Specialized Nutrition Support: Enteral & Parenteral Nutrition

Back to the Basic: Parenteral Nutrition 101
Osama Tabbara

Disclosure Information
Back to the Basic: Parenteral Nutrition 101
Osama Tabbara
• I have no financial relationship to disclose.
AND
• I will not discuss off label use and/or investigational use in my presentation.
OR
• I will discuss the following off label use and/or investigational use in my presentation

3.5 years in Operation
JCIA
HIMSS 7

CCAD
• 364-bed facility (Max 480)
• Five centers of excellence:• Heart and Vascular
• Neurology
• Digestive Diseases
• Ophthalmology
• Respiratory & Critical Care
• 300 Physicians
• 120 Pharmacy Caregivers
• 1000 Nurses
• Cleveland Clinic USA • #2 in USA
• #1 in Cardiology x 24 years

IVPN Experts Network - Gulf Region
•1251 IVPNeers from 400 hospitals

• At the completion of this activity, you will be able to:
• Apply the basic physiology and biochemistry knowledge in understanding PN
• Interpret the biochemical markers with PN therapy
• Utilize scenarios to describe the complications of PN
- List References here
Learning Objectives

Multiple Choice Question:
Which lab marker is not important to monitor with Protein therapy
• Liver Function Tests
• BUN
• Dextrose
• Albumin
Polling/ Assessment Questions

Multiple Choice Question:
As classified by ISMP, which of the following are high Alert medications
• IV Potassium
• Insulin
• Heparin
• All of the above
Polling/ Assessment Questions [For Workshops]

Multiple Choice Question:
As per 2003 Survey, major errors with PN are originated:
• Protein
• Lipid
• Electrolytes
• Trace elements
Polling/ Assessment Questions [For Workshops]

Background
• PN represents of the most notable achievements of modern medicine
• PN can serve as a therapeutic modality for all age groups across the
health care continuum
• PN offers life-sustaining option in intestinal failure patients
• PN is artificial, expensive and associated with serious adverse
events10

K
Na
PO4, K, Mg
Insulin
C
NF
Mitochondria
ATPCO2
Vitamins
Tr.Elem.

Na-K-ATPase pump
K(135-145mEq/L)
K(3.5-5mEq/L)
Na(3.5-5mEq/L)
Na(135-145mEq/L)
Intravascular
Intracellular
Interstitial
Albumin

Na+ 10 mmol/L
K+ 155 mmol/L
Mg++ 26 mmol/L
PO4 -- 100 mmol/L
Protein 65 mmol/L
Na+ 142 mmol/L
K+ 4 mmol/L
Mg++ 1 mmol/L
PO4-- 1 mmol/L
Protein-- 16 mmol/L
IntravascularIntracellullar
3.5 L 30 L 10 L
Electrolyte Distribution

Dextrose
(100mg/dl)
(0.1%)
K:
60 mMol/L
K(3.5 – 5 mMol/L)
Dextrose
20%
SERUM PN

TPN replaced with PN:•PPN•CPN
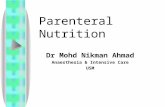
Parenteral Nutrition

Central or Peripheral PN?

• Iso-Osmolar
• Physiological pH
• Sterile
What is Safe Admixture?

• SVC = 2000 ml/min
• SCV= 800ml/min
• Cephalic/Basilic: 40-95ml/min

• Partial support
• Phlebitis
• No surgery
• Low risk Sepsis
• Max Dextrose
• Neonate: 12.5%
• Peds: 10%
• Adult: 7.5%
• Max Protein: 2.5%
• Max osmolarity: 900/L
• Full support
• No Phlebitis
• Surgery
• Sepsis
• No Max for Dextrose
• No max for Protein
• No max osmolarity
PERIPHERAL CENTRAL

No limit with CPN
Maximum Dextrose with PPN:7.5 - 12.5% in neonates
Maximum Osmolarity with PPN:900 - 1100 mOsm/L
What is Maximum Dextrose % and Osmolarity?

Central or Peripheral PN?
• Adel c/o severe pain at injection site; Phlebitis!
• RN called R.Ph. and asked if she can reduce the rate from 80ml to 40ml/hour to reduce venous intolerance!
• Does rate reduction reduce venous intolerance?
• NO!!!
• It is not the rate, it is the components!
• Hold PN and replace with D5W at same rate of PN

Considerations for Vascular Access for PPN
• Extravasation of nutrients can lead to tissue injury and
necrosis
• Risk Factors for Vascular Access
• Obesity
• Extremes in age (neonates and elderly)
• History of multiple venous cannulations
• History of IV drug use
Worthington P. JPEN, 2017;41:324-377

What is Phlebitis?
• Inflammation of vein (typically
endothelial cells)
• Most common causes:• High Osmolarity of IV solution
• Traumatic IV Placement
• Prolonged use of IV Site

Signs of Phlebitis
• Redness of the vein
• Swelling of the vein
• Tenderness over the vein
• Site warm to touch
• Sluggish flow of infusate

Preventing Peripheral PN Complications

• Maximum dextrose = 12.5%
• Maximum Protein = 2.5%
• Calculate final osmolarity (< 1100 mOsm/L)
• Minimize Na, K, Ca
• Add Heparin and Hydrocortisone
• Re-site the veins q 24-48 hours
• Maximize IV LIPID
Preventing Peripheral PN Complications

• Protect veins from phlebitis
• Safe at any dose with PPN
IV Lipid is Safe!

Scenario #1 Peripheral PN
• Mona is a 54-yr-old female, cachexia, severely malnourished
• Dx: Partial Esophageal Obstruction
• Can drink limited volume of oral formula
• PPN to be started
• Poor peripheral veins
QUESTION:
• How can we reduce the chance of phlebitis?

Phlebitis Prevention
• Frequent site changes
• Filter
• Hydrocortisone 6mg/L
• Heparin 1unit/ml
• Less K
• Less Ca
• Extra IV lipid
Tighe MJ., et al., JPEN 19:507-509, 1995Anderson ADG., et al. Brit J Surg 90:1048-1054, 2003Isaacs JW. et al., AJCN 30(4):552-9, 1977Tighe MJ., et al., JPEN 19:507-509, 1995

Peripheral PN
• No standard Patient = No standard Osmolarity.
• To program your software, use a max of 1100 mOsm/L.
• If your patient is osteopenic, don’t go with peripheral PN.
• If a patient is severely hypokalemic, consider central line.
• Consider Heparin 0.5 -1 unit/ml with Peripheral PN unless contraindicated.
• Less Sodium, Less K, Less Ca with PN means better tolerance of peripheral PN.
• “Outside ICU, PPN is the choice for short courses with early PO/NG feeding”

How Much Calories?

The Science and Art of PN
FEED AS TOLERATED

“ A total caloric intake of 25 Kcal/kg usual body
weight per day appears to be adequate for
ALL patients”
Cerra FB, et al. “Applied nutrition in ICU patients: A consensus
Statement of ACCP”. Chest 1997 111:769-777
ACCP Recommendation

• 11-14 Kcal/kg actual BW • or 22-25 Kcal/kg IBW/d
• Protein at 2-2.5 g/kg IBW/d
SCCM & ASPEN Guidelines, Crit Care Med, 37(5), 2009
How Much Calories for Obese ICU Pts. (BMI > 30)?

Chwals WJ. New Horiz 2:147-155, 1994
Clein CG. Et al., J Am Diet Assoc 98:795-806, 1998
“Underfeeding is safer than overfeeding.”

• RQ = VCO2/ VO2
• Dextrose = 1
• Protein = 0.8
• Fat = 0.7
• Liponeogenesis= 8
RQ > 1 : Overfeeding
RQ = 0.825: Ideal
RQ < 0.82: Underfeeding
Melinda S. et al. JPEN Vol23, No5, p300, 1999
Indirect Calorimetry

Dextrose

• Basal metabolic rateAdults: 2mg/kg/min (150g)
Pediatrics: 6mg/kg/min (6g/kg/d)
• 50-60% of total calories
• 1g = 3.4 Kcal
• Watch Refeeding Syndrome
Dextrose

2003 Survey of PN Practices ASPEN Task Force: Error Results
•Electrolytes: 69%
•Dextrose/insulin: 31%
•Fat Emulsion 26%
Seres D. et al., JPEN 2006; 30:259-265

• 12-yr-old male with chronic intractable diarrhea, severe dehydration, severe malnutrition, cachexic, hypoglycemic
• Wt = 15 kg
• Admitted to ER
• Rx: Dextrose 15% @ 100ml/hr
• Few hours after, admitted to PICU with myocardial infarction
• What was wrong?

How much dextrose in DW 15% at 100 ml/hr?
•360g
•16mg/kg/minute

• Hypophosphatemia
• Myocardial ischemia
• Respiratory arrest
• Hypokalemia
• Arrythmia
Refeeding Syndrome

• Advance TPN gradually
• Increase K, Mg, PO4
• Minimize Na
• Extra Vitamins and Trace Elements
• Daily lab
Crook MA. et al., Nutrition 17:632, 2001
Solomon S. JPEN 14(1):90-97,1990
Marek PE. et al., Arch Surg 124:1325, 1996
Refeeding Syndrome: Prevention

• K: Up to 16 mMol/kg/day
• PO4: Up to 4 mMol/kg/day
• Mg: Up to 2 mMol/kg/day
Tabbara O., KFSHRC Refeeding Syndrome:
KFSHRC Experience

• Day 1: Start with 150g (2mg/kg/min)
• Day 2: increase by 50g every day up to 400 g/day
• Do not exceed 4mg/kg/minute
• More dextrose = more electrolytes
• Do not dose by concentration
Dextrose Dosing Guidelines

Dex 17% of 5 ml/hr
= 20.4gDex 18% of 4ml/hr
= 17.2g
Which Concentration Gives More Sugar per Day?

• BG
• Acid-Base
• LFTs
• Electrolytes
Monitor

• Avoid adding Insulin to PN bag
Safer PN

• Dex 20%
• AA 3g/kg/day
• K 4 mMol/kg/d
@ 6 ml/hr
• 9ml/hr of TPN = 50% extra of all nutrients + running out earlier
Catching-up Fluid with PN

• Abrupt discontinuation of PN
Common NICU PN Complication

Amino Acids

• Specialized formulas
• 10% of total calories
• 1g = 4 Kcal
Protein = Amino Acids

• Day 1: 0.7 g/kg/day
• Day 2: 1.2 g/kg/day
• Day 3: 1.5-2g/kg/day
Protein Dosing Guidelines

• BUN
• Acid-Base
• LFTs
• Albumin
Protein Tolerance Monitoring

Lipids

IVFE is a Good Media for Microbial Growth
Neutral pH of 8
Isotonic
High Fat content
•Substantial growth of E. coli, C. albicans, Ps. aeruginosa and coag-neg Staph spp.
• Flourished 12- 48 hrs post contamination
Keammerer D. et al., Am J Health Syst Pharm. 1983;40(10:1650-1653
Crill CM. et al., Am J Health Syst Pharm. 2010;67(11):914-918

• Concentrated source of calories
• 1g = 10 Kcal
• 20-40% of total calories
• Isotonic
• MCT: LCT / SMOF Lipid
Lipids

• Day 1: Start with 0.5 g/kg/day
• Day 2: 1 g/kg/day
• Day 3: 1.2 – 1.5 g/kg/day
• Do not exceed 0.15 g/kg/hour
• Better to be infused over 12 hours
IV Lipid Dosing Guidelines

• TG
• LFTs
• Platelets
Lipid Tolerance Monitoring

PN & Fat Allergy

Fat Allergy
4 different types:
1. Egg Phospholipid (Fat emulsifier)• Is patient allergic to eggs?
2. Soya Bean• Check with the patient if he/she ever had food allergy particularly to Soya bean.
3. Glycerine: to render IV isotonic• Check with the patient if he/she has any allergy to particular soaps, prepacked food, drugs containing
glycerine containing lozenges, laxatives, suppositories, etc.
4. MCT allergy• in case you use MCT:LCT. Check with the patient if she/he has peanut allergy.

PN Allergy
• Some AA products contain metabisulfite• Few reported allergic reactions
• Paraben preservatives in the product also may be associated with systemic reaction
• Multivitamins and trace elements could cause allergic reactions.
- Noura Albenyan, Mason Assaf

Interpretation of Lab Data

Treat the patient•Not only numbers
PN: What is Wrong & What
is Right?
What is Right?

10-y-old-female
Dx: Severe intractable diarrhea, severe dehydration
Start PN 80ml/hour
How much Na shall we add in PN?
Add 150 mMol/L + Close monitoring
Na 158 Cl 116 BUN 15 Glucose 90
K 4.9 CO2 20 Cr. 2.5 PO4 1.4
What is Right? Treat the Patient not the Numbers

10% of all cases: High intake of Na: NS, ABx, Albumin, etc.
Rx: D5W + Furosemide
90% of all cases: Volume depletion Fever, Hyperventilation, Sweating, GI losses
Symptoms: Thirst , Weight loss,
Signs: High BUN, Albumin, Hct
Rx: NS or D5 NS
What is Right About Hypernatremia?

• Eliminate Manganese and Copper with cholestasis
• ½ regular doses of TE
PN in Cholestasis

IV Lipid Dosing & Infusion Time

IVFE Dosing
Neonates & Infants:• 0.25 g/kg per day minimum to prevent EFAD• Maximum of 3–4 g/kg per day • (0.13–0.17 g/kg/hour) in infants
Term Infants & Older Children• 0.1 g/kg per day minimum to prevent EFAD• Maximum of 2–3 g/kg per day• 0.08-0.13g/kg/hour in older children.
Adults:• 0.1 g/kg/day minimum to prevent EFAD• Maximum of 1.5-2g/kg/day• 0.11 g/kg/hour for most cases and increase MAX to 0.15g/kg/hour

IV Fat Emulsion
•Absolute contraindication:•TG more than 4 mmol/L
•Acute Pancreatitis induced by Hypertriglyceridemia

Filtering Lipid

Shall we Filter IV Lipid
• Yes if manipulated
• No if original container is used.
• IVPN:
“1.22 micron filter with IV lipid infused with 2-in-1 only if the required volume is mixed/transferred and not to filter if we use the original Lipid bottle.”
http://www.nutritioncare.org/News/General_News/Parenteral_Nutrition_%E2%80%93_New_Recommendati
ons_for_In-line_Filters/

Shortage of 0.2 micron Filters
•Use 1.2 micron filters for 2-in 1 and TNA
- List References here

Case Scenario
POTASSIUM

“ Identified as the drug most commonly implicated in fatal incidents
in acute care facilities”
National Patient Safety Agency, UK, 2002Medication Safety Alerts, CJHP, Canada, 2002
Potassium

1.IV Potassium2.Insulin3.Heparin
USP/MedMarx 1996Institute of Safe Medication Practice (ISMP), 2003

78

• 14 yr-old male
• Dx: s/p BMT, complicated with GVHD, diarrhea, severe malnutrition
• On Ampho B, Furosemide, Steroids, Insulin
• PN day +4, 40 Kcal/kg/day, 2g protein/kg/d, Dextrose 4 mg/kg/min
Na 135(135-147)
Cl 101(98-111)
BUN 12(2.4 – 7)
Glucose 9(3-8)
K 2.1(3.5-5)
CO2 30(22-21)
Cr 44(44-123)
PO4 0.39 (0.7-1.45)
Mg 0.3 (0.7-1)
Potassium

Potassium
• 14 yr-old male
• Dx: s/p BMT, complicated with GVHD, diarrhea, severe malnutrition
• On Ampho B, Furosemide, Steroids, Insulin
• TPN day +4, 40 Kcal/kg/day, 2g protein/kg/d, Dextrose 4 mg/kg/min
• Why severe hypokalemia?
• How can we reduce potassium requirements?
Na 135(135-147)
Cl 101(98-111)
BUN 12(2.4 – 7)
Glucose 9(3-8)
K 2.1(3.5-5)
CO2 30(22-21)
Cr 44(44-123)
PO4 0.39 (0.7-1.45)
Mg 0.3 (0.7-1)

• Amphotericin B
• Insulin / Dextrose load
• Diuretics
• GI Loss
• Steroids / Salbutamol
• NPO
• Magnesium wasting drugs
• DKA
Why High K Requirement?

Investigate First then Add K
• Why hypokalemic?
• Symptomatic?
• Acute or chronic hypokalemia
• Lab error
• Check previous K level
• Kidney function?
• Central or peripheral?
• Magnesium level?
• Can take PO? Absorption?
• Need for a STAT order ?!!!

• Onset of hypokalemia with Ampho-B is 24-36 hours
• Increase K in IV empirically
• Reduce dextrose load!!

•Keep Magnesium levels between 0.9-1 mmol/dL
•Start Ranitidine with upper GI loss
How To Prevent Severe Hypokalemia?

Case Scenario
Hyponatremia

Hyponatremia
• 42-year-old lady admitted with Pneumonia
• PMH: Home PN due to SBS, Type II DM, HTN
• Dx?
• Should you increase Na in PN?

Factitious Hyponatremia
• Excess BG in serum:• ↑Serum Osmolarity
• Correct BG + NS + fluid restriction
• Excess BUN, Lipid:• Isotonic serum
• NS + fluid restriction

Sodium in PN
• Always ¼ to NS in PN
• PN is not the vehicle to correct severe hyponatremia (less than 120)

Scenario #2CPN or PPN?

Case Scenario: CPN
• Adel to start CPN, 2 liters:• Dextrose 8%• Amino Acid 3%• Sodium 80 mmol• Potassium 80 mmol• Ca 6 mmol
• Central line, through External Jugular Vein
• RN started CPN at 80 ml/hour
• After 2 hours: Neck swelling with severe pain
• What went wrong?• RN started CPN / CXR not checked

Case Scenario: CPN
• Adel to start CPN 2 Liters:• Dextrose 8%• Amino Acid 3%• Sodium 80 mmol• Potassium 80 mmol• Ca 6 mmol
• MD ordered to give same formula peripherally
• Can we infuse above formula peripherally?• Always calculate the osmolarity.

Central or Peripheral PN?
• Always calculate the Osmolarity• Dextrose 8% x 50 = 400• Amino Acids 3% x 100 = 300 mOsm/L• Sodium 40 mmol/L x 2 = 80 mOsml/L• Potassium 40mmol/L x 2 = 80 mOsm/L• Calcium 6 mmol/L
• Total = 860 mOsm/L
• Can we infuse peripherally?
• Answer: YES….. Reduce Ca to 2 mmol
• Caution: Monitor venous tolerance.

PN Cholestasis: Treatment & Prevention
• Do not overfeed
• Avoid NPO: Minimal PO even if not tolerated
• Manage Sepsis
• Specialized amino acids
• Omega 3 FA instead of omega 6
• Ursodecoxycholic acid/ Oral Metronidazole
• L-Glutamine*
• Rule out drug-induced
• Reduce Manganese & Copper*Babu R. et al., J Ped Surg. 36(2):282-6, 2001Teitlbaum DH. et al. JPEN 21(2):100-3, 2000Dotty et al. Ann Surg. 210(1):76-80, 1993Kubota A. et al., J Ped Surg 25:618, 1990

• Chwals WJ. New Horiz 2:147-155, 1994
• Clein CG. Et al., J Am Diet Assoc 98:795-806, 1998
• Teitlbaum DH. et al. JPEN 21(2):100-3, 2000
• Babu R. et al., J Ped Surg. 36(2):282-6, 2001
• SCCM & ASPEN Guidelines, Crit Care Med, 37(5), 2009
• Worthington P. et al., 41:324-377, 2017
Additional Literature/References











![Parenteral Nutrition[1]](https://static.fdocuments.us/doc/165x107/5469fe10af79593b558b4f0d/parenteral-nutrition1.jpg)