvements might be
needed to meet the Global Strategy targets. Consideration should be given to using the
Tool periodically, every several years, to track trends on the various indicators, report on
progress, identify areas still needing improvement, and assist in the planning process.
Parts of the Tool
Part one, Infant and young child feeding practices can be used to assess progress
made on key practices in infant and young child feeding and to help identify background
data which interact with these practices. Practice indicators are based on those
recommended by WHO for global use.
Part two, National infant and young child feeding policies and targets are focused
on the key actions and targets identified by the Innocenti Declaration, which
governments have been encouraged to achieve, as well as on additional targets
identified in the Global Strategy for Infant and Young Child Feeding. This part of the Tool
provides a mechanism for assisting countries in assessing their progress in meeting
these key targets.
Part three, National infant and young child feeding programme is focused on other
important aspects of a comprehensive national programme that take more time to
evaluate. These include, for example, up-to-date pre-service education, community
outreach activities, and contraceptive support for breastfeeding women. The material in
this section will help to guide in an initial assessment of progress in the development and
implementation of key components of a national programme. The key components
included here have been shown to play an integral role in the overall approach needed
to protect, promote, and support optimal infant feeding practices.

6
These three parts of the Tool will help to provide assessment data that can assist
planners and decision-makers at various levels in identifying the strengths and
weaknesses of their current policies and programmes. This, in turn, will enable them to
plan effectively for any needed improvements.
Suggested Sources of data. Usually a high-quality source of data is the Demographic
and Health Survey (DHS) conducted in collaboration with Macro International and
national research organizations, with support from USAID. If this source is used, the
data are likely to be comparable across countries. Other sources include the UNICEF
Multiple Indicator Cluster Survey (MICS) and the WHO Global Data Bank on
Breastfeeding and Complementary Feeding . Local sources like recent national surveys
may have the most recent information.
Asia Pacific Participatory Action Research (APPAR) Toolkit Software developed
by IBFAN Asia Pacific
The Toolkit - The APPAR Toolkit helps to assess the infant feeding situation in relation
to the Global Strategy for Infant and Young Child Feeding. This uses a simplified
questionnaire adapted from that of Global Strategy. It is a long-term effort to protect,
promote and support breastfeeding in and around the Asia Pacific Region.
The APPAR Toolkit (Software) is a web-based utility that allows different users across a
wide geographical area to pool in data to a central database. It provides a computer-
based interface for extending and simplifying the usage of the original toolkit for
assessment and monitoring purposes. It maintains the record of various indicators
reflecting the status of Infant and Young Child Feeding Practices and helps to analyze
the situation by using an objective scoring of these indicators.
The objective score is then used to assign colour codes representing status of indicators
for various countries. These features are then stored in the APPAR Databank and can
be used to generate color-coded tables, graphs, charts and maps.
The Toolkit thus helps documenting programme success in a quick and easily
understandable manner and also stimulates further action to improve the status of the
Infant and Young Child Feeding Practices.

7
The Databank - The APPAR databank uses the information collected by the APPAR
Toolkit to provide a data resource center for Infant and Young Child Feeding (IYCF) data
in the Asia Pacific Region. It provides a fast and simple access to IYCF data through an
interface called the APPAR Smart Chart.
The Smart Chart Tool helps to generate customized tables, bar graphs, trend charts and
color-coded maps for simple and effective visualization of information, which can be
used to create fast and impressive reports.
The Smart Chart Tool can thus be used as a useful, up-to-date and simple data
visualization and research assistant for topics requiring IYCF data from the Asia Pacific
region.
The toolkit assesses IYCF situation in the following 15 areas:
SCORE 1 Early Initiation of Breastfeeding Rates SCORE 2 Exclusive Breastfeeding for first 6 months SCORE 3 Median duration of Breastfeeding Rates SCORE 4 Bottle Feeding Rates SCORE 5 Complementary Feeding Rates SCORE 6 National Policy, Programme and Coordination SCORE 7 Baby Friendly Hospital Initiative (Ten Steps to Successful Breastfeeding) SCORE 8 Implementation of the International Code SCORE 9 Maternity Protection SCORE 10 Health and Nutrition Care SCORE 11 Community Outreach SCORE 12 Information Support SCORE 13 Infant Feeding and HIV SCORE 14 Infant Feeding During Emergencies SCORE 15 Monitoring and Evaluation

8
Background
Bangladesh Breastfeeding Foundation (BBF) has been working in the country since its
inception to ensure exclusive breastfeeding for all children up to complete 6 months,
optimum cpmplementary feeding after 6 months of age along with continued
breastfeeding up to 2 years or more, and ensuring optimum maternal nutrition. These
programme objectives are very much in line with WHO`s Global Strategy for Infant and
Young Child Feeding (IYCF). BBF also believes that appropriate infant feeding is the
key to achieve the Millennium Development Goals (MDGs). The fourth goal (MDG 4)
commits the international community to reduce mortality in children aged younger than 5
years by two-thirds between 1990 and 2015. There has been a significant improvement
in the survival and development of children over past decades; however, a lot more
needs to be done. Countries are struggling to attain the required pace of reduction of
child mortality. According to UNICEF, only Bangladesh, with a lower rate of child
mortality, is on track to meet MDG 4. It reduced under-5 deaths to almost half of its 1990
level by 2002, on an average annual rate of reduction of 5.2 per cent.
Since BBF was founded in 1989 the breastfeeding movement has helped to improve the
health and nutritional status of children and mothers in Bangladesh. Other child health
programs in Bangladesh, including those addressing immunization, diarrhoeal disease
and vitamin A capsule distribution have individually and collectively contributed to better
health and nutrition in Bangladesh. Breastfeeding programs contributed directly to the
success of these programs.
International Baby Food Action Network (IBFAN) is proposing a rapid assessment of the
Status of Global Strategy for Infant and Young Child Feeding as a part of Strategic Plan
2003-2008 and to measure the situation at the national level and to document existing
gaps. The identified gaps will be presented at the forthcoming South Asia Breastfeeding
Partners Forum II scheduled for Kathmandu, Nepal from 26-28 October 2005. In the last
year the South Asia Breastfeeding Partners Forum I was held in Bangladesh.
Bangladesh Breastfeeding Foundation (BBF) hosted the forum. The findings would be
utilized further for publishing a `South Asia Report – Status of Global Strategy`.
As a nodal agency for the protection, promotion and support of breastfeeding in the
country, IBFAN delegated the responsibility to Bangladesh Breastfeeding Foundation
(BBF) to assess the country situation and reach consensus.

9
Method of report preparation:
1. A national workshop has been organized involving key persons related to specific issues e.g. HIV/AIDS, Feeding during emergency, MIS of DGHS etc.
2. Recent statistical reports have been reviewed to obtain quantitative data for part 1
3. Draft output of the workshop has been shared among the participants and brainstorming has been done to come to consensus.
4. The draft report has been circulated among those who could not be present.
The Workshop
Bangladesh Breastfeeding Foundation (BBF) organized a workshop on National
Assessment of the status of Global Strategy for IYCF practices and Finding gaps &
reaching consensus. The workshop was held on August 27, 2005 Saturday.
Objectives of the workshop
• To find out gaps in the existing policy, program and practices with reference to IYCF
• To build a consensus among all the partners Inaugural ceremony
The coordinator BBF welcomed all the participants in her inaugural speech and
described the objectives of the workshop. After her speech Dr. S. K. Roy Secretary, BOT
of BBF expressed his concern regarding the malnutrition situation of Bangladesh. He
emphasized that to achieve the Millennium Development Goals our country needs to
address the Infant and Young Child Feeding practices. Dr. Roy requested Dr. M
Quamrul Hassan, member of BOT of BBF, to facilitate the workshop. Dr. Quamrul made
a graphical presentation and discussed Infant and Young Child Feeding (IYCF) in
Bangladesh. In the presentation, the concept of IYCF has been reviewed APPAR tool kit
has been introduced and Assessment questionnaire has been discussed.
The facilitator briefed the participants on how the group work will be continued.
Thirty-three participants attended the workshop such as: Director General of Health
Services (DGHS), Director General of Family Planning (DGFP), officials of National
Nutrition Programme (NNP), Institute of Public Health Nutrition (IPHN), National
AIDS/STD Programme (NASP), WHO, UNICEF, Plan Bangladesh, Hellen Keller
International (HKI) etc.

10
The participants were divided into four groups according to expertise and involvement in
the following categories:
Group A Co-facilitator Dr. Rowshan Jahan
- National IYCF policy & program - BFHI
Group B Co-facilitator Mr. A M M Samsad
- Infant Feeding and HIV - Infant feeding during Emergencies
Group C Co-facilitator Ms. Shaheen Sultana Ms. Syeda Khaleda
- Maternity Protection - Health and Nutrition care - Community outreach
Group D Co-facilitator Mr. Nuruzzaman Ms. Labin Rahman
- Information support - Monitoring and Evaluation - BMS code
Each group had been assigned to fill up questionnaire related to 2 -3 issues.
Each group also analyzed the existing activities, strengths and weaknesses.
They brain stormed on the activities to fill up the gaps.
Output of each group had been shared in plenary and consensus had been reached
after discussion and necessary modification.
Closing ceremony
The closing ceremony was chaired by Mr. Md. Abul Quashem Executive Director,
National Nutrition Programme. Participants presented the group work. Executive Director
expressed his gratitude to the participants for doing the whole work.
11
Compilation of the Group Work

12
Part I Sl. No. Practices Results Source
(1) Percentage of babies breastfed with one hour of birth
98.5% BBF Surveillance
(2) Percentage of babies 0<6 months of age exclusively breastfed in the last 24 hours
25.9% BBF Surveillance
(3) Babies are breastfed for a median duration of how many months?
30 months
BDHS
(4) Percentage of breastfed babies less than 6 months old receiving other foods or drink from bottles
44.4% BBF Surveillance
(5) Percentage of breastfed babies receiving complementary foods at 6-9 months of age
60.1%
6-7 months
BDHS
Summary of background data Background indicator Result Source and date
1. Population (in thousands) % urban % rural % children under 5 years
129947230 23.39% 76.61% 12.8%
BBS 2001 BBS 2001 BBS 2001 BDHS 2004
2. IMR rate (per 1000) 65 per 1000 live births BDHS 2004 3. Underweight (under-five) 88 per 1000 live births BDHS 2004 4. Diarrhoeal disease rate 0–5.9 months 6–11.9 months 12–23.9 months
3.9% 12.1% 12.5%
5. ARI rate 0–5.9 months 6–11.9 months 12–23.9 months
28.3% 29.5% 24.9%
6. Births in health facility 09% BDHS 2004 7. Total fertility rate
3.0
8.. Contraceptive prevalence 58%
13
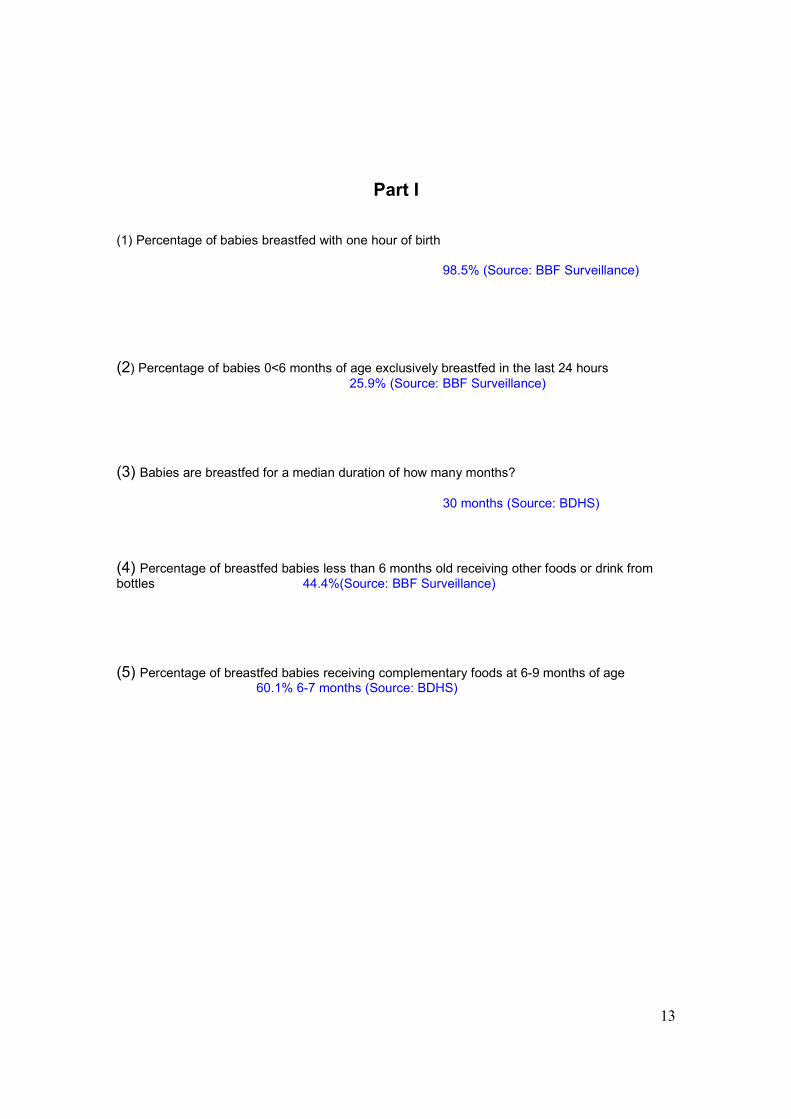
Part I
(1) Percentage of babies breastfed with one hour of birth
98.5% (Source: BBF Surveillance)
(2) Percentage of babies 0<6 months of age exclusively breastfed in the last 24 hours
25.9% (Source: BBF Surveillance)
(3) Babies are breastfed for a median duration of how many months?
30 months (Source: BDHS)
(4) Percentage of breastfed babies less than 6 months old receiving other foods or drink from bottles 44.4%(Source: BBF Surveillance)
(5) Percentage of breastfed babies receiving complementary foods at 6-9 months of age 60.1% 6-7 months (Source: BDHS)

14
Part II
(6) National Policy, Programme and Coordination
Is there a national infant and young child feeding / breastfeeding policy that protects, promotes and supports optimal infant and young child feeding and the policy is supported by a government programme? Is there a mechanism to coordinate like National infant and young child committee and coordinator?
6.1) A national infant and young child feeding / breastfeeding policy has been officially adopted/approved by the government No
6.2) The policy promotes exclusive breastfeeding for first six months and appropriate and adequate complementary feeding thereafter along with continued breastfeeding for two years and beyond. Yes
6.3) A national plan of action developed with the policy Yes
6.4) The plan is adequately funded No
6.5) There is a National Breastfeeding Committee No
6.6) The national breastfeeding (infant and young child feeding) committee meets and reviews on a regular basis Not applicable
6.7) The national breastfeeding (infant and young child feeding) committee links with all other sectors like health, nutrition, information etc. effectively Yes
6.8) Breastfeeding Committee is headed by a coordinator with clear terms of reference Not applicable
Summarize aspects of IYCF policy, program and coordination and find out gaps and suggest recommendations for action
- National Stakeholder Workshop held in July 2004 - National IYCF Strategy in the process of finalization - National Plan of Action is also under process of development involving
different stakeholders
(7) Baby Friendly Hospital Initiative (Ten Steps to Successful Breastfeeding)

15
(7A) What percentage of hospitals and maternity facilities that provide maternity services have been designated "Baby Friendly" based on the national criteria?
7.1) Percentage of hospitals and maternity facilities that provide maternity services have been designated "Baby Friendly" for implementing ten steps to successful breastfeeding 84%
(7B) What is the skilled training input in BFHI programme?
7.2) Percentage of BFHI designated hospitals that have been certified after a minimum recommended training of 18 hrs for its entire staff working in maternity services. 88%
(7C) What is the quality of BFHI programme implementation? Good quality
7.3) BFHI programme relies on training of health workers Yes (for all level
Health Care Providers)
7.4) A standard monitoring system is in place A monitoring system is in place
but needs to be strengthened further
7.5) An assessment system relies on interviews of mothers Yes
7.6) Reassessment systems have been incorporated in national plans Not yet
Summarize the situation and Find out gaps and suggest recommendations for action
� More involvement of technical persons � Institutionalizing MIS in Government system � Reassessment system � Development of skilled counselor at BFHI - LMC � Linkage of BFHI with community � To develop a guiding principle for refresher training of BFHI
(8) Implementation of the International Code

16
Is the International Code of Marketing of Breastmilk substitutes in effect and implemented? Has any new action been taken to give effect to the aims and principles of the code?
8.1) No action taken / planned or no information Not Applicable
8.2) The best approach is being studied Not Applicable
8.3) Law drafted, awaiting final approval Not Applicable
8.4) Some articles of the code as a voluntary measure Not Applicable
8.5) Code as a voluntary measure to be deleted Not Applicable
8.6) Some articles of Code as law Not Applicable
8.7) All articles of the Code as law, monitored Yes
8.8) All articles of the Code as law, monitored and enforced Yes
8.9) New / additional legislation to protect breastfeeding to give effect to the aims and principles of the code exist Proposed
Summarize the situation and Find out gaps and suggest recommendations for action
� Additional legislation has been proposed & � Additional Secretary Ministry of Health & Family Welfare has agreed to
work on that
(9) Maternity Protection

17
Is there legislation that meets International Labor Organization (ILO) standards for protecting and supporting breastfeeding among working mothers?
9.1) Women covered by the legislation are allowed at least 14 weeks of paid maternity leave Yes
9.2) Women covered by the convention are allowed at least one paid breastfeeding break daily Yes (Not in practiced/partly practiced
9.3) Private sector employers of women in the country give at least 14 weeks paid maternity leave and paid nursing breaks No
Required Registration of employers, required supervision
9.4) There is language in national legislation that encourages work site accommodation for breastfeeding and/or childcare in work places in the formal sector Yes
9.5) Women in informal / unorganized sector are provided same protection No
Required RRReeegggiiissstttrrraaattt iiiooonnn///dddeeefff iiinnniii tttiiiooonnn,,, RRReeeqqquuuiiirrreeeddd SSSuuupppeeerrrvvviiisssiiiooonnn
9.6) There is legislation prohibiting employment discrimination and assuring job protection for women workers during breastfeeding period Yes
9.7) The ILO MPC No 183 has been ratified Partially Yes
9.8) The ILO MPC No 183 has been enacted Partially Yes
Ref: Bengal Maternity protection Rule 1953, Bengal maternity protection act 1993, Bangladesh Service rule
Summarize the situation and Find out gaps and suggest recommendations for action
� Raise awareness among stakeholders � Maintain Supervision � Conduct consultation with Trade union, CAB � Advocacy in major Metropolitan areas � Introduce Creche through resources (seed grand), technical support
(10) Health and Nutrition care
Do workers in these systems undergo skills training, and do their pre-service education curriculum support optimal infant and young child feeding; Do these services support birth practices, do the policies of health

18
care services support mothers and children, and whether health workers responsibilities to Code are in place?
10.1) A review of health provider schools and pre-service education programmes in the country indicates that infant & young child feeding curricula or session plans are adequate inadequate No-reference
10.2) Standards and guidelines for mother-friendly childbirth procedures and support have been developed and disseminated to all facilities and personnel providing maternity care
yes to some degree No
10.3) There are in-service training programmes providing knowledge and skills related to infant & young child feeding for relevant health/nutrition care providers.
yes to some degree No
10.4) Health workers are trained with responsibility towards Code implementation as a key input.
yes to some degree No
10.5) Infant feeding-related content and skills are integrated, as appropriate, into training programmes focusing on relevant topics (diarrheal disease, acute respiratory infection, IMCI, well-child care, family planning, nutrition, the Code, HIV/AIDS, etc.) yes to some degree No
10.6) These in-service training programmes are being provided throughout the country yes to some degree No
10.7) Child health policies allow mothers and babies to stay together when one of them is sick yes to some degree No
Summarize the situation and Find out gaps and suggest recommendations for action
� Need to improve/develop guidelines, training and policies from ‘Some degree’ to 100% with training monitoring, supervision and advocacy
19
(11) Community Outreach
Are there community outreach and support mechanisms in place to protect, promote and support optimal infant and young child feeding? (See annex-5 in the main document)
11.1) Women have access to counseling services on infant and young child feeding in the community during pregnancy?
yes to some degree No
11.2) Women have access to infant and young child feeding counseling after birth yes to some degree No 11.3) The infant and young child feeding counseling services have national coverage yes to some degree No
11.4) Counseling services are integrated into an overall infant and child health strategy (inter-sectoral and intra-sectoral).
yes to some degree No
11.5) Counselors are trained in skills
yes to some degree No
Summarize the situation and Find out gaps and suggest recommendations for action
Community outreach activities are partially implemented, that needs to be improved through
� Policy formulation for integration
� Training for skill development
� Developing awareness
� Advocacy
20
(12) Information Support
Are comprehensive Information, education and communication (IEC) strategies for improving infant and young child feeding practices (breastfeeding and complementary feeding) being implemented?
12.1) There is a comprehensive national IEC strategy for improving infant and young child feeding
Yes To some degree No
12.2) IEC programmes (either governmental or non-governmental) that include infant and young child feeding are being actively implemented at local levels
Yes To some degree No -NNP selected NGO
12.3) Individual counselling and group education services related to infant and young child feeding are available within the health/nutrition care system or through community outreach
Yes To some degree No
12.4) The content of IEC messages is technically correct, sound, based on national or international guidelines
Yes To some degree No
12.5) A national IEC Campaign or programme using electronic and print media and activities has channeled messages on infant and young child feeding to targeted audiences in the last 12 months
Yes To some degree No
BF- Going on
CF- “
Summarize the situation and Find out gaps and suggest recommendations for action
� Needs improvement � Tested successful IEC strategies for important? � Child health can be undertaken - Mina Cartoon � Why Govt. outreach setup are not fully activated to be identified
21
(13) Infant Feeding and HIV
Are appropriate policies and programmes in place to ensure that mothers with HIV are informed about risks and benefits of different infant feeding options and supported in their infant feeding decisions?
13.1) The country has a comprehensive policy on infant and young child feeding that includes infant feeding and HIV
Yes To some degree No
13.2) The infant feeding and HIV policy gives effect to the International Code/National Legislation
Yes To some degree No
13.3) Health staff and community workers receive training on HIV and infant feeding policies, the risks associated with various feeding options for infants of HIV-positive mothers and how to provide counseling and support
Yes To some degree No
13.4) Antenatal VCCT is available and offered routinely to couples that are considering pregnancy and to pregnant women and their partners
Yes To some degree No
13.5) Locally appropriate infant feeding counseling in line with current international recommendations is provided to HIV positive mothers
Yes To some degree No
13.6) Mothers are supported in their infant feeding decisions with further counselling and follow up to make these decisions as safe as possible
Yes To some degree No
13.7) Special efforts are made to counter misinformation on HIV and infant feeding and to promote, protect and support breastfeeding in the general population
Yes To some degree No
13.8) On-going monitoring is in place to determine the effects of interventions to prevent HIV transmission on infant feeding practices and health outcomes for mothers and infants, including those who are HIV negative or of unknown status Yes To some degree No
13.9) The Baby-friendly hospital initiative provides guidance to hospital administrators and staff in settings with high HIV prevalence on how to assess the needs and provide support for HIV positive mothers

22
Yes To some degree No
Summarize the situation and Find out gaps and suggest recommendations for action
� Currently no comprehensive natural policy on IYCF & HIV � Limited services for counseling & support for Infant Feeding options for
HIV+ve mothers- inline with UNICEF/WHO Guidelines � No ANC- VCT monitoring available in the country
Recommendations
• Need to develop a comprehensive policy on HIV & IYCF
• Raise awareness among general population regarding PPTCT
• Routine ANC – HIV community should be included in ANC clinics
(14) Infant Feeding During Emergencies
Are appropriate policies and programmes in place to ensure that mothers, infants and children will be provided adequate protection and support for appropriate feeding during emergencies?
23
14.1) A policy that addresses key issues related to infant and young child feeding in emergencies has been endorsed or developed
Yes To some degree No
14.2) Person(s) tasked with responsibility for national coordination with the UN, donors, military and NGOs regarding infant and young child feeding in emergency situations have been appointed
Yes To some degree No
14.3) A contingency plan to undertake activities to facilitate exclusive breastfeeding and appropriate complementary feeding and to minimize the risk of artificial feeding has been developed
Yes To some degree No
14.4) Resources identified for implementation of the plan during emergencies. Yes To some degree No
14.5) Appropriate material on infant and young child feeding in emergencies has been integrated into pre-service and in-service training for emergency management and relevant health care personnel
Yes To some degree No
Summarize the situation and Find out gaps and suggest recommendations for action
Summary
5. No approved IYCF 6. IYCF options incorporated to Pre & In-service training
Recommendation
� National IYCF
� Capacity Building
� Advocacy/Mass Awareness
� Food security Infant and young child
(15) Monitoring and Evaluation
Are monitoring and evaluation data routinely collected and used to improve infant and young child feeding practices?

24
15.1) Monitoring and evaluation components are built into major infant and young child feeding programme activities
Yes To Some degree No
15.2) Monitoring and Management Information System (MIS) data are considered by programme managers as part of the planning and management process
Yes To Some degree No
15.3) Adequate baseline and follow-up data are collected to measure outcomes for major infant and young child feeding programme activities
Yes To Some degree No
15.4) Evaluation results related to major infant and young child feeding programme activities are reported to key decision-makers, both at national and regional/local levels.
Yes To Some degree No
15.5) Monitoring of key infant and young child feeding practices is built into a broader nutritional surveillance and/or health monitoring system or periodic national health surveys
Yes To Some degree No
Summarize the situation and Find out gaps and suggest recommendations for action
- IYCF- Not exits
- MIS- Data Collected to some extend- But no intervention
- Strong Monitoring Unit
- Regular publication system of surveillance report

25
Conclusion
The status of Infant and Young Child Feeding in Bangladesh is depicted in the report.
Bangladesh is progressing in the area of IYCF. In fact, Bangladesh has started the IYCF
activities timely and is in a leading position compared to many other developing
countries. At the same time, we have many indicators to improve to reach MDG.
Background data shows the achievement of the country in reducing IMR, U5 MR. There
is definite improvement in different indicators like exclusive BF, Continued BF rates. Still
there are many areas where we need more effort, strategic planning and concerted
action by government and NGOs.
APPAR toolkit is a useful instrument to assess country status on IYCF. Use of this
simple instrument in a highly participatory manner involving all stakeholders helps in
obtaining authentic data in a short time, and this participatory process helps in ensuring
a sense ofbelongingness to the IYCF programmes and helps in development of feasible
action plan.
Recommendation:
• Exercise every year with prior planning
• Monitor throughout the year
• Try to gather updated data throughout the year
• Maintain regular communication with the stakeholders
• Try to develop a formal mechanism of APPAR exercise at govt./official level and
develop govt. approved data sheet every year. It will help govt. assess, analyze
and take appropriate action. It will authenticate any country data, which will go to
the WEB

26
Annex A
Participants list Sl. No.
Name & Designation Organization Phone
1. Md. Abul Quashem, Executive Director
NNP 8629934
2. Dr. S.K. Roy ICDDR,B 0171849558 3. Prof. Soofia Khatoon ICHM 4. Dr. M Q Hassan ICMH 0189 234 018 5. Dr. T.M. Alamgir Azad Plan Bangladesh 6. Dr. A. N. Md. Gainal Abed IST, DGHS 015236422, 9898938 7. Dr. S M Mustafizur Rahman NNP 0171056953 8. Dr. Afsaruzzaman NNP 8652707, 0178-322798 9. Ms. Sohana Shafique Helen Keller International 0176323979 10. Dr. Md. Abdul Jalil MIS, DGHS 9899163 11. Dr. S.K Razzaque NICVD, Dhaka 9665564, 0152314586 12. Dr. Md. Nurul Haque Mollah DGHS 9899088 13. Dr. Ismat Ara IPHN 8017704, 0189-288-235 14. Dr. Rezaul Haque AD-DIN 0171827907, 9353391-93 15. Ms. Shahara Banu Kona ICDDR,B 0152-368640 16. Dr. Md. Nazmul Islam Primary Health, DGHS 0171477121, 9860680 17. Dr. Meherunessa Masood 8111567, 0173008116 18. Ms. Barnali Chakraborty ICDDR,B 011022812 19. Dr. Rabeya Khatoon WHO 011804127 20. Dr. Md. Bariul Islam Reproductive Health DGHS 9860680, 0187519173 21. Dr. G.U. Ahsan IST TTU, DGHS 0175005324, 9898934 22. Dr. Nurul Islam EPI Coordinator 0176-554638 23. Dr. Md. Mizanur Rahman BAN EHAOOL 9889694, 0187-526904 24. Dr. Syeeda Begum UNICEF 0173030513,
9336701, 461 25. Dr. Iqbal Kabir ICDDR,B 8151066 26. Dr. Rowshan Ara NASP, DGHS 0173036846 27. Dr. M A Rahman MCHTI, Azimpur, DGFP 0171106731 28. Dr. AZM Abul Fazal IST, DGHS 0171234600 29. Ms. Shaheen Sultana,
Coordinator BBF 0171592944
30. Ms Syeda Khaleda Begum Asstt. Coordinator
BBF
31. A M. M Samsad Asst. Coordinator
BBF
32. Md. Nuruzzaman Asst. Coordinator
BBF
33. Ms. Labin Rahman Asst. Coordinator
BBF
Annex B

27
Data on Exclusive Breastfeeding rate and Complementary feeding starting rate compiled from different sources Exclusive Breastfeeding rate 25.6% Complementary Feeding started: 19.6% at 5 months, 12.6% at 6 months and 32.5% beyond 6 months Source: Surveillance on Breastfeeding By Bangladesh Breastfeeding Foundation (BBF) July 2005 Average Exclusive Breastfeeding rate 19.63% 4-5 months of age in six divisions of Bangladesh (n=415) Average Complementary Feeding started 87.78% 6-11 months in six divisions of Bangladesh 2004 Annual Report of the Nutritional Surveillance By IPHN & HKI Exclusive Breastfeeding rate 21.3% 4-5 months and 4.8% 6-7 months Complementary Feeding started 23.8% 4-5 months 60.1% 6-7 months Bangladesh Demographic and Health Survey (BDHS) 2004 By NIPORT

28

29
Annex C : Sample of APPAR Toolkit table
[Frame1] Top of Form
0 Bangladesh 1994 Bangladesh 1996 Bangladesh
2000 Bangladesh 2001 Bangladesh 2003
Country Name
Year Score
1 Score
2 Score
3 Score
4 Score
5 Part I Total
Score 6
Score 7
Score 8
Score 9
Score 10
Score 11
Score 12
Score 13
Score 14
Score 15
Part II Total
Total
Bangladesh 1994 N/A 54.0* N/A N/A N/A 0.0 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Bangladesh 1996 N/A 51.0* N/A N/A N/A 0.0 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Bangladesh 2000 N/A 53.0* N/A N/A N/A 0.0 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
Bangladesh 2001 N/A 46.0 N/A N/A N/A 5.0 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A 5.0
Bangladesh 2003 N/A 46.0 N/A N/A 78.0 10.0 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A 10.0
* = Data is for exclusive breastfeeding upto 4 months instead of upto 6 months and hence cannot be scored/coloured/analysed by the toolkit

30
Executive Summary Introduction Process/Method Workshop output Assessment Draft Action Plan Future plan Conclusion Output: IYCF has been clarified among relevant govt. and NGO officials. They have appreciated the initiative. There was a good discussion on various issues related to IYCF. It has improved our awareness and will help in developing Action plan. The important stakeholders felt comfortable in coming to a common platform with facilitation from BBF. Future plan: To involve more stakeholders. To expand the methodology of data gathering and ensuring participation, obtaining contribution and making authentic data sheet. Concern: Question may arise on Government approval. We need to make a simple mechanism to get Government approval on the gathered data so that it can be disseminated in world forum like IBFAN ASIA web. Conclusion: APPAR toolkit is a useful instrument to assess country status on IYCF. Use of this simple instrument in a highly participatory manner involving all stakeholders helps in obtaining authentic data in a short time, and this participatory process helps in ensuring belongingness to the IYCF programmes and helps in development of feasible action plan. Summary findings: Bangladesh is progressing in the area of IYCF. In fact, Bangladesh has started the IYCF activities timely and is in a leading position compared to many other developing countries. At the same time, we have many indicators to improve to reach the MDG. Recommendation:
� Exercise every year with prior planning � Monitor throughout the year � Try to gather updated data throughout the year � Maintain regular communication with the stakeholders � Try to develop a formal mechanism of APPAR exercise at
Government/official level and develop Government approved data sheet every year. It will help Government assess, analyze and take appropriate action. It will authenticate any country data which will go to the WEB.
� Disseminate the assessment result among stakeholders. Stimulate them to take action plan based on the findings.
31