Balance: Decreasing Fall Risk
48
Balance: Decreasing Fall Risk Presented By: Jennifer Bell, MSPT, DPT Contributors: Katie Aakre, DPT; Patty Carroll, OTR/L
Transcript of Balance: Decreasing Fall Risk

Balance:Decreasing Fall Risk
Presented By: Jennifer Bell, MSPT, DPT
Contributors: Katie Aakre, DPT; Patty Carroll, OTR/L

Presentation Objectives
• Identify factors that increase risk of falling
• Understand the role of the musculoskeletal, neurological, and vestibular systems in balance
• Understand how to screen for falls risk
• Understand how to improve balance

Facts & Statistics
• Falls are a major public health concern
• Falls are a leading cause of injury related death and non-fatal injury in the U.S.
• According to the CDC, each year three million older people are treated for fall injuries in emergency departments
• One out of five falls causes a serious injury including broken bone or head injury
• Less than half of people who fall tell their doctor

Falls are costly!
• 40% of all nursing home admissions are in some way related to fall (Tinetti, 1988)
• The average cost per fall is >$30,000!
• Direct medical costs for fall injuries totals >$28 billion annually • Medicaid and Medicare are responsible for the majority of these costs

Falls and hip fractures
• Each year, over 300,000 older people (>65 years old) are hospitalized for hip fractures
• 25-50% of those who sustain a hip fracture from a fall die within one year
• More than 95% of hip fractures are caused by falling, usually by falling sideways
• Women experience three-quarters of all hip fractures• Women fall more often than men
• Osteoporosis

How do you define a “fall”?
• According to CMS, a fall is “an episode where a person lost his/her balance, and would have fallen, were it not for staff intervention”• Injury is not a factor in the determination of a fall
• Many patients do not report falls because they don’t sustain injury
• According to the WHO, a fall is “defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level”
• According to the American Nurses Association, “a patient fall is an unplanned descent to the floor”

What increases fall risk for our patients?
• Musculoskeletal impairments
• Age
• Cognition
• Pain
• Neurological problems
• History of stroke, TBI, Parkinson’s Disease, MS
• Environmental factors
• Outdoor hazards
• Hazards in the home
• Medication considerations
• Orthostatic hypotension
• Vision problems
• Vestibular Dysfunction

Musculoskeletal impairments
• ROM
• Strength
• Gait
• Impaired somatosensory system

Musculoskeletal impairments: ROM
• Patients need adequate ROM in ankle, hip and trunk for postural adjustments to prevent a fall• Ex: need at least 5-10 degrees of ankle dorsiflexion for “ankle strategy”
• Decreased ROM of the spine and increased kyphosis can lead to a stooped posture
• Loss of spinal flexibility can also contribute to a shift in center of mass
• Arthritis

Musculoskeletal impairments: strength
• Patient’s need sufficient strength to produce a force strong enough to correct a perturbation
• Muscle strength is directly proportional to gait velocity (Bendall et al. 1989)
• Muscles active during stance: • Gastroc/soleus, and tibialis anterior
• Gluteus medius, and TFL
• Iliopsoas
• Erector spine and abdominals

Musculoskeletal impairments: changes in gait
• Gait speed declines with aging • Decreased power
• Impaired balance
• Gait pattern changes • Shortened stride and step length
• More time in stance phase
• Hips slightly flexed
• “Toe out” foot position
• Widened BOS
• Poor plantar flexion power in terminal stance
(Judge et al. 1996)

Musculoskeletal impairments: somatosensory system
• Arises from muscle, joint, skin, fascia
• Gives us conscious perception of pressure, pain, touch, movement, position
• Constantly active, providing input to the soles of the feet
• This contributes to postural reactions • Ex: center of mass is displaced forward and plantar flexors activate

Postural reactions and anticipatory control
• Anticipatory control: patient’s ability to prepare for displacement• Influenced by experience, practice, knowledge of physical restraints
• Muscles “prepare” before actual movement occurs
• Muscle groups work in synergy as a unit to recover stability after center of mass is displaced to produce a postural reaction

Postural reactions
• Postural reactions• Ankle strategy
• Initial strategy
• Forward fall: gastrocnemius, hamstrings, paraspinals
• Backwards fall: anterior tibialis, quadriceps, abdominals
• Hip strategy• Larger perturbations
• Forward fall: abdominals, quadriceps
• Backwards fall: paraspinals, hamstrings
• Stepping strategy • Final strategy
• Very strong perturbation
• Center of mass is outside base of support

Sensory strategies
• On different surfaces, our body relies on different systems to allow us to balance • On a firm surface
• 70% somatosensory system
• 20% vestibular system
• 10% visual system
• On an unstable surface
• 60% vestibular system
• 30% visual system
• 10% somatosensory system

Dementia and memory loss
• Independent risk factor for falling
• Impaired judgement, gait, visual-spatial perception, and ability to avoid and recognize hazards
• In one study, the fall rate for residents in a nursing home with dementia was 4.05 falls per year, compared with 2.33 falls per year for residents without dementia
(Van Doorn et al. 2003)

Neurological Problems
Parkinson’s Disease
Multiple Sclerosis
Neuropathy
Stroke
TBI

Neurological impairments: Parkinson’s Disease
• Postural instability
• Typically in later stages
• Causes a forward or backwards lean - stooped posture
• Anticipatory postural adjustments are impaired or absent
• Most commonly in posterior direction
• Bradykinesia
• Slowing of movement
• Increased reaction time
• Gait difficulties
• “Freezing”
• Festination Image credit: The Dana Foundation, dana.org

Neurological impairments: multiple sclerosis
• Weakness due to deconditioning or damage to nerves
• Fatigue
• Spasticity • More common in legs, but can occur in any limb
• Vision problems such as blurred vision
• Numbness/tingling in extremities

Neurological impairments: peripheral neuropathy
• Damage to the peripheral nervous system
• Sensory nerves
• Numbness
• Tingling
• Motor nerves
• Weakness
• Muscle spasms
• Muscle atrophy
Image credit: Living with Diabetes. Diabetes.org.
• Diabetes
• Kidney failure
• Small vessel disease
• Infection
• Cancer
• Genetic diseases
• Exposure to toxins
• Autoimmune conditions• RA, Sjogren’s, lupus, MS,
CIDP, Guillain-Barre

Neurological impairments: stroke
• Falls is one of the most common complications of stroke
• Prevention of falls is one of the most important factors in recovery of independent ADL’s
• Reduced muscle tone
• Paralysis
• Impaired dynamic balance
• Patients with hemiplegia > hemiparesis are at higher risk for falls
(Tsur, 2010)

Neurological impairments: traumatic brain injury
• Acute brain injury• Mild TBI and concussion
• Post concussion symptoms: headache, fatigue, anxiety, nausea, emotional lability, cognitive problems
• Between 40-80% of individuals exposed to mild head injury experience some post concussion symptoms. Most recover within days to weeks, and about 10-15% have complaints after one year
• Chronic brain injury• Repetitive head trauma
• Catastrophic brain injury • acute severe brain injury
• Intracranial bleeding or cerebral contusions
• Balance, vestibular, and visual impairments(Blennow et al. 2012)
Image credit: Sports concussion. UCLAhealth.org

Environmental Factors-Home Modification
• Keep pathways clear and be aware of where your are
walking including uneven surfaces
• Get rid of all rugs
• Keep frequently used items close by
• Light your way
• Add supports to the bathroom
• Stay safe on the stairs
(Fall Prevention Center of Excellence, 2012)

Preventing Medication Related Falls
• Common medications for the following health problems may increase fall risk:• Heart and blood pressure
• Sleep, anxiety and depression
• Dementia symptoms
• Arthritis and pain
• Bladder control
• Digestive, stomach and nausea
• Blood Clots
• Colds, flu and allergies
Medication Side Effects that
Increase Fall Risk:• Dizziness
• Orthostatic hypotension
• Slow response to loss of balance
• Loss of concentration
• Decreased alertness, drowsiness
• Blurred vision(Fall Prevention Center of Excellence, 2012)

Vision Loss and Fall Risk
• Effects of vision loss• Difficulty with balance
• Difficulty seeing obstacles
• Difficulty seeing steps/curbs
• Reduced activity resulting in decreased strength
• Individuals with vision problems are more than twice as likely
to fall as people without vision problems. (Fall Prevention Center of Excellence, 2012)

The Vestibular System and Balance
• To maintain balance, information from the vestibular, visual and somatosensory systems are integrated within the central nervous system.
• The vestibular system is a primary contributor to equilibrium as it references where our head is in space.
• Vision and somatosensory are references that tell our brain about the world outside.
• When there is a conflict between these references, the result is the brain’s inaccurate perception or hallucination of motion (vertigo). This can result in a loss of balance or a fall
• The vestibular system can be damaged by disease, aging, poisoning by drugs, or injury. Many vestibular disorders occur from unexplained causes.

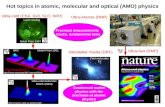
Vestibular anatomy
• The vestibular system consists of a peripheral and a central portion
• Peripheral - includes a labyrinth that is lined with hair cells(cilia) and is filled with fluid. Head motion causes the fluid to move. The moving fluid bends the cilia and this leads to neural firing of the vestibular nerve
• Central – includes the brain and brainstem. The central vestibular system process all the balance and spatial information coming in
Image credit: anatomy of vestibular system. anatomysciences.com

Vestibular Facts
• 80% of individuals aged >65 years have experienced dizziness and BPPV (benign positional paroxysmal vertigo).
• Vestibular disorders are difficult to diagnose. It is common to seek care from several providers over a period of many years before receiving an accurate diagnosis.
• There is no cure for most vestibular disorders. They can be treated with therapy, medication, surgery and life style changes.

Common symptoms of vestibular dysfunction
• Dizziness and Vertigo
• Nausea/vomiting
• Imbalance
• Spatial disorientation
• Vision disturbance
• Hearing changes
• Cognitive and/or psychological changes
• Other-tinnitus, fatigue, anxiety

Screening for balance and falls risk
• In physical therapy, we use a variety of different balance tests and measures depending on patient function
• Examples commonly used in outpatient:• Timed Up and Go (TUG)• 30 second sit to stand • Gait speed• 4 square step test • Functional reach test• Tinetti• mCTSIB• Berg Balance Assessment• Dynamic gait index• Functional gait index• HiMat• Mini-BESTest• 6 Minute Walk Test

Tests covered today
1. Timed get up and go
2. 30 second chair stand test
3. Gait speed 10 M walk test

Timed Get Up and Go Test
• Purpose: quick screening tool to measure functional mobility in community dwelling adults (Podsiadlo, 1991)
• Task: Patient is instructed to rise from a chair, ambulate 3 meters (10 feet), turn 180 degrees, ambulate back to the chair and return to sitting
• Equipment• Marked line at 10 feet• Standard chair• Watch
• Assistive device is optional
• 3 timed trials taken• 1 practice• 2 timed trials, average taken

Timed Get Up and Go
• Predictive validity:• ≤10-12 seconds = normal
• >13.5 seconds indicative of falls risk
• ≥20 seconds indicative of frail for functional independence
• >30 seconds indicative of dependence (Boulgarides, 2003)
• Other variations for dual task: • TUG Motor
• Carry a cup of water
• TUG Cognitive • Counting backwards by 3’s from 100

The 30-Second Chair Stand Test
• Purpose: to assess leg strength and endurance
• Task: • Patient is instructed to sit in the middle of the chair with arms crossed to
opposite shoulder, feet flat on the floor, back straight
• On “Go”, patient rises to full standing and back to sitting
• Repeated for 30 seconds
• Equipment• Standard chair
• Watch

The 30-Second Chair Stand Test
• Patient can be allowed a warm-up trial for correct form
• If patient cannot stand without use of arms, stop the test• Score of 0
• Allowed to repeat test using upper extremity support on standard chair
• Below average score indicates high falls risk
Image credit: physical measures. Duke.edu.

Chair stand average scores
Age Men Women
60-64 <14 <12
65-69 <12 <11
70-74 <12 <10
75-79 <11 <10
80-84 <10 <9
85-89 <8 <8
90-94 <7 <4
(Center for Disease Control)

Gait Speed
• Can be assessed quickly and accurately
• Improvements in walking speed can be linked to clinical meaningful changes in quality of life
• Easy to use as a predictor and outcome measure for many diagnoses
• “The 6th vital sign”
• Not a measure of endurance

Gait Speed: 10 meter walk test
• Purpose: to identify risk for falls
• Task: patient is asked to “walk at your normal, comfortable speed” over a 10 meter distance• Middle 6 meters is timed
• Equipment: 20 m path, stop watch
• Can also test for maximum walking speed, “walk as fast as you can”• With increased age, maximum gait speed declines more steeply than
comfortable gait speed (Bohannon et al. 1997)

Gait Speed: 10 meter walk test
Image credit: gait speed.Dovepress.com

Gait speed norms for health populations
Age Comfortable Mean
(m/s)
Fast Mean
(m/s)
60-69 1.44 female ±.25
1.59 male ± .24
1.87 female ± .30
2.05 male ± .31
70-79 1.32 female ± .23
1.38 male ± .23
1.71 female ± .26
1.83 male ± .44
80-89 1.15 female ± .21
1.21 male ± .18
1.59 female ± .28
1.65 male ± .24
(Steffen et al. 2002)

What can we do ??
• Refer to Rehab for strengthening, Gait, ROM, Assistive device or vestibular rehabilitation
• Consider medication factors
• Suggest home modification
• Consider vision factors

Multifactorial interventions
• Tinetti et al. studied 301 men and women age >70 living in the community who had at least one risk factor for falling• Intervention group: adjustments in medication, behavioral instructions, and
exercise programs aimed at modifying risk factor
• Control group: usual health care plus social visits
• During 1 year follow up, 35% of intervention group fell as compared to 47% control group• Significant reduction in risk for falling
• Total cost of the intervention was an average of $891 per subject
• The cost for preventing one fall that required medical attention was $12,392

Examples of rehab interventions
• Assistive device assessment and training
• Gait training
• Transfer training
• Recommendations for grab bars or railings
• Aerobic exercise
• Strengthening program
• Balance program

HealthEast Optimum Rehabilitation
We’re here to help!
• Come see us for physical or occupational therapy

Questions???Please feel free to contact me with any questions
Jennifer Bell, MSPT, DPT
651-232-0496 – or – [email protected]

Thank You!

References
1. Bendall, M. J., et al. “Factors Affecting Walking Speed of Elderly People.” Age and Ageing, vol. 18, no. 5, 18 Sept. 1989, pp. 327–332., doi:10.1093/ageing/18.5.327.
2. Blennow, Kaj, et al. “The Neuropathology and Neurobiology of Traumatic Brain Injury .” Neuron, vol. 76, no. 5, 6 Dec. 2012.
3. Bohannon, R. W. “Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants." Age Ageing. 1997;26(1): 15-9.
4. Boulgarides, Lois K, et al. “Use of Clinical and Impairment Based-Tests to Predict Falls by Community-Dwelling Older Adults.” Physical Therapy, vol. 88, no. 4, 2003.
5. HealthEast Falls Handouts, Fall Prevention Coalition Los Angeles, August 2018. www.stopfalls.org/coalitions-networks/fpc-la/
6. “Hip Fractures Among Older Adults.” Centers for Disease Control and Prevention, CDC Injury Center, Sept. 2016, www.cdc.gov/homeandrecreationalsafety/falls/adulthipfx.html
7. “Important Facts about Falls.” Centers for Disease Control and Prevention, CDC Injury Center, Oct. 2017, www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html.
8. Judge, J O, et al. “Effects of Age on Biomechanics and Physiology of Gait.” Effects of Age on Biomechanics and Physiology of Gait, vol. 12, no. 4, 1 Nov. 1996.
9. Kihun, Cho, et al. “Risk Factors Related to Falling in Stroke Patients: a Cross-Sectional Study. ” Journal of Physical Therapy Science, vol. 27, 2015, pp. 1751–1753.
10. Koveleski Kraut, Sara. “Evidence-Based Rehab Techniques for Parkinson's Disease, Multiple Sclerosis and Peripheral Neuropathy.” North American Seminars, 2016.
11. O'Sullivan, Susan B, and Thomas J Schmitz. Physical Rehabilitation. 5th ed., F.A Davis, 2007.
12. Podsiadlo D, Richardson S. The timed “Up and Go”. A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society 1991; 39: 142-148.
13. “STEADI Materials for Healthcare Providers.” STEADI - Older Adult Fall Prevention , Centers for Disease Control and Prevention, 2017, www.cdc.gov/steadi/materials.html.
14. Steffen, Teresa M, et al. “Age- and Gender-Related Test Performance in Community-Dwelling Elderly People: Six Minute Walk Test, Berg Balance Scale, Timed up & Go Test, and Gait Speed.” Physical Therapy, vol. 82, no. 2, Feb. 2002.
15. Tinetti, Mary E, et al. “Risk Factors for Falls among Elderly Persons Living in the Community.” The New Englad Journal of Medicine, vol. 319, Dec. 1988.
16. Tsur, A, and Z Segal. “Falls in Stroke Patients: Risk Factors and Risk Management.” Israel Medical Association , no. 4, Apr. 2010, pp. 216–219.
17. Van Doorn, Carol, et al. “Dementia as a Risk Factor for Falls and Fall Injuries among Nursing Home Residents.” Journal of American Geriatrics Society, vol. 51, 2003, pp. 1213–1218.
18. “Top Ten Facts About Vestibular Disorders.” Vestibular Disorder Association, August 2018, www.vestibular.org/understanding-vestibular-disorder

• HealthEast Care System is an approved provider of continuing nursing
education by the Wisconsin Nurses Association, an accredited approver by
the American Nurses Credentialing Center’s Commission on Accreditation.
• No conflict of interest in planning, writing, reviewing, or editing of this
program content was identified or discovered during the development of
the class. No conflicts exist of personal, professional, or financial nature.