Back to Basics: Common Errors in Quantitation in Everyday...mitral annulus should be measured from...
14
1 Rebecca T. Hahn, MD Director of Interventional Echocardiography Columbia University Back to Basics: Common Errors in Quantitation in Everyday Practice Core Lab Director for multiple tricuspid device trials for which I receive no direct compensation: SCOUT Trial TriluminateTrial Tri‐Repair Trial Speaker: Abbott Structural, GE, Philips, Boston Scientific Consultant: Gore&Associates, NaviGATE, Abbott Structural, GE, Philips
Transcript of Back to Basics: Common Errors in Quantitation in Everyday...mitral annulus should be measured from...

1
Rebecca T. Hahn, MD
Director of Interventional Echocardiography
Columbia University
Back to Basics: Common Errors in Quantitation in Everyday
Practice
Core Lab Director for multiple tricuspid device trials for which I receive no direct compensation: SCOUT Trial TriluminateTrial Tri‐Repair Trial
Speaker: Abbott Structural, GE, Philips, Boston Scientific
Consultant: Gore&Associates, NaviGATE, Abbott Structural, GE, Philips

2
82 yomale, S/P CABG 10 years ago, S/P AVR for severe, symptomatic aortic stenosis 3 months ago, now presents with increasing DOE and 2+ pitting edema x 3 weeks.
Echo in outside hospital reported normal AVR function, mildly reduced LVEF (50%) and mild MR
On examination: BP = 92/55 mmHg, pulse = 58 bpm Lungs: decreased breath sounds at the bases with bronchial breath
sounds in mid lung field, clear in apices Cardiac: normal S1 with prominent S2. 3/6 high pitched “seagull” type
early systolic murmur, loudest over the apex but radiating throughout the chest
Extremities: 2+ pitting edema at ankles bilaterally

3
Case 1
Vena Contracta = 7.1 mm

4
Case 1
Estimated PASP = 51 mmHgEstimated Mean PAP = 37 mmHg
Case 1

5
Case 1
Case 1

6
4 Chamber
2 Chamber
3 Chamber
Case 1
1. Mild
2. Moderate
3. Severe
4. Cannot tell (need more information)

7
Case 1
MR VTI = 172 cm

8

9
1. Mild
2. Moderate
3. Severe
4. Cannot tell (need more information)
MR PISA radius = 1.1 cmAliasing velocity = 28.8 cm/sMR velocity = 5.4 m/sMR VTI = 172 mmHg
EROA = 40 mm2
Regurgitant volume = 69 cc

10
MV stroke volume = 168 mlLVOT stroke volume = 95 cc
Regurgitant volume = 73 ccEROA = 42 mm2
Regurgitant Volume = 53 cc
Forward (Systolic) Stroke Volume = 83 cc
LVOT = 2.3 cmVTI = 20 cm
Total (Diastolic) Stroke Volume = 145 cc
MV annulus = 3.3 cm
VTI = 16 cm
MV Annulus = 3.3 cm, VTI = 16 cm
Diastolic Stroke Volume =
[0.785 x (3.3)2] x 16 = 136 cc
2D (Biplane) Stroke volume = 136 cc
2D Regurgitant Volume = 53 cc
LVOT annulus = 2.3 cm, VTI = 20 cm
Forward Stroke Volume = [0.785 x (2.3)2]
x 20 = 83 cc

11
Assessment of Forward Stroke Volume
Failure to measure the valve annulus properly (error is squared in the formula)
Failure to trace the modal velocity (brightest signal representing laminar flow) of the pulsed Doppler tracing
Failure to position the sample volume correctly, at the level of the annulus
NOT MEASURING ALL COMPONENTS

12
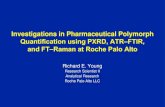
The diameter of the mitral annulus should be measured from the base of the posterior and anterior leaflets during early to mid‐diastole
1 frame after the leaflets begin to close after its initial opening
Quiñones MA, et al. J Am Soc Echocardiogr 2003;16:777‐802
9.4cm2
MA area (cm2) estimated by dilatation(n=33)
No LVdilatation (n=37)
MA area by 3D planimetry
4Ch diameter (circular) R =0.94, P 0.001 R = 0.90, P 0.001
4Ch / 2Ch diameters (ellipse) R=0.95, P 0.001 R = 0.96, P 0.001
4Ch / CC diameters (ellipse) R = 0.96, P 0.001
4Ch / LAX diameters (ellipse) R = 0.96, P 0.001
LAX / CC diameters (ellipse) R = 0.96, P 0.001 R = 0.98, P 0.001
2Ch / LAX diameters (ellipse) R = 0.91, P 0.001
Hyodo E et al. Eur Heart J CV Imaging (2012) 13, 605–611

13
The sample volume is positioned so that in diastole it is at the level of the annulus.
PW flow should be laminar Trace the outer edge of the most
dense (or brightest) portion of the spectral tracing (ie, the modal velocity) and ignore the dispersion that occurs near peak velocity.
Reduce low velocity filters
Quiñones MA, et al. J Am Soc Echocardiogr 2003;16:777‐802
A‐C: annulus or between tips Lower peak velocities and
shorter Mdt E decreasing more than A the
more superior into LA
D: at tips Highest peak velocities
E‐F: in the LV (greater diameter, less laminar flow) Lower peak velocities Spectral broadening Longer Mdt and longer A
duration DiastoleMV Stroke Volume

14
Tips MV
1.85 m/s
MV Annulus
1.6 m/s LA1.4 m/s
ZoghbiWA et al. J Am Soc Echocardiogr 2017; 30: 303‐371.