Bad back in a person with diabetes
1
DIABETES V IGNETTE 182 Pract Diab Int June 2010 Vol. 27 No. 5 Copyright © 2010 John Wiley & Sons A 53-year-old female patient with a 13- year history of type 2 diabetes (HbA1c range 10.2–11.0% over the preceding two years) and chronic kidney disease stage 5 (eGFR 9–16ml/min/1.73 2 over the previous two years) was admitted with several days’ weakness of her right hand and severe mid-thoracic back pain. She was afebrile, but had a raised C-reactive protein (132mg/L). Magnetic resonance (MR) imaging of the spine (Figure 1) demonstrated discitis at the T6/T7 disc space with destruction of the adjacent vertebrae and heterogeneous material extending posteriorly into the spinal canal compressing the cord. Specialist management of her stage 4 chronic renal failure required transfer to a renal unit, although dialysis was not required. She was then transferred to a spinal unit and eventually required spinal fixation with interpedicular screws at T4/5 and T8/9 and rods. Despite surgery, compression of the spinal cord resulted in paraplegia. No organisms were grown from cultures of peripheral blood or tissue samples; this may be consequent to initial treatment for a presumed lower respiratory tract infection. Long-term broad spectrum antibiotics were pre- scribed empirically. Ten months later the patient was readmitted complaining of similar back pain, associated with a raised C-reactive protein but normal temperature and neutrophil count. Repeat MR demon- strated the previous discitis and metalwork, and a small fluid collection suspicious of an abscess in the remnant disc space. This was treated medically without further surgery. Discussion Diabetes has been described as a risk factor for septic discitis, 1,2 and septic discitis may progress more rapidly in patients with diabetes. Prompt imaging should be performed to clarify the diag- nosis, and early referral to a specialist unit is important to avoid the disastrous complication of spinal cord compres- sion. Tissue samples to guide anti- microbial therapy have a better yield than peripheral blood culture or needle biopsies, 3 and alter management strat- egy in around a third of patients. 4 It is felt that rapid institution of appro- priate antibiotics improves outcomes, but obviously this has not been subjected to randomised controlled trial. Difficulties arise in older patients. Firstly, back pain is very common, but increased pain should arouse susp- icion. Secondly, one can be misled by possible infection elsewhere; elderly folk often have a few basal crepitations on chest examination and 20% of elderly females have asymptomatic bacteriuria; one should be aware that these chest and urine infections might be red herrings. In diabetic patients presenting with signs of infection associated with back pain, septic discitis must be considered. R Parker, MRCP KO Hill, MRCP, MRes SCM Croxson*, MD, FRCP Departments of Diabetic and Geriatric Medicine, University Hospitals Bristol NHS Foundation Trust, Bristol Royal Infirmary, Bristol, UK *E-mail: [email protected] References 1. Hopkinson N, Stevenson, Benjamin S. A case ascertainment study in septic arthritis: clinical, microbiological and radiological features. Q J Med 2001; 94: 465–470. 2. Rath SA, Neff U, Schneider O, et al. Neurosurgical management of thoracic and lumbar vertebral osteomyelitis and discitis in adults: a review of 43 consecutive surgically treated patients. Neurosurgery 1996; 38(5): 926–933. 3. Luzzati R, Giacomazzi D, Danzi MC, et al. Diagnosis, management and outcome of clin- ically-suspected spinal infection. J Infect 2009; 58(4): 259–265. 4: Enoch DA, Cargill JS, Laing R, et al. Value of CT-guided biopsy in the diagnosis of septic discitis. J Clin Pathol 2008; 61: 750–753. Diabetes Vignette Bad back in a person with diabetes Practical Diabetes International invites you to submit your favourite slide with clinical details for possible publication in this series. Figure 1. MRI thoracic spine (T2 weighted sequence); the grossly abnormal T6/7 disc is arrowed CONFERENCE NOTICE Meeting the quality and productivity challenge in diabetes Tuesday 8 June 2010, 76 Portland Place, London Topics include: The National Service Framework for Diabetes: six years on. Improving care for children and young people with diabetes. A nurse led approach to diabetes care: care planning in long term conditions. Screening for early diagnosis and identification of diabetes. CPD accredited by the Royal College of Physicians, London and the Royal College of Nursing. Contact: Matt at Healthcare Events, e-mail: [email protected], tel: 020 8541 1399, website: www.healthcare-events.co.uk
Transcript of Bad back in a person with diabetes

DIABETES VIGNETTE
182 Pract Diab Int June 2010 Vol. 27 No. 5 Copyright © 2010 John Wiley & Sons
A 53-year-old female patient with a 13-year history of type 2 diabetes (HbA1c
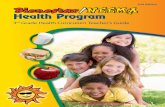
range 10.2–11.0% over the preceding two years) and chronic kidney diseasestage 5 (eGFR 9–16ml/min/1.732 over theprevious two years) was admitted withseveral days’ weakness of her right hand and severe mid-thoracic back pain.She was afebrile, but had a raised C-reactive protein (132mg/L). Magneticresonance (MR) imaging of the spine(Figure 1) demonstrated discitis at theT6/T7 disc space with destruction of theadjacent vertebrae and heterogeneousmaterial extending posteriorly into thespinal canal compressing the cord.Specialist management of her stage 4chronic renal failure required transfer to arenal unit, although dialysis was notrequired. She was then transferred to aspinal unit and eventually required spinalfixation with interpedicular screws at T4/5and T8/9 and rods. Despite surgery, compression of the spinal cord resulted in paraplegia. No organisms were grownfrom cultures of peripheral blood or tissue samples; this may be consequentto initial treatment for a presumed lowerrespiratory tract infection. Long-termbroad spectrum antibiotics were pre-scribed empirically.
Ten months later the patient wasreadmitted complaining of similar backpain, associated with a raised C-reactiveprotein but normal temperature and neutrophil count. Repeat MR demon-strated the previous discitis and metalwork, and a small fluid collectionsuspicious of an abscess in the remnantdisc space. This was treated medicallywithout further surgery.
DiscussionDiabetes has been described as a riskfactor for septic discitis,1,2 and septicdiscitis may progress more rapidly inpatients with diabetes. Prompt imagingshould be performed to clarify the diag-nosis, and early referral to a specialistunit is important to avoid the disastrouscomplication of spinal cord compres-sion. Tissue samples to guide anti -microbial therapy have a better yieldthan peripheral blood culture or needlebiopsies,3 and alter management strat-egy in around a third of patients.4
It is felt that rapid institution of appro-priate antibiotics improves outcomes, butobviously this has not been subjected torandomised controlled trial.
Difficulties arise in older patients.Firstly, back pain is very common, butincreased pain should arouse susp -icion. Secondly, one can be misled bypossible infection elsewhere; elderlyfolk often have a few basal crepitationson chest examination and 20% of elderly females have asymptomaticbacteriuria; one should be aware thatthese chest and urine infections mightbe red herrings.
In diabetic patients presenting withsigns of infection associated with back pain, septic discitis must be considered.
R Parker, MRCPKO Hill, MRCP, MResSCM Croxson*, MD, FRCPDepartments of Diabetic and GeriatricMedicine, University Hospitals BristolNHS Foundation Trust, Bristol RoyalInfirmary, Bristol, UK*E-mail: [email protected]
References1. Hopkinson N, Stevenson, Benjamin S. A
case ascertainment study in septic arthritis: clinical, microbiological and radiological features. Q J Med 2001; 94:465–470.
2. Rath SA, Neff U, Schneider O, et al.Neurosurgical management of thoracic andlumbar vertebral osteomyelitis and discitis inadults: a review of 43 consecutive surgicallytreated patients. Neurosurgery 1996; 38(5):926–933.
3. Luzzati R, Giacomazzi D, Danzi MC, et al.Diagnosis, management and outcome of clin-ically-suspected spinal infection. J Infect2009; 58(4): 259–265.
4: Enoch DA, Cargill JS, Laing R, et al. Value of CT-guided biopsy in the diagnosis of septic discitis. J Clin Pathol 2008; 61:750–753.
Diabetes VignetteBad back in a person with diabetes
Practical Diabetes International invites you to submit your favourite slide with clinical details for possible publication in this series.
Figure 1. MRI thoracic spine (T2weighted sequence); the grosslyabnormal T6/7 disc is arrowed
CONFERENCE NOTICE
Meeting the quality and productivity challenge in diabetesTuesday 8 June 2010, 76 Portland Place, LondonTopics include: The National Service Framework for Diabetes: six years on. Improving care for children and youngpeople with diabetes. A nurse led approach to diabetes care: care planning in long term conditions. Screening for earlydiagnosis and identification of diabetes.CPD accredited by the Royal College of Physicians, London and the Royal College of Nursing. Contact: Matt at Healthcare Events, e-mail: [email protected], tel: 020 8541 1399, website: www.healthcare-events.co.uk